 Alessandro G. Campolina1,2,3
Alessandro G. Campolina1,2,3 Tania Y. Yuba4
Tania Y. Yuba4 Tassia C. Decimoni4
Tassia C. Decimoni4 Roseli Leandro4Maria del Pilar Estevez Diz1Hillegonda M. D. Novaes3,4
Roseli Leandro4Maria del Pilar Estevez Diz1Hillegonda M. D. Novaes3,4 Patrícia C. de Soárez3,4*
Patrícia C. de Soárez3,4*- 1Department of Oncology, Instituto do Câncer do Estado de São Paulo, São Paulo, Brazil
- 2Instituto do Câncer do Estado de São Paulo, São Paulo, Brazil
- 3National Institute for Science and Technology for Health Technology Assessment (IATS/CNPq), Porto Alegre, Brazil
- 4Preventive Medicine, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil
Background: A large number of health economic evaluation (HEE) studies have been published in developed countries. However, Brazilian HEE literature in oncology has not been studied. Objective: To investigate whether the scientific literature has provided a set of HEE in oncology capable of supporting decision making in the Brazilian context.
Methods: A systematic review was conducted to identify and characterize studies in this field. We searched multiple databases selecting partial and full HEE studies in oncology (1998-2013).
Results: Fifty-five articles were reviewed, of these, 33 (60%) were full health economic evaluations. Type of cancers most frequently studied were: breast (38.2%), cervical (14.6%), lung (10.9%) and colorectal (9.1%). Procedures (47.3%) were the technologies most frequently evaluated. In terms of the intended purposes of the technologies, most (63.6%) were treatments. The majority of the incremental cost-effectiveness ratios (ICERs) reported have been below the cost-effectiveness threshold suggested by the World Health Organization (WHO).
Conclusions: There has been an increase in the number of HEEs related to cancer in Brazil. These studies may support decision-making processes regarding the coverage of and reimbursement of healthcare technologies for cancer treatment in Brazil.
Introduction
Every year, there are approximately 12.7 million new cases of cancer worldwide. It is estimated that, by 2030, the annual number of new cases of cancer in Latin America and the Caribbean will reach 1.7 million, resulting in more than 1 million deaths (1).
In Brazil, the annual number of new cases of cancer is expected to reach 600,000 by the end of 2018. Among males, the most common types of neoplasia are cancer of the prostate, lung, stomach, and oral cavity, whereas the most common types among women are cancer of the breast, cervix, lung, and thyroid gland, as well as nonmelanoma skin cancer (2). Within this context, major advances in the early diagnosis of certain types of cancer and greater understanding of the pathogenesis of neoplasia have led to the development of strategies for preventing and reducing the risk of cancer. Such advances, together with the development of new therapies, have helped reduce the rates of cancer-related mortality in various countries. However, this success has resulted in a substantial increase in health care expenditures for cancer treatment (3).
In parallel with the advances in cancer management, health care systems in Latin America have faced challenges related to demographic and epidemiological changes, characterized by the increased incidence of chronic noncommunicable diseases (1). Despite much progress being made in the restructuring of health care systems, such as: progress on development of cancer registries, adjustments to funding toward universal health care and support of the underserved, there are still a number of obstacles to the efficient management of chronic diseases. In the case of cancer, one particular challenge is to offer a basic level of care, including initiation of programmes for primary cancer prevention (1).
In this scenario, health economic evaluations (HEEs) play a fundamental role by helping identify the best means of allocating the financial resources of a health care system to provide the maximum benefit to the population served (4). There are two major types of HEEs: partial and full (5). Partial HEEs describes the costs and consequences of a single service or program, or compare two or more interventions only in terms of their costs. Full HEE designs include cost-consequences analysis, cost-minimization analysis, cost-effectiveness analysis, cost-utility analysis, and cost-benefit analysis (5).
A large number of HEE studies in oncology have been published in developed countries and their results highlight many opportunities for efficient investment in cancer care across cancer sites and levels of prevention (6, 7). The characteristics of the body of HEEs related to cancer in Brazil remain unknown. A systematic review of these studies could identify studies that were or are relevant for informing health care priorities and their potential economic impact (8).
In addition, the information collected may contribute to aid decision making at different levels of the health system. Clinicians would be able to better visualize the high cost of some prescriptions and the magnitude of the benefits related to them, contributing to a more rational and responsible use of the technologies offered by the health system. Researchers would be able to visualize knowledge gaps to propose health technology assessment not yet carried out in the Brazilian context. Healthcare managers would benefit from a comparative panel of the various cancer technologies, previously evaluated in Brazil. Policymakers would be able to visualize the most efficient technologies in proposing strategies and programs for delivering cancer care in the country.
Therefore, the research question that moves the present study is to investigate whether the scientific literature has provided a set of HEE in oncology capable of supporting decision making in the Brazilian context. The objective of this study was to describe the scientific literature of Brazil, in terms of HEEs related to cancer, over an extended period (1998-2013) (8).
Methods
This systematic review forms part of a larger research project that systematically reviewed all HEEs related to Brazil and published between 1980 and 2013 (9). This study is in accordance with the guidelines for systematic review of HEEs published by the UK National Health Service (NHS) Center for Reviews and Dissemination (10). We searched multiple databases, including Medline; ExcerptaMedica; the Latin American and Caribbean Health Sciences Literature database; the Scientific Electronic Library Online; the database of the Center for Reviews and Dissemination; the NHS Economic Evaluation Database; the NHS Health Technology Assessment database; and Health Economics database of the Brazilian Virtual Library of Health (search strategy in Appendix 1 in the Supplementary Material). We searched the citation indexes: Scopus; Web of Science; and the Brazilian Network for the Evaluation of Health Technologies. We also performed hand-searching, a way to scan the content of journals and other sources, page by page. It was done to identify articles from journals that are not indexed by electronic database and for full identification of relevant reports published in journals, even for those that are indexed in Medline (10). We performed hand-searching from the reference lists of included articles, and all issues of the Brazilian Journal of Health Economics (BJHE), a non-indexed journal in that period.
Articles were included if they were partial or full economic evaluations, if they dealt with cancer, if they were conducted in Brazilian setting, and if at least one of the authors was affiliated with an institution in Brazil (5). The language of article was not an exclusion criterion. For the inclusion of economic evaluation studies, the main outcomes considered, in addition to the cost of illness, were: life year gained (LYG), deaths averted, diagnostics averted, quality-adjusted life years (QALYs) and disability-adjusted life years (DALYs).
QALYs and DALYs are technically similar in that they both express health in time (life years) and give a weight to years lived with a disease. However, the difference between these measures depends on whether the quality of life is expressed as a gain (QALY) or a loss (DALY) (11). Since DALY is a widely used measure in economic evaluations conducted in developing countries or in a country for which no local health state preference values exist (5), the World Health Organization (WHO) have recommended their use in cost-effectiveness analysis and proposed a willingness to pay threshold of one to three times the per capita gross domestic product (GDP) per DALY averted, which have been considered an alternative to the QALY gained as a measure of health benefit (12). So, for the purpose of the present study the QALY gained will be used as a proxy of DALY averted, when using the WHO threshold.
Two reviewers, working independently, selected studies and extracted data using a template developed specifically for this study. Data extracted from each study included the following: year and journal of publication; type of HEE (partial and full); category of technology assessed (medications, vaccines, equipment, procedures, public health, and health promotion programs); purpose of the technology assessed (treatment, prevention, screening and diagnosis); the type of affiliation of the first author; the geographical location of the first author; conflicts of interest, as defined estimates of cost-effectiveness; and the conclusions of the studies (favorable, unfavorable, or neutral) (11). To compare the results of the studies, we converted the incremental cost-effectiveness ratios (ICERs) into United States Dollars (USD) for 2013. For studies in which the cost year was not specified, we assumed that the cost year was the same the year of publication, a strategy that has been adopted in previous reviews of the literature (13). To transform every monetary value at the same year to compare, we used the Brazilian Extended National Consumer Price Index (IPCA), available from the Central Bank of Brazil1 As an indicator of cost-effectiveness, we used the WHO cost-effectiveness threshold (12). A qualitative narrative synthesis was conducted.
Results
In total 11,841 records were identified from database searches, and 105 further articles were identified in other sources (BJHE - Brazilian Journal of Health Economics, SISREBRATS-Brazilian Network for Health Technology Assessment Database, and gray literature). We identified 9,304 non-duplicate citations, of which 721 were recognized as potentially relevant and full papers were retrieved. Out of the 721 studies 186 of them were excluded. Reasons for exclusion included: thesis (50 studies), not HEE (88 studies), no Brazilian author (19 studies), reviews (98), and other (11 studies). It resulted in 535 HEEs studies (9).
Among those 535 HEEs studies related to Brazil Figure 1, there were 55, published between 1998 and 2013, that dealt with cancer-related technologies (12, 14–68). The yearly number of studies increased over the period as did the proportion of full HEEs (in relation to that of partial HEEs) Figure 2. Of the 55 cancer-related HEEs, 47 (85.5%) were published between 2006 and 2013 and 33 (60.0%) were full HEEs. As shown in the Table 1, the most frequent study design was cost-effectiveness analysis (23.6%) and the least frequent cost-minimization analysis (3.6%). Among the partial HEEs, the most frequent study design was cost-description (14.6%), followed by cost-of-illness (10.9%).
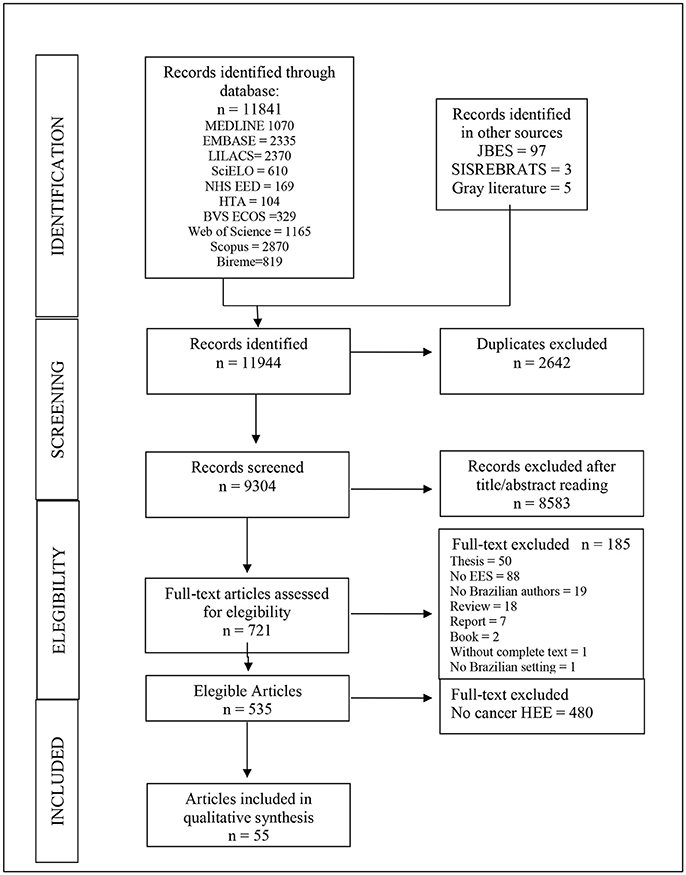
Figure 1. Flow diagram of the process for the selection of health economic evaluations related to cancer in Brazil, 1998–2013. Bireme, Biblioteca Regional de Medicina (Regional Library of Medicine); BVS ECOS, Biblioteca Virtual em Saúde Economia da Saúde (Health Economics [database] of the [Brazilian] Virtual Library of Health); EED, Economic Evaluation Database; EMBASE, Excerpta Medica; JBES, Jornal Brasileiro de Economia da Saúde (Brazilian Journal of Health Economics); LILACS, Latin American and Caribbean Health Sciences Literature; SciELO, Scientific Electronic Library Online; SISREBRATS, Sistema de Informação da Rede Brasileira de Avaliação de Tecnologias em Saúde (Brazilian Network for the Evaluation of Health Technologies).
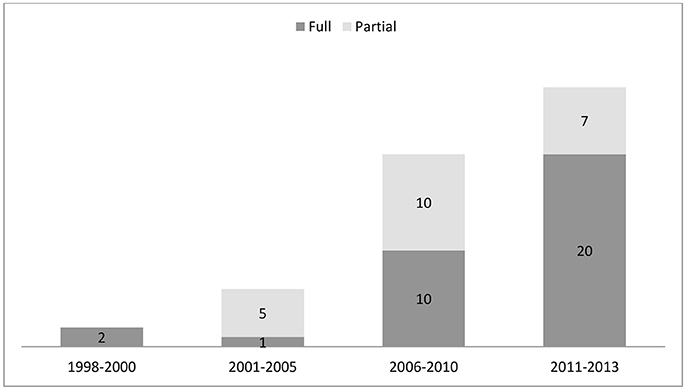
Figure 2. Number and proportional distribution of health economic evaluations related to cancer in Brazil, by publication date and type, 1998–2013.
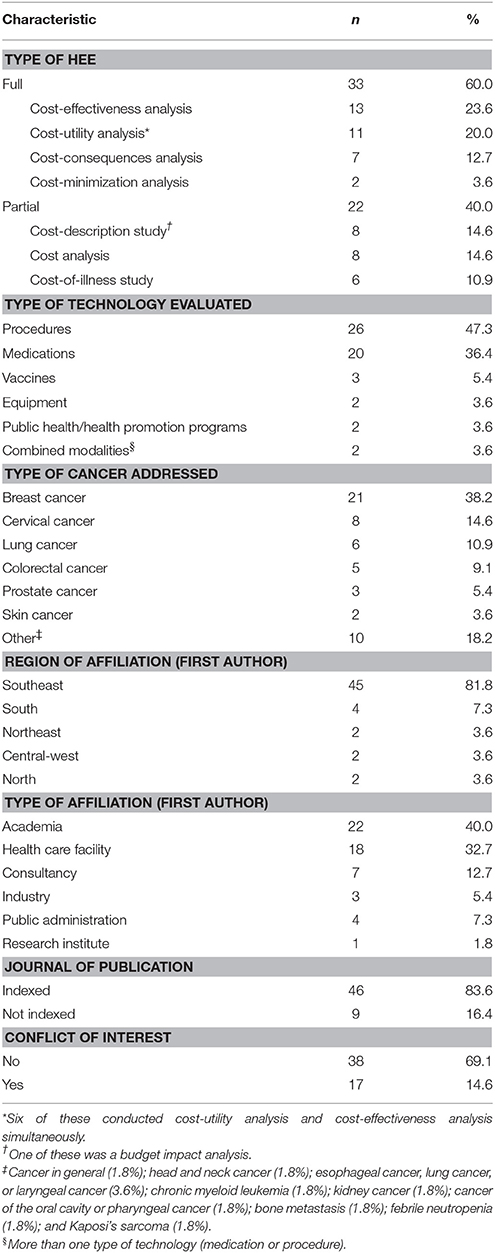
Table 1. Characteristics of health economic evaluations related to cancer in Brazil, 1998-2013.
The top five types of cancer addressed in the HEEs were: breast cancer (38.2%); cervical cancer (14.6%); lung cancer (10.9%); colorectal cancer (9.1%); and prostate cancer (5.4%).
As shown in Table 1, the technological modalities most often evaluated in the HEEs identified were procedures (47.3%), followed by medications (36.4%) and vaccines (5.4%). In terms of the intended purposes of the technologies evaluated, most (63.6%) were treatments, whereas screening methods, diagnostic procedures, and preventive measures accounted for 16.4, 14.6, and 5.4%, respectively.
Among the HEEs dealing with breast cancer (14–34), the technologies evaluated included strategies for screening with conventional and digital mammography, as well as with magnetic resonance imaging; a gene expression panel to inform decisions regarding therapy; medications (docetaxel, vinorelbine, trastuzumab, anastrozole, lapatinib, and capecitabine); screening tests for metastasis (mammography, bone scintigraphy, routine chest X-ray, and ultrasound of the liver); and procedures such as postmastectomy breast reconstruction and core biopsy. The HEEs dealing with cervical cancer (35–42) evaluated strategies for screening with liquid-based cytology; human papillomavirus (HPV) detection by hybrid capture assay; Pap smear; molecular biology methods for the diagnosis of HPV infection; and vaccination against HPV. Among the HEEs related to lung cancer (43–48), the technologies evaluated included medications such as erlotinib, gefitinib, and the pemetrexed-cisplatin combination; and strategies for clinical follow-up and metabolic staging with positron emission tomography. The HEEs related to colorectal cancer (49–53) dealt with technologies such as chemotherapy regimens (modified 5-fluorouracil/leucovorin/oxaliplatin; 5-fluorouracil/folinic acid/oxaliplatin; folinic acid/5-fluorouracil/irinotecan; capecitabine/oxaliplatin; and capecitabine/irinotecan); and a procedure involving transanal endoscopic microsurgery.
Analyzing the geographic distribution of the affiliations of the first authors, we noted a concentration of HEEs from southeastern Brazil, which accounted for 45 (81.8%) of the 55 studies identified Table 1, of which 31 (56.4%) and 12 (21.8%) were from the states of São Paulo and Rio de Janeiro, respectively, both of which are in the southeastern region. The first authors of the selected articles had the following types of affiliations Table 1: academia, in 22 studies (40.0%); health care facilities, in 18 (32.7%); and industry or consultancy, in 10 (18.2%). Potential conflicts of interest were identified in 14.6% Table 1. The majority (83.6%) of the HEEs evaluated were published in indexed journals Table 1.
The ICERs were presented in relation to two outcome measures: LYG and QALYs gained. The ICER per QALY gained ranged from USD466.45 to USD374,630.96.
Of the 55 studies evaluated in our review, 23 (41.8%) calculated the ICERs. We found that the ICERs for technologies used in the treatment of breast cancer ranged from USD914.89 to USD285,874 (across 8 studies), compared with USD436.48 to USD16,706.75 (across 6 studies) for cervical cancer, USD6,380 to USD320,880 (between 2 studies) for lung cancer, USD47,399 to USD66,892 (between 2 studies) for colorectal cancer, and USD3,123 to USD190,193 (across 4 studies) for other types of cancer.
The lowest ICER per QALY value was for vaccination against HPV (vs. no vaccination), whereas the highest value was for the treatment of breast cancer (lapatinib + capecitabine vs. capecitabine or trastuzumab + capecitabine), as depicted in Figure 3. The ICER per LYG ranged from USD3,505.45 to USD120,832.12. The lowest ICER per LYG value was for the treatment of head and neck cancer (cisplatin-based chemotherapy vs. radiotherapy), whereas the highest value was for the treatment of breast cancer (lapatinib + capecitabine vs. capecitabine or trastuzumab + capecitabine), as depicted in Figure 4. In only four of the HEEs evaluated (19,57,58,67), the ICERs reported were above the threshold of three times the per capita GDP per DALY averted, established by the WHO (12).
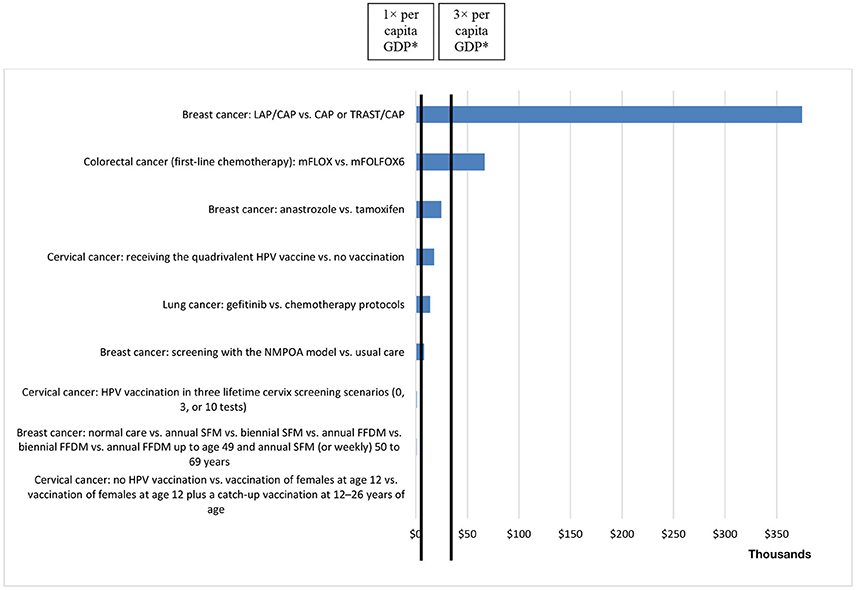
Figure 3. ICERs per QALY gained, in United States Dollars (at 2013 rates), reported in health economic evaluations related to cancer in Brazil, 1998–2013 (× USD 1,000). *1× per capita GDP = USD 14,588.62; 3× per capita GDP = USD 43,765.86 (2013). CAP, capecitabine; LAP, lapatinib; mFLOX, modified 5-fluorouracil, leucovorin, and oxaliplatin; mFOLFOX6, modified 5-fluorouracil, folinic acid, and oxaliplatin (mFOLFOX6); NMPOA, Núcleo Mama Porto Alegre (Breast Center of Porto Alegre); SFM, screen-film mammography; FFDM, full-field digital mammography; TRAST, trastuzumab.
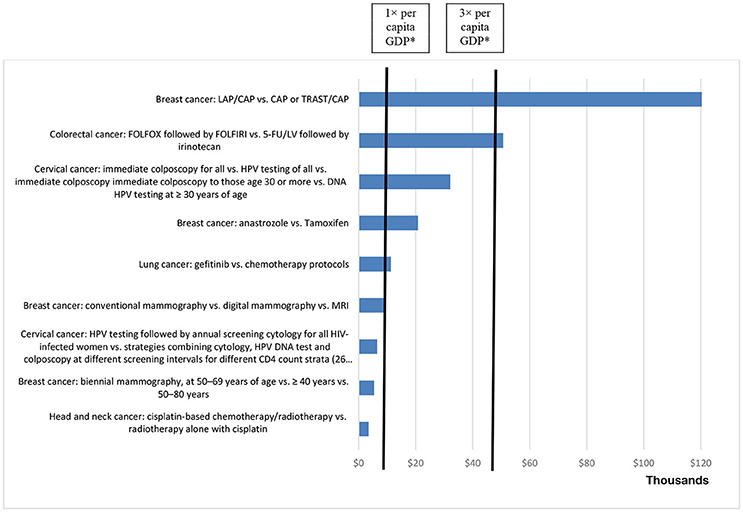
Figure 4. ICERs per life year gained, in United States Dollars (at 2013 rates), reported in health economic evaluations related to cancer in Brazil, 1998–2013 (× USD 1,000). *1× per capita GDP = USD 14,588.62; 3× per capita GDP = USD 43,765.86 (2013). 5-FU/LV, 5-fluorouracil plus leucovorin; FOLFIRI, folinic acid, 5-fluorouracil, and irinotecan; FOLFOX, 5-fluorouracil, folinic acid, and oxaliplatin; MRI, magnetic resonance imaging.
Discussion
Because of the shortage of health care resources, together with the great technological development over recent decades, health technology assessments (HTAs), like HEEs, have come to play a greater role in the process of incorporating new technologies into health care systems (5). In Brazil, the growth of scientific literature in this field of knowledge has occurred within the context of the process of devising the Brazilian Ministry of Health (MoH) statement of the National Policy on Health Technologies Management. In the second half of the preceding decade, there was a significant increase in the number of HEEs related to cancer in Brazil, most of which were published in indexed journals (4).
There was a predominance of HEEs evaluating procedures and medications, which can be attributed to the fact that, in Brazil, the articulation of the Agência Nacional de Vigilância Sanitária (ANVISA, National Health Surveillance Agency) with MoH Department of Science, Technology, and Strategic Resources and with the National Health Agency. Since 2000, ANVISA has been regulating the sales of medications. In 2004, ANVISA required HEE as part of the decision-making process related to determining the price of any new medication (4).
In other countries, medications have also been the health technologies most often evaluated in economic studies (7). However, when dealing with a complex condition like cancer, studies evaluating other types of technologies, such as surgical interventions, are of great importance. Without such studies, decisions regarding incorporation of such procedures would be made at the health care facility level, with or without the approval of local committees for the evaluation and management of health technologies (6, 69).
There is a lack of robust evidence on the cost-effectiveness of surgical intervention in the treatment of breast, colorectal, and prostate cancer (69). Among the 17 cancer-related economic evaluations identified in a review, surgical interventions for the treatment of breast cancer were evaluated in only three, all of which were published before 2003. Because surgical interventions are often associated with great potential benefits (cure vs. no cure) or harms (morbidity and mortality), the limited number of economic evaluations of such interventions raises the question of what type of evidence has been used in the development of the corresponding coverage and reimbursement recommendations (7, 69).
Although evidence on the cost effectiveness of radiotherapy in cancer is heterogeneous, a systematic review highlights the importance of the identification of specific types of patients in whom radiotherapy is cost effective (70). Furthermore, it is important to consider that studies might be dated due to improvements in clinical practice, since radiotherapy techniques have evolved rapidly over the last decade and many newer techniques are currently being evaluated in clinical trials (7, 70).
The development of targeted therapies and personalized cancer medicine appears to be another key issue (71). The consequences for technology joint assessment of a diagnostic technology and a treatment has additional methodological complexities and are not yet fully worked out. One view is that the basic principles of HTA still apply and that this is not different from undertaking HTA for diagnostics and treatments in other diseases. Another view is that the new paradigm changes not only the regulatory assessments but also the way the broader aspects of the technology are assessed (71).
In the present review, we found that breast cancer was the type of neoplasia most often addressed in economic evaluations related to Brazil. We identified two HEEs related to the use of mammography in breast cancer screening in Brazil. Despite the fact that the scientific literature has contained evidence that such screening reduces mortality since 1993 (1), those two studies (a partial HEE and a full HEE) were published only in 2005 and 2010, respectively. Similarly, the breast cancer drugs anastrozole and trastuzumab, approved by the United States Food and Drug Administration (FDA) in 1996 and 1998, respectively, were not evaluated in HEEs related to Brazil until 2009 and 2008, respectively (27, 33). Although HEEs related to breast cancer have been conducted only recently in Brazil, as have those related to other aspects of oncology, these results indicate the importance of breast cancer, not to mention that of nonmelanoma skin cancer, the former representing the most common type of neoplasia among women in developed and developing countries alike, as well as being the leading cause of cancer death among women worldwide (2).
The second most common topic addressed in HEEs dealing with cancer in Brazil is cancer of the cervix, the importance of which is recognized due to the fact that it is a major public health problem, principally in the northern region of the country, where it has an incidence rate higher than that of any other type of neoplasia (1, 2). Economic studies of HPV screening in the population of Brazil were published in 2006 and 2007, coinciding with FDA approval of the first HPV vaccine, in 2006. The HPV vaccine shows great promise as a tool in the battle against cervical cancer. Its incorporation into the standard practices of the Sistema Único de Saúde (SUS, the Brazilian National Health System), via which it has been available since 2014, was supported by HEEs conducted in Brazil (39).
The third most common type of cancer evaluated in HEEs related to cancer in Brazil is lung cancer (2). That apparently reflects the level of concern regarding a condition that is recognized as the leading cause of cancer death worldwide (2, 3). Economic evaluations of lung cancer drugs, commissioned by the pharmaceutical industry, began to appear in Brazil between 2008 and 2012, a period during which the FDA was in the process of approving the anaplastic lymphoma kinase inhibitor crizotinib for the treatment of small cell lung cancer, providing prospects for improved survival (43, 48). Lung cancer is typically detected in the advanced stages, often requiring chemotherapy, despite the high mortality associated with the disease (2). Therefore, it is highly advisable to conduct rigorous economic evaluations of the therapeutic measures employed in cases of lung cancer (6, 7).
Colorectal cancer, which is estimated to be the second and third leading cause of cancer death among women and men, respectively, worldwide, is another important topic to be addressed in HEEs (1–3). The increased incidence of colorectal cancer has been attributed to greater urbanization and to the growing consumption of highly processed foods, and data related to colorectal cancer in the more developed regions of Brazil are comparable to those reported worldwide (2). Although recommended measures for the prevention of colorectal cancer (the use of the fecal occult blood test, flexible sigmoidoscopy, or colonoscopy) have been widely recognized and employed since 1993 (1), there have yet to be any HEEs of the use of such technologies in Brazil. The majority of studies of colorectal cancer in Brazil have focused on medications used in its treatment, which have been evaluated since 2008, including biologics such as the monoclonal antibody bevacizumab, approved by the FDA in 2004 and evaluated in an HEE related to Brazil in 2012 (49–52).
Consistent with these findings, another review of 242 cancer-related CUAs published in different parts of the world, through 2007, showed that the most frequent cancers studied were breast cancer (36% of studies), colorectal cancer (12%), and hematologic cancers (10%) (70, 71). In Spain, 13.0% of economic evaluations, published between 1990 and 2009, referred to cancer-related processes (72), and the disease most frequently evaluated was non-small cell lung cancer (31 %) (73).
Cancer treatment is a major focus of innovation in the field of medicine. Worldwide, the pharmacological treatment of cancer has an annual cost of approximately 40 billion US dollars (74). There have been a great number of studies showing that ICERs for oncological treatments, especially for new pharmacological therapies, are not below the threshold that would favor the incorporation of such treatments (6, 7). However, despite the general perception that the costs of treating cancer have increased, it should be borne in mind that technological innovations in the area of individualized medical treatment and the fact that the patents for many high-cost medications have lapsed present opportunities for reducing those costs (75).
Because the cost-effectiveness threshold for the incorporation of new technologies has yet to be defined in Brazil, the comparison of the ICERs estimated in oncology studies, using similar measures in different areas of medicine, could guide health care managers in their resource allocation decisions or at least inform them of which cancer treatments are the most costly. The WHO recommended, as a reference, that the threshold for the incorporation of a new technology into a health care system should be between one and three times the per capita GDP (12), but there is still no consensus on the subject (76). According to the Brazilian Institute of Geography and Statistics, the per capita GDP in Brazil, for 2013, was USD14,588.62. The ICERs reported for most of the health technologies evaluated in the HEEs under study were below the upper limit of the threshold suggested by the WHO. On the other hand, if the upper limit of York threshold were used (USD14,109.70), only 4 technologies would be considered cost-effective (77). However, of those same articles, 87.0% made recommendations in favor of incorporating the technologies evaluated, despite not having a cost-effectiveness threshold defined for Brazil and not even drawing comparisons with an international reference (such as that suggested by the WHO) or with technologies employed in other areas of medicine. This suggests a tendency, on the part of the scientific literature, to pressure health care systems to incorporate new technologies. Nevertheless, studies that addressed the relative value of oncologic pharmaceuticals used higher value thresholds and reported higher ICERs than studies evaluating noncancer drugs (78). Furthermore, because HTAs represent a relatively new research area in Brazil, it would not be surprising if most still do not rigorously adhere to international protocols and recommendations for the execution and publication of HEEs.
Only six technologies (five medications: Imatinib Mesylate, Rituximab, Erbitux, Trastuzumab, Gefitinib, Erlotinib, and one diagnostic test: PET-CT) evaluated in the HEE studies included in this review were analyzed by the Commission on Technology Incorporation—CITEC and National Committee for Health Technology Incorporation in SUS—CONITEC, advisory committees of the MoH on assignments relating to incorporation, exclusion or modification of health technologies by the SUS.
Our review has certain limitations that merit consideration. First, we did not evaluate the quality of the studies in accordance with established guidelines. Furthermore, it should be borne in mind that a considerable portion of the studies conducted in Brazil are supported by industries, and it is therefore possible that, in some cases, studies whose results were unfavorable to the incorporation of the technologies evaluated were not published. Coincidence or not, we noted that industry-supported studies tended to report lower ICERs, thus favoring the incorporation of the technologies evaluated (7).
Faced with budgetary constraints and rising health care costs, many countries have used HEEs as guides in making decisions regarding coverage, which has often limited patient access to costly new treatments (5). The lack of evidence from HEEs and unfavorable ICERs have both been used in order to justify the refusal to cover such treatments (7). Therefore, the explosion of high-cost innovations in oncology (71, 74) has created a common need to realign economic incentives, to improve communication at the clinical level, and to give greater weight to scientific evidence regarding the cost-effectiveness of cancer care (6, 7).
It is fundamental that growth in the area of HEEs related to Brazil be stimulated and that reviews of that literature be conducted in order to aggregate the data and allow the technologies employed in various areas of health care to be compared, in terms of their cost-effectiveness. Likewise, it is important to encourage discussions regarding the cost-effectiveness threshold in Brazil, which could serve as yet another objective criterion to inform and increase the transparency of the decision-making process surrounding the incorporation of new technologies into the standard practices of the SUS.
The incidence of cancer is on the rise worldwide, and the economic burden associated with its management has risen apace (1–3). Low- to middle-income countries, such as Brazil, will bear the brunt of that burden. One of the major challenges facing those countries is that of devising strategies to deal with their limited resources, allocating those resources appropriately in their management of cancer cases (79). Therefore, we hope that our findings will promote the incorporation of cost-effectiveness analyses in the decision-making processes regarding the coverage of and reimbursements for the use of cancer treatment technologies in Brazil.
Conclusion
There has been an increase in the number of HEEs related to cancer in Brazil. The majority of the ICERs reported in such studies have been below the cost-effectiveness threshold suggested by the WHO for the incorporation of new health technologies. From a research standpoint, we emphasize the need to evaluate the quality of such studies conducted in Brazil.
The findings may contribute to support policymakers, researchers and clinicians in different ways. Policymakers can identify the most efficient technologies, which leads to a better allocation of resources. Researchers can visualize knowledge gaps to propose new HTA studies not yet carried out in the Brazilian context. Furthermore, clinicians can better visualize the high relation between costs and benefits, thus they can contribute to a more rational and responsible use of the technologies offered by the health system.
Author Contributions
All authors drafted the systematic review protocol. AC, TY, TD, RL, and PdS conducted the search, selection of records, and data extraction. Quality appraisal was conducted by TY, TD, RL, and PdS. All authors have read and approved the final manuscript.
Funding
Supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP, São Paulo Research Foundation), as part of a larger project entitled Systematic review of health economic evaluations conducted in Brazil, 1980–2013, carried out under the leadership of Professor Patricia Coelho de Soárez (FAPESP Research Grant no. 2012/22126-3 and 2015/02713-0) and by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; National Counsel of Technological and Scientific Development) (CNPq Research Grant No. 305614/2013-4).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2018.00205/full#supplementary-material
Footnotes
References
1. Strasser-Weippl K, Chavarri-Guerra Y, Villarreal-Garza C, Bychkovsky BL, Debiasi M, Liedke PER, et al. Progress and remaining challenges for cancer control in Latin America and the Caribbean. Lancet Oncol. (2015) 16:1405–38. doi: 10.1016/S1470-2045(13)70048-2
2. Instituto Nacional de Câncer José Alencar Gomes da Silva (INCA). Estimativa 2018: Incidência de Câncer no Brasil. Coordenação de Prevenção e Vigilância (2017). Available online at: http://www2.inca.gov.br/wps/wcm/connect/en-inca/portal/home
3. American Society of Clinical Oncology (ASCO). Major Cancer Milestones. American Society of Clinical Oncology. (2014). Available online at: https://www.asco.org/research-progress/cancer-progress-timeline
4. Novaes HMD, de Soárez PC. Organizaciones de evaluación de tecnologías en salud (ETS): dimensiones del marco institucional y político. Cad Saúde Pública. (2016) 32:S1–14. doi: 10.1590/0102-311X00022315
5. Drummond M, Sculpher M, Torrance G, O'Brien B SG. Methods for the Economic Evaluation of Health Care Programmes. New York, NY: Oxford University Press (2015).
6. Winn AN, Ekwueme DU, Guy GP, Neumann PJ. Cost-utility analysis of cancer prevention, treatment, and control: a systematic review. Am J Prev Med. (2016) 50:241–48. doi: 10.1016/j.amepre.2015.08.009
7. Greenberg D, Earle C, Fang C-H, Eldar-Lissai A, Neumann PJ. When is cancer care cost-effective? A systematic overview of cost-utility analyses in oncology. J Natl Cancer Inst. (2010) 102:82–8. doi: 10.1093/jnci/djp472
8. Anderson R. Systematic reviews of economic evaluations: utility or futility? Health Econ. (2010) 19:350–64. doi: 10.1002/hec.1486
9. Decimoni TC, Leandro R, Rozman LM, Craig D, Iglesias CP, Novaes HMD, et al. Systematic review of health economic evaluation studies developed in Brazil from 1980 to 2013. Front Public Health (2018) 6:52. doi: 10.3389/fpubh.2018.00052
10. Centre for Reviews and Dissemination (CRD). Systematic Reviews. CRD's Guindance for Undertarking Reviews in Health Care. University of York (2008). Available online at: https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf
11. Gold MR, Stevenson D, Fryback DG. HALYs and QALYs and DALYs, Oh My: similarities and differences in summary measures of population Health. Annu Rev Public Health (2002) 23:115–34. doi: 10.1146/annurev.publhealth.23.100901.140513
12. World Health Organization (WHO). Macroeconomics and health : investing in health for economic development: executive summary/report of the Commission on Macroeconomics and Health. World Health Organization. (2001). Available online at: http://apps.who.int/iris/handle/10665/42435
13. Anonychuk AM, Tricco AC, Bauch CT, Pham B, Gilca V, Duval B, et al. Cost-effectiveness analyses of hepatitis A vaccine: a systematic review to explore the effect of methodological quality on the economic attractiveness of vaccination strategies. Pharmacoeconomics (2008) 26:17–32. doi: 10.2165/00019053-200826010-00003
14. Abdo Filho E, Takemoto MLS, Teich VD, Quintella FF, Fernandes RA, Passos RBF, et al. Advanced breast cancer treatment, hormone- receptor-positive with endocrine therapy versus chemotherapy: economic analysis in the Brazilian Public Healthcare System (BPHS) Advanced breast cancer treatment, economic analysis. J Bras Econ Saúde (2010) 2:46–51.
15. Teich V, Pereira ML, Morais A. Análise de custo-efetividade do tratamento do mieloma múltiplo em primeira, segunda e terceira linha sob a perspectiva do Sistema Único de Saúde Brasileiro (SUS). J Bras Econ Saúde (2010) 2:134–43.
16. Marques RM, Mendes A, Leite MG, Barbosa E. Custos da cadeia de procedimentos do câncer de mama nos hospitais brasileiros de excelência e especializados. J Bras Econ Saúde (2011) 3:251–58.
17. Fernandes RA, Takemoto MLS, Cammarota MC, Arcoverde MM, Fraga M. Utilização de recursos e custos associados às cirurgias de reconstrução de mama pós- mastectomia com expansores temporários versus expansores permanentes sob a perspectiva do Sistema de Saúde Suplementar. J Bras Econ Saúde (2011) 3:211–16.
18. Chein MBC, Brito LM, Rotstein S, Gebrim LH, Reis AFF, Padilha L. Rastreamento de metástases no pré-operatório do câncer de mama. Rev Bras Ginecol Obstet. (1998) 20:475–79. doi: 10.1590/S0100-72031998000800008
19. Kemp C, Elias S, Gebrim LH, Nazário ACP, Baracat EC, Lima G. Estimativa de custo do rastreamento mamográfico em mulheres no climatério. Rev BrasGinecol Obstet. (2005) 27:415–20. doi: 10.1590/S0100-72032005000700008
20. Bianchessi PT, Souza AG, Bianchessi S. Desempenho da biópsia de agulha grossa (de fragmento) e o seu impacto na conduta de pacientes com lesões mamárias suspeitas não palpáveis. Rev Bras Mastol. (2006) 1:12–6.
21. Martins S. Implicações clínicas e econômicas da quimioterapia adjuvante no câncer de mama HER-2/NEU positivo. Rev Bras Mastol. (2007) 3:97–101.
22. Asevedo FMF, Koch H. Avaliaçao dos custos para implantaçao de um serviço de mamografia. Radiol Bras. (2004) 37:101–5. doi: 10.1590/S0100-39842004000200007
23. Bacchi CE, Prisco F, Carvalho FM, Saad E. Potential economic impact of the 21 - gene expression assay on the treatment of breast cancer in brazil. Rev Assoc Med Bras. (2010) 56:186–91. doi: 10.1590/S0104-42302010000200017
24. Cerci JJ, Trindade E, Pracchia LF, Pitella FA, Linardi CC, Soares J Jr, et al. Cost effectiveness of positron emission tomography in patients with Hodgkin's lymphoma in unconfirmed complete remission or partial remission after first-line therapy. J Clin Oncol. (2010) 28:1415–21. doi: 10.1200/JCO.2009.25.4367
25. Coelli FC, Almeida RMVR, Pereira WC. A cost simulation for mammography examinations taking into account equipment failures and resource utilization characteristics. J Eval Clin Pract. (2010) 16:1198–202. doi: 10.1111/j.1365-2753.2009.01294.x
26. Oliveira ATR, Rabelo LM, Costa AD, Lessa I. Características da demanda por tomografia computadorizada crânio-encefálica. Arq Neuro-Psiquiat. (1992) 50:91–8. doi: 10.1590/S0004-282X1992000100016
27. Fonseca M, Araújo GT, Saad E. Cost-effectiveness of anastrozole, in compatison with tamoxifen, in the adjuvant treatment of early breast cancer in Brazil. Rev Assoc Med Bras. (2009) 55:410–15. doi: 10.1590/S0104-42302009000400015
28. Marconato RRF, Soárez PC, Ciconelli R. Custos dos mutirões de mamografia de 2005 e 2006 na Direção Regional de Saúde de Marília, São Paulo, Brasil. Cad Saúde Publica. (2011) 27:1529–36. doi: 10.1590/S0102-311X2011000800008
29. Sasse AD, Sasse E. Estudo de custo-efetividade do anastrozol adjuvante no câncer de mama em mulheres pós - menopausa. Rev Assoc Med Bras. (2009) 55:535–40. doi: 10.1590/S0104-42302009000500015
30. Lima DE, Veiga Filho J, Ribeiro LM, Morais TB, Rocha LRM, Juliano Y, et al. Oncoplastic approach in the conservative treatment of breast cancer. Analysis of costs. Arq Cirúrgica Bras. (2012) 27:311–14. doi: 10.1590/S0102-86502012000500006
31. Machado M, Einarson T. Lapatinib in patients with metastatic breast cancer following initial treatment with trastuzumab : an economic analysis from the Brazilian public health care perspective. Breast Cancer Targets Ther. (2012) 4:173–82. doi: 10.2147/BCTT.S37003
32. Augusto A, Peregrino DF, Gonzáles GB, Eduardo C, Machado SCF, Costa e Silva FV, et al. Análise de Custo-efetividade do rastreamento do câncer de mama com mamografia convencional, digital e ressonância. Cien Saude Colet. (2012) 17:215–22. doi: 10.1590/S1413-81232012000100023
33. Martins SJ, Yamamoto C. Aspectos clinico-econômicos da quimioterapia adjuvante no câncer de mama HER-2 positivo. Rev Assoc Med Bras. (2008) 54:494–9. doi: 10.1590/S0104-42302008000600012
34. Peregrino AAF, Vianna CMM, Caetano R, Mosegui GBG, Almeida CEV, Machado S. Análise de Custo-Efetividade da Idade de Início do Rastreamento Mamográfico. Rev Bras Cancerol. (2010) 56:187–93.
35. Fonseca AJ, Ferreira LP, Dalla-Benetta AC, Roldan CN, Ferreira M. Epidemiologia e impacto econômico do câncer de colo de útero no Estado de Roraima: a perspectiva do SUS. Rev Bras Ginecol Obstet. (2010) 32:386–92. doi: 10.1590/S0100-72032010000800005
36. Vanni T, Legood R, Franco EL, Villa LL, Luz PM, Schwartsmann G. Economic evaluation of strategies for managing women with equivocal cytological results in Brazil. Int J Cancer (2011) 129:671–79. doi: 10.1002/ijc.25708
37. Nomelini RS, Guimarães PDN, Campos ANC, Michelin MA, Murta E. Prevention of cervical cancer in women with ASCUS in the Brazilian unified national health system: cost-effectiveness of the molecular biology method for HPV detection Prevenção de câncer de colo uterino em pacientes com ASCUS no Sistema Único de Saúde. Cad Saúde Publica. (2012) 28:2043–52. doi: 10.1590/S0102-311X2012001100004
38. Vanni T, Luz PM, Grinsztejn B, Veloso VG, Foss A, Mesa-Frias M, et al. Cervical cancer screening among HIV-infected women: an economic evaluation in a middle-income country. Int J Cancer (2012) 131:E96–104. doi: 10.1002/ijc.26472
39. Fonseca AJ Da, Ferreira LCDL, Neto GB. Cost-effectiveness of the vaccine against human papillomavirus in the Brazilian Amazon region. Rev Assoc Med Bras. (2013) 59:442–51. doi: 10.1016/j.ramb.2013.03.004
40. Vanni T, Mendes Luz P, Foss A, Mesa-Frias M, Legood R. Economic modelling assessment of the HPV quadrivalent vaccine in Brazil: a dynamic individual-based approach. Vaccine (2012) 30:4866–71. doi: 10.1016/j.vaccine.2012.04.087
41. Kawai K, de Araujo GTB, Fonseca M, Pillsbury M, Singhal PK. Estimated health and economic impact of quadrivalent HPV (types 6/11/16/18) vaccination in Brazil using a transmission dynamic model. BMC Infect Dis. (2012) 12:250. doi: 10.1186/1471-2334-12-250
42. Caetano R, Vianna CMM, Thuler LCS, Girianelli V. Custo-efetividade no diagnóstico precoce do câncer de colo uterino no Brasil. PHYSIS. Rev Saúde Colet. (2006) 16:99–118. doi: 10.1590/S0103-73312006000100007
43. Souza CPRS, Paladini L, Monteiro DCM, Paiva B. Análise de custo-efetividade de pemetrexede + cisplatina versus paclitaxel + carboplatina versus paclitaxel + carboplatina + bevacizumabe no tratamento de câncer de pulmão células não pequenas avançado sem tratamento prévio. J Bras Econ Saúde (2012) 4:382–90.
44. Marques M, Paladini L, Teich V. Avaliação econômica do tratamento de segunda linha do câncer de pulmão não pequenas células sob a perspectiva do sistema suplementar de saúde. J Bras Econ Saúde (2012) 4:335–40.
45. Piha T, Marques M, Paladini L, Teich V. Análise de custo-efetividade do uso de gefitinibe versus protocolos de quimioterapia no tratamento de primeira linha do câncer de pulmão não-pequenas células metastático, EGFR positivo. J Bras Econ Saúde (2011) 3:269–77.
46. Cerci JJ, Takagaki TY, Trindade E, Morgado R, Morabito F, Musolino RS, et al. A tomografia por emissão de pósitrons com 2-[18F]-fluoro-2-desoxi-D-glicose é custo-efetiva em pacientes com câncer de pulmão não pequenas células no Brasil. Radiol Bras. (2012) 45:198–204. doi: 10.1590/S0100-39842012000400004
47. Stefani SD, Saggia MG, Santos EAV. Cost-minimisation analysis of erlotinib in the second-line treatment of non-small-cell lung cancer: a Brazilian perspective. J Med Econ. (2008) 11:383–96. doi: 10.3111/13696990802208186
48. Younes RN, Gross JL, Deheinzelin D. Follow-up in lung cancer how often and for what purpose? Chest (1999) 115:1494–99. doi: 10.1378/chest.115.6.1494
49. Carvalho AC, Sasse EC, Sasse A. Estudo de custo-efetividade de FOLFOX seguido de FOLFIRI versus 5-FU / LV seguido de irinotecano em pacientes com câncer colorretal metastático no Sistema Único de Saúde do Brasil. J Bras Econ Saúde (2012) 4:413–19.
50. Moraes RS, Sobottka WH, Zanchet MV, Lima JHF, Morgenstern GA, Schulz GJ, et al. Custo comparado da microcirurgia endoscópica transanal (TEM) com a retossigmoidectomia anterior e com a cirurgia de amputaçao abdômino-perineal do reto. ABCD. Arq Bras Cir Dig. (2007) 20: 150–3. doi: 10.1590/S0102-67202007000300006
51. Torres US, Almeida TEP, Netinho J. Increasing hospital admission rates and economic burden for colorectal cancer in Brazil, 1996–2008. Rev Panam Salud Publica. (2010) 28:244–8. doi: 10.1590/S1020-49892010001000002
52. Caponero R, Ribeiro RDA, Santos E, Cirrincione A, Saggia M. Medical resource use and cost of different first-line treatments for metastatic colorectal cancer in Brazil. J Med Econ. (2008) 11:311–25. doi: 10.3111/13696990802160817
53. da Silveira E, Artifon E. Cost-effectiveness of palliation of unresectable esophageal cancer. Dig Dis Sci. (2008) 53:3103–11. doi: 10.1007/s10620-008-0302-2
54. Hourneaux G, Moura E, Sakai P, Cecconello I, Ishioka S. Tratamiento paliativo del cáncer avanzado de esófago. Estudio comparativo: prótesis metálica autoexpansible y tubo gástrico isoperistáltico. Acta Gastroent Latinoamer. (2001) 31:13–22.
55. Moellmann-coelho A, Asano EF, Nita ME, Junior JWRB, Messias ERR, Donato B. Budget impact analysis of chronic myeloid leukemia treatment in patients with imatinib failure from the Brazilian public health system perspective: supporting health care decisions on central and local levels. Rev Bras Cancerol. (2010) 56:471–81.
56. Costa VC, Ferraz MB, Petrilli S, Pereira C, Rogerio JW. Resource utilization and cost of episodes of febrile neutropenia in children with acute leukemias and lymphomas. SupportCare Cancer (2003) 11:356–61. doi: 10.1007/s00520-002-0429-1
57. Cunio Machado Fonseca M, Tannus Branco de Araújo G, Etto H, Schiola A, Santoni N, Machado M. Economic evaluation of clodronate and zoledronate in patients diagnosed with metastatic bone disease from the perspective of public and third party payors in Brazil. Clin Ther. (2011) 33:1769–80. doi: 10.1016/j.clinthera.2011.09.025
58. Pinto M, Ugá MAD. Cost of treating patients with smoking history in a specialized cancer hospital. Rev Saúde Pública. (2011) 45:1–7. doi: 10.1590/S0034-89102011005000026
59. Lopes LC, Barberato-Filho S, Costa AC, Osorio-de-Castro C. Uso racional de medicamentos antineoplásicos e ações judiciais no Estado de São Paulo. Rev Saúde Pública. (2010) 44:620–28. doi: 10.1590/S0034-89102010000400005
60. Peppe C, Veich V, Asano EF, Pereira M. Avaliação econômica do acetato de abiraterona para o tratamento de pacientes com câncer de próstata metastático resistente à castração previamente tratados com docetaxel no sistema privado de saúde do Brasil. J Bras Econ Saúde (2012) 4:444–53.
61. Paula AAPDE, Piccelli HRS, Pinto NP, Teles AG, Franqueiro AG, Maltez ARL, et al. Economic impact orchiectomy for advanced prostate cancer. J Brazilian Soc Urol. (2003) 29:127–32. doi: 10.1590/S1677-55382003000200006
62. Suaid HJ, Gonçalves MA, Jr AAR, João P, Cologna AJ, Martins ACP. Estimated costs of treatment of cenign prostate hyperplasia in Brazil. J Brazilian Soc Urol. (2003) 29:234–37. doi: 10.1590/S1677-55382003000300007
63. Teich V, Hashizume CM, Cunha TMB, Charbonneau C, Naves A. Análise econômica do sunitinibe versus alfa-interferona e bevacizumabe associado à alfa-interferona no tratamento do carcinoma de células renais metastático (RCCm) sob a perspectiva do sistema suplementar de saúde Brasileiro. J Bras Econ Saúde (2011) 3:166–73.
64. Vanni T, Fonseca BAL, Polanczyk CA. Cost-effectiveness analysis comparing chemotherapy regimens in the treatment of AIDS-related Kaposi's sarcoma in Brazil. HIV Clin Trials (2006) 7:194–202. doi: 10.1310/hct0704-194
65. Souza R, Rezende ML, Adriana Prest M, Corrêa MP. Estimativa do custo do tratamento de câncer de pele tipo melanoma no Estado de São Paulo-Brasil. An Bras Dermatol. (2009) 84:237–43. doi: 10.1590/S0365-05962009000300004
66. Souza RJSP, Corrêa MP, Ferreira ACA, Mattedi AP, Rezende M. Estimativa do custo do tratamento do câncer de pele tipo não-melanoma no Estado de São Paulo-Brasil. An Bras Dermatol. (2011) 86:657–62. doi: 10.1590/S0365-05962011000400005
67. Maciel SSS, Maciel WV, Silva RB, Sobral LV, Souza IRS, Siqueira M. Morbidade por câncer da boca e faringe em capitais brasileiras. Rev da AMRIGS (2012) 56:38–45.
68. Brentani A, de Castro GJ, Federico MH. Cost-effectiveness analysis of cisplatin-based chemoradiation to treat patients with unresectable, nonmetastatic head and neck cancer in Brazil. Head Neck (2011) 33:1199–205. doi: 10.1002/hed.21601
69. Ara R, Basarir H, Keetharuth AD, Barbieri M. Are policy decisions on surgical procedures informed by robust economic evidence? A systematic review. Int J TechnolAssess Health Care (2014) 4:1–13. doi: 10.1017/S0266462314000531
70. Barbieri M, Weatherly HL, Ara R, Basarir H, Sculpher M, Adams R, et al. What is the quality of economic evaluations of non-drug therapies? A systematic review and critical appraisal of economic evaluations of radiotherapy for cancer. Appl Health Econ Health Policy (2014) 12:497–510. doi: 10.1007/s40258-014-0115-8
71. Jönsson B. Technology assessment for new oncology drugs. Clin Cancer Res. (2013) 19:6–11. doi: 10.1158/1078-0432.CCR-12-1819
72. odriguez JM, Paz S, Lizan L, Gonzalez P. The use of quality-adjusted life-years in the economic evaluation of health technologies in Spain: a review of the 1990-2009 literature. Value Health (2011) 14:458–64. doi: 10.1016/j.jval.2010.10.039
73. Sanz-Granda Á, Hidalgo Á, Del Llano JE, Rovira J. Analysis of economic evaluations of pharmacological cancer treatments in Spain between 1990 and 2010. Clin Transl Oncol. (2013) 15:9–19. doi: 10.1007/s12094-012-0934-8
74. Schickedanz A. Of value: a discussion of cost, communication, and evidence to improve cancer care. Oncologist (2010) 15(Suppl. 1):73–9. doi: 10.1634/theoncologist.2010-S1-73
75. Bergstrom R. Drivers of the cost of cancer care. Lancet Oncol (2012) 13:14–5. doi: 10.1016/S1470-2045(11)70370-9
76. Bertram MY, Lauer JA, De Joncheere K, Edejer T, Hutubessy R, Kieny MP, et al. Cost-effectiveness thresholds: pros and cons. Bull World Health Organ. (2016) 94:925–30. doi: 10.2471/BLT.15.164418
77. Woods B, Revill P, Sculpher M, Claxton K. Country-level cost-effectiveness thresholds: initial estimates and the need for further research. Value Health (2016) 19:929–35. doi: 10.1016/j.jval.2016.02.017
78. Bae YH, Mullins CD. Do value thresholds for oncology drugs differ from nononcology drugs? J Manag Care Spec Pharm. (2014) 20:1086–92. doi: 10.18553/jmcp.2014.20.11.1086
Keywords: costs and cost analysis, cost-benefit analysis, health care costs, neoplasms, Brazil
Citation: Campolina AG, Yuba TY, Decimoni TC, Leandro R, Diz MdPE, Novaes HMD and de Soárez PC (2018) Health Economic Evaluations of Cancer in Brazil: A Systematic Review. Front. Public Health 6:205. doi: 10.3389/fpubh.2018.00205
Received: 02 April 2018; Accepted: 04 July 2018;
Published: 27 July 2018.
Edited by:
Mihajlo Jakovljevic, Faculty of Medical Sciences, University of Kragujevac, SerbiaReviewed by:
Zoltán Vokó, Eötvös Loránd University, HungaryMary Codd, University College Dublin, Ireland
Julie Abimanyi-Ochom, Deakin University, Australia
Copyright © 2018 Campolina, Yuba, Decimoni, Leandro, Diz, Novaes and de Soárez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patrícia C. de Soárez, cGF0cmljaWEuc29hcmV6QHVzcC5icg==