
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 28 August 2020
Sec. Public Health Education and Promotion
Volume 8 - 2020 | https://doi.org/10.3389/fpubh.2020.00330
 M. Larissa Avilés-Santa1*
M. Larissa Avilés-Santa1* Laura Hsu2Tram Kim Lam3
Laura Hsu2Tram Kim Lam3 S. Sonia Arteaga4†‡
S. Sonia Arteaga4†‡ Ligia Artiles5‡
Ligia Artiles5‡ Sean Coady4‡Lawton S. Cooper4‡
Sean Coady4‡Lawton S. Cooper4‡ Jennifer Curry6‡
Jennifer Curry6‡ Patrice Desvigne-Nickens4‡Holly L. Nicastro4†‡
Patrice Desvigne-Nickens4‡Holly L. Nicastro4†‡ Adelaida Rosario5†‡
Adelaida Rosario5†‡Hispanics/Latinos are expected to constitute 25% of the U.S. population by 2060. Differences in the prevalence of health risk factors, chronic diseases, and access to and utilization of health-care services between Hispanics/Latinos and other populations in the U.S. have been documented. This study aimed to describe and analyze the landscape of Research Program Grants (RPGs) funded by the National Institutes of Health (NIH) between 2008 and 2015 involving Hispanic/Latino health research in six health condition areas—asthma, cancer, dementia, diabetes, liver/gallbladder disease, and obesity—and to identify opportunities for continued research in these areas. Using an NIH internal search engine, we identified new and renewal Hispanic/Latino health RPGs searching for specific Hispanic/Latino identifiers in the Title, Abstract, and Specific Aims. We used descriptive statistics to examine the distribution of funded RPGs by NIH disease-based classification codes for the six health condition areas of interest, and other selected characteristics. The most prominent clusters of research subtopics were identified within each health condition area, and performance sites were mapped at the city level. Within the selected time frame, 3,221 Hispanic/Latino health-related unique RPGs were funded (constituting 4.4% of all funded RPGs), and of those 625 RPGs were eligible for review and coding in the present study. Cancer and obesity were the most commonly studied health condition areas (72%), while studies on mechanisms of disease—biological and non-biological—(72.6%), behavioral research (42.1%) and epidemiological studies (38.1%) were the most common types of research. Most of the primary performance sites were in California, Texas, the northeastern U.S., and Illinois. The predominance of mechanistic, behavioral, and epidemiological studies in our analysis poses opportunities to evaluate knowledge gained and their clinical application, explore new research questions, or to update some methods or instruments. The findings of the present study suggest opportunities to expand research in understudied mechanisms of disease that could explain differences in prevalence of conditions like diabetes and cancer among different heritage groups. In addition, our findings suggest that the impact of interventions or policies designed to reduce health disparities, innovative multi-level interventions, implementation and dissemination studies, the role of health information technology on health outcomes, and the intersectionality of individual, sociocultural, geographic, and other factors on health outcomes, among others, are understudied approaches, which could potentially advance research in Hispanic/Latino health and contribute to the achievement of better health outcomes in this diverse population.
As more precise diagnostic and prognostic algorithms are developed in clinical medicine, understanding the manifestation of health and diseases across age, sex/gender, and racial/ethnic groups has continued gaining critical interest among biomedical researchers. To reach this goal, studies specifically dedicated to understanding patterns of wellness, disease, risk or protective factors (including gene-environment interactions), mechanisms of disease, and effective preventive and treatment strategies, especially among populations affected by health disparities, need to be effectively supported (1–3).
Hispanics/Latinos, the largest U.S. racial/ethnic minority group, are expected in 2060 to constitute a quarter of the U.S. population (4, 5). Differences in access to care and prevalence of chronic diseases between Hispanics/Latinos and other populations in the U.S. have been documented (6–13). Also, differences in prevalence of some chronic diseases or their risk factors among different heritage groups in the contemporary U.S. Hispanic/Latino population have been described by the landmark study, the Hispanic Community Health Study/Study of Latinos (HCHS/SOL) (14–20). However, the underlying mechanisms mediating such differences are yet to be determined. In addition, despite the well-described disproportional burden of health risk factors and adverse social determinants of health, all-cause mortality among U.S. Hispanics/Latinos is lower and their life expectancy is longer for both men and women than other racial/ethnic groups (13, 21–24). The reasons for this health paradox are not fully understood, and further study of the Hispanic/Latino populations may lead to important scientific discoveries.
Motivated by an interest in advancing research in Hispanic/Latino health, the National Institutes of Health (NIH) and the Hispanic Health Research Scientific Interest Group (HHRSIG) (25) reviewed the NIH portfolio of extramural research program grants (RPGs) funded from 2008 to 2015. The goal of this review was to perform a descriptive analysis of funded RPGs in which Hispanics/Latinos had been identified as a population of interest to understand the scope of topics and types of research and identify areas of future research potential. Upon considering the leading causes of death (13, 26–28) as an ethnic group, and the high or increasing prevalence of some chronic diseases (8–20) within the ethnic group or among some Hispanic/Latino heritage groups, this portfolio analysis focused on funded RPGs studying asthma, cancer, dementia, diabetes, liver disease-gallbladder disease (GBD), and obesity.
Extramural staff members of the HHRSIG conducted the portfolio analysis. The analysis team designed a protocol to identify, review, and code select elements of the proposed research in funded RPG applications, as described below. The query/view/report (QVR) is an internal tool that lets NIH extramural staff search, review, and retrieve detailed information about grant applications and awards. QVR was utilized to identify RPG applications funded between fiscal years (FY) 2008 and 2015. This time frame was selected based on a higher accuracy and completeness of the digital database, which tracks starting in 2008 and contained complete data up to 2015 at the time that the portfolio analysis was performed.
The study protocol was pilot-tested and revised before implementation. Applications were randomly distributed among three reviewing teams. A primary and a secondary reviewer were assigned to each application. Disagreements were resolved via team discussion including a third reviewer. The final coding was collected from each team, and the results merged into a single dataset for analysis. The review of applications was initiated in June 2016 and finished in September 2017.
RPGs constitute most of the annually funded extramural projects (29, 30) and include investigator-initiated projects and those responding to specific NIH initiatives or funding opportunity announcements (FOA) funded through grants. RPGs include the activity codes listed in the NIH Funding—Budget and Spending page (29).
Hispanic/Latino health research was defined as (1) projects that specifically identified Hispanics/Latinos as the population or one of the populations of interest in the U.S. or abroad, and (2) projects in which the recruitment of Hispanics/Latinos in the U.S. or abroad was an intended component of the research plan. Although biomedical research that impacts human health could be performed with animal models or other resources, we defined Hispanic/Latino health research from the perspective of human participants (or their biospecimens or data). To identify projects that specifically identified Hispanics/Latinos as the population or one of the populations of interest in the U.S. or abroad, we used a cluster of 52 Hispanic/Latino search terms that included the Office of Management and Budget (OMB) racial/ethnic categories (31, 32), Latin American nationalities, and other demonyms, countries, capitals, and regions (33–35) (Table 1). Most of these search terms already exist in QVR as NIH Research, Condition, and Disease Category (RCDC) concepts (36), whereas others were added manually. The QVR system would identify these terms throughout the Titles, Abstracts and Specific Aims of the funded RPG applications previously identified. Demonyms, nationalities, and names of countries and capitals or regions were searched in English; no accents or tildes were used.
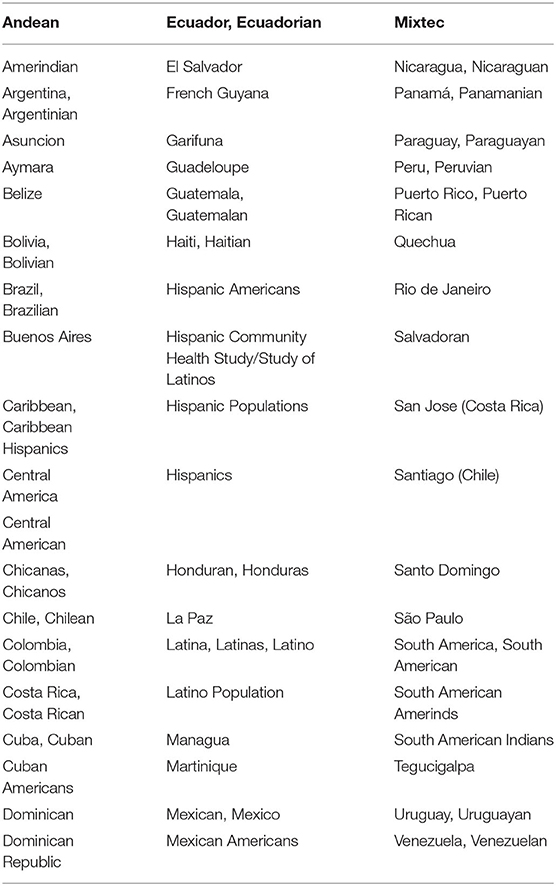
Table 1. Internal search engine Hispanic/Latino identifiers.
Health condition areas were defined based on existing RCDC categories and concepts (36). These included: asthma, diabetes, obesity, liver disease (chronic liver disease, cirrhosis, liver disease, hepatitis), GBD (digestive diseases—gallbladder disease), and cancer (all types). For dementia, we used a cluster of established categories and concepts that comprised acquired cognitive impairment, vascular cognitive impairment, dementia, Alzheimer's disease-related dementias, Alzheimer's disease including related dementias, frontotemporal dementia, and Lewy body dementia. We did not modify any of these RCDC categories and concepts.
Types of research were defined as basic, mechanistic studies (biological and non-biological), clinical—including epidemiology and clinical trials—and translational research, according to the NIH Glossary and Acronym List (37–41). Health services research, secondary data analyses, and community-based participatory research (CBPR) were defined according to other resources (42–44).
Many applications stated the minimum age of study participants (to be enrolled or already enrolled in renewal studies) or the inclusion of children, whereas some stated the specific age range. For simplicity, we created the following age group categories: infants (0–24 months), children (0–17 years), young adults (18–25 years), adults (18–64 years), older adults (65 years and older), and family studies (e.g., dyads or triads of children and parents or guardians).
Primary performance site was defined as the city where the institution receiving the RPG award was located. Secondary performance sites were the cities where institutions subawarded or contracted by the institutions receiving the RPGs were located.
The identification of eligible RPGs for the analysis involved tiers of search criteria. These criteria included type of application (new or renewal), projects involving Hispanic/Latino health research (as defined by identifiers described above), and projects in health condition areas of interest.
Only new and renewal funded RPG applications were reviewed. RPGs funded by more than one NIH Institute were counted once. RPGs with multiple sites or multi-awards with identical project number were also counted once. In addition, RPG applications were eligible for review based on: identification of Hispanics/Latinos as a population of interest in the Title, Abstract, or Specific Aims; RCDC-based health condition area of interest; recruitment of human research participants (e.g., Hispanics/Latinos), or collecting their data or biospecimens (primary data collection), or analyzing previously collected data or biospecimens (secondary data analysis); availability of an enrollment table in the application; and identifying Hispanics/Latinos in the planned enrollment table.
Non-RPG applications funded through contracts or cooperative agreements (other than U01) or intramural projects were not included in the search or analyses. Any RPGs that were originally funded prior to 2008, even if renewed between FY2008-FY2015, were excluded because both the original applications and planned enrollment tables were not electronically traceable at the time the review and analyses were performed. Interim or final progress reports, final enrollment tables, publications of study findings, or the principal investigators' self-reported race/ethnicity were not reviewed, since these data elements were outside of the scope of this analysis.
The review of eligible applications involved coding for a set of variables including: health condition area, planned total sample size, planned Hispanic/Latino sample size; incorporation of race/ethnicity into the power calculation of the sample size; Hispanic/Latino heritage group(s) to be represented in the study; age range of participants to be enrolled or already enrolled (for renewals); whether the application was submitted in response to a topic-specific FOA; type of research and performance sites.
Projects were categorized based on whether Hispanic/Latino ethnicity had been accounted for in the power calculation of the planned sample size, as described under the Research Design section of the RPG applications. Projects in which the power calculation had not accounted Hispanic/Latino ethnicity (including those in which ethnicity was only a confounder or effect modifier) were defined as Planned Enrollment, Not Powered (Not Powered). Projects in which the power of the sample calculation accounted Hispanic/Latino ethnicity were defined as Planned Enrollment, Powered (Powered). Projects in which the Specific Aims clearly stated their focus was exclusively on Hispanics/Latinos or whose projected sample size was 100% Hispanic/Latino (independent of the heritage group) were defined as Focused. These categories were applied whether the studies involved primary recruitment/collection of human research participants/data or secondary analyses of biospecimens or data. We did not evaluate whether the power of the planned sample size was adequately estimated based on race/ethnicity or to address the proposed research questions.
The descriptive analysis was performed using SAS version 9.4 (Cary, NC). Statistical tests were carried out using the non-parametric Mann-Whitney-Wilcoxon rank sums test to compare some of the variables (e.g., sample size by power category, and by new planned enrollment compared to existing cohorts/datasets). Since some RPG applications involved more than one health condition area and most involved more than one type of research (explained under Results), comparisons of these variables were not performed. Performance sites were also mapped at the city level using SAS.
The frequency and grouping of research subtopics within each health condition area were analyzed using text mining and language processing methods. Within each health condition area, the selected RPGs were further clustered by subtopics using iSearch v2.4 a suite of applications for portfolio analyses created by the NIH Office of Portfolio Analysis (45), and only accessible to NIH staff. Within iSearch Grants Module, the Visualize Results tool uses a clustering algorithm that uses words and phrases from the Title, Abstract, and Specific Aims of grants to create “foam trees.” Titles are given more weight in the clustering algorithm. Before clustering, the Title, Abstract, and Specific Aims of each selected RPG were preprocessed using stemming, stop words, and synonym normalization. The clusters displayed were scaled to the number of grant applications.
From FY2008 to FY2015, a total of 3,221 Hispanic/Latino health-related unique RPGs were funded, and of those, 625 RPGs were eligible for review and coding in the present study. Figure 1 shows the numbers of peer-reviewed and funded new and renewal RPG applications both NIH-wide and involving Hispanic/Latino health. From FY2008 to FY2015, over 450,000 new and renewal RPG applications were reviewed by study sections, and ~18.0% were funded every year, which is congruent with NIH funding rates and success rates reports (30, 46). Among the peer-reviewed RPGs, QVR identified Hispanic/Latino search terms in the Titles, Abstracts, or Specific Aims of 5.3% of the applications. Among these, 3,221 unique new or renewal applications were funded (representing 14.9% of the Hispanic/Latino peer-reviewed pool and 4.4% the NIH-wide funded RPG pool). Similar reviews and funding trends are observed from FY2016 to FY2019.
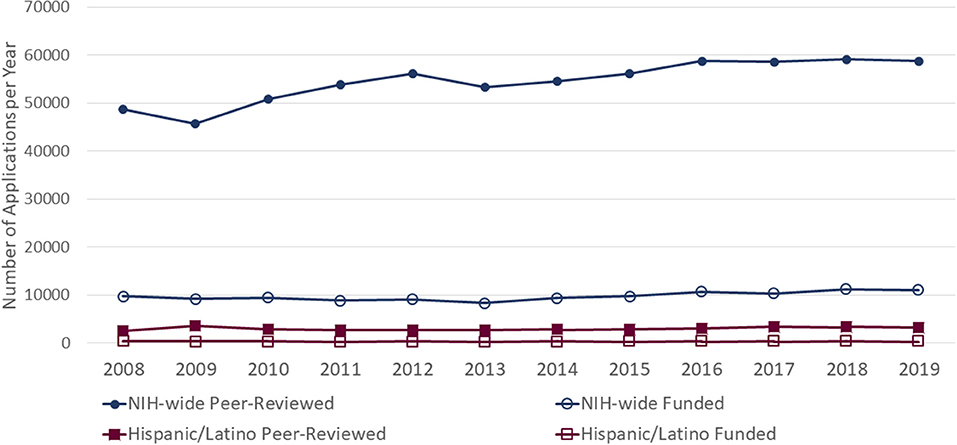
Figure 1. Peer-reviewed and funded New and Renewal RPG applications, 2008–2019.
Among the total 3,221 funded RPGs studying Hispanic/Latino health, 1,237 addressed at least one of the six health condition areas of interest (Figure 2). Of these, 612 were excluded from the analysis for the following reasons: 309 included animal subjects only; 100 involved basic research and did not describe either animal or human research subjects; 73 did not include an enrollment table or race/ethnic breakdown of participants; and 107 did not mention Hispanic/Latinos in the planned enrollment table. In addition, four (4) projects explicitly mentioned Hispanics/Latino in the proposed enrollment table, but the main hypotheses were focused on other populations and Hispanics/Latinos were not mentioned in the statistical plan. We also decided to not review R56 (bridge) awards (n = 19) since they did not incorporate new enrollment of participants or major changes in study activities compared to the parent grant. Although the NIH Annual Fiscal Year Funding Report does not include American Recovery and Reinvestment Act (ARRA) awards, we included 18 ARRA-awarded applications addressing Hispanic/Latino research in the review. Therefore, a total of 625 applications were coded and comprised the analytical dataset.
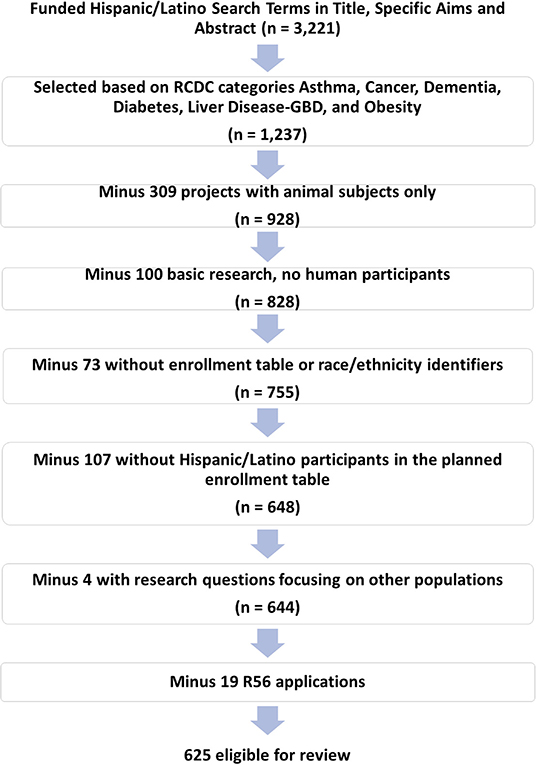
Figure 2. Selection of RPGs and review eligibility criteria.
Although 625 unique RPGs were coded, some of the RPGs fell within more than one RCDC category. Table 2 illustrates the breakdown of the coded RPGs by health condition area. Applications with more than one RCDC category included: Asthma and Obesity (1), Cancer and Liver Disease-GBD (1), Cancer and Obesity (1), Dementia and Diabetes (1), Dementia and Diabetes and Obesity (1), Diabetes and Liver Disease-GBD (3), Diabetes and Liver Disease-GBD and Obesity (2), Diabetes and Obesity (45), Liver Disease-GBD and Obesity (2), and Obesity and Dementia (1). Upon counting for these, the number of applications by health condition area added up to 686. Most applications (89.8%) were new projects, 73% focused on Cancer and Obesity, and 83% of the applications were funded through R01, R03, and R21 grants. Overall, slightly more than half of the applications were solicited (responded to topic-specific FOAs). Studies involving mechanisms of disease (72.6%), behavioral components (42.1%), and epidemiology (38.7%) were the most predominant types of research and overlapped, especially across asthma, diabetes, and obesity health condition areas (data not shown). Translational, CBPR, and health services research were the least common type of research. Also, 191 clinical trials were identified, of which 54% tested behavioral interventions (data not shown). Phase III clinical trials made up just 4% of the coded RPGs (n = 26) (data not shown).
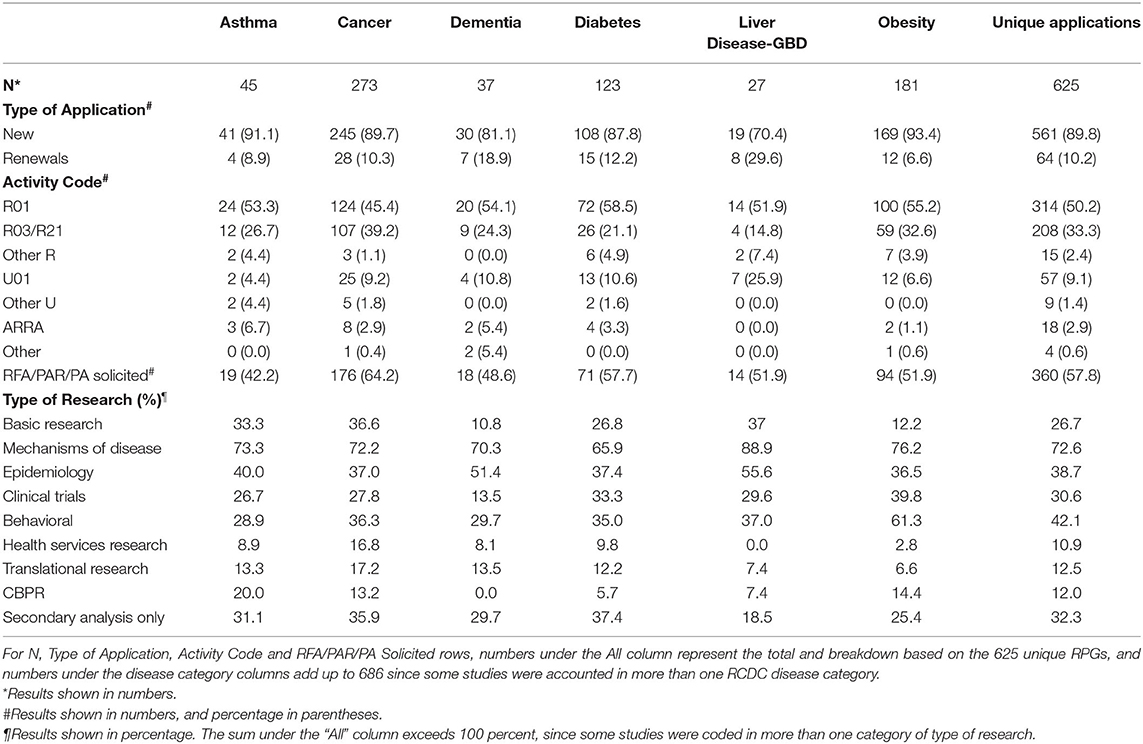
Table 2. Overview of funded Hispanic/Latino health RPGs by Health Condition Area.
Although outside of the scope of our analysis, information on the self-reported Hispanic/Latino ethnicity of the principal investigators of the projects included in the analysis was requested to the NIH Office of Extramural Research (OER) following an established protocol. The data were analyzed by OER and provided in clusters by disease area, not individual answers. Among the 625 RPGs reviewed in this analysis, ~12% of the principal investigators self-reported Hispanic/Latino ethnicity (data not shown). These data were not further analyzed.
Within each health condition area, research subtopics were clustered by number of grants (Figure 3 foam tree panels). Projects could have addressed more than one subtopic within each health condition area.
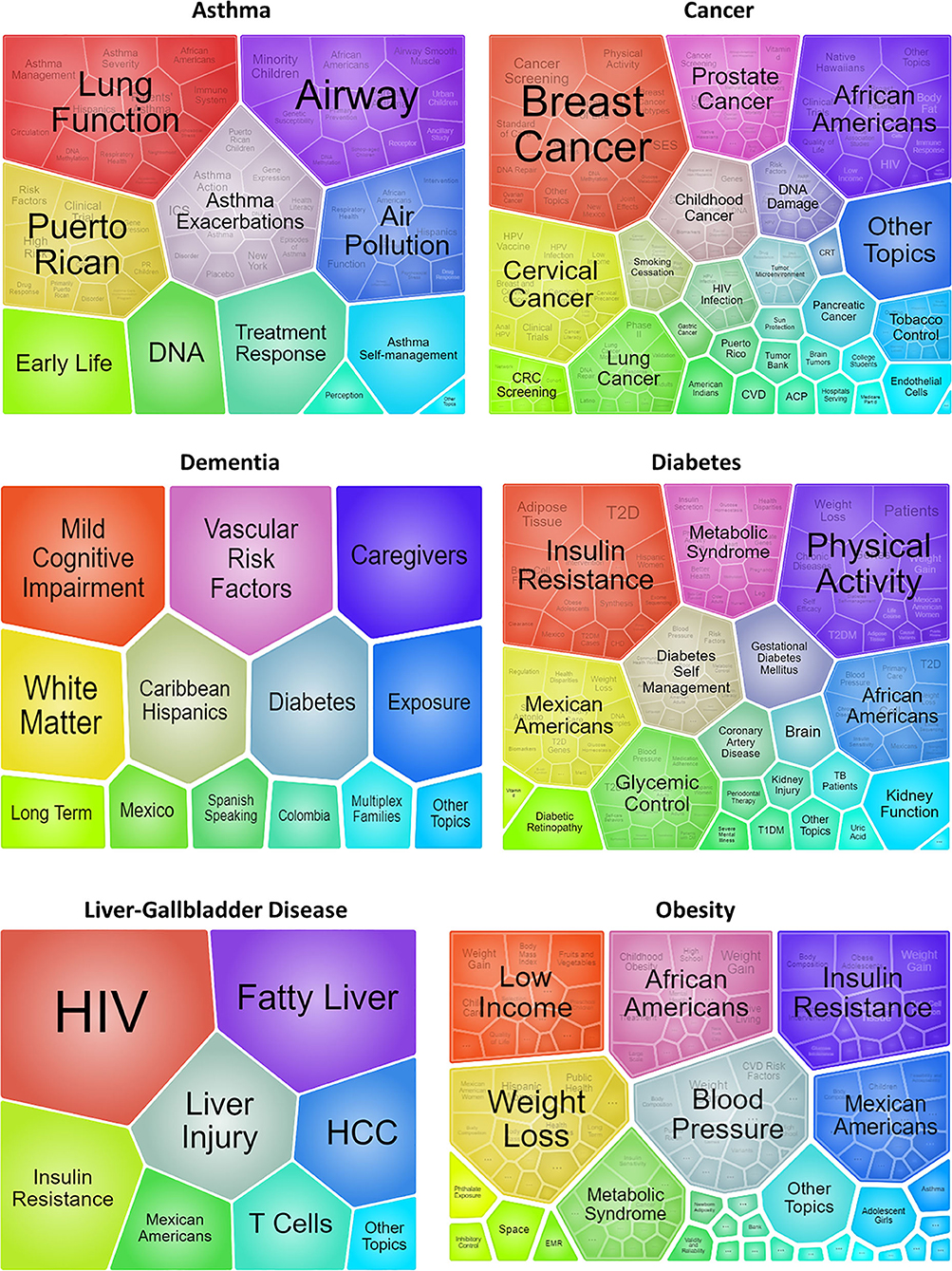
Figure 3. Clusters of research subtopics and cross-cutting themes by Health Condition Area. Each foam tree shows clusters of subtopics within each Health Condition Area scaled to the number of grants.
In the Asthma area, the five largest clusters of subtopics included lung function, airway inflammation and reactivity, asthma exacerbations, air pollution (environmental exposures), and studies focused on Puerto Ricans. Studies involving DNA methylation (e.g., epigenetics) and/or gene expression were present within each of these large clusters. Studies involving interventions, especially with dyads (Family studies in Table 3), or in which African Americans or school-age children were populations of interest within some of the largest clusters.
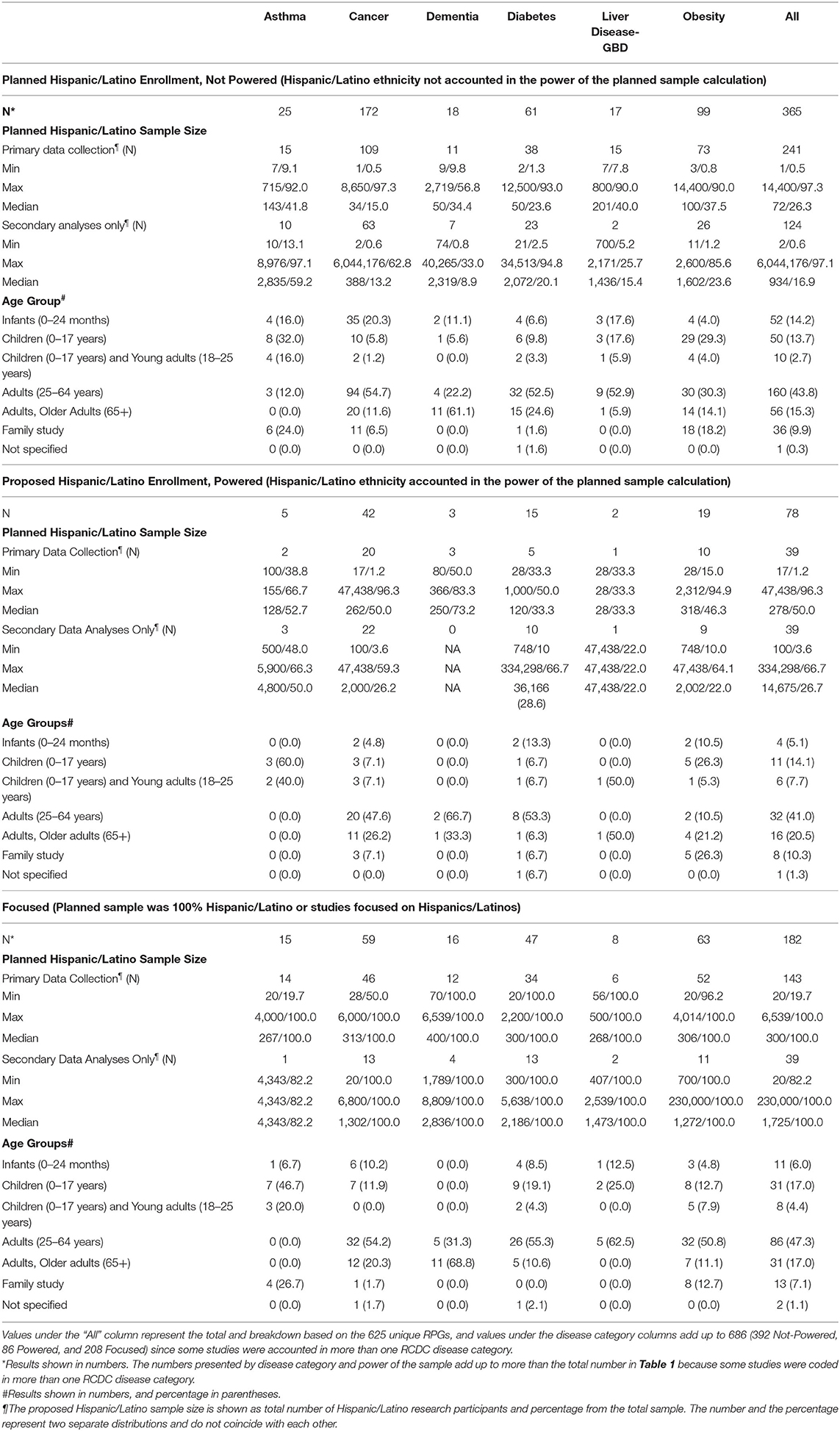
Table 3. General descriptors of funded RPGs by Health Condition Area and accounting for Hispanic/Latino ethnicity on the power of the planned sample size.
In the Cancer area, the five largest clusters of subtopics involved breast, cervical, prostate, lung, and childhood cancers. Genetics/genomic studies were common among each cluster, and especially under lung and childhood cancer. Quality of care, socioeconomic status, or barriers and strategies to increase or facilitate cancer screening were also common topics addressed across the largest clusters.
In the Dementia health condition area, the larger clusters of subtopics were almost evenly distributed, but the three largest clusters involved mild cognitive impairment (including screening), vascular risk factors, and studies (interventions) involving caregivers.
Within the Diabetes area, the largest clusters of subtopics by number of grants involved insulin resistance and physical activity, followed by Mexican Americans, African Americans, metabolic syndrome, self-management, and glycemic control. Studies in which Mexican Americans or African Americans were populations of interest were prominent and represented in various clusters. Genetic research was prominent in the physical activity cluster.
The Liver-GBD area had the smallest number of RPGs, and the largest clusters of subtopics involved HIV and fatty liver, which included non-alcoholic fatty liver disease (NAFLD) or non-alcoholic steatohepatitis (NASH).
Within the Obesity area, the largest clusters of subtopics included studies on insulin resistance, weight loss, blood pressure, Mexican Americans, African Americans, and the metabolic syndrome. Studies on body composition, children, adipose tissue, and genetic/genomic studies were common across these large clusters. Mexican Americans and African Americans were populations of interest across multiple subtopics, especially those involving weight loss and control of cardiovascular risk factors.
In a preliminary overview of the clusters of topics for RPGs funded in 2016–2019, similar groups of subtopics within each health condition area areas were observed (data not shown).
Forty-two percent (42%) of the coded RPGs incorporated Hispanic/Latino ethnicity in the power calculation of the sample size or focused exclusively on Hispanics/Latinos. Table 3 shows the breakdown of coded RPGs by health condition area and accounting of Hispanic/Latino ethnicity into the sample size calculation. The distribution of types of RPGs was similar across power categories, except that U01 applications were more common within the Not-Powered category (data not shown). Hispanic/Latino sample size of the Focused studies were significantly larger than those of the Not Powered studies (P < 0.001), while no difference was observed for total number of participants (P = 0.115). Planned sample sizes were subcategorized into primary recruitment/data collection and secondary analyses. Most studies (66% Not Powered, 50% Powered, and 78% Focused) involved primary recruitment and/or data collection. Secondary analyses had overall median planned Hispanic/Latino sample size consistently larger than studies involving primary recruitment/data collection (P < 0.001). Independent of the power category, most of the studies on asthma focused on children and young adults, most cancer and diabetes studies focused on adults aged 25–64 years, studies on liver/gallbladder disease and obesity covered different ages, and most of the dementia studies focused on adults aged 25–64 years and older adults.
Primary performance sites predominated in California (n = 142), Texas (n = 64), the Northeast [New York (n = 59), and Massachusetts (n = 41)], Illinois (n = 26), and Florida (n =22). Arizona (n = 16), New Mexico (n = 12), Colorado (n = 9) and Puerto Rico (n = 7) and had the lowest number of primary performance sites (Figure 4). Secondary performance sites predominated in California (n = 118), Texas (n = 57), New York (n = 53), and Massachusetts (n = 52).

Figure 4. Primary and secondary U.S. performance sites of coded Hispanic/Latino RPGs.
In addition, 45 of the coded RPGs planned to enroll participants or perform the studies in Latin America and represented 7 primary and 38 secondary performance sites (data not shown). Most of these sites were in Mexico (3 primary and 21 secondary sites), while others were in Argentina, Brazil, Chile, Colombia, Costa Rica, Dominican Republic, Guatemala, Honduras, Peru, Uruguay, and Venezuela. Twenty-six (26) of the RPGs in Latin America focused on Cancer, 11 on Diabetes and/or Obesity, 5 on Dementia, and 2 on Asthma. Also 20 (43.5%) of the RPGs proposed studies of mechanisms of disease, 17 (37%) basic research, 19 (41.3%) epidemiology, 15 (32.6%) behavioral studies, 13 (28.2%) clinical trials, and 4 (8.7%) secondary data analyses (data not shown).
Overall, 67% of applications used the term “Hispanic,” “Latino,” or “Spanish speakers” to describe the population of interest and did not further specify a Hispanic/Latino heritage group. Figure 5 shows how investigators described Hispanic/Latino populations of interest in the U.S. and abroad by sample/power category. Whereas, most of the Not Powered studies used the umbrella terms “Hispanics” or “Latinos,” most of the focused studies identified individual Hispanic/Latino heritage groups of interest. Sixty-seven (67) projects specified heritage groups of interest to be recruited in the U.S. Mainland: Mexican (13 Not Powered, 9 Powered, 30 Focused), Puerto Rican (2 Not Powered, 2 Powered, 2 Focused), Dominican (3 Not Powered, 1 Powered, 4 Focused), and Haitian (1 Focused) (data not shown). Forty-nine (49) projects identified specific heritage groups of interest to be recruited outside of the U.S. Mainland: Mexican (1 Not Powered, 1 Powered, 10 Focused), Puerto Rican (11 Focused), Central American (5 Focused), and South American (2 Not Powered, 2 Powered, 17 Focused) (data not shown). Across sample/power categories, Mexican was the most common individual Hispanic/Latino heritage group of interest of studies.
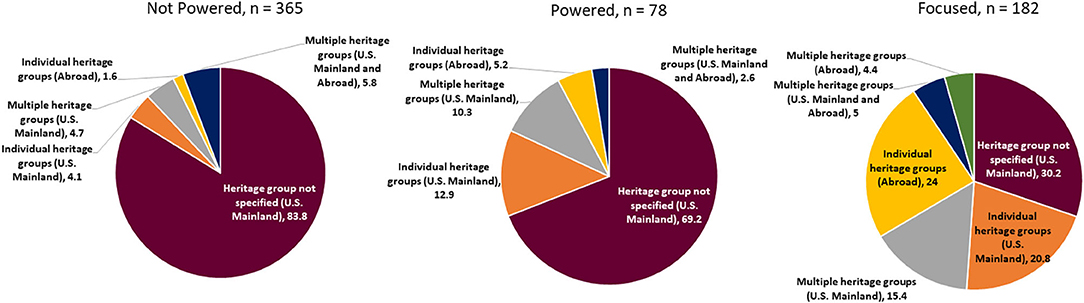
Figure 5. Hispanic/Latino heritage groups of interest by sample power category.
As described under Methods, RPGs that were originally funded prior to FY2008, even if renewed between FY2008-FY2015, were excluded because both the original applications and enrollment tables were not traceable. Similarly, non-RPGs funded prior to FY2008 or during the selected timeframe were not included. Table 4 shows RPGs funded prior to FY2008 and non-RPGs funded prior to and during FY2008, which were not included in the analysis but addressed any of the six health condition areas of interest and in which Hispanics/Latinos were the focus or one of the populations of interest or recruited (14–20, 47–80).
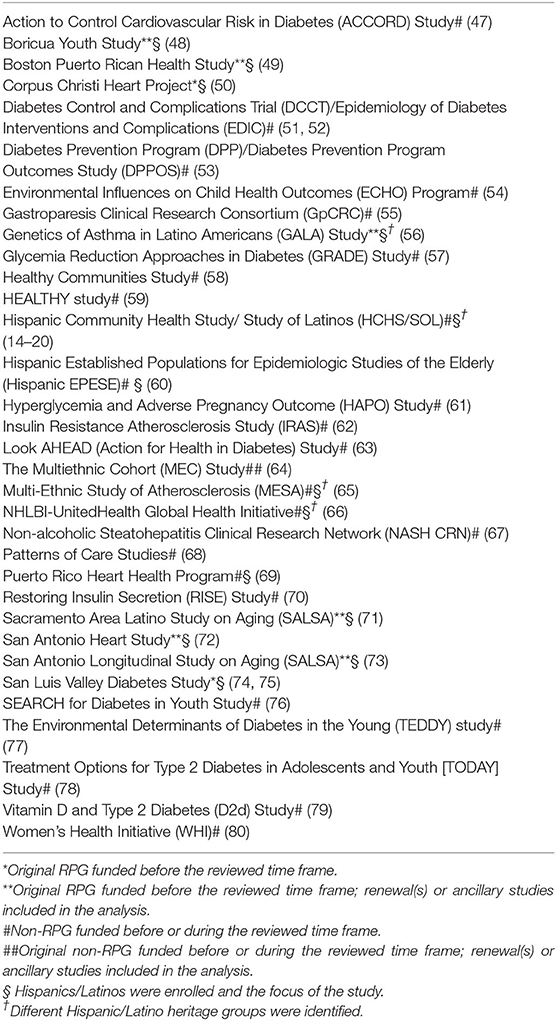
Table 4. Non-RPG studies in the six Health Condition Areas funded before or during FY2008-FY2015 with recruitment of Hispanics/Latinos in the U.S and/or Abroad.
In 1940, photographer Jack Delano was employed by the Farmers Security Administration (FSA) to photograph not only farmers, but all aspects of current social conditions in the U.S Virgin Islands and Puerto Rico. In the introduction to his book Puerto Rico Mío (81), Delano recalls a letter from a 14-year-old boy from El Paso, Texas. The young boy shared his admiration for the FSA pictures that Delano had taken and asked for his autograph. Compelled by the young boy's personal story of poverty and interest in photography, Delano sent him an autographed picture and asked him “What is it that you like about the FSA pictures?” The young boy wrote back: “I like the pictures because they make ordinary people important.”
The present study is a picture, a snapshot of the NIH-funded RPGs on Hispanic/Latino health. Our analysis demonstrated that 4.4% of RPGs funded between FY2008 and FY2015 identified Hispanics/Latinos as a population or the main population of interest. Among the RPGs addressing any of the health conditions of interest, mechanistic, behavioral, and epidemiological studies were the most common type of research, over 70% of the studies involved Obesity or Cancer as their main health condition of interest, 42% proposed a powered sample size or focused on Hispanics/Latinos, and the majority of the performance sites were located in U.S. areas with the highest concentration of Hispanic/Latino population.
The percentage of funded RPGs in which Hispanics/Latinos were a population of interest identified through our methods warrants consideration. The number of funded RPGs identified by our analysis paralleled the number of peer-reviewed RPG applications during the selected time frame. Approximately 12% of the principal investigators in the RPGs included in our analysis self-reported Hispanic/Latino ethnicity. In a previously published NIH-based analysis (82), the percent of NIH R01/RPG-awarded Hispanic/Latino investigators from FY2009 to FY2016 ranged from 3.4 to 5.0%. Although these two analyses evaluated slightly different portfolio metrics, both suggest the previously documented need for greater diversity in the biomedical workforce (83–89), and specifically for promoting the career development of more Hispanic/Latino biomedical researchers. Future studies could assess whether increasing the number of funded Hispanic/Latino investigators may increase the number of RPGs focused on Hispanic/Latino health research.
The types of research identified by our analysis need to be examined through the lens of the progressive recognition and increase in prevalence of chronic diseases and health risk factors and persistent health disparities experienced by many Hispanic/Latino communities. The predominance of mechanistic, behavioral studies (which could have included intervention or retrospective analyses) and epidemiological studies presents opportunities to evaluate knowledge gained and its clinical application, to test newly generated research hypotheses refocus scientific questions (90), update, or integrate novel research methods redesign (91, 92) that connect science with the health profile and health-care needs of the contemporary Hispanic/Latino populations.
At the same time, our analysis suggests that health services research, translational medicine, and/or CBPR are types of research that could be further developed within the context of the six health condition areas that were reviewed. Whereas the focus on implementation science and translational research at the NIH has been increasing (92, 93), our findings suggest that future research could focus on understudied approaches in Hispanic/Latino health, including, but not limited to, deeper understanding of effectiveness of currently recommended therapies and potential differences among heritage groups (56, 94–96); participation and/or increased inclusion in genetics/genomic studies (97–99); innovative strategies to implement recommended guidelines of care, and especially those move beyond the “sideways” approach (100); the intersection (101–103) of social determinants of health other factors on disease risk and the effectiveness of clinical or multi-level interventions (104–107); design and analysis of multi-level or multi-sectoral (108–110) interventions; implementation and dissemination studies in real-world settings (92, 111); the role of health information technologies on health-care delivery and health outcomes (112–118); the impact of interventions or policies designed to reduce health and health-care disparities (119–126); and the effects of national or local policies on health-care services and health outcomes (e.g., natural experiments) (127, 128) among Hispanic/Latino populations.
Although a literature review would offer a comprehensive view of the six health condition areas, the present analysis suggests some opportunities where research in Hispanic/Latino health could be expanded. For example, while asthma tends to be more prevalent in children, it is also highly prevalent in Puerto Rican adults as described in the HCHS/SOL (15). The study of asthma in adults could contribute to further understanding mechanisms of disease and response to treatment, especially in adults with coexisting chronic conditions. Also, most of the asthma interventions/clinical trials (67%) were focused on behavior (data not shown), suggesting that expanding research to other types of interventions could be considered. Many studies on cancer focused on increasing individual and/or community screening, awareness of risk factors, and prevention. Since cancer type and mortality vary by Hispanic/Latino heritage group (26–28, 129), additional research could focus on understanding mechanisms of disease, response to treatment, and risk or protective factors across heritage groups. Research in dementia could expand in multiple dimensions, from novel or unique mechanisms of cognitive decline (130), understanding differences in risk (131, 132) or manifestations of disease, and potential interventions to prevent the disease or delay its progression. Many diabetes studies in our analysis included clinical interventions focused on prevention (e.g., weight loss). The prevalence of diabetes mellitus among U. S. Hispanics/Latinos as a sole ethnic group has been consistently higher than NHWs (9), and varies by heritage group (17). Conversely, Hispanics/Latinos with diabetes mellitus are at increased risk of preventable acute and chronic complications (133, 134) and hospital readmissions (135, 136), and diabetes mellitus is one of the leading causes of death in these populations (137–139). Research on mechanisms underlying these inter-heritage differences, and on implementation of diabetes guidelines of care (140, 141), could potentially generate more targeted interventions that effectively prevent diabetes and its complications. A significant number of liver disease studies focused on hepatitis C within the context of HIV/AIDS, and risk and long-term consequences of liver injury, which are highly relevant among some Hispanic/Latino communities (142–144). Since gallbladder disease is highly prevalent among Hispanics/Latinos (11, 12, 145), and it has been associated with cardiometabolic disease risk factors (146–148), research dedicated to its prevention could impact not only Hispanics/Latinos, but other populations (149–151). Although outside of the scope of our analysis, factors mediating the lower mortality rates documented for Hispanics/Latinos as a group (23, 24, 139, 152, 153) are still not fully understood.
Forty-two percent of the projects included in the analysis focused on Hispanics/Latinos or incorporated Hispanic/Latino ethnicity into the planned sample size power estimates. The incorporation of Hispanic/Latino ethnicity in the power estimation of the planned sample size was an indicator of a deliberate interest to enroll Hispanics/Latinos in the study. In some studies, correlation analyses were proposed when Hispanic/Latino ethnicity was not accounted in the calculation of the power of the proposed sample (data not shown). Although it is not always possible to estimate the power of the planned sample size based on race/ethnicity (154), including a rationale for not doing so and acknowledging the limitations of correlation analyses in answering the central research question could be considered.
In 67% of the RPGs included in our analysis the ethnic identification of prospective participants (and/or data and biospecimen resources) was limited to the general Hispanic or Latino terms. Of note, 73 RPGs were not included in the analysis because the source of data or materials provided no race/ethnicity information. Including other heritage descriptors (e.g., birthplace, heritage or family roots, preferred language, parents' place of birth) could enhance the interpretation of study findings (155–157), since differences in the prevalence of some chronic diseases have been documented among different Hispanic/Latino heritage groups (13–15, 17). Socioeconomic descriptors (e.g., education attained, income) could also enhance the interpretation of health outcomes analyses, which would also be applicable to studies dedicated to other minority and underserved groups. Although confidentiality and data-sharing parameters might need to be evaluated, the collection of a minimum of such identifiers by biobanks, administrative databases, or registries would magnify the contribution of those unique resources to mechanistic studies, including genetics/genomics and precision medicine and health services research (158).
The location and distribution of the primary and secondary performance sites in the U.S. parallels the location of large academic centers and some of the states and cities with the highest concentration of Hispanics/Latinos (159, 160). This may result in potentially geographic, or heritage, specific findings, which may not apply to every location or Hispanic/Latino heritage group. Investments in multi-institutional collaborations across different geographic locations, training, and research capacity building of U.S. academic centers outside of major cities and near emerging Hispanic/Latino communities could fill this gap. Also, collaborations with research teams in Latin America could enhance research capacity building, key information exchange, and best research/clinical practices and to reduce the burden of chronic diseases throughout the Western hemisphere (161–163).
The findings of this analysis need to be interpreted within the context of some limitations. The degree of completeness of grant electronic data restricted our search to RPGs funded in or after 2008 and prevented the coding and analysis of large NIH-led initiatives (14–20, 47–80). RPGs alone do not reflect the NIH's full scope of funding of Hispanic/Latino health research. Although the search engine used RCDC-curated Hispanic/Latino identifiers, 107 applications (out of the 1,237) were not eligible for review because they did not mention Hispanics/Latinos in the planned enrollment tables. Based on NIH funding trends and the methods used in the present analysis, a significant percentage of the projects involved animal models or other non-human studies only. Hence, the overall percentage (4.4%) of all RPGs in which Hispanics/Latinos were truly as a population of interest could have been lower. On the other hand, the approach used to identify eligible RPGs in the present analysis differed from assessing inclusion of women, children and minorities in clinical research, as defined by the NIH OER (164), which considers inclusion as the participation of at least one human research participant from OMB-defined racial/ethnic minority groups and requires monitoring of enrollment of participants by sex and race/ethnicity in clinical research studies (165, 166). Therefore, during the selected time frame, there could have been additional RPGs that planned the inclusion of Hispanics/Latinos but did not identify them as a population of interest. This analysis focused on six health condition areas, and the distribution of funding mechanisms, types of research, age groups, and proposed enrollment might be different for projects in other health condition areas. Finally, we reviewed the proposed research work and planned enrollment of newly funded RPGs, not their completed enrollment and study findings. The final sample size and study findings derived from the RPGs included in this analysis might reveal scientific lessons learned about Hispanic/Latino health that could be evaluated in future analyses.
Twenty-seven years ago, the National Hispanic-Latino Initiative (156), led by U.S. Surgeon General Antonia Novello, identified “the need to increase research in Hispanic health and the participation of Hispanics in research” as top priorities. In 1995, the Secretary of the U.S. Department of Health and Human Services formed the Departmental Working Group on Hispanic Issues (157). This working group recommended plans of action on specific priority areas, including the assurance of “appropriate representation of Hispanics in research and identifying gaps in knowledge of health problems disproportionately affecting Hispanics and taking action to address them” (157). Since then, the NIH has sponsored initiatives—funded through cooperative agreements or contracts—in which Hispanics/Latinos have been the focus or a population of interest (14–20, 47–80). The Hispanic Community Health Study/Study of Latinos (HCHS/SOL), the most recent NIH initiative dedicated to Hispanic/Latino health, has set a foundation to better understand similarities and differences in the prevalence of selected chronic diseases and their risk factors and health events in a cohort of Hispanics/Latinos living in four U.S. cities (14–20).
Although such initiatives have advanced our understanding of the health of Hispanics/Latinos, our analysis posits both the need and the opportunities for continued research in Hispanic/Latino health. The present analysis highlights a percentage of investigator-initiated projects with interest in Hispanic/Latino health for which there is evident room for expansion. The role and scientific contributions of large initiatives and smaller-scale investigator-initiated studies is an ongoing discussion (167–170), which brings to mind a quote attributed to activist Cesar Chavez: “The fight is never about grapes or lettuce. It is always about the people.” Considering the diversity of the Hispanic/Latino populations and the complexity and persistence of the health disparities experienced across heritage groups, research on Hispanic/Latino health should propel scientific discoveries that harness cutting-edge science with the imminent health and health-care needs of the populations. While there is no formula for the right or acceptable number of Hispanic/Latino health RPGs that should be funded, a larger proportion of investigator-initiated projects that embrace new paradigms and transform knowledge into action would be an enriching ingredient to the “right mix” (169). It is research that improves health outcomes and changes the portrait of health of the Hispanic/Latino people.
The datasets for this article are not publicly available because they represent U.S. government funded biomedical research projects and considered confidential. Some of the data presented in our analysis are available through https://report.nih.gov. Requests to access the NIH datasets beyond those available in RePORT should be made to http://www.nih.gov/icd/od/foia/.
MA-S led the team. MA-S, LH, TL, SA, LA, LC, PD-N, HN, and AR conceptualized the design of the coding protocol, including use of the internal search engine, and data extraction for review. MA-S, LH, TL, SA, LA, LC, JC, PD-N, HN, and AR participated in some or all the data review (coding). LH and SC did the statistical analyses. MA-S wrote the manuscript. LH, TL, SC, SA, LA, LC, JC, HN, and AR provided critical review and revisions. All authors approved the final version.
The views expressed in this manuscript are those of the authors and do not necessarily reflect the official views of the National Institute on Minority Health and Health Disparities, the National Heart, Lung, and Blood Institute, the National Cancer Institute, the National Institutes of Health, or the U.S. federal government.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to thank Dr. Iván Navarro (NIH-NIA) and Dr. Mary L. García-Cazarín (NIH-OD) for their valuable input during the design of the review protocol. The authors would also like to thank the NIH Office of Extramural Research (OER) for providing additional data, analyses, and consultation and Dr. Jean L. Olson (previously at NIH-NHLBI) and Dr. Eliseo J. Pérez-Stable (Director of NIMHD) for their critical review of the manuscript.
1. Oh SS, Galanter J, Thakur N, Pino-Yanes M, Barcelo NE, White MJ, et al. Diversity in clinical and biomedical research: a promise yet to be fulfilled. PLoS Med. (2015) 12:e1001918. doi: 10.1371/journal.pmed.1001918
2. Mathew SS, Barwell J, Khan N, Lynch E, Parker M, Qureshi N. Inclusion of diverse populations in genomic research and health services: genomix workshop report. J Commun Genet. (2017) 8:267–73. doi: 10.1007/s12687-017-0317-5
3. Burchard EG, Oh SS, Foreman MG, Celedon JC. Moving toward true inclusion of racial/ethnic minorities in federally funded studies. A key step for achieving respiratory health equality in the United States. Am J Respir Crit Care Med. (2015) 191:514–21. doi: 10.1164/rccm.201410-1944PP
4. Features FF. Hispanic Heritage Month 2019 United States Census Bureau. (2019). Available online at: https://www.census.gov/newsroom/facts-for-features/2019/hispanic-heritage-month.html (accessed May 28, 2020).
5. Krogstad JM, Noe-Bustamante L. 7 Facts for National Hispanic Heritage Month. Pew Research Center (2019). Available online at: https://www.pewresearch.org/fact-tank/2019/10/14/facts-for-national-hispanic-heritage-month/ (accessed May 28, 2020).
6. Vargas Bustamante A, Fang H, Rizzo JA, Ortega AN. Understanding observed and unobserved health care access and utilization disparities among US Latino adults. Med Care Res Rev. (2009) 66:561–77. doi: 10.1177/1077558709338487
7. Twarog JP, Charyalu AM, Subhani MR, Shrestha P, Peraj E. Differences in HbA1C% screening among US adults diagnosed with diabetes: findings from the National Health And Nutrition Examination Survey (NHANES). Prim Care Diabetes. (2018) 12:533–6. doi: 10.1016/j.pcd.2018.07.006
8. Miller KD, Goding Sauer A, Ortiz AP, Fedewa SA, Pinheiro PS, Tortolero-Luna G, et al. Cancer statistics for Hispanics/Latinos, 2018. CA Cancer J Clin. (2018) 68:425–45. doi: 10.3322/caac.21494
9. Menke A, Casagrande S, Geiss L, Cowie CC. Prevalence of and trends in diabetes among adults in the United States, 1988-2012. JAMA. (2015) 314:1021–9. doi: 10.1001/jama.2015.10029
10. Arif AA, Delclos GL, Lee ES, Tortolero SR, Whitehead LW. Prevalence and risk factors of asthma and wheezing among US adults: an analysis of the NHANES III data. Eur Respir J. (2003) 21:827–33. doi: 10.1183/09031936.03.00054103a
11. Everhart JE, Khare M, Hill M, Maurer KR. Prevalence and ethnic differences in gallbladder disease in the United States. Gastroenterology. (1999) 117:632–9. doi: 10.1016/S0016-5085(99)70456-7
12. Everhart JE. Gallstones and ethnicity in the Americas. J Assoc Acad Minor Phys. (2001) 12:137–43.
13. Dominguez K, Penman-Aguilar A, Chang MH, Moonesinghe R, Castellanos T, Rodriguez-Lainz A, et al. Vital signs: leading causes of death, prevalence of diseases and risk factors, and use of health services among Hispanics in the United States - 2009-2013. Morb Mortal Wkly Rep. (2015) 64:469–78.
14. Daviglus ML, Talavera GA, Aviles-Santa ML, Allison M, Cai J, Criqui MH, et al. Prevalence of major cardiovascular risk factors and cardiovascular diseases among Hispanic/Latino individuals of diverse backgrounds in the United States. JAMA. (2012) 308:1775–84. doi: 10.1001/jama.2012.14517
15. Barr RG, Aviles-Santa L, Davis SM, Aldrich TK, Gonzalez F 2nd, Henderson AG, et al. Pulmonary disease and age at immigration among Hispanics. Results from the Hispanic community health study/study of Latinos. Am J Respir Crit Care Med. (2016) 193:386–95. doi: 10.1164/rccm.201506-1211OC
16. Heiss G, Snyder ML, Teng Y, Schneiderman N, Llabre MM, Cowie C, et al. Prevalence of metabolic syndrome among Hispanics/Latinos of diverse background: the Hispanic Community Health Study/Study of Latinos. Diabetes Care. (2014) 37:2391–9. doi: 10.2337/dc13-2505
17. Schneiderman N, Llabre M, Cowie CC, Barnhart J, Carnethon M, Gallo LC, et al. Prevalence of diabetes among Hispanics/Latinos from diverse backgrounds: the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Diabetes Care. (2014) 37:2233–9. doi: 10.2337/dc13-2939
18. Kuniholm MH, Jung M, Everhart JE, Cotler S, Heiss G, McQuillan G, et al. Prevalence of hepatitis C virus infection in US Hispanic/Latino adults: results from the NHANES 2007-2010 and HCHS/SOL studies. J Infect Dis. (2014) 209:1585–90. doi: 10.1093/infdis/jit672
19. Kuniholm MH, Jung M, Del Amo J, Talavera GA, Thyagarajan B, Hershow RC, et al. Awareness of hepatitis C virus seropositivity and chronic infection in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). J Immigr Minor Health. (2016) 18:1257–65. doi: 10.1007/s10903-016-0350-1
20. Kallwitz ER, Daviglus ML, Allison MA, Emory KT, Zhao L, Kuniholm MH, et al. Prevalence of suspected nonalcoholic fatty liver disease in Hispanic/Latino individuals differs by heritage. Clin Gastroenterol Hepatol. (2015) 13:569–76. doi: 10.1016/j.cgh.2014.08.037
21. Markides KS, Coreil J. The health of Hispanics in the southwestern United States: an epidemiologic paradox. Public Health Rep. (1986) 101:253–65.
22. Sorlie PD, Backlund E, Johnson NJ, Rogot E. Mortality by Hispanic status in the United States. JAMA. (1993) 270:2464–8. doi: 10.1001/jama.270.20.2464
23. Fenelon A, Chinn JJ, Anderson RN. A comprehensive analysis of the mortality experience of Hispanic subgroups in the United States: variation by age, country of origin, and nativity. SSM Popul Health. (2017) 3:245–54. doi: 10.1016/j.ssmph.2017.01.011
24. Kochanek KD, Murphy SL, Xu J, Arias E. Deaths: Final Data for 2017. National Vital Statistics Reports (2019). Available online at: https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_09-508.pdf
25. National Institutes of Health Office of Intramural Research. Hispanic Health Research Scientific Interest Group. Available online at: https://oir.nih.gov/sigs/hispanic-health-research-scientific-interest-group (accessed on May 28, 2020).
26. Pinheiro PS, Callahan KE, Siegel RL, Jin H, Morris CR, Trapido EJ, et al. Cancer mortality in Hispanic ethnic groups. Cancer Epidemiol Biomarkers Prev. (2017) 26:376–82. doi: 10.1158/1055-9965.EPI-16-0684
27. Pinheiro PS, Callahan KE, Gomez SL, Marcos-Gragera R, Cobb TR, Roca-Barcelo A, et al. High cancer mortality for US-born Latinos: evidence from California and Texas. BMC Cancer. (2017) 17:478. doi: 10.1186/s12885-017-3469-0
28. Martinez Tyson D, Medina-Ramirez P, Flores AM, Siegel R, Aguado Loi C. Unpacking Hispanic ethnicity-cancer mortality differentials among Hispanic subgroups in the United States, 2004-2014. Front Public Health. (2018) 6:219. doi: 10.3389/fpubh.2018.00219
29. NIH Research Portfolio Online Reporting Tools (RePORT). Funding: Budget and Spending. Available online at: https://report.nih.gov/budget_and_spending/index.aspx (accessed May 28, 2020).
30. NIH Research Portfolio Online Reporting Tools (RePORT). NIH Databook: Success Rates R01-Equivalent and Research Project Grants. Available online at: https://report.nih.gov/nihdatabook/category/10 (accessed May 28, 2020).
31. National Institutes of Health. NIH Policy on Reporting Race and Ethnicity Data: Subjects in Clinical Research. (2001). Available online at: https://grants.nih.gov/grants/guide/notice-files/NOT-OD-01-053.html (accessed May 28, 2020).
32. National Institutes of Health. Racial and Ethnic Categories and Definitions for NIH Diversity Programs and for Other Reporting Purposes. (2015). Available online at: https://grants.nih.gov/grants/guide/notice-files/not-od-15-089.html (accessed on May 28, 2020).
33. Rojas Mix M. Los Cien Nombres de América. Barcelona: Editorial Lumen, Editorial Andres Bello (1991).
34. Reid M. Forgotten Continent: The Battle for Latin America's Soul. New Haven, CT; London, UK: Yale University Press (2009).
36. National Institutes of Health. NIH Research Portfolio Online Reporting Tools (RePORT): The Research, Condition, and Disease Categorization Process. Available online at: https://report.nih.gov/rcdc/ (accessed May 28, 2020).
37. National Institutes of Health. NIH Glossary and Acronym List – Basic Research. (2020). Available online at: https://grants.nih.gov/grants/glossary.htm#BasicResearch (accessed May 28, 2020).
38. National Institutes of Health. NIH Glossary and Acronym List – Mechanistic Study. Available online at: https://grants.nih.gov/grants/glossary.htm#MechanisticStudy (accessed May 28, 2020).
39. National Institutes of Health. NIH Glossary and Acronym List – Clinical Research. Available online at: https://grants.nih.gov/grants/glossary.htm#ClinicalResearch (accessed May 28, 2020).
40. National Institutes of Health. NIH Glossary and Acronym List – Clinical Trial. Available online at: https://grants.nih.gov/grants/glossary.htm#ClinicalTrial (accessed May 28, 2020).
41. National Institutes of Health. NIH Glossary and Acronym List – Translational Research. Available online at: https://grants.nih.gov/grants/glossary.htm#TranslationalResearch (accessed May 28, 2020).
42. Agency for Healthcare Research and Quality. Health Services Research. Available online at: https://www.ahrq.gov/funding/training-grants/hsrguide/hsrguide.html (accessed May 28, 2020).
43. Johnston MP. Secondary data analysis: a method of which the time has come. QQML. (2014) 3:619–26.
44. Israel BA, Parker EA, Rowe Z, Salvatore A, Minkler M, Lopez J, et al. Community-based participatory research: lessons learned from the Centers for Children's Environmental Health and Disease Prevention research. Environ Health Perspect. (2005) 113:1463–71. doi: 10.1289/ehp.7675
45. National Institutes of Health. Office of Portfolio Analysis. Available online at: https://dpcpsi.nih.gov/opa (accessed May 28, 2020).
46. NIH Research Portfolio Online Reporting Tools (RePORT). NIH Databook: Funding Rates. Available online at: https://report.nih.gov/nihdatabook/category/22 (accessed May 28, 2020).
47. Gerstein HC, Miller ME, Genuth S, Ismail-Beigi F, Buse JB, Goff DC, et al. Long-term effects of intensive glucose lowering on cardiovascular outcomes. N Engl J Med. (2011) 364:818–28. doi: 10.1056/NEJMoa1006524
48. Feldman JM, Ortega AN, Koinis-Mitchell D, Kuo AA, Canino G. Child and family psychiatric and psychological factors associated with child physical health problems: results from the Boricua Youth Study. J Nerv Ment Dis. (2010) 198:272–9. doi: 10.1097/NMD.0b013e3181d61271
49. Tucker KL, Mattei J, Noel SE, Collado BM, Mendez J, Nelson J, et al. The Boston Puerto Rican Health Study, a longitudinal cohort study on health disparities in Puerto Rican adults: challenges and opportunities. BMC Public Health. (2010) 10:107. doi: 10.1186/1471-2458-10-107
50. Orlander PR, Goff DC, Morrissey M, Ramsey DJ, Wear ML, Labarthe DR, et al. The relation of diabetes to the severity of acute myocardial infarction and post-myocardial infarction survival in Mexican-Americans and non-Hispanic whites. The Corpus Christi heart project. Diabetes. (1994) 43:897–902. doi: 10.2337/diabetes.43.7.897
51. Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, Davis M, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. (1993) 329:977–86. doi: 10.1056/NEJM199309303291401
52. Epidemiology of Diabetes Interventions and Complications Research Group. Epidemiology of diabetes interventions and complications (EDIC). Design, implementation, and preliminary results of a long-term follow-up of the diabetes control and complications trial cohort. Diabetes Care. (1999) 22:99–111.
53. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. (2002) 346:393–403. doi: 10.1056/NEJMoa012512
54. National Institutes of Health. The Environmental Influences on Child Health Outcomes (ECHO) Program. Available online at: https://www.nih.gov/research-training/environmental-influences-child-health-outcomes-echo-program (accessed May 28, 2020).
55. Koch KL, Hasler WL, Yates KP, Parkman HP, Pasricha PJ, Calles-Escandon J, et al. Baseline features and differences in 48 week clinical outcomes in patients with gastroparesis and type 1 vs type 2 diabetes. Neurogastroenterol Motil. (2016) 28:1001–15. doi: 10.1111/nmo.12800
56. Burchard EG, Avila PC, Nazario S, Casal J, Torres A, Rodriguez-Santana JR, et al. Lower bronchodilator responsiveness in Puerto Rican than in Mexican subjects with asthma. Am J Respir Crit Care Med. (2004) 169:386–92. doi: 10.1164/rccm.200309-1293OC
57. Nathan DM, Buse JB, Kahn SE, Krause-Steinrauf H, Larkin ME, Staten M, et al. Rationale and design of the glycemia reduction approaches in diabetes: a comparative effectiveness study (GRADE). Diabetes Care. (2013) 36:2254–61. doi: 10.2337/dc13-0356
58. Arteaga SS, Loria CM, Crawford PB, Fawcett SB, Fishbein HA, Gregoriou M, et al. The Healthy Communities study: its rationale, aims, and approach. Am J Prev Med. (2015) 49:615–23. doi: 10.1016/j.amepre.2015.06.029
59. Hirst K, Baranowski T, deBar L, Foster GD, Kaufman F, Kennel P, et al. HEALTHY study rationale, design and methods: moderating risk of type 2 diabetes in multi-ethnic middle school students. Int J Obes. (2009) 33(Suppl. 4):S4–20. doi: 10.1038/ijo.2009.112
60. Beard HA, AlGhatrif M, Samper-Ternent R, Gerst K, Markides KS. Trends in diabetes prevalence and diabetes-related complications in older Mexican Americans from 1993-1994 to 2004-2005. Diabetes Care. (2009) 32:2212–7. doi: 10.2337/dc09-0938
61. Lowe LP, Metzger BE, Dyer AR, Lowe J, McCance DR, Lappin TR, et al. Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study: associations of maternal A1C and glucose with pregnancy outcomes. Diabetes Care. (2012) 35:574–80. doi: 10.2337/dc11-1687
62. Wagenknecht LE, Mayer EJ, Rewers M, Haffner S, Selby J, Borok GM, et al. The Insulin Resistance Atherosclerosis Study (IRAS) objectives, design, and recruitment results. Ann Epidemiol. (1995) 5:464–72. doi: 10.1016/1047-2797(95)00062-3
63. Bray G, Gregg E, Haffner S, Pi-Sunyer XF, WagenKnecht LE, Walkup M, et al. Baseline characteristics of the randomised cohort from the Look AHEAD (Action for health in diabetes) study. Diab Vasc Dis Res. (2006) 3:202–15. doi: 10.3132/dvdr.2006.031
64. Kolonel LN, Altshuler D, Henderson BE. The multiethnic cohort study: exploring genes, lifestyle and cancer risk. Nat Rev Cancer. (2004) 4:519–27. doi: 10.1038/nrc1389
65. Sharrett AR, Ding J, Criqui MH, Saad MF, Liu K, Polak JF, et al. Smoking, diabetes, and blood cholesterol differ in their associations with subclinical atherosclerosis: the Multiethnic Study of Atherosclerosis (MESA). Atherosclerosis. (2006) 186:441–7. doi: 10.1016/j.atherosclerosis.2005.08.010
66. Bloomfield GS, Xavier D, Belis D, Alam D, Davis P, Dorairaj P, et al. Training and capacity building in LMIC for research in heart and lung diseases: the NHLBI-United Health Global Health Centers of excellence program. Glob Heart. (2016) 11:17–25. doi: 10.1016/j.gheart.2016.01.004
67. Brunt EM, Kleiner DE, Wilson LA, Unalp A, Behling CE, Lavine JE, et al. Portal chronic inflammation in nonalcoholic fatty liver disease (NAFLD): a histologic marker of advanced NAFLD-Clinicopathologic correlations from the nonalcoholic steatohepatitis clinical research network. Hepatology. (2009) 49:809–20. doi: 10.1002/hep.22724
68. National Cancer Institute. Patterns of Care Studies. Available online at: https://healthcaredelivery.cancer.gov/poc/ (accessed May 28, 2020).
69. Cruz-Vidal M, Garcia-Palmieri MR, Costas R Jr, Sorlie PD, Havlik RJ. Abnormal blood glucose and coronary heart disease: the Puerto Rico heart health program. Diabetes Care. (1983) 6:556–61. doi: 10.2337/diacare.6.6.556
70. RISE Consortium. Restoring Insulin Secretion (RISE): design of studies of beta-cell preservation in prediabetes and early type 2 diabetes across the life span. Diabetes Care. (2014) 37:780–8. doi: 10.2337/dc13-1879
71. Wu JH, Haan MN, Liang J, Ghosh D, Gonzalez HM, Herman WH. Diabetes as a predictor of change in functional status among older Mexican Americans: a population-based cohort study. Diabetes Care. (2003) 26:314–9. doi: 10.2337/diacare.26.2.314
72. Wei M, Gaskill SP, Haffner SM, Stern MP. Effects of diabetes and level of glycemia on all-cause and cardiovascular mortality. The San Antonio heart study. Diabetes Care. (1998) 21:1167–72. doi: 10.2337/diacare.21.7.1167
73. Fowler SP, Williams K, Hazuda HP. Diet soda intake is associated with long-term increases in waist circumference in a biethnic cohort of older adults: the San Antonio longitudinal study of aging. J Am Geriatr Soc. (2015) 63:708–15. doi: 10.1111/jgs.13376
74. Hildreth KL, Grigsby J, Bryant LL, Wolfe P, Baxter J. Cognitive decline and cardiometabolic risk among Hispanic and non-Hispanic white adults in the San Luis Valley health and aging study. J Behav Med. (2014) 37:332–42. doi: 10.1007/s10865-013-9491-z
75. Marshall JA, Hamman RF, Baxter J, Mayer EJ, Fulton DL, Orleans M, et al. Ethnic differences in risk factors associated with the prevalence of non-insulin-dependent diabetes mellitus. The San Luis valley diabetes study. Am J Epidemiol. (1993) 137:706–18. doi: 10.1093/oxfordjournals.aje.a116731
76. Mayer-Davis EJ, Lawrence JM, Dabelea D, Divers J, Isom S, Dolan L, et al. Incidence trends of type 1 and type 2 diabetes among youths, 2002-2012. N Engl J Med. (2017) 376:1419–29. doi: 10.1056/NEJMoa1610187
77. Krischer JP, Lynch KF, Schatz DA, Ilonen J, Lernmark A, Hagopian WA, et al. The 6 year incidence of diabetes-associated autoantibodies in genetically at-risk children: the TEDDY study. Diabetologia. (2015) 58:980–7. doi: 10.1007/s00125-015-3514-y
78. TODAY Study Group. Design of a family-based lifestyle intervention for youth with type 2 diabetes: the TODAY study. Int J Obes. (2010) 34:217–26. doi: 10.1038/ijo.2009.195
79. LeBlanc ES, Pratley RE, Dawson-Hughes B, Staten MA, Sheehan PR, Lewis MR, et al. Baseline characteristics of the vitamin D and type 2 diabetes (D2d) study: a contemporary prediabetes cohort that will inform diabetes prevention efforts. Diabetes Care. (2018) 41:1590–9. doi: 10.2337/db18-765-P
80. Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the women's health initiative randomized controlled trial. JAMA. (2002) 288:321–33. doi: 10.1001/jama.288.3.321
82. Nikaj S, Roychowdhury D, Lund PK, Matthews M, Pearson K. Examining trends in the diversity of the US National Institutes of Health participating and funded workforce. FASEB J. (2018) 2018:fj201800639. doi: 10.1096/fj.201800639
83. Cohen JJ, Gabriel BA, Terrell C. The case for diversity in the health care workforce. Health Aff. (2002) 21:90–102. doi: 10.1377/hlthaff.21.5.90
84. Institute of Medicine Committee on Institutional Policy-Level Strategies for Increasing Diversity of the US Healthcare Workforce. In the Nation's Compelling Interest: Ensuring Diversity in the Health-Care Workforce. Smedley BD, Stith Butler A, Bristow LR, editors. Washington, DC: National Academies Press (2004).
85. Ginther DK, Schaffer WT, Schnell J, Masimore B, Liu F, Haak LL, et al. Race, ethnicity, and NIH research awards. Science. (2011) 333:1015–9. doi: 10.1126/science.1196783
86. Ginther DK, Haak LL, Schaffer WT, Kington R. Are race, ethnicity, and medical school affiliation associated with NIH R01 type 1 award probability for physician investigators? Acad Med. (2012) 87:1516–24. doi: 10.1097/ACM.0b013e31826d726b
87. Wilder EL, Tabak LA, Pettigrew RI, Collins FS. Biomedical research: strength from diversity. Science. (2013) 342:798. doi: 10.1126/science.342.6160.798-a
88. Heggeness ML, Evans L, Pohlhaus JR, Mills SL. Measuring diversity of the National Institutes of Health-Funded Workforce. Acad Med. (2016) 91:1164–72. doi: 10.1097/ACM.0000000000001209
89. Rubio DM, Mayowski CA, Norman MK. A multi-pronged approach to diversifying the workforce. Int J Environ Res Public Health. (2018) 15:2219. doi: 10.3390/ijerph15102219
90. Lauer MS. Time for a creative transformation of epidemiology in the United States. JAMA. (2012) 308:1804–5. doi: 10.1001/jama.2012.14838
91. Khoury MJ, Lam TK, Ioannidis JP, Hartge P, Spitz MR, Buring JE, et al. Transforming epidemiology for 21st century medicine and public health. Cancer Epidemiol Biomarkers Prev. (2013) 22:508–16. doi: 10.1158/1055-9965.EPI-13-0146
92. Mensah GA, Cooper RS, Siega-Riz AM, Cooper LA, Smith JD, Brown CH, et al. Reducing cardiovascular disparities through community-engaged implementation research: a National Heart, Lung, and Blood Institute workshop report. Circ Res. (2018) 122:213–30. doi: 10.1161/CIRCRESAHA.117.312243
93. Engelgau MM, Peprah E, Sampson UKA, Mishoe H, Benjamin IJ, Douglas PS, et al. Perspectives from NHLBI global health think tank meeting for late stage (T4) translation research. Glob Heart. (2017) 12:341–8. doi: 10.1016/j.gheart.2016.03.640
94. Goel S, Negassa A, Khot A, Goyal D, Guo S, Nandikolla A, et al. Comparative effectiveness research: the impact of biologic agents in ethnic minorities with metastatic colorectal cancer. Clin Colorectal Cancer. (2017) 16:286–92. doi: 10.1016/j.clcc.2017.03.004
95. Mak M, Lam C, Pineda SJ, Lou M, Xu LY, Meeks C, et al. Pharmacogenetics of warfarin in a diverse patient population. J Cardiovasc Pharmacol Ther. (2019) 24:521–33. doi: 10.1177/1074248419843530
96. Claudio-Campos K, Labastida A, Ramos A, Gaedigk A, Renta-Torres J, Padilla D, et al. Warfarin anticoagulation therapy in Caribbean Hispanics of Puerto Rico: a candidate gene association study. Front Pharmacol. (2017) 8:347. doi: 10.3389/fphar.2017.00347
97. Sirugo G, Williams SM, Tishkoff SA. The missing diversity in human genetic studies. Cell. (2019) 177:26–31. doi: 10.1016/j.cell.2019.02.048
98. Haga SB. Impact of limited population diversity of genome-wide association studies. Genet Med. (2010) 12:81–4. doi: 10.1097/GIM.0b013e3181ca2bbf
99. Wojcik GL, Graff M, Nishimura KK, Tao R, Haessler J, Gignoux CR, et al. Genetic analyses of diverse populations improves discovery for complex traits. Nature. (2019) 570:514–8. doi: 10.1038/s41586-019-1310-4
100. Alvidrez J, Stinson N Jr. Sideways progress in intervention research is not sufficient to eliminate health disparities. Am J Public Health. (2019) 109:S102–4. doi: 10.2105/AJPH.2019.304953
101. Burris HH, Hacker MR. Birth outcome racial disparities: a result of intersecting social and environmental factors. Semin Perinatol. (2017) 41:360–6. doi: 10.1053/j.semperi.2017.07.002
102. Vega IE, Cabrera LY, Wygant CM, Velez-Ortiz D, Counts SE. Alzheimer's disease in the latino community: intersection of genetics and social determinants of health. J Alzheimers Dis. (2017) 58:979–92. doi: 10.3233/JAD-161261
103. Gkiouleka A, Huijts T, Beckfield J, Bambra C. Understanding the micro and macro politics of health: inequalities, intersectionality & institutions - a research agenda. Soc Sci Med. (2018) 200:92–8. doi: 10.1016/j.socscimed.2018.01.025
104. Paskett E, Thompson B, Ammerman AS, Ortega AN, Marsteller J, Richardson D. Multilevel interventions to address health disparities show promise in improving population health. Health Aff. (2016) 35:1429–34. doi: 10.1377/hlthaff.2015.1360
105. Evans CR, Williams DR, Onnela JP, Subramanian SV. A multilevel approach to modeling health inequalities at the intersection of multiple social identities. Soc Sci Med. (2018) 203:64–73. doi: 10.1016/j.socscimed.2017.11.011
106. Agurs-Collins T, Persky S, Paskett ED, Barkin SL, Meissner HI, Nansel TR, et al. Designing and assessing multilevel interventions to improve minority health and reduce health disparities. Am J Public Health. (2019) 109:S86–93. doi: 10.2105/AJPH.2018.304730
107. Alvidrez J, Castille D, Laude-Sharp M, Rosario A, Tabor D. The National Institute on minority health and health disparities research framework. Am J Public Health. (2019) 109:S16–20. doi: 10.2105/AJPH.2018.304883
108. Philbin MM, Flake M, Hatzenbuehler ML, Hirsch JS. State-level immigration and immigrant-focused policies as drivers of Latino health disparities in the United States. Soc Sci Med. (2018) 199:29–38. doi: 10.1016/j.socscimed.2017.04.007
109. Milman HM, Castillo CA, Sansotta AT, Delpiano PV, Murray J. Scaling up an early childhood development programme through a national multisectoral approach to social protection: lessons from Chile Crece Contigo. BMJ. (2018) 363:k4513. doi: 10.1136/bmj.k4513
110. Rivillas JC, Colonia FD. Reducing causes of inequity: policies focused on social determinants of health during generational transitions in Colombia. Glob Health Action. (2017) 10:1349238. doi: 10.1080/16549716.2017.1349238
111. Nápoles AM, Stewart AL. Transcreation: an implementation science framework for community-engaged behavioral interventions to reduce health disparities. BMC Health Serv Res. (2018) 18:710. doi: 10.1186/s12913-018-3521-z
112. Gopalan A, Makelarski JA, Garibay LB, Escamilla V, Merchant RM, Wolfe MB, et al. Health-Specific information and communication technology use and its relationship to obesity in high-poverty, urban communities: analysis of a population-based biosocial survey. J Med Internet Res. (2016) 18:e182. doi: 10.2196/jmir.5741
113. Manganello JA, Gerstner G, Pergolino K, Graham Y, Strogatz D. Media and technology use among Hispanics/Latinos in New York: implications for health communication programs. J Racial Ethn Health Disparities. (2016) 3:508–17. doi: 10.1007/s40615-015-0169-9
114. Ramírez AS, Estrada E, Ruiz A. Mapping the health information landscape in a rural, culturally diverse region: implications for interventions to reduce information inequality. J Prim Prev. (2017) 38:345–62. doi: 10.1007/s10935-017-0466-7
115. Gonzalez M, Sanders-Jackson A, Wright T. Web-based health information technology: access among Latinos varies by subgroup affiliation. J Med Internet Res. (2019) 21:e10389. doi: 10.2196/10389
116. Mitchell UA, Chebli PG, Ruggiero L, Muramatsu N. The digital divide in health-related technology use: the significance of race/ethnicity. Gerontologist. (2019) 59:6–14. doi: 10.1093/geront/gny138
117. Zhang X, Hailu B, Tabor DC, Gold R, Sayre MH, Sim I, et al. Role of health information technology in addressing health disparities: patient, clinician, and system perspectives. Med Care. (2019) 57(Suppl. 6):S115–20. doi: 10.1097/MLR.0000000000001092
118. National Academies of Sciences Engineering Medicine Policy Global A Government-University-Industry Research R. The National Academies Collection: Reports Funded by National Institutes of Health. In: Casola L, editor. Using Research and Technology to Address Compounding Disparities: Proceedings of a Workshop-in Brief. The National Academies Collection: Reports Funded by National Institutes of Health. Washington, DC: National Academies Press (2020).
119. Buchmueller TC, Levinson ZM, Levy HG, Wolfe BL. Effect of the affordable care act on racial and ethnic disparities in health insurance coverage. Am J Public Health. (2016) 106:1416–21. doi: 10.2105/AJPH.2016.303155
120. Mahmoudi E, Tarraf W, Maroukis BL, Levy HG. Does medicare managed care reduce racial/ethnic disparities in diabetes preventive care and healthcare expenditures? Am J Manag Care. (2016) 22:e360−7.
121. Okoro CA, Zhao G, Fox JB, Eke PI, Greenlund KJ, Town M. Surveillance for health care access and health services use, adults aged 18-64 years - behavioral risk factor surveillance system, United States, 2014. MMWR Surveill Summ. (2017) 66:1–42. doi: 10.15585/mmwr.ss6607a1
122. Bloodworth R, Chen J, Mortensen K. Variation of preventive service utilization by state medicaid coverage, cost-sharing, and medicaid expansion status. Prev Med. (2018) 115:97–103. doi: 10.1016/j.ypmed.2018.08.020
123. Shi Q, Fonseca V, Krousel-Wood M, Zhao Y, Nellans FP, Luo Q, et al. Will the Affordable Care Act (ACA) improve racial/ethnic disparity of eye examination among US working-age population with diabetes? Curr Diab Rep. (2016) 16:58 doi: 10.1007/s11892-016-0749-z
124. Barnes JM, Brown DS, Harris JK, King AA, Johnson KJ. Impact of the affordable care act dependent coverage provision on young adult cancer patient insurance coverage by sociodemographic and economic characteristics. Cancer Causes Control. (2020) 31:33–42. doi: 10.1007/s10552-019-01246-3
125. Buchmueller TC, Levy HG. The ACA's impact on racial and ethnic disparities in health insurance coverage and access to care. Health Aff. (2020) 39:395–402. doi: 10.1377/hlthaff.2019.01394
126. Gai Y, Jones K. Insurance patterns and instability from 2006 to 2016. BMC Health Serv Res. (2020) 20:334. doi: 10.1186/s12913-020-05226-1
127. Mbah OM, Kinlaw AC, Trogdon JG, Wheeler SB, Samuel CA. The affordable care act and ethnic disparities in colorectal cancer screening. Am J Prev Med. (2020) 58:175–81. doi: 10.1016/j.amepre.2019.09.002
128. Albini PT, Cochran-Yu MR, Godat LN, Costantini TW, Doucet JJ. Who's being left behind? Uninsured emergency general surgery admissions after the ACA. Am J Surg. (2019) 218:1102–9. doi: 10.1016/j.amjsurg.2019.10.005
129. Stern MC, Fejerman L, Das R, Setiawan VW, Cruz-Correa MR, Perez-Stable EJ, et al. Variability in cancer risk and outcomes within US Latinos by national origin and genetic ancestry. Curr Epidemiol Rep. (2016) 3:181–90. doi: 10.1007/s40471-016-0083-7
130. Weissberger GH, Gollan TH, Bondi MW, Nation DA, Hansen LA, Galasko D, et al. Neuropsychological deficit profiles, vascular risk factors, and neuropathological findings in Hispanic older adults with autopsy-confirmed Alzheimer's disease. J Alzheimers Dis. (2019) 67:291–302. doi: 10.3233/JAD-180351
131. Luchsinger JA, Tang MX, Stern Y, Shea S, Mayeux R. Diabetes mellitus and risk of Alzheimer's disease and dementia with stroke in a multiethnic cohort. Am J Epidemiol. (2001) 154:635–41. doi: 10.1093/aje/154.7.635
132. Qian J, Wolters FJ, Beiser A, Haan M, Ikram MA, Karlawish J, et al. APOE-related risk of mild cognitive impairment and dementia for prevention trials: an analysis of four cohorts. PLoS Med. (2017) 14:e1002254. doi: 10.1371/journal.pmed.1002254
133. Skrepnek GH, Mills JL Sr, Armstrong DG. A diabetic emergency one million feet long: disparities and burdens of illness among diabetic foot ulcer cases within emergency departments in the United States, 2006-2010. PLoS ONE. (2015) 10:e0134914. doi: 10.1371/journal.pone.0134914
134. Tan TW, Shih CD, Concha-Moore KC, Diri MM, Hu B, Marrero D, et al. Disparities in outcomes of patients admitted with diabetic foot infections. PLoS ONE. (2019) 14:e0211481. doi: 10.1371/journal.pone.0211481
135. Tseng CL, Soroka O, Pogach LM. An expanded prevention quality diabetes composite: quantifying the burden of preventable hospitalizations for older adults with diabetes. J Diabetes Complicat. (2018) 32:458–64. doi: 10.1016/j.jdiacomp.2018.01.013
136. Rodriguez-Gutierrez R, Herrin J, Lipska KJ, Montori VM, Shah ND, McCoy RG. Racial and ethnic differences in 30-day hospital readmissions among US adults with diabetes. JAMA Netw Open. (2019) 2:e1913249. doi: 10.1001/jamanetworkopen.2019.13249
137. Alegre-Díaz J, Herrington W, López-Cervantes M, Gnatiuc L, Ramirez R, Hill M, et al. Diabetes and cause-specific mortality in Mexico city. N Engl J Med. (2016) 375:1961–71. doi: 10.1056/NEJMoa1605368
138. Colón-Ramos U, Rodríguez-Ayuso I, Gebrekristos HT, Roess A, Pérez CM, Simonsen L. Transnational mortality comparisons between archipelago and mainland Puerto Ricans. J Immigr Minor Health. (2017) 19:1009–17. doi: 10.1007/s10903-016-0448-5
139. McDonald JA, Paulozzi LJ. Parsing the paradox: Hispanic mortality in the us by detailed cause of death. J Immigr Minor Health. (2019) 21:237–45. doi: 10.1007/s10903-018-0737-2
140. Ogilvie RP, Patel SA, Narayan KMV, Mehta NK. Are the US territories lagging behind in diabetes care practices? Prim Care Diabetes. (2018) 12:432–7. doi: 10.1016/j.pcd.2018.04.005
141. Lundeen EA, Wittenborn J, Benoit SR, Saaddine J. Disparities in receipt of eye exams among medicare part B fee-for-service beneficiaries with diabetes - United States, 2017. Morb Mortal Wkly Rep. (2019) 68:1020–3. doi: 10.15585/mmwr.mm6845a3
142. Turner BJ, Wang CP, Melhado TV, Bobadilla R, Jain MK, Singal AG. Significant increase in risk of fibrosis or cirrhosis at time of HCV diagnosis for Hispanics with diabetes and obesity compared with other ethnic groups. Clin Gastroenterol Hepatol. (2019) 17:1356–63. doi: 10.1016/j.cgh.2018.11.059
143. Kim D, Li AA, Perumpail RB, Cholankeril G, Gonzalez SA, Kim W, et al. Disparate trends in mortality of etiology-specific chronic liver diseases among Hispanic subpopulations. Clin Gastroenterol Hepatol. (2019) 17:1607–15.e2. doi: 10.1016/j.cgh.2018.10.045
144. Kanwal F, Kramer JR, Mapakshi S, Natarajan Y, Chayanupatkul M, Richardson PA, et al. Risk of hepatocellular cancer in patients with non-alcoholic fatty liver disease. Gastroenterology. (2018) 155:1828–37.e2. doi: 10.1053/j.gastro.2018.08.024
145. Miquel JF, Covarrubias C, Villaroel L, Mingrone G, Greco AV, Puglielli L, et al. Genetic epidemiology of cholesterol cholelithiasis among Chilean Hispanics, Amerindians, and Maoris. Gastroenterology. (1998) 115:937–46. doi: 10.1016/S0016-5085(98)70266-5
146. Boland LL, Folsom AR, Rosamond WD. Hyperinsulinemia, dyslipidemia, and obesity as risk factors for hospitalized gallbladder disease. A prospective study. Ann Epidemiol. (2002) 12:131–40. doi: 10.1016/S1047-2797(01)00260-5
147. Liew PL, Lee WJ, Wang W, Lee YC, Chen WY, Fang CL, et al. Fatty liver disease: predictors of nonalcoholic steatohepatitis and gallbladder disease in morbid obesity. Obes Surg. (2008) 18:847–53. doi: 10.1007/s11695-007-9355-0
148. Chavez-Tapia NC, Kinney-Novelo IM, Sifuentes-Renteria SE, Torres-Zavala M, Castro-Gastelum G, Sanchez-Lara K, et al. Association between cholecystectomy for gallstone disease and risk factors for cardiovascular disease. Ann Hepatol. (2012) 11:85–9. doi: 10.1016/S1665-2681(19)31490-5
149. Everhart JE, Yeh F, Lee ET, Hill MC, Fabsitz R, Howard BV, et al. Prevalence of gallbladder disease in American Indian populations: findings from the strong heart study. Hepatology. (2002) 35:1507–12. doi: 10.1053/jhep.2002.33336
150. Stinton LM, Myers RP, Shaffer EA. Epidemiology of gallstones. Gastroenterol Clin North Am. (2010) 39:157–69, vii. doi: 10.1016/j.gtc.2010.02.003
151. Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut Liver. (2012) 6:172–87. doi: 10.5009/gnl.2012.6.2.172
152. Shor E, Roelfs D, Vang ZM. The “Hispanic mortality paradox” revisited: meta-analysis and meta-regression of life-course differentials in Latin American and Caribbean immigrants' mortality. Soc Sci Med. (2017) 186:20–33. doi: 10.1016/j.socscimed.2017.05.049
153. Velasco-Mondragon E, Jimenez A, Palladino-Davis AG, Davis D, Escamilla-Cejudo JA. Hispanic health in the USA: a scoping review of the literature. Public Health Rev. (2016) 37:31. doi: 10.1186/s40985-016-0043-2
154. Bacchetti P. Current sample size conventions: flaws, harms, and alternatives. BMC Med. (2010) 8:17. doi: 10.1186/1741-7015-8-17
155. Delgado JL, Estrada L. Improving data collection strategies. Public Health Rep. (1993) 108:540–5.
156. Novello AC, Soto-Torres LE. One voice, one vision–uniting to improve Hispanic-Latino health. Public Health Rep. (1993) 108:529–33.
157. Brooks J. HHS' Hispanic Agenda for Action: Closing the Gap, Hispanic Agenda for Action. US Department of Health and Human Services OoMHRC (1998). Available online at: https://www.minorityhealth.hhs.gov/assets/pdf/checked/HHS'%20Hispanic%Agenda%for%Action.pdf (accessed May 28, 2020).
158. Aviles-Santa ML, Heintzman J, Lindberg NM, Guerrero-Preston R, Ramos K, Abraido-Lanza AL, et al. Personalized medicine and Hispanic health: improving health outcomes and reducing health disparities - a National heart, lung, and blood institute workshop report. BMC Proc. (2017) 11(Suppl. 11):11. doi: 10.1186/s12919-017-0079-4
159. Ennis SR, Rios-Vargas M, Albert NG. The Hispanic Population 2010 Census Briefs US Department of Commerce, Economics and Statistics Administration, US. Census Bureau. (2011) C2010BR-04.
160. Krogstad JM. Key Facts About How the US Hispanic Population is Changing. Fact Tank, Pew Research Center (2016). Available online at: https://www.pewresearch.org/fact-tank/2016/09/08/key-facts-about-how-the-u-s-hispanic-population-is-changing/ (accessed May 28, 2020).
161. Forno E, Gogna M, Cepeda A, Yanez A, Sole D, Cooper P, et al. Asthma in Latin America. Thorax. (2015) 70:898–905. doi: 10.1136/thoraxjnl-2015-207199
162. Custodio N, Wheelock A, Thumala D, Slachevsky A. Dementia in Latin America: epidemiological evidence and implications for public policy. Front Aging Neurosci. (2017) 9:221. doi: 10.3389/fnagi.2017.00221
163. Kaselitz E, Rana GK, Heisler M. Public policies and interventions for diabetes in Latin America: a scoping review. Curr Diab Rep. (2017) 17:65. doi: 10.1007/s11892-017-0888-x
164. National Institutes of Health. NIH Policy and Guidelines on the Inclusion of Women and Minorities as Subjects in Clinical Research. Available online at: https://grants.nih.gov/grants/funding/women_min/guidelines.htm) (accessed May 28, 2020).
165. Corbett D. Preparing the NIH protection of human subjects section and an overview of the NIH's new policies. In: OER Regional Seminars. (2018). Available online at: https://grants.nih.gov/sites/default/files/OER%20Regionals%2010-2018%20Human.Subject.Reviews-Preparing-NIH-HSSection-Policy-Overview%20508c%20version%20Rev.pdf (accessed May 28, 2020).
166. Corbett D. Inclusion of women, minorities, and individuals across the lifespan. In: Presentation at the 47th Meeting of the Advisory Committee on Research on Women's Health. Bethesda, MD: Spring (2019). Available online at: https://orwh.od.nih.gov/sites/orwh/files/docs/ACRWH-CorbettInclusion-Spring2019-508C.pdf (accessed May 28, 2020).
168. Fortin JM, Currie DJ. Big Science vs little science: how scientific impact scales with funding. PLoS One. (2013) 8:e65263. doi: 10.1371/journal.pone.0065263
169. Lauer MS. Personal reflections on big science, small science, or the right mix. Circ Res. (2014) 114:1080–2. doi: 10.1161/CIRCRESAHA.114.303627
Keywords: Hispanics, Latinos, diabetes, cancer, asthma, obesity, dementia, liver disease
Citation: Avilés-Santa ML, Hsu L, Lam TK, Arteaga SS, Artiles L, Coady S, Cooper LS, Curry J, Desvigne-Nickens P, Nicastro HL and Rosario A (2020) Funding of Hispanic/Latino Health-Related Research by the National Institutes of Health: An Analysis of the Portfolio of Research Program Grants on Six Health Topic Areas. Front. Public Health 8:330. doi: 10.3389/fpubh.2020.00330
Received: 03 March 2020; Accepted: 15 June 2020;
Published: 28 August 2020.
Edited by:
Melody Goodman, New York University, United StatesReviewed by:
Stacie Craft DeFreitas, University of Houston–Downtown, United StatesCopyright © 2020 Avilés-Santa, Hsu, Lam, Arteaga, Artiles, Coady, Cooper, Curry, Desvigne-Nickens, Nicastro and Rosario. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: M. Larissa Avilés-Santa, YXZpbGVzc2FudGFsQG5paC5nb3Y=
†Present address: S. Sonia Arteaga, National Institutes of Health, Bethesda, MD, United States
Holly L. Nicastro, Office of Nutrition Research at the National Institute of Diabetes, and Digestive and Kidney Diseases, Bethesda, MD, United States
Adelaida Rosario, The U.S. Department of Health and Human Services, Rockville, MD, United States
‡These authors are listed in alphabetical order
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.