 Eva Guérin1
Eva Guérin1 Hamdi Jaafar
Hamdi Jaafar Denis Prud'homme
Denis Prud'homme Céline Aguer
Céline Aguer- 1Institut du Savoir Montfort-Recherche, Ottawa, ON, Canada
- 2Department of Biochemistry, Microbiology, and Immunology, Faculty of Medicine, University of Ottawa, Ottawa, ON, Canada
- 3Faculty of Health Sciences, School of Human Kinetics, University of Ottawa, Ottawa, ON, Canada
Background: Type 2 diabetes (T2D)-related depression has a significant impact on quality of life and leads to greater morbidity and mortality. Current educational and treatment programs for T2D rarely include a specific depression-prevention component, focusing largely on remediating depressive symptoms that have reached clinical levels.
Objective: Given the vast field of research on the association between T2D and depression, and the unknown status of prevention efforts for the latter, the goal of this scoping review was to conduct a synopsis of intervention strategies specifically targeting the prevention of depression among adults with T2D.
Eligibility Criteria: (1) participants aged 18 and over with T2D; (2) experimental and quasi-experimental designs (3) intervention strategies seeking to prevent the onset or worsening of (non-clinical) depressive symptoms; (4) a valid measure of depressive symptoms; (5) full-text articles available in English or French.
Sources of Evidence: Databases including Medline, PubMed, and SCOPUS were searched between 2000 and 2018 resulting in 4,219 potential articles.
Charting Methods: This review was conducted in-line with the current methodological framework for scoping reviews. Titles, abstract and full text articles were screened independently and in duplicate. A narrative analysis was conducted to synthesize study characteristics and the nature of intervention strategies and components.
Results: Twelve studies were identified with the primary aim of preventing the incidence of depressive symptoms or improving non-clinical depression levels. Individual and group-based approaches included educational interventions incorporating diabetes self-management, problem-solving, and resilience-focused approaches, emotion-targeted techniques as well as alternative interventions. Self-monitoring, home practices, and motivational interviewing were common elements.
Conclusions: This review lays the groundwork for future studies seeking to develop, validate, and improve prevention strategies targeting the diabetes-depression comorbidity. More studies over longer periods and with larger samples are needed to capture the effects of prevention efforts.
Introduction
Diabetes mellitus, the seventh leading causes of death worldwide (1), is a metabolic disorder characterized by dysfunction in the production, secretion, or action of insulin, which results in a state of hyperglycaemia. Type 2 diabetes (T2D) represents 90% of the different forms of diabetes (2).
The societal and economic burden of diabetes is significant (3). In fact, the impact of T2D on quality of life, life expectancy, and premature morbidity and mortality is devastating (4). Premature deaths among patients with T2D are primarily attributable to complications of this disease, including heart disease, stroke, and peripheral neuropathy (5). Living with T2D and its corollaries can also have important mental health consequences that can affect the disease's course and treatment (6). Specifically, it is known that depression is a major comorbid disorder in individuals with T2D (7).
Studies have shown that the incidence of depression is up to three times greater among individuals with T2D than the general population (8), and one in four people with T2D develops clinically significant depression (9). Whereas, the term diabetes distress is used to define emotional distress stemming from the burden of living with a chronic disease (10), major depression is a clinical mood disorder characterized by persistent and severe feelings of sadness and/or disinterest (11). Other presenting symptoms include lack of sleep, loss or gain of appetite, lack of concentration, agitation, etc. as defined by the Diagnostic and Statistical Manual of Mental Disorders-V (DSM-V) criteria. Validated clinical tools are used to identify symptoms and establish a diagnosis of depression (12).
Diabetes-related depression has a significant impact on quality of life and significantly increases rates of morbidity and mortality (13, 14). In particular, depression influences health care behaviors among individuals with T2D, impacting their nutrition, treatment adherence, glycemic control, motivation, and productivity (15, 16). Likewise, several studies have shown that depression worsens T2D-related complications, primarily stemming from poorer glycemic control and an impaired ability to manage diabetes-related comorbidities (e.g., hypertension) in general (17). Moreover, there is evidence of an interactive effect of the two disorders, such that decrements in health go beyond their additive harm (18). Therefore, it is not surprising that healthcare expenses are significantly higher among individuals with T2D and depression (13). Therefore, it is critical to identify strategies that will prevent the development and progression of depression among people with T2D.
For individuals with T2D, available treatment plans usually target cardiometabolic factors (e.g., glycaemia, blood pressure, and lipids) and diabetes management. There is an abundance of clinical programs aimed at glycemic control as well as exercise and nutritional programs targeting weight loss and improved insulin action (19). Such interventions primarily focus on underlying biological factors of T2D rather than psychological factors and depression specifically. Nonetheless, greater knowledge of the incidence and severity of depression in individual with T2D has propelled research on depression management and treatment options, though results have been mixed (9). Among the most commonly cited interventions are those combining psychotherapy with pharmacotherapy in addition to standard T2D management guidelines (20, 21). Conventional intervention elements include education about both illnesses, healthy lifestyle behaviors, and the acquisition of problem solving skills, and their effectiveness is more pronounced for T2D individuals with mild or moderate depressive symptoms (22, 23).
However, the volume, availability, and content of educational interventions delivered to individuals with T2D that include a specific depression-prevention component is unknown. To our knowledge, interventions to date have focused primarily on remediating individuals with T2D once depressive symptoms have reached clinical levels (24, 25). Given the aforementioned costs and burden of this comorbidity and considering high rates of non-adherence and failure of T2D treatments among major depression suffers (13–17), it seems paramount to properly target risk factors for depression in individuals with T2D in order to aid in its prevention. It is therefore critical to understand the current state of knowledge and identify fruitful avenues for future prevention studies.
The objective of this study was to identify available intervention strategies to prevent the onset or the worsening of depressive symptoms among individuals with T2D. Given the vast field of work on T2D and its associated mental health complications, and the unknown status of research on preventing depression, we carried out a scoping review with the goal of gathering and mapping scientific information. We conducted a narrative synopsis of existing intervention strategies that can be used to target the prevention of depression among individuals with T2D. In this reviewer, we refer to depressive symptoms as the different signs and manifestations that characterize depression rather than a clinical (DSM-V) diagnosis of major depressive disorder (i.e., five or more symptoms, >2 weeks, causing significant impairment).
Methods
Study Design and Protocol
The goal of a scoping review is to explore a complex and broad theme of research and to provide a global synthesis of content and/or results on a particular topic. A scoping review is preferred when there may be deficiencies or uncertainties in the volume of literature on a topic or heterogeneity in regards to various facets of the research, including population, measurement instruments, and interventions (26). Scoping reviews identify and describe existing studies on a particular subject by considering a variety of designs and without systematically extracting and appraising results in relation to methodological quality. In scoping reviews, researchers are not expected to conduct a meta-analysis of the available data. For this review, a protocol was prepared (available on request) in accordance with guidelines put forward by the Joanna Briggs Institute (27, 28). The conduct of this scoping review was consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) extension for Scoping Reviews (PRISMA-ScR) which have since been recently released (29).
Eligibility Criteria
The inclusion criteria were follows: (1) participants aged 18 and over with diagnosed (or otherwise confirmed or established) T2D; (2) experimental design such as randomized controlled trials as well as quasi-experimental designs (including pre-post schemes), cohort studies, case control studies, and mixed-method studies; (3) any form of prevention approach or intervention strategy including educational programs or other seeking to prevent the onset of depression or prevent the worsening of (non-clinical) depressive symptoms; (4) a valid measure of depressive symptoms, for example, the Beck Depression Inventory (BDI) (30), and the Center for Epidemiological Studies Depression Scale (CES-D) (31); (5) full-text articles available in English or French.
Exclusion criteria included: (1) participants <18 years old and other diabetes types (e.g., type, gestational); (2) presence of clinical complications of diabetes (including, but not limited to heart disease, nephropathy, retinopathy, stroke), (3) diagnosis of major depressive disorder or other clinical mood disorder; (4) interventions to treat depression (e.g., pharmacological, psychological, behavioral, etc.) where the primary objective was remediating an existing (i.e., clinical/diagnosed or otherwise elevated) depressive state rather than preventing onset or worsening of depressive symptoms; (5) interventions that target multiple chronic diseases (e.g., T2D and heart disease); (6) correlational and observational studies focused on prevalence of depression and or T2D or on predictive factors; (7) systematic reviews, meta-analyses, dissertations, or conference presentation abstracts1; (8) sole focus on screening or diagnosis of depression (including instrument validation studies).
Information Sources and Search Strategy
Pertinent articles were identified by searching several databases, including Medline, Embase, Cochrane Database of Systematic Reviews, PsycINFO, PubMed, and Scopus. A search strategy was developed and tested using a combination of terms (Supplemental File 1). A preliminary exploration of the keywords “type 2 diabetes,” “depression,” and “prevention” in PubMed resulted in only 6 manuscripts published between 1986 and 1999. The number of publications increased significantly after 2000, reflecting a growing interest in this area post-2000. The search was thus limited to publication dates between January 2000 and May 2018. Articles reporting secondary analyses of data were included. The final search strategy was deemed satisfactory following independent screening by two evaluators (EG, LA) of the first 100 excluded articles to confirm warranted removal.
Source Selection (Screening)
Results of the database search were uploaded to Distiller Systematic Review (DSR) software to facilitate the process of article screening and selection as well as data extraction between the three reviewers (EG, LA, HJ). Screening forms were developed in DSR for each level of screening. These were pilot tested and refined accordingly by the evaluators.
Independently and in duplicate, the three evaluators screened titles for relevance. Titles deemed relevant by one or both evaluators were retained for abstract screening. Similarly, the evaluators subsequently examined the list of abstracts to identify those deemed worthy of full article screening. In the case of disagreement during abstract screening, discrepancies were discussed until agreement was reached regarding inclusion. Lastly, the full-texts of the remaining articles were surveyed for final inclusion. As required, an impartial third evaluator (CA) provided their advice regarding the article's selection.
Data Items and Charting Process
For all studies included in the final review, data were extracted conforming to the PICO framework with the following variables:
Population
Sample size, location of study, sex or gender, ethnicity, age, and if available HbA1c levels, body mass index (BMI), and duration of T2D (months or years).
Intervention
Intervention target, intervention type and modality (e.g., mindfulness) and/or intervention approach (e.g., cognitive behavioral therapy), delivery (i.e., group vs. individual), context (e.g., community, hospital, home, etc.), dose (when applicable, i.e., length of sessions in minutes), frequency (i.e., number of sessions per week), duration (i.e., weeks or months).
Comparator
(if applicable) number of comparators and type(s) of comparator(s) (e.g., control group, active control, distinct treatment, etc.).
Outcome
Primary depression measure (instrument), list of all outcomes evaluated in the study (i.e., primary and secondary outcomes reported in published article); time-points of assessment. In regards to depression, as the goal of this study was not to systematically evaluate intervention effects quantitatively, a general synopsis of impact was extracted. Specifically, the following information was pulled for each intervention study as available: (a) statistical change in depression over time from baseline (i.e., in terms of symptom severity or level of depression) and/or (b) statistical change in the prevalence of depression among participants over time.
As the goal of this scoping review was to identify and examine studies in which the main aim was preventing the onset or worsening of depressive symptoms, included studies were divided as follows: (1) depressive symptoms or levels as the primary or sole outcome; (2) depressive symptoms or levels as a secondary or unspecified intervention measure or outcome.
Synthesis of Results
The reviewed studies were first described according to study and intervention characteristics (Table 1), participant characteristics (Table 2), and intervention effects on depression (Table 3). We conducted a narrative, descriptive synthesis of contextual delivery factors and active intervention ingredients. In a scoping review, experts recommend a qualitative content analysis be conducted in light of the emerging body of evidence on the topic as well as variability in study designs and participant samples. In our study, we consider the similarities, differences, and implications of the included intervention strategies, including their design and implementation.
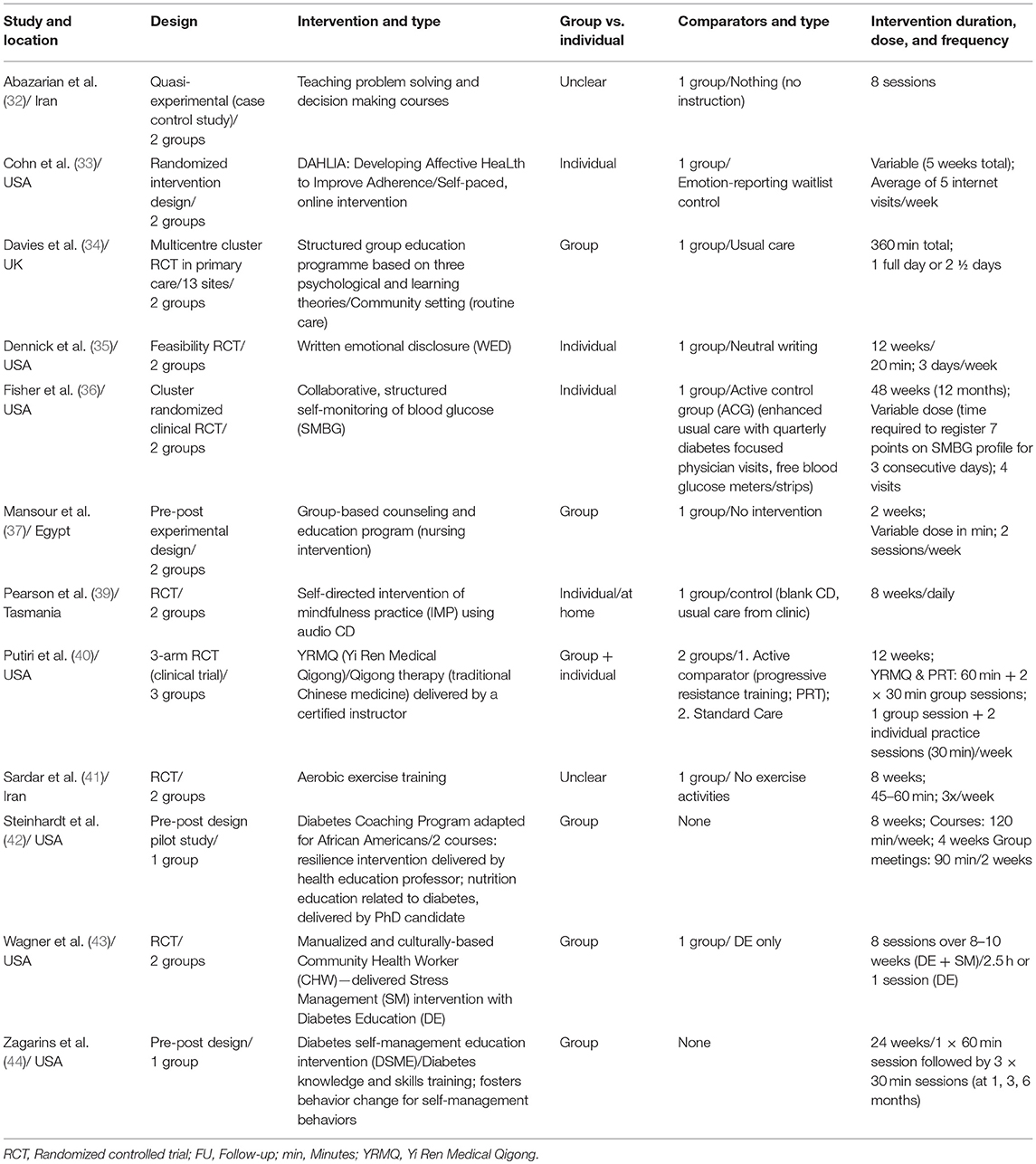
Table 1. Study and intervention characteristics for 12 included studies.
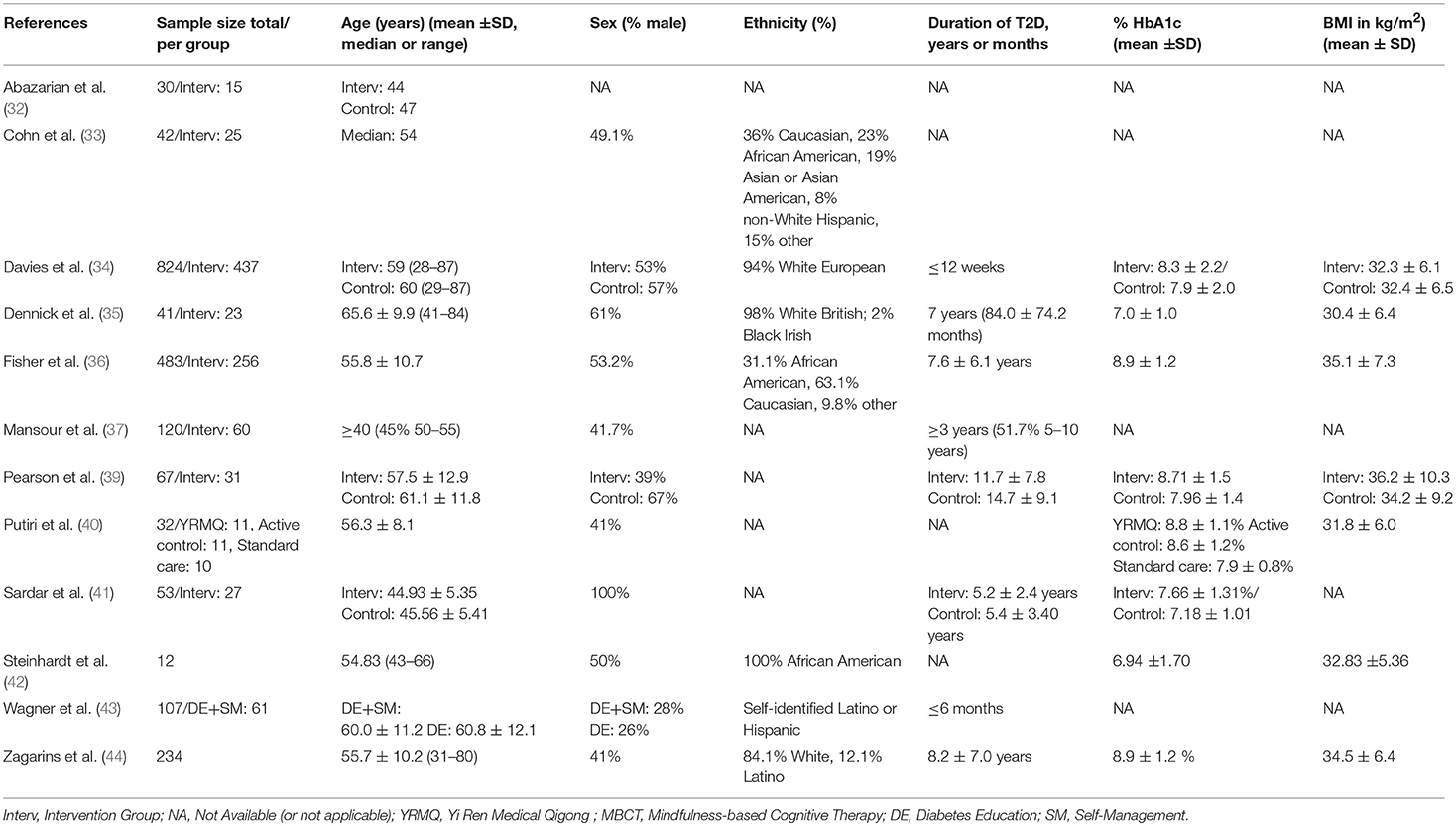
Table 2. Participant characteristics for 12 included studies (results provided for the full sample unless otherwise specified).
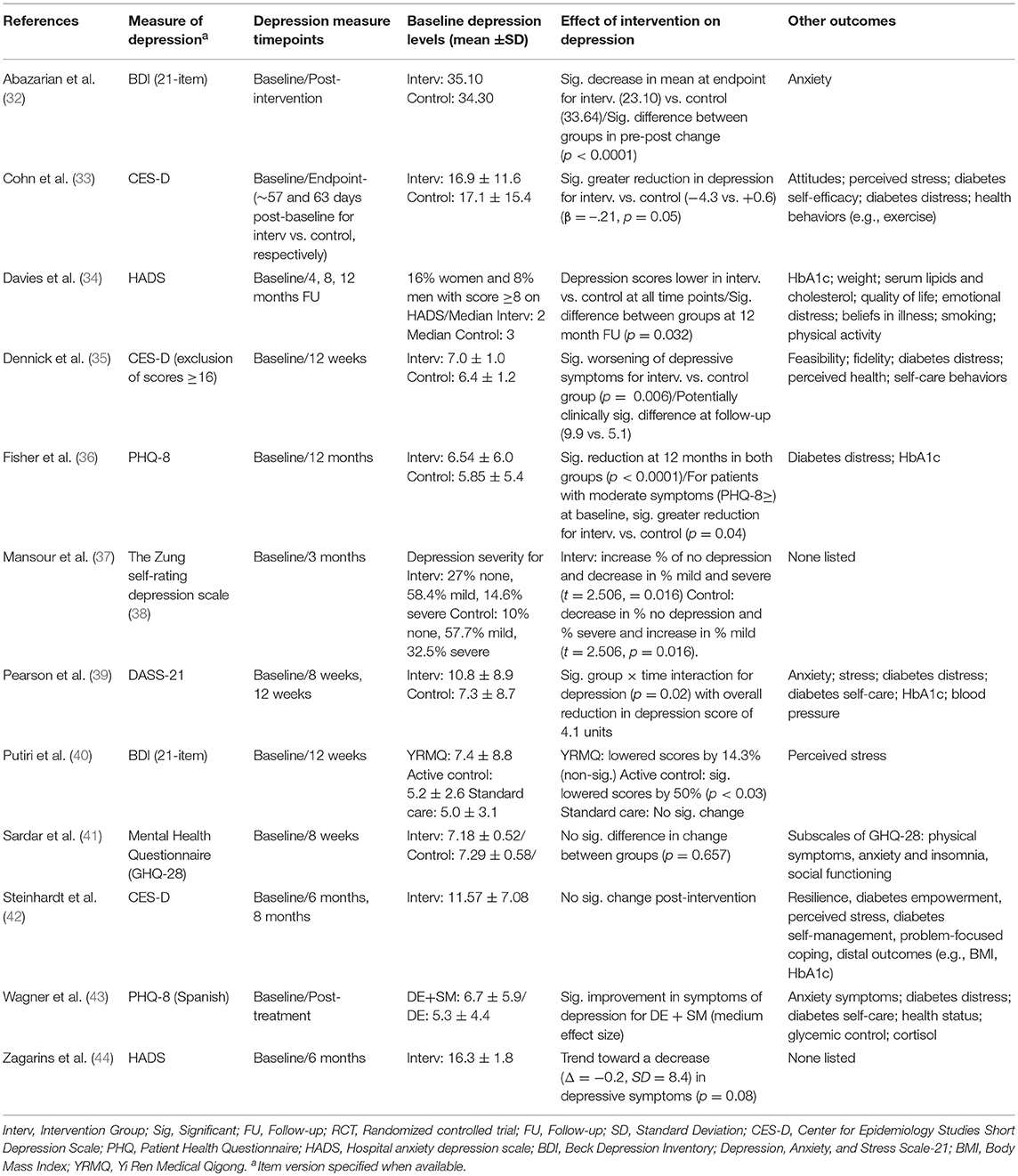
Table 3. Depression measurement, outcomes and results for 12 included studies.
Risk of Bias
Consistent with scoping review recommendations and the Joanna Briggs Institute manual (28, 29), an appraisal of the quality of included sources and an assessment of risk of bias were not conducted (27).
Results
Selection of Sources and Characteristics
The initial search identified 4,219 studies for triage after duplicate removal (Figure 1). After inspection of the titles, the reduced list consisted of 2013 entries for abstract screening. Filtering of the abstracts resulted in 158 articles deemed relevant for full-text screening. The product of the full-text examination consisted in 12 eligible articles that focused specifically on preventing depression or improving (non-clinical) depressive symptoms as a primary objective, and 56 studies in which depression was considered a secondary aim (i.e., a non-priority outcome or not explicitly defined). For the purposes of this study, we present a detailed synopsis of the 12 intervention studies that focused on preventing depression (Tables 1–3). A tabular overview of the secondary studies is available as a Supplementary Table S1.
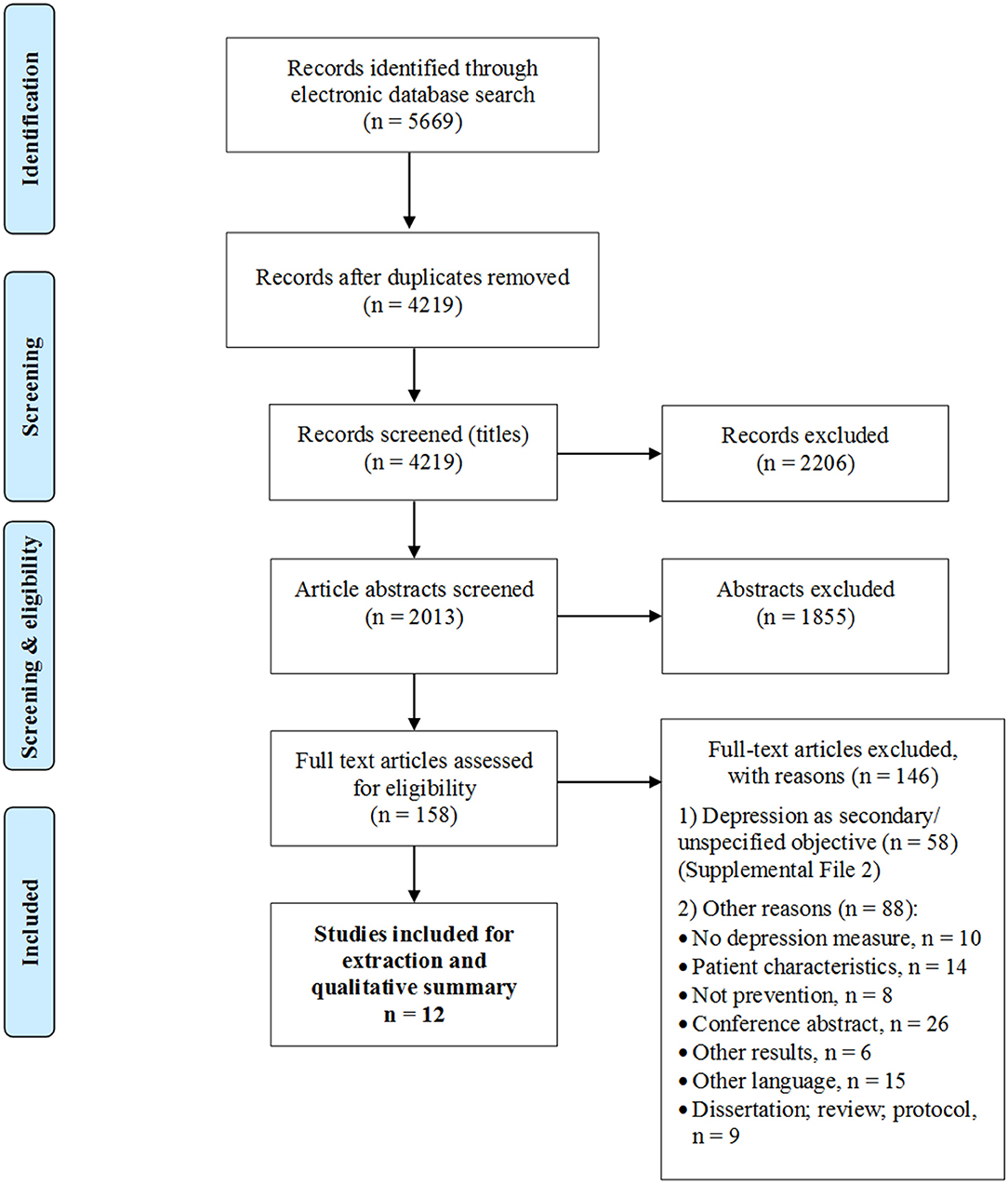
Figure 1. PRISMA flow diagram of included studies.
As shown in Table 3, the most common measure of depression was the CES-D (31). Four studies (33, 35, 36, 39) were individual-based while five (34, 37, 42–44) used group formats and one study (40) reported a combination of individual and group approaches. Two studies (32, 41) did not specify the delivery format and at least one study (33) exploited an online delivery. Eight of the 12 studies (33–36, 39–41, 43) used a variant of a randomized design while three studies (37, 42, 44) followed a pre-post scheme and one (32) used a quasi-experimental design. The duration of each intervention was variable, ranging from a few hours [e.g., 360 min over 2 days (34)] to multiple practice sessions (individual, group) several times per week for 12 weeks [e.g., Putiri et al. (40)].
Based on the findings presented in Table 3, a significant positive effect on levels of depression was reported in six of the 12 studies (32–34, 36, 39, 43).
In the sections that follow, key intervention components and delivery strategies are described for the 12 included studies. We grouped the interventions on a spectrum from structured programs (i.e., focus on T2D management and education), to problem-solving and emotion-based approaches to alternative and exercise-based intervention strategies.
Synthesis of Results
Structured Programs: T2D Management and Education
Fisher et al. (36) tested a collaborative, structured self-monitoring of blood glucose (SMBG) intervention wherein participants also recorded meal sizes and calorie composition. Participants received instructions about how to identify problematic glycemic patterns. They recorded their SMBG profile during three consecutive days prior to scheduled study visits. During visits, forms were reviewed with a physician and suggestions for changes to exercise, nutrition, and medication were made. Given positive results of the intervention on depressive symptoms, particularly among participants with more elevated depression scores, the authors concluded that this type of collaborative approach between patient and physician could help patients deal with the emotional strain of managing their T2D. In itself, self-monitoring of glucose is a strongly advocated strategy among health professionals for facilitating treatment adherence (45). The observational element is also thought to improve patient experiences and encourage more positive attitudes toward T2D, thereby increasing disease and treatment satisfaction (46). This may in turn prevent the development of negative mood patterns in individuals with T2D.
Focused educational programs may be used in conjunction with specific diabetes management. In a cluster randomized RCT, Davies et al. (34) tested the Diabetes Motivation Strengthening (DESMOND) intervention for ongoing and newly diagnosed individuals with T2D. The program was grounded in a philosophy of patient empowerment and based on several learning theories (47). The design of the program was particularly suitable for preventing depression given its implementation within 12 weeks of T2D novo diagnosis. Key process elements included its delivery in the community by registered health professionals and its integration into routine care. A non-didactic approach was favored to elicit learning with an emphasis on activating participants to move toward specific, achievable goals in self-management (34). The content of the learning curriculum was broad, with a focus on risk and lifestyle factors. Overall, participants who received the intervention experienced less depression at 12 months than those in the standard education control condition.
Zagarins et al. (44) also examined a multifaceted Diabetes Self-Management Education (DSME) intervention. Participants received four sessions over a 6-month period by trained instructors, two of whom also incorporated motivational interviewing, thus strengthening the patient-clinician relationship and empowering patients to improve their health. This collaborative element is similar to the approach used by Fisher et al. (36). Although levels of depression did not diminish significantly from baseline, Zagarins et al. (44) suggested that this type of intervention could be more effective for preventing depression if implemented over a longer term. Depressive symptoms were not specifically addressed in the DSME-based intervention despite their importance as an outcome of the study, therefore an intensified focus on depression may be required.
Problem Solving and Resilience Building Approaches
Developing skills to help individuals manage their T2D is a common goal among educational programs in diabetes care and this often includes problem-solving. Researchers in Iran (32) tested an intervention that was based on a model stipulating that solving psychosocial problems can mediate the impact of stressful events on well-being (48). While intervention strategies by Davies et al. (34) and Fisher et al. (36) employed more standard approaches that help individuals manage their T2D by focusing on the disease itself, the approach from Abazarian et al. (32) had a distinct emphasis on wellness. In particular, an instruction-based intervention was delivered via eight sessions focused on recognizing problems, on key aspects of decision-making such as values and feelings, and on problem solving skills such as evaluating resources. The positive influence of the intervention on depression levels of participants at endpoint provided evidence that improving daily decision-making can help participants improve their well-being in the face of problems related to managing T2D.
Effective problem solving can also help individuals with T2D build resilience. Steinhardt et al. (42) pilot tested a 4-week Diabetes Coaching Program (DCP), adapted for African Americans, which combined a resilience intervention with nutrition education. The content of Transforming Lives Through Resilience Education was consistent with a resilience model based on previous work on the topic [e.g., Carver (49)]. Examples of curriculum components in weeks 1 and 3 were problem- and emotion-focused coping strategies and an empowering interpretation model. With nutrition education, the goal was to provide realistic, practical suggestions for improving diabetes care (e.g., reading food labels). Bi-weekly support-group follow-up meetings were devoted to problem solving, reviewing course content, and providing social support. Noted benefits in distal outcomes like HbA1c levels were not, however accompanied by decreases in depressive symptoms post-intervention. Akin to Zagarins et al. (44), it was suggested that a longer duration might be required to influence key psychological processes.
Another culturally sensitive intervention was delivered by Wagner et al. (43) over a period of 8–10 weeks, and with favorable results. In the Community Health Workers Assisting Latinos Manage Stress and Diabetes (CALMS-D) trial, diabetes education was paired with stress management training. The educational piece covered basic information about managing diabetes (e.g., nutrition, medication, glucose monitoring). Most notably, the core components of the manualized intervention were group psychoeducational skills training and physiological relaxation skills training. At each session, learning objectives were framed around a culturally relevant analogy or story. In session and at-home relaxation activities (e.g., via CD) were used in combination. Improvements in symptoms of depression with the intervention were significant, suggesting that interventions focused explicitly on managing stress and the psychological symptoms of diabetes are justified.
Emotion-Based Approaches and Positive Psychology
A subset of interventions focused on individuals' emotional health in lieu of diabetes-specific content. Mansour et al. (37) showed equivocal support for a counseling intervention focused directly on preventing clinical depression, though they offered very little description of the nature of the counseling method itself. The researchers were attentive to creating an optimal environment in which to develop of an effective therapeutic relationship. Specifically, their intervention rested on principles of trust and attentive listening and on therapist qualities such as demonstrating interest, concern, and friendliness, which naturally require a higher level of training and competencies from counselors and resources (time).
Intensive counseling interventions stand in stark contrast with the approach taken by Dennick et al. (35). The team implemented Written Emotional Disclosure (WED), a theoretically grounded, self-administered low-intensity technique that has the potential to respond to low-level psychological needs. Backed by the premise that WED is comparatively inexpensive and more widely available for widespread dissemination, participants were instructed to engage in 20 min writing sessions at home in private on 3 days over 1 week. Participants were incited to write their thoughts and feelings regarding any stressful experience over the last month or a current, non-diabetes concern. Results showed a worsening effect for the WED group, notably depressive symptoms were significantly more severe at 3-month follow-up. Coupled with feasibility issues, there were important limitations in the potential effectiveness of the WED intervention for use in primary care in its current form. The authors proposed a better evaluation of the appropriateness of WED based on individual characteristics and readiness, to which can be added the need for more proactive psychological skills training.
In this regard, Developing Affective HeaLth to Improve Adherence (DAHLIA) was an online, self-paced intervention that taught positive affect skills in order to improve daily positive emotions and adaptation as well as general coping abilities and well-being (33). Grounded in the Stress and Coping Theory (50, 51) and the Broaden-and-Build theory of positive emotion (52), targeted skills included positive reappraisal, setting attainable goals, performing acts of kindness, and mindfulness. Participants learned to practice one or more of these skills every day via weekly lessons and home assignments. Participants were encouraged to keep a learning journal and to apply acquired skills to manage their T2D and in other life domains. A mindfulness practice (i.e., 10 min reflection and mindful breathing) was promoted to harness an awareness of positive events. Results showed a significant reduction in symptoms of depression with the intervention, regardless of baseline levels (33). The authors reported good adherence and argued that an online format offers a low-cost alternative intervention to prevent depression among individuals with T2D who have more limited options for face-to-face care.
Alternative Approaches and Exercise
Mindfulness can be used as an adjunct strategy in multicomponent interventions like DAHLIA or it may be a worthy approach in and of itself. As demonstrated by Cohn et al. (33), an advantage of mindfulness is its potential to be self-directed. In an effectiveness study among individuals with T2D who demonstrated a need for psychological support, Pearson and colleagues (39) examined a novel delivery approach for mindfulness practice. Over an 8 week period, patients used an audio compact disc (CD) to engage in a daily 30 min mindfulness intervention. The CD was developed by a trainer with over 25 years of mindfulness practice. Participants in the intervention group showed an overall reduction in depression scores at 12 weeks.
Mindfulness is one of several alternative practices that teach awareness regarding the interplay between movement, breath and thoughts. Putiri et al. (40) compared Yi Ren Medical Qigong (YRMQ) to progressive resistance training and standard care in adults with T2D. Qigong is a traditional Chinese practice designed to maintain health and cultivate spiritual well-being. Exercises are performed with a heighted sense of feeling and focus which cultivates self-awareness of internal energy conditions. Although weekly YRMQ delivered by a certified instructor lowered participants' BDI scores by 14.3%, the effect was not significant. Since developing a regular Qigong practice may take time, an intervention period longer than 12 weeks may be necessary to achieve success. Interestingly, participants in the progressive resistance-training physical activity (PA) group showed significant reductions in depression.
Conversely, the results of another study that targeted aerobic PA behavior specifically were not consistent in regards to depression. In Sardar et al. (41), participants engaged in an aerobic exercise-training program (45–60 min on an ergocycle at 60–70% of maximum heart rate, three times per week for 8 weeks). Unfortunately, a detailed description of the context in which the exercise training was delivered and what strategies were used to ensure adherence throughout were lacking. Although the intervention was consistent with recommendations for aerobic training in diabetes, it did not result in significant changes in depression in this all-male sample. It is likely that the duration, intensity, and type of exercise training may need to be considered, particularly given that enjoyment of the activity may have particular relevance in regards to depression.
Nonetheless, various forms of PA and lifestyle change have been the focus of many intervention studies to date, including those considered in the current review in which depression was presented as a secondary or auxiliary outcome (53–59). Descriptive information and main findings of these studies are available as a Supplementary Table S1. These tables can be consulted to extract learning points and relevant strategies for developing future intervention studies.
Discussion
Summary of Evidence
Over four thousand titles met our initial search strategy but only 12 studies satisfied our inclusion criteria. We determined that the volume of research studies that have developed and tested intervention strategies focusing specifically on preventing depression in individuals with T2D is limited. Interestingly, in the initial exclusion stages of our review we identified several studies relating to the treatment of depression. Specifically, over 10% of the consulted abstracts and over a dozen full-texts were excluded based on a treatment approach for diagnosed or confirmed clinical depression. This suggests that research to date has overwhelmingly emphasized alleviating depressive symptoms once they develop rather than preventing the development or progression of depressive symptoms.
Still, our narrative review allowed us to hone in on the general success, limitations, and key elements of preventative approaches that have been tested, namely educational interventions incorporating diabetes self-management, problem-solving and resilience-focused approaches, emotion-targeted techniques as well as alternative interventions.
Overall, six studies with a primary focus on depression showed a significant positive effect while six studies showed inconsistent or non-significant findings. However, given that study quality was not assessed (e.g., using GRADE or a similar tool) and that we acknowledge variations in study design and reporting of results, the effectiveness of the interventions should be interpreted with caution. Nonetheless, we were able to extract specific components that can be integrated in revised interventions and tested over longer periods, in larger samples and including both sex.
Key Intervention Components and Future Studies
Self-management education and support (SMES) has a long history in diabetes care. Consistent with National Standards for SMES (60) and studies we presented, interventions can take on many forms and include components of nutritional and lifestyle counseling, safe medication practices, monitoring of glucose and other parameters, and the development of personal strategies to deal with psychosocial problems. In the larger context of chronic disease, programs that include a psychotherapeutic component (behavioral or psychosocial) tend to demonstrate better results as they allow patients to modify negative perspectives about their illness, which can be a principal factor in developing comorbid mental disorders such as depression (61, 62). One review showed a large combined effect of psychotherapy and self-management education in treating depression among individuals with T2D (21). In the CALMS-D trial (43), a specific focus on stress management in facing diabetes and on building psychoeducational skills yielded superior improvements compared to education only. Thus, even if levels of personal responsibility for T2D increase with an intervention, participants may feel better equipped to manage it (34). Therefore, we suggest that incorporating a defined psychological element to patient education might be valuable for preventing the development or the exacerbation of depressive symptoms.
Moreover, studies have shown that T2D self-management programs that are adapted to the age, language, and culture of individuals are more effective compared to generic programs (63–65). This may be particularly true in the context of addressing depression given different risk factors between racial and ethnic groups as well as cultural values and expectations about mental disorders (66). Cultural adaptation can take many forms that extent beyond translation, including the integration of culturally salient values and an understanding of stigma related to living with depression. Apart from Steinhardt et al. (42), Wagner et al. (43), and a few secondary studies targeting Latinos specifically [e.g., Castillo et al. (67), Wang et al. (68)], few studies seemed to explicitly integrate or describe cultural adaptations. A unique characteristic of T2D management interventions is that they are typically patient-centered and adapted to patient needs, which should include evaluating multiple parameters such as beliefs and attitudes (60). Therefore, future studies could strive to consider the ethno-linguistic background and diversity of targeted participants and the appropriateness of activities and messages.
The capacity to adapt or individualize an intervention may vary as a function of delivery. Online interventions can offer flexible options that address individual preferences and needs (33, 69). In addition, online interventions can be delivered anonymously, at lower cost, and at convenient locations and times, which may increase efficacy (33, 70). While at least six secondary studies used a computer-based or online delivery (57, 70–73) and another four tested mobile phone applications (74–77), only one of the primary studies reported using a web-based format (33). Specifically, the DAHLIA positive affect intervention lead to lower levels of depression compared to an emotion-reporting waitlist control condition (33). Other mediums for self-directed or home-based interventions such as the audio for a mindfulness practice (39) have also shown promise, although issues regarding how to measure and address compliance and adherence may compromise their potential (70).
In addition, since elements of interaction, interpersonal dynamics, and peer learning are lacking from screen/web based approaches, commitment to the intervention and thus effectiveness may wane over time. In the context of depression, a meta-analysis demonstrated the potential for web-based interventions to significantly improve well-being outcomes in individuals with T2D, but not depression specifically (69). Yet, given RCT evidence that web-based self-help intervention can reduce the incidence of major depressive disorder over 12 months in participants not affected by T2D (78), further testing is warranted.
On the other hand, research has shown that group-based (in-person) diabetes education programs are particularly effective for improving clinical, lifestyle, and psychosocial outcomes in individuals with T2D (79–81). Our findings in the context of reducing depressive symptoms strengthen the efficacy of group approaches. Allowing participants to share their thoughts and insights may be particularly pertinent to problem-solving interventions, where skills, advice and strategies can be learned and integrated among group participants with similar experiences (32, 42, 43). It is noteworthy that some interventions herein emphasized not only problem solving and coping skills in relation to diabetes, but also general psychosocial preparedness, competencies, and resilience. Thus, when considering the mental health risks that accompany the demands of a disease like T2D, it may be beneficial to integrate an awareness of an individual's life and emotional experiences beyond the disease itself (32).
In particular, we saw the emergence of interventions that were more holistic in nature. Two studies (33, 39) suggested a distinct mindfulness component to complement their programs, with the DAHLIA intervention (33) also targeting patients' general cognitions and emotions. The practice of mindfulness helps people take a nonjudgmental and observing stance on their thoughts, leading to less worry and rumination, which are important correlates of depression (82). Regarding implementation, mindfulness is a unique approach in that unlike mainstream or other diabetes-orientated interventions, it can be delivered as an adjunct therapy by non-specialists and can be a cheaper and more accessible long-term alternative (83). It has shown promise for preventing symptoms of depression in patients with type 1 and 2 diabetes (84). Given that the incidence of T2D and depression are increasing at alarming rates, further research is needed to develop low-cost approaches and alternative means of delivery that will be available to a more diverse population of individuals with T2D.
Limitations
While the strengths of this review include a comprehensive search of multiple databases, a rigorous screening process for inclusion, and an explicit focus on prevention, the findings should be interpreted within the scope of a few limitations. Firstly, this review does not provide a quantitative summary of effect size. Thus, we cannot objectively discuss efficacy or compare efficacy across the different intervention delivery formats. Likewise, we did not assess moderators of intervention effects, thus we cannot conclude for whom (e.g., age group) and under what conditions (i.e., latency of T2D diagnosis) preventive programs are most effective. Similarly, common mechanisms linking diminished depressive symptoms to improvements in glycemic control with treatment (or other disease indicators) were not examined and could be explored in future studies. Secondly, although we excluded studies that did not utilize a valid measure of depressive symptoms, there was variability in the choice of instruments across studies, which could have led to differences in terms of effects and participant selection (i.e., symptom severity cut-offs). Thirdly, the inclusion of a study was based on the specification of depression as a primary outcome and it is likely that some studies were excluded, or depression was deemed secondary, based on semantics. Lastly, the timeline for outcome measurement in regards to prevention was not objectively defined (i.e., 6 months), thus we do not know whether the changes observed in some studies were fleeting improvements or sustained prevention.
Conclusions
More research is needed in the preluding or early stages of depression development in individuals with T2D such that the exacerbation of depressive symptoms can be avoided. Thwarting rates of major depression in this population has important implications in terms of treatment success, recovery, and healthcare costs (85, 86). Our findings suggest that incorporating a psychological component can be of practical benefit in comprehensive T2D educational approaches; specific attention to an individual's general mental state while cultivating positivity and well-being is also promising. Future studies will help us understand how to tailor preventive efforts to sub-group of individuals with T2D as well as how and when to deliver specific program components.
Author Contributions
EG, HJ, LA, DP, and CA defined the search strategy. EG, HJ, and LA did the article screening, selection, and data extraction. EG conducted the synthesis and drafted the narrative summary. HJ, DP, and CA revised the summary and manuscript critically for important intellectual content.
Funding
This work was supported by operating funds to CA, postdoctoral scholarships to EG and HJ and summer scholarship to LA from Institut du Savoir Montfort—Recherche.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Jean Grenier, Paul Greenman, Pascal Imbeault, and Isabelle Giroux for their advice on the review protocol and establishing inclusion/exclusion criteria.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2019.00035/full#supplementary-material
Footnotes
1. ^As the objective of this scoping review was not to evaluate efficacy but rather the intervention components, we excluded reviews from our analyses, although the reference lists were checked for relevant studies.
References
2. Forouhi NG, Wareham NJ. Epidemiology of diabetes. Medicine. (2014) 42:698–702. doi: 10.1016/j.mpmed.2014.09.007
3. da Rocha Fernandes J, Ogurtsova K, Linnenkamp U, Guariguata L, Seuring T, Zhang P, et al. IDF Diabetes Atlas estimates of 2014 global health expenditures on diabetes. Diabetes Res Clin Pract. (2016) 117:48–54. doi: 10.1016/j.diabres.2016.04.016
4. Tancredi M, Rosengren A, Svensson AM, Kosiborod M, Pivodic A, Gudbjornsdottir S, et al. Excess mortality among persons with type 2 diabetes. N Engl J Med. (2015) 373:1720–32. doi: 10.1056/NEJMoa1504347
5. Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1.9 million people. Lancet Diabetes Endocrinol. (2015) 3:105–13. doi: 10.1016/S2213-8587(14)70219-0
6. Gregg EW, Sattar N, Ali MK. The changing face of diabetes complications. Lancet Diabetes Endocrinol. (2016) 4:537–47. doi: 10.1016/S2213-8587(16)30010-9
7. Jeong JH, Um YH, Ko SH, Park JH, Park JY, Han K, et al. Depression and mortality in people with type 2 diabetes mellitus, 2003 to 2013: a Nationwide population-based cohort study. Diabetes Metabol J. (2017) 41:296–302. doi: 10.4093/dmj.2017.41.4.296
8. Andreoulakis E, Hyphantis T, Kandylis D, Iacovides A. Depression in diabetes mellitus: a comprehensive review. Hippokratia. (2012) 16:205–14.
9. Semenkovich K, Brown ME, Svrakic DM, Lustman PJ. Depression in type 2 diabetes mellitus: prevalence, impact, and treatment. Drugs. (2015) 75:577–87. doi: 10.1007/s40265-015-0347-4
10. Esbitt SA, Tanenbaum ML, Gonzalez JS. Disentangling clinical depression from diabetes-specific distress: making sense of the mess we've made. In: Lloyd CE, Pouwer F, Hermanns N, editors. Screening for Depression and Other Psychological Problems in Diabetes: A Practical Guide. London: Springer (2013). p. 27–46.
11. APA. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5 ed. Arlington, VA (2013). p. 947
12. Pettersson A, Bostrom KB, Gustavsson P, Ekselius L. Which instruments to support diagnosis of depression have sufficient accuracy? A systematic review. Nordic J Psychiatry. (2015) 69:497–508. doi: 10.3109/08039488.2015.1008568
13. Egede LE, Zheng D, Simpson K. Comorbid depression is associated with increased health care use and expenditures in individuals with diabetes. Diabetes Care. (2002) 25:464–70. doi: 10.2337/diacare.25.3.464
14. Holt RI, van der Feltz-Cornelis CM. Key concepts in screening for depression in people with diabetes. J Affect Disord. (2012) 142(Suppl):S72–9. doi: 10.1016/S0165-0327(12)70011-3
15. Ciechanowski PS, Katon WJ, Russo JE. Depression and diabetes: impact of depressive symptoms on adherence, function, and costs. Arch Intern Med. (2000) 160:3278–85. doi: 10.1001/archinte.160.21.3278
16. Gonzalez JS, Schneider HE, Wexler DJ, Psaros C, Delahanty LM, Cagliero E, et al. Validity of medication adherence self-reports in adults with type 2 diabetes. Diabetes Care. (2013) 36:831–7. doi: 10.2337/dc12-0410
17. Holt RI, Katon WJ. Dialogue on diabetes and depression: dealing with the double burden of co-morbidity. J Affect Disord. (2012) 142(Suppl):S1–3. doi: 10.1016/S0165-0327(12)00632-5
18. Berge LI, Riise T. Comorbidity between type 2 diabetes and depression in the adult population: directions of the association and its possible pathophysiological mechanisms. Int J Endocrinol. (2015) 2015:164760. doi: 10.1155/2015/164760
19. Chrvala CA, Sherr D, Lipman RD. Diabetes self-management education for adults with type 2 diabetes mellitus: a systematic review of the effect on glycemic control. Patient Educ Counsel. (2016) 99:926–43. doi: 10.1016/j.pec.2015.11.003
20. Katon WJ. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin Neurosci. (2011) 13:7–23.
21. van der Feltz-Cornelis CM, Nuyen J, Stoop C, Chan J, Jacobson AM, Katon W, et al. Effect of interventions for major depressive disorder and significant depressive symptoms in patients with diabetes mellitus: a systematic review and meta-analysis. General Hospital Psychiatry. (2010) 32:380–95. doi: 10.1016/j.genhosppsych.2010.03.011
22. Casanas R, Catalan R, del Val JL, Real J, Valero S, Casas M. Effectiveness of a psycho-educational group program for major depression in primary care: a randomized controlled trial. BMC Psychiatry. (2012) 12:230. doi: 10.1186/1471-244X-12-230
23. Munoz RF, Ying YW, Bernal G, Perez-Stable EJ, Sorensen JL, Hargreaves WA, et al. Prevention of depression with primary care patients: a randomized controlled trial. Am J Commun Psychol. (1995) 23:199–222. doi: 10.1007/BF02506936
24. Atlantis E, Fahey P, Foster J. Collaborative care for comorbid depression and diabetes: a systematic review and meta-analysis. BMJ Open. (2014) 4:e004706. doi: 10.1136/bmjopen-2013-004706
25. Markowitz SM, Gonzalez JS, Wilkinson JL, Safren SA. A review of treating depression in diabetes: emerging findings. Psychosomatics. (2011) 52:1–18. doi: 10.1016/j.psym.2010.11.007
26. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
27. Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthcare. (2015) 13:141–6. doi: 10.1097/XEB.0000000000000050
28. Peters M, Godfrey C, McInerney P, Soares C, Khalil H, Parker D. The Joanna Briggs Institute Reviewers' Manual 2015: Methodology for JBI Scoping Reviews. Adelaide, SA Australia: The Joanna Briggs Institute (2015). p. 24.
29. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
30. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch General Psychiatry. (1961) 4:561–71. doi: 10.1001/archpsyc.1961.01710120031004
31. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Measur. (1977) 1:385–401. doi: 10.1177/014662167700100306
32. Abazarian E, Baboli MT, Abazarian E, Ghashghaei FE. The effect of problem solving and decision making skills on tendency to depression and anxiety in patients with type 2 diabetes. Adv Biomed Res. (2015) 4:112. doi: 10.4103/2277-9175.157830
33. Cohn MA, Pietrucha ME, Saslow LR, Hult JR, Moskowitz JT. An online positive affect skills intervention reduces depression in adults with type 2 diabetes. J Positive Psychol. (2014) 9:523–34. doi: 10.1080/17439760.2014.920410
34. Davies MJ, Heller S, Skinner TC, Campbell MJ, Carey ME, Cradock S, et al. Effectiveness of the diabetes education and self management for ongoing and newly diagnosed (DESMOND) programme for people with newly diagnosed type 2 diabetes: cluster randomised controlled trial. BMJ. (2008) 336:491–5. doi: 10.1136/bmj.39474.922025.BE
35. Dennick K, Bridle C, Sturt J. Written emotional disclosure for adults with Type 2 diabetes: a primary care feasibility study. Primary Health Care Res Dev. (2015) 16:179–87. doi: 10.1017/S1463423614000188
36. Fisher L, Polonsky W, Parkin CG, Jelsovsky Z, Amstutz L, Wagner RS. The impact of blood glucose monitoring on depression and distress in insulin-naive patients with type 2 diabetes. Curr Med Res Opin. (2011) 27(Suppl 3):39–46. doi: 10.1185/03007995.2011.619176
37. Mansour EA, Gemeay EM, Moussa IM. Counseling and depression among diabetic patients. Saudi Med J. (2013) 34:295–301.
39. Pearson S, Wills K, Woods M, Warnecke E. Effects of mindfulness on psychological distress and HbA1c in people with diabetes. Mindfulness. (2018) 9:1615–26. doi: 10.1007/s12671-018-0908-1
40. Putiri AL, Lovejoy JC, Gillham S, Sasagawa M, Bradley R, Sun GC. Psychological effects of Yi Ren Medical Qigong and progressive resistance training in adults with type 2 diabetes mellitus: a randomized controlled pilot study. Altern Ther Health Med. (2012) 18:30–4.
41. Sardar MA, Boghrabadi V, Sohrabi M, Aminzadeh R, Jalalian M. The effects of aerobic exercise training on psychosocial aspects of men with type 2 diabetes mellitus. Global J Health Sci. (2014) 6:196–202. doi: 10.5539/gjhs.v6n2p196
42. Steinhardt MA, Mamerow MM, Brown SA, Jolly CA. A resilience intervention in African American adults with type 2 diabetes: a pilot study of efficacy. Diabetes Educ. (2009) 35:274–84. doi: 10.1177/0145721708329698
43. Wagner JA, Bermudez-Millan A, Damio G, Segura-Perez S, Chhabra J, Vergara C, et al. A randomized, controlled trial of a stress management intervention for Latinos with type 2 diabetes delivered by community health workers: outcomes for psychological wellbeing, glycemic control, and cortisol. Diabetes Res Clin Pract. (2016) 120:162–70. doi: 10.1016/j.diabres.2016.07.022
44. Zagarins SE, Allen NA, Garb JL, Welch G. Improvement in glycemic control following a diabetes education intervention is associated with change in diabetes distress but not change in depressive symptoms. J Behav Med. (2012) 35:299–304. doi: 10.1007/s10865-011-9359-z
45. Malanda UL, Welschen LM, Riphagen II, Dekker JM, Nijpels G, Bot SD. Self-monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst Rev. (2012) 1:CD005060. doi: 10.1002/14651858.CD005060.pub3
46. O'Kane MJ, Bunting B, Copeland M, Coates VE, Group ES. Efficacy of self monitoring of blood glucose in patients with newly diagnosed type 2 diabetes (ESMON study): randomised controlled trial. BMJ. (2008) 336:1174–7. doi: 10.1136/bmj.39534.571644.BE
47. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. (1977) 84:191–215. doi: 10.1037/0033-295X.84.2.191
48. Malouff JM, Thorsteinsson EB, Schutte NS. The efficacy of problem solving therapy in reducing mental and physical health problems: a meta-analysis. Clin Psychol Rev. (2007) 27:46–57. doi: 10.1016/j.cpr.2005.12.005
49. Carver CS. Resilience and thriving: issues, models, and linkages. J Soc Issues. (1998) 54:245–66. doi: 10.1111/j.1540-4560.1998.tb01217.x
50. Folkman S. Positive psychological states and coping with severe stress. Soc Sci Med. (1997) 45:1207–21. doi: 10.1016/S0277-9536(97)00040-3
51. Folkman S. The case for positive emotions in the stress process. Anxiety Stress Coping. (2008) 21:3–14. doi: 10.1080/10615800701740457
52. Fredrickson BL. What good are positive emotions? Rev General Psychol. (1998) 2:300–19. doi: 10.1037/1089-2680.2.3.300
53. Kempf K, Martin S. Autonomous exercise game use improves metabolic control and quality of life in type 2 diabetes patients - a randomized controlled trial. BMC Endocr Disord. (2013) 13:57. doi: 10.1186/1472-6823-13-57
54. Fiocco AJ, Scarcello S, Marzolini S, Chan A, Oh P, Proulx G, et al. The effects of an exercise and lifestyle intervention program on cardiovascular, metabolic factors and cognitive performance in middle-aged adults with type II diabetes: a pilot study. Canad J Diabetes. (2013) 37:214–9. doi: 10.1016/j.jcjd.2013.03.369
55. Lincoln AK, Shepherd A, Johnson PL, Castaneda-Sceppa C. The impact of resistance exercise training on the mental health of older Puerto Rican adults with type 2 diabetes. J Gerontol Ser B Psychol Sci Soc Sci. (2011) 66:567–70. doi: 10.1093/geronb/gbr034
56. Yucel H, Uysal O. Pilates-based mat exercises and parameters of quality of life in women with type 2 diabetes. Iran Red Crescent Med J. (2016) 18:e21919. doi: 10.5812/ircmj.21919
57. Williams GC, Lynch M, Glasgow RE. Computer-assisted intervention improves patient-centered diabetes care by increasing autonomy support. Health Psychol. (2007) 26:728–34. doi: 10.1037/0278-6133.26.6.728
58. Rubin RR, Wadden TA, Bahnson JL, Blackburn GL, Brancati FL, Bray GA, et al. Impact of intensive lifestyle intervention on depression and health-related quality of life in type 2 diabetes: the Look AHEAD Trial. Diabetes Care. (2014) 37:1544–53. doi: 10.2337/dc13-1928
59. Allen N, Whittemore R, Melkus G. A continuous glucose monitoring and problem-solving intervention to change physical activity behavior in women with type 2 diabetes: a pilot study. Diabetes Technol Ther. (2011) 13:1091–9. doi: 10.1089/dia.2011.0088
60. Haas L, Maryniuk M, Beck J, Cox CE, Duker P, Edwards L, et al. National standards for diabetes self-management education and support. Diabetes Care. (2014) 37(Suppl 1):S144–53. doi: 10.2337/dc14-S144
61. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Counsel. (2002) 48:177–87. doi: 10.1016/S0738-3991(02)00032-0
62. Skinner TC, Cradock S, Arundel F, Graham W. Four theories and a philosophy: self-management education for individuals newly diagnosed with type 2 diabetes. Diabetes Spectrum. (2003) 16:75–80. doi: 10.2337/diaspect.16.2.75
63. Anderson-Loftin W, Barnett S, Bunn P, Sullivan P, Hussey J, Tavakoli A. Soul food light: culturally competent diabetes education. Diabetes Educ. (2005) 31:555–63. doi: 10.1177/0145721705278948
64. Attridge M, Creamer J, Ramsden M, Cannings-John R, Hawthorne K. Culturally appropriate health education for people in ethnic minority groups with type 2 diabetes mellitus. Cochrane Database Syst Rev. (2014) 9:CD006424. doi: 10.1002/14651858.CD006424.pub3
65. Sarkisian CA, Brown AF, Norris KC, Wintz RL, Mangione CM. A systematic review of diabetes self-care interventions for older, African American, or Latino adults. Diabetes Educ. (2003) 29:467–79. doi: 10.1177/014572170302900311
66. Kalibatseva Z, Leong FT. A critical review of culturally sensitive treatments for depression: recommendations for intervention and research. Psychol Serv. (2014) 11:433–50. doi: 10.1037/a0036047
67. Castillo A, Giachello A, Bates R, Concha J, Ramirez V, Sanchez C, et al. Community-based diabetes education for latinos: the diabetes empowerment education program. Diabetes Educ. (2010) 36:586–94. doi: 10.1177/0145721710371524
68. Wang ML, Lemon SC, Whited MC, Rosal MC. Who benefits from diabetes self-management interventions? The influence of depression in the Latinos en Control trial. Ann Behav Med. (2014) 48:256–64. doi: 10.1007/s12160-014-9606-y
69. Hadjiconstantinou M, Byrne J, Bodicoat DH, Robertson N, Eborall H, Khunti K, et al. Do web-based interventions improve well-being in type 2 diabetes? A systematic review and meta-analysis. J Med Internet Res. (2016) 18:e270. doi: 10.2196/jmir.5991
70. McKay HG, King D, Eakin EG, Seeley JR, Glasgow RE. The diabetes network internet-based physical activity intervention: a randomized pilot study. Diabetes Care. (2001) 24:1328–34. doi: 10.2337/diacare.24.8.1328
71. Glasgow RE, Nutting PA, Toobert DJ, King DK, Strycker LA, Jex M, et al. Effects of a brief computer-assisted diabetes self-management intervention on dietary, biological and quality-of-life outcomes. Chronic Illness. (2006) 2:27–38. doi: 10.1177/17423953060020011001
72. Glasgow RE, Boles SM, McKay HG, Feil EG, Barrera M Jr. The D-Net diabetes self-management program: long-term implementation, outcomes, and generalization results. Prevent Med. (2003) 36:410–9. doi: 10.1016/S0091-7435(02)00056-7
73. Quinn CC, Shardell MD, Terrin ML, Barr EA, Ballew SH, Gruber-Baldini AL. Cluster-randomized trial of a mobile phone personalized behavioral intervention for blood glucose control. Diabetes Care. (2011) 34:1934–42. doi: 10.2337/dc11-0366
74. Quinn CC, Khokhar B, Weed K, Barr E, Gruber-Baldini AL. Older adult self-efficacy study of mobile phone diabetes management. Diabetes Technol Ther. (2015) 17:455–61. doi: 10.1089/dia.2014.0341
75. Wayne N, Perez DF, Kaplan DM, Ritvo P. Health coaching reduces HbA1c in type 2 diabetic patients from a lower-socioeconomic status community: a randomized controlled trial. J Med Internet Res. (2015) 17:e224. doi: 10.2196/jmir.4871
76. Ma Y, Olendzki BC, Chiriboga D, Rosal M, Sinagra E, Crawford S, et al. PDA-assisted low glycemic index dietary intervention for type II diabetes: a pilot study. Eur J Clin Nutr. (2006) 60:1235–43. doi: 10.1038/sj.ejcn.1602443
77. Rosal MC, Heyden R, Mejilla R, Capelson R, Chalmers KA, Rizzo DePaoli M, et al. A virtual world versus face-to-face intervention format to promote diabetes self-management among african american women: a pilot randomized clinical trial. JMIR Res Protocols. (2014) 3:e54. doi: 10.2196/resprot.3412
78. Buntrock C, Ebert DD, Lehr D, Smit F, Riper H, Berking M, et al. Effect of a web-based guided self-help intervention for prevention of major depression in adults with subthreshold depression: a randomized clinical trial. JAMA. (2016) 315:1854–63. doi: 10.1001/jama.2016.4326
79. Mensing CR, Norris SL. Group education in diabetes: effectiveness and implementation. Diabetes Spectrum. (2003) 16:96–103. doi: 10.2337/diaspect.16.2.96
80. Odgers-Jewell K, Ball LE, Kelly JT, Isenring EA, Reidlinger DP, Thomas R. Effectiveness of group-based self-management education for individuals with Type 2 diabetes: a systematic review with meta-analyses and meta-regression. Diabetic Med. (2017) 34:1027–39. doi: 10.1111/dme.13340
81. Tang TS, Funnell MM, Anderson RM. Group education strategies for diabetes self-management. Diabetes Spectrum. (2006) 19:99–105. doi: 10.2337/diaspect.19.2.99
82. Desrosiers A, Vine V, Klemanski DH, Nolen-Hoeksema S. Mindfulness and emotion regulation in depression and anxiety: common and distinct mechanisms of action. Depress Anxiety. (2013) 30:654–61. doi: 10.1002/da.22124
83. Ruff KM, Mackenzie ER. The role of mindfulness in healthcare reform: a policy paper. Explore J Sci Heal. (2009) 5:313–23. doi: 10.1016/j.explore.2009.10.002
84. van Son J, Nyklicek I, Pop VJ, Blonk MC, Erdtsieck RJ, Pouwer F. Mindfulness-based cognitive therapy for people with diabetes and emotional problems: long-term follow-up findings from the DiaMind randomized controlled trial. J Psychosomat Res. (2014) 77:81–4. doi: 10.1016/j.jpsychores.2014.03.013
85. Katon W, Fan MY, Unutzer J, Taylor J, Pincus H, Schoenbaum M. Depression and diabetes: a potentially lethal combination. J Gener Intern Med. (2008) 23:1571–5. doi: 10.1007/s11606-008-0731-9
Keywords: type 2 diabetes, depressive disorder, prevention, comorbidity, diabetes education program
Citation: Guérin E, Jaafar H, Amrani L, Prud'homme D and Aguer C (2019) Intervention Strategies for Prevention of Comorbid Depression Among Individuals With Type 2 Diabetes: A Scoping Review. Front. Public Health 7:35. doi: 10.3389/fpubh.2019.00035
Received: 06 December 2018; Accepted: 12 February 2019;
Published: 05 March 2019.
Edited by:
Jochen Mutschler, Private Clinic Meiringen, SwitzerlandReviewed by:
Chantal Ski, Queen's University Belfast, United KingdomElena Sanchez Zaballos, Pontifical University of Salamanca, Spain
Copyright © 2019 Guérin, Jaafar, Amrani, Prud'homme and Aguer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Céline Aguer, Y2VsaW5lYWd1ZXJAbW9udGZvcnQub24uY2E=