 Chien-Ming Wang
Chien-Ming Wang Hsin-Pei Hsueh
Hsin-Pei Hsueh Fangjhy Li
Fangjhy Li Cheng-Feng Wu
Cheng-Feng Wu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health, 20 November 2019
Sec. Health Economics
Volume 7 - 2019 | https://doi.org/10.3389/fpubh.2019.00324
This article is part of the Research TopicAccelerated Globalization and its Impact to the World’s Health Care AchievementView all 5 articles
Using annual time-series data over the period 1975–2017, the researcher applied the bootstrap autoregressive-distributed lag (ARDL) cointegration model developed by McNown et al. (1) to examine whether there is a long run relationship among health expenditure, CO2 emissions, and gross domestic product (GDP) per capita in 18 Organization for Economic Cooperation and Development (OECD) countries. We find cointegration exists in Netherlands when real GDP per capita serves as a dependent variable, in New Zealand when health expenditure is the dependent variable, and in the United States when CO2 emissions are dependent variables. The main results show evidence of a short run relationship between the three variables. The empirical results support that there is a bidirectional causality between health expenditure and GDP growth for Germany and the United States, between CO2 emissions and GDP growth for Canada, Germany, and the United States, and between health expenditure and CO2 emissions for New Zealand and Norway. The results also indicate that there are unidirectional causality in other countries.
Climate change caused by increased greenhouse gas emissions not only causes temperature rise but also affects global precipitation. Climate change has become an indisputable fact that poses a serious threat to the sustainable development of human survival, society, economy, and the environment (2). There is an important link between high concentrations of greenhouse gases and climate change that there is the impact of climate change on public health. In recent decades, however, the relationship among economic growth, environment deterioration, and health expenditure has received increasing attention in the literature. Economic growth, environmental degradation, and health care expenditure vary between these relationships—complex and important. Therefore, the negative externalities of low environmental quality due to the impact on human health expenditure are ignored (3).
Health is one of the most important factors to decide the quality of human capital. There are many factors that can affect the health status of the population, such as environmental health, socioeconomic status, economic development, and the environment quality. As environmental quality deteriorates, the deterioration of global environmental quality poses a serious challenge to healthy living. Particles from the burning of fossil fuels, sulfur dioxide, and CO2 emissions are a major contributor to global climate change, and this has been a topic of policy makers and a focus of researchers in many different fields of research (4).
Most of the literature in the past examined the pairwise relationship CO2 emissions, gross domestic product (GDP), and health expenditure. Over the past decade, the first empirical study is based on Grossman and Krueger (5), and a number of researchers have followed the Environmental Kuznets Curve (EKC) between economic growth and environmental quality (6–10). The second pairwise of empirical study shows that many researches have focused on the relationship between health expenditure and GDP (11–13). The majority of previous economists have studied to estimate the health care demand about the size of income elasticity and allocate health care resources. Finally, the third pairwise of empirical study was on the relationship between CO2 emissions and health expenditure (3, 14, 15). There are many researchers focusing on one-way causation from CO2 emissions to health expenditure and finding a positive relationship. However, only a limited number of empirical studies have concentrated on two-way causation between CO2 emissions and health expenditure.
CO2 emissions from Organization for Economic Cooperation and Development (OECD) countries account for half of global O2 emissions, yet CO2 emissions in OECD countries have been reduced since 2001. During this period, the OECD has made huge efforts to reduce CO2 emission intensity. CO2 emissions per unit of GDP decreased from 4.9 kg/USD in 2001 to 2.7 kg/USD in 2015. The share of CO2 emissions in global CO2 emissions also fell from 54% in 2001 to 38% in 2015 (13). Therefore, it is important to examine CO2 emissions for health expenditures and economic development in OECD countries.
This article aims to examine the health, CO2 emissions, and GDP growth nexus for 18 OECD countries by applying a bootstrap autoregressive-distributed lag (ARDL) test proposed by McNown et al. (1). This new method helps identify the occurrence of degenerate cases in ARDL tests. We, for the first time (compared to previous literature in OECD countries), used bootstrap models estimated by the ARDL test for long- and short-run relationships.
The main contribution of our research work to the existing studies is helpful for policy makers of OECD countries in particular and will provide some imperative understanding to other developed countries that include the 18 OECD countries. We used bootstrap ARDL approach for the long-run relationship and Granger causality tests to find directions of the links among the three variables. Therefore, this study aims at filling the gap in the literature by analyzing the health expenditure, CO2 emissions, and GDP growth using the newly proposed econometric methodology to test.
The study will be separated into five sections. Section Literature presents a review of the literature. The data and methods used are described in section Materials and Methods. Section Results presents the results. Section Discussion has discussions. Section Conclusion concludes the research.
The purpose of this study was to demonstrate the interaction between CO2 emissions, health spending, and GDP growth in OECD countries. The pairwise correlation variables between the primary studies will be discussed.
Most of the literature in the past concentrate on the relationship between environmental pollution and economic growth. First, the previous study was done to test the validity of the EKC hypothesis, which assumes that the relationship between economic growth and the environment is in the form of an inverted U. Selden and Song (9) used a nation's panel of data and the results confirm the inverted U. This hypothesis, however, was first proposed by Grossman and Krueger (5), where environmental degradation increases proportionally to income, then reaches a certain threshold when income reaches a stable point and then begins to decrease. Holtz-Eakin and Selden (16) examined marginal propensity to emit (MPE) and found that a diminishing MPE carbon dioxide as GDP per capita rises. Some authors (17–20) have reported the existence of the EKC hypothesis. Not all results support the ECK hypothesis. Cole et al. (21) have found evidence against the EKC hypothesis.
Using the cointegration technique of ARDL bound test and Graager causality, Halicioglu (22) examined the feedback hypothesis between CO2 emissions and economic expansion for Turkey. Saboori et al. (23) utilized ARDL bound approach to study the causal relationship between GDP growth and CO2 emissions for Malaysia and found unidirectional causality from GDP growth to CO2 emissions. Saboori and Sulaiman (24) determined a significant relationship between CO2 emissions and economic growth that supported the EKC hypothesis in Singapore and Thailand for the long run. Jebli et al. (25) found that two-way causalities existed in the long run between CO2 emissions and economic growth for 25 OECD countries. Cai et al. used the application of the newly introduced bootstrap ARDL bound test with structural breaks to examine the relationship among clean energy consumption, economic growth, and CO2 emissions. They found the existence of a long-term and short-term relationship between economic growth and CO2 emissions for the G7 nations (6).
The second part focuses on health expenditures and GDP growth. Much of the previous research has focused on estimating the impact of health care income elasticity on scale, except for distribution of health care resources.
Gerdtham and Löthgren test the cointegration between health expenditure and GDP in the 25 OECD nations for the period 1960–1997. The outcomes revealed that health expenditure and GDP are cointegrated for the 12 OECD nations (26). Baltagi and Moscone (27) also considered OECD countries using a panel of data to reconsider the long-run relationship between health care expenditure and income for the period 1971–2004. Their findings suggest that health care, a necessity, is in elastic demand. Wang applied the quantile panel-type analysis to determine the causality between health expenditure and economic growth from 1986 to 2007. The findings indicated that the estimation of quantile regression of the effect of health expenditure growth on economic growth is different (28). Albulescu et al. utilized health care spending for six EU member countries for the time period 1972–2013. The findings indicated that no significant convergence occurred with regard to the ratio of health care expenditure to GDP (29). Erçelik and Murthy and Okunade used ARDL to estimate the relationship between health expenditure and economic growth (30, 31).
The third research strand on the issue that has limited literature regarding the relationship between CO2 emissions and health expenditure discusses the relationship between environmental pollution (carbon emissions) and health expenditure.
Yazdi et al. (3) applied the ARDL approach to investigate carbon monoxide and sulfur oxide that have a positive relationship on health expenditures. Beatty and Shimshack used a cohort analysis to study relationships between carbon monoxide exposure and children's health outcome. They find that the increase in carbon monoxide resulted in positive and significant increases in children's health treatment (32). Boachie et al. in Ghana utilized health care expenditure for the time period 1970–2008. The finding revealed that a negative relationship exists between health care expenditure and CO2 emissions (14). According to the result presented in the study by Chaabouni et al. and Chaabouni and Saidi found that the low-income group countries have unidirectional causality from CO2 emissions to health expenditure (33, 34). Lu et al. (15) verified a negative effect of CO2 emissions and other pollutants on human health in 30 Chinese provinces.
Only a few studies have focused on the relationship among health expenditures, CO2 emissions, and economic growth. Chaabouni et al., Chaabouni and Saidi, and Chaabouni and Abdnnadher provide evidence of causality among health expenditures, CO2 emissions, and economic growth (33–35). Zaidi and Saidi showed a one-way causal relationship from health expenditure to GDP and a two-way causal relationship between health expenditure and CO2 emissions in sub-Saharan African countries (36). Ghorashi and Rad applied dynamic simultaneous equation model to investigate health expenditures, CO2 emissions, and economic growth in Iran. The empirical findings supported the presence of two-way causality flowing among CO2 emissions and economic growth and one-way causality from health expenditure to economic growth (37). Wang (28) used the ARDL model for the time period 1995–2017 to examine the dynamic linkages among CO2 emissions, health expenditures, and economic growth in Pakistan. The results of their empirical study show a long-run relationship among the three variables and a two-way relationship of causality between health expenditure and CO2 emissions and between health expenditure and economic growth, as well as a one-way causal relationship from CO2 emissions to health expenditure.
This study covers 18 OECD countries between 1975 and 2017. The 18 OECD countries selected for this study are Australia, Austria, Belgium, Canada, Denmark, Finland, Germany, Ireland, Japan, Netherland, New Zealand, Norway, Portugal, Spain, Sweden, Turkey, the United Kingdom, and the United States. Real GDP per capita (GDP) are obtained from the World Development Indicators, World Bank. Per capita real health expenditure (HE) in U.S. PPP dollars older came from OECD Statistics. CO2 emissions (CO2) data are retrieved from The BP Statistical Review of World Energy (available at: http://www.bp.com/). All variables are transformed into natural logarithm form.
The ARDL model is as follows:
i and j are the indicators of the lag period, i = 1, 2…, k; j = 0, 1…, k; h = 0, 1…, p. t represent time t = 1, 2,…, T. The yt in the equation is the explanatory variable, xt and zt are the explanatory variables, and the variable St, j is a dummy variable. The parameters αi, βI, and γi are the coefficients of the lag of yi, xi, and γi. The error term is μt, and Equation (2) can be rewritten and expanded into the following equation:
where and other parameters are the function values of the original parameters in Equation (1).
McNown et al. showed the bootstrap method to the ARDL tests of cointegration and proposed a cointegration that requires rejecting the F-test (denoted as F′) H0 : b1 = b2 = b3 = 0 and the other F-test (denoted as F″) H0 : b2 = b3 = 0; t-test on the lagged dependent variable H0 : a1 = 0 (28). They showed that two degenerate situations can arise. Situation 1 occurs when F′ and t are significant but F″ is not significant. In this situation, the joint significance of the error correction terms is due solely to the lag of the dependent variable. Thus, the explanatory variables are not part of the long-run cointegrating relation. The other situation, degenerate situation 2, occurs when F′and F″are significant but t is not significant. McNown et al. added a test on the lagged independent variables (F-test denoted as F″) to complement the existing F′and t-tests for cointegration as proposed by Pesaran et al. (1, 38).
McNown et al. showed that the bootstrap ARDL test has better size and power properties than the asymptotic test in the ARDL bound test. After testing the long-term relationships, we concluded that short-run causal relationship will be determined by standard Granger causality tests if there is no cointegration relationship among y, x and z. We used the Granger causality test for x and z, which should include the lagged difference on x or z, and we tested a2, j = 0 or a3, j = 0 in Equation (2). However, if there is cointegration between the dependent variable and the independent variable, they will form a fixed linear combination. In this case, the short-term relationship test should include the hysteresis difference of x or z and the hysteresis level of x or z, that is, test a2, j and b2 or a3, j and b3.
The ARDL bound test allows the variables with different orders of integration [I(0) or I(1), not for I(2)] (29). The Augmented Dickey–Fuller (ADF), Kwiatkowski-Phillips-Schmidt-Shin (KPSS), and Zivot-Andrews (ZA) unit root tests were employed to test the integration level (39–41). We found that all series have a unit root at 5% level of significanec, but all variables are stationary in the first differences when AD, KPSS, and ZA tests are used. To conserve space, the unit root test results are not shown here.
Table 1 provides the results of the Bootstrap ARDL tests. This study uses the two F-test ( and ) and one T-test (tc) as critical values for determining the long-run forcing variable found in McNown et al. We believe that only several estimated equations are able to reject the null hypothesis of the t-test and both F-tests simultaneously. We could only find cointegrated evidence for Netherlands when GDP serves as the dependent variable, for New Zealand when health expenditure is the dependent variable, and for the United States when CO2 emission is the dependent variable. Degenerated case 2 also occurs for Finland, where both the F′-test and F″-test are statistically significant but not the t-test. Besides, we believe that no cointegration can be revealed by bootstrap ARDL test among the GDP, health expenditures, and CO2 emissions for Australia, Austria, Belgium, Canada, Denmark, Germany, Ireland, Japan, Norway, Portugal, Spain, Sweden, Turkey, and the United Kingdom. Although not many countries show a long-run relationship between GDP, health expenditures, and CO2 emissions, however, some causality patterns are identified in the short run.

Table 1. Cointegration results: health expenditures (HE), CO2 emissions (CO2), and gross domestic product (GDP) growth.
Based on the results from ARDL cointegration test, we test the causality among the variables for 18 OECD countries by standard Granger causality test to indicate the casual relationship among health expenditure, GDP growth, and CO2 emissions. From Table 2, we can see that a feedback exists between health expenditure and GDP, between health expenditure and CO2 emissions, and between CO2 emissions and GDP.
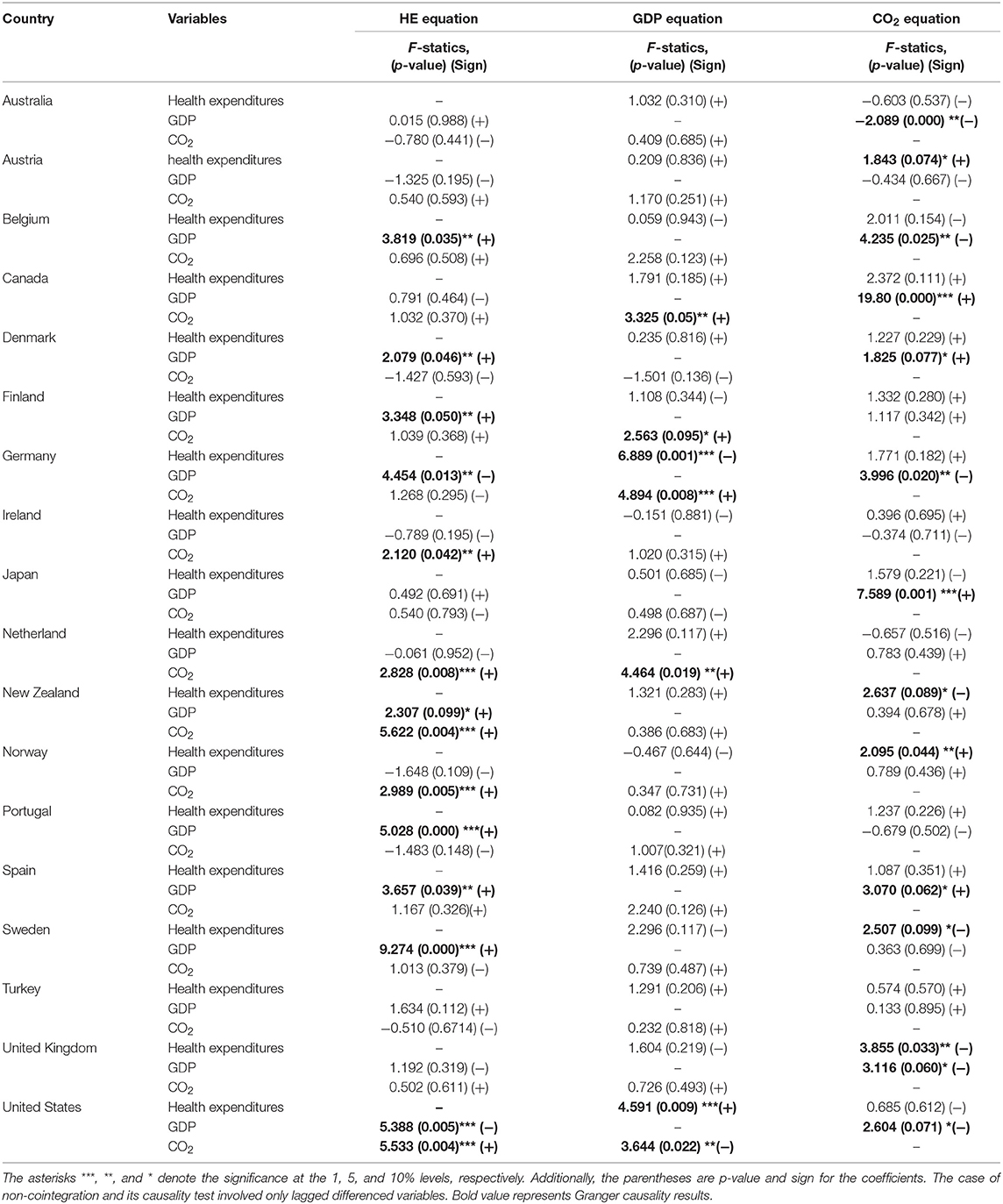
Table 2. Granger causality results: health expenditures, CO2 emissions, and gross domestic product (GDP) growth.
We find a two-way Granger causality running between health expenditure and GDP for Germany and the United States. This finding supports the past empirical studies (42–44). The results from Granger causality tests indicate the existence of bidirectional causality between health expenditure and CO2 emissions for New Zealand and Norway. Studies look at the causal relationship between health expenditures and GDP growth that, in most of these countries, have bidirectional causality (35). We report the causal link between CO2 emissions and GDP growth for Canada, Germany, and the United States by employing a bootstrap ARDL approach. In the short running analysis, many studies also find evidence to support the two-way Granger causality between CO2 emissions and GDP growth (28, 37, 45, 46).
There was unidirectional causality running from GDP to health expenditures for Belgium, Denmark, Finland, New Zealand, Sweden, Portugal, and Spain. The short-run relationship Granger causality was found from health expenditure to CO2 emissions for Austria, Belgium, Sweden, and the United Kingdom, and from CO2 emissions to health expenditures in Germany, Ireland, Japan, Netherlands, and the United States, and these countries exhibit only unidirectional causality. In the short run, it is unidirectional causality. Granger causality tests indicate that CO2 emissions Granger causes GDP in Finland and Netherlands, and GDP Granger causes CO2 emissions in Australia, Denmark, Japan, Spain, Sweden, and the United Kingdom.
The overall results revealed that there is no long-run relationships in the 18 OECD countries. There is no long-run relationship among health expenditures, CO2 emissions, and GDP growth that we support Atay and Ergun that we get the same result in Turkey (40). Wang et al. found a long-run relationship among CO2 emissions, health expenditure, and GDP in Pakistan (47). The researchers examined health expenditure, environmental pollution (CO2 emissions; nitrous oxide emissions), and GDP growth and indicated the long-run relationship among them in the sub-Saharan African countries (36). We only report a long-run relationship among health expenditure, CO2 emissions, and GDP growth in Netherlands, New Zealand, and the United States. There is important available that examined the link between health expenditure, CO2 emissions, and GDP growth in Netherlands, New Zealand and the United States.
Furthermore, we also estimated the Granger causality based on the ARDL model. The short-run relationship among the three variables, the coefficient value for CO2 emissions, reports a positive and significant effect with health expenditures in Ireland, Netherlands, United States, New Zealand, and Norway that means CO2 emissions increase health expenditures. The important policy is that the government actively limits carbon emissions because environmental pollution will increase health expenditures. The coefficient for GDP growth is showing the positive and significant effect between GDP and health expenditures, which shows that in the short run, the increasing level of GDP increases health expenditures. GDP growth sacrifices health factors because economic development may cause environmental pollution, and low-quality human capital forms more health losses. However, there do exist negative relations with short-run relationship running from GDP growth to health expenditures for a number of countries, including Germany and the United States. This may be the reason of the negative link between GDP and health expenditure for the case of Germany and the United States because human capital and institutional quality are in good condition. When growth increases, people's investment in physical exercise reduces the expenditure for health.
There are negative relations with short-run relationship from health expenditures to GDP growth for Germany but positive relations for the United States. Increasing health expenditures is associated with low productivity of human being because health creates disturbance for the economic growth (48). Health expenditures cannot lead to social security, efficient resource allocation, and better economies of scale in Germany (37). The human capital stock is positive and statistically significantly affects GDP growth in the United States (34). CO2 emissions have a positive and significant relation to GDP growth in Finland, Netherlands, Canada, and Germany. These countries have a high intensity of CO2 emissions due to the use of fossil fuels and rapid GDP growth. However, energy consumption and CO2 emissions do not increase the GDP growth of the United States but have a negative effect.
This study has found that health expenditure has a significant and positive effect on CO2 emissions at the level of 5% in Austria and Norway. In addition, CO2 emissions are negatively and significantly affected by health expenditures in Belgium, Sweden, the United Kingdom, and New Zealand. There are two effects on health expenditures that affect carbon emissions. The effect of health expenditures is related to population growth, thus as long as population increases, the rise in energy consumption results in greater environment pollution (33). On the other hand, health expenditures increase people's awareness of pollution and reduce carbon emissions. The first effect is significantly larger than the second effect in Austria and Norway and vice versa in Belgium, the United Kingdom, and New Zealand. In addition, GDP has a positive and significant effect on CO2 emissions in Canada, Denmark, Japan, and Spain but a negative effect on CO2 emissions in the United Kingdom, Australia, Germany, and the United States.
This study contributes to the literature in the dynamic relationship among CO2 emissions, health care expenditure, and GDP growth for the 18 OECD countries over the period of 1975–2017. We investigate the bidirectional causal relationship between health expenditure and GDP and between CO2 emissions and GDP and between health expenditure and CO2 emissions for the three ARDL models. The results show that the bootstrap ARDL analysis is useful in evaluating the effects of different socioeconomic scenarios in the context of different positions for health expenditure and environment policy in OECD countries.
Our study results showed that there is cointegration existing in Netherlands when real GDP per capita serves as the dependent variable, in New Zealand when health expenditure is the dependent variable, and in the United States when CO2 emission is the dependent variable. The short-run relationship exists in a unidirectional causality relationship from CO2 emissions to health expenditure for Germany, Ireland, Japan, Netherlands, and the United States and from health expenditure to CO2 emissions for Austria, Belgium, Sweden, and the United Kingdom. There is a bidirectional causality relationship between health expenditure and CO2 emissions in New Zealand and Norway. This empirical result supports previous researches (33, 34, 47). There is a unidirectional causality relationship from GDP to health expenditure for Belgium, Denmark, Finland, New Zealand, Sweden, Portugal, and Spain. There is a bidirectional causality relationship between GDP and health expenditure for Germany and the United States (42–44). It is unidirectional causality from CO2 emissions to GDP for Finland and Netherlands, and GDP Granger causes CO2 emissions for Australia, Belgium, Denmark, Japan, Spain, and the United Kingdom. Our study results showed the bidirectional causality relationship between Canada, Germany, and the United States (28, 37).
The most important policy of these OECD countries is to limit CO2 emissions. In addition, these countries should adopt measures and policies to protect the quality of the environment to reduce the occurrence of health diseases. Environmental quality as a contributing factor to increased health spending has been proven. Our results demonstrate a significant increase in health spending on CO2 emissions in Ireland, Netherlands, the United States, New Zealand, and Norway. In some countries, health factors are sacrificed because of GDP growth because economic development may cause environmental pollution and low-quality human capital will cause more health losses. For some economies, however, including Germany and the United States, Granger causality does have a negative correlation from GDP to health spending. This may be the reason for the negative relations between GDP and health expenditure in Germany and the United States, as institutional quality and human capital are in good condition. When growth increases, people's investment in physical exercise reduces health spending. Therefore, environmental degradation is becoming a contemporary issue, and we urgently need to reexamine health and environmental policies so that GDP growth should not increase at the expense of public health or the environment. Due to the consumption of fossil fuels by OECD countries, industrial and household natural resources contribute significantly to CO2 emissions. It seems that policy makers should study the need for investment to promote technology transfer to protect environment quality.
The datasets generated for this study are available on request to the corresponding author.
C-MW designed the research, performed the experiments, and wrote the paper. H-PH collected the data. FL analyzed the results. C-FW edited the paper.
This work was supported by Hubei Provincial Department of Education (grant number: Q20192205).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. McNown R, Sam CY, Goh SK. Bootstrapping the autoregressive distributed lag test for cointegration. Appl Econ. (2018) 50:1509–21. doi: 10.1080/00036846.2017.1366643
2. Muntean M, Guizzardi D, Schaaf E, Crippa M, Solazzo E, Olivier J, et al. Fossil CO2 Emissions of All World Countries. Luxembourg: Publications Office of the European Union (2018).
3. Yazdi S, Zahra T, Nikos M. Public healthcare expenditure and environmental quality in Iran. In: Recent Advances in Applied Economics. (2014). Available Online at: http://www.wseas.us/e-library/conferences/2014/Lisbon/AEBD/AEBD-17.pdf (accessed January 12, 2018).
4. Bank AD. ADB Annual Report 2012. Asian Development Bank (2013) Available online at: https://www.adb.org/documents/adb-annual-report-2012 (accessed October 6, 2019).
5. Grossman GM, Krueger AB. Economic growth and the environment. Q J Econ. (1995) 110:353–77. doi: 10.2307/2118443
6. Cai Y, Sam CY, Chang T. Nexus between clean energy consumption, economic growth and CO2 emissions. J Clean Prod. (2018) 182:1001–11. doi: 10.1016/j.jclepro.2018.02.035
7. List JA, Gallet CA. The environmental Kuznets curve: does one size fit all? Ecol Econ. (1999) 31:409–23. doi: 10.1016/S0921-8009(99)00064-6
8. Pata UK. Renewable energy consumption, urbanization, financial development, income and CO2 emissions in Turkey: testing EKC hypothesis with structural breaks. J Clean Prod. (2018) 187:770–9. doi: 10.1016/j.jclepro.2018.03.236
9. Selden TM, Song D. Environmental quality and development: is there a Kuznets curve for air pollution emissions? J Environ Econ Manag. (1994) 27:147–62. doi: 10.1006/jeem.1994.1031
10. Stern DI, Common MS. Is there an environmental Kuznets curve for sulfur? J Environ Econ Manag. (2001) 41:162–78. doi: 10.1006/jeem.2000.1132
11. Chen W-Y. Health progress and economic growth in the USA: the continuous wavelet analysis. Empir Econ. (2016) 50:831–55. doi: 10.1007/s00181-015-0955-6
12. Fogel RW. New sources and new techniques for the study of secular trends in nutritional status, health, mortality, and the process of aging. Hist Methods J Quant Interdiscip Hist. (1993) 26:5–43. doi: 10.3386/h0026
13. Liu Y-H, Chang W-S, Chen W-Y. Health progress and economic growth in the United States: the mixed frequency VAR analyses. Qual Quant. (2019) 53:1895–911. doi: 10.1007/s11135-019-00847-z
14. Boachie MK, Mensah IO, Sobiesuo P, Immurana M, Iddrisu A-A, Kyei-Brobbey I. Determinants of public health expenditure in Ghana: a cointegration analysis. J Behav Econ Finance Entrep Acc Transp. (2014) 2:35–40. doi: 10.12691/jbe-2-2-1
15. Lu Z-N, Chen H, Hao Y, Wang J, Song X, Mok TM. The dynamic relationship between environmental pollution, economic development and public health: evidence from China. J Clean Prod. (2017) 166:134–47. doi: 10.1016/j.jclepro.2017.08.010
16. Holtz-Eakin D, Selden TM. Stoking the fires? CO2 emissions and economic growth. J Public Econ. (1995) 57:85–101. doi: 10.1016/0047-2727(94)01449-X
17. Akbostanci E, Türüt-Aşik S, Tunç GI. The relationship between income and environment in Turkey: is there an environmental Kuznets curve? Energy Policy. (2009) 37:861–7. doi: 10.1016/j.enpol.2008.09.088
18. Bimonte S. Information access, income distribution, and the Environmental Kuznets Curve. Ecol Econ. (2002) 41:145–56. doi: 10.1016/S0921-8009(02)00022-8
19. Lise W. Decomposition of CO2 emissions over 1980–2003 in Turkey. Energy Policy. (2006) 34:1841–52. doi: 10.1016/j.enpol.2004.12.021
20. Fodha M, Zaghdoud O. Economic growth and pollutant emissions in Tunisia: an empirical analysis of the environmental Kuznets curve. Energy Policy. (2010) 38:1150–6. doi: 10.1016/j.enpol.2009.11.002
21. Cole MA, Rayner AJ, Bates JM. The environmental Kuznets curve: an empirical analysis. Environ Dev Econ. (1997) 2:401–16. doi: 10.1017/S1355770X97000211
22. Halicioglu F. An econometric study of CO2 emissions, energy consumption, income and foreign trade in Turkey. Energy Policy. (2009) 37:1156–64. doi: 10.1016/j.enpol.2008.11.012
23. Saboori B, Sulaiman J, Mohd S. Economic growth and CO2 emissions in Malaysia: a cointegration analysis of the environmental Kuznets curve. Energy Policy. (2012) 51:184–91. doi: 10.1016/j.enpol.2012.08.065
24. Saboori B, Sulaiman J. CO2 emissions, energy consumption and economic growth in Association of Southeast Asian Nations (ASEAN) countries: a cointegration approach. Energy. (2013) 55:813–22. doi: 10.1016/j.energy.2013.04.038
25. Jebli MB, Youssef SB, Ozturk I. Testing environmental Kuznets curve hypothesis: the role of renewable and non-renewable energy consumption and trade in OECD countries. Ecol Indic. (2016) 60:824–31. doi: 10.1016/j.ecolind.2015.08.031
26. Gerdtham U-G, Löthgren M. New panel results on cointegration of international health expenditure and GDP. Appl Econ. (2002) 34:1679–86. doi: 10.1080/00036840110116397
27. Baltagi BH, Moscone F. Health care expenditure and income in the OECD reconsidered: evidence from panel data. Econ Model. (2010) 27:804–11. doi: 10.1016/j.econmod.2009.12.001
28. Wang K-M. Health care expenditure and economic growth: quantile panel-type analysis. Econ Model. (2011) 28:1536–49. doi: 10.1016/j.econmod.2011.02.008
29. Albulescu CT, Oros C, Tiwari AK. Is there any convergence in health expenditures across EU countries? Econ Bull. (2017) 37:2095–101. Retrieved from: https://ideas.repec.org/a/ebl/ecbull/eb-17-00577.html
30. Erçelik G. The relationship between health expenditure and economic growth in Turkey from 1980 to 2015. J Polit Econ Manag. (2018) 1:1–8. Retrieved from: https://dergipark.org.tr/tr/pub/jopem/issue/36356/369537
31. Murthy VN, Okunade AA. Determinants of US health expenditure: Evidence from autoregressive distributed lag (ARDL) approach to cointegration. Econ Model. (2016) 59:67–73. doi: 10.1016/j.econmod.2016.07.001
32. Beatty TK, Shimshack JP. Air pollution and children's respiratory health: a cohort analysis. J Environ Econ Manag. (2014) 67:39–57. doi: 10.1016/j.jeem.2013.10.002
33. Chaabouni S, Zghidi N, Mbarek MB. On the causal dynamics between CO2 emissions, health expenditures and economic growth. Sustain Cities Soc. (2016) 22:184–91. doi: 10.1016/j.scs.2016.02.001
34. Chaabouni S, Saidi K. The dynamic links between carbon dioxide (CO2) emissions, health spending and GDP growth: a case study for 51 countries. Environ Res. (2017) 158:137–44. doi: 10.1016/j.envres.2017.05.041
35. Chaabouni S, Abednnadher C. The determinants of health expenditures in Tunisia: an ARDL bounds testing approach. Int J Inf Syst Serv Sect. (2014) 6:60–72. doi: 10.4018/ijisss.2014100104
36. Zaidi S, Saidi K. Environmental pollution, health expenditure and economic growth in the Sub-Saharan Africa countries: Panel ARDL approach. Sustain Cities Soc. (2018) 41:833–40. doi: 10.1016/j.scs.2018.04.034
37. Ghorashi N, Rad AA. CO2 emissions, health expenditures and economic growth in Iran: application of dynamic simultaneous equation models. growth. JCHR. (2017) 6:109–16. Retrieved from: https://pdfs.semanticscholar.org/4df6/4a73ad03b0605efcb216e95789c52645b9f3.pdf
38. Pesaran MH, Shin Y, Smith RJ. Bounds testing approaches to the analysis of level relationships. J Appl Econom. (2001) 16:289–326. doi: 10.1002/jae.616
39. Dickey DA, Fuller WA. Likelihood ratio statistics for autoregressive time series with a unit root. Econom J Econom Soc. (1981) 1057–2. doi: 10.2307/1912517
40. Kwiatkowski D, Phillips PC, Schmidt P, Shin Y. Testing the null hypothesis of stationarity against the alternative of a unit root: how sure are we that economic time series have a unit root? J Econom. (1992) 54:159–78. doi: 10.1016/0304-4076(92)90104-Y
41. Zivot E, Andrews DWK. Further evidence on the great crash, the oil-price shock, and the unit-root hypothesis. J Bus Econ Stat. (2002) 20:25–44. doi: 10.1198/073500102753410372
42. Amiri A, Ventelou B. Granger causality between total expenditure on health and GDP in OECD: Evidence from the Toda–Yamamoto approach. Econ Lett. (2012) 116:541–4. doi: 10.1016/j.econlet.2012.04.040
43. Elmi ZM, Sadeghi S. Health care expenditures and economic growth in developing countries: panel co-integration and causality. Middle-East J Sci Res. (2012) 12:88−91. doi: 10.5829/idosi.mejsr.2012.12.1.64196
44. Mladenović I, Milovančević M, Mladenović SS, Marjanović V, Petković B. Analyzing and management of health care expenditure and gross domestic product (GDP) growth rate by adaptive neuro-fuzzy technique. Comput Hum Behav. (2016) 64:524–30. doi: 10.1016/j.chb.2016.07.052
45. Ghosh S. Examining carbon emissions economic growth nexus for India: a multivariate cointegration approach. Energy Policy. (2010) 38:3008–14. doi: 10.1016/j.enpol.2010.01.040
46. Cherni A, Jouini SE. An ARDL approach to the CO2 emissions, renewable energy and economic growth nexus: Tunisian evidence. Int J Hydrog Energy. (2017) 42:29056–66. doi: 10.1016/j.ijhydene.2017.08.072
47. Wang Z, Asghar MM, Zaidi SAH, Wang B. Dynamic linkages among CO2 emissions, health expenditures, and economic growth: empirical evidence from Pakistan. Environ Sci Pollut Res. (2019) 26:15285–99. doi: 10.1007/s11356-019-04876-x
Keywords: health expenditure, CO2 emissions, GDP growth, long run relation, bootstrap ARDL
Citation: Wang C-M, Hsueh H-P, Li F and Wu C-F (2019) Bootstrap ARDL on Health Expenditure, CO2 Emissions, and GDP Growth Relationship for 18 OECD Countries. Front. Public Health 7:324. doi: 10.3389/fpubh.2019.00324
Received: 30 July 2019; Accepted: 22 October 2019;
Published: 20 November 2019.
Edited by:
Mihajlo (Michael) Jakovljevic, Lund University, SwedenReviewed by:
Khalid Zaman, University of Wah, PakistanCopyright © 2019 Wang, Hsueh, Li and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chien-Ming Wang, Y213YW5nOEBnbWFpbC5jb20=; Cheng-Feng Wu, d3VjaGVuZ2ZlbmdAaGJ1ZS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.