
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Vet. Sci. , 29 September 2020
Sec. Parasitology
Volume 7 - 2020 | https://doi.org/10.3389/fvets.2020.00571
This article is part of the Research Topic Zoonotic Diseases: Their Hosts and Vectors View all 19 articles
 Sara Savić1*
Sara Savić1* Marina Zekic Stosic1Doroteja Marcic1
Marina Zekic Stosic1Doroteja Marcic1 Isabel Hernández2
Isabel Hernández2 Aleksandar Potkonjak3
Aleksandar Potkonjak3 Suzana Otasevic4
Suzana Otasevic4 Maja Ruzic5
Maja Ruzic5 Rodrigo Morchón2*
Rodrigo Morchón2*Dirofilariasis is a vector-borne zoonotic disease caused mainly by Dirofilaria immitis and Dirofilaria repens that affect dogs and humans all over the world. Serbia is considered an endemic country to both forms of dirofilariasis, although most of the population is concentrated in the north of the country. The aims of this study were to show the prevalence of D. immitis and D. repens in dogs and the seroprevalence in humans compared to previous studies in Northern Serbia. In total, 346 dog sera samples and 265 human samples were analyzed. Dog blood samples were analyzed using the modified Knott's method to check whether there were Dirofilaria spp. microfilariae and serum samples were checked by a commercial D. immitis antigen test. Human serum samples were analyzed with a non-commercial ELISA for detection of specific anti-D. immitis, anti-D. repens, and anti-Wolbachia IgG antibodies, and confirmed by western blotting. The overall prevalence for Dirofilaria spp. in dogs was 29.19%. The overall prevalence for D. immitis was 26.30%. The percentages of D. immitis and D. repens microfilaremia in dogs were 25.72 and 1.45%, respectively, while D. immitis./D. repens microfilaremia co-infections were also 1.45%. The overall seroprevalence for Dirofilaria spp. in humans was 3.77%. The overall seroprevalence for D. immitis was 1.51, 1.13% for D. repens, and for D. immitis/D. repens co-infections was 1.13%. The results indicate that D. immitis and D. repens are present in dogs and humans in the province of Vojvodina, in the northern part of Serbia. It is most likely associated with the presence of many rivers, the climate, and presence of mosquitoes in the area, so there could be a real public health risk.
Dirofilariasis is a vector-borne zoonotic disease caused mainly by Dirofilaria immitis and Dirofilaria repens. Dirofilaria immitis causes heartworm disease in canines and pulmonary dirofilariasis in humans, whereas D. repens causes canine subcutaneous dirofilariasis and ocular/subcutaneous dirofilariasis in humans. Both parasites are transmitted by culicid mosquitoes, which inoculate larva 3 into definitive hosts in both animals and humans. For that reason, dirofilariasis is considered a veterinary and public health problem (1, 2).
Canine heartworm disease is a chronic, progressive, and life-threatening disease in which adult worms stay in the pulmonary artery and the heart, in the right ventricle of definitive hosts. In canine subcutaneous dirofilariasis, the adult worms are usually beneath the skin forming a subcutaneous nodule. In both cases, microfilariae circulate in the blood stream and are ingested by several species of mosquito vectors during their blood-feeding (3) and after two successive molts, during the next blood meal (4), stage-3 larvae are inoculated into the definitive host. In humans, D. immitis immature worms cause embolization in the pulmonary microarteries, leading to the formation of benign lung nodules (pulmonary dirofilariasis), although most cases are asymptomatic (1). On the other hand, D. repens worms do not usually reach the adult stage and immature worms may cause larva migrans syndrome and form subcutaneous nodules, in the ocular region and other organs (1, 3, 5–7). Pulmonary dirofilariasis usually has no clinical symptoms, so most diagnostic tools cannot be used, making it much more difficult to identify. However, subcutaneous/ocular dirofilariasis presents clinical signs that are easier to detect (1, 3). Moreover, D. immitis and D. repens harbor endosymbiotic bacteria of the genus Wolbachia. This bacteria participates in the parasite's life cycle and embryogenesis and plays a key role in the immune and inflammatory response of the organism to the disease (4, 8–10).
Dirofilariasis is on the rise in the European population of dogs and humans (1, 3, 11, 12). It is considered to be an endemic disease in southern European countries and in central and northern countries such as Switzerland, Germany, Netherlands, Lithuania, Slovenia, Czech Republic, Slovakia, and Russia (2, 4, 13–18). In addition, in the last decade, different epidemiological and seroepidemiological studies, alongside clinical reporting, have shown that dirofilariasis has been introduced into the countries of the Balkans peninsula (1, 3, 4, 11, 19). Serbia is considered as an endemic country to both forms of dirofilariasis in dogs (20–24). Few human cases have been reported to be caused by D. repens or have had specific antibodies found (25, 26). To explain the rise of dirofilariasis, studies suggest that red foxes and golden jackals may serve as reservoir hosts (27) and Culex pipiens and Aedes vexans act as vectors of both diseases in Northern Serbia (28).
The aim of this study was to show the prevalence of D. immitis and D. repens in dogs and the seroprevalence in humans compared to previous studies in Northern Serbia.
The northern part of Serbia (Province of Vojvodina) lies between Hungary, Croatia, and Romania. This northern part of the country is largely plains with a continental climate and a lot of rivers. Summers are hot and have lengthened over time due to climate change, so temperatures over 14°C usually last even through to the end of October. Winters are less and less cold and there has not been much snow during the last several winters. All this means that the mosquito season is prolonged from March to October. The air humidity during the warm period of the year is mostly high, meaning that the conditions for the development of mosquitoes are appropriate. During springtime there is a lot of rain and often in some parts of the country there are floods.
In the province of Vojvodina there is the Danube river, which crosses the country from east to west, while the Tisa river flows from north to south, and there are smaller rivers all around the region (Figure 2). There is also an artificial canal system called Danube–Tisa–Danube Canal. It covers the total area in Vojvodina of about 12,700 km2 and it consists of a number of canals. This Canal is a unique hydro-engineering system for flood control and hydrotechnical management, forestry, water supply, wastewater evacuation, navigation, tourism, fishing, and hunting. Besides these purposes, it also represents a substantial amount of water, convenient for development of mosquitos.
We analyzed a total of 611 sera samples: 346 dog sera samples (173 male and 173 female) were obtained from dogs analyzed by several veterinary clinics (Table 1) and 265 human samples (208 male and 57 female) were provided to the research laboratory from different departments of clinical centers in Northern Serbia (Table 2). Human samples were taken from patients with different symptoms, not only those with specific symptoms that could point to dirofilariasis. Variables considered for the analyses were gender, age, and municipality of residence. Samples were collected preserving the privacy of the patients and informing them of how the samples would be used. All samples were collected during the period of 2018 to 2019.
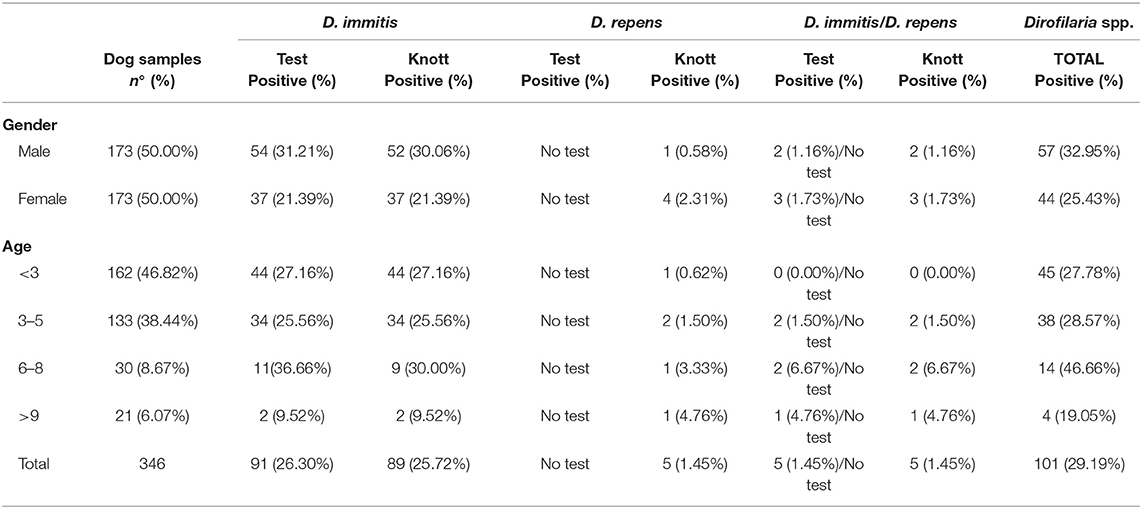
Table 1. Distribution of prevalence of D. immitis, D. repens, and co-infections in dogs in Northern Serbia by gender and age.
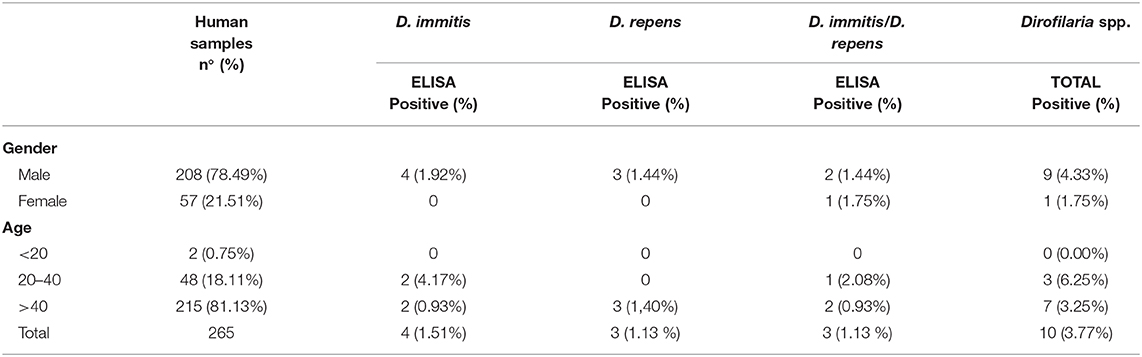
Table 2. Distribution of seroprevalence of D. immitis, D. repens, and co-infections in humans in Northern Serbia by gender and age.
Dog blood samples were analyzed by applying the modified Knott's technique (29) to check whether there were Dirofilaria spp. microfilariae in the blood of the animals included in the study. Morphological characteristics of microfilariae (cephalic and caudal ends) were used in order to differentiate D. immitis and D. repens microfilariae (30). Dog serum samples were tested for the presence of D. immitis adult antigens using a commercial immunochromatographic test kit (VetLine Dirofilaria Antigen, NovaTec, Germany) according to the manufacturer's instructions. There is no commercial laboratory test of any kind for D. repens in dogs.
Human serum samples were analyzed using a non-commercial ELISA for detection of specific anti-D. immitis, anti-D. repens, and anti-Wolbachia IgG antibodies with some modifications (16, 17, 31, 32). D. immitis and D. repens adult worm extracts (DiSA and DrSA, respectively) and 1:100 serum dilutions were used to detect the presence of anti-DiSA and DrSA IgG antibodies. Sera samples diluted at 1:40 with a recombinant form of the Wolbachia Surface Protein (rWSP) were used to detect the presence of anti-rWSP IgG antibodies. In both cases, goat anti-human IgG (H+L) conjugated to horseradish peroxidase (Sigma-Aldrich, Spain) was used at a 1:4000 dilution. Easy Reader (Bio-Rad laboratories, USA) was used for measuring optical densities (OD) at 492 nm. The cut-off point (OD = 0.8 for DiSA and DrSA and 0.5 for rWSP) was determined by calculating the mean value + 3 standard deviations (3SD) of 50 serum samples obtained from dogs and clinically healthy humans (negative controls) who belonged to an area free of D. immitis and D. repens. When both non-commercial ELISAs gave positive results for the same serum sample, that human sera were considered positive. Additionally, by using western blot analysis performed according to a previously described methodology (16, 33–36), these results were confirmed. Both antigenic extracts were subjected to SDS–PAGE in 12% gels under reduced conditions, and proteins were transferred onto nitrocellulose. Human sera were analyzed at a 1:40 dilution and anti-conjugates at a 1:500 dilution. All samples that were positive with these kits were also analyzed by western blot to determine if they recognized the specific bands for D. immitis (17–22 kDa) and for D. repens (43–70 kDa).
The ArcGIS Pro online software was used for the construction of a map of the sampling area. All layers of relevant environmental information (rivers, irrigated croplands, natural parks, among others) were included and symbolized for a better understanding of the map. All dog and human samples infected with D. immitis, D. repens, and co-infections were manually georeferenced by GPS at the point of capture. Georeferenced positive data for both hosts are shown in the map.
The SPSS Base 18.0 software for Windows was used for the data analysis. The descriptive analysis of the considered variables was carried out studying the proportions in the qualitative variables. To compare proportions, Chi-square tests were performed. In all the cases, the significance level was established at p < 0.05.
The overall prevalence for Dirofilaria spp. in dogs was 29.19% (Table 1). The overall prevalence for D. immitis was 26.30%. The percentage of D. immitis microfilaremia in dogs was 25.72% (in all cases with a positive D. immitis antigen test), 1.45% for D. repens microfilaremia, and 1.45% for D. immitis/D. repens microfilaremia co-infections (in all cases with a positive D. immitis antigen test). There are significant differences between the prevalence for D. immitis infected male and female dogs with a higher prevalence in male dogs, whereas the prevalence of D. repens was higher in females (p < 0.05).
The overall seroprevalence for Dirofilaria spp. in humans was 3.77%. These results are shown in Table 2. The overall seroprevalence for D. immitis was 1.51, 1.13% for D. repens, and 1.13% for D. immitis/D. repens co-infections. All positive cases were detected in males with significant differences (p < 0.05) for D. immitis (1.92%) and D. repens (1.44%), but not in co-infection (1.44%). All positive samples via western blot analysis are shown in Figure 1.
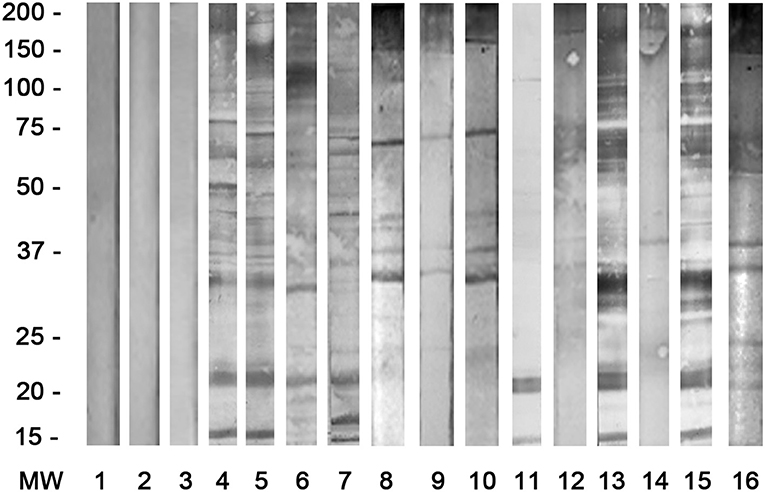
Figure 1. Western blot in all human seropositive cases for D. immitis (4–7) with specific bands at 17–22 kDa; for D. repens (8–10) with bands at 43–70 kDa; for co-infections D. immitis/D. repens (11/12, 13/14, 15/16), and negative sera (1–3).
By age, there are significant differences between the seroprevalences of D. immitis between the 20–40 range and the other ranges, the seroprevalences of D. repens between the over-40 age group and the other ranges and the seroprevalences of co-infections between the 20–40 age group and the other ranges (p < 0.05).
Regarding the geolocation of the positive samples of both dogs and people on a map (Figure 2), all of them were located in the vicinity of rivers, forest parks, green areas, and even within some cities in northern Serbia. There are only two cases of humans infected with D. immitis and D. repens in the northeast of the country.
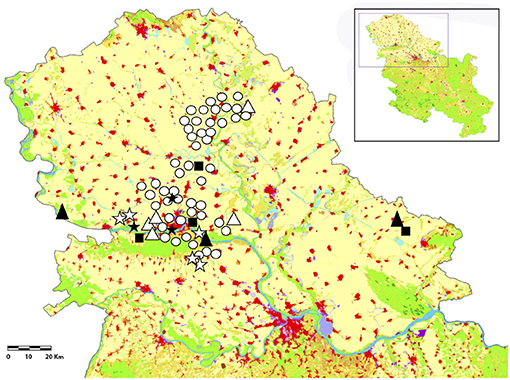
Figure 2. Localization of the D. immitis and D. repens positive dogs and humans and co-infections in Northern Serbia: D. immitis in dogs (O), D. repens in dogs (Δ), D. immitis/D. repens in dogs (⋆), and D. immitis in humans (■), D. repens in humans (▴), and D. immitis/D. repens in humans (⋆). In green (natural grasslands, mixed forest, broad-leaved forest, moors and heathland, parks, forest parks), in red (continuous and discontinuous urban areas) and in blue (rivers, areas of stagnant water, and water bodies).
Wherever canine dirofilariasis exists, there is a risk of human infection. The general climatic conditions, local environmental factors, human interventions on the environment, and pet management are also factors that determine the distribution and incidence of illness (36). Humans and Dirofilaria spp. species have developed limited mutual adaptation (1). L3s inoculated by mosquitoes are usually eliminated from the host by the immune system. However, an undetermined percentage survives and continues to develop until pre-adult, and in some cases of D. repens, until adult, causing pulmonary and subcutaneous nodules or sometimes in the eye area, encapsulated or non-encapsulated. In any case, contact with the infecting larvae and subsequent stages of development stimulates an immune response that can be measured with appropriate techniques (37).
Epidemiological studies of human dirofilariasis, unlike in the dog population, have followed two different approaches. One is reported retrospective reviews and the other is seroepidemiological analyses. Each of these approaches provides information on different yet complementary aspects of human infections. The information obtained through retrospective reviews of reported cases offer only a partial view, since it only includes the part of the affected population that develops some type of clinical manifestation, and regions of endemicity showing vectors with zoo-anthropophilic habits probably have higher frequencies of human infections than reported in the literature. The problem of underreporting may exist due to the fact that symptoms in dirofilariasis patients, especially in pulmonary infections, may be misdiagnosed or unnoticed (1). Seroepidemiological studies compliment this information by detecting contact through the measurement of anti-Dirofilaria antibodies, allowing the evaluation of the risk of dirofilariasis infection in a defined geographical region, and constituting an excellent measure of the risk of infection for the human population which resides in an endemic area. Seroepidemiological studies of residents of areas of endemicity reported higher rates of infection in a similar manner to those of canines of the same areas (1, 5, 13, 16, 17, 34).
The aim of the present study was to analyze the prevalence in dogs and the response to anti-D. immitis and/or anti-D. repens antibodies in the northern region of Serbia (Vojvodina), taking into account that this region has been considered endemic for some time. Furthermore, the aim was to identify the potential risk of infection of the human population in an endemic area.
In Serbia, humidity and temperature conditions during a large proportion of the year allow for the transmission of dirofilariasis, with seroepidemiological data revealing noteworthy prevalence rates in the country's dog populations and human clinical cases caused by both D. immitis and D. repens (1, 3, 24).
In the current study, a prevalence of 26.30% was observed in dogs infected by D. immitis, with 25.72% microfilaremia in the total population, and the presence of D. repens larvae in 1.45% of the analyzed dogs. In two regions of Vojvodina (Pancevo and Veliko Gradiste), the previously reported seroprevalence was 22.9% for D. immitis and the presence of D. repens microfilariae was 39.34% (38). In Bulgaria and Croatia, two neighboring countries, there are studies about the prevalence of D. immitis and D. repens in dogs (8.1 and 11.1%, respectively) and co-infections (3.2%) (11). Several studies point to an increase in D. immitis infections and a decrease of an infection with D. repens in recent years (21–23) which is corroborated by results in this study. In addition, infections have also been found to be prevalent in wild canids (39), which could mean there is a risk of D. immitis infection between the dog population and the wild canid population. Meanwhile, D. repens was found to circulate mostly in golden jackal and red fox populations (27).
With regards to the human population, the seroprevalence for Dirofilaria spp. in humans was 3.77, 1.51% for D. immitis, 1.13% for D. repens, and 1.13% for D. immitis/D. repens co-infections. This is the first time these tests have been conducted in this region of Serbia. Human cases originating from D. repens have only previously been reported in the region of southeastern Serbia (24, 40, 41). In addition, other studies have reported seroprevalences of 9.7% and 8.1% against D. repens and D. immitis polyproteins specific antibodies, respectively, and 2.3% in individuals with specific antibodies to both species (26). Similar studies in neighboring countries such as Romania and Moldova have reported seroprevalences of 10.7% for D. immitis, 0.2% for D. repens, and 0.9% for both parasites (16). In addition, in Croatia there have been human D. repens cases reported (3). These seroepidemiological studies are a good tool to measure the risk of infection in a population where there is a high population of infected animals, as well as the presence of vectors, which serve as a vehicle for transmission of the disease (1, 42).
Both animals and infected people were geolocated in the immediate vicinity or in a relatively close environment of potential mosquito breeding areas, which poses a risk to those areas. The two cases of humans infected by D. immitis and D. repens in the northeast of the country are close to cities where cases of dogs and humans had already been reported (38) and were located in areas near rivers and green areas where mosquitoes breed. The spatial distribution of positive cases has a clear association with different geo-environmental factors, humidity and temperature, the existence of irrigated areas, areas with abundant water, rivers in valleys protected from winds, and proximity to the coast, which are considered risk factors for the transmission of dirofilariasis (43).
In conclusion, the results indicate that D. immitis and D. repens are present in dogs and humans in the province of Vojvodina, in the northern part of Serbia. It is most probably associated with the presence of many rivers, the climate, and the presence of mosquitoes, so there is a real public health risk. Serology studies in humans can be very useful for indicating the exposure to Dirofilaria spp. in a healthy population in order to obtain useful data on the epidemiological scenario of human dirofilariasis in Serbia and in Europe. That exposure was confirmed in the current study. Further studies addressing the control of dirofilariasis in the dog population are needed to reduce the risk of infection in the human population.
All datasets generated for this study are included in the article/supplementary material.
Ethical approval was not provided for this study on human participants because People data don't require permission, everyone has verbal consent. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. Ethical review and approval was not required for the animal study because the blood samples were taken during a regular blood checkup of the dogs and the consent was gained from the owners so there was no need for the ethical approval. Written informed consent for participation was not obtained from the owners because Verbal consent of client owned dogs.
SS and RM designed the study and wrote the manuscript. MS, DM, IH, AP, SO, and MR performed the fieldwork, collected the data, and performed the experiments. All authors participated in the discussion of the results, corrected, read, and approved the final manuscript.
The presented work is part of research done for the project TR31084 granted by the Serbian Ministry of Education and Science and Agencia de Desarrollo Económico de Castilla y León (co-funded by FEDER funds), Spain.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer AG declared a past co-authorship with one of the authors SS to the handling editor.
We would like to thank the staff of veterinary clinics and the different departments of human clinics for their assistance in obtaining blood and serum samples from dogs and humans.
1. Simón F, Siles-Lucas M, Morchón R, González-Miguel J, Mellado I, Carretón E, et al. Human and animal dirofilariasis: the emergence of a zoonotic mosaic. Clin Microbiol Rev. (2012) 25:507–44. doi: 10.1128/CMR.00012-12
2. Genchi C, Kramer L. Subcutaneous dirofilariasis (Dirofilaria repens): an infection spreading throughout the old world. Parasit Vectors. (2017) 10:517. doi: 10.1186/s13071-017-2434-8
3. Capelli G, Genchi C, Baneth G, Bourdeau P, Brianti E, Cardoso L, et al. Recent advances on Dirofilaria repens in dogs and humans in Europe. Parasit Vectors. (2018) 11:663. doi: 10.1186/s13071-018-3205-x
4. Morchón R, Carretón E, González-Miguel J, Mellado-Hernández I. Heartworm disease (Dirofilaria immitis) and their vectors in Europe - new distribution trends. Front Physiol. (2012) 3:196. doi: 10.3389/fphys.2012.00196
5. Kartashev V, Batashova I, Kartashov S, Ermakov A, Mironova A, Kuleshova Y, et al. Canine and human dirofilariasis in the rostov region (southern Russia). Vet Med Int. (2011) 2011:685713. doi: 10.4061/2011/685713
6. Ilyasov B, Kartashev V, Bastrikov N, Morchón R, González-Miguel J, Simón F. Delayed diagnosis of dirofilariasis and complex ocular surgery, Russia. Emerg Infect Dis. (2013) 19:326–8. doi: 10.3201/eid1902.121388
7. Ilyasov B, Kartashev V, Bastrikov N, Madjugina L, González-Miguel J, Morchón R, et al. Thirty cases of human subcutaneous dirofilariasis reported in Rostov-on-Don (Southwestern Russian Federation). Enferm Infecc Microbiol Clin. (2015) 33:233–7. doi: 10.1016/j.eimc.2014.04.002
8. Kramer LH, Tamarozzi F, Morchón R, López-Belmonte J, Marcos-Atxutegi C, Martín-Pacho R, et al. Immune response to and tissue localization of the Wolbachia surface protein (WSP) in dogs with natural heartworm (Dirofilaria immitis) infection. Vet Immunol Immunopathol. (2005) 6:303–8. doi: 10.1016/j.vetimm.2005.03.011
9. Grandi G, Morchón R, Kramer L, Kartashev V, Simón F. Wolbachia in Dirofilaria repens, an agent causing human subcutaneous dirofilariasis. J Parasitol. (2008) 94:1421–3. doi: 10.1645/GE-1575.1
10. Simón F, Kramer LH, Román A, Blasini W, Morchón R, Marcos-Atxutegi C, et al. Immunopathology of Dirofilaria immitis infection. Vet Res Commun. (2007) 31:161–71. doi: 10.1007/s11259-006-3387-0
11. Farkas R, Mag V, Gyurkovszky M, Takács N, Vörös K, Solymosi N. The current situation of canine dirofilariasis in Hungary. Parasitol Res. (2020) 119:129–35. doi: 10.1007/s00436-019-06478-5
12. Velev V, Vutova K, Pelov T, Tsachev I. Human Dirofilariasis in Bulgaria between 2009 and 2018. Helminthologia. (2019) 56:247–51. doi: 10.2478/helm-2019-0016
13. Kartashev V, Tverdokhlebova T, Korzan A, Vedenkov A, Simón L, González-Miguel J, et al. Human subcutaneous/ocular dirofilariasis in the Russian Federation and Belarus, 1997-2013. Int J Infect Dis. (2015) 33:209–11. doi: 10.1016/j.ijid.2015.02.017
14. Diosdado A, Gómez PJ, González-Miguel J, Simón F, Morchón R. Current status of canine dirofilariasis in an endemic area of western Spain. J Helminthol. (2018) 92:520–3. doi: 10.1017/S0022149X17000591
15. Miterpáková M, Valentová D, Cabanová V, Berešíková L. Heartworm on the rise-new insights into Dirofilaria immitis epidemiology. Parasitol Res. (2018) 117:2347–50. doi: 10.1007/s00436-018-5912-9
16. Ciuca L, Simón F, Rinaldi L, Kramer L, Genchi M, Cringoli G, et al. Seroepidemiological survey of human exposure to Dirofilaria spp. in Romania and Moldova. Acta Trop. (2018) 187:169–74. doi: 10.1016/j.actatropica.2018.07.012
17. Fontes-Sousa AP, Silvestre-Ferreira AC, Carretón E, Esteves-Guimarães J, Maia-Rocha C, Oliveira P, et al. Exposure of humans to the zoonotic nematode Dirofilaria immitis in northern Portugal. Epidemiol Infect. (2019) 147:e282. doi: 10.1017/S0950268819001687
18. Sabunas V, Radzijevskaja J, Sakalauskas P, Petkevičius S, Karveliene B, Žiliukiene J, et al. Dirofilaria repens in dogs and humans in Lithuania. Parasit Vectors. (2019) 12:177. doi: 10.1186/s13071-019-3406-y
19. Ionică AM, Matei IA, D'Amico G, Ababii J, Daskalaki AA, Sándor AD, et al. Filarioid infections in wild carnivores: a multispecies survey in Romania. Parasit Vectors. (2017) 10:332. doi: 10.1186/s13071-017-2269-3
20. Savić-Jevdenić S, Vidić B, Grgić Ž, Milovanović A. Brza dijagnostika dirofilarioze pasa u regionu Novog Sada. Vet Glasnik. (2004) 58:693–8.
21. Tasić A, Rossi L, Tasic-Otasevic S, Miladinovic-Tasic N, Ilic T, Dimitrijevic S. Survey of canine dirofilariasis in Vojvodina, Serbia. Parasitol Res. (2008) 103:1297–302. doi: 10.1007/s00436-008-1132-z
22. Spasojević-Kosić LJ, Lalošević V, Lalošević D, Simin S, Vasić I, Kuruca LJ. Prevalence of dirofilariasis in pet dogs in Novi Sad. Contemp Agric. (2012) 61:247–54.
23. Spasojević-Kosić LJ, Lalošević V, Simin, Kuruca LJ. Dirofilariasis and Angiostrongilosis in pet and hunting dogs in Novi Sad, Vojvodina, Serbia. Arhiv Vet Med. (2016) 9:53–62. doi: 10.46784/e-avm.v9i2.89
24. Krstić M, Gabrielli S, Ignjatović M, Savić S, Cancrini G, Randelović G, et al. An appraisal of canine and human cases reveals an endemic status of dirofilariasis in parts of Serbia. Mol. Cell Probes. (2017) 31:37–41. doi: 10.1016/j.mcp.2016.08.005
25. DŽamić AM, Colović IV, Arsić-Arsenijević VS, Stepanović S, Boričić I, DŽamić Z, et al. Human Dirofilaria repens infection in Serbia. J Helminthol. (2009) 83:129–37. doi: 10.1017/S0022149X09341346
26. Tasić-Otašević SA, Gabrielli SV, Tasić AV, Miladinovićtasić NL, Kostić JT, Ignjatović AM, et al. Seroreactivity to Dirofilaria antigens in people from different areas of Serbia. BMC Infect Dis. (2014) 14:68. doi: 10.1186/1471-2334-14-68
27. Potkonjak A, Rojas A, Gutiérrez R, Nachum-Biala Y, Kleinerman G, Savić S, et al. Molecular survey of Dirofilaria species in stray dogs, red foxes and golden jackals from Vojvodina, Serbia. Comp Immunol Microbiol Infect Dis. (2020) 68:101409. doi: 10.1016/j.cimid.2019.101409
28. Kurucz K, Kepner A, Krtinic B, Zana B, Földes F, Bányai K, et al. First molecular identification of Dirofilaria spp. (Onchocercidae) in mosquitoes from Serbia. Parasitol Res. (2016) 115:3257–60. doi: 10.1007/s00436-016-5126-y
29. Acevedo RA, Theis JH, Kraus JF, Longhurst WM. Combination of filtration and histochemical stain for detection and differentiation of Dirofilaria immitis and Dipetalonema reconditum in the dog. Am J Vet Res. (1991) 42:537–40.
30. Genchi G, Venco L, Genchi M. Guideline for the laboratory diagnosis of canine and feline Dirofilaria infections. In: Genchi C, Rinaldi L, Cringoli G, editors. Mappe Parassitologighe 8, Dirofilaria immitis and Dirofilaria repens in dog and cat and human infection, eds. Rolando Editore, Salamanca (2007). p. 137–45.
31. Simón F, Muro A, Cordero M, Martin J. A seroepidemiologic survey of human dirofilariasis in Western Spain. Trop Med. arasitol. (1991) 42:106–8.
32. Simón F, Prieto G, Morchón R, Bazzocchi C, Bandi C, Genchi C. Immunoglobulin G antibodies against the endosymbionts of filarial nematodes (Wolbachia) in patients with pulmonary dirofilariasis. Clin Diagn Lab Immunol. (2003) 10:180–1. doi: 10.1128/CDLI.10.1.180-181.2003
33. Perera L, Muro A, Cordero M, Villar E, Simón F. Evaluation of a 22kDa Dirofilaria immitis antigen for the immunodiagnosis of human pulmonary dirofilariasis. Trop Med Parasitol. (1994) 45:249–52.
34. Perera L, Pérez-Arellano JL, Cordero M, Simón F, Muro A. Utility of antibodies against a 22 kD molecule of Dirofilaria immitis in the diagnosis of human pulmonary dirofilariasis. Trop Med Int Health. (1998) 3:151–5. doi: 10.1046/j.1365-3156.1998.00209.x
35. Santamaría B, Cordero M, Muro A, Simón F. Evaluation of Dirofilaria immitis excretory/secretory products for seroepidemiological studies on human dirofilariasis. Parasite. (1995) 2:269–73.
36. Simon F, Prieto G, Muro A, Cancrini G, Cordero M, Genchi C. Human humoral immune response to Dirofilaria species. Parassitologia. (1997) 39:397–400.
37. Carretón E, Morchón R, Montoya-Alonso JA. Chapter 1. Dirofilariasis cardiopulmonar canina. In: Montoya-Alonso JA, Carretón E, editors. Dirofilariasis. Pautas de Manejo Clínico. Barcelona: Multimédica Ediciones Veterinarias (2012). p. 1–130.
38. Tasić A, Tasić-Otašević S, Gabrielli S, Miladinović-Tasić N, Ignjatović A, Dordević J, et al. Canine Dirofilaria infections in two uninvestigated areas of Serbia: epidemiological and genetic aspects. Vector Borne Zoonot Dis. (2012) 12:1031–5. doi: 10.1089/vbz.2011.0949
39. Cirović D, Penezić A, Pavlović I, Kulišić Z, Cosić N, Burazerović J, et al. First records of Dirofilaria repens in wild canids from the region of central Balkan. Acta Vet Hung. (2014) 62:481–8. doi: 10.1556/avet.2014.021
40. Dzamić AM, Arsić-Arsenijević V, Radonjić I, Mitrović S, Marty P, Kranjcić-Zec IF. Subcutaneous Dirofilaria repens infection of the eyelid in Serbia and Montenegro. Parasite. (2004) 11:239–40.
41. Tasić S, Stoiljković N, Miladinović-Tasić N, Tasić A, Mihailović D, Rossi L, et al. Subcutaneous dirofilariasis in south-east Serbia - case report. Zoonoses Public Health. (2011) 58:318–22. doi: 10.1111/j.1863-2378.2010.01379.x
42. Cabrera E, Carretón E, Morchón R, Falcón-Cordón Y, Falcón-Cordón S, Simón F, et al. The Canary Islands as a model of risk of pulmonary dirofilariasis in a hyperendemic area. Parasitol Res. (2018) 117:933–6. doi: 10.1007/s00436-018-5774-1
43. Simón L, Afonin A, López-Díez LI, González-Miguel J, Morchón R, Carretón E, et al. Geo-environmental model for the prediction of potential transmission risk of Dirofilaria in an area with dry climate and extensive irrigated crops. The case of Spain. Vet Parasitol. (2014) 200:257–4. doi: 10.1016/j.vetpar.2013.12.027
Keywords: Dirofilaria immitis, Dirofilaria repens, Serbia, dogs, humans, prevalence, seroprevalence, Europe
Citation: Savić S, Stosic MZ, Marcic D, Hernández I, Potkonjak A, Otasevic S, Ruzic M and Morchón R (2020) Seroepidemiological Study of Canine and Human Dirofilariasis in the Endemic Region of Northern Serbia. Front. Vet. Sci. 7:571. doi: 10.3389/fvets.2020.00571
Received: 11 March 2020; Accepted: 17 July 2020;
Published: 29 September 2020.
Edited by:
David Modrý, University of Veterinary and Pharmaceutical Sciences Brno, CzechiaReviewed by:
Martina Miterpáková, Institute of Parasitology (SAS), SlovakiaCopyright © 2020 Savić, Stosic, Marcic, Hernández, Potkonjak, Otasevic, Ruzic and Morchón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sara Savić, c2FyYUBuaXYubnMuYWMucnM=; Rodrigo Morchón, cm1vcmdhckB1c2FsLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.