 Aarón Salinas-Rodríguez1
Aarón Salinas-Rodríguez1 Betty Manrique-Espinoza1
Betty Manrique-Espinoza1 Irina Torres Mussot2
Irina Torres Mussot2 Julio Cesar Montañez-Hernández2*
Julio Cesar Montañez-Hernández2*- 1Center for Surveys and Evaluation, National Institute of Public Health, Cuernavaca, Mexico
- 2Center for Health Systems Research, National Institute of Public Health, Cuernavaca, Mexico
Background: Dependence is a significant health-related condition for older adults (OA) and implies that self-care is transferred to other people, the community or institutions. Recent studies have analyzed the relationship between out-of-pocket (OOP) healthcare expenditures and dependence. Nonetheless, these studies were not specifically designed to estimate the economic impact of dependence. Our aim was to estimate the total adjusted annual OOP healthcare expenditures in dependent older adults compared to independent ones. Additionally, we explore the potential combined effect of basic activities of daily living (ADL) and instrumental activities of daily living (IADL) dependence on OOP healthcare expenditures.
Methods: Data comes from the cross-sectional study “Economic impact of physical dependence in older adults and the burden of informal care” conducted in 2018 with a sample of 735 community-dwelling older Mexican adults ages 60 and older. We used direct (medical and non-medical) and indirect costs to estimate the OOP healthcare expenditures associated with dependence. We applied the Katz scale to assess dependence in ADL and the Lawton scale to assess dependence in IADL. Two-Part regression models were used to analyze the relationship between dependence and OOP health expenditures.
Results: Presence of ADL dependence represented a higher level of expenditure, 107% compared to non-dependent OA (β = 1.07, CI95%: 0.43–1.71), and 97% for IADL dependence (β = 0.97, CI95%: 0.49–1.45). The combined effect of ADL and IADL dependence (132%) was greater (β = 1.32, CI95%: 0.74–1.90) than the effect of ADL or IADL dependence alone. In monetary terms, OA with ADL dependence had a total annualized mean OOP healthcare expenditure of $31,865 (Mexican pesos), OA with IADL $26,912, and combined ADL and IADL $39,520.
Conclusions: ADL and IADL dependence are associated with the total annualized OOP healthcare expenditures. This association is even higher when both conditions are present together. These findings highlight the economic implications of the dependence for individuals, their families, and the health system. Given that current evidence on effective interventions to prevent dependence in OA is insufficient, future studies should be conducted to estimate their costs and determine what interventions work, as well as their effectiveness and cost-effectiveness in different sub-groups of the population, and how these might be appropriately implemented.
Introduction
Dependence is a significant health-related condition for older adults (OA), and its presence implies that self-care is transferred to other people, the community or institutions (1). The World Health Organization (WHO) defines dependence as an event that occurs when the functional or intrinsic capacity has decreased to a point where the person is no longer able to carry out the basic tasks of daily life on their own (2). Dependence in OA is a complex and multidimensional concept that goes beyond a single physical component, encompassing a psychological, and socioeconomic dimension (3). Even so, the dimension of dependence that has been most analyzed in gerontological literature is the physical or functional dependence, and particularly that focused on the functional loss of bodily or sensory abilities (4).
The prevalence of dependence for OA populations in high-income countries ranges from 15 to 17%, while in low and middle-income countries it ranges from 3 to 16%. In Mexico, by 2012, 21.7% of OA had basic activities of daily living (ADL) limitations, and 5.1% were dependents (5).
Dependence has a variety of consequences at different levels. At an individual level, dependence can generate feelings of depression, low self-esteem, and hopelessness (6). At the level of family, it can generate a cycle of impoverishment and reallocation of care roles (7), while at the societal level, dependence can increase demand for health and care services (8). This increase demand for health and care services can also increase the costs associated with healthcare of dependent older people.
The aging process in Mexico (similar to other low- and middle-income countries) has occurred amid a fragile economy marked by high levels of poverty and limited access to health services and resources (9). In that context dependency in old age is one of most critical challenges facing by the social health protection system. Given this scenario, the Mexican Health System, a mixture of public-private schemes, has sought to achieve universal access to health, as well as universal coverage of health services, through three public insurance schemes mainly: The Mexican Institute of Social Security (IMSS by its Spanish acronym), the Institute of Security and Social Services of State Workers [ISSSTE (9)], and by the Seguro Popular, today converted into the Institute of Health for Well-being [INSABI (9)]. Despite this, none of these schemes specifically covers the potential health-related costs of physically dependent OA.
In 2012, 13% of older adults (60 years or older) did not have health insurance and 53.5% did not have an economic pension (10). However, since 2009 Mexico has a non-contributory pension program (formerly known as 70 y más−70 and over, and now as the Programa para el Bienestar de los Adultos Mayores-Program for the Welfare of Older Adults) which consists of the bimonthly payment of 2,750 Mexican pesos (115 US dollars approx.), and is intended to be universal to all individuals 68 years of age or older (11, 12).
Recent studies have analyzed the relationship between out-of-pocket (OOP) healthcare expenditures and different health outcomes related to the functional capacity of the OA, namely frailty (13), multimorbidity (14), and disability (15). Some other studies have also examined the relationship between dependence and OOP healthcare expenditures (16–19). Yet, other studies have treated functional dependence as a covariate, rather than the main exposure of interest (20–22). Despite this evidence, some gaps remain, because findings on dependence and healthcare costs have been produced from studies that were not explicitly designed to estimate the economic impact of dependence in older adults.
Also, the combined effects of basic activities of daily living (ADL) and instrumental activities of daily living (IADL) dependence on OOP healthcare expenditures has not been explored. We have designed a study that expressly seeks to better understand the economic implications of dependence in the elderly. Our main objective was to estimate the total adjusted annual OOP healthcare expenditures in dependent older adults compared to independent ones. Additionally, we explored a potential combined effect of ADL and IADL dependence on OOP healthcare expenditures.
Materials and Methods
Study Design and Sample
Data comes from the cross-sectional study “Economic impact of physical dependence in older adults and the burden of informal care” conducted in 2018 with a sample of community-dwelling older Mexican adults age 60 and older (23). According to a previous study in which the costs associated with frailty among older Mexican adults were estimated (13), a sample size of 735 OA would have sufficient power to detect significant differences in healthcare costs when comparing individuals with and without dependence based on a significance level of 5%, power of 90%, and one-sided tests. OA in this study were residents of two urban and three rural communities in the Mexican state of Estado de México, located at the central part of Mexico. We defined the analytical sample according to the following criteria: we included all older adults aged ≥60 and were excluded those with hearing or speech impairment. Also, a key informant (proxy) was considered if the OA reported severe memory problems (present if the answer was yes for the question: Have you had difficulties with your memory that are a problem for you?). In that case, the caregiver provided the information (9.7% of the sample). The final analytical sample was comprised of 735 older adults.
We administered an extensive questionnaire to study participants to collect data on the expenditures related to medications, consultations, hospitalizations, laboratory studies, devices, prostheses, and loss of labor productivity. Direct (medical and non-medical) and indirect costs were both used to estimate the economic burden of dependence.
Measures
Out-of-pocket Healthcare Expenditures
We calculated total healthcare expenditures based on the estimation of cumulative costs found through the questionnaires. All costs were annualized for 2018. We grouped data in direct and indirect costs as described below.
Direct Costs
Medical and non-medical expenditures were estimated using a micro-costing analysis, which allows monetary valuing of the individual use of health resources and services by study participants. Medical costs included medical consultations, specialist consultations, medications (including vitamins), laboratory tests, and hospitalization. Non-medical costs included nursing services, devices (visual, hearing, orthopedic), prostheses, and other costs (personal hygiene, healing material, traditional medicine).
Indirect Costs
We operationalized the indirect costs considering the monthly loss of productivity for the OA and his/her carer/relative as follows:
a) Loss of labor productivity (OA). We determined the economic loss of labor productivity in working OA by asking about the number of days of work they had missed due to health-related reasons.
b) Loss of labor productivity in the household (caregiver or relative). We quantified the loss of labor productivity at the household level by asking relatives how much they thought they had lost on income due to caring for the OA.
Dependence
We applied two widely known instruments to evaluate the functional capacity of the OA: the Katz and Lawton scales. The Katz scale (24) assess difficulties in ADL, which include bathing, dressing, using the toilet, incontinence, and feeding. The Lawton scale (25) assess difficulties in IADL, including using the phone, going shopping, managing drugs and money, and using public or private transportation.
Based on the information about ADL and IADL, an OA was considered dependent if: (1) they were unable to perform at least one of the ADL or IADL, (2) he/she had a primary caregiver who provided assistance for ADL or IADL, and accompanied him/her to health facilities. Using these criteria, we generated two variables that define either ADL or IADL dependence combining the difficulties in performing ADL or IADL and the presence of a caregiver. These were operationalized as binary variables, where 0 = independent, and 1 = dependent.
Covariates
We included factors associated with healthcare expenditures in the literature (26, 27) as potential covariates and categorized them as follows:
Socio-Demographic Characteristics
Sex (female = 1), age, health insurance (yes = 1), retirement pension (yes = 1), schooling (years of formal instruction), paid job (yes = 1), marital status (married/cohabited = 1), area of residence (urban = 1 vs. rural = 0).
Health
We included 19 indicator variables for each of the following conditions that were obtained from participants' self-report (1 = present, 0 = absent): hypertension, diabetes, hypercholesterolemia, heart disease (angina pectoris, heart failure), embolism, stroke or cerebral thrombosis, arthritis or rheumatism, bronchitis, or pulmonary emphysema, osteoporosis, kidney chronic disease, tuberculosis, cataracts (one or both eyes), urinary incontinence, prostate disease (men only), and cancer (skin/melanoma, cervix, breast, prostate, stomach, leukemia / blood). With this information, we generated a count variable to express the total number of chronic conditions in each participant. This variable was included in our regression models as a proxy for the general health status.
Use of Health Services
We measured this variable using two indicators: number of outpatient visits in the last 6 months, and the number of hospitalizations in the last 12 months.
Socioeconomic Status (SES)
For SES measurement, we created an asset index following a standard approach proposed by the WHO to estimate the permanent income of the household through the ownership of goods and some characteristics of the housing (28–30). In particular, we used nine dichotomous variables (yes/no) that evaluated possession of household assets. The asset index was created using a polychoric correlation matrix through the application of principal component analysis (PCA). The first component explained 44% of the variation in the data. The index generated by PCA is continuous, with higher values denoting higher household SES.
Statistical Analysis
Variables were described using means (standard deviations) or proportions, as appropriate. In bivariate analysis, the following statistical procedures were used according to the characteristics of each variable: Chi-squared test for categorical data and Mann-Whitney test for continuous data. Exploratory analyses, including graphs (histograms and scatter plots), were also used to determine the probability distributions of the outcome variable. At this stage, we observed a considerable percentage of OA that did not show out-of-pocket expenses (30%), and the distribution of expenditure showed a right-skewed distribution, so in the multivariate analysis we used a two-part regression model (14, 31).
In the Two-Part model, the outcome variable is analyzed in two phases. In the first part, a regression for dichotomous variables (logit or probit) is used to estimate the probability of incurring OOP health expenditures. In our case, we coded the dependent variable (OOP health expenditures) as a binary indicator, where one equaled older adult that incurred OOP health expenditures and zero equaled those that did not. In the second part, to reduce the effect of skewness of healthcare costs, a linear regression model on the natural logarithm of this variable is applied to estimate the average expenditures among individuals that incurred health expenditures. In general, it is recommended the use of the natural logarithm of healthcare costs to reduce the effects of the skewed nature of this variable. Results are interpreted (β) as semi-elasticities (i.e., as the percentage increase observed in the response variable for one increment in the independent variable). Finally, total expenditures for each individual are estimated by multiplying the probability by the average results obtained through the first and second parts of the model, using Duan's smearing retransformation to obtain fitted values (32).
We further conducted several sensitivity analyses to check the robustness of our results. First, we examined the combined effect of ADL and IADL dependence on OOP health expenditures. The combined effect of ADL and IADL dependence was analyzed by creating a new dichotomous variable, where 1 reflected the simultaneous presence of ADL & IADL, and 0 the presence of neither. Second, instead of modeling mean of healthcare expenditures, we modeled the median of OOP healthcare expenditures using a quantile regression model (33, 34).
All regression models were adjusted for variables described in the Covariates section. Statistical analyses were performed using STATA version 15.1 software (StataCorp. 2015. College Station, TX.). Ninety-five percent confidence intervals and p-values were reported. Differences were considered statistically significant if p < 0.05.
Results
The following sociodemographic and health characteristics were observed in our sample. Mean age of participants was 71.1 years (SD = 8.4 years). 57.8% were female, 56.0% married/cohabited, and 31% current workers. Mean of years of formal education was 4.2 (SD = 4.4). Regarding health characteristics, 63.4% reported at least one chronic condition, and 32.1% had multimorbidity, defined as the presence of two or more chronic diseases. Prevalence of ADL and IADL dependence was 8.6 and 15.0%, respectively.
Table 1 displays the study sample characteristics according to the presence of ADL and IADL dependence. Overall, dependent OA were mostly female (p < 0.01), older (p < 0.01), and single or widowed (p < 0.01). They worked less (p < 0.01) and had fewer years of schooling (p < 0.01). They had more visits to a physician (p < 0.01), more hospital overnight stays (p < 0.01), and a greater number of chronic diseases (p < 0.01). Regarding OOP healthcare expenditures, dependent OA had a greater probability of incurring expenses than non-dependent OAs (p < 0.01) and also a higher annual mean expenditure (p < 0.01). This general profile was similar for ADL and IADL dependent OA. Finally, OA with ADL dependence had an unadjusted total annualized mean OOP healthcare expenditure of $29,272 (Mexican pesos), while the amount in OAs with IADL was $18,196.
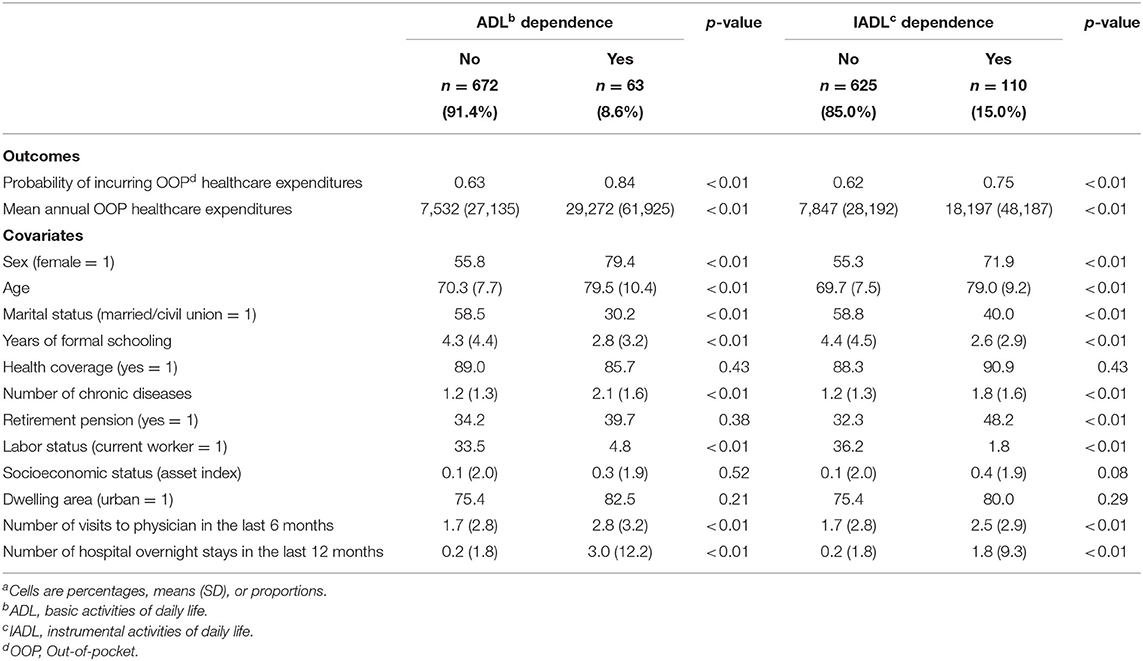
Table 1. Health and sociodemographic characteristics of older adults according to the status of ADL and IADL dependencea.
The results of OOP healthcare expenditures for specific items are shown in Tables 2, 3. For ADL dependence, expenditures from medications, nursing services, and medical consultations, mostly contributed to total OOP healthcare expenditures (Table 2). As for IADL dependence, medications and nursing services were the highest contributors (Table 3).
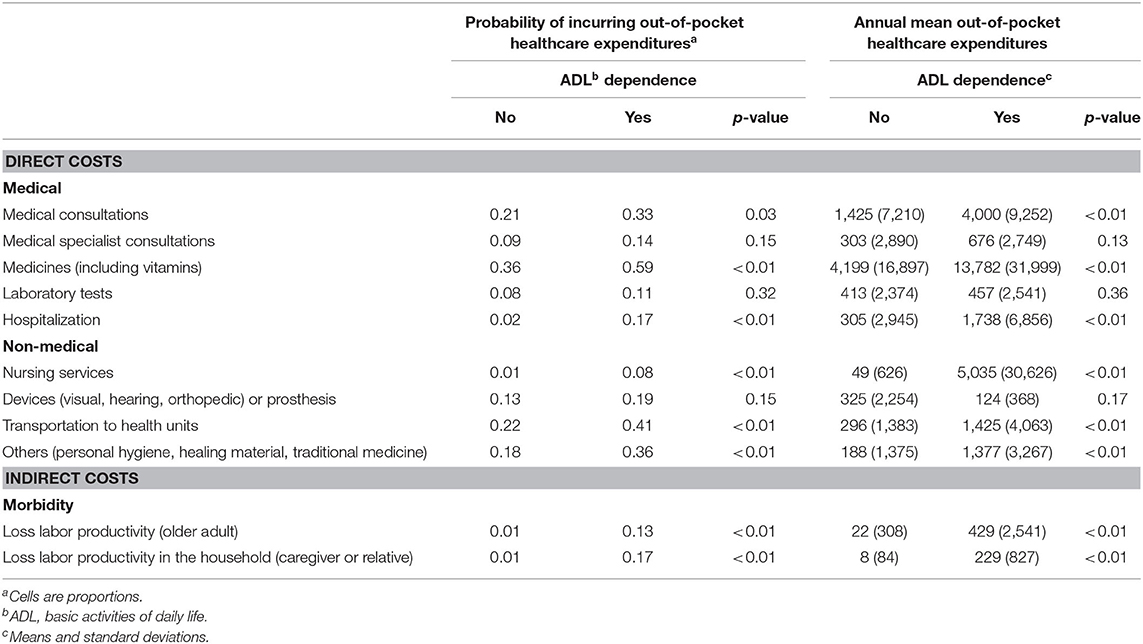
Table 2. Out-of-pocket health expenditures by specific cost items according to the status of ADL dependence.
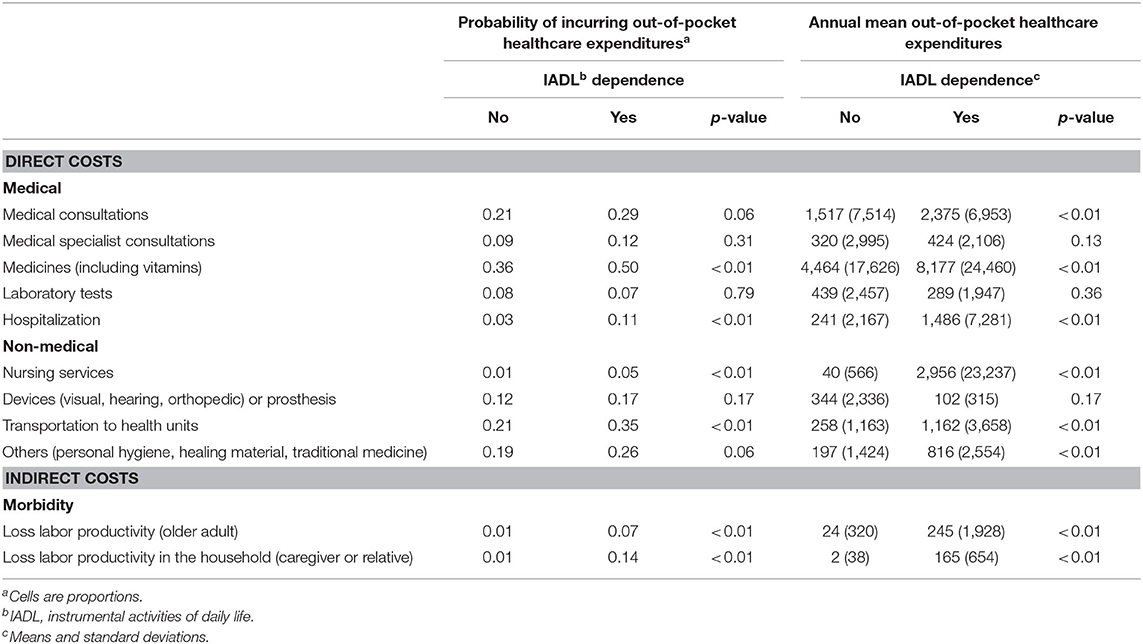
Table 3. Out-of-pocket health expenditures by specific cost items according to the status of IADL dependence.
The results of the adjusted two-part regression models are presented in Table 4. Neither ADL dependence (OR = 1.86, CI95%: 0.85–4.11) nor IADL dependence (OR = 1.27, CI95%: 0.72–2.25) was found to be associated with the probability of incurring total annual OOP expenditures. We also did not observe a significant association for the combined presence of ADL and IADL dependence (OR = 1.73, CI95%: 0.78–3.81).
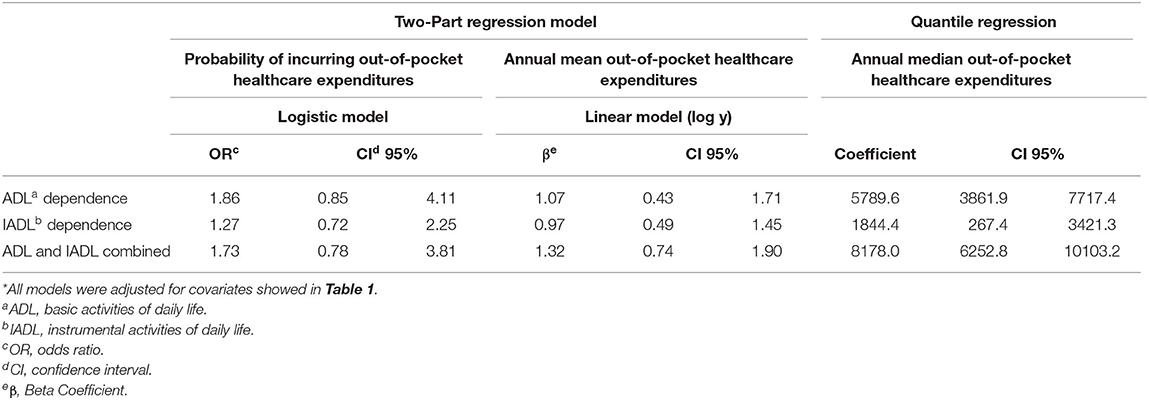
Table 4. Results of two-part and quantile regression models*.
The presence of ADL dependence was associated with an 107% higher mean OOP health expenditure compared to non-dependent OA (β = 1.07, CI95%: 0.43–1.71). This was 97% for IADL dependence (β = 0.97, CI95%: 0.49–1.45). The combined effect of ADL and IADL dependence (132%) was greater (β = 1.32, CI95%: 0.74–1.90) than the isolated presence of ADL or IADL dependence.
With regard to the median of OOP healthcare expenditure, we found that ADL dependent individuals had a median annual expenditure $5,798 higher than non-dependent individuals (Mexican pesos), while the IADL dependent OA had an expenditure that was $1,844 higher than their non-dependent counterparts. This number was greater for the combined ADL and IADL dependence ($8,178 Mexican pesos) (Table 4).
Finally, Figures 1, 2 show the estimated OOP healthcare expenditures according to the presence of dependence in OA. Figure 1 displays the data for mean annual expenditure, while Figure 2 displays median expenditure. The average expenditure was 4.1, 3.3, and 2.8 times larger for the ADL and IADL, ADL-only, and IADL-only groups, in relation to the group without dependence. Meanwhile, the same data for median expenditure was 5.4, 4.1, and 1.9, respectively.
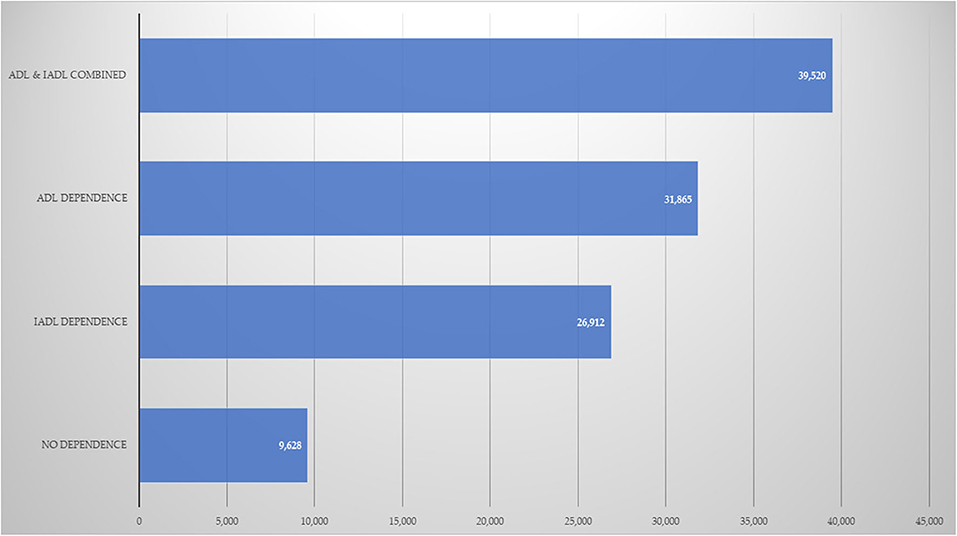
Figure 1. Annual mean OOP healthcare expenditures (Mexican pesos). ADL, basic activities of daily life; IADL, instrumental activities of daily life.
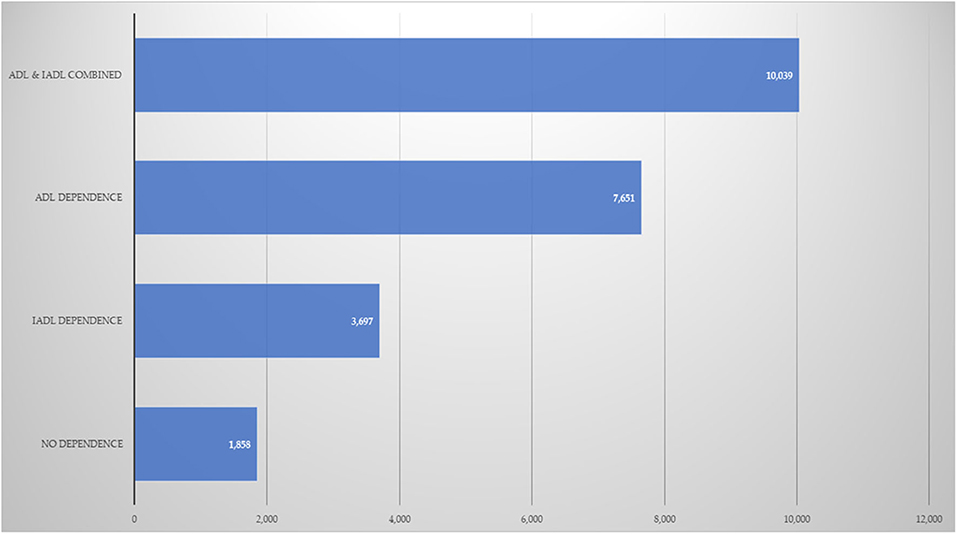
Figure 2. Annual median OOP healthcare expenditures (Mexican pesos). ADL, basic activities of daily life; IADL, instrumental activities of daily life.
Discussion
Our findings corroborate that there is a significant association between dependence in OA and OOP healthcare expenditures. Based on a sample of 735 community-dwelling older Mexican adults, we observed that the presence of ADL or IADL dependence as well as their combined presence was associated with a significant increase in the total annualized OOP healthcare expenditures.
Consistent with previous studies, we found a significant association between dependence in OA and healthcare costs. One study with European older adults age 65+ found that ADL and IADL dependence were associated with higher societal costs (including primary, secondary, social, home, and informal care). Although, this study measured ADL and IADL dependence on a continuous scale and was focused on societal costs rather than OOP expenditures (17). Even so, we similarly found that dependent OA tend to have higher healthcare cost than their independent counterparts. Another study among US adults found that ADL and IADL difficulties were associated with total annual cost of care (TACC). In this study, however, ordinal variables were used to measure ADL and IADL difficulties (0, 1–2, and 3 or more difficulties), and results showed that having three or more difficulties was associated with a higher TACC (18). In our study, we observed significant associations from the presence of a single difficulty. Two possible explanations could be advanced for this difference. First, we just include OA while they included adults age 18 or more, so our study sample could have worse health and functional conditions that would make it possible to observe significant associations with minor levels of ADL or IADL difficulties. Second, our definition of dependence includes not just difficulties in ADL or IADL, but also the need for someone to help in the execution of these activities. Finally, a study conducted with older US adults, including beneficiaries of Medicare and participants of the Health and Retirement Study, reported that compared to those with no ADL impairment, the most severely impaired (two or more ADL difficulties) had a 33% higher cost (19). It is interesting to note that the sample considered for this study were OA who were admitted to a hospital at least once in a previous period of 10 years, while our sample was comprised of community-dwelling individuals who were not hospitalized or institutionalized. Despite this difference, our results are consistent regarding the association between ADL dependence and OOP healthcare costs.
Despite the similarity in the described results, we should note that none of the studies -to the best of our knowledge- on the economic impact of dependency have used the two-part model approach. This fact has two important implications. On the one hand, the results are not strictly comparable, given that those studies conceive of healthcare spending as a single-stage process (i.e., the estimation of the total amount disbursed). Meanwhile, the two-part model recognizes the potential presence of two phases: (a) to incur or not in healthcare expenditures (i.e., the probability of incurring in spending), and (b) given the incidence of healthcare expenses, what was the amount disbursed? (i.e., the estimation of the average expenses).
On the other hand, we found that neither ADL nor IADL was associated with the probability of incurring OOP healthcare expenditures (even the two conditions combined). Although a similar result has not been reported in the literature, one study found that the severity of disability in older adults, assessed through the WHO Disability Assessment Schedule -WHODAS 2.0, was associated with a higher probability of healthcare expenses (14). Given that disability reported in that study included six domains (cognition, mobility, self-care, getting along, life activities, and social participation) that encompassing more characteristics than a single component of physical limitations, then the isolated presence of physical dependency could not be enough to increase the probability of having healthcare expenses. However, future studies are needed to confirm or dismiss this hypothesis.
The results of our study have several implications. First, the high prevalence of dependence among OA calls for concerted efforts of healthcare professionals, clinical researchers, and policy-makers to design effective interventions that prevent or ameliorate the adverse effects of dependence in advanced ages. For example, in Mexico the creation of a National Care System (Sistema Nacional de Cuidados, SNC by its Spanish acronym) is currently being considered. The objective would be to provide public services that are accessible, pertinent, of quality, and sufficient to guarantee the right of all people to be cared for, and also the rights of caregivers (35). It is expected to be financed with public funds, but also through the families' corresponsability. In particular, the SNC proposes that a catalog of care services be generated that includes financial benefits, home care assistance and care support centers. It would also include support for unpaid carers through a cash payment (for hiring a caregiver). Second, the health systems should be prepared for the increased demand on the use of health services by dependent OA, given that the OOP healthcare expenditures of these individuals will grow exponentially in the next few years. Third, gerontological research on the functional status of the older adults should highlight the joint assessment of ADL and IADL dependence for the estimation of healthcare expenditures, because their economic impact might be more significant than either on its own.
Our study has some strengths. To the best of our knowledge, our study is the first designed to deliberately estimate the economic impact of ADL and IADL dependence. It is also the first attempt to analyze the combined effects of ADL and IADL dependence on OOP healthcare expenditures. Nevertheless, some limitations must be considered also. First, recall and survivor bias can be limitations for epidemiological studies with older adult participants. It could be, for example, that older adults with chronic conditions tend to overestimate their healthcare expenditures in comparison with healthiest older adults. Second, healthcare costs variables are self-reported. This may have led to overestimation or underestimation of true OOP healthcare expenditures. In spite of this, consistent associations between dependence and healthcare costs have been reported previously in the literature (16, 19). Third, the results from the current study came from a cross-sectional study, and thus a causal pathway between dependence and OOP healthcare expenditures cannot be determined. And fourth, our measurement of dependency has been expressed dichotomously, which implies that severity levels of dependency are not properly captured, which could restrict the generalization of our results to even more vulnerable populations, like OA with a greater number of limitations in ADL or IADL.
Conclusion
Our study shows that ADL and IADL dependence are associated with total annualized OOP healthcare expenditures. This association is even higher when both conditions are present together. These findings tried to highlight the economic implications of dependence on individuals, their families, and the health system. Finally, given that the current evidence is insufficient to conclude which strategies to prevent dependence in OA are more effective, future studies should be conducted to estimate the costs and effectiveness of different interventions to address dependence in OA.
Data Availability Statement
The datasets analyzed during the current study are freely available in the figshare repository [doi: 10.6084/m9.figshare.9978599].
Ethics Statement
The ethics and Research Committees of the National Institute of Public Health in Mexico approved the study economic impact of physical dependence in older adults and the burden of informal care (No. 1203-2018). All participants were provided with a detailed explanation of study procedures and signed an informed consent letter.
Author Contributions
AS-R, BM-E, and JM-H conceived and designed the study. AS-R and JM-H carried out the analysis. AS-R, IT, and JM-H drafted the manuscript. All authors reviewed, edited, contributed to rewriting of the manuscript, and granted final approval to the version submitted for publication.
Funding
This study was funded by the National Council of Science and Technology of Mexico (CONACYT; Grant SALUD-2018-S0008-2017-2-290487). This institution has no further role in the study design, collection, analysis and interpretation of data, drawing up of the manuscript, or the decision to submit the paper for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. Facts about ageing. Geneva: WHO (2014). Available online at: http://www.who.int/ageing/about/facts/en/ (accessed October 17, 2019).
2. World Health Organization. World Report on Ageing and Health. Luxemburg (2015). Available online at: https://apps.who.int/iris/bitstream/handle/10665/186463/9789240694811_eng.pdf?sequence=1 (accessed October 17, 2019).
3. Baltes M. The Many Faces of Dependency in Old Age. New York, NY: Cambridge University Press (1996).
4. Gutiérrez-Robledo L, Téllez-Rojo M, Manrique-Espinoza B, Acosta Castillo I, López Ortega M, Salinas-Rodríguez A, et al. Disability and dependency in Mexican older adults: a healthy course for a full old age (Discapacidad y dependencia en adultos mayores mexicanos: un curso sano para una vejez plena). México Instituto Nacional de Salud Pública (2013). Available online at: http://ensanut.insp.mx/doctos/analiticos/DiscapacidAdultMayor.pdf (accessed October 17, 2019).
5. Gómez-Dantés H, García-Peña M, Sánchez-García S, Rosas-Carrasco O, Campuzano-Rincón J, Lozano R, et al. Scenarios of dependency in Mexico (Escenarios de la dependencia en México). In: Gutiérrez-Robledo LM, García-Peña MC, Jiménez-Bolón JE, editores. Aging and Dependency. Realities and Forecast for the Coming Years. (Envejecimiento y Dependencia. Realidades y Previsión Para los Próximos Años. Documento de postura). Academia Nacional de Medicina/ Instituto Nacional de Geriatría (2014). p. 63–89. Available online at: https://www.anmm.org.mx/publicaciones/CAnivANM150/L11-Envejecimiento-y-dependencia.pdf (accessed October 17, 2019).
6. Woo J, Leung J. Multi-morbidity, dependency, and frailty singly or in combination have different impact on health outcomes. Age. (2014) 36:923–31. doi: 10.1007/s11357-013-9590-3
7. Guerchet MM, Guerra M, Huang Y, Lloyd-Sherlock P, Sosa AL, Uwakwe R, et al. A cohort study of the effects of older adult care dependence upon household economic functioning, in Peru, Mexico and China. PLoS ONE. (2018) 13:e0195567. doi: 10.1371/journal.pone.0195567
8. Pacolet J. Social protection of dependent elderly people in Europe (Protección social de personas mayores dependientes en Europa). In: González AA, Moreno FJ, editors. Dependency Treatment in Contemporary European Welfare Regimes (El tratamiento de la dependencia en los regímenes de bienestar europeos contemporáneos). Madrid: Instituto de Mayores y Servicios Sociales (2009). p. 61–94.
9. Salinas-Rodríguez A, Manrique-Espinoza B, De la Cruz-Góngora V, Rivera-Almaraz A. Socioeconomic inequalities in health and nutrition among older adults in Mexico. Salud Publica Mex. (2019) 61:898–906. doi: 10.21149/10556
10. Manrique-Espinoza B, Salinas-Rodríguez A, Moreno-Tamayo KM, Acosta-Castillo I, Sosa-Ortiz AL, Gutiérrez-Robledo LM, et al. Health conditions and functional status of older adults in Mexico. Salud Publica Mex. (2013) 55(Suppl.2):S323–31. doi: 10.21149/spm.v55s2.5131
11. Salinas-Rodríguez A, Torres-Pereda Mdel P, Manrique-Espinoza B, Moreno-Tamayo K, Téllez-Rojo Solís MM. Impact of the non-contributory social pension program 70 y más on older adults' mental well-being. PLoS ONE. (2014) 9:e113085. doi: 10.1371/journal.pone.0113085
12. Salinas-Rodríguez A, Moreno-Tamayo K, Hernández-Serrato M, Enríquez-Rosas MDR, Manrique-Espinoza BS. Multidimensional social support is associated with healthcare utilization among older Mexican adults. Eur J Ageing. (2017) 15:77–85. doi: 10.1007/s10433-017-0428-1
13. Salinas-Rodríguez A, Manrique-Espinoza B, Heredia-Pi I, Rivera-Almaraz A, Ávila-Funes JA. Healthcare costs of frailty: implications for long-term care. J Am Med Dir Assoc. (2019) 20:102–3.e2. doi: 10.1016/j.jamda.2018.09.019
14. Rivera-Almaraz A, Manrique-Espinoza B, Chatterji S, Naidoo N, Kowal P, Salinas-Rodríguez A. Longitudinal associations of multimorbidity, disability and out-of-pocket health expenditures in households with older adults in Mexico: the study on global AGEing and adult health (SAGE). Disabil Health J. (2019) 12:665–72. doi: 10.1016/j.dhjo.2019.03.004
15. Mitra S, Palmer M, Kim H, Mont D, Groce N. Extra costs of living with a disability: a review and agenda for research. Disabil Health J. (2017) 10:475–84. doi: 10.1016/j.dhjo.2017.04.007
16. Brinda EM, Rajkumar AP, Enemark U, Attermann J, Jacob KS. Cost and burden of informal caregiving of dependent older people in a rural Indian community. BMC Health Serv Res. (2014) 14:207. doi: 10.1186/1472-6963-14-207
17. van Lier LI, van der Roest HG, Oosten BS, Garms-Homolová V, Onder G, Finne-Soveri H, et al. Predictors of societal costs of older care-dependent adults living in the community in 11 European countries. Health Serv Insights. (2019) 12:1178632918820947. doi: 10.1177/1178632918820947
18. Johnston KJ, Wen H, Hockenberry JM, Joynt Maddox KE. Association between patient cognitive and functional status and medicare total annual cost of care: implications for value-based payment. JAMA Intern Med. (2018) 178:1489–97. doi: 10.1001/jamainternmed.2018.4143
19. Greysen SR, Stijacic Cenzer I, Boscardin WJ, Covinsky KE. Functional impairment: an unmeasured marker of medicare costs for postacute care of older adults. J Am Geriatr Soc. (2017) 65:1996–2002. doi: 10.1111/jgs.14955
20. Hohls JK, König HH, van den Bussche H, Eisele M, Wiese B, Oey A, et al. Association of anxiety symptoms with health care use and costs in people aged 85 and over. Int J Geriatr Psychiatry. (2019) 34:765–76. doi: 10.1002/gps.5089
21. Ribbink ME, van Seben R, Reichardt LA, Aarden JJ, van der Schaaf M, van der Esch M, et al. Determinants of post-acute care costs in acutely hospitalized older adults: the hospital-adl study. J Am Med Dir Assoc. (2019) 20:1300–6. doi: 10.1016/j.jamda.2019.03.013
22. Lutomski JE, Baars MA, Boter H, Buurman BM, den Elzen WP, Jansen AP, et al. Frailty, disability and multi-morbidity: the relationship with quality of life and healthcare costs in elderly people. Ned Tijdschr Geneeskd. (2014) 158:A7297.
23. Montañez JC, Salinas-Rodríguez A, Manrique-Espinoza B, Heredia-Pi I. Economic Impact of Physical Dependence on Older Adults and Estimation of the Burden Associated With Informal Care (Impacto Económico de la Dependencia Física en Los Adultos Mayores y Estimación de la Carga Asociada a los Cuidados Informales). México: Instituto Nacional de Salud Pública (2017).
24. Katz S, Branch LG, Branson MH, Papsidero JA, Beck JC, Greer DS. Active life expectancy. N Engl J Med. (1983) 309:1218–24. doi: 10.1056/NEJM198311173092005
25. Lawton MP, Brody EM. Assessment of older people: self maintaining and instrumental activities of daily living. Gerontologist. (1969) 9:179–86. doi: 10.1093/geront/9.3_Part_1.179
26. Picco L, Abdin E, Vaingankar JA, Pang S, Shafie S, Sambasivam R, et al. Prevalence and risk factors of caregiver dependence among older adults in a southeast asian population. Ann Acad Med Singapore. (2016) 45:486–94.
27. Connolly D, Garvey J, McKee G. Factors associated with ADL/IADL disability in community dwelling older adults in the Irish longitudinal study on ageing (TILDA). Disabil Rehabil. (2017) 39:809–16. doi: 10.3109/09638288.2016.1161848
28. Booysen F, van der Berg AE, Burger R, von Maltitz M, du Rand G. Using an asset index to assess trends in poverty in seven Sub-Saharan African countries. World Dev. (2008) 36:1113–30. doi: 10.1016/j.worlddev.2007.10.008
29. Moser C. Assets and livelihoods: a framework for asset-based social policy. In: Moser C, Anis D, editors. Assets, Livelihoods, and Social Policy. Washington, DC: The World Bank (2008) 43–81. doi: 10.1596/978-0-8213-6995-1
30. Howe LD, Galobardes B, Matijasevich A, Gordon D, Johnston D, Onwujekwe O, et al. Measuring socio-economic position for epidemiological studies in low- and middle-income countries: methods of measurement in epidemiology paper. Int. J. Epidemiol. (2012) 41:871–86. doi: 10.1093/ije/dys037
31. Buntin MB, Zaslavsky AM. Too much ado about two-part models and transformation? Comparing methods of modeling Medicare expenditures. J Health Econ. (2004) 23:525–42. doi: 10.1016/j.jhealeco.2003.10.005
32. Duan N. Smearing estimate: a nonparametric retransformation method. J Am Stat Assoc. (1983) 78:605–10. doi: 10.1080/01621459.1983.10478017
33. Chen J, Vargas-Bustamante A, Mortensen K, Thomas SB. Using quantile regression to examine health care expenditures during the Great Recession. Health Serv Res. (2014) 49:705–30. doi: 10.1111/1475-6773.12113
34. Zhao J, Zhong H. Medical expenditure in urban China: a quantile regression analysis. Int J Health Econ Manag. (2015) 15:387–406. doi: 10.1007/s10754-015-9174-0
35. Secretaría de la Función Pública. Elements to discuss a National Care Strategy (ENAC) in Mexico. (Elementos para discutir una Estrategia Nacional de Cuidados (ENAC) en México). México (2019). Available online at: http://aga.funcionpublica.gob.mx/aga/Home/Documento?doc=Producto%20cuidados.pdf (accessed October 17, 2019).
Keywords: dependent older adults, OOP healthcare expenditures, two-part regression model, basic activities of daily living, instrumental activities of daily living
Citation: Salinas-Rodríguez A, Manrique-Espinoza B, Torres Mussot I and Montañez-Hernández JC (2020) Out-of-Pocket Healthcare Expenditures in Dependent Older Adults: Results From an Economic Evaluation Study in Mexico. Front. Public Health 8:329. doi: 10.3389/fpubh.2020.00329
Received: 19 February 2020; Accepted: 15 June 2020;
Published: 24 July 2020.
Edited by:
Louise Lafortune, University of Cambridge, United KingdomReviewed by:
Alexjandro C. Daviano, EBSCO Health, United StatesKate O'Loughlin, University of Sydney, Australia
Copyright © 2020 Salinas-Rodríguez, Manrique-Espinoza, Torres Mussot and Montañez-Hernández. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julio Cesar Montañez-Hernández, anVsaW8ubW9udGFuZXpAaW5zcC5teA==