 Iain Barton1*
Iain Barton1* Anton L. V. Avanceña
Anton L. V. Avanceña- 1Imperial Logistics, Germiston, South Africa
- 2Department of Health Management and Policy, School of Public Health, University of Michigan, Ann Arbor, MI, United States
- 3Stephen M. Ross School of Business, University of Michigan, Ann Arbor, MI, United States
Many life-saving drugs are still inaccessible and unaffordable in low- and middle-income countries, particularly in Sub-Saharan Africa. This contributes to poor health outcomes, wider health and socioeconomic inequities, and higher patient spending on healthcare. While resource limitations facing national regulatory authorities (NRAs) contribute to the problem, we believe that (1) fragmented and complex drug regulations, (2) suboptimal enforcement of existing regulations, and (3) poorly designed disincentives for non-compliance play a larger role. These “unintended consequences” that are a direct result of our current regulatory regimes limit competition, keep drug costs high, and lead to shortages and the proliferation of illegitimate and unregistered drugs. While NRAs can gain a lot from increased investment in their work, regulatory harmonization and innovation can arrest and reverse the regulatory failures we still see today and improve medicine access in Africa. Unfortunately, harmonization initiatives in Sub-Saharan Africa have made modest impact and have done so slowly. We encourage greater attention and investment in harmonization and other downstream functions of NRAs. We also urge increased participation of national governments–particularly executive agencies in health and the treasury—and patient advocacy groups in advancing harmonization across the subcontinent.
Introduction
In most countries, a national regulatory agency (NRA) ensures that medicines are safe, effective, affordable, and are high-quality (1–4). NRAs develop and enforce pharmaceutical regulations that protect consumers who cannot judge on their own whether a drug is completely safe or authentic (4). Drug regulation also promotes health security and limits the rise of drug-resistant microbial diseases by ensuring that medicines have the correct and sufficient amount of active pharmaceutical ingredient. Many targets under Goal 3 of the Global Goals for Sustainable Development (e.g., achieving universal health coverage) can only be achieved when countries are supported by well-functioning and sufficiently- funded NRAs that safeguard access to essential medicines (2). Effective drug regulation can also build trust between the public and the government and promote research and development of new treatments (5). All in all, NRAs carry out a continuum of functions; upstream processes affect market entry and quality control, while downstream processes emphasize post-market surveillance (Figure 1).
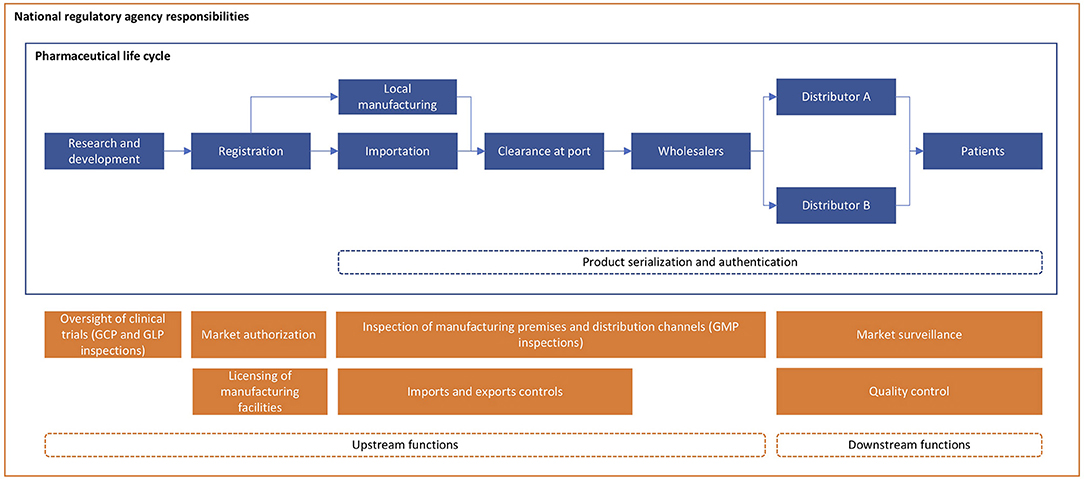
Figure 1. Roles and responsibilities of national regulatory agencies.
Low- and middle-income countries (LMICs), particularly Sub-Saharan African (SSA) countries, have made great strides in establishing their own NRAs and drug regulatory regimes; however, the availability, affordability, and quality of life-saving drugs are still not guaranteed (6). In this perspective article, we propose a framework that explains how (1) fragmented and complex drug regulations, (2) suboptimal enforcement of regulations, and (3) poor disincentives for non-compliance create unintended consequences that lead to poor health outcomes and health inequities. We posit that in carrying out certain functions and advancing their legitimacy, NRAs often create a regulatory environment that discourages manufacturers from entering, or staying in, certain markets; this limits competition, keeps drug costs high, and leads to shortages and the proliferation of illegitimate and unregistered drugs. We argue that some of the issues around drug availability, affordability, and quality result not from poor NRA capacity (e.g., weak management structures, inadequate human, and financial resources) but from the misguided belief that each LMIC must establish its own NRA with its own standalone regulations. Finally, we urge the involvement of various stakeholders to effectively address these issues.
Conceptual Framework
We developed the conceptual framework (Figure 2) below based on a systematic review of peer-reviewed literature (in MEDLINE via PubMed), gray literature identified through snowball and convenience sampling, and insights from key informant interviews. We also drew from our experiences and insights as practitioners and researchers in supply chain management and organizers of one of the largest global health supply chain conferences that is now on its 12th year (7).
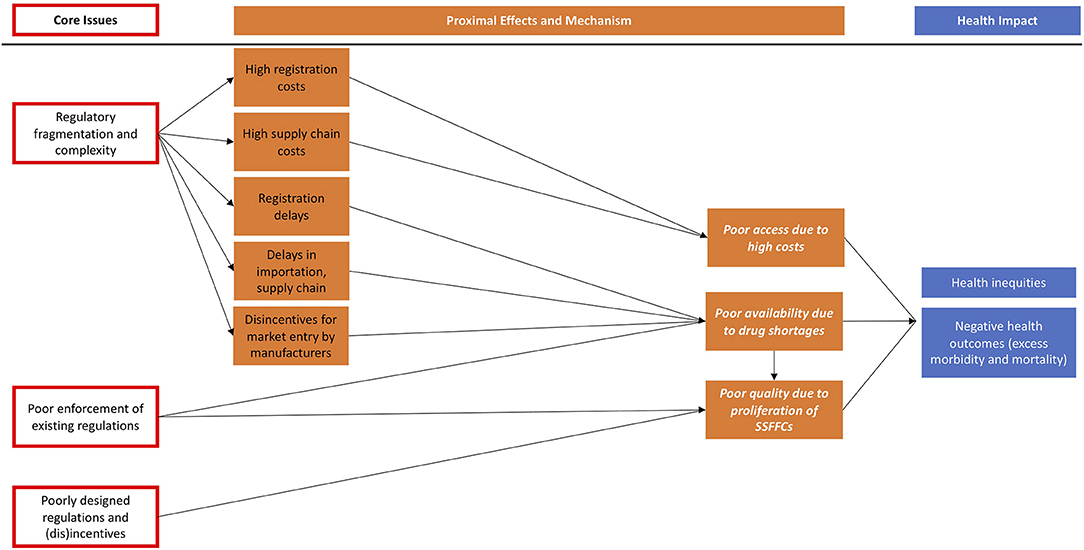
Figure 2. Framework for understanding the unintended consequences of regulatory fragmentation and complexity, poor enforcement, and ineffective disincentives.
Our framework demonstrates how regulatory fragmentation, poor policy design, and enforcement issues lead directly or indirectly to unintended consequences, which in turn influence population health and health equity. It is important to note that other core issues such as corruption and complex international trade agreements are not depicted in the framework but are also important causes of poor affordability, availability, and quality of drugs (1, 8, 9). In the following section, we explain each pathway and provide evidence. We hope that this framework will be refined over time by empirical research.
Regulatory Fragmentation and Complexity
Regulatory fragmentation and complexity arise from convoluted and duplicative requirements imposed on drug manufacturers by each NRA before granting initial market authorization (MA) or renewal. Examples include redundant and non-transparent registration procedures that are unaligned with international standards; widely divergent requirements across countries for establishing bioequivalence; complex country-specific labeling and packaging requirements; and costly requirements for good manufacturing practice (GMP) inspections (4, 10, 11). There may even be divergent rules between national and subnational regulations.
Once MA has been granted, fragmented and complex regulations can increase supply chain costs or lead to stockouts (Figure 2) (1). For example, regulations on residual shelf life of medicines at time of import, which were first imposed decades ago to protect against dumping of short-shelf life medicines, significantly reduce the ability of manufacturers to supply country orders from large batch runs or from more agile and responsive regional stock locations. These regulations also force manufacturers to supply using expensive modes (e.g., airfreight) to reduce delivery lead times, while others may even decide to withdraw from the market if operational costs are prohibitive relative to potential revenues.
The health impact of drug stockouts are significant, leading to delayed treatment initiation, incomplete treatments and treatment interruptions, disengagements with patients, and increased out-of-pocket expenditures (12–14). Consequently, patients face higher risks of developing drug-resistant or more severe forms of disease, complications, and death (12, 13, 15–17).
For new market entrants, fragmented, complex regulations can serve as a disincentive or barrier to supply (18). The “mosaic of regulations” that each country's NRA puts in place significantly delay registration or licensing (5). Work by Ahonkhai et al. (19) found that new, life-saving drugs will take 4–7 years to be approved in SSA after being submitted for approval to a well-resourced NRA such as the US Food and Drug Administration (FDA) or the European Medicines Agency (EMA) (19). These issues help explain why fewer medicines are available in SSA compared to other regions and countries, and why drug costs tend to remain higher for longer (20).
Fragmented, complex regulations can also lead to significant costs for a manufacturer. In a survey of 33 drug manufacturers operating in Africa, respondents cited high registration, retention, and GMP inspection costs as the main reason for deciding against entering certain African markets (11). Though published registration costs for new drugs are lower in SSA than in high-income countries (21), duplicative and resource-intensive regulatory processes require companies to invest significant financial resources to get a drug approved. The increased costs can be passed to consumers; some companies however, particularly manufacturers of generic medicines and other smaller-margin products, may decide against supplying the drug altogether. Thus, competition is limited, drug costs stay high, and health and social inequities are exacerbated as primarily well-off families can afford life-saving but expensive medications (1, 4, 5, 10).
When effective and legitimate drugs are inaccessible or unaffordable, demand is quickly filled by illegitimate drugs (4, 8). The World Health Organization (WHO) estimates that 1 in 10 medical products in LMICs are illegitimate, though this likely masks the wide heterogeneity across countries where over 35% of certain types of drugs (e.g., antimalarials) are substandard or falsified (2, 22, 23). A recent systematic review estimates that almost 19% of medicines in SSA and 13.7% in Asia are poor-quality (24).
Illegitimate and unregistered drugs can lead to poisoning, untreated disease or treatment failure, and premature death (4, 22, 25). A 2017 WHO report estimates that 72,000–169,000 deaths among children per year may be due to substandard and falsified antibiotics used to treat pneumonia, and an additional 116,000 (range: 64,000–158,000) caused by illegitimate antimalarials in SSA annually (26).
Illegitimate drugs also lead to significant opportunity costs for consumers and healthcare systems, as money, time, and efforts are wasted on ineffective medications and additional treatments (2, 4, 24, 27). Globally, the economic burden of illegitimate drugs is estimated to be between $10–200 billion (24). The same 2017 WHO report estimates the cost of additional care due to illegitimate antimalarials to be US$38.5 million per year (range: US$21.4 million−52.4 million) (26). In the Democratic Republic of Congo (DRC) alone, a recent modeling study estimates that illegitimate antimalarials cost $20.9 million (or 35% of malaria costs) in Kinshasa province and an additional $130 million in Katanga region (28).
As with stockouts, substandard and falsified drugs can also result in drug resistance, forcing additional costs in developing new drugs to replace ineffective regimens (2, 4, 23, 25, 29). For example, in the DRC development of antimalarial drug resistance is estimated to cost an additional $90 million per year in additional treatments (28). Finally, illegitimate drugs induce distrust among consumers, ultimately weakening other public health efforts (4, 26, 30).
Poor Enforcement of Existing Regulations
Countries with stringent laws safeguarding pharmaceutical quality still experience many problems because regulations are poorly enforced, and illegitimate drugs still end up in ports and drug shops. News media have covered several raids and interceptions performed by local law enforcement in Africa (31–33). INTERPOL seized 420 tons of illegitimate drugs worth approximately US$21.8 million in West Africa during its Operation Heera in May–June 2017 (4, 34). Previous operations in East, Southern, and West Africa have also seized millions of units of illegitimate drugs (35).
The market for substandard and falsified drugs is substantial; the WHO estimates upwards of US$30 billion is spent on illegitimate drugs globally per year, while the Center for Medicines in the Public Interest thinks the amount is closer to US$75 billion (2, 9). The UN Office on Development and Crime believes the sale of illegitimate drugs in West Africa alone is worth more than the combined value of crude oil and cocaine trafficking (roughly US$1 billion) (4). Thus, as long as unscrupulous manufacturers have a good chance of getting away with their crime, illegitimate drugs are likely to persist and proliferate (4). Currently drug counterfeiters are less likely to be caught than narcotic drug traffickers, suggesting that significantly more effort can be directed toward stopping illegitimate medicines from spreading (9, 33).
Poor enforcement may be the result of resource constraints and poor capacity among NRAs (4). However, other factors such as low political commitment and prioritization, corruption, and ineffective management are also to blame (9). Poor hiring policies limit performance; for example, NRAs commonly hire pharmacists in roles requiring different competencies than what they were trained for. NRAs disproportionally allocate resources on upstream functions (Figure 1) that can be simplified or de-duplicated through regulatory harmonization (36). Finite NRA resources should instead be spent on downstream functions such as post-market surveillance and detection of illegitimate drugs.
Poorly Designed Regulations and Disincentives
In many countries throughout SSA, disincentives for producing, selling, and distributing illegitimate drugs are insufficient to deter illegal manufacturers (37, 38). In fact, the penalties for drug falsifiers and counterfeiters are far more lenient than for drug traffickers who are often fined large sums and given long prison sentences when caught and successfully prosecuted (4). For example, the minimum prison sentence for a manufacturer of falsified drugs in Tanzania is 2 years, with a corresponding maximum civil penalty of up to US$57,000 (4). For drug traffickers, the minimum sentence is 30 years to a lifetime (39). Because counterfeiting and falsification are lucrative activities and are largely risk-free, the market for illegitimate drugs is believed to be larger than for illegal drugs (9). Given the health, social, and economic costs illegitimate drugs exact on LMICs, NRAs must push for legislation that increases the punishment for lawbreaking manufacturers. To be effective, penalties must meet or exceed the potential revenue from illegitimate drug production, trade, and sale. Policies should also address drug shortages and the high costs of genuine drugs as these can give rise to a significant unmet demand for cheap, accessible medicines—a void that illegitimate drugs are designed to fill (4, 9).
What can be Done?
While NRAs can gain a lot from increased investment in their work, we think regulatory harmonization of current regulations and innovation can arrest and reverse the regulatory failures we still see today and improve medicine access in SSA.
Defining Regulatory Harmonization and Its Benefits
Harmonization refers to the development and adoption of common technical requirements and guidelines for pharmaceutical regulation. Harmonization is not the same as convergence, which the FDA defines as the process in which “regulatory requirements across countries or regions become more similar or ‘aligned' over time.”(40). Harmonization goes further than convergence in that it emphasizes deduplication and mutual recognition of technical guidelines and standards, registration processes, and requirements across participating NRAs (40). Under convergence, countries may set similar but separate requirements for manufacturers applying for MA; with harmonization, several countries may participate in a joint assessment in lieu of country-by-country approval.
Harmonization will result in streamlined regulations and processes, which can reduce redundancy and drug registration times, leading to increased access to new and effective treatments (5, 23). For example, the Mexican NRA established a unilateral agreement with EMA that says the NRA will recognize findings from EMA's assessment of a drug manufacturer that is also applying for a new drug MA in Mexico (41). Mexico has similar arrangements with the US, Canada, Australia, and Switzerland.
SSA as a whole can benefit from similar mutual recognition agreements as they will reduce administrative and cost burdens faced by resource-limited NRAs and pharmaceutical manufacturers alike (11, 23). By relying on the expertise and resources of other countries, NRAs in SSA that are significantly more strapped for resources than Mexico's can focus their efforts and resources on downstream functions (Figure 1) (4, 6, 36, 42). Bilateral and multilateral donors should support NRAs' efforts to improve post-market surveillance, to streamline regulatory processes, and to enforce existing laws and regulations (17).
All-in-all, we believe harmonization will indeed strengthen resource-constrained NRAs in SSA and ensure the supply of effective and high-quality products. A 2018 modeling study by the global health organization PATH estimated that 23,000 lives in the East African Community (EAC) and in Zazibona countries (Botswana, Namibia, South Africa, Zambia, and Zimbabwe) could be saved by accelerating the authorization of dispersible amoxicillin tablets, an antibiotic used to treat childhood pneumonia, by 2 years (43).
Current Harmonization Efforts
There are several regulatory harmonization efforts underway, though in practice many of them are focused only on convergence (Table A1 in Supplementary Material). Some initiatives claim to have demonstrated results, while others were recently established to overcome new challenges and persistent gaps; however, no impact has yet been demonstrated on the macro-scale issues described above such as the prevalence of illegitimate medicines and low registration rates due to regulatory cost and complexity. Most initiatives are also not legally binding, which can create issues with compliance and uniformity across countries. Finally, the participants of most initiatives are from the NRAs themselves, effectively excluding patient advocacy groups and government executives such as those from ministries of health or treasury.
Among the models of regulatory harmonization that exist, the EMA framework holds the most promise for the SSA region. The EMA's centralized procedure grants MA to a new drug that is valid for the 28 countries of the European Union and the three countries in the European Economic Area (44). The EMA assessment, which requires the approval of the European Commission, is usually completed within 210 days (45). The centralized procedure is required for many classes of drugs (e.g., HIV, cancer, and diabetes drugs) and optional for others. Drug manufacturers who wish to seek MA in one or several European countries can do so through national MA procedures or other routes (46). But because regulatory requirements and processes have been harmonized throughout the EU, data requirements and standards across MA routes are the same (4).
In Africa, the African Medicines Regulatory Harmonization (AMRH) initiative's regional project is leading efforts in pursuit of regulatory harmonization. Coordinated by the African Union's (AU) NEPAD Agency, the AMRH has led to improvements with real potential, including harmonization of (1) guidelines for registration of generic medicines, (2) GMP inspections, (3) quality management systems, and (4) information management systems in the EAC and the Southern African Development Community (SADC) (6, 17). The EAC has successfully conducted joint assessment of manufacturer dossiers, which has reduced drug approval timelines by 40–60% for branded medicines (6, 42, 47). As of 2017, 12 African countries have adapted the AU Model Law on Medical Products Regulation which aims to establish common pharmaceutical laws throughout the continent (6).
A Path Forward: Some Recommendations
The progress of the AMRH should be supported and accelerated. To sustain the initiative's momentum, several actions should be undertaken. First, the joint assessment process can still benefit from further streamlining in the short term; for example, separate country registration forms and fees are still required in the EAC. In the long term, the AMRH should also move aggressively to establish the African Medicines Agency, which will serve as a pan-African regulatory agency (6). Second, the AMRH and NRAs should allocate resources on educating and encouraging manufacturers to use the regional MA route to expand access to drugs quickly and efficiently. Related to this, certain classes of drugs should be required to go through joint assessments as opposed to country-by-country MA. Third, the AMRH should swiftly replicate successes in the EAC and SADC regions to other economic communities in SSA. Throughout this process, we encourage ministers of health to be more involved and ensure political commitment at the national level. Fourth, the AMRH should work with the EMA, the FDA, and other NRAs in order to achieve optimal streamlining and de-duplication of efforts. It would be unfortunate to achieve sub-regional harmonization in the African continent yet preserve regulatory fragmentation and complexity at the continental level. To reduce barriers to medicines importation, trade authorities including ministries of commerce should also get involved. Finally, once the AMRH achieves regulatory harmonization, the initiative should continue its work streamlining and strengthening positive NRA functions such as post-market surveillance and enforcement.
In addition to regulatory harmonization, two innovations—serialization, which is the assignment of unique, traceable numbers to individual items, and mobile technology-based product verification—hold promise in fighting the scourge of illegitimate and unregistered drugs. Product verification through services like mPedigree and Sproxil allows consumers to determine whether drugs are authentic at the point of sale (48). Serialization using GS1 barcodes like 2D data matrices allow various agencies and actors along the supply chain to determine the source and authenticity of various drugs. Information from these technologies can then be used in cross-border intelligence and operations; for example, INTERPOL's collaborative operations have been successful in thwarting illegal drug manufacturers and distributions in select SSA countries and should be supported by manufacturers, governments, and donors (38).
Conclusion
National regulatory authorities and pharmaceutical regulatory regimes are key to promoting access and quality of life-saving drugs. However, NRAs that have fragmented, unnecessarily complex, ineffective, and poorly enforced regulations contribute to poor health and health inequities. To date, NRA-led initiatives pursuing harmonization, while many, have delivered few results very slowly. We encourage NRAs, regional initiatives, national governments, and donors to exert significant leadership and action in pursuit of regulatory harmonization.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
IB is Healthcare Strategy Executive and NG is Healthcare Programme Manager at Imperial Logistics, a private logistics and supply chain management company that has commercial contracts with numerous pharmaceutical companies operating and trading in Africa, as well as a range of donors and national governments.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors extend their gratitude to Ajiffa Labor of Imperial Logistics and various key informants for their input on various aspects of this article. The authors also thank the reviewers who provided valuable feedback that helped to improve this article.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2019.00342/full#supplementary-material
References
1. Seiter A. A Practical Approach to Pharmaceutical Policy. Washington, DC: The International Bank for Reconstruction and Development; The World Bank (2010).
2. World Health Organization. WHO Global Surveillance and Monitoring System for Substandard and Falsified Medical Products. Geneva: World Health Organization (2017).
3. World Health Organization. Assessment of Medicines Regulatory Systems in Sub-Saharan African Countries: An Overview of Findings From 26 Assessment Reports. (2010). Available online at: http://apps.who.int/medicinedocs/documents/s17577en/s17577en.pdf (accessed January 29, 2018).
4. Institute of Medicine. Countering the Problem of Falsified and Substandard Drugs. Washington, DC: National Academies Press (2013).
5. Zerhouni E, Hamburg M. The need for global regulatory harmonization: a public health imperative. Sci Transl Med. (2016) 8:338ed6. doi: 10.1126/scitranslmed.aaf1396
6. Ndomondo-Sigonda M, Miot J, Naidoo S, Ambali A, Dodoo A, Mkandawire H. The African medicines regulatory harmonization initiative: progress to date. Med Res Arch. (2018) 6:1–15. doi: 10.18103/mra.v6i2.1668
7. Global Health Suply Chain Summit. About. (2019). Available online at: https://ghscs.com/program/ (accessed August 2, 2019).
8. Newton PN, Green MD, Fernández FM, Day NP, White NJ. Counterfeit anti-infective drugs. Lancet Infect Dis. (2006) 6:602–13. doi: 10.1016/S1473-3099(06)70581-3
9. Dégardin K, Roggo Y, Margot P. Understanding and fighting the medicine counterfeit market. J Pharm Biomed Anal. (2014) 87:167–75. doi: 10.1016/j.jpba.2013.01.009
10. Institute of Medicine. Improving Access to Essential Medicines for Mental, Neurological, and Substance Use Disorders in Sub-Saharan Africa: Workshop Summary. Washington, DC: The National Academies Press (2014).
11. Narsai K, Williams A, Mantel-Teeuwisse AK. Impact of regulatory requirements on medicine registration in African countries – perceptions and experiences of pharmaceutical companies in South Africa. South Med Rev. (2012) 5:31–7.
12. Gils T, Bossard C, Verdonck K, Owiti P, Casteels I, Mashako M, et al. Stockouts of HIV commodities in public health facilities in Kinshasa: barriers to end HIV. PLoS ONE. (2018) 13:e0191294. doi: 10.1371/journal.pone.0191294
13. Mikkelsen-Lopez I, Tediosi F, Abdallah G, Njozi M, Amuri B, Khatib R, et al. Beyond antimalarial stock-outs: implications of health provider compliance on out-of-pocket expenditure during care-seeking for fever in South East Tanzania. BMC Health Serv Res. (2013) 13:444. doi: 10.1186/1472-6963-13-444
14. Poku RA, Owusu AY, Mullen PD, Markham C, McCurdy SA. HIV antiretroviral medication stock-outs in Ghana: contributors and consequences. Afr J AIDS Res. (2017) 16:231–9. doi: 10.2989/16085906.2017.1364275
15. Pasquet A, Messou E, Gabillard D, Minga A, Depoulosky A, Deuffic-Burban S, et al. Impact of drug stock-outs on death and retention to care among HIV-infected patients on combination antiretroviral therapy in Abidjan, Côte d'Ivoire. PLoS ONE. (2010) 5:e13414. doi: 10.1371/journal.pone.0013414
16. Seunanden T, Day C. The extent and impact of TB drug stock-outs. In: Padarath A, English R, editors. South African Health Review 2013/14. Durban: Health Systems Trust (2014). Available online at: http://www.hst.org.za/publications/south-african-health-review-2013/14
17. New Partnership for Africa's Development. African Medicines Regulatory Harmonization (AMRH) Strategic Plan 2016 – 2020. (2016). Available online at: http://www.nepad.org/resource/amrh-summarized-strategic-framework-2016-2020 (accessed January 29, 2018).
18. Lionberger RA. FDA critical path initiatives: opportunities for generic drug development. AAPS J. (2008) 10:103–9. doi: 10.1208/s12248-008-9010-2
19. Ahonkhai V, Martins SF, Portet A, Lumpkin M, Hartman D. Speeding access to vaccines and medicines in low- and middle-income countries: a case for change and a framework for optimized product market authorization. PLoS ONE. (2016) 11:e0166515. doi: 10.1371/journal.pone.0166515
20. New Partnership for Africa's Development, World Health Organization. African Medicines Registration Harmonisation (AMRH) Initiative: Summary, Status and Future Plan. (2009). Available online at: http://apps.who.int/medicinedocs/documents/s20130en/s20130en.pdf (accessed January 29, 2018).
21. Morgan SG, Yau B, Lumpkin MM. The cost of entry: an analysis of pharmaceutical registration fees in low-, middle-, and high-income countries. PLoS ONE. (2017) 12:e0182742. doi: 10.1371/journal.pone.0182742
22. Newton PN, Green MD, Fernández FM. Impact of poor-quality medicines in the ‘developing' world. Trends Pharmacol Sci. (2010) 31:99–101. doi: 10.1016/j.tips.2009.11.005
23. Bassat Q, Tanner M, Guerin PJ, Stricker K, Hamed K. Combating poor-quality anti-malarial medicines: a call to action. Malar J. (2016) 15. doi: 10.1186/s12936-016-1357-8
24. Ozawa S, Evans DR, Bessias S, Haynie DG, Yemeke TT, Laing SK, et al. Prevalence and estimated economic burden of substandard and falsified medicines in low- and middle-income countries: a systematic review and meta-analysis. JAMA Netw Open. (2018) 1:e181662. doi: 10.1001/jamanetworkopen.2018.1662
25. Kelesidis T, Falagas ME. Substandard/counterfeit antimicrobial drugs. Clin Microbiol Rev. (2015) 28:443–64. doi: 10.1128/CMR.00072-14
26. World Health Organization. A Study on the public Health and Socioeconomic Impact of Substandard and Falsified Medical Products. Geneva: World Health Organization (2017).
27. Blackstone EA, Fuhr JP, Pociask S. The health and economic effects of counterfeit drugs. Am Health Drug Benefits. (2014) 7:216–24.
28. Ozawa S, Haynie DG, Bessias S, Laing SK, Ngamasana EL, Yemeke TT, et al. Modeling the economic impact of substandard and falsified antimalarials in the Democratic Republic of the Congo. Am J Trop Med Hyg. (2019) 100:1149–57. doi: 10.4269/ajtmh.18-0334
29. Panda S, Swaminathan S, Hyder KA, Christophel EM, Pendse RN, Sreenivas AN, et al. Drug resistance in malaria, tuberculosis, and HIV in South East Asia: biology, programme, and policy considerations. BMJ. (2017) 358:j3545. doi: 10.1136/bmj.j3545
30. Karunamoorthi K. The counterfeit anti-malarial is a crime against humanity: a systematic review of the scientific evidence. Malar J. (2014) 13:209. doi: 10.1186/1475-2875-13-209
31. AFP. Benin Suspends Pharmacy Body Over ‘Fake Drugs' Scandal. The Citizen (2018). Available online at: http://citizen.co.za/news/news-africa/1856279/benin-health-drugs/ (accessed March 26, 2018).
32. Akinyelure D. Nigeria Fake Drugs: ‘My Patient Woke Up Mid-surgery'. BBC News (2017). Available online at: http://www.bbc.com/news/av/world-africa-42396949/nigeria-fake-drugs-my-patient-woke-up-mid-surgery (accessed January 29, 2018).
33. Ossola A. The Fake Drug Industry is Exploding, and We Can't Do Anything About It. Newsweek (2015). Available online at: http://www.newsweek.com/2015/09/25/fake-drug-industry-exploding-and-we-cant-do-anything-about-it-373088.html (accessed January 29, 2018).
34. INTERPOL. Hundreds of Tonnes of Illicit Medicines Seized in African Operation. (2017). Available online at: https://www.interpol.int/News-and-media/News/2017/N2017-107 (accessed March 20, 2018).
35. INTERPOL. Operations. (2018). Available online at: https://www.interpol.int/Crime-areas/Pharmaceutical-crime/Operations (accessed March 24, 2018).
36. Keyter A, Banoo S, Salek S, Walker S. The South African regulatory system: past, present, and future. Front Pharmacol. (2018) 9:1407. doi: 10.3389/fphar.2018.01407
37. Attaran A. Stopping murder by medicine: introducing the Model Law on Medicine Crime. Am J Trop Med Hyg. (2015) 92:127–32. doi: 10.4269/ajtmh.15-0154
38. Nayyar GML, Breman JG, Mackey TK, Clark JP, Hajjou M, Littrell M, et al. Falsified and substandard drugs: stopping the pandemic. Am J Trop Med Hyg. (2019) 100:1058–65. doi: 10.4269/ajtmh.18-0981
39. The Parliament of the United Republic of Tanzania. The Drug Control and Enforcement Act, 2015. (2015).
40. U.S. Food & Drug Administration. Regulatory Harmonizabtion and Convergence. (2018). Available online at: https://www.fda.gov/BiologicsBloodVaccines/InternationalActivities/ucm271079.htm (accessed February 5, 2018).
41. Luigetti R, Bachmann P, Cooke E, Salmonson T. Collaboration, not competition: developing new reliance models. WHO Drug Inf . (2016) 30:558–66. Available online at: http://apps.who.int/medicinedocs/en/m/abstract/Js23135en/
42. Ndomondo-Sigonda M, Miot J, Naidoo S, Dodoo A, Kaale E. Medicines regulation in Africa: current state and opportunities. Pharm Med. (2017) 31:383–97. doi: 10.1007/s40290-017-0210-x
43. PATH. Making the Case: How Regulatory Harmonisation Can Save Lives in Africa. (2018). Available online at: https://path.azureedge.net/media/documents/Regulatory_harmonisation_report.pdf (accessed March 20, 2019).
44. European Medicines Agency. What We Do. (2018). Available online at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/about_us/general/general_content_000091.jsp&mid=WC0b01ac0580028a42 (accessed February 23, 2018).
45. Kashyap UN, Gupta V, Raghun HV. Comparison of drug approval process in United States & Europe. J Pharm Sci Res. (2013) 5:131–6. Available online at: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.375.519&rep=rep1&type=pdf
46. European Medicines Agency. Authorisation of Medicines. (2018). Available online at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/about_us/general/general_content_000109.jsp&mid=WC0b01ac0580028a47 (accessed February 23, 2018).
47. NEPAD. African Medicines Regulatory Harmonization Newsletter Quarter 1: January - March 2017. (2017). Available online at: http://www.nepad.org/resource/amrh-newsletter-march-2017 (accessed January 29, 2017).
Keywords: pharmaceutical regulation, regulatory harmonization, drug access, Sub-Saharan Africa, drug quality, health impact
Citation: Barton I, Avanceña ALV, Gounden N and Anupindi R (2019) Unintended Consequences and Hidden Obstacles in Medicine Access in Sub-Saharan Africa. Front. Public Health 7:342. doi: 10.3389/fpubh.2019.00342
Received: 29 May 2019; Accepted: 30 October 2019;
Published: 15 November 2019.
Edited by:
Edward I. Broughton, Bristol Myers Squibb, United StatesReviewed by:
Afolaranmi Olumide Tolulope, Jos University Teaching Hospital, NigeriaM. Rashad Massoud, University Research Co., United States
Copyright © 2019 Barton, Avanceña, Gounden and Anupindi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iain Barton, SWFpbi5CYXJ0b24mI3gwMDA0MDtpbXBlcmlhbGxvZ2lzdGljcy5jb20=