 Belinda-Rose Young1,2*
Belinda-Rose Young1,2* Clement K. Gwede2,3
Clement K. Gwede2,3 Bria Thomas2Coralia Vázquez-Otero2Aldenise Ewing2Alicia L. Best2
Bria Thomas2Coralia Vázquez-Otero2Aldenise Ewing2Alicia L. Best2 Claudia X. Aguado Loi2,4
Claudia X. Aguado Loi2,4 Dinorah Martinez-Tyson2Tali Schneider2Cathy D. Meade2,3Julie A. Baldwin2,5Carol Bryant2
Dinorah Martinez-Tyson2Tali Schneider2Cathy D. Meade2,3Julie A. Baldwin2,5Carol Bryant2- 1Department of Health Behavior, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States
- 2Prevention Research Center, College of Public Health, University of South Florida, Tampa, FL, United States
- 3Moffitt Cancer Center & Research Institute and Morsani, College of Medicine, University of South Florida, Tampa, FL, United States
- 4Health Sciences and Human Performance Department, University of Tampa, Tampa, FL, United States
- 5Health Sciences Department, Northern Arizona University, Flagstaff, AZ, United States
Background: We examined colorectal cancer screening (CRCS) intervention effectiveness, through the effect sizes associated with: (1) screening modality, (2) intervention level (e.g., client-directed), and (3) intervention component (e.g. client reminders) within published CRCS intervention systematic reviews (SRs).
Methods: A search of peer-reviewed CRCS SRs that were written in English was employed utilizing five databases: CINAHL, Cochrane Library, rTIPS, PubMed, and PsycINFO EBSCOHOST. SRs that included CRCS interventions with a randomized controlled trial, quasi-experimental, or single arm design were eligible. Data on effect sizes by screening modality, intervention level, and intervention component were extracted and synthesized.
Results: There were 16 eligible CRCS intervention SRs that included 116 studies published between 1986 and 2013. Reviews organized data by CRCS screening modality, or intervention component. Effect size reporting varied by format (i.e., ranges, medians of multiple studies, or effect size per study), and groupings of modalities and components. Overall, the largest effect sizes were for studies that utilized a combination of colonoscopy, fecal occult blood test (FOBT), and sigmoidoscopy as screening options (16–45 percentage point difference).
Conclusions: Evidence suggests that CRCS interventions which include a combination of screening modalities may be most effective. This is the first SR to examine effect sizes of published CRCS SRs. However, because some SRs did not report effect sizes and there were tremendous variability reporting formats among those that did, a standard reporting format is warranted. Synthesizing findings can contribute to improved knowledge of evidence-based best-practices, direct translation of findings into policy and practice, and guide further research in CRCS.
Introduction
Rationale
Colorectal cancer (CRC) is the second leading cause of cancer-related deaths in the U.S. (1, 2). Despite steady decreases in CRC incidence and mortality, screening modalities are still markedly underutilized among some populations. Racial/ethnic minorities, medically underserved, and rural residents experience the highest CRC mortality rates in the U.S.(3). In addition, The Guide to Community Preventive Services (The Community Guide) identifies a number of evidence gaps for effective colorectal cancer screening (CRCS) interventions (4–10).
Objectives and Research Question
On the hierarchy of evidence, systematic reviews represent the highest level of evidence and are often used by practitioners, policy-makers, and researchers to inform their work (11, 12). Several systematic reviews that examine CRCS interventions exist; however, the screening modality (i.e., type of screening test), priority population, and intervention level (i.e., client, provider, or system-directed) and component (i.e., behavior change strategy) vary widely. In this systematic review of systematic reviews, we sought to answer the question: what are the effective evidence-based interventions for CRCS, their effect size, and their characteristics? We synthesize evidence from published systematic reviews of CRCS interventions to provide a comprehensive and coherent picture of what is known, and to identify gaps in knowledge. The objective of this systematic review was to examine the effect sizes of CRCS interventions by (1) screening modality, (2) intervention level, and (3) intervention component.
In this systematic review, we examine published systematic reviews of interventions whose primary or secondary outcome was increased CRCS. To identify CRCS best-practices and address evidence gaps, we aimed to abstract the effect size(s) associated with the interventions. Through this review we, indirectly and to some extent, also assessed the quality of effect size reporting by CRCS systematic reviews more largely. The synthesis of evidence from this paper benefits the field by undergirding effective CRCS policy and practice efforts, ultimately leading to better patient care.
Methods
Search Strategy
A comprehensive search of published CRCS intervention systematic reviews was conducted, adhering to the Cochrane Collaboration guidelines (Figure 1) (13). In collaboration with experienced clinical research librarians, we performed a wide search in electronic databases (CINAHL, rTIPS, PubMed, Cochrane Library, and PsycINFO EBSCOHOST), and reviewed the reference section of each systematic review to see if they listed additional published CRCS systematic reviews. Among the electronic databases, PubMed included e-publications (i.e., “Ahead of print citations”), which decreased the risk of missing potential publications (14).
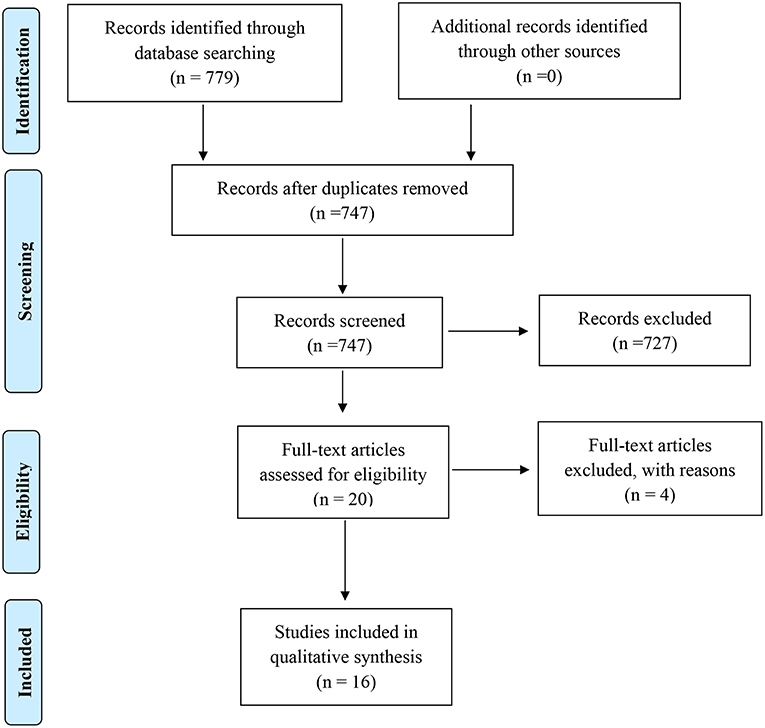
Figure 1. Flow diagram of the studies retrieved for the review.
Our search aimed to locate any published systematic review that focused on improving CRCS through client, provider, and/or system-directed interventions. Search terms included (1) database-specific terms (e.g., MeSH terms) (Table 1) and identified key words for the databases that use booleans, or (2) only keywords for databases that do not have database-specific terms (e.g., rTIPS, Cochrane Library). The keywords were informed by the literature and added to by the healthcare librarians and experts in the field.
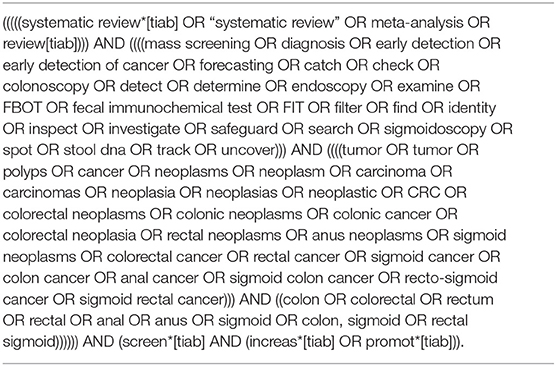
Table 1. Syntax for identifying CRCS intervention-focused systematic reviews within PubMed.
Participants, Interventions, and Comparators
Eligible systematic reviews included those that were published in English, included studies conducted within the U.S. and/or its territories, utilized a RCT, quasi-experimental, or single arm intervention design, and whose primary or secondary outcome was CRCS uptake with any of the established screening modalities recommended by the U.S. Preventive Services Task Force (15). Studies were restricted to U.S.-based studies written in English in order to facilitate comparison among a more homogeneous group (e.g., federal laws, governing bodies, territories subject to recommendations by U.S. Preventive Services Task Force). Articles that solely focused on improving intentions to be screened were not included. Ineligible systematic reviews included: (1) all other review types (e.g., narrative literature reviews); or (2) systematic reviews that did not include any of the aforementioned design types or whose primary or secondary outcome was not CRCS uptake. Since our aim was to better understand the scope of existing published literature, we did not include gray literature.
The eligible CRCS modalities included: colonoscopy, sigmoidoscopy, CT colonography or virtual colonoscopy, double contrast barium enema (DCBE), or any stool test (i.e., DNA, fecal immunochemical test [FIT], fecal occult blood test [FOBT], high sensitivity guaiac FOBT [gFOBT]) as recommended by the U.S. Preventive Services Task Force (15). All other forms of CRCS were excluded from this review.
The research team co-developed a standardized review form to assess potential study eligibility; and based on the title and abstract, potentially eligible systematic reviews were selected by the primary reviewer using that form. Both the primary and secondary reviewer searched the full-text of each potentially eligible systematic review. If there were doubts concerning whether the systematic review met the eligibility criteria, the article was brought to the larger research team. The team then used the review form to systematically examine the article in question. Overall, at least two research team members assessed each systematic review for eligibility. The reference sections of the eligible systematic reviews were examined (i.e., hand-searched) to determine if any additional reviews were potentially eligible.
Data Sources, Studies Sections, and Data Extraction
The research team was interested in gathering evidence of effective interventions more generally; therefore, we did not employ the entire PICO (participants, intervention, comparison, and outcome) method—which has been used within systematic reviews to identify components of clinical evidence. Employing the entire PICO method would have limited our understanding of available evidence since it would require us to hone in on a specific population (16–18). However, the portions of PICO that we did utilize were intervention and outcome—that is, systematic reviews had to include intervention studies whose primary or secondary outcomes centered on an increase in CRCS as an outcome of the intervention.
A data abstraction form was developed to assess and log the characteristics of the eligible systematic reviews and the effect sizes of the studies included within the systematic reviews. The items collected in the data abstraction form included: author(s); year of publication; eligibility criteria for publication; number of studies within the publication; study setting; and effect sizes (e.g., median, ranges) by screening modality, intervention level(s), and intervention component(s). This form was created, reviewed and pretested by three authors prior to abstraction. After extensive training and discussion, one author abstracted the data, while another independently reviewed all data. Minor disagreements were resolved by an arbitrator. The individual articles were not assessed for data quality as they were already reported within the respective systematic review.
Data Analysis
The effect size is a measure to describe the magnitude of effect, which is a quantification of the difference between two groups in the observed outcome (here, screening uptake). The effect size can also be described as the percentage point difference between two groups, or the percent change from baseline of a single group. Effect sizes are often more telling than tests of statistical significance (p-values) (19). This is because they show the magnitude of difference between two groups, as opposed to stating that there was an observed difference (19). Thus, the effect size can help us to prioritize one effective intervention over another.
Data were synthesized in two ways. First, data were synthesized more generally by screening modality, intervention level, and intervention component. Next, to address CRCS evidence gaps as identified by The Community Guide, data were synthesized around the seven gaps (as detailed in the results section).
Results
Study Selection and Characteristics
Out of 747 systematic reviews screened from five databases, 16 systematic reviews met the inclusion criteria (2.14%) (Figure 1). Most reviews were ineligible because they did not include CRCS studies, or because they did not include a behavioral intervention (e.g., focused on attitudes and beliefs of certain cancer risk factors). The 16 systematic reviews contained 206 studies, of which 116 were unique. The publication dates of the studies included within the 16 systematic reviews ranged from 1986 to 2013, representing over 27 years' worth of knowledge. Of the 16 eligible systematic reviews, 12 reported information about effect sizes.
Each of the 16 systematic reviews varied in their inclusion criteria used to determine study eligibility. Though some eligibility criteria could be inferred based upon the descriptions of the studies examined, we did not denote the eligibility criteria if they were not explicitly stated within the systematic review. The most frequent criteria (Table 2) included research design restriction (n = 9; 56%), an increase in CRCS as the primary outcome (n = 7; 44%), and CRCS behavioral intervention (n = 16). Six systematic reviews, published between 2003 and 2012, containing studies between 1986 and 2007, required eligible studies to be the primary scientific publication, and not a secondary article of the same study. Six systematic reviews published between 2008 and 2012 had a study publication date range restriction (collectively, 1997–2010) for their inclusion criteria.
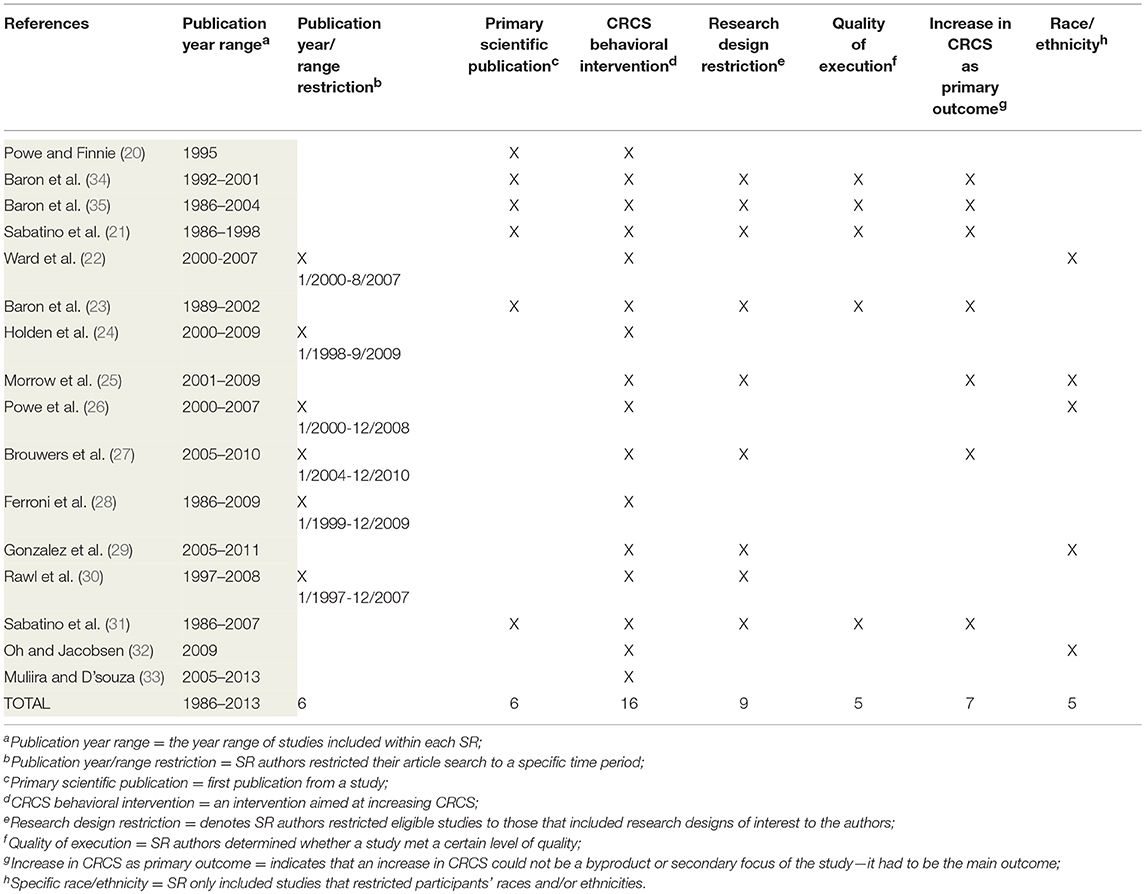
Table 2. Frequent inclusion criteria across the 16 systematic reviews.
Less than half included restrictions on quality of study execution (n = 5; 31%), race/ethnicity (n = 5; 31%), intervention level or component (n = 2, 13%), and age range (n = 2, 13%). A minority of systematic reviews (n = 5) included a restriction that was not used within other reviews: specific screening modality; cultural appropriateness of intervention; intervention sample size; setting of intervention; and study effect sizes reported (25, 26, 28, 29, 33).
Synthesized Findings
Across the 16 eligible systematic reviews, findings included interventions at the three levels described by The Community Guide. Briefly, these are client-directed/oriented (e.g., small-media, mass-media, education/counseling, structural barriers), provider-directed/oriented (e.g., assessment and feedback, computer generated reminders), and system-directed/oriented (e.g., shared decision making, systematic screening, patient navigator, referral system). Many systematic reviews focused on one specific intervention level, mostly client-directed (n = 9; 56.25%) (20, 25, 27–29, 32–35). However, five additional systematic reviews (31.25%) included client-directed and at least one other intervention level (22, 24, 26, 30, 31). Table 3 describes the intervention level(s) and component(s) of each eligible SR. The interventions took place in several settings (e.g., health clinics, churches, community events, homes).
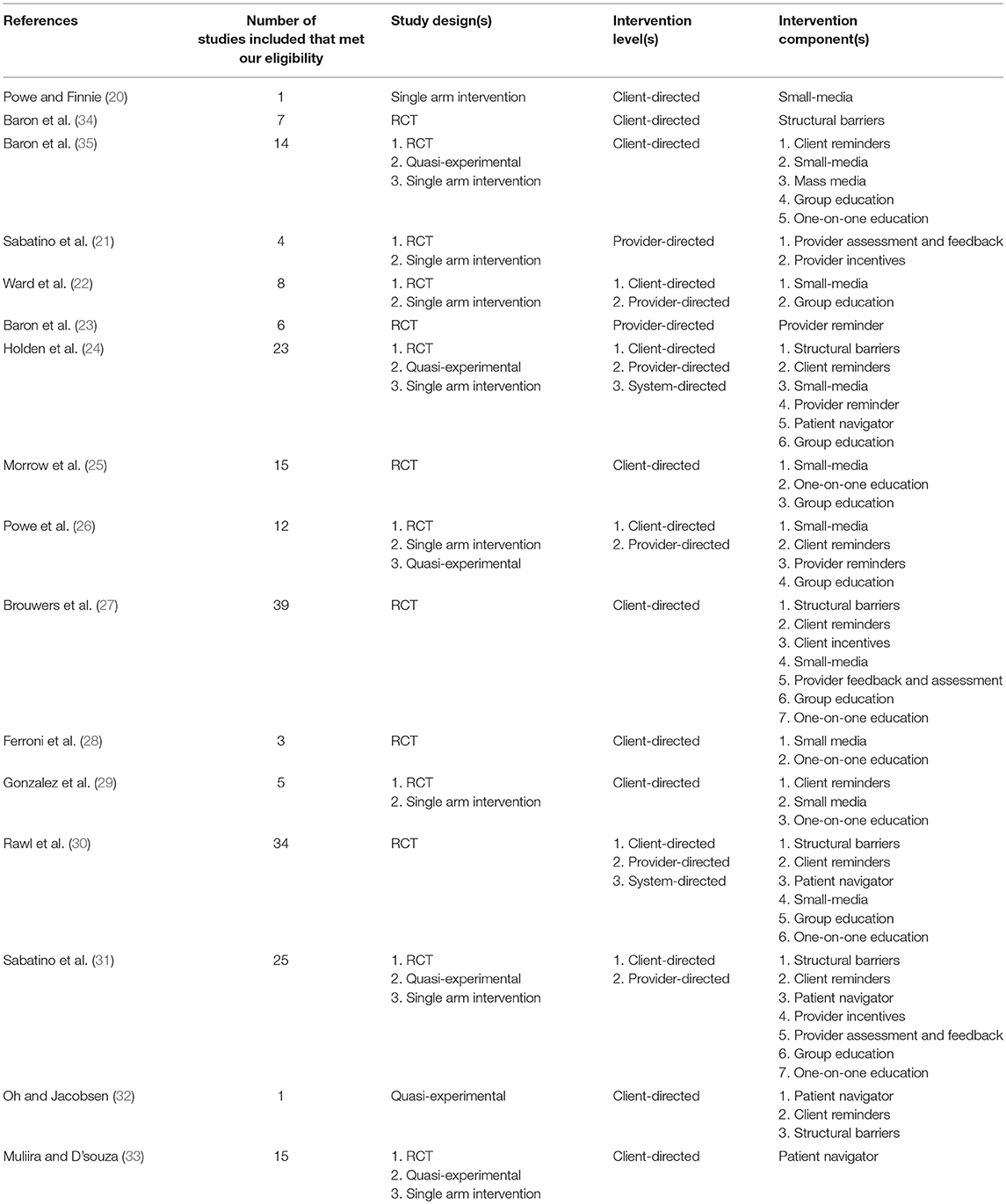
Table 3. Characteristics of eligible systematic reviews.
Effect Size
Authors of the published CRCS systematic reviews organized the papers by intervention component or screening modality, and then described the studies accordingly. Some were individually described, while others were presented in an aggregated format. In most cases, the systematic review authors described the effect sizes in the same way they described study characteristics—individually or aggregated. If stated, the effect sizes were described as: (1) the median difference in percentage points (compared to the control group); (2) range of percentage point difference; or (3) both.
Because some systematic reviews included studies at different intervention levels and varied in intervention components (i.e., behavior change strategies), it was possible for a single systematic review to be utilized multiple times in our analysis. For instance, a systematic review could contain studies that included a client-directed group education intervention, and other studies that were provider-directed, with the intervention component being provider incentives. Thus, one systematic review could provide effect size data for multiple screening modalities, intervention levels, and/or intervention components. We thought this was the strongest approach to analyzing the data, because it allowed us to accurately reflect the breadth of information and prevalence of effect size reporting. Ultimately, we examined effect sizes by: (1) screening modality, (2) intervention level, and (3) intervention component by intervention level.
Effect Size by Screening Modality
Among systematic reviews that assessed the effect size by screening modality, data from studies were reported in the context of a particular screening modality only, a combination of modalities, or both (i.e., included both a predetermined group of modalities compared and a singular option) (Table 4). Eight systematic reviews included a combination(s) of screening modalities in their analysis. The frequency of systematic reviews that contained a modality within a particular combination is as follows: colonoscopies (n = 6), sigmoidoscopy (n = 6), FOBT (n = 6), FIT (n = 3), DCBE (n = 3), and endoscopic (n = 2). Seven systematic reviews included at least one study that did not report the screening modality, but rather reported only the difference in screening uptake. The effect size by screening modality varied both within modality and across modalities.
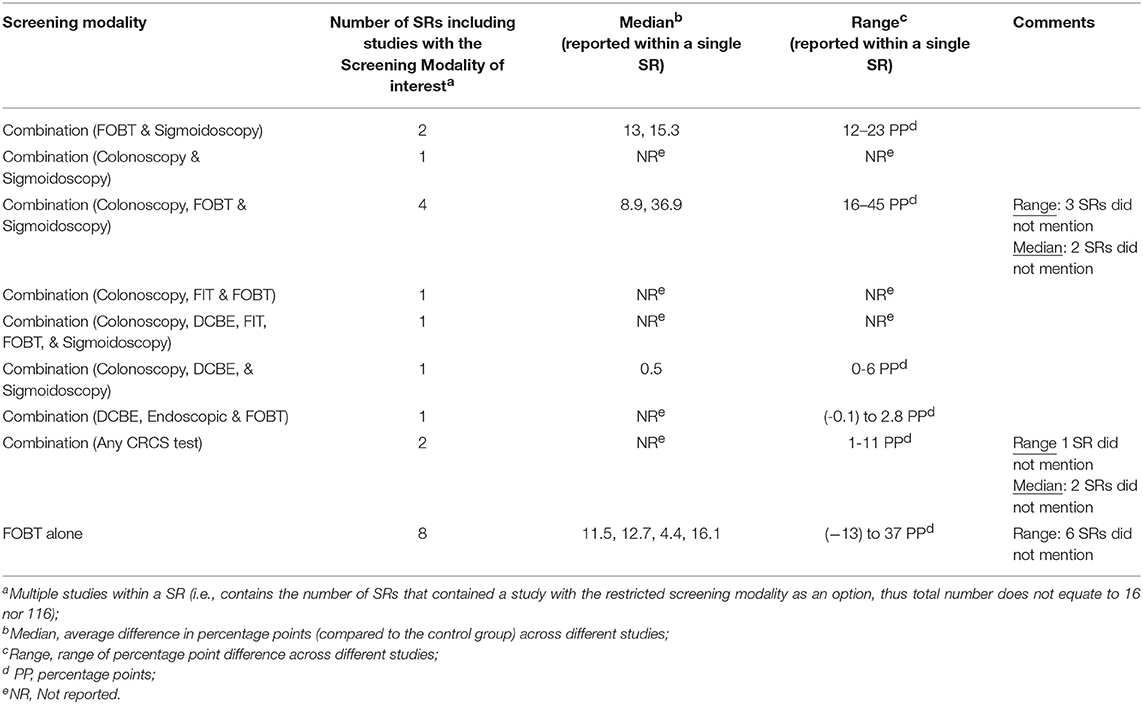
Table 4. Magnitude of effects medians and range by screening modality (as a screening outcome).
Half of the systematic reviews (n = 8) included a section of studies that used FOBT as the sole screening outcome and, among available data, reported a percentage point difference ranging from −13 to 37%. It is important to note that of those eight systematic reviews, only two reported a range; and half reported a median percentage point increase (4.4, 11.5, 12.7, and 16.1). The systematic reviews that did not include an effect size typically indicated that there was an “increase in screening.”
Effect Size by Intervention Level
We also assessed the effect size by intervention level. Fourteen of the 16 systematic reviews included at least one study that intervened at the client-level (−13 to 42 percentage points). Seven systematic reviews included at least one study that intervened at the provider-level (−0.1 to 23 percentage points) (21–24, 26, 30, 31). Two systematic reviews included a study that intervened at the system-level (7–28 percentage points) (24, 30).
Effect Size by Intervention Component
Among the client-directed interventions, the most frequent intervention component was one-on-one education (n = 4) (effect sizes not reported), client-reminders (n = 3) (0.0–0.6 percentage points), and small-media (n = 3) (effect sizes not reported). However, nine SRs presented a combination of client-directed intervention components—most of which included client-reminders (n = 5) (−7 to 42 percentage points). The least frequent component, overall, was the use of patient navigators (n = 1) (effect sizes not reported).
Fewer systematic reviews included either provider-directed (n = 7), or system-directed interventions (n = 2). Within provider-directed interventions, provider reminder (n = 2) (15.3 percentage point median reported in one of the systematic reviews), provider assessment and feedback (n = 2) (13 to 45 percentage point median range), and provider incentives (n = 2) (−0.1 to 2.8 percentage points reported in one of the systematic reviews) were the most common. The system-directed intervention components included patient navigators and a patient-referral system (7–28 percentage points) and/or a multi-component office-based intervention (e.g., checklists, chart stickers, audits) (effect size not reported).
Evidence for the Community Guide
The Community Guide has identified seven CRCS intervention areas that currently have “insufficient evidence.” These intervention areas span multiple intervention levels and include various intervention components and screening modalities. We use data from our systematic review to corroborate and/or inform the seven CRCS intervention areas gaps (Table 5).
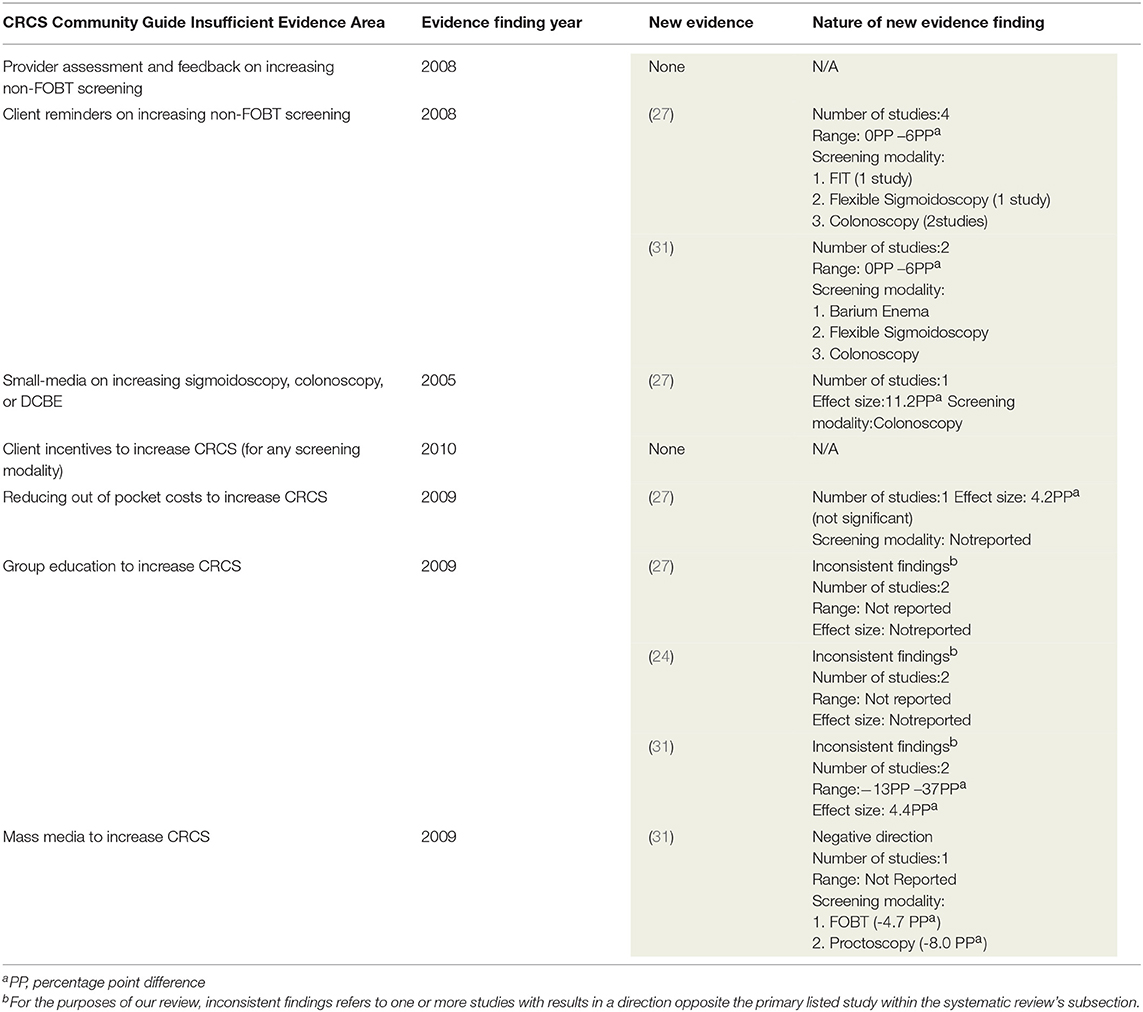
Table 5. The Community Guide's Areas of Insufficient CRCS evidence identified by this study.
Gap 1: Impact of Provider Assessment and Feedback on Increasing Non-FOBT Screening
We found two systematic reviews that included information about provider assessment interventions (21, 31). Both reviews included the same three studies. However, only one of the studies included a screening modality other than FOBT-Sigmoidoscopy-for which there was no CRCS uptake change (36).
Gap 2: Impact of Client Reminders on Increasing Non-FOBT Screening
Five of the systematic reviews included studies with a client reminder intervention component; however, two of those included FOBT as the screening modality outcome (29, 35). Of the remaining three systematic reviews, two included studies (n = 11 studies; n = 33 studies) with multiple screening modality outcomes (27, 30). One systematic review found significant, positive percentage point change (3–40.8) among four studies where the screening modality outcome was FIT, flexible sigmoidoscopy, or colonoscopy; with colonoscopy studies being associated with the highest percentage point differences (11.7 to 40.8) (27). Of the 33 studies included in the second systematic review, 10 included an outcome of FOBT and 16 included an outcome of “any CRCS test” (30). The remaining seven used endoscopy procedures (flexible sigmoidoscopy, or colonoscopy), five of which reported to have significant intervention effects; however, due to variable reporting styles (“actual percent completing the test, to percent increase from baseline, to odds ratios,” p.177), authors indicated that comparisons were unable to be made between the studies. The last applicable systematic review included two studies with barium enema, flexible sigmoidoscopy, or colonoscopy as the outcome (31). Collectively, these studies contained five intervention arms, and showed a median increase of 0.5 percentage points (range: 0.0 to 6.0).
Gap 3: Impact of Small Media on Increasing Sigmoidoscopy, Colonoscopy, or DCBE
Seven systematic reviews included small media interventions; however, three did not state the testing outcome of the studies, and one included FOBT as the screening modality outcome. Three systematic reviews remained that included the test outcomes of interest (25–27). One systematic review included nine studies that had the outcome option of “any screening modality,” whereas the last study only included colonoscopies as an outcome (11.2 percentage points) (27). Another systematic review included seven studies that used small media, but the effect estimate chosen (odds ratio) was only available for two of the studies, for which multiple screening modalities were an option (25). While the last systematic review included studies with the desired intervention and screening modality, they either included multiple intervention components, thus muddying the understanding of small-media's direct impact, or no effect estimates were provided (26).
Gap 4: Client Incentives to Increase CRCS for Any Screening Modality
No studies in the 16 systematic reviews that we examined discussed this intervention component.
Gap 5: Reducing Out-of-Pocket Costs to Increase CRCS
One systematic review included this intervention component; however, the findings were not significant (4.2 percentage points) (27).
Gap 6: Impact of Client Education for Increasing CRCS
Six systematic reviews included studies with group education as an intervention component; however, one indicated that there was “insufficient evidence” (35). Two systematic reviews included studies that employed multiple components within their intervention, thus making it difficult to determine which component was most impactful (22, 25). Three systematic reviews included studies that only utilized group education as the intervention component, yet had inconsistent findings (24, 27, 31). For example, one systematic review included studies where the control group had a higher increase in CRCS than the intervention group; in another study (within the same SR) the opposite was true (27). Another systematic review included two group education intervention studies in their review, with one showing a negative effect (-7%) and the other a positive increase in screening (12%) (24). The last systematic review included two studies with a median of 4.4 percentage points, and a range of −13 to 37% (31). Our findings mirror those of The Community Guide—there is inconsistent evidence.
Gap 7: Impact of Mass Media on CRCS
Only one systematic review included a study that utilized mass media as the intervention (31). Two screening modality options were available—FOBT and proctoscopy—and both yielded results in a negative direction (−4.7 and −8.0 percentage points, respectively). More evidence is needed about utility and feasibility of mass media CRCS interventions.
Discussion
Summary of Main Findings
Through this systematic review of systematic reviews, we were able to examine 116 CRCS studies and found that consistently, based on effect sizes, the most effective intervention characteristics were those that: provided clients with the option to select from a colonoscopy, FOBT, or sigmoidoscopy screening modality (16–45 PP); targeted systems through patient navigators or a patient-referral structures (7–28 PP); or intervened at the provider-level through provider assessment and feedback (13–45 PP). By seeking to understand the most effective CRCS evidence-based interventions and their characteristics, we were able to provide a synthesis of effect estimates by screening modality, intervention level, and intervention component. Furthermore, our findings help to fill in some of the gaps identified by The Community Guide, and reinforce what current evidence is needed.
The interpretation of individual or a group of studies within the context of the totality of evidence can provide better decision aids, inform guidelines, and advance health policies. The results of individual studies may be misleading due to potential variation in findings and interpretation (37). Thus, to help inform clinical and research decisions, we synthesized all available CRCS intervention data from eligible systematic reviews. We assessed interventions to increase CRCS, which contributes to improved knowledge of the impact of screening modality, intervention level, and/or intervention component on CRCS uptake. Using effect sizes (rather than p-values) improves interpretation of intervention results because it facilitates an understanding of the magnitude and direction of the significance. Ultimately, this enables consistent evidence-based decision-making.
Strengths
This systematic review included a comprehensive search strategy, guided by expert opinion, and utilized five separate electronic databases. We followed Cochrane Collaboration guidelines and used a two-reviewer approach with arbitration as necessary, and larger research team input. We also included 27 years' worth of published data through 16 systematic reviews that were nuanced, yet consistent in purpose.
For the systematic reviews that reported summary statistics (n = 12), we were able to either corroborate conclusions or add evidence to six of the seven gaps identified by The Community Guide. These findings represent an important step toward advancing the CRCS intervention evidence base knowledge. Although four of the 16 systematic reviews did not include summary statistics, our analysis of these provided valuable evidence on the types of CRCS interventions being implemented, including screening modality, intervention level, and intervention components.
Limitations
Although our systematic review included 116 unique studies, our purpose was to get a better understanding of the effect sizes and the best evidence by abstracting data at the systematic review level. We also, in a sense, were evaluating the structure of, and what was missing from, CRCS intervention systematic reviews. Findings reported were based on available evidence. Because effect sizes were not reported within every category (e.g., intervention component), it is possible that the ranges for a particular category could be wider.
While we were able to quantify that the 16 systematic reviews included 116 unique studies by reviewing the reference sections, we are not always told (within the systematic review itself) which studies were examined to answer each of their research questions. Because we abstracted data at the systematic review level, it is possible that some systematic reviews included the same studies (to answer similar research questions), thus resulting in more evidence for a particular category (e.g., screening modality, intervention level, intervention component) or any of its sub-categories.
Finally, since the focus of this systematic review was to examine the evidence at the systematic review level, the reviewers did not examine the studies within each systematic review. Thus, we cannot determine if the lack of effect size reporting from four systematic reviews was due to the systematic review authors' omission, or the lack of reporting by the study authors. This information would be helpful for prioritizing future reporting directives.
Future Directives and Implications for Research, Policy, and Practice
This review of systematic reviews has broadened our understanding of prevailing evidence. Gaining a deeper insight into what CRCS interventions are truly promising provides a sound basis for clinical research translation into best practices and further research. In addition, it decreases the likelihood of wasting resources, and, most importantly, can lead to an increase in CRCS among individuals with greatest risk. We provided data that begins to fill some of the gaps in the CRCS evidence base identified by The Community Guide. For example, we found that while most interventions were aimed at the client-directed level, the interventions conducted at system and provider-levels had the most marked effects. Further, interventions that offered another screening modality in addition to FOBT were often more effective than when FOBT was the sole option. Nonetheless, a number of questions remain about the evidence of effectiveness for certain intervention components and CRCS modalities. Additionally, questions about the reporting structure of CRCS systematic reviews emerged. For example, many systematic reviews reported a summary statistic (e.g., effect size median), making it easier for the reader to understand and apply the information. However, some systematic reviews did not, which made it more challenging to compare data within and across systematic reviews.
Future research should examine and propose criteria for reporting effect sizes for screening uptake in systematic reviews. If necessary intervention features are missing, then the use of the systematic review for program planning, research and funding decisions is less appreciable. Failure to publish effect sizes of studies included within a systematic review may lead to a lack of research uptake. Variance in effect size reporting among CRCS systematic reviews calls for the creation of minimum standards that could also be applied to systematic reviews more widely, possibly leading to greater uptake (37). Such standards may result in a trickle-down effect of increased effect size reporting within publications of individual studies. These enhancements will aid in research interpretation, better practice decision-making, and overall improved care.
Conclusion
This study provides a systematic review of available peer-reviewed evidence on CRCS interventions. Findings suggest that CRCS interventions that utilized a combination of colonoscopy, FOBT, and sigmoidoscopy screening modalities, or targeted systems through patient navigators or a patient-referral structures, or intervened at the provider-level through provider assessment and feedback were most effective. Evidence from this study provides public health stakeholders with the information needed to make informed decisions about potential interventions to increase CRCS interventions. Findings also illuminate gaps in knowledge that should be prioritized by future research.
Author Contributions
BY and CV-O contributed to the design of the study, data acquisition, data interpretation, manuscript development and revisions, and approved the final version of the submitted manuscript. CG, BT, AE, CA, DM-T, CM, JB, and CB contributed to the design of the study, data interpretation, manuscript development and revisions, and approved the final version of the submitted manuscript. AB contributed to data interpretation, manuscript revisions, and approved the final version of the submitted manuscript. TS contributed to the design of the study, manuscript development and revisions, and approved the final version of the submitted manuscript.
Funding
This publication was supported by the Cooperative Agreement Number, 1U48DP005024-01, funded by the Centers for Disease Control and Prevention—Prevention Research Centers Program. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the following Shimberg Library reference librarians John Orriola, MA, M.Ed, AHIP, Allison M. Howard, MLIS, AHIP, and Randy Polo, J.D., M.A. for their assistance in the search strategy.
References
1. American Cancer Society. Cancer Facts & Figures. Atlanta, GA: American Cancer Society. (2017). Available online at: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2017/cancer-facts-and-figures-2017.pdf
2. U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2013 Incidence and Mortality Web-Based Report. (2016). US Department of Health and Human Services, National Cancer Institute, CDC. Available online at: http://www.cdc.gov/uscs (accessed October 1, 2018).
3. Jackson CS, Oman M, Patel AM, Vega KJ. Health disparities in colorectal cancer among racial and ethnic minorities in the United States. J Gastrointest Cancer. (2016) 7(Suppl. 1): S32–43. doi: 10.3978/j.issn.2078-6891.2015.039
4. The Guide to Community Preventive Services. Cancer Prevention and Control, Provider-Oriented Screening Interventions: Provider Assessment and Feedback – Colorectal Cancer. US Department of Health and Human Services, CDC. (2008). Available online at: https://www.thecommunityguide.org/sites/default/files/Cancer-Screening-Provider-Assessment-and-Feedback-Archive-Colorectal-FOBT_1.pdf (accessed October 1, 2018).
5. The Guide to Community Preventive Services. Cancer Prevention and Control, Client-Oriented Screening Interventions: Client Reminders – Colorectal Cancer. US Department of Health and Human Services, CDC. (2008). Available online at: https://www.thecommunityguide.org/sites/default/files/Cancer-Screening-Client-Reminders-Archive-Colorectal-Other.pdf (accessed October 1, 2018).
6. The Guide to Community Preventive Services. Increasing Cancer Screening: Small Media Targeting Clients. US Department of Health and Human Services, CDC. (2005). Available online at: https://www.thecommunityguide.org/sites/default/files/assets/Cancer-Screening-Small-Media.pdf (accessed October 1, 2018).
7. The Guide to Community Preventive Services. Increasing Cancer Screening: Client Incentives. US Department of Health and Human Services, CDC. (2010). Available online at: https://www.thecommunityguide.org/sites/default/files/assets/Cancer-Screening-Client-Incentives.pdf (accessed October 1, 2018).
8. The Guide to Community Preventive Services. Increasing Cancer Screening: Reducing Client Out-of-Pocket Costs. US Department of Health and Human Services, CDC. (2009). Available online at: https://www.thecommunityguide.org/sites/default/files/assets/Cancer-Screening-Reducing-Out-of-Pocket-Costs.pdf (accessed October 1, 2018).
9. The Guide to Community Preventive Services. Increasing Cancer Screening: Group Education for Clients. US Department of Health and Human Services, CDC. (2009). Available online at: https://www.thecommunityguide.org/sites/default/files/assets/Cancer-Screening-Group-Education.pdf (accessed October 1, 2018).
10. The Guide to Community Preventive Services. Increasing Cancer Screening: Mass Media Targeting Clients. US Department of Health and Human Services, CDC. (2009). Available online at: https://www.thecommunityguide.org/sites/default/files/assets/Cancer-Screening-Mass-Media.pdf (accessed October 1, 2018).
11. Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg. (2011) 128:305–310. doi: 10.1097/PRS.0b013e318219c171
12. Hopewell S, Boutron I, Douglas A, Ravaud P. Deficiencies in the publication and reporting of the results of systematic reviews presented at scientific medical conferences. J Clin Epidemiol. (2015) 68:1488–1495. doi: 10.1016/j.jclinepi.2015.03.006
13. JPT Higgins and S Green editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. (2011). Available online at: http://handbook.cochrane.org/ (accessed October 1, 2018).
14. Thompson J, Quigley J, Halfpenny N, Scott D, Hawkins N. Importance and methods of searching for e-publications ahead of print in systematic reviews. Evid Based Med. (2016) 21:55–59. doi: 10.1136/ebmed-2015-110374
15. US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, Curry SJ, Davidson KW, Epling JW Jr, et al. Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA. (2016) 315:2564–2575. doi: 10.1001/jama.2016.5989
16. Huang X, Lin J, Demner-Fushman D. Evaluation of PICO as a knowledge representation for clinical questions. AMIA Annu Symp Proc. (2006) 2006:359–363.
17. Agoritsas T, Merglen A, Courvoisier D, Combescure C, Garin N, Perrier A, et al. Sensitivity and predictive value of 15 PubMed search strategies to answer clinical questions rated against full systematic reviews. J Med Internet Res. (2012) 14:e85. doi: 10.2196/jmir.2021
18. Ho GJ, Liew SM, Ng CJ, Hisham Shunmugam R, Glasziou P. Development of a search strategy for an evidence based retrieval service. PLoS ONE. (2016) 11:e0167170. doi: 10.1371/journal.pone.0167170
19. Sullivan GM, Feinn R. Using effect size – or why the p value is not enough. J Grad Med Educ. (2012) 4:279–282. doi: 10.4300/JGME-D-12-00156.1
20. Powe BD, Finnie R. Cancer fatalism: the state of the science. Cancer Nurs. (2003) 26:454–467. doi: 10.1097/00002820-200312000-00005
21. Sabatino S, Habarta N, Baron RC, Coates RJ, Rimer BK, Kerner J, et al. Intervention to increase recommendation and delivery of screening for breast, cervical, and colorectal cancers by healthcare providers: Systematic reviews of provider assessment and feedback and provider incentives. Am J Prev Med. (2008) 35:S67–74. doi: 10.1016/j.amepre.2008.04.008
22. Ward SH, Lin K, Meyer B, Bass SB, Parameswaran L, Gordon TF, et al. Increasing colorectal cancer screening among African Americans, linking risk perception to interventions targeting patients, communities and clinicians. J Natl Med Assoc. (2008) 100:748–758. doi: 10.1016/S0027-9684(15)31356-0
23. Baron RC, Melillo S, Rimer BK, Coates RJ, Kerner J, Habarta N, et al. Intervention to increase recommendation and delivery of screening for breast, cervical, and colorectal cancers by healthcare providers. Am J Prev Med. (2010) 38:110–117. doi: 10.1016/j.amepre.2009.09.031
24. Holden DJ, Jonas DE, Porterfield DS, Reuland D, Harris R. Systematic review: Enhancing the use and quality of colorectal cancer screening. Ann Intern Med. (2010) 152:668–676. doi: 10.7326/0003-4819-152-10-201005180-00239
25. Morrow JB, Dallo FJ, Julka M. Community-based colorectal cancer screening trials with multi-ethnic groups: a systematic review. J Community Health. (2010) 35:592–601. doi: 10.1007/s10900-010-9247-4
26. Powe BD, Faulkenberry R, Harmond L. A review of intervention studies that seek to increase colorectal cancer screening among African-Americans. Am J Health Promot. (2010) 25:92–99. doi: 10.4278/ajhp.080826-LIT-162
27. Brouwers MC, De Vito C, Bahirathan L, Carol A, Carroll JC, Cotterchio M, et al. What implementation interventions increase cancer screening rates? A systematic review. Implement Sci. (2011) 6:1–17. doi: 10.1186/1748-5908-6-111
28. Ferroni E, Camilloni L, Jimenez B, Furnari G, Borgia P, Guasticchi G, et al. How to increase uptake in onocologic screening: a systematic review of studies comparing population-based screening programs and spontaneous access. Prev Med. (2012) 55:587–596. doi: 10.1016/j.ypmed.2012.10.007
29. Gonzalez SA, Ziebarth TH, Wang J, Noor AB, Springer DL. Interventions promoting colorectal cancer screening in the Hispanic population: a review of the literature. J Nurs Scholarsh. (2012) 44:332–340. doi: 10.1111/j.1547-5069.2012.01474.x
30. Rawl SM, Menon U, Burness A, Breslau ES. Interventions to promote colorectal cancer screening: an integrative review. Nurs Outlook. (2012) 60:172–181. doi: 10.1016/j.outlook.2011.11.003
31. Sabatino SA, Lawrence B, Elder R, Mercer SL, Wilson KM, DeVinney B, et al. Effectiveness of interventions to increase screening for breast, cervical, and colorectal cancers: nine updated systematic reviews for the guide to community preventive services. Am J Prev Med. (2012) 43:97–118. doi: 10.1016/j.amepre.2012.04.009
32. Oh KM, Jacobsen KH. Colorectal cancer screening among Korean Americans: a systematic review. J Community Health. (2014) 39:193–200. doi: 10.1007/s10900-013-9758-x
33. Muliira JK, D'souza MS. Effectiveness of patient navigator interventions on uptake of colorectal cancer screening in primary care settings. Jpn J Nurs Sci. (2015) 13:205–219. doi: 10.1111/jjns.12102
34. Baron RC, Rimer BK, Coates RJ, Kerner J, Kalra GP, Melillo S, et al. Client-directed interventions to increase community access to breast, cervical, and colorectal cancer screening: a systematic review. Am J Prev Med. (2008) 35:S56–66. doi: 10.1016/j.amepre.2008.04.001
35. Baron RC, Rimer BK, Breslow RA, Coates RJ, Kerner J, Melillo S, et al. Client-directed interventions to increase community demand for breast, cervical, and colorectal cancer screening: a systematic review. Am J Prev Med. (2008) 35:S34–55. doi: 10.1016/j.amepre.2008.04.002
36. McPhee S, Bird J, Jenkins C, Fordham D. Promoting cancer screening: a randomized, controlled trial of three interventions. Arch Intern Med. (1989) 149:1866–72. doi: 10.1001/archinte.149.8.1866
Keywords: colorectal cancer screening (CRCS), evidence-based intervention (EBI), systematic review, effect size, research translation, evidence-based practice
Citation: Young B-R, Gwede CK, Thomas B, Vázquez-Otero C, Ewing A, Best AL, Aguado Loi CX, Martinez-Tyson D, Schneider T, Meade CD, Baldwin JA and Bryant C (2019) A Systematic Review of U.S.-Based Colorectal Cancer Screening Uptake Intervention Systematic Reviews: Available Evidence and Lessons Learned for Research and Practice. Front. Public Health 7:145. doi: 10.3389/fpubh.2019.00145
Received: 15 October 2018; Accepted: 21 May 2019;
Published: 11 June 2019.
Edited by:
Michal Grivna, United Arab Emirates University, United Arab EmiratesReviewed by:
Sankalp Das, Baptist Health South Florida, United StatesBojana Matejic, University of Belgrade, Serbia
Copyright © 2019 Young, Gwede, Thomas, Vázquez-Otero, Ewing, Best, Aguado Loi, Martinez-Tyson, Schneider, Meade, Baldwin and Bryant. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Belinda-Rose Young, YnJ5b3VuZzJAbGl2ZS51bmMuZWR1