 Yui Takebayashi1,2
Yui Takebayashi1,2 Masaharu Maeda1,2*Masatsugu Orui3,4
Masaharu Maeda1,2*Masatsugu Orui3,4 Satomi Nakajima5Maho Momoi1,2Akiko Ito1,2
Satomi Nakajima5Maho Momoi1,2Akiko Ito1,2 Hideki Sato1,2
Hideki Sato1,2 Seiji Yasumura2,3Hitoshi Ohto2
Seiji Yasumura2,3Hitoshi Ohto2- 1Department of Disaster Psychiatry, Fukushima Medical University School of Medicine, Fukushima, Japan
- 2Radiation Medical Science Center for the Fukushima Health Management Survey, Fukushima Medical University, Fukushima, Japan
- 3Department of Public Health, Fukushima Medical University School of Medicine, Fukushima, Japan
- 4Sendai City Mental Health and Welfare Center, Sendai, Japan
- 5Faculty of Human Sciences, Musashino University, Tokyo, Japan
Aim: The aims of the present study were to develop and validate a psychological resilience scale reflecting the specificity of the Fukushima disaster, and to examine the effects of this scale on mental health.
Methods: The Fukushima Resilience Scale was developed based on data obtained from semi-structured interviews with seven people who had lived in the affected area of Fukushima Prefecture at the time of the disaster. The reliability and validity of the scale were then examined in cross-sectional studies conducted on 500 evacuees through an epidemiological mail survey. To examine the effects of the scale and disaster-related factors on the general mental health status of the respondents, a logistic regression analysis was performed using the six-item Kessler psychological distress scale.
Results: The newly developed scale consisted of a four-factor structure: “coping with stigma-related issues,” “sharing experiences of the disaster,” “action-oriented approach,” and “sense of support.” Internal consistency coefficients ranged from 0.66 to 0.79. The multivariable logistic regression analysis showed that the only significant association was between “action-oriented approach” (odds ratio = 1.26) and respondents with a K6 score <5 points.
Conclusion: The reliability and concurrent validity of the new developed scale in residents of the evacuation area of Fukushima Prefecture were acceptable. A significant association was found between “action-oriented approach” and good mental health among the evacuees, which suggests that this may improve resilience among people affected by the Fukushima disaster.
Introduction
The Great East Japan Earthquake (GEJE) and the consequent severe accident at the Fukushima Daiichi Nuclear Power Plant (FDNPP) caused devastating damage to Fukushima Prefecture and its residents. Over 40,000 people remain evacuees inside or outside of Fukushima and continue to suffer from not only worry about the adverse health effects from exposure to radiation, but also unfounded rumors and public stigma (1). In fact, the result of a recent major survey conducted on evacuees by Fukushima Medical University indicated that as much as 7% of these evacuees are at risk of depression (2). In addition, more than 100 disaster-related suicides have been reported in Fukushima since the disaster, exceeding the numbers in Miyagi and Iwate Prefectures, which were affected mainly by the tsunami (3).
Regardless of such difficulties in terms of relief efforts, several items identified in panel data from Fukushima have suggested positive and hopeful change after the disaster (4). For example, remarkable increases in residential construction, agricultural production, job growth, and industrial output have been observed. However, although such physical improvements have been seen, few studies have revealed any positive changes in terms of psychological issues among disaster-affected people in Fukushima. In particular, psychological resilience factors, which should play an important role in recovery efforts after natural disasters (5), have yet to be comprehensively examined.
With regard to resilience, epidemiological studies in natural and technological disasters such as Nias–Simeulue earthquake (2005), Sichuan earthquake (2008), Haiti earthquake (2010), Hurricane Katrina (2005), and Deepwater Horizon Oil Spill accident (2010) showed substantial association between psychological problems and individual resilience (6–10). Studies performed in the Tohoku area also revealed that individual resilience among medical workers in the first year after the GEJE predicted high work engagement after 4 years (11), and that resilience among initial responders such as firefighters was associated with a low severity of post-traumatic stress disorder (PTSD) symptoms (12). In addition, one study involving high school students in Miyagi Prefecture showed an increase in those having high resilience, as well as a negative correlation between high resilience and depressive symptoms (13). Furthermore, a study of evacuees from a town located near the FDNPP suggested that resilience could be an important meditator of depression, PTSD, and other general mental health issues (14). Another recent study conducted on evacuees after the GEJE revealed a positive association between mental health recovery and desirable lifestyles and social networks, particularly in regard to social roles (15).
Although these studies suggested that psychological resilience could contribute to the retention or restoration of mental health among people affected by GEJE, in the case of complex disasters such as the Fukushima disaster that cause long-term psychological effects, resilience factors remain unclear. Especially in Fukushima, multidimensional psychosocial issues, including the fragmentation of communities and the weakening of social capital, resulting from situations of ambiguous loss and differing opinions toward radiation effects, exert long-term influence on the mental health of those affected (1). For example, in contrast with other prefectures affected mainly by tsunami (e.g., Miyagi and Iwate Prefectures), people experiencing the nuclear power plant accident in Fukushima Prefecture tended to relocate to remoter area across the country. Actually, there are over 40,000 still staying out of Fukushima Prefecture due to fear for radiation exposure or other related reasons; on the other hand, only a few evacuees who had met tsunami in Miyagi and Iwate Prefecture were evacuated outside their original prefectures. Such remote, prolonged evacuation of the Fukushima people, leading family separation and/or loss of their future plans as well as stable lives, could damage preexisting community structure and culture. In addition, the Fukushima evacuees have been more likely to be stigmatized due to stereotype and prejudice among the public relating to genetic effects of radiation exposure and/or compensation from Tokyo Electric Power Company. Such stigmatization is also considered to be one of very unique social consequences emerging among Fukushima evacuees, while not seen in natural disasters (1).
Given these specific features of Fukushima evacuees, resilience in relation to natural disasters may work in different ways. To clarify the situation regarding psychological resilience among disaster-affected people in Fukushima and establish further mental health care strategies, we attempted to identify resilience factors reflecting the specificity of the Fukushima disaster. For this purpose, a new scale to assess individual resilience among them should be made, because existing measurements such as the Connor–Davidson Resilience Scale (CD-RISC) focused on only psychological factors without including social factors (16). This study, thus, involved two procedures: the first (preliminary study) was to extract possible resilience factors relating to the Fukushima disaster through individual interviews with a small number of evacuees; the second (main study) was to conduct an epidemiological mail survey on a larger group of evacuees based on the above procedure. The findings obtained were expected to contribute to the establishment of mental health policies that promote recovery among those affected by the Fukushima disaster.
Incidentally, the concepts and definitions of resilience are considerably diverse (17).
In this study, we adopted the definition of resilience proposed by Rutter (18) in 1985, which was somewhat obscure but had been commonly used in domains of psychiatry and psychology; namely, resilience is the ability to bounce back or cope successfully despite substantial adversity.
Preliminary Study (Study 1)
Method
This preliminary study was conducted to develop a useful measurement for the main study (Study 2), as described later.
Participants
This study sample comprised seven affected people (1 man, 6 women; mean age ± standard deviation, 53.0 ± 13.6 years) who had once lived in the affected area of Fukushima Prefecture at the time of the disaster; five of these residents were thereafter evacuated to another area for at least 6 years. They all had experienced traumatic events related to the disaster, especially the FDNPP accident. For example, almost all of the evacuees felt extremely fearful and realized that they were driven to critical moments when hearing about the meltdown at the FDNPP. When this survey was conducted, all the participants were engaged in group activities supporting reconstruction in Fukushima, even though they were not professionals. People having apparent severe psychiatric symptoms such as depressive symptoms, including suicidal ideation, delusions, or other psychotic symptoms, were excluded. Written informed consents were obtained by mail from all the participants before their interviews. This survey was approved by the ethics review committee of Fukushima Medical University on July 29, 2016 (No. 2738).
Survey Procedure and Variables
All participants took part in individual semi-structured interviews with a psychiatrist (SN) or clinical psychologists (YT and MMo) at their workplace; each interview lasted about 60 min. After inquiring about their history and personal experience after the disaster, the participants were asked about matters relating to their resilience using the following questions: (1) Do you think something contributed to your life even after the disaster? If so, what?; (2) Do you think something changed in terms of your mind or lifestyle after the disaster? If so, what?; (3) Do you think you got something from the disaster? If so, what?; (4) Do you feel as though you have some pleasure or satisfaction now? If so, from what?; and (5) What do you think could contribute to happiness among disaster-affected people in the future?
These questions were considered necessary to assess whether there were some positive changes related to resilience among disaster-affected people, even after the experience of the disaster and subsequent long-term evacuation life.
Analysis
The results of the interviews were qualitatively analyzed using the KJ method with our research team (consisting of YT, SN, MMo, and AI). The KJ method was developed by Kawakita in the 1960s, and has been widely used in Japan for the sake of grouping data and making affinity diagrams (19).
Results
As a result of the KJ method, items relating to resilience were classified into the following eight categories: (1) receiving support (e.g., support from family members or others); (2) positive acceptance in an evacuation area or other new address (e.g., good interaction in an evacuation area, participation in some social activities); (3) interaction with people evacuated from the same affected area (e.g., interaction with friends before the disaster occurred, opportunities to talk about life as an evacuee with each other); (4) work and related issues (e.g., employment or unemployment, job satisfaction, having a job that is somewhat helpful to others, good relationship with coworkers); (5) hobbies and pleasure; (6) changes in personal awareness (e.g., feeling of gratitude for daily life, self-efficacy, being able to do something new, acceptance of current difficulties); (7) sense of distance from one's hometown; and (8) reduction of anxiety related to radiation exposure.
These eight categories were composed of a total of 16 question items; these were arranged to devise the new resilience questionnaire for evacuees of the Fukushima disaster (Fukushima Resilience Scale; FRS) (Table 1).
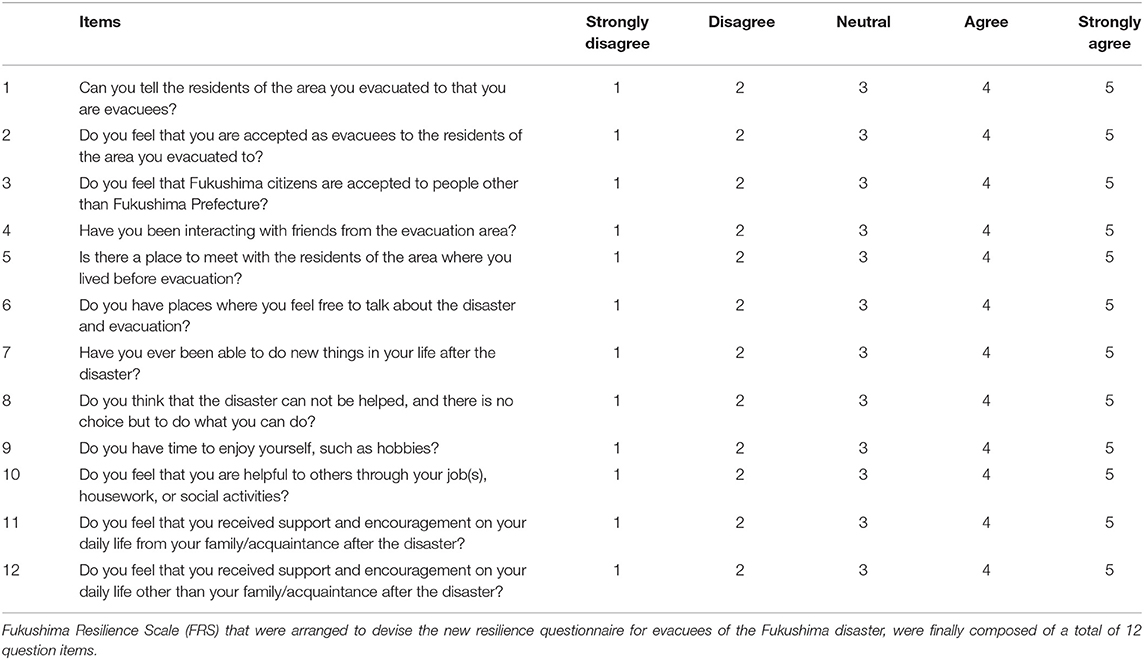
Table 1. The items of the Fukushima Resilience Scale (FRS).
Main Study (Study 2)
Method
The main study was conducted using the new questionnaire devised in the preliminary study (Study 1).
Participants
This was a cross-sectional questionnaire survey of 1,000 residents of Fukushima Prefecture aged 20 years and above. Among these, 500 people from the evacuation area consisting of Tamura city, Minami-soma city, Kawamata town, Hirono town, Naraha town, Tomioka town, Okuma town, Futaba town, Namie town, Kawauchi village, Katsurao village, and Iitate village were selected. The Japanese government has indicated evacuation areas according to spatial radiation dose rates as follows: (1) difficult-to-return areas with a radiation dose rate ≥50 mSv per year; (2) residence-restricted areas with a radiation dose rate ≥20 and <50 mSv per year; and (3) areas where evacuation orders were ready to be lifted as of April 22, 2011. The residents of the evacuation area were forced to leave their homes at the direction of the Japanese government. In total, 500 people in the non-evacuation area were selected using a two-stage stratified random sampling method. We sent an anonymous, self-reporting postal questionnaire to participants from January to February 2018. In addition, 500 people were targeted from the evacuation area.
This survey was approved by the ethics review committee of Fukushima Medical University on October 10, 2017 (No. 29206). Part of the data obtained from the same participants was reported in another article (15) that analyzed and showed the recovery patterns of mental health among these individuals.
Survey Variables
1) Disaster-related experiences
Disaster-related experiences (e.g., housing damage, loss of family, relatives, or friends, separation from family members, and disaster-related loss of employment) were evaluated on a two-point scale, defined as “Experienced” or “Never.”
2) Intention about future living place
Intention about future living place was assessed on a four-point scale, defined as “Not yet determined,” “Returned,” “Intend to return,” and “Do not intend to return.”
3) Economic status
We assessed economic status using the following question “Do you feel that you can get by according to your current economic status?,” which was assessed on a five-point scale, defined as “Difficult,” “Somewhat difficult,” “Average,” “Somewhat adequate,” and “Adequate.” Occupational category was evaluated on a five-point scale, defined as “Employed,” “Owner,” “Part-time,” “Homemaker,” and “Unemployed.”
4) Resilience
We used the FRS devised in the preliminary study (Study 1). To assess its concurrent validity, we used the Connor–Davidson Resilience Scale (CD-RISC). The CD-RISC was developed to assess an individual's ability to cope with traumatic stress (16). It is composed of 25 items, all of which are rated on a five-point Likert scale, with higher scores indicating greater resilience. The reliability and validity of the Japanese version of the CD-RISC have been confirmed (20).
5) General mental health status
We used the 6-item Kessler psychological distress scale (K6), which is a self-administered measure used to screen for mood or anxiety disorders. Participants scoring 5–12 points were classified as having psychological distress (21), whereas those scoring 13–24 points were classified as having probable severe psychological distress (22). The reliability and validity of the Japanese version of the K6 have been confirmed (23).
Statistical Analysis
The factorial validity for the FRS for the triple disaster (earthquake, tsunami, and nuclear accident) was evaluated using an exploratory analysis utilizing the least-squares method with promax rotation. The number of factors was determined by minimum average partial (MAP) correlation and parallel analysis. We evaluated the internal consistency of the newly developed FRS using Cronbach's alpha. Concurrent validity was evaluated using a correlation analysis between the CD-RISC, FRS, and K6.
The chi-squared test was used to estimate the associations between general mental health status (K6 score) and disaster-related experiences, intention regarding future living place, and economic status. Next, a multivariable logistic regression model was carried out with general mental health status (K6 score) as the dependent variable. The independent factors used in this analysis were only those showing significant differences or tendencies according to the chi-squared test; these included economic status, disaster-related factors, and factors obtained from the above exploratory factor analysis. With regard to the independent factors, groups with a K6 score >5 in were adopted as a reference. All statistical analyses were performed using SPSS 25.0 (IBM Corp., Armonk, NY, USA).
Results
Participants
After excluding 58 individuals that were returned to sender because no one was residing at the address, from among the remaining 442 questionnaires sent out, we received 191 responses (response rate, 43.2%). After excluding five respondents who failed to provide information regarding their age or gender, and 11 who did not complete the K6, the final study population consisted of 175 respondents (Figure 1).
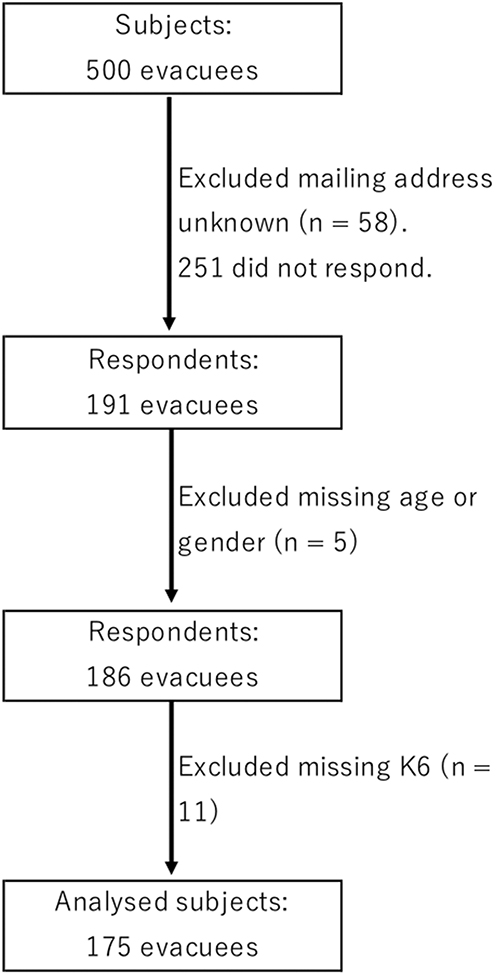
Figure 1. Flow chart of study procedures. From the targeted population (n = 500), 58 were excluded due to mailing address unknown. Two hundred fifty-one did not respond. Final number of valid responses was 175 after excluding respondents with missing data regarding age, gender or the 6-item Kessler psychological distress scale (K6).
Respondent Characteristics
Finally, 175 respondents (82 men, 93 women; mean age ± standard deviation, 60.0 ± 14.2 year) were analyzed. In total, 69 respondents (37.1%) had a K6 score of ≤4 points, and 106 (62.9%) had a score of ≥5 points. In this study, the participants were divided into two groups for analysis (those with <5 points and those with ≥5 points). Table 2 shows the distribution of the participants' basic characteristics and disaster-related experiences. Difficult economic status and disaster-related loss of employment were significantly higher in the group with a K6 score of ≥5 points.
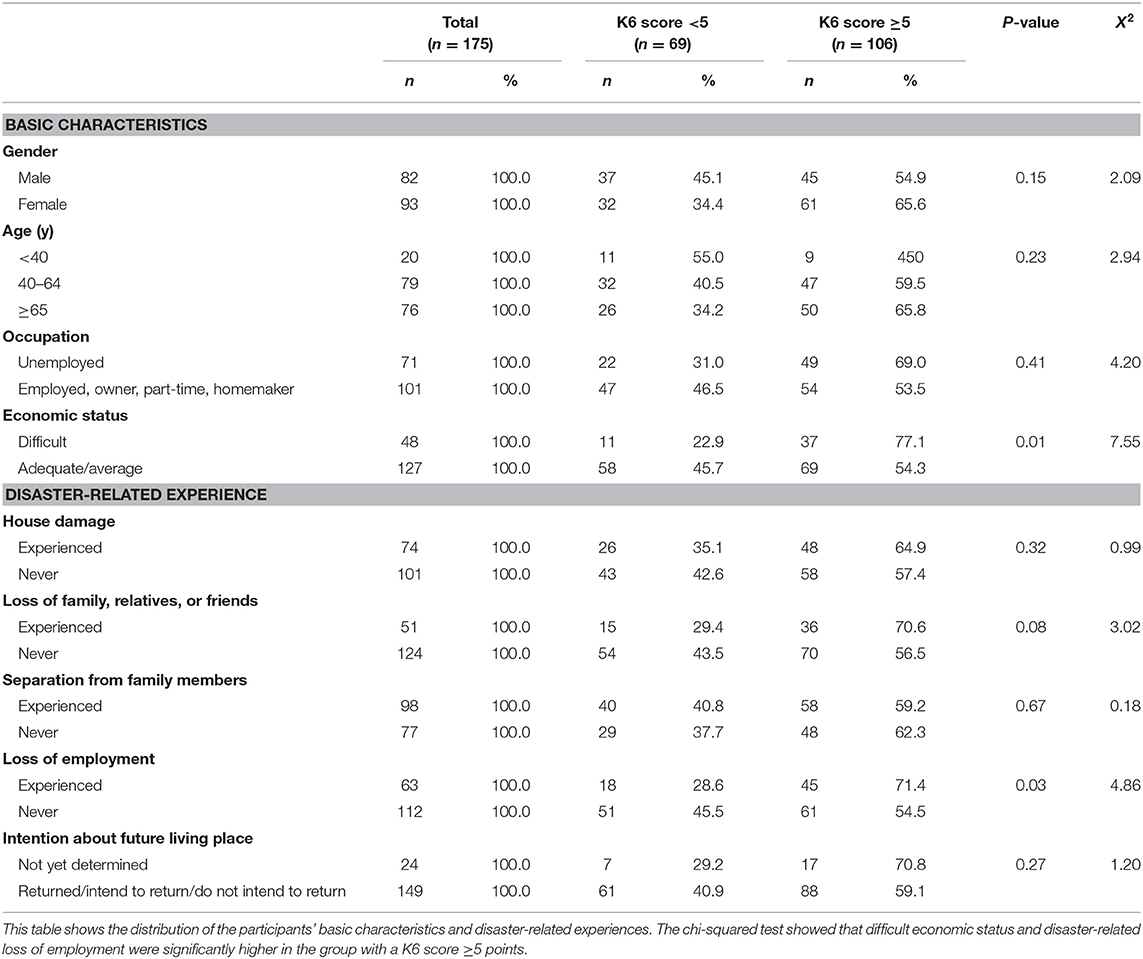
Table 2. Basic characteristics and disaster-related experiences of the participants.
Factor Analysis
The MAP correlation indicated a one-factor solution, and parallel analysis indicated a five-factor solution. From the viewpoint of interpretability, we decided that the four-factor solution was appropriate. Namely, the exploratory factor analysis showed that the FRS consisted of a four-factor structure. Items with factor loadings <0.40 were deleted, and 12 items were extracted as follows: 1st factor, three items; 2nd factor, three items; 3rd factor, four items; and 4th factor, two items (Table 3). The overall Cronbach's alpha coefficient of the scale was 0.81. Cronbach's alpha coefficients for the four factors were 0.79, 0.77, 0.66, and 0.75, which accounted for 14.9, 23.0, 8.9, and 6.5% of the variance between items, respectively. Here, we named the 1st factor “coping with stigma-related issues,” the 2nd “sharing experiences of the disaster,” the 3rd “action-oriented approach,” and the 4th “sense of support.”
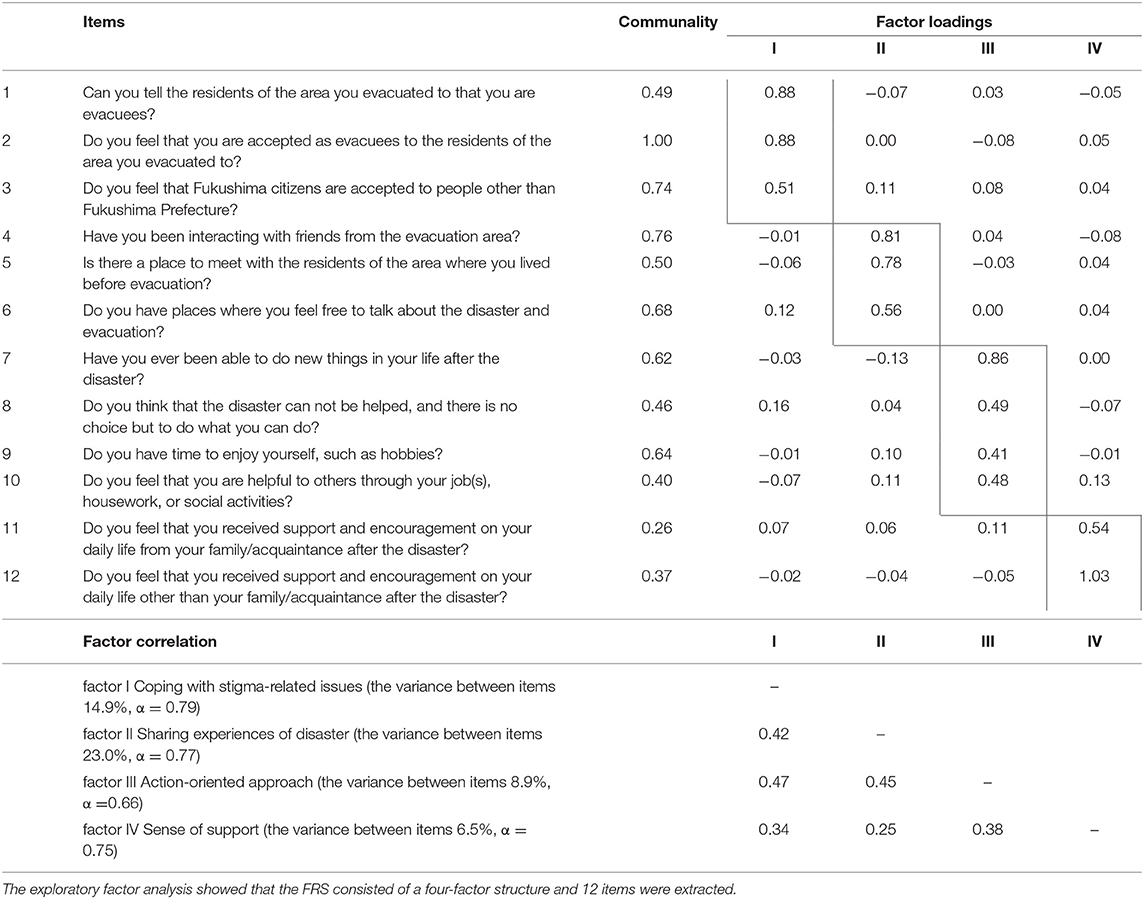
Table 3. Results of exploratory factor analysis of the Fukushima Resilience Scale (FRS).
The correlation analysis showed a significant correlation between the CD-RISC and total score of the FRS (r = 0.52, p < 0.001), as well as four factors: “coping with stigma-related issues” (r = 0.35, p < 0.001), “sharing experiences of the disaster” (r = 0.34, p < 0.001), “action-oriented approach” (r = 0.61, p < 0.001), and “sense of support” (r = 0.23, p < 0.01). Also, the correlation analysis showed a significant correlation between the K6 and total score of the FRS (r = −0.47, p < 0.001), as well as the CD-RISC (r = −0.54, p < 0.001).
Multivariable Logistic Regression Model
In the multivariable logistic regression analysis, the independent factors were economic status, loss of family, relatives, or friends and loss of employment which were observed the association with a K6 score in the chi-squared test. The result showed that only “action-oriented approach” on the FRS (odds ratio = 1.26, 95% confidence interval: 1.09–1.45) was significantly associated with the group of respondents with a K6 score of <5 points (Table 4).
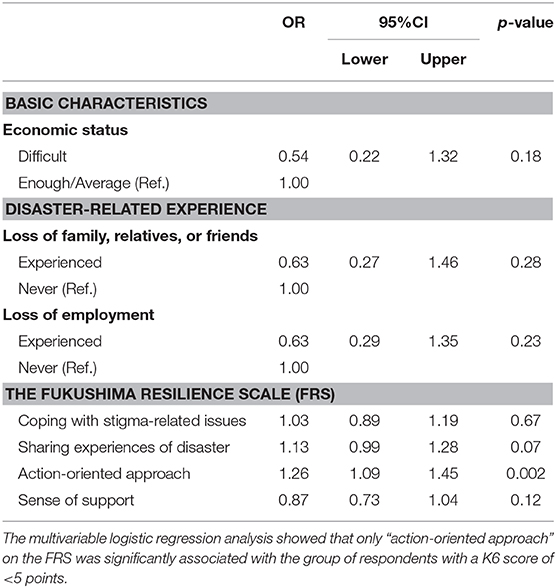
Table 4. Multivariable logistic regression analysis between K6 score and related factors.
Discussion
In the present study, we examined possible factors relating to the psychological resilience of people who were evacuated as a result of the accident at the FDNPP after the GEJE. First, semi-structured interviews were conducted with a few evacuees to clarify resilience-related factors and, as a result, a new questionnaire composed of 16 items was devised. Second, these new questionnaires were mailed to the target population of randomly selected individuals in the disaster area, and the results were analyzed mainly using exploratory factor analysis. The data gathered from the collected questionnaires (response rate: 43.2%) indicated high reliability (internal consistency) and concurrent validity with CD-RISC. The exploratory factor analysis also showed that the questionnaire was structured with four factors—“sense of support,” “action-oriented approach,” “coping with stigma-related issues,” and “sharing experiences of the disaster”—from which, 12 items were extracted (Table 3). The first two factors (“sense of support” and “action-oriented approach”) were considered to be similar to general, non-specific resilience factors demonstrated by the CD-RISC, whereas the second two factors (“coping with stigma-related issues” and “sharing experiences of the disaster”) may specifically relate to psychosocial issues caused by the Fukushima nuclear disaster and long-term evacuation life. As the result, while the CD-RISC focuses on only psychological factors that an individual might have, this newly developed scale named Fukushima Resilience Scale includes more social factors.
Previous studies have revealed that social support and fostering close relationships with other community members are important to enhance psychological resilience among disaster-affected people. Our results obtained from the factor analysis indicated the importance of good relationships with community members that had been established before the disaster, as well as good current relationships with those living in the towns that the evacuees relocate to. However, binomial logistic regression analysis including the above four factors showed that only one factor, “action-oriented approach,” was significantly associated with good mental health among the evacuees, as identified by the K6. The factor “action-oriented approach” was regarded as an important measure for resilient people (18), and represents several individual abilities related to making something to do on one's own, playing some social roles, and having leisure time. These results suggest the possibility that an “action-oriented approach” could contribute to the promotion of mental health among people affected by a major disaster. A previous study examining the influence of individual coping skills on psychological resilience also reported the significance of an action-oriented approach (24).
Many evacuees are experience ambiguous loss rather than apparent loss, such as the deaths of a loved one resulting from the tsunami (1), which may lead to the loss of certain social roles or individual life goals. Even in such ambiguous situations, evacuees who are able to set some positive new goals, do something meaningful such as recreation and foster good relationships with others, may also be able to maintain a healthy status. In the context of mental health care and treatment, promoting activities among evacuees through various types of interventions performed by different health care providers, including local health care centers, can be effective to reinforce resilience. In addition, if possible, behavioral activation used in cognitive behavioral therapy may contribute to the improvement of psychiatric symptoms such as depressive symptoms.
Despite not reaching significance level (p = 0.07), the factor “sharing experiences of the disaster,” which reflected the existence of good relationship with others even before the disaster, tended to be associated with good mental health. Given this factor, it may be effective to utilize positively social capital originally existing in different communities in Fukushima, even though such social capital has been facing a crisis, as described above. For example, numerous types of facilities or organizations, including non-profit organizations, offer community-based activities for evacuees. These resources have helped to ameliorate the fragmentation of communities in Fukushima caused by different reasons, such as long-term, repeated relocation, and differences in risk perception toward radiation exposure or delayed relief (1). Unfortunately, 8 years after the disaster, these resources remain inhibited by a lack of not only funds, but also human resources. Thus, national and municipal governments need to support these resources to develop and reestablish the strength of existing social capital.
On the other hand, several factors, including economic status, bereavement, and unemployment, were not associated with good mental health among the participants. These findings are inconsistent with previous studies conducted in regard to natural disasters. A recent meta-analysis of risk factors for depression after natural disasters revealed that serious loss experiences such as bereavement and unemployment were strongly associated with depression among affected people (25). One possible reason to explain this inconsistency is that, if we analyze the data using a group with more severe psychological distress (K6 score >13) as a reference, the loss experiences as described above might be associated with a healthy condition among the participants. Because of the difficulties involved with conducting a logistic regression analysis with a considerably small number of participants in the high distress group, we need to avoid adopting this model. Interestingly, a major mental health survey conducted on evacuees from Fukushima also showed that bereavement was not a significant factor influencing mental health, whereas radiation risk perception was the strongest factor (26). Considering this specific tendency in Fukushima, while an apparent loss experience such as bereavement was not a prominent factor affecting mental health status, many affected people in Fukushima might conceivably feel that the fragmentation or alternation of their communities was a more traumatic experience.
This study had several limitations. First, the study design was not longitudinal, but rather cross-sectional. The former can clarify more possible factors contributing to the resilience of affected people. Second, the target population of this study (Studies 1 and 2) was not large. In addition, we adopted the Rutter's concept as a definition of resilience in this study, whereas the concept of psychological resilience, essentially, is diverse and includes different ideas (27), For example, which level does resilience depend on individual or community? What does resilience stand for? Individual predispositions, including inheritance, some skills that can be acquired, or the course of recovery from disasters?
Despite these limitations, this study has shed light on resilience as opposed to vulnerability, which has been the focus of many previous studies. Furthermore, FRS newly developed in this study can be applied to other Chemical Biological Nuclear Explosive (CBRNE) disasters that might produce negative social reactions such as public stigma similar to the Fukushima disaster. Our results could help clarify the mental health care strategies that should be followed for people affected by technological disasters in public health care settings.
Data Availability Statement
Requests to access the datasets should be directed to Yui Takebayashi, dGFrZWIta3lAZm11LmFjLmpw.
Ethics Statement
The studies involving human participants were reviewed and approved by the ethics review committee of Fukushima Medical University. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
HO, SY, MMa, and SN conceived and designed the framed study. SN, MMo, and YT conducted the interview in the preliminary study. SN, MMo, AI, and YT performed the analysis in the preliminary study. MMa, MO, SN, MMo, AI, SY, HO, and YT contributed to designing the questionnaire in the main study. MO conducted the questionnaire survey in the main study. YT analyzed the data in the main study. YT, HS, and MMa wrote the paper. All authors contributed to revisions of the manuscript and critical discussion.
Funding
This study was supported by a grant from KAKENHI, the Japan Society for the Promotion of Science (JSPS), as a Grant-in-Aid for Scientific Research (C) research (JSPS KAKENHI Grant No. 16K09136).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Maeda M, Oe M. Mental health consequences and social issues after the Fukushima disaster. Asia Pac J Public Health. (2017) 29(Suppl. 2):36–46S. doi: 10.1177/1010539516689695
2. Radiation Medical Science Center for the Fukushima Health Management Survey. Results of Mental Health and Lifestyle Survey for FY 2016 (Revised Version). (2018). Available online at: http://fmu-global.jp/download/results-of-mental-health-and-lifestyle-survey-for-fy-2016-revised-version/?wpdmdl=4454 (accessed April 26, 2020).
3. Japan Ministry of Health, Labour and Welfare. The Number of Suicides Relating to Great East Japan Earthquake 2019. (2019). Available online at: https://www.mhlw.go.jp/content/201902-shinsai.pdf (accessed April 26, 2020).
4. Ohto H, Yasumura S, Maeda M, Kainuma H, Fujimori K, Nollet KE. From devastation to recovery and revival in the aftermath of Fukushima's nuclear power plants accident. Asia Pac J Public Health. (2017) 29(Suppl. 2):10–17S. doi: 10.1177/1010539516675700
5. Chrisman AK, Dougherty JG. Mass trauma. Child Adolesc Psychiatr Clin N Am. (2014) 23:257–79. doi: 10.1016/j.chc.2013.12.004
6. Irmansyah I, Dharmono S, Maramis A, Minas H. Determinants of psychological morbidity in survivors of the earthquake and tsunami in Aceh and Nias. Int J Ment Health Syst. (2010) 4:8. 4:8. doi: 10.1186/1752-4458-4-8
7. Ying L, Wu X, Lin C, Jiang L. Traumatic severity and trait resilience as predictors of posttraumatic stress disorder and depressive symptoms among adolescent survivors of the Wenchuan earthquake. PLoS ONE. (2014) 9:e89401. doi: 10.1371/journal.pone.0089401
8. Blanc J, Rahill GJ, Laconi S, Mouchenik Y. Religious beliefs, PTSD, depression and resilience in survivors of the 2010. Haiti earthquake. J Affect Disord. (2016) 190:697–703. 190:697–703. doi: 10.1016/j.jad.2015.10.046
9. McCanlies EC, Mnatsakanova A, Andrew ME, Burchfiel CM, Violanti JM. Positive psychological factors are associated with lower PTSD symptoms among police officers: post hurricane katrina. Stress Health J Int Soc Investig Stress. (2014) 30:405–15. doi: 10.1002/smi.2615
10. Osofsky HJ, Osofsky JD, Hansel TC. Deepwater horizon oil spill: mental health effects on residents in heavily affected areas. Disaster Med Public Health Prep. (2011) 5:280–6. 5:280–6. doi: 10.1001/dmp.2011.85
11. Nishi D, Kawashima Y, Noguchi H, Usuki M, Yamashita A, Koido Y, et al. Resilience, post-traumatic growth, and work engagement among health care professionals after the Great East Japan earthquake: a 4-year prospective follow-up study. J Occup Health. (2016) 58:347–53. 58:347–53. doi: 10.1539/joh.16-0002-OA
12. Noda Y, Asano K, Shimizu E, Hirano Y. Assessing subgroup differences in posttraumatic stress disorder among rescue workers in japan with the impact of event scale-revised. Disaster Med Public Health Prep. (2018) 27:1–10. doi: 10.1017/dmp.2018.62
13. Okuyama J, Funakoshi S, Tomita H, Yamaguchi T, Matsuoka H. Longitudinal characteristics of resilience among adolescents: a high school student cohort study to assess the psychological impact of the Great East Japan Earthquake: youth resilience affected by disaster. Psychiatry Clin Neurosci. (2018) 72:821–35. doi: 10.1111/pcn.12772
14. Kukihara H, Yamawaki N, Uchiyama K, Arai S, Horikawa E. Trauma, depression, and resilience of earthquake/tsunami/nuclear disaster survivors of Hirono, Fukushima, Japan. Psychiatry Clin Neurosci. (2014) 68:524–33. doi: 10.1111/pcn.12159
15. Orui M, Nakajima S, Takebayashi Y, Ito A, Momoi M, Maeda M, et al. Mental health recovery of evacuees and residents from the Fukushima Daiichi nuclear power plant accident after seven years-contribution of social network and a desirable lifestyle. Int J Environ Res Public Health. (2018) 15:2381. 15:2381. doi: 10.3390/ijerph15112381
16. Connor KM, Davidson JRT. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. (2003) 18:76–82. 18:76–82. doi: 10.1002/da.10113
17. Nakamura Y, Umebayashi A, Takino Y. Resilience research trends in Japan by developmental stage: from ihfancy to adolescence. Res Sch Crisis Ment Care. (2010) 2:35–46.
18. Rutter M. Resilience in the face of adversity. Protective factors and resistance to psychiatric disorder. Br J Psychiatry. (1985) 147:598–611. 147:598–611. doi: 10.1192/bjp.147.6.598
20. Nakajima S, Kim Y, Takako K, Masaya I, Shirai A. Reliability and validity of Japanese version Conner-Davidson Resilience Scale. (Annual Report of Ministry of Health, Labour and Welfare funded research 2010. 大模害や犯罪被害等による精神科疾患の把握と介入手法のにする研究) (2010). p. 93–7.
21. Sakurai K, Nishi A, Kondo K, Yanagida K, Kawakami N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan: screening performance of K6/K10. Psychiatry Clin Neurosci. (2011) 65:434–41. 65:434–41. doi: 10.1111/j.1440-1819.2011.02236.x
22. Kessler RC, Barker PR, Colpe LJ, Epstein JF, Gfroerer JC, Hiripi E, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry. (2003) 60:184–9. 60:184–9. doi: 10.1001/archpsyc.60.2.184
23. Furukawa TA, Kawakami N, Saitoh M, Ono Y, Nakane Y, Nakamura Y, et al. The performance of the Japanese version of the K6 and K10 in the world mental health survey Japan. Int J Methods Psychiatr Res. (2008) 17:152–8. doi: 10.1002/mpr.257
24. Whitehead K, Dorstyn D, Ward L. Psychological adjustment in families affected by autism spectrum disorder. J Dev Phys Disabil. (2015) 27:703–17. 27:703–17. doi: 10.1007/s10882-015-9446-0
25. Tang B, Liu X, Liu Y, Xue C, Zhang L. A meta-analysis of risk factors for depression in adults and children after natural disasters. BMC Public Health. (2014) 14:623. 14:623. doi: 10.1186/1471-2458-14-623
26. Oe M, Maeda M, Nagai M, Yasumura S, Yabe H, Suzuki Y, et al. Predictors of severe psychological distress trajectory after nuclear disaster: evidence from the Fukushima health management survey. BMJ Open. (2016) 6:e013400. doi: 10.1136/bmjopen-2016-013400
Keywords: community survey, depression, Fukushima nuclear disaster, mental health, psychological resilience
Citation: Takebayashi Y, Maeda M, Orui M, Nakajima S, Momoi M, Ito A, Sato H, Yasumura S and Ohto H (2020) Resilience Factors Contributing to Mental Health Among People Affected by the Fukushima Disaster: Development of Fukushima Resilience Scale. Front. Public Health 8:159. doi: 10.3389/fpubh.2020.00159
Received: 18 February 2020; Accepted: 14 April 2020;
Published: 06 May 2020.
Edited by:
Karsten Heekeren, University of Zurich, SwitzerlandReviewed by:
Sae Ochi, Jikei University School of Medicine, JapanMasanori Nagamine, National Defense Medical College Research Institute, Japan
Copyright © 2020 Takebayashi, Maeda, Orui, Nakajima, Momoi, Ito, Sato, Yasumura and Ohto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Masaharu Maeda, bWFzYWdlbkBmbXUuYWMuanA=