 Laura Lauwers
Laura Lauwers Hilde Bastiaens1
Hilde Bastiaens1 Roy Remmen
Roy Remmen- 1Department for Interdisciplinary and Primary Care, University of Antwerp, Wilrijk, Belgium
- 2Research Institute Nature & Forest (INBO), Belgian Biodiversity Platform, Brussels, Belgium
Nature's contributions to human health (NCH) have gained increased attention internationally in scientific and policy arenas. However, little attention is given to the role of the health care sector in this discussion. Primary health care (PHC) is a vital backbone for linking knowledge and practice within the organization of health care. The objective of this scoping review is to evaluate how international overview reports and scientific literature on NCH address to PHC. More specifically, we extracted data on arguments, practice supporting tools and guidelines, challenges and constraints, and management approaches to integrate NCH and PHC. The scientific literature search was run in Web of Science. Two independent reviewers screened the scientific publications. Through the scientific literature search, we identified 1,995 articles of which 79 were eligible for analysis. We complemented the search with a selection of six international overview reports. Both the international overview reports and the scientific publications paid limited attention to the role of PHC regarding NCH. To cope with the current challenges and constraints to integrate NCH and PHC, more evidence on NCH, further development of PHC practice supporting tools, bottom–up integrated approaches, and closer interdisciplinary collaborations are required.
Introduction
Nature is known to affect human health in different ways. The manner in which nature's contributions to human health (NCH) have been studied reflects the changes in concepts of health. Health has long been defined as “the absence of disease” and approached by focusing on the pathogenesis or mechanisms that cause diseases (1). In this context, nature is simultaneously considered a threat to health due to the cause of diseases associated with mass mortalities and a source for curative care through the provision of medicinal compounds. In 1978, the World Health Organization (WHO) redefined the concept of health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” in the Alma-Ata Declaration (1). This change of health concept illustrates the shift in mainly focusing on disease-causing factors to considering factors supporting human health and well-being. In this context, only recently, more attention is paid to the benefits of nature contact to human health. The range of mechanisms, from supporting physical activity to enhancing immune function, and effects of nature contact to human health, from improved mental health to reduced diabetes, were recently reviewed (2).
This shift from emphasizing health risks to including health benefits from nature is reflected in international overview reports of interdisciplinary collaborations on NCH. In 2005, the WHO contributed to the Millennium Ecosystem Assessment (MEA) with a state-of-the-art overview of the broad range of NCH (3). In this overview, the relation between human health and an ecosystem approach of nature is addressed. The review focuses on the risks of the degradation of ecosystems to human health, such as natural disasters and malnutrition. In 2010, the United Nations Food and Agriculture Organization (FAO), the World Organization for Animal Health (OIE), and the WHO produced a collaborative statement on One Health (4). This collaboration aimed at sharing responsibilities and coordinating global activities to address health risks at the animal–human–ecosystems interfaces (4). In parallel, Wildlife Trust and the Consortium for Conservation Medicine joined the EcoHealth Alliance, an international nonprofit organization dedicated to a “One Health” approach to protecting the health of people, animals, and the environment from emerging infectious diseases (5). In 2015, the initial steps in the collaboration between WHO and the Convention on Biological Diversity (CBD) regarding biodiversity and health began (6). The state of knowledge review resulting from this collaboration includes health benefits of nature in terms of biodiversity. In this period, the Rockefeller Foundation–Lancet Commission on planetary health introduces the concept of planetary health as an alternative to One Health and EcoHealth (5). The commission defined this planetary health as “the achievement of the highest attainable standard of health, well-being, and equity worldwide through judicious attention to the human systems—political, economic, and social—that shape the future of humanity and the Earth's natural systems that define the safe environmental limits within which humanity can flourish” (5). In 2016, the European OneHealth/EcoHealth (OH/EH) workshop aimed at integrating these concepts given the similarities in their objectives (7). Here again, the benefits of nature to human health are included in the final report. In the same period, the European Union itself published a recent report on nature-based solutions (NBS) and renaturing cities from a European expert group commissioned by the Directorate-General for Research and Innovation (8). In this report, the potential human health benefits of NBS are explicitly addressed, as are in research calls related to that report. However, despite growing interest from scientific and policy arenas for NCH, the role of the health care sector, and more specifically the role of PHC in relation to NCH, has not been thoroughly reviewed.
The integration of NCH and PHC fits well in the initial WHO 1978 vision of PHC as to be comprehensive (1). Comprehensive PHC encourages to improve social and environmental contexts that create disease and risks for disease and pays attention to disease prevention and health promotion (9). Due to pragmatic reasons, a more selective approach with marginalized attention for preventive and promotive actions took over this comprehensive vision, especially in low- and mid-income countries (9). However, today, there is an increased demand to close the gap between PHC and Public Health by strengthening the preventive and promotive character of PHC (10). The role of PHC has become strategically important for several reasons. PHC is the first level of contact of individuals, the family, and community with the national health system (1). Its coordinating role helps people to navigate the maze of health services and to mobilize the support of other facilities by referring patients or calling on the support of specialized services (11). A further asset is the close link between health care practice and local communities, which potentially makes it an ideal sector for implementing and communicating scientific findings of NCH research (1). Additionally, PHC plays an important role in coaching and medical follow-up for patients with chronic diseases, and therefore lowering the threshold for nature-based interventions among that vulnerable group. Thus, it is important to look at NCH in relation to PHC, and as a first step, we examined what has already been published. The objective of this scoping review is to evaluate how international overview reports and scientific literature on NCH address to PHC. To scope the available knowledge, the following research question was developed: What does the literature mention on the integration of NCH and PHC? To do so, this scoping review summarizes the literature into four themes: arguments, practice supporting tools and guidelines, challenges and constraints, and management approaches characterizing the integration of NCH and PHC.
Methods
Definitions
Nature-based care: we developed this umbrella term for health care interventions related to nature, such as green prescriptions, nature-based health interventions, nature-assisted therapies, and green care.
Green Prescription: a physical activity scripting scheme (written and verbal) whereby patients are initially screened for physical inactivity and receive a physical activity prescription from their GP (12).
Nature-based health intervention: a program, activity, or strategy that aims to engage people in nature-based experiences with the specific goal of achieving improved health and well-being (13).
Nature-assisted therapy: an intervention with the aim to treat, hasten recovery, and/or rehabilitate patients with a disease or a condition of ill health, with the fundamental principle that the therapy involves plants, natural materials, and/or outdoor environment, without any therapeutic involvement of extra human mammals or other living creatures (14, 15).
Green care: another umbrella term for denoting interventions that use elements of nature and defined as a targeted therapeutic or treatment intervention that is specifically designed for people with a defined need and is delivered by trained/qualified practitioners. However, this term has very broad implications, also including social rehabilitation or health promotion, and also contains animal-assisted therapy (14, 15).
Complementary medicine or alternative medicine: a broad set of health care practices that are not part of a country's own tradition or conventional medicine and are not fully integrated into the dominant health-care system (16).
Protocol
A full review protocol was drafted a priori by the research team (LL, HK, RR, and HB), and is available in JMIR protocols (https://www.researchprotocols.org/2019/1/e12510/) (17). A summary of the methodology follows.
Search Criteria
We used a two-step approach to explore the domain of NCH in relation to PHC. First, we searched the gray literature for recent international overview reports on NCH. We complemented this by a scientific literature search in Web of Science (WOS). With the help of PHC professionals and the application of PubMed Search Builder, we developed a search string for PHC. This search string was combined with search strings for nature and the nature–health subthemes presented in the WHO-CBD report: human microbiome, infectious diseases, natural disasters, medicinal plants, and nutrition (6). These search strings were adopted from the search strategy for the Regional Assessment for Europa and Central Asia by the Intergovernmental Platform on Biodiversity and Ecosystem Services (IPBES) (18). We developed an additional subtheme “nature-based care” and considered it as an umbrella term for health care interventions related to nature. The diverse range of topics covered by those nature–health subthemes allowed to fully grasp the full potential connections between all aspects of NCH and PHC. The relevance of the subthemes and an overview of the search strings are presented in the published protocol (17). The search strings were combined as follows:
• Nature–health subtheme AND primary health care.
• Nature–health subtheme AND primary health care AND nature.
• Nature AND primary health care.
Inclusions and Exclusion Criteria
We considered all literature dating from 1900 to May 2017. We did not consider foreign language material, except for papers with an English abstract because of the cost and time involved for translation. Two independent reviewers (first reviewer: HK, second reviewer: HB or RR) checked the titles and abstracts of the search results for relevance. Relevance was attributed if the publications approached the nature–health subthemes in accordance to their relevance to health and if they paid attention to PHC in a nonsuperficial manner. Publications were included when explicitly relating the research findings on NCH to PHC, with references to PHC according to the keywords of the search string. Publications were excluded from further analysis when only mentioning PHC, but not linking the NCH knowledge to PHC. At title and abstract stage, for each publication, reviewers made one of following decisions: relevant, in doubt, or irrelevant. In the case of doubt or disagreement, the first reviewer made a final decision at the full paper stage in consultation with the second reviewer. As we were more interested to explore a broad range of topics related to NCH than to go into great detail on a specific topic, for pragmatic reasons, papers were only checked for relevance when the number of results of a combination of search strings was below 100. Reviews were always considered. The quality of the papers was not assessed. Figure 1 illustrates the selection process for the scientific literature. More details can be found in the published protocol (17).
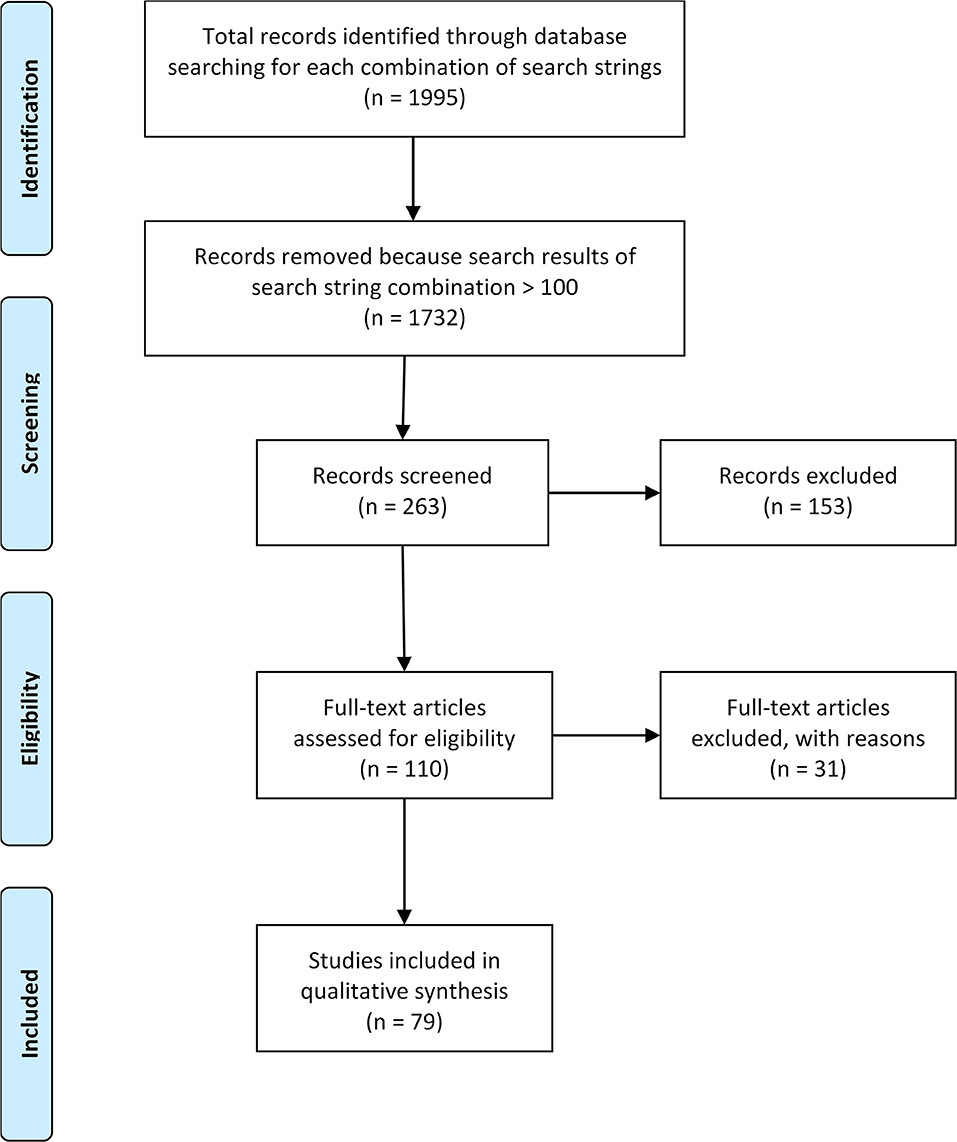
Figure 1. Prisma diagram of articles included in study.
Extraction of Data
For the international overview reports, we only screened and extracted data with keywords associated to PHC. Since the results were very limited, we screened and extracted additionally data containing the keywords “health care,” “healthcare,” and “health prof.”
For the scientific literature, we read the full article and extracted data following a list of extraction fields, including “year of publication,” “country of origin,” and key findings that relate to the research question: What does the literature mention on the integration of NCH and PHC?
Based on first insights in the data extracted in relation to our research question, we decided during the development of our protocol to sort all data under four main categories: (1) arguments, (2) practice supporting tools and guidelines, (3) challenges and constraints, and (4) management approaches characterizing the integration of NHI in PHC. This data extraction approach is akin to a “narrative review,” where we used the four categories as an analytical framework to all data extracted from the international overview reports and scientific literature (19). We sought to apply a uniform approach to all literature included in the review, but in practice it was sometimes impossible to extract information on all four categories where some literature failed to include relevant material. Since the spatial and temporal information of the scientific literature did not show remarkable trends in topical foci, we did not report on those results.
Results
Results From International Overview Reports
Six international overview reports on NCH were selected to complement the scientific literature (Table 1).
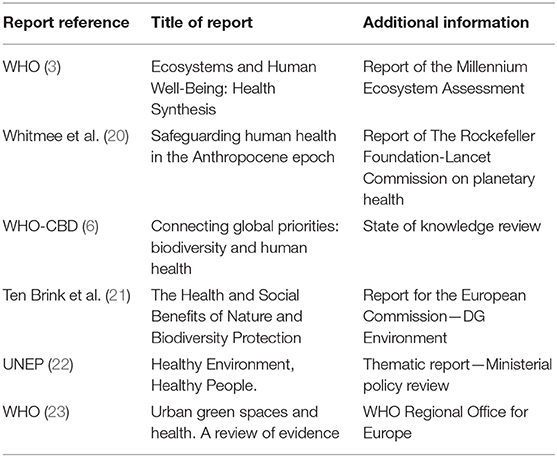
Table 1. Selected international overview reports.
The role of PHC remained mainly underreported in the selected international overview reports on NCH. The WHO contribution to the Millennium Ecosystem Assessment (3) and the UNEP report “Healthy Environment, Healthy People” (22) did not include key terms associated to PHC. Especially in the WHO–CBD review (6), attention to PHC became more specific. None of the reports referred to practice supporting tools or guidelines. Arguments, challenges and constraints, and management approaches to integrate NCH and PHC could be extracted from the reports (Supplementary Table 1).
Arguments
We derived several arguments from the reports to better integrate NCH and PHC. First of all, natural disasters already have a great impact on the (primary) health care costs and infrastructure (3, 6, 20). Contrary, (primary) health care itself has an impact on natural ecosystems that subsequently can have a negative effect on human health (6). Second, through the central role of PHC in communities, PHC possesses interesting health data that can be spatially linked to environmental data and strengthen the response and preparedness to health impacts of the environment (20, 23). This central role can further support health professionals to mobilize a wide community of actors to increase awareness for NCH (20, 21). Third, worldwide medicinal plant use continues to be an important part of (primary) health care systems where training local communities could help to protect biodiversity and local knowledge and to reduce poverty (3, 6). At last, evidence for the effectiveness and preventive potential of NCH is increasing and could reduce health care costs (21–23).
Challenges and Constraints
A big challenge is that poor populations are often more dependent on natural resources in their environment due to inadequate access to health care, but often live in areas that are becoming more prone to flooding or other natural disasters (20). Additionally, a minimum threshold of health-worker capacity is required to prevent and respond to the health consequences of environmental change (20). Besides the increase in health inequalities, the integration of NCH and PHC is constraint by the general trend of budget cuts in preventive care (21). This trend reflects the current challenge to increase awareness on the preventive functions of nature. Consequently, dedicated measures for awareness raising are required to facilitate the mainstreaming of NCH (21).
Management Approaches
From the extracted management approaches, we learn that an integration of PHC and NCH is required on different levels, involving different actors. First, knowing the reciprocal impact of the health care sector and the natural environment, the integration of NCH and PHC requires the integration of policies advancing both human health and environmental sustainability (20). Second, data integration should be obtained, for example, by including environmental metrics in facility and population-based health surveys (20). Third, interdisciplinary collaborations between health and environmental actors are required and could be stimulated by the local authorities through collaboration calls or collaboration platforms (20–22). Fourth, the integration of NCH and PHC can be further enabled by providing trainings: trainings to local community members to protect their natural resources, to researchers to gain skills in producing and commercializing traditional medicines, and to health professionals in understanding and applying concepts and practices of NCH (6, 20, 21). Regarding medicinal plant research, the reports emphasize the importance of respecting local health culture and knowledge, for example, by informing the local community on the research project or by developing memoranda of understanding between researchers and traditional healers (6, 20). Fifth, NCH and PHC could be spatially integrated by establishing medicinal plant conservation areas, planning green space for health, recognizing nature areas as “preventive health care centers” or “health hubs,” financially supporting health care services to utilize urban green spaces, or incorporating green areas in health services. Health professionals can take an active role in this integration by joining environmental health research, writing green referrals, and using their central role to mobilize a wide community of actors (6, 20, 21). At last, the integration can be stimulated by copying good practices on small scales and applying them on a wider set of regions (6, 21).
Results From Scientific Literature
We identified 1,995 articles of which 79 (28 reviews, 51 papers) were eligible for analysis. Table 2 gives a quantitative overview of the search string combinations. The last column illustrates the total amount of reviews and papers included for a specific nature–health subtheme. Some articles were moved to the results of another subtheme if they fitted better content-wise. We did not identify relevant articles that fitted the nature–health subthemes “human microbiome” and “nutrition.”
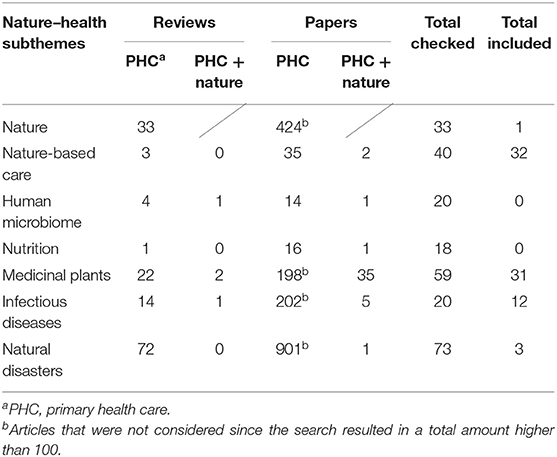
Table 2. Quantitative overview of the search string combinations applied in WOS.
The results of each search string combination with PHC that were considered relevant to our research question showed considerable differences in topical foci (Supplementary Table 2). The scientific literature allowed us to draw lessons on arguments, practice supporting tools and methods, challenges, constraints, and management approaches to integrate NCH and PHC.
Arguments
The arguments to integrate NCH and PHC relate strongly to the comprehensive vision of PHC by focusing on the potential for health promotion and disease prevention, both on individual and population level. Literature regarding “nature-based care” describes the potential of PHC in disease prevention on the individual level through health-promoting interventions, e.g., physical activity interventions, nature-based care, and complementary therapies. On a population level, this literature emphasizes the potential of PHC professionals to have a broad public health impact as they are considered highly credible resources for health information and are often visited on a regular basis by their patients (12, 24). Literature regarding “medicinal plants” describes the potential of PHC in disease prevention on the individual level through holistic care interventions, for example, Ayurveda complementary therapies. On a population level, this literature emphasizes that although interventions of conventional medicines dominate in the western countries, three quarters of the world population rely on herbal and traditional medicine as a basis for PHC because of its affordability, accessibility, and long cultural history (25–31). As traditional medicinal knowledge is disappearing, PHC has the potential to conserve and integrate this knowledge as a response to the growing demand for traditional healing, also in western countries (28, 32). Further, literature regarding both “nature-based care” and “medicinal plants” underlines a reduction in consumption and costs of PHC as a result of the preventive and therapeutic potential of the presented interventions (29, 33–37). Literature regarding “infectious diseases” and “natural disasters” describes the potential of PHC in disease control and prevention only on the population level through early interventions during the detection and treatment of diseases (38–40).
Practice Supporting Tools and Guidelines
Only two articles of the included literature provide tools to support PHC workers that directly relate to NCH. One article within the subtheme “infectious diseases” introduces a pathogen source questionnaire to gain insights in the zoonotic contact of the patient (41). The other article within “natural disasters” considers two summarized checklists, one for the early warning system, as well as when doing post-disaster risk assessment, and the other for prevention and control of recorded diseases (38). Two articles within “natural disasters” provide useful traumatic screening instruments, but mentioned “natural disasters” only once as an example of possible trauma exposures (42, 43). Although not published as a guideline, one article on “natural disasters” reviews all skin diseases related to floods and summarized the appropriate management or treatment (39). “Nature-based care” literature discusses specific trainings to support the PHC professional in writing green prescriptions (34, 44–46). To give written advice to a patient to be physically active, PHC trainings on motivational interviewing techniques and behavioral counseling strategies are recommended (34, 45, 47). However, again these articles lack references to specific practice supporting guidelines and refer mostly to physical activity in general without giving attention to the natural component (12, 24).
Challenges and Constraints
Literature concerning “nature-based care” and “medicinal plants” assigns the difficulty to integrate NCH and PHC to a general lack of collaboration and communication between different areas of knowledge (48–50). Where ethnobotanical research is predominated by descriptive works of useful plants, the translation of this traditional knowledge into PHC practice requires more interchange of theories and methods among related disciplines, like ethnopharmacology (48). Furthermore, the development of wide-scoped interdisciplinary projects that recognize intellectual property rights and reward the communities for their knowledge contribution are needed to counteract the disappearance of traditional medicinal knowledge, opposing the growing demand for traditional healing (48, 49). Articles about “nature-based care” provide several reasons to explain why the green prescribing practice remains low despite the growing evidence on the health benefits of green space (50). First of all, this interdisciplinary field requires the development of a consistent terminology to support a better collaboration. Besides a need for interdisciplinary collaboration, a behavioral change is required both from the patient and the PHC professional as the new approaches extend the traditional biomedical model (24, 34, 45, 46). However, the lack of resources and time in the PHC sector greatly challenge the practical trainings and substantial support from the physician toward the patient required for these behavioral changes to succeed (24, 34, 46). At last, where strong evidence is needed to convince PHC professionals of a certain practice, there is little academic interest in the field, for example, for phytotherapy, or the type of evidence cannot compete with evidence base using methodologies like randomized controlled trials (RCTs) (36, 50). The type of evidence used to indicate the effects of an intervention is mostly based on subjective measures, like self-reported health status (51–53). The latter is also reflected in the literature on “medicinal plants,” where the evidence for the healing effects of medicinal plants is often limited to the traditional, and, to a certain extent, subjective use of plants by local communities (26).
Management Approaches
The paragraphs below illustrate that the integration of NCH and PHC should preferably be done in a bottom–up manner and that horizontal networks among PHC practices and community-based facilities should be stimulated. Articles addressing “medicinal plants” emphasize the importance of community participation in studies on traditional knowledge acquisition. These articles tell us that local communities and local stakeholders are willing to contribute to scientific research and participate in the conservation of medicinal plants and the associated knowledge, but that the state health care negatively influences traditional-based healing practices by promoting allopathic health care (28, 49, 54). Literature regarding "infectious diseases” discusses community participation in relation to successful disease control (55–59). Decentralized or inadequate public health infrastructure, shortage of financial resources, and human resistance to programs emerge as reasons for failures of vertical health projects and a shift to community-oriented PHC systems in many countries (55–59). To engage community members in public health programs, community participants should define their idea of “participation” and what they perceive as their “communities” (36). For “nature-based care,” literature discusses community involvement in PHC mainly in relation to physical activity programs (24, 34, 45, 46, 58, 59). These studies show that giving advice only to increase physical activity through green prescriptions is not as effective as tailored interventions involving a personalized action plan supported by a strong network between PHC and sport or other facilities in the community (24, 46, 58). Such a network builds the opportunity to share the load of intervention activities, as PHC professionals are limited by consultation time (24, 34). These communal facilities can help in motivating and monitoring the patients in the performance of their physical activities or in providing opportunities for health promotion in general, e.g., the provision of community vegetable gardens or health education activities (24, 34, 45, 46, 58–61).
Discussion
This review aimed to get an overview of the state of the art of NCH in relation to PHC. To this end, this review indicates that a potential role for PHC in NCH is perhaps not fully recognized. The role of PHC was most clearly defined in the literature on “nature-based care” in terms of disease prevention and health promotion through the application of green prescriptions, and in the literature on “medicinal plants” in terms of curative care through the application of knowledge on traditional medicine. Additionally, the international overview reports highlighted the potential role of PHC professionals in mobilizing a wide community and contributing to environmental health research. However, the included literature did not cover specific tools to support PHC practices. PHC practice- supporting tools and guidelines were in general limited and very context-specific. The given tools and guidelines were based on an overall recognition of the importance of “context” to integrate NCH and PHC. Not only increased attention to the patient's history and background but also to the context of the PHC professional and of the health issue itself was mentioned by the included literature. The limited number of tools and guidelines presented in the included literature might on one hand be associated with the underrecognition of evidence on NCH by health professionals, since the available data deviates from the strict criteria for RCTs (50). On the other hand, some research fields within NHC are quite recent, such as the contribution of microbial diversity in the natural environment to immune function. Despite a lack of practice supporting tools and guidelines, the review covered a wide range of arguments to integrate NCH and PHC. Most arguments related to the economic costs of PHC, the preventive potential of NCH, and the need to protect our natural health resources. However, this integration is not without challenges and constraints. The included literature highlighted the need to tackle health inequalities related to poverty, to better inform on NCH among PHC professionals, to improve interdisciplinary collaborations, and to provide PHC practices with the necessary resources. Finally, the scientific literature and international overview reports emphasized the need for integrated, bottom–up approaches to successfully link NCH and PHC. Regarding these management approaches, the included literature highlighted the importance of respecting local environmental and health knowledge, linking environmental and health data collection, and a better coordination of environmental and health policies. However, at present, policy makers seem to struggle to scale up these integration models, while at the same time responding to local conditions and needs of the community (62).
The findings of this review should be viewed in light of limitations in our method. The main limitation of the review is the lack of capacity for a content analysis when the number of the results crossed the self-determined threshold of 100. This implies that the included literature does not fully cover the quantitative presence of certain topics in the scientific literature.
By linking to PHC, this review adds priorities to the research agenda published by Frumkin et al. to guide future studies on NCH (63). Overall, knowledge on NCH in PHC and the role for PHC regarding the application of that knowledge in health care practice remains in its infancy in both science and practice. Based on this research, we suggest that research priority should be given to real-time examples of practice with the assessment of the process and time- and cost-effectiveness to identify best practices. Based upon this research, necessary tools and guidelines to support the integration of NCH and PHC could be developed. The growing interest for green prescriptions opens research opportunities to investigate benefits of nature on health in a PHC setting. As the included literature is mostly restricted to physical activity in general without mentioning the benefits related to physical activity in a natural setting, for example, the improvement in mental well-being or immune function, it would be interesting to further investigate the added value of a natural environment for physical activities and how the patient can be stimulated through a community-based referral network to visit natural environments for physical activities (64–66). Regarding medicinal plants, this review provides an overview of scientific literature that can serve as a starting point to develop management plans urgently needed to conserve the medicinal resources and the associated traditional knowledge. The literature on infectious diseases relates to the One Health approach by emphasizing the necessity to further investigate ways to strengthen the collaboration between environmental, human, and animal health care sectors for disease control and prevention, with PHC being an ideal setting to converge those disciplines (20). The unpredictable outcomes of natural disasters might challenge the reporting of NCH in the context of such events; however, with the growing climate threat, these reports become highly important to mobilize PHC in an efficient manner.
PHC provides a relevant and valuable evaluation testing ground for studies on the integration of NCH in health care practices. PHC can report back to research, as it is close to community health developments, and as such delivers important data to science and policy. Further, it focuses on reducing health inequalities in communities (67). To conclude, this review provides a broad overview of the potential of integrating NCH and PHC and calls for a better uptake of this potential in future scientific studies and international policy directives on NCH.
Data Availability Statement
All data generated or analyzed during this study are included in this published article and in the published protocol of this article (17).
Author Contributions
HK, RR, and HB conceptualized the review and involved in the selection of relevant scientific literature. HK developed the search strategy with guidance from Conor Kretsch (COHAB) and Bram Oosterbroek (ICIS-University of Maastricht). LL analyzed the literature and wrote the manuscript of the review with critical inputs and appraisal from HK, RR, and HB. All authors have read and approved the manuscript.
Funding
This study results from the project Green light (in Dutch: Licht op Groen), hosted by the University of Antwerp and funded by the Province of Antwerp in Belgium.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors express gratitude to Conor Kretsch (COHAB Initiative, Co-Operation On Health and Biodiversity) and Bram Oosterbroek [International Centre for Integrated Assessment and Sustainable Development (ICIS)-University of Maastricht] who have closely collaborated with the colead author, HK, of this paper in adapting and applying the literature search strings in the context of the nature–health-related sections of the IPBES Assessment Report on Biodiversity and Ecosystem Services for Europe and Central Asia 2018. The authors greatly acknowledge Carolyn Daher who proofread the manuscript for language-related errors and gave critical inputs.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2020.00052/full#supplementary-material
References
1. WHO. Declaration of Alma-Ata. Alma-Ata: the International Conference on Primary Health Care. USSR: Alma-Ata (1978).
2. Hartig T, Mitchell R, de Vries S, Frumkin H. Nature and health. Annu Rev Public Health. (2014) 35:207–28. doi: 10.1146/annurev-publhealth-032013-182443
3. WHO. Ecosystems and Human Well-Being: Health Synthesis. A Report of the Millennium Ecosystem Assessment. Geneva: WHO (2005).
4. FAO - OIE - WHO. Sharing Responsibilities and Coordinating Global Activities to Address Health Risks at the Animal-Human- Ecosystems Interfaces. Hanoi: A Tripartite Concept Note (2010).
5. Lerner H, Berg C. A comparison of three holistic approaches to health: one health, EcoHealth, and planetary health. Front Vet Sci. (2017) 4:163. doi: 10.3389/fvets.2017.00163
6. WHO - CBD. Connecting Global Priorities: Biodiversity and Human Health: A State of Knowledge review. Geneva: WHO (2015).
7. Keune H, Flandroy L, Thys S, De Regge N, Mori M, Antoine-Moussiaux N, et al. The need for European OneHealth/EcoHealth networks. Arch Public Health. (2017) 75:64. doi: 10.1186/s13690-017-0232-6
8. European Commision. Towards an EU Research and Innovation Policy Agenda for Nature-Based Solutions & Re-Naturing Cities. Final Report of the Horizon 2020 Expert Group on 'Nature-Based Solutions and Re-Naturing Cities'. Brussels: Directorate-General for Research and Innovation (2015).
9. Baum F, Freeman T, Lawless A, Labonte R, Sanders D. What is the difference between comprehensive and selective primary health care? Evidence from a five-year longitudinal realist case study in South Australia. BMJ Open. (2017) 7:e015271. doi: 10.1136/bmjopen-2016-015271
10. WHO. Technical Series on Primary Health Care. Primary Health Care: Closing the Gap Between Public Health and Primary Care Through Integration. Astana: WHO (2018).
12. Croteau K, Schofield G, McLean G. Physical activity advice in the primary care setting: results of a population study in New Zealand. Aust N Z J Public Health. (2006) 30:262–7. doi: 10.1111/j.1467-842X.2006.tb00868.x
13. Shanahan DF, Astell-Burt T, Barber EA, Brymer E, Cox DTC, Dean J, et al. Nature-based interventions for improving health and wellbeing: the purpose, the people and the outcomes. Sports. (2019) 7:141. doi: 10.3390/sports7060141
14. Howarth M, Brettle A, Hardman M, Maden M. What Evidence is There to Support the Impact of Gardens on Health Outcomes? A Systematic Scoping Review of the Evidence. Project Report. Salford: Centre for Applied Research in Health, Welfare and Policy (2017).
15. Annerstedt M, Währborg P. Nature-assisted therapy: Systematic review of controlled and observational studies. Scand J Public Health. (2011) 39:371–88. doi: 10.1177/1403494810396400
16. WHO. Enhancing the Role of Traditional Medicine in Health Systems: A Strategy for the African Region (AFR/ RC63/6): 63rd Session of the Regional Committee for Africa. Brazzaville: WHO Regional Office for Africa (2013).
17. Lauwers L, Bastiaens H, Remmen R, Keune H. The integration of interlinkages between nature and human health in primary health care: protocol for a scoping review. JMIR Res Protoc. (2019) 8:e12510. doi: 10.2196/12510
18. Fischer M RM, Torre-Marin, Rando A, Mader A, Church A, Elbakidze M, et al. Summary for Policymakers of the Regional Assessment Report on Biodiversity and Ecosystem Services for Europe and Central Asia of the Intergovernmental Science-Policy Platform on Biodiversity and Ecosystem Services. Bonn: IPBES secretariat (2018).
19. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
20. Whitmee S, Haines A, Beyrer C, Boltz F, Capon AG, de Souza Dias BF, et al. Safeguarding human health in the Anthropocene epoch: report of The Rockefeller Foundation-Lancet Commission on planetary health. Lancet. (2015) 386:1973–2028. doi: 10.1016/S0140-6736(15)60901-1
21. Ten Brink P, Mutafoglu K, Schweitzer J-P, Kettunen M, Twigger-Ross C, Baker J, et al. The Health and Social Benefits of Nature and Biodiversity Protection. London/Brussels: Report for the European Commission, Institute for European Environmental Policy (2016).
22. UNEP. Healthy Environment, Healthy People. Nairobi: Thematic report - Ministerial policy review session - Second session of the United Nations Environment Assembly of the United Nations Environment Programme (2016).
23. WHO. Urban Green Spaces and Health. A Review of Evidence. Copenhagen: WHO Regional Office for Europe (2016).
24. Estabrooks PA, Glasgow RE. Translating effective clinic-based physical activity interventions into practice. Am J Prev Med. (2006) 31:S45–56. doi: 10.1016/j.amepre.2006.06.019
25. Efferth T, Kaina B. Toxicities by herbal medicines with emphasis to traditional Chinese medicine. Curr Drug Metab. (2011) 12:989–96. doi: 10.2174/138920011798062328
26. de Boer HJ, Lamxay V, Bjork L. Comparing medicinal plant knowledge using similarity indices: a case of the Brou, Saek and Kry in Lao PDR. J Ethnopharmacol. (2012) 141:481–500. doi: 10.1016/j.jep.2012.03.017
27. Maroyi A. Traditional use of medicinal plants in south-central Zimbabwe: review and perspectives. J Ethnobiol Ethnomed. (2013) 9:31. doi: 10.1186/1746-4269-9-31
28. Mathibela MK, Egan BA, Du Plessis HJ, Potgieter MJ. Socio-cultural profile of Bapedi traditional healers as indigenous knowledge custodians and conservation partners in the Blouberg area, Limpopo Province, South Africa. J Ethnobiol Ethnomed. (2015) 11:49. doi: 10.1186/s13002-015-0025-3
29. Rasool S, Khan MH, Hamid S, Sultan PS, Qazi P, Butt T. An overview and economical importance of few selected endangered medicinal plants grown in Jammu and Kashmir region of India. Ann Phytomed. (2016) 5:27–37. doi: 10.21276/ap.2016.5.2.3
30. Shil S, Dutta Choudhury M, Das S. Indigenous knowledge of medicinal plants used by the Reang tribe of Tripura state of India. J Ethnopharmacol. (2014) 152:135–41. doi: 10.1016/j.jep.2013.12.037
31. Vandebroek I, Van Damme P, Van Puyvelde L, Arrazola S, De Kimpe N. A comparison of traditional healers' medicinal plant knowledge in the Bolivian Andes and Amazon. Soc Sci Med. (2004) 59:837–49. doi: 10.1016/j.socscimed.2003.11.030
32. Schveitzer MC, Zoboli EL. Role of complementary therapies in the understanding of primary healthcare professionals: a systematic review. Rev Escola Enfermagem USP. (2014) 48:184–91. doi: 10.1590/S0080-623420140000500026
33. Dalziel K, Segal L, Elley CR. Cost utility analysis of physical activity counselling in general practice. Aust N Z J Public Health. (2006) 30:57–63. doi: 10.1111/j.1467-842X.2006.tb00087.x
34. Lobelo F, Stoutenberg M, Hutber A. The exercise is medicine global health initiative: a 2014 update. Br J Sports Med. (2014) 48:1627–33. doi: 10.1136/bjsports-2013-093080
35. Wahrborg P, Petersson IF, Grahn P. Nature-assisted rehabilitation for reactions to severe stress and/or depression in a rehabilitation garden: long-term follow-up including comparisons with a matched population-based reference cohort. J Rehabil Med. (2014) 46:271–6. doi: 10.2340/16501977-1259
36. Antonio GD, Tesser CD, Moretti-Pires RO. Phytotherapy in primary health care. Rev Saude Public. (2014) 48:541–53. doi: 10.1590/S0102-311X2007000600021
37. Hossen MJ, Uddin MB, Uddin Ahmed SS, Yu ZL, Cho JY. Traditional medicine/plants for the treatment of reproductive disorders in Asia Nations. Pak Vet J. (2016) 36:127–33.
38. Kouadio IK, Aljunid S, Kamigaki T, Hammad K, Oshitani H. Infectious diseases following natural disasters: prevention and control measures. Exp Rev Anti Infect Ther. (2012) 10:95–104. doi: 10.1586/eri.11.155
39. Tempark T, Lueangarun S, Chatproedprai S, Wananukul S. Flood-related skin diseases: a literature review. Int J Dermatol. (2013) 52:1168–76. doi: 10.1111/ijd.12064
40. Haider Z, Ahmad FZ, Mahmood A, Waseem T, Shafiq I, Raza T, et al. Dengue fever in Pakistan: a paradigm shift; changing epidemiology and clinical patterns. Perspect Public Health. (2015) 135:294–8. doi: 10.1177/1757913915599019
41. Warwick C. Gastrointestinal disorders: are health care professionals missing zoonotic causes? J R Soc Promot Health. (2004) 124:137–42. doi: 10.1177/146642400412400316
42. Crosby SS. Primary care management of non-English-speaking refugees who have experienced trauma: a clinical review. JAMA. (2013) 310:519–28. doi: 10.1001/jama.2013.8788
43. Spoont MR, Williams JW, Jr, Kehle-Forbes S, Nieuwsma JA, Mann-Wrobel MC, et al. Does this patient have posttraumatic stress disorder? Rational clinical examination systematic review. JAMA. (2015) 314:501–10. doi: 10.1001/jama.2015.7877
44. Swinburn BA, Walter LG, Arroll B, Tilyard MW, Russell DG. Green prescriptions: attitudes and perceptions of general practitioners towards prescribing exercise. Br J Gen Pract. (1997) 47:567–9.
45. Elley CR, Kerse N, Arroll B, Robinson E. Effectiveness of counselling patients on physical activity in general practice: cluster randomised controlled trial. BMJ. (2003) 326:793. doi: 10.1136/bmj.326.7393.793
46. Huijg JM, Gebhardt WA, Verheijden MW, et al. Factors influencing primary health care professionals' physical activity promotion behaviors: a systematic review. Int J Behav Med. (2014) 22:32–50. doi: 10.1007/s12529-014-9398-2
47. Anderson YC, Taylor GM, Grant CC, Fulton RB, Hofman PL. The green prescription active families programme in Taranaki, New Zealand 2007-2009: Did it reach children in need? JPHC. (2015) 7:192–7. 10.1071/HC15192 doi: 10.1071/HC15192
48. Bermúdez A, Oliveira-Miranda T, Velázquez D. Ethnobotanical research on medicinal plants: a review of its goals and current approaches. Interciencia. (2005) 30:453–515.
49. Bhattarai S, Chaudhary RP, Quave CL, Taylor RS. The use of medicinal plants in the trans-himalayan arid zone of Mustang district, Nepal. J Ethnobiol Ethnomed. (2010) 6:14. doi: 10.1186/1746-4269-6-14
50. Van den Berg AE. From green space to green prescriptions: challenges and opportunities for research and practice. Front Psychol. (2017) 8:268. doi: 10.3389/fpsyg.2017.00268
51. Korpela KM, Ylen M, Tyrvainen L, Silvennoinen H. Determinants of restorative experiences in everyday favorite places. Health Place. (2008) 14:636–52. doi: 10.1016/j.healthplace.2007.10.008
52. Barley EA, Robinson S, Sikorski J. Primary-care based participatory rehabilitation: users' views of a horticultural and arts project. Br J Gen Pract. (2012) 62:e127–34. doi: 10.3399/bjgp12X625193
53. Arsenijevic J, Groot W. Physical activity on prescription schemes (PARS): do programme characteristics influence effectiveness? Results of a systematic review and meta-analyses. MJ Open. (2017) 7:e012156. doi: 10.1136/bmjopen-2016-012156
54. Panyaphu K, On TV, Sirisa-ard P, Srisa-nga P, ChansaKaow S, Nathakarnkitkul S. Medicinal plants of the Mien (Yao) in Northern Thailand and their potential value in the primary healthcare of postpartum women. J Ethnopharmacol. (2011) 135:226–37. doi: 10.1016/j.jep.2011.03.050
55. Lines J, Harpham T, Leake C, Schofield C. Trends, priorities and policy directions in the control of vector-borne diseases in urban environments. Health Policy Plan. (1994) 9:113–29. doi: 10.1093/heapol/9.2.113
56. Atkinson J-A, Vallely A, Fitzgerald L, Whittaker M, Tanner M. The architecture and effect of participation: a systematic review of community participation for communicable disease control and elimination. Implications for malaria elimination. Malar J. (2011) 10:225. doi: 10.1186/1475-2875-10-225
57. Corley AG, Thornton CP, Glass NE. The role of nurses and community health workers in confronting neglected tropical diseases in sub-Saharan Africa: A Systematic Review. PLOS Negl Trop Dis. (2016) 10:e0004914. doi: 10.1371/journal.pntd.0004914
58. Lamb SE, Bartlett HP, Ashley A, Bird W. Can lay-led walking programmes increase physical activity in middle aged adults? A randomised controlled trial. J Epidemiol Community Health. (2002) 56:246–52. doi: 10.1136/jech.56.4.246
59. Hamlin MJ, Yule E, Elliot CA, Stoner L, Kathiravel Y. Long-term effectiveness of the New Zealand Green Prescription primary health care exercise initiative. Public Health. (2016) 140:102–8. doi: 10.1016/j.puhe.2016.07.014
60. Costa CG, Garcia MT, Ribeiro SM, Salandini MF, Bogus CM. Community vegetable gardens as a health promotion activity: an experience in Primary Healthcare Units. Ciencia Saude Coletiva. (2015) 20:3099–110. doi: 10.1590/1413-812320152010.00352015
61. Pereira BS, Silva KSS, de Souza RP. Citizens in the making: a contribution to children's environmental health education. Saude soc. (2009) 18:93–5. doi: 10.1590/S0104-12902009000600016
62. Dhondt S, Hermans K, Molema H, Boermans S, van der Klauw D, Vrijhoef HJ. Mechanisms of integrated care in Flanders: A bottom-up perspective. Int J Care Coord. (2017) 20:87–97. doi: 10.1177/2053434517734464
63. Frumkin H, Bratman GN, Breslow SJ, Cochran B, Kahn PH Jr, Lawler JJ, et al. Nature contact and human health: a Research Agenda. Environ Health Perspect. (2017) 125:075001. doi: 10.1289/EHP1663
64. Thompson Coon J, Boddy K, Stein K, Whear R, Barton J, Depledge MH. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ Sci Technol. (2011) 45:1761–72. doi: 10.1021/es102947t
65. York M, Wiseman T. Gardening as an occupation: a critical review. Br J Occup Ther. (2012) 75:76–84. doi: 10.4276/030802212X13286281651072
66. Steigen AM, Kogstad R, Hummelvoll JK. Green Care services in the Nordic countries: an integrative literature review. Eur J Soc Work. (2015) 19:692–715. doi: 10.1080/13691457.2015.1082983
Keywords: primary health care, nature, health, infectious diseases, natural disasters, medicinal plants, nature-based care
Citation: Lauwers L, Bastiaens H, Remmen R and Keune H (2020) Nature's Contributions to Human Health: A Missing Link to Primary Health Care? A Scoping Review of International Overview Reports and Scientific Evidence. Front. Public Health 8:52. doi: 10.3389/fpubh.2020.00052
Received: 20 August 2019; Accepted: 13 February 2020;
Published: 18 March 2020.
Edited by:
Craig Stephen, University of Saskatchewan, CanadaReviewed by:
Donald C. Cole, University of Toronto, CanadaErin Fraser, British Columbia Centre for Disease Control, Canada
Copyright © 2020 Lauwers, Bastiaens, Remmen and Keune. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura Lauwers, bGF1cmEubGF1d2Vyc0B1YW50d2VycGVuLmJl