 Raoul Muteganya
Raoul Muteganya Serge Goldman1
Serge Goldman1 Simone Albisinni
Simone Albisinni
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg. , 07 December 2018
Sec. Genitourinary Surgery
Volume 5 - 2018 | https://doi.org/10.3389/fsurg.2018.00074
This article is part of the Research Topic Lymph Node Dissection in Uro-Oncology View all 6 articles
Introduction: Lymph node metastases (LNM) represent a proven prognostic factor for biochemical recurrence (BCR)-free survival, metastatic free survival and overall survival in prostate cancer (PCa). Although pelvic node dissection remains the gold standard for the detection of LNM, novel imaging techniques are entering clinical practice, in the effort to improve LNM detection and spare unnecessary surgeries. Aim of the current review is to describe such imaging techniques and explore their advantages and limitations.
Evidence Acquisition: The National Library of Medicine Database was searched for relevant articles published between January 2013 and August 2018. A wide search was performed including the combination of following words: “Prostate” and “Cancer” and “staging” and “Lymph Node” and “imaging” and (“MRI” or “PET”). The initial list of selected papers was enriched by individual suggestions of the authors of the present review.
Evidence Synthesis: DWI-MRI in detection of lymph node invasion has a sensitivity and specificity of 41 and 94%, respectively. For SPIO MRI using ferumoxtran-10, the sensitivity for detection of LNM with short axis diameter of 5–10 mm is reported at 96.4%, compared to 28.5% with MRI alone. PSMA PET/CT is growing exponentially, both in the initial detection of LNM and for BCR evaluation. Fluciclovine PET could improve detection of subcentimetric pathologic lymph nodes. Sentinel lymph node techniques remain experimental and not validated in the field of PCa.
Conclusions: Molecular imaging, particularly PSMA ligand PET imaging, present interesting diagnostic accuracy in LN diagnosis even in subcentimetric LN. DWI-MRI yields good results in LN involvement evaluation and the use of contrast agent such SPIO may improve the detection rate. The SLN technique is limited to experimental protocols and for intermediate or high-risk PCa. Prospective trials are awaited to evaluate the true clinical impact of these imaging techniques on PCa oncologic outcomes.
In men, prostate cancer (PCa) represents the second cause of cancer and the fifth leading cause of cancer-related death worldwide (1). Tumor lymph node metastasis (LNM) is proven to be a prognostic factor for biochemical recurrence (BCR)-free survival, metastatic free survival and overall survival (OS) in PCa (2). Currently, pelvic lymph node dissection (PLND) is the gold standard for the evaluation of the lymph node extension and is recommended for patients harboring high-risk prostate cancer and also for intermediate risk if the estimated risk for a positif lymph node invasion exceed 5% (3). Multiple validated nomograms (4, 5) are currently employed by surgeons to decide whether PLND should be performed. The accepted recommendation is that if risk of LNM exceeds 5%, a PLND should be performed at the time of radical prostatectomy (3). Nonetheless, PLND is not devoid of complications (6, 7) and to date many patients undergo the procedure although harboring specimen confined disease, with limited oncologic advantage and undoubted increase in surgical time and morbidity (8, 9). Various radiological and nuclear medicine imaging techniques have been proposed to evaluate the pre-operatory lymph node staging but also for the evaluation of tumor lymph node invasion in case of biochemical recurrence (BCR). However, to date, the ideal exam does not yet exist: indeed, a highly sensitive imaging exam, limiting false negative cases, would be greatly welcomed by the urologic surgical community, in order to identify those patients who truly need PLND, and sparing the others from the procedure.
The aim of this review is to give an overview of the role of radiological and molecular imaging currently used in lymph node staging for PCa, and to explore future directions of research in this field.
The National Library of Medicine Database was searched for relevant articles published between January 2013 and August 2018. A wide search was performed including the combination of following words: “Prostate” AND “Cancer” AND “staging” AND “Lymph Node” AND “imaging” AND (“MRI” OR “PET”). Although recent articles were prioritized, works with relevant historical findings were referenced if necessary. Only publications in English language were considered and evidence was limited to human data. Each article's title, abstract and text were reviewed for their appropriateness and their relevance. The initial list of selected papers was enriched by individual suggestions of the authors of the present review. Table 1 presents a synoptic view of available techniques.
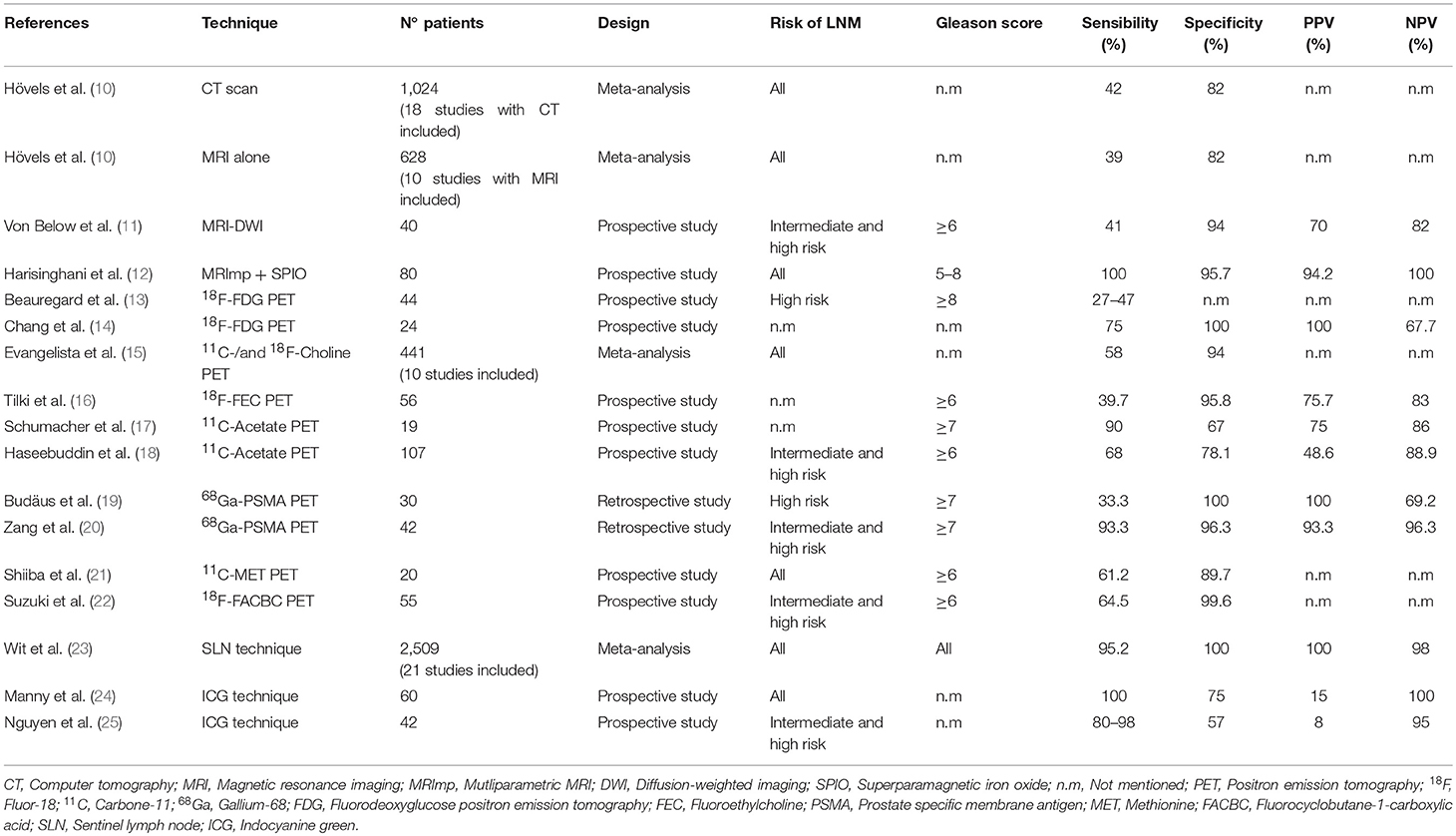
Table 1. Different imaging techniques for lymph node staging in prostate cancer.
CT and MRI, with cross sectional imaging, use morphological characteristics for the nodal staging, such as size and shape (oval or round) of the node. The criteria used as indicators of metastatic node are a diameter, in short axis, >1 cm for oval nodes and >0.8 cm for round nodes (26). With such criteria, a meta-analysis found that for detection of positive nodes, CT has a pooled sensitivity of 42% and a specificity of 82% and MRI a sensitivity of 39% and a specificity of 82% (10), thus confirming the limited value of morphological exams in LN staging. MRI, however, offers the possibility to evaluate other nodal characteristics, such as the “Apparent Diffusion Coefficient” (ADC) calculated via diffusion-weighted imaging (DWI), which pictures the Brownian movements of water's molecule. Moreover, another technique currently employed in MRI for pathologic node detection is the use of superparamagnetic iron oxide (SPIO) nanoparticles that can be used as contrast agents for improving LNM detection sensitivity.
In DWI sequences, MRI may be performed without any contrast agent and malignant tissue tends to have restricted water diffusion due to increased cellularity, enlarged nuclei, macromolecular proteins in the cytoplasm and extracellular disorganization. Malignant lesions appear hyperintense at high coefficient values (b-value of 800–1,000 s/mm2) and hypointense on the ADC maps (lower ADC value). Nonetheless, DWI-MRI can misclassify necrotic lymph nodes due to free diffusion of water, which was described in a study on diagnostic accuracy of MRI of lymph node metastasis in the neck (27). A recent prospective study using the combination of morphological criteria and DWI sequence on a 3T MRI showed a specificity of 94% and a sensitivity of 41% for the detection of LNM (11).
In SPIO MRI, nanoparticles are avidly taken up by macrophages. When a lymph node is metastatic, there is a paucity of macrophages and therefore a reduced uptake of SPIO. SPIO causes a loss of signal on T2 weighted image; as such, benign lymph nodes appear dark while metastatic nodes appear bright. After injection of SPIO nanoparticles, the lymphatic areas are analyzed on T2-weighted fast spin-echo or gradient-echo sequences. The initial studies with SPIO were performed with Ferumoxtran-10; however, this compound did not receive FDA approval. Ferumoxytol, on the other hand, is a new SPIO agent that has been tested for detection of malignant lymph node, which already had FDA and EMA approvals for iron replacement therapy in patients with chronic kidney failure. SPIO nanoparticles increase the sensitivity compared to MRI alone from 45 to 100% with 95.7% specificity in the sentinel lymph node detection (28). They also demonstrated the ability to detect metastatic lymph nodes with < 7 mm diameter in short axis (29). The initial study using ferumoxtran-10 reported a sensitivity for detection of malignant lymph nodes with short axis diameter of 5–10 mm of 96.4% (compared to 28.5% with MRI alone) (12). However, Ferumoxytol is not approved for MR imaging and currently, SPIO MRI remains in research field with no clinical routine application.
The combination of DWI sequences and administration of SPIO represent promising techniques for the evaluation of LNM. The combination of DWI-MRI and SPIO contrast agent improves the sensitivity and the specificity and it decreases the time needed for interpreting images (30).
PET imaging offers a better spatial resolution than planar scintigraphy and single photon emission computed tomography (SPECT). Multiple radiotracers have been explored and are currently tested in the field of prostate cancer.
18F-Fluorodeoxyglucose (18F-FDG), the most used in oncological investigations, that explores glucose consumption by malignant cells with increased glycolytic activity, has limited utility in PCa due to low metabolic activity of PCa cells particularly in the early phase of disease (31). It can be useful for the detection of metastatic lesions (32) or in poorly differentiated PCa (33). A study analyzing intermediate and high risk PCa, reported that 18F-FDG PET had a sensitivity of 80% and a positive predictive value (PPV) of 87% for detection of primary lesion in case of Gleason score ≥7 (34). In the Beauregard et al. study on pre-operative staging with FDG PET for high grade PCa, 41 patients had ePLND, 11 of them had LN metastasis at histological analysis but FDG PET detected only 3 of those (27%) with LNM pathology-proven, if non-surgical LN FDG were included and suspicion confirmed by response to ADT, the sensitivity were evaluated to 47%. Moreover, FDG PET found 7 patients with suspected LNM but only 3 were confirmed histologically (13). In the Chang et al. study on the role of FDG PET to detect LNM in case of PSA relapse after treatment for localized PCa, they find a sensitivity, specificity, PPV and NPV of 75, 100, 100, and 67.7%, respectively (14). The literature is limited on the diagnostic accuracy of FDG PET in LN staging for PCa, but it still probably have a place in the staging for advanced PCa with high Gleason score or undifferentiated PCa. A further disadvantage of 18F-FDG is the urinary excretion of this tracer that can potentially decrease the sensitivity for the detection of pelvic lesions. Therefore, 18F-FDG PET plays a particularly limited role in the detection of pelvic lymph node metastases.
Other radiotracers have been studied for PCa imaging at initial staging and BCR. The most studied are choline derivatives radiolabeled with Carbone-11 (11C) or Fluor-18 (18F). Choline is naturally incorporated into tumor cells after phosphorylation by choline kinase that is upregulated in malignant PCa cells (35). Choline derivatives show minimal urinary excretion and therefore less activity in the bladder compared to 18F-FDG.
In a meta-analysis 11C-Choline PET presented a performance for detecting lymph node metastases with a pooled sensitivity of 58% and a pooled specificity of 94%. 18F-Choline, on the other hand, had a lower sensitivity (40 vs. 58% for 11C-Choline, respectively) but improved specificity (96 vs. 94% for 11C-Choline) (15). Tilki et al. performed a study on detection rate for 18F-Fluoroethylcholine with a lesion-based analysis in 1,149 lymph nodes. The result was a sensitivity of 39.7% and a specificity of 95.8% with a NPV of 83% and a PPV of 75.7%, respectively (16). Globally, 11C- or 18F- radiolabeled choline derivatives present similar performances for detection of LN invasion. However, detection rates increase with increasing PSA serum levels and in the Mitchell et al. study they found that the optimal PSA serum level for lesion detection in case of BCR was a value ≥2 ng/ml (36). Currently, the EAU recommend PET imaging with choline derivatives for BCR after radical prostatectomy with PSA serum level ≥1 ng/ml (37).
Acetate PET imaging explores the fatty acid metabolic pathway which is overexpressed in PCa (38). Acetate is a naturally present fatty acid precursor and is converted to acetyl-CoA that is incorporated into cholesterol and fatty acids. Most studies have been performed using 11C-Acetate PET imaging. The major elimination route is through the respiratory system with a lack of significant renal activity (39). Therefore, imaging can be performed without interference of urinary activity. Nonetheless, as 11C presents a half time of 20 min, its use is limited to centers equipped with a cyclotron.
Schumacher et al. analyzed the performance of 11C-Acetate PET/CT: Sensitivity, specificity, PPV and NPV were calculated at 90, 67, 75, and 86%, respectively. The nodal-region-based sensitivity was 62% with a specificity of 89% and a PPV of 62% with a NPV of 89% (17). Haseebuddin et al. evaluated 11C-Acetate PET/CT in 107 men with intermediate and high-risk PCa, reporting a performance for pathologic lymph node involvement with a sensitivity of 68% and a specificity of 78% with a PPV of 49% and a NPV of 89% (18). Compared to choline derivative PET imaging, studies found no significant difference in detection rate between 11C-Acetate and 18F-Choline PET/CT in case of BCR with low PSA level (40). To date there is no clear evidence that 11C-Acetate PET/CT performs better than choline derivatives in lymph node staging, and both tracers present increased detection with increasing PSA serum level.
PSMA is a transmembrane type II glycoprotein also called folate hydrolase I or glutamate carboxipeptidase II, which has a 19-amino-acid intracellular portion, a 24-amino-acid transmembrane portion and a 707-amino-acid extracellular portion (41). PSMA is expressed by prostate cells and overexpressed in PCa cells. The first PSMA imaging agent used was ProstaScintTM, an 111Indium-labeled monoclonal antibody. This PSMA target was an intracellular domain of PSMA, therefore targeting antigens only accessible in apoptotic or necrotic cells (not viable tissue) where the membrane was permeable with limited sensitivity and specificity (42, 43). Furthermore, the ProstascintTM showed slow kinetics requiring imaging 5–7 days after the injection.
Recently, novel small molecules targeting the extracellular domain of PSMA have been developed such as:
• N-{N-[(S)-1,3-dicarboxypropyl] carbamoyl}-4-(18F)fluoro benzyl-L-cysteine [(18F)DCFBC],
• 68Ga-N,N′-bis [2-hydroxy5-(carboxyethyl)benzyl] ethylenediamine-N,N′-diacetic acid (HBED-CC)
• 2-(3-(1-carboxy-5-[(6-[18F]fluoro-pyridine-3-carbonyl)-amino]-pentyl)-ureido)-pentanedioic acid ([18F]DCF PyL)
• EuK-Subkff-68Ga-DOTAGA (68Ga-PSMA I&T)
The most widely used and studied PSMA tracer is 68Ga-PSMA (HBED-CC), with multiple PET/CT studies analyzing the diagnostic value of PSMA ligand radiotracer in lymph node detection in case of BCR. Budaus et al. retrospectively evaluated the diagnostic value of PSMA PET/CT in preoperative high-risk PCa. The overall sensitivity, specificity, PPV, and NPV were 33.3, 100, 100, and 69.2%, respectively (19). In their study, the authors also reported that the detection rate varied with the median size of LNM. The false negative LN metastases had a median diameter of 4.3 mm (vs. 13.6 mm for the positive nodes) (19).
Zang et al. explored PSMA in intermediate and high-risk PCa: the pre-operative 68Ga-PSMA PET/CT lymph node diagnostic value showed a sensitivity of 93.3% with a specificity of, 96.3%, and a PPV of 93.3% with a NPV of 96.3%, on patient-based analysis. On LN-based analysis, sensitivity, specificity, PPV and NPV were 96.1, 99.6, 96.1, and 99.6%, respectively (20).
In PCa patients with BCR, Eiber et al. found detection rates of 96.8, 93.0, 72.7, and 57.9% for PSA values of ≥2, 1 to < 2, 0.5 to < 1, and 0.2 to < 0.5 ng/mL, respectively, and detection rates increased with a higher PSA velocity to 81.8, 82.4, 92.1, and 100% in < 1, 1 to < 2, 2 to < 5, and ≥5 ng/mL/year, respectively (44).
In a large retrospective study by Afshar-Oromieh et al. that included 319 PCa patients with BCR, a correlation of rate detection was found in multivariate analysis with PSA level and androgen deprivation therapy (ADT), probably linked with a PSMA expression by PCa cells upregulated by ADT. No correlation was found with Gleason score (compared to low Gleason score of 5–6) or PSA doubling time (45). Furthermore, in a multicenter prospective study on the impact of 68Ga-PSMA PET/CT in the management of PCa, Roach et al. found that PSMA ligand imaging detected additional nodal disease compared to conventional imaging in 39% patients at sites previously unknown and led to a change in planned management in 51% of patients (46).
Nonetheless, PSMA ligand uptake can be seen in other malignancies (glioblastoma, hepatocellular carcinoma, lung cancer, renal cell cancer, thyroid cancer, follicular lymphoma) and benign conditions (schwannomas, thyroid adenoma, hemangioma, sarcoidosis, inflammatory lymph node). This requires interpretation of data by a dedicated nuclear medicine team, capable of correctly interpreting the images of these PET examinations. Moreover, a major limitation of most PSMA studies is the lack of histological confirmations of positive lesions. As such, what investigators “see” as PCa metastases on imaging may not necessarily correspond to pathologic disease, albeit extremely high specificity rates were reported in studies in which histological confirmation was obtained (19).
Amino acid transport and metabolism is upregulated in malignant cells, including PCa cells. Various amino acid transporter systems or pathways can be targeted. The first radiolabeled amino acid studies in PCa were involving 11C-Methionine and 11C-hydroxy-Tryptophane. They showed excellent and promising results, although in few and small series, which served nonetheless as a proof of concept (21, 47, 48, 49, 50).
Other non-natural amino-acids have been synthesized and the most studied is the anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (18F-FACBC or 18F-Fluciclovine). Fluciclovine has minimal urinary excretion and minimal brain uptake which allow imaging of cerebrum, retroperitoneum and pelvis. The highest uptake is seen in pancreas, liver, bone marrow, salivary glands, lymphoid tissues and pituitary as found with other amino acid based radiotracers. In a multicenter phase IIb clinical trial, 18F-Fluciclovine PET/CT was compared to conventional imaging with CT and bone scan. The overall accuracies were similar for 18F-Fluciclovine PET/CT and conventional imaging (85.5 vs. 87.3%). However, 18F-fluciclovine PET/CT was positive in 5–9 mm lymph nodes that were not detected by conventional imaging (22). Currently, 18F-Fluciclovine seems to present promising results in the characterization of primary disease as the uptake is significantly higher in PCa compared to normal prostate tissue (51).
The sentinel lymph node dissection techniques rely on the principle that by detecting the primary nodal landing sites where tumor cells would spread by following the lymphatic pathway and by analyzing if there is a tumor invasion in these site a limited and less invasive lymph node dissection could be performed, thereby reducing the morbidity caused by an extensive lymph node dissection. In uro-oncology, the sentinel lymph node (SLN) technique was first described for the penile cancer in 1977 (52). In PCa the first study was reported in 1999 by Wawroschek et al. (53).
Albeit current international guidelines do not recommend performing SLN techniques for PCa (3), this is a field of active research, especially with the introduction of indocyanine green and fluorescence guided surgery. The two most widely used SLN techniques are the radio-isotope injection of 99mTc-nanocolloid and fluorescence imaging with the indocyanine green.
In the 99mTc-nanocolloid technique, the radiotracer is injected transrectally in the prostate. Lymphoscintigraphy with static planar acquisitions are performed 15 min and 2 h after the injection followed by SPECT/CT imaging. Thereafter, during surgery, the SLN is detected using gamma probes. The technique has been developed over the last 15 years, and is routinely used in breast cancer and melanoma surgery (54, 55). The technique is feasible in PCa patients and Holl et al. demonstrated that SLN could be detected in up to 98.2% of patients with clinically localized PCa disease. They conducted a large study in 2020 clinically localized PCa patients. Preoperative planar lymphoscintigraphy detected drainage patterns in 97.6% of patients while intraoperative SLN detection using a handheld probe was successful in 98% of cases. They reported a false negative rate of 5.9% with an increase up to 14% in patients with Gleason > 8 (56).
In a recent systematic review of SLN in PCa, the overall median pre-operative and intraoperative detection rates were 97.8 and 96.1%, respectively, with an overall median false negative rate of 7.1% (57).
Wawroschek et al. demonstrated the validity of the technique with a 97% sensitivity to detect the location of lymphatic spread in node positive patients and improved detection of micrometastases (53, 58, 59). Two meta-analyses suggested a sensitivity around 95% to detect LNM (23, 60). The most common areas of LN metastases detected with SLN technique is the external and internal iliac regions, followed by the obturator, common iliac, and presacral regions. Frequently, the SLN technique detected bilateral LN (56, 61, 62).
Nonetheless, the SLN technique presents major limitations, hampering its introduction in routine surgical practice. First of all, there is a lack of standardized protocol (number and sites of injections) and difficulties for the intra-operatory detection with gamma probe (distance between the lymph node and probe in open surgery, large gamma cameras not adequate in robotic-assisted surgery). Second, the false negative rate may be due to an obliteration or obstruction of lymphovascular vessels and nodes by metastatic cells. Other causes of false negative results are the modifications of lymphatic drainage due to previous treatments (surgery, TRUS, radiotherapy) or inflammation and infection conditions. In such situations, the SLN technique should be analyzed with caution.
For the indocyanine green (ICG) technique, ICG is also injected in the prostate via a transrectal route and the SLN is detected preoperatively with polarized light. It can be injected before the surgery or intra-operatory. The ICG present the advantage to be non-radioactive. It has been used for more than 50 years for hepatic clearance and cardiovascular function evaluation as well as in ophthalmic angiography, with few reported allergic reactions to its iodine content. It undergoes rapid hepatic metabolism and excretion in bile. In uro-oncology, the first study with ICG was reported in 2011 by Inoue et al. in 14 patients with open radical prostatectomy (63). Since then, different studies have been published with the ICG technique and the median intraoperative fluorescence detection rates ranged between 76 and 97% with a sensitivity of 100% for metastatic lymph node detection (24, 25, 64, 65). Chennamsetty et al. performed an ICG lymph node mapping during robotic assisted radical prostatectomy in 20 patients with high or intermediate risk PCa. They found a sensitivity, specificity, PPV and NPV of 62, 50, 8, and 95%, respectively (66).
Van der Poel et al. were the first, in 2011, to demonstrate the feasibility of an hybrid fluorescent-radiotracer technique in 11 patients undergoing robotic radical prostatectomy. They used a colloid to which the ICG was bound additionally to form an “hybrid tracer” (67). Jeschke et al. published a study of 26 patients undergoing laparoscopic lymph node dissection guided by hybrid fluorescent-radiotracer. In their study, 18 h before surgery the patient received the conventional radio-isotope intraprostatic injection and ICG was then injected intra-operatively (68). Both studies concluded that the combination of tracer improves the detection rate and the ICG added the advantage of visualizing the lymphatic vessels in real time.
The ICG technique present the same accuracy and limitations as the conventional radio-isotope technique and the study by Chennamsetty et al. found a poor diagnostic accuracy of SLN technique in high and intermediate risk PCa probably in relation with the metastatic obliteration of lymphovascular vessels and nodes (66). Due to the complex drainage pattern of the prostate, and the low sensitivity of the technique for the detection of nodal metastases, fluorescence SLN detection is not enough reliable, at present, to be considered as an alternative to an accurate PLND in higher risk patients.
Winter et al. reported on the first human study using superparamagnetic iron oxide (SPIO) nanoparticles as magnetic SLN tracer in 2014 (28). They published a detection rate of 90% with a 100% sensitivity for metastatic nodes. The SPIO seems to improve the sensitivity of MRI from 45 to 100% with a specificity of 97%. In a feasibility study with PSMA-labeled radiotracer (111In-PSMA-I&T) for SLN, Maurer et al. detected in five patients 2–4 mm LN lesions and additional nodes that 68Ga-PSMA PET did not detect (69). As such, this PSMA-labeled radiotracer could facilitate lymphadenectomy in patients with very high-risk and oligometastatic PCa, in which metastatic LNs have initially been detected by PSMA imaging.
Finally, in in vitro model and in a murine model, the feasibility of SPIO nanoparticle-bound PSMA ligands has been shown, with an increased uptake of SPIO by PCa cells lines that expressed PSMA (70, 71). This represents a potential tracer for the evaluation of lymph node and metastatic extension in PCa with PET/MR device. Further clinical investigations are required.
Optimal lymph node staging in prostate cancer remains an important goal in the management of patient with PCa at pre-operative evaluation and for BCR investigation. Molecular imaging, particularly PSMA ligand PET imaging, presents interesting diagnostic accuracy in LN diagnosis even in subcentimetric LN particularly in low PSA value BCR. Nonetheless, the clinical significance of positive PSMA PET/CT findings, and its impact on oncologic outcomes, remains to be defined. Other PET tracers have been developed and continued to be studied. DWI-MRI presents good results in LN involvement evaluation and the use of contrast agent such SPIO may improve the detection rate. The SLN technique is limited to experimental protocols and for intermediate or high-risk PCa. Well-designed, prospective trials are needed to determine the place of novel imaging techniques and their clinical impact in management and decision making for PCa patients.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer (2014) 136:E359–86. doi: 10.1002/ijc.29210
2. Grivas N, Wit E, Pos F, de Jong J, Vegt E, Bex A, et al. Sentinel lymph node dissection to select clinically node-negative prostate cancer patients for pelvic radiation therapy: effect on biochemical recurrence and systemic progression. Int J Radiat Oncol Biol Phys. (2017) 97:347–54. doi: 10.1016/j.ijrobp.2016.10.016
3. Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. (2017) 71:618–29. doi: 10.1016/j.eururo.2016.08.003
4. Briganti A, Larcher A, Abdollah F, Capitanio U, Gallina A, Suardi N, et al. Updated nomogram predicting lymph node invasion in patients with prostate cancer undergoing extended pelvic lymph node dissection: the essential importance of percentage of positive cores. Eur Urol. (2012) 61:480–7. doi: 10.1016/j.eururo.2011.10.044
5. Pre-Radical, Prostatectomy,. Memorial Sloan Kettering Cancer Center. Available online at: https://www.mskcc.org/nomograms/prostate/pre_op (Accessed May 10, 2018).
6. Briganti A, Blute ML, Eastham JH, Graefen M, Heidenreich A, Karnes JR, et al. Pelvic lymph node dissection in prostate cancer. Eur Urol. (2009) 55:1251–65. doi: 10.1016/j.eururo.2009.03.012
7. Ploussard G, Briganti A, de la Taille A, Haese A, Heidenreich A, Menon M, et al. Pelvic lymph node dissection during robot-assisted radical prostatectomy: efficacy, limitations, and complications—a systematic review of the literature. Eur Urol. (2014) 65:7–16. doi: 10.1016/j.eururo.2013.03.057
8. Fossati N, Willemse P-PM, Van den Broeck T, van den Bergh RCN, Yuan CY, Briers E, et al. The benefits and harms of different extents of lymph node dissection during radical prostatectomy for prostate cancer: a systematic review. Eur Urol. (2017) 72:84–109. doi: 10.1016/j.eururo.2016.12.003
9. Van Huele A, Poelaert F, Fonteyne V, Decaestecker K, Ost P, Lumen N. Pelvic lymph node dissection in prostate cancer staging: evaluation of morbidity and oncological outcomes. Acta Chir Belg. (2018) 8:1–7. doi: 10.1080/00015458.2018.1470294
10. Hövels AM, Heesakkers RAM, Adang EM, Jager GJ, Strum S, Hoogeveen YL, et al. The diagnostic accuracy of CT and MRI in the staging of pelvic lymph nodes in patients with prostate cancer: a meta-analysis. Clin Radiol. (2008) 63:387–95. doi: 10.1016/j.crad.2007.05.022
11. von Below C, Daouacher G, Wassberg C, Grzegorek R, Gestblom C, Sörensen J, et al. Validation of 3 T MRI including diffusion-weighted imaging for nodal staging of newly diagnosed intermediate- and high-risk prostate cancer. Clin Radiol. (2016) 71:328–34. doi: 10.1016/j.crad.2015.12.001
12. Harisinghani MG, Barentsz J, Hahn PF, Deserno WM, Tabatabaei S, van de Kaa CH, et al. Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. N Engl J Med. (2003) 348:2491–9. doi: 10.1056/NEJMoa022749
13. Beauregard J-M, Blouin A-C, Fradet V, Caron A, Fradet Y, Lemay C, et al. FDG-PET/CT for pre-operative staging and prognostic stratification of patients with high-grade prostate cancer at biopsy. Cancer Imaging (2015) 15:2. doi: 10.1186/s40644-015-0038-0
14. Chang C-H, Wu H-C, Tsai JJP, Shen Y-Y, Changlai S-P, Kao A. Detecting metastatic pelvic lymph nodes by 18F-2-deoxyglucose positron emission tomography in patients with prostate-specific antigen relapse after treatment for localized prostate cancer. Urol Int. (2003) 70:311–5. doi: 10.1159/000070141
15. Evangelista L, Guttilla A, Zattoni F, Muzzio PC, Zattoni F. Utility of choline positron emission tomography/computed tomography for lymph node involvement identification in intermediate- to high-risk prostate cancer: a systematic literature review and meta-analysis. Eur Urol. (2013) 63:1040–8. doi: 10.1016/j.eururo.2012.09.039
16. Tilki D, Reich O, Graser A, Hacker M, Silchinger J, Becker AJ, et al. 18F-Fluoroethylcholine PET/CT identifies lymph node metastasis in patients with prostate-specific antigen failure after radical prostatectomy but underestimates its extent. Eur Urol. (2013) 63:792–6. doi: 10.1016/j.eururo.2012.08.003
17. Schumacher MC, Radecka E, Hellström M, Jacobsson H, Sundin A. [11C]Acetate positron emission tomography-computed tomography imaging of prostate cancer lymph-node metastases correlated with histopathological findings after extended lymphadenectomy. Scand J Urol. (2015) 49:35–42. doi: 10.3109/21681805.2014.932840
18. Haseebuddin M, Dehdashti F, Siegel BA, Liu J, Roth EB, Nepple KG, et al. (11)C-Acetate PET/CT before radical prostatectomy: nodal staging and treatment failure prediction. J Nucl Med. (2013) 54:699–706. doi: 10.2967/jnumed.112.111153
19. Budäus L, Leyh-Bannurah S-R, Salomon G, Michl U, Heinzer H, Huland H, et al. Initial experience of 68Ga-PSMA PET/CT imaging in high-risk prostate cancer patients prior to radical prostatectomy. Eur Urol. (2016) 69:393–6. doi: 10.1016/j.eururo.2015.06.010
20. Zhang Q, Zang S, Zhang C, Fu Y, Lv X, Zhang Q, et al. Comparison of (68)Ga-PSMA-11 PET-CT with mpMRI for preoperative lymph node staging in patients with intermediate to high-risk prostate cancer. J Transl Med. (2017) 15:230. doi: 10.1186/s12967-017-1333-2
21. Shiiba M, Ishihara K, Kimura G, Kuwako T, Yoshihara N, Sato H, et al. Evaluation of primary prostate cancer using 11C-methionine-PET/CT and 18F-FDG-PET/CT. Ann Nucl Med. (2012) 26:138–45. doi: 10.1007/s12149-011-0551-6
22. Suzuki H, Inoue Y, Fujimoto H, Yonese J, Tanabe K, Fukasawa S, et al. Diagnostic performance and safety of NMK36 (trans-1-amino-3-[18F]fluorocyclobutanecarboxylic acid)-PET/CT in primary prostate cancer: multicenter phase IIb clinical trial. Jpn J Clin Oncol. (2016) 46:152–62. doi: 10.1093/jjco/hyv181
23. Wit EMK, Acar C, Grivas N, Yuan C, Horenblas S, Liedberg F, et al. Sentinel node procedure in prostate cancer: a systematic review to assess diagnostic accuracy. Eur Urol. (2017) 71:596–605. doi: 10.1016/j.eururo.2016.09.007
24. Manny TB, Patel M, Hemal AK. Fluorescence-enhanced robotic radical prostatectomy using real-time lymphangiography and tissue marking with percutaneous injection of unconjugated indocyanine green: the initial clinical experience in 50 patients. Eur Urol. (2014) 65:1162–8. doi: 10.1016/j.eururo.2013.11.017
25. Nguyen DP, Huber PM, Metzger TA, Genitsch V, Schudel HH, Thalmann GN. A specific mapping study using fluorescence sentinel lymph node detection in patients with intermediate- and high-risk prostate cancer undergoing extended pelvic lymph node dissection. Eur Urol. (2016) 70:734–7. doi: 10.1016/j.eururo.2016.01.034
26. Créhange G, Chen CP, Hsu CC, Kased N, Coakley FV, Kurhanewicz J, et al. Management of prostate cancer patients with lymph node involvement: a rapidly evolving paradigm. Cancer Treat Rev. (2012) 38:956–67. doi: 10.1016/j.ctrv.2012.05.005
27. Sumi M, Van Cauteren M, Nakamura T. MR microimaging of benign and malignant nodes in the neck. Am J Roentgenol. (2006) 186:749–57. doi: 10.2214/AJR.04.1832
28. Winter A, Woenkhaus J, Wawroschek F. A novel method for intraoperative sentinel lymph node detection in prostate cancer patients using superparamagnetic iron oxide nanoparticles and a handheld magnetometer: the initial clinical experience. Ann Surg Oncol. (2014) 21:4390–6. doi: 10.1245/s10434-014-4024-8
29. Triantafyllou M, Studer UE, Birkhäuser FD, Fleischmann A, Bains LJ, Petralia G, et al. Ultrasmall superparamagnetic particles of iron oxide allow for the detection of metastases in normal sized pelvic lymph nodes of patients with bladder and/or prostate cancer. Eur J Cancer (2013) 49:616–24. doi: 10.1016/j.ejca.2012.09.034
30. Birkhäuser FD, Studer UE, Froehlich JM, Triantafyllou M, Bains LJ, Petralia G, et al. Combined ultrasmall superparamagnetic particles of iron oxide–enhanced and diffusion-weighted magnetic resonance imaging facilitates detection of metastases in normal-sized pelvic lymph nodes of patients with bladder and prostate cancer. Eur Urol. (2013) 64:953–60. doi: 10.1016/j.eururo.2013.07.032
31. Minamimoto R, Senda M, Jinnouchi S, Terauchi T, Inoue T. Detection of prostate cancer by an FDG-PET cancer screening program: results from a Japanese nationwide survey. Asia Ocean J Nucl Med Biol. (2014) 2:19–23.
32. Shreve PD, Grossman HB, Gross MD, Wahl RL. Metastatic prostate cancer: initial findings of PET with 2-deoxy-2-[F-18]fluoro-D-glucose. Radiology (1996) 199:751–6. doi: 10.1148/radiology.199.3.8638000
33. Effert P, Beniers Aj, Tamimi Y, Handt S, Jakse G. Expression of glucose transporter 1 (Glut-1) in cell lines and clinical specimens from human prostate adenocarcinoma. Anticancer Res. (2004) 24:3057–64.
34. Minamimoto R, Uemura H, Sano F, Terao H, Nagashima Y, Yamanaka S, et al. The potential of FDG-PET/CT for detecting prostate cancer in patients with an elevated serum PSA level. Ann Nucl Med. (2011) 25:21–7. doi: 10.1007/s12149-010-0424-4
35. Ackerstaff E, Glunde K, Bhujwalla ZM. Choline phospholipid metabolism: a target in cancer cells? J Cell Biochem. (2003) 90:525–33. doi: 10.1002/jcb.10659
36. Mitchell CR, Lowe VJ, Rangel LJ, Hung JC, Kwon ED, Karnes RJ. Operational characteristics of 11C-choline positron emission tomography/computerized tomography for prostate cancer with biochemical recurrence after initial treatment. J Urol. (2013) 189:1308–13. doi: 10.1016/j.juro.2012.10.069
37. Cornford P, Bellmunt J, Bolla M, Briers E, De Santis M, Gross T, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part II: treatment of relapsing, metastatic, and castration-resistant prostate cancer. Eur Urol. (2017) 71:630–42. doi: 10.1016/j.eururo.2016.08.002
38. Vāvere AL, Kridel SJ, Wheeler FB, Lewis JS. 1-11C-Acetate as a PET radiopharmaceutical for imaging fatty acid synthase expression in prostate cancer. J Nucl Med. (2008) 49:327–34. doi: 10.2967/jnumed.107.046672
39. Seltzer MA, Jahan SA, Sparks R, Stout DB, Satyamurthy N, Dahlbom M, et al. Radiation dose estimates in humans for 11C-acetate whole-body PET. J Nucl Med. (2004) 45:1233–6.
40. Vees H, Buchegger F, Albrecht S, Khan H, Husarik D, Zaidi H, et al. 18F-choline and/or 11C-acetate positron emission tomography: detection of residual or progressive subclinical disease at very low prostate-specific antigen values (< 1 ng/mL) after radical prostatectomy. BJU Int. (2007) 99:1415–20. doi: 10.1111/j.1464-410X.2007.06772.x
41. Teo MY, Morris MJ. Prostate-specific membrane antigen–directed therapy for metastatic castration-resistant prostate cancer. Cancer J. (2016) 22:347–52. doi: 10.1097/PPO.0000000000000221
42. Rosenthal S, Haseman M, Polascik T. Utility of capromab pendetide (ProstaScint) imaging in the management of prostate cancer. Tech Urol. (2001) 7:27–37.
43. Ponsky LE, Cherullo EE, Starkey R, Nelson D, Neumann D, Zippe CD. Evaluation of preoperative ProstaScint™ scans in the prediction of nodal disease. Prostate Cancer Prostatic Dis. (2002) 5:132. doi: 10.1038/sj.pcan.4500570
44. Eiber M, Maurer T, Souvatzoglou M, Beer AJ, Ruffani A, Haller B, et al. Evaluation of hybrid 68Ga-PSMA ligand PET/CT in 248 patients with biochemical recurrence after radical prostatectomy. J Nucl Med. (2015) 56:668–74. doi: 10.2967/jnumed.115.154153
45. Afshar-Oromieh A, Avtzi E, Giesel FL, Holland-Letz T, Linhart HG, Eder M, et al. The diagnostic value of PET/CT imaging with the (68)Ga-labelled PSMA ligand HBED-CC in the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging (2015) 42:197–209. doi: 10.1007/s00259-014-2949-6
46. Roach PJ, Francis R, Emmett L, Hsiao E, Kneebone A, Hruby G, et al. The impact of 68Ga-PSMA PET/CT on management intent in prostate cancer: results of an Australian Prospective Multicenter Study. J Nucl Med. (2018) 59:82–8. doi: 10.2967/jnumed.117.197160
47. Macapinlac HA, Humm JL, Akhurst T, Osman I, Pentlow K, Shangde C, et al. Differential metabolism and pharmacokinetics of l-[1-11C]-methionine and 2-[18F] fluoro-2-deoxy-d-glucose (FDG) in androgen independent prostate cancer. Clin Posit Imaging (1999) 2:173–81. doi: 10.1016/S1095-0397(99)00015-1
48. Nuñez R, Macapinlac HA, Yeung HWD, Akhurst T, Cai S, Osman I, et al. Combined 18F-FDG and 11C-methionine PET scans in patients with newly progressive metastatic prostate cancer. J Nucl Med. (2002) 43:46–55.
49. Tóth G, Lengyel Z, Balkay L, Salah Ma, Trón L, Tóth C. Detection of prostate cancer with 11C-methionine positron emission tomography. J Urol. (2005) 173:66–9. doi: 10.1097/01.ju.0000148326.71981.44
50. Kälkner K-M, Ginman C, Nilsson S, Bergström M, Antoni G, Ahlström H, et al. Positron emission tomography (PET) with 11C-5-hydroxytryptophan (5-HTP) in patients with metastatic hormone-refractory prostatic adenocarcinoma. Nucl Med Biol. (1997) 24:319–25. doi: 10.1016/S0969-8051(97)00064-4
51. Turkbey B, Mena E, Shih J, Pinto PA, Merino MJ, Lindenberg ML, et al. Localized prostate cancer detection with (18)F FACBC PET/CT: comparison with MR imaging and histopathologic analysis. Radiology (2014) 270:849–56. doi: 10.1148/radiol.13130240
52. Cabanas RM. An approach for the treatment of penile carcinoma. Cancer (2006) 39:456–66. doi: 10.1002/1097-0142(197702)39:2<456::AID-CNCR2820390214>3.0.CO;2-I
53. Wawroschek F, Vogt H, Weckermann D, Wagner T, Harzmann R. The sentinel lymph node concept in prostate cancer–first results of gamma probe-guided sentinel lymph node identification. Eur Urol. (1999) 36:595–600.
54. Qiu S-Q, Zhang G-J, Jansen L, de Vries J, Schröder CP, de Vries EGE, et al. Evolution in sentinel lymph node biopsy in breast cancer. Crit Rev Oncol. Hematol. (2018) 123:83–94. doi: 10.1016/j.critrevonc.2017.09.010
55. Wong SL, Faries MB, Kennedy EB, Agarwala SS, Akhurst TJ, Ariyan C, et al. Sentinel lymph node biopsy and management of regional lymph nodes in melanoma: American Society of Clinical Oncology and Society of Surgical Oncology clinical practice guideline update. JCO (2017) 36:399–413. doi: 10.1200/JCO.2017.75.7724
56. Holl G, Dorn R, Wengenmair H, Weckermann D, Sciuk J. Validation of sentinel lymph node dissection in prostate cancer: experience in more than 2,000 patients. Eur J Nucl Med Mol Imaging (2009) 36:1377–82. doi: 10.1007/s00259-009-1157-2
57. Munbauhal G, Seisen T, Gomez FD, Peyronnet B, Cussenot O, Shariat SF, et al. Current perspectives of sentinel lymph node dissection at the time of radical surgery for prostate cancer. Cancer Treat Rev. (2016) 50:228–39. doi: 10.1016/j.ctrv.2016.09.020
58. Wawroschek F, Vogt H, Wengenmair H, Weckermann D, Hamm M, Keil M, et al. Prostate lymphoscintigraphy and radio-guided surgery for sentinel lymph node identification in prostate cancer. Urol Int. (2003) 70:303–10. doi: 10.1159/000070140
59. Wawroschek F, Wagner T, Hamm M, Weckermann D, Vogt H, Märkl B, et al. The influence of serial sections, immunohistochemistry, and extension of pelvic lymph node dissection on the lymph node status in clinically localized prostate cancer. Eur Urol. (2003) 43:132–7. doi: 10.1016/S0302-2838(02)00450-5
60. Sadeghi R, Tabasi K., Bazaz SMM, Kakhki VRD, Massoom AF, Gholami H, et al. Sentinel node mapping in the prostate cancer. Nuklearmedizin (2017) 50:107–15. doi: 10.3413/nukmed-0339-10-07
61. Mattei A, Fuechsel FG, Bhatta Dhar N, Warncke SH, Thalmann GN, Krause T, et al. The template of the primary lymphatic landing sites of the prostate should be revisited: results of a multimodality mapping study. Eur Urol. (2008) 53:118–25. doi: 10.1016/j.eururo.2007.07.035
62. Joniau S, Van den Bergh L, Lerut E, Deroose CM, Haustermans K, Oyen R, et al. Mapping of pelvic lymph node metastases in prostate cancer. Eur Urol. (2013) 63:450–8. doi: 10.1016/j.eururo.2012.06.057
63. Inoue S, Shiina H, Arichi N, Mitsui Y, Hiraoka T, Wake K, et al. Identification of lymphatic pathway involved in the spreading of prostate cancer by fluorescence navigation approach with intraoperatively injected indocyanine green. Can Urol Assoc J. (2011) 5:254–9. doi: 10.5489/cuaj.10159
64. Hruby S, Englberger C, Lusuardi L, Schätz T, Kunit T, Abdel-Aal AM, et al. Fluorescence guided targeted pelvic lymph node dissection for intermediate and high risk prostate cancer. J Urol. (2015) 194:357–63. doi: 10.1016/j.juro.2015.03.127
65. Yuen K, Miura T, Sakai I, Kiyosue A, Yamashita M. Intraoperative fluorescence imaging for detection of sentinel lymph nodes and lymphatic vessels during open prostatectomy using indocyanine green. J Urol. (2015) 194:371–7. doi: 10.1016/j.juro.2015.01.008
66. Chennamsetty A, Zhumkhawala A, Tobis SB, Ruel N, Lau CS, Yamzon J, et al. Lymph node fluorescence during robot-assisted radical prostatectomy with indocyanine green: prospective dosing analysis. Clin Genitourin Cancer (2017) 15:e529–34. doi: 10.1016/j.clgc.2016.10.014
67. van der Poel HG, Buckle T, Brouwer OR, Valdés Olmos RA, van Leeuwen FWB. Intraoperative laparoscopic fluorescence guidance to the sentinel lymph node in prostate cancer patients: clinical proof of concept of an integrated functional imaging approach using a multimodal tracer. Eur Urol. (2011) 60:826–33. doi: 10.1016/j.eururo.2011.03.024
68. Jeschke S, Lusuardi L, Myatt A, Hruby S, Pirich C, Janetschek G. Visualisation of the lymph node pathway in real time by laparoscopic radioisotope- and fluorescence-guided sentinel lymph node dissection in prostate cancer staging. Urology (2012) 80:1080–7. doi: 10.1016/j.urology.2012.05.050
69. Maurer T, Weirich G, Schottelius M, Weineisen M, Frisch B, Okur A, et al. Prostate-specific membrane antigen–radioguided surgery for metastatic lymph nodes in prostate cancer. Eur Urol. (2015) 68:530–4. doi: 10.1016/j.eururo.2015.04.034.
70. Pellico J, Llop J, Fernández-Barahona I, Bhavesh R, Ruiz-Cabello J, Herranz F. Iron oxide nanoradiomaterials: combining nanoscale properties with radioisotopes for enhanced molecular imaging. Contrast Media Mol Imaging (2017) 2017:1549580. doi: 10.1155/2017/1549580
Keywords: imaging, MRI, lymph nodes, PET, PSMA, prostate cancer
Citation: Muteganya R, Goldman S, Aoun F, Roumeguère T and Albisinni S (2018) Current Imaging Techniques for Lymph Node Staging in Prostate Cancer: A Review. Front. Surg. 5:74. doi: 10.3389/fsurg.2018.00074
Received: 14 September 2018; Accepted: 19 November 2018;
Published: 07 December 2018.
Edited by:
Umberto Capitanio, San Raffaele Hospital (IRCCS), ItalyReviewed by:
Marco Roscigno, Azienda Socio-Sanitaria Territoriale Papa Giovanni XXIII, ItalyCopyright © 2018 Muteganya, Goldman, Aoun, Roumeguère and Albisinni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Simone Albisinni, c2ltb25lLmFsYmlzaW5uaUBlcmFzbWUudWxiLmFjLmJl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.