 Ao Yang1†
Ao Yang1† Qian Qiu2†
Qian Qiu2† Xianghua Kong3Yanyu Sun4Tingying Chen5Yujie Zuo6Danfeng Yuan1Wei Dai1Jihong Zhou1
Xianghua Kong3Yanyu Sun4Tingying Chen5Yujie Zuo6Danfeng Yuan1Wei Dai1Jihong Zhou1 Anzhou Peng3*
Anzhou Peng3*- 1Department of Traffic Injury Prevention Research Office, Army Medical Center of the PLA, Daping Hospital, Chongqing, China
- 2Department of Tuberculosis Research Office, Chongqing Public Health Medical Treatment Center, Chongqing, China
- 3Department of the Fifth Tuberculosis, Chongqing Public Health Medical Treatment Center, Chongqing, China
- 4Department of the Third Infection, Chongqing Public Health Medical Treatment Center, Chongqing, China
- 5Department of General Internal Medicine, Chongqing Public Health Medical Treatment Center, Chongqing, China
- 6Department of the Second Tuberculosis, Chongqing Public Health Medical Treatment Center, Chongqing, China
Objectives: To study in-depth the clinical and epidemiological characteristics of pneumonia resulting from COVID-19 and provide evidence for effective public health decisions.
Methods: This was a retrospective, single-center research study. Participants were enrolled from patients presenting at the Chongqing Public Health Medical Treatment Center from Jan 24 to Feb 7, 2020, and were confirmed as having COVID-19.
Results: A total of 114 COVID-19 patients (99 mild, 4 severe, 11 critical) of which 56 (56/114; 49.1%) were male, 58 (58/114; 50.9%) were female with a mean age of 46.05 years. Twenty nine (29/114; 25.44%) patients suffered from chronic diseases. Neutrophils counts in 23.68% (27/114) of patients were abnormally low and abnormally high in 21.05% (24/114). Erythrocyte sedimentation rate and the C-reactive protein levels were abnormally elevated in 76.5% (62/81) and 62.9% (66/105) of patients, respectively. Creatine kinase isoenzymes (CK-MB), pro-brain natriuretic peptide (pro-BNP) and troponin levels were above the normal range in 7.10% (8/112), 66.7% (10/15), and 100% of patients, respectively. The percentage of patients in which the partial pressure of oxygen (PaO2)/fraction of inspired O2(FiO2) ratio exceeded 200 was 60%. A total of 91 (91/114; 79.82%) patients displayed severe bilateral pneumonia, 52 (52/114; 45.61%) exhibited ground-glass opacity, and pulmonary consolidation was observed in 4 (3.51%) patients. Differences in shortness of breath, insomnia, inappetence, the procalcitonin (PCT) levels, FiO2 and PaO2/FiO2 among the three groups were statistically significant (p < 0.05). Differences between the mild and severe groups was observed in neutrophil and lymphocyte counts, CD4 expression, and levels of C-reactive protein, alanine aminotransferase, aspartate aminotransferase and albumin (P < 0.05). Between the mild and critical groups, differences were observed in neutrophils, platelets, and CD4 expression (P < 0.05). A difference in C-reactive protein levels between severe and critical groups was also found (P < 0.05).
Conclusions: In the majority of cases no gender differences were observed and mostly the symptoms were mild. Evidence of efficient human-to-human virus transmission was found. The elderly with comorbidities were more prone to develop into severe or critical illness. Age and comorbidity may be risk factors for poor outcome.
Introduction
As of December of 2019, a new coronavirus disease (COVID-19) caused by the SARS-CoV2 virus emerged in Wuhan, Hubei Province, China, and has spread globally via travel (1, 2). The pandemic was initially declared a Public Health Emergency of International Concern on January 20th, 2020 by the World Health Organization (WHO) (1, 3). By February 17th, there had been 72,436 confirmed cases and 1,868 confirmed deaths in Chinese Provinces and affiliated entities as of, according to the Chinese Healthy Authority, and 332,930 confirmed cases globally as of March 23rd, 2020, there being no antiviral treatments so far proven to be efficacious (4). Efforts to contain the pandemic have instead focused on public health measures such as social distancing, prohibition of public gatherings, and increased use of face masks. These measures alone, however, are unlikely to stop the pandemic owing to the highly contagious nature of the disease (5).
Chongqing Public Health Medical Center, a designated treatment hospital for such patients, received nearly 200 COVID-19 patients. To facilitate diagnosis and treatment, additional clinical and epidemiological features of SARS-CoV-2 pneumonia are required (6–8). Therefore, a study of the clinical and epidemiology features of 114 patients admitted to Chongqing Public Health Medical Center confirmed to have COVID-19, was conducted.
Methods
Study Design
A retrospective, single-center study was conducted. All participants presented at the Chongqing Public Health Medical Treatment Center (the designated treatment hospital for COVID-19 patients), from Jan 24 to Feb 7, 2020.
All presenting subjects diagnosed with COVID-19 in accordance with the “COVID-19 Prevention and Control Plan (Sixth Edition)” were enrolled in the study. They were confirmed using two methods, real-time RT-PCR (from an upper respiratory tract throat swab) and the chest computed tomography (CT) scan. The Chinese Center for Disease Control (CDC) was the source of RT-PCR detection reagents.
In accordance with the “COVID-19 Prevention and Control Plan (Sixth Edition),” patients were categorized by the severity of COVID-19 into three groups: mild, severe, or critical. Biochemical indicators were compared between groups, then analyzed. Epidemiological, demographic, clinical, and laboratory information were obtained from patients' medical records. Three physicians reviewed all data.
The epidemiological data of all patients (i.e., history of exposure to wildlife, history of travel or work in the epidemic area of Wuhan), confirmed patient contact history and details of family grouping; demographics (i.e., sex, age, work, period since onset, period since diagnosis and treatment), symptoms upon admission, basic disease, laboratory results, chest radiographic/CT findings and treatments that had been administered for severe COVID-19, were recorded. A comparison of these data was conducted among the mild, severe and critical patient groups.
The study information has filtered the patient's personal identity and other private information and therefore the requirements for ethical approval and informed consent were waived by the relevant authorities for the purposes this study. Access to the data was provided to the authors under permission by the Medical Administration Division of Chongqing Public Health Medical Treatment Center.
Statistical Analysis
Continuous measurements that were normally distributed are expressed as means (SD). Median (inter quartile range [IQR]) values were used to express continuous variables that were not normally distributed. Categorical variables were presented as count (%). Laboratory results outside the normal range were included. SPSS software was used for statistical testing. Count data were compared using a Chi-squared test, while measured data were compared using an ANOVA or Student's t-test as appropriate. Variance was evaluated using a Kruskal-Wallis test. All statistical testing was two-sided, with P < 0.05 considered statistically significant. Study data are expressed as means ± SD.
Results
Overall Analysis Results of 114 Patients
A total of 114 COVID-19 patients (99 mild, 4 severe, 11 critical; Table 1) were included in the study. Of these, 56 (56/114; 49.12%) were male and 58 (58/114; 50.87%) female. The mean age was 46.05 years (SD: 15.15; Table 1). A total of 44 (44/114; 38.60%) patients had a history of travel to Wuhan, 1 (1/114; 0.90%) patient was exposed to wildlife, 66 (66/114; 57.89%) patients had a history of close contact with COVID-19 patients, and 48 (48/114; 42.11%) patients lived in a close family grouping.
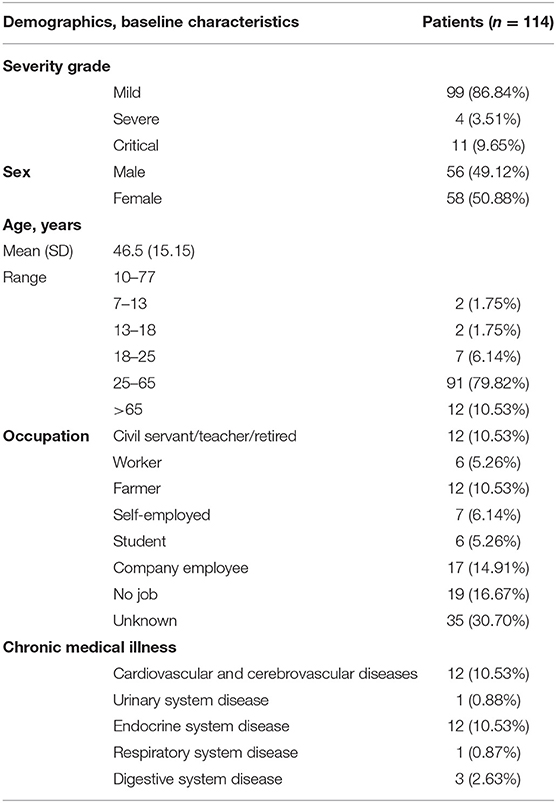
Table 1. Demographics, baseline characteristics and severity grade of COVID-19 of 114 patients admitted to Chongqing Public Health Medical Treatment Center (Jan-18, 2020) with COVID-19.
The occupations of patients were diverse. Company employees accounted for 14.91% (17/114). Twenty nine (29/114; 25.44%) patients had chronic diseases, mostly cardiovascular, endocrine, or cerebrovascular conditions (Table 1).
The symptoms at admission included mainly fever, cough, sputum, inappetence and dyspnea. Other symptoms are displayed in Table 2. All patients enrolled in the study accepted symptomatic treatment. Mechanical ventilation (8 non-invasive, 3 invasive) was used to treat the 11 critical patients.
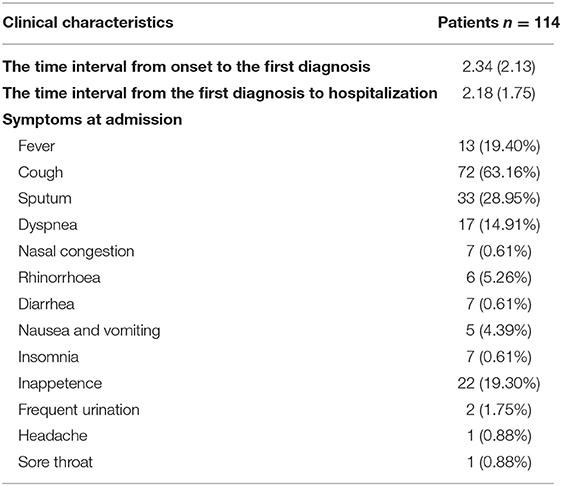
Table 2. Clinical characteristics of critical COVID-19 patients.
The mean (SD) time interval from onset to first diagnosis was 2.34 (2.13) days, while from first diagnosis to hospitalization it was 2.18 (1.75).
Body temperature was measured in 67 patients and ranged from 37.2 to 39.2°C. The temperature exceeded 38.5°C in 13 (13/67; 19.40%).
On admission, the number of neutrophils was abnormally low in 23.70% (27/114) of patients, and abnormally elevated in 21.90% (24/114) (Table 3). In many patients, numbers of leucocytes, lymphocytes, platelets, hemoglobin content, and CD4 expression were below the normal range (Table 3).
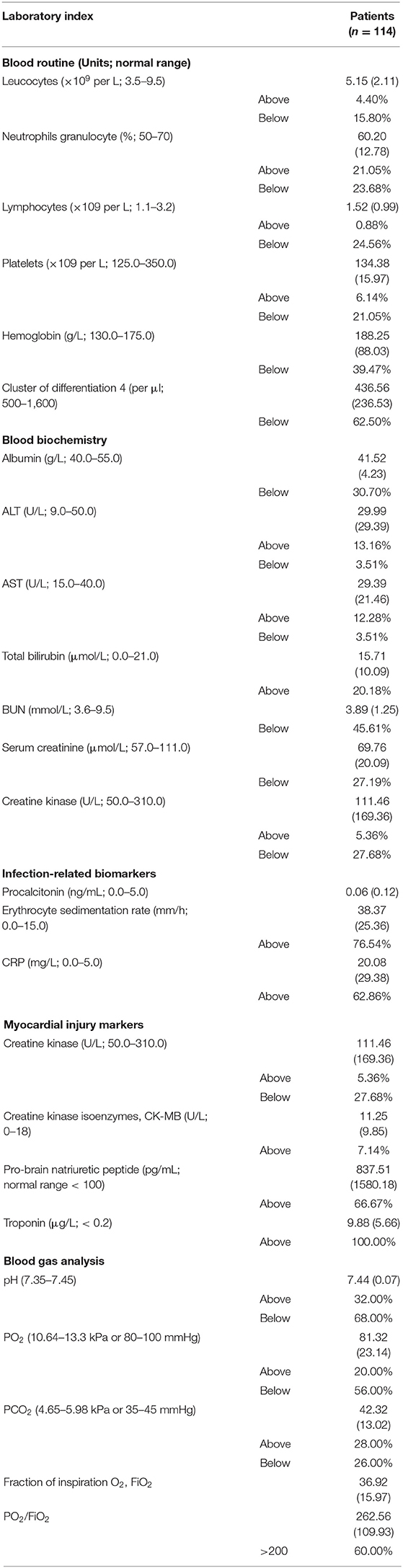
Table 3. Laboratory results of critical COVID-19 patients.
Albumin, blood urea nitrogen and serum creatinine were below the normal range in many patients, but total bilirubin was above the normal range. Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were mostly above the normal range, but the creatine kinase was generally below the normal range in many patients.
Procalcitonin (PCT) levels were normal in all cases, but erythrocyte sedimentation rate and C-reactive protein (CRP) levels were above normal in 76.5% (62/81) and 62.9% (66/105) of patients, respectively. Myocardial injury markers such as creatine kinase isoenzymes (CK-MB), pro-brain natriuretic peptide (pro-BNP) and troponin were above the normal range in 7.10% (8/112), 66.7% (10/15), and 100% of patients respectively.
PaO2 as measured by blood gas analysis was low in 56% (14/25) of patients. Blood pH was above the normal range in 44% (8/25) of patients. PaCO2 was both above and below the normal range in 20% (5/25) and 56% (14/25) of patients, respectively. The percentage of patients in whom the PaO2/FiO2 ratio exceeded 200 was 60% (15/25) (Table 3).
From CT chest scans, 91 (91/114; 79.82%) patients exhibited severe bilateral pneumonia, 52 (52/114; 45.61%) patients displayed ground-glass opacity, and 4 (4/114; 3.51%) patients showed pulmonary consolidation.
Comparison of Patient Characteristics in the Different Patient Groups by Severity of COVID-19 Symptoms
Differences in sex, age group, interval from onset to first diagnosis and first diagnosis to hospitalization, and exposure history was not statistically significant between the mild, severe, and critical group patients (p > 0.05). The mean (SD) age of the three groups was 44 years (14.62), 63.75 years (9.67), and 58.09 years (12.03), respectively. The differences between the mild group and the other two groups were statistically significant (p < 0.001). The greatest difference in number in each occupation between the three groups was between the mild and the critical groups (p < 0.001). Of all signs and symptoms at admission, only differences in shortness of breath, insomnia, and inappetence were statistically significant, and that was true for all three groups (p < 0.001; Table 4).
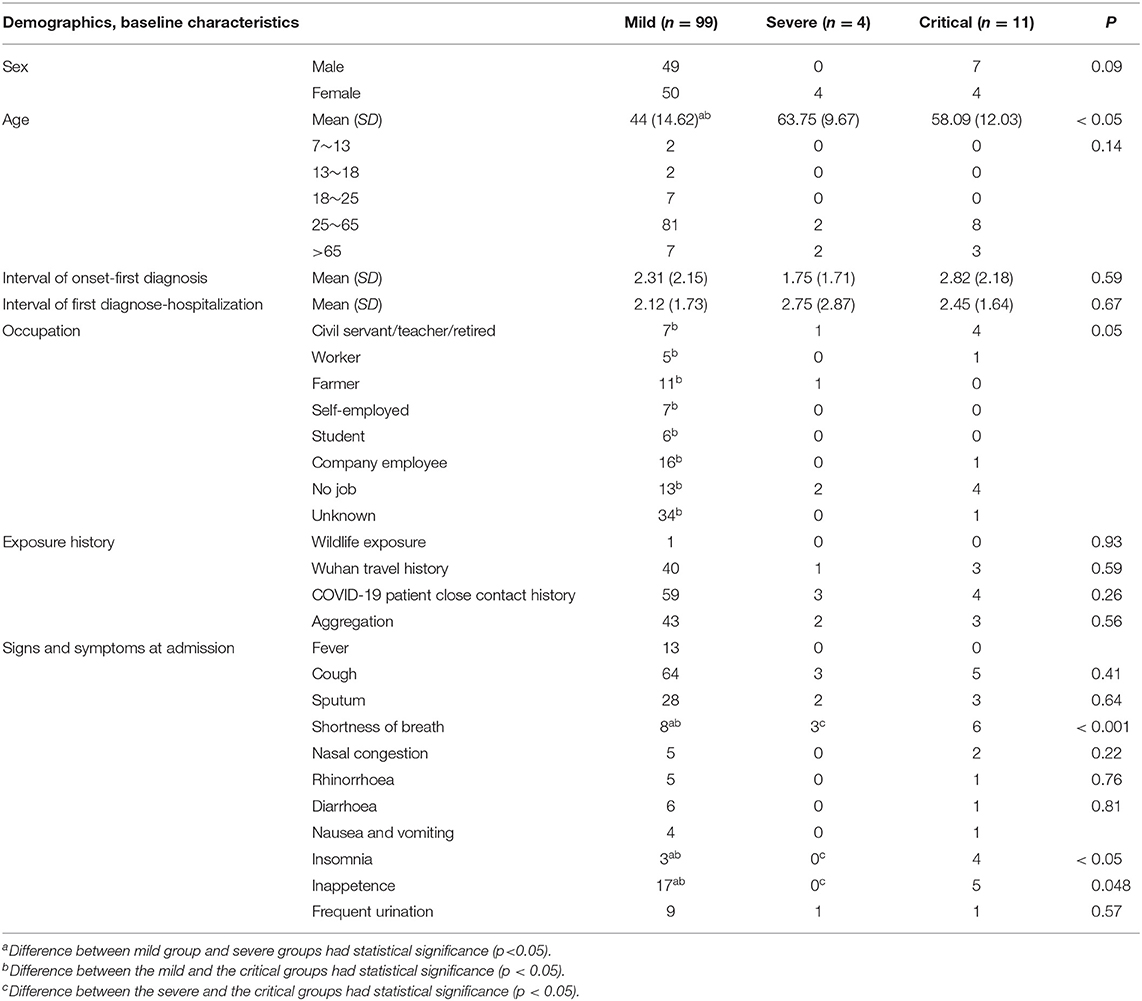
Table 4. Comparison results of demographics, baseline characteristics of different severity grade COVID-19 patients.
Levels of procalcitonin (PCT), fraction of inspired O2 (FiO2), and the PaO2/FiO2 ratio among the different patient groups were significantly different (P < 0.05). In addition, the differences in numbers of neutrophils, lymphocytes, CD4 expression, and levels of C-reactive protein, alanine aminotransferase, aspartate aminotransferase and albumin observed in the mild group compared with the severe group were significant (P < 0.05). Compared with the mild group, the difference in numbers of neutrophils, platelets, and CD4 expression in the critical group was significant (P < 0.05). A difference in C-reactive protein levels was evident between the severe and critical groups (P < 0.05), as presented in Table 5.
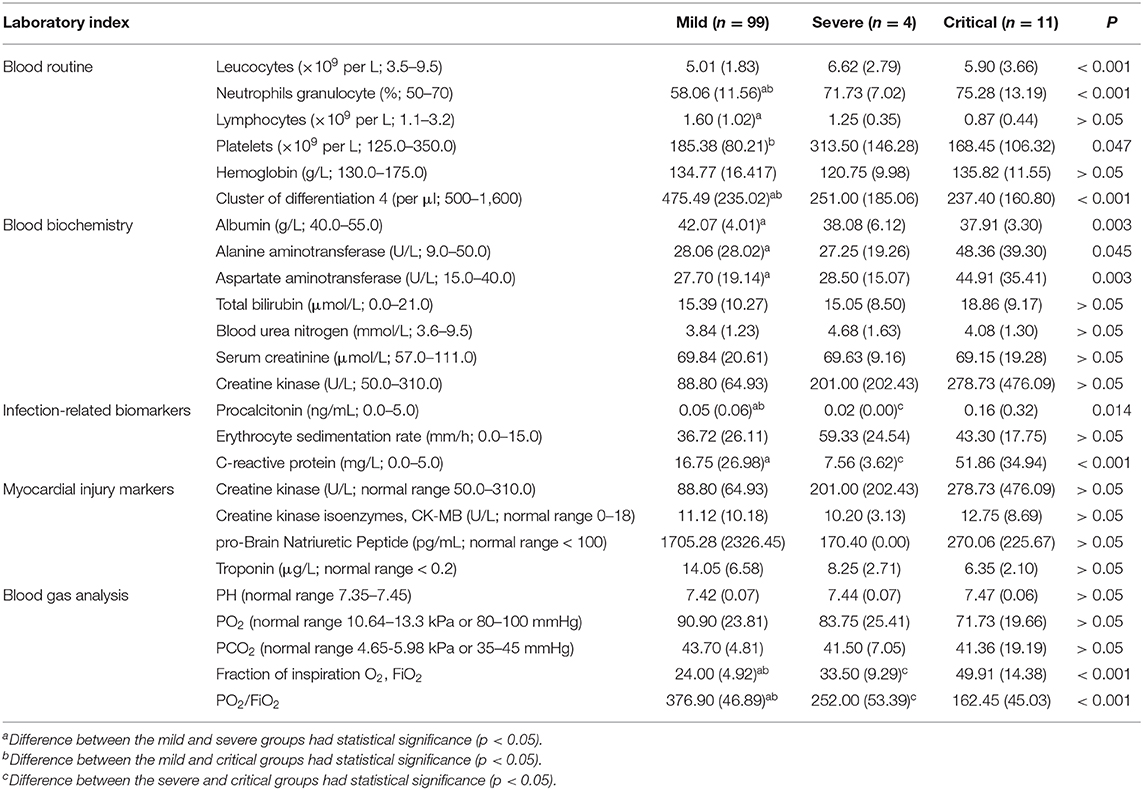
Table 5. Comparison results of laboratory of different severity grade patients with COVID-19.
Discussion
The present study reported on almost all hospitalized COVID-19 patients to date in Chongqing, and recorded the epidemiological and clinical features of the disease. Of all 114 hospitalized COVID-19 patients, 99 were classified as mild, 4 as severe, and 11 as critical. The mean time interval from onset to first diagnosis was 2.34 and 2.18 days from first diagnosis to hospitalization. Common symptoms included fever, cough, sputum, inappetence and shortness of breath. However, a significant proportion of patients initially presented with atypical symptoms, such as nausea, vomiting, and frequent urination. According to chest CT scans, 91 (79.82%) patients displayed bilateral pneumonia. Multiple mottling and ground-glass opacity is a hallmark of chest CT scans for COVID-19. Laboratory features included abnormalities of hemocytes, depressed CD4, expression, hemoglobin and PaO2, in addition to elevated total bilirubin, ALT, AST, pro-BNP, and troponin. The majority of critical patients were older and had a greater number of underlying medical conditions than did mild patients.
No statistically significant gender bias was experienced in the patients enrolled in this study, consistent with a report evaluating 138 patients hospitalized in Zhongnan Hospital in Wuhan between January 1 and 28 (9). However, these data differ from early reports that indicated that SARS-CoV-2 infection was more likely to affect males (8, 10). A possible explanation is that cases in previous studies were from the earliest phase of local outbreak and the subsequent phase of the local epidemic, mostly related to exposure associated with the Huanan Seafood Wholesale Market, most workers of which were males. The cases described herein were from the widespread national outbreak stage (9). In the current stage, no male dominance among the patients was evident, with fewer patients having been exposed to the Seafood Market (11). Furthermore, the mean age of COVID-19 patients presenting in the present study was 46.5 years. This result is consistent with the research of Yang Yao in Shaanxi province outside Wuhan (12). In that study, the majority were mild cases (86.84%), and only 9.6% required a ventilator, far fewer than those reported in prior studies from the early stages of the COVID-19 pandemic (11), indicating that this disease has potentially become more mild as the chains of transmission have grown. However, the majority of COVID-19 cases, including those which are mild, can still quickly become severe or critical without medical support (13).
A number of studies have suggested that rapid person-to-person transmission of SARS-CoV-2 was the major mode of transmission (9, 14). The data in this study indicate a history of high family grouping (42.1%) and close contact with COVID-19 patients (57.9%). These data are evidence of efficient human-to-human viral transmission. A reason for the rapid spread may due to abundant routes of transmission. According to the sixth edition of guidance for diagnosis and treatment of COVID-19 issued by the National Health Commission of China, SARS-CoV-2 is transmitted through respiratory aspirates, droplets, contact and feces, and even vertical transmission (15). Another explanation may be atypical symptoms in the early stages of SARS-CoV-2 infection. From data-driven analysis, the basic reproduction number in the early stage ranged from 2 to 3.5, such that each case was linked to 2–3.5 new infections (16–19). Government-implemented quarantine efforts are thus required for the control of further COVID-19 outbreaks.
A number of changes in symptomatology have already been observed in patients in Chongqing. The presenting symptoms included fever (19.4%), cough (63.16%), sputum (28.95%), inappetence (19.30%), and shortness of breath (14.91%), followed by nasal congestion, rhinorrhea, diarrhea, nausea, and vomiting, insomnia, frequent urination, headache and sore throat. In comparison, fever was observed in more than 90% of hospitalized patients (9, 10, 14). We speculate that increases in confirmed asymptomatic cases were due to the wide use of RT-PCR fast detection technology and intense surveillance. Compared with symptoms in mild patients, more common in severe or critical patients included shortness of breath, insomnia, and inappetence. Symptom onset may allow physicians to identify patients with poor prognosis.
Individuals suffering from viral pneumonia typically exhibit low oxygen saturation, deviations in blood gas levels, and clear abnormalities in chest imaging scan including areas of patchy consolidation, ground glass opacity, alveolar exudate, and interlobular involvement (20). The present study found similar chest imaging results. The most common laboratory abnormalities observed in the present study were depressed numbers of leucocytes, lymphocytes, lower hemoglobin content, platelets, CD4 expression and PaO2, and reduced levels of albumin, blood urea nitrogen, serum creatinine, and creatine kinase, in addition to elevated total bilirubin, ALT, AST, pro-BNP, and troponin. These laboratory abnormalities are consistent with prior findings in those with SARS-CoV2 infection (14), and even MERS-CoV and SARS-CoV infection (9), suggesting that SARS-CoV-2 infection may be associated with cellular immunodeficiency, myocardial and hepatic injury, nutrient consumption and hypoxemia. Compared with patients with mild symptoms, those with severe or critical symptoms exhibited differences in neutrophil count and CD4 expression. Differences in CRP levels were also found in severe and critical groups (Table 5). The difference in neutrophil count and CRP may be related to the cytokine storm induced by virus invasion of the virus. These parameters possibly predict disease severity and represent potential biomarkers.
The present study also indicated that patients in severe and critical groups were mostly elderly, the majority with comorbidities prior to admission. This suggests that age and comorbidities are linked to risk of poor outcome. Wang et al. found that the median time from onset of symptoms to death in persons aged 70+ was 11.5 days, significantly lower than in younger individuals (20 days) (21). These findings suggest the disease may progress faster in the elderly than in the young. In addition to older individuals being more likely to be infected with SARS-CoV-2 (16). From the above, although a definitive association could not be made, attention should be paid to the elderly as they may be more vulnerable to the SARS-CoV-2 (21).
The duration of the study was relatively short (January 24th to February 7th, 2020), studying a sudden outbreak of an infectious disease, of which only confirmed cases during this period were examined. Thus, the small sample size, and lack of additional centers within the study were limitations. Despite these limitations, some specific conclusions can be drawn, from which subsequent studies should be built.
In this single-center case series of 114 hospitalized patients with confirmed COVID-19 in Chongqing, China, epidemiological and clinical features were recorded, which may help provide guidance for frontline medical staff in the clinical management of the outbreak. However, the present study is limited by its geographical location and the insufficient sample size. A large-scale multicenter study is required to verify our findings.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The study information has filtered the patient's personal identity and other private information and therefore the requirements for ethical approval and informed consent were waived by the relevant authorities for the purposes this study. Access to the data was provided to the authors under permission by the Medical Administration Division of Chongqing Public Health Medical Treatment Center.
Author Contributions
AY, QQ, and AP were involved in the conception and design of the study. AY performed the data analysis, had full access to all of the study data, and take responsibility for the integrity of the data and the accuracy of the analyses. XK, YS, TC, and YZ were responsible for collecting and organizing all patients' data. DY and WD were responsible for aggregating data. JZ was in charge of guiding our research design. AY and QQ drafted the manuscript. All authors were involved in the interpretation of the results, made major contributions to critically reviewing the manuscript for important intellectual content, and read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
COVID-19, Corona Virus Disease 2019; SD, standard deviation; RT-PCR, Reverse Transcription-Polymerase Chain Reaction; CRP, C-reactive protein; CK-MB, creatine kinase isoenzymes; pro-BNP, pro-brain natriuretic peptide; PCT, procalcitonin; CD4, cluster of differentiation 4; WHO, World Health Organization; CDC, Center for Disease Control; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CT, Computed Tomography; PH, hydrogen ion concentration; FiO2, fraction of inspiration O2.
References
1. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. (2020) 382:727–33. doi: 10.1056/NEJMoa2001017
2. Novel Coronavirus (2019-nCoV): Situation Report-10 30 January 2020. Geneva: World Health Organization (2020). Available online at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200130-sitrep-10-ncov.pdf
3. WHO. Statement on the Second Meeting of the International Health Regulations. (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV) (2020). Available online at: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov)
4. Yang Y, Lu Q, Liu M, Wang Y, Zhang A, Jalali N, et al. Epidemiological and clinical features of the 2019 novel coronavirus outbreak in China. medRxiv. (2020) doi: 10.1101/2020.02.10.20021675. [Epub ahead of print].
5. Peak CM, Childs LM, Grad YH, Buckee CO. Comparing nonpharmaceutical interventions for containing emerging epidemics. Proc Natl Acad Sci USA. (2017) 114:4023–8. doi: 10.1073/pnas.1616438114
6. Lu H, Stratton CW, Tang YW. Outbreak of pneumonia of unknown etiology in Wuhan China: the mystery and the miracle. J Med Virol. (2020) 92:401–2. doi: 10.1002/jmv.25678
7. Hui DS, Azhar EI, Madani TA, Ntoumi F, Kock R, Dar O, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health - the latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. (2020) 91:264–66. doi: 10.1016/j.ijid.2020.01.009
8. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
9. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. (2020) 323:1061–9. doi: 10.1001/jama.2020.1585
10. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
11. Brussow H. The novel coronavirus - a snapshot of current knowledge. Microb Biotechnol. (2020) 13:607–12. doi: 10.1111/1751-7915.13592
12. Yao Y, Tian Y, Zhou J, Ma X, Yang M, Wang S. Epidemiological characteristics of 2019-ncoV infections in Shaanxi, China by February 8, 2020. Eur Respir J. (2020) 55:2000310. doi: 10.1183/13993003.00310-2020
13. Pan Y, Guan H, Zhou S, Wang Y, Li Q, Zhu T, et al. Initial CT findings and temporal changes in patients with the novel coronavirus pneumonia (2019-nCoV): a study of 63 patients in Wuhan, China. Eur Radiol. (2020). doi: 10.1007/s00330-020-06731-x. [Epub ahead of print].
14. Wang Y, Wang Y, Chen Y, Qin Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J Med Virol. (2020). doi: 10.1002/jmv.25748. [Epub ahead of print].
15. Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. (2020) 395:809–15. doi: 10.1016/S0140-6736(20)30360-3
16. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. (2020) 382:1199–207. doi: 10.1056/NEJMoa2001316
17. Riou J, Althaus CL. Pattern of early human-to-human transmission of Wuhan 2019 novel coronavirus (2019-nCoV), December 2019 to January 2020. Euro Surveill. (2020) 25:2000058. doi: 10.2807/1560-7917.ES.2020.25.4.2000058
18. Wu JT, Leung K, Leung GM. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: a modelling study. Lancet. (2020) 395:689–97. doi: 10.1016/S0140-6736(20)30260-9
19. Liu Y, Gayle AA, Wilder-Smith A, Rocklov J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. (2020) 27:taaa021. doi: 10.1093/jtm/taaa021
20. Velavan TP, Meyer CG. The COVID-19 epidemic. Trop Med Int Health. (2020) 25:278–80. doi: 10.1111/tmi.13383
Keywords: SARS-Cov-2, COVID-19, epidemiological, clinical characteristics, China
Citation: Yang A, Qiu Q, Kong X, Sun Y, Chen T, Zuo Y, Yuan D, Dai W, Zhou J and Peng A (2020) Clinical and Epidemiological Characteristics of COVID-19 Patients in Chongqing China. Front. Public Health 8:244. doi: 10.3389/fpubh.2020.00244
Received: 24 March 2020; Accepted: 19 May 2020;
Published: 29 May 2020.
Edited by:
Zisis Kozlakidis, International Agency for Research on Cancer (IARC), FranceReviewed by:
Elima Jedy-Agba, Institute of Human Virology, Nigeria (IHVN), NigeriaFengping Liu, Jiangnan University, China
Copyright © 2020 Yang, Qiu, Kong, Sun, Chen, Zuo, Yuan, Dai, Zhou and Peng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anzhou Peng, cGVuZ2FuemhvdTIwMTBAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship