 Rodrigo Ramalho1*
Rodrigo Ramalho1* Frances Adiukwu2
Frances Adiukwu2 Drita Gashi Bytyçi3
Drita Gashi Bytyçi3 Samer El Hayek4
Samer El Hayek4 Jairo M. Gonzalez-Diaz5
Jairo M. Gonzalez-Diaz5 Amine Larnaout6
Amine Larnaout6 Paolo Grandinetti7
Paolo Grandinetti7 Marwa Nofal8
Marwa Nofal8 Victor Pereira-Sanchez9
Victor Pereira-Sanchez9 Mariana Pinto da Costa10,11,12
Mariana Pinto da Costa10,11,12 Ramdas Ransing13
Ramdas Ransing13 Andre Luiz Schuh Teixeira14
Andre Luiz Schuh Teixeira14 Mohammadreza Shalbafan15
Mohammadreza Shalbafan15 Joan Soler-Vidal16
Joan Soler-Vidal16 Zulvia Syarif17
Zulvia Syarif17 Laura Orsolini18
Laura Orsolini18- 1Department of Social and Community Health, School of Population Health, University of Auckland, Auckland, New Zealand
- 2Department of Neuropsychiatry, University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
- 3Mental Health Center Prizren, Hospital and University Clinical Service of Kosovo, Prizren, Kosovo
- 4Department of Psychiatry, American University of Beirut, Beirut, Lebanon
- 5CERSAME, School of Medicine and Health Sciences, Universidad del Rosario—Clínica Nuestra Señora de la Paz, Bogotá, Colombia
- 6Razi Hospital, Faculty of Medicine of Tunis, Tunis El Manar University, Tunis, Tunisia
- 7Addictions Services (SerD), Department of Territorial Assistance, ASL Teramo, Teramo, Italy
- 8Helwan Mental Health Hospital, Cairo, Egypt
- 9Department of Child and Adolescent Psychiatry, NYU Grossman School of Medicine, New York, NY, United States
- 10Unit for Social and Community Psychiatry, WHO Collaborating Centre for Mental Health Services Development, Queen Mary University of London, London, United Kingdom
- 11Institute of Biomedical Sciences Abel Salazar, University of Porto, Porto, Portugal
- 12Hospital de Magalhães Lemos, Porto, Portugal
- 13Department of Psychiatry, BKL Walalwalkar Rural Medical College, Maharashtra, India
- 14Department of Childhood and Adolescent Psychiatry, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
- 15Mental Health Research Center, Iran University of Medical Sciences, Tehran, Iran
- 16Fidmag Research Foundation, Hermanas Hospitalarias, Barcelona, Spain
- 17Department of Psychiatry, Tarakan General Hospital, Jakarta, Indonesia
- 18Unit of Clinical Psychiatry, Department of Clinical Neurosciences/DIMSC, School of Medicine, Polytechnic University of Marche, Ancona, Italy
Background: The rapid spread of the Coronavirus disease 2019 (COVID-19) has forced most countries to take drastic public health measures, including the closure of most mental health outpatient services and some inpatient units. This has suddenly created the need to adapt and expand telepsychiatry care across the world. However, not all health care services might be ready to cope with this public health demand. The present study was set to create a practical and clinically useful protocol for telemental health care to be applied in the context of the current COVID-19 pandemic.
Methods: A panel of psychiatrists from 15 different countries [covering all World Health Organization (WHO) regions] was convened. The panel used a combination of reactive Delphi technique and consensus development conference strategies to develop a protocol for the provision of telemental health care during the COVID-19 pandemic.
Results: The proposed protocol describes a semi-structured initial assessment and a series of potential interventions matching mild, moderate, or high-intensity needs of target populations.
Conclusions: Telemedicine has become a pivotal tool in the task of ensuring the continuous provision of mental health care for the population, and the outlined protocol can assist with this task. The strength of this protocol lies in its practicality, clinical usefulness, and wide transferability, resulting from the diversity of the consensus group that developed it. Developed by psychiatrists from around the globe, the proposed protocol may prove helpful for many clinical and cultural contexts, assisting mental health care providers worldwide.
Introduction
The Coronavirus disease 2019 (COVID-19) pandemic has placed the world in an exceptional situation, forcing communities and governments to make fast decisions. The World Health Organization (WHO) has highlighted the importance of measures aimed at delaying the spread of the virus (1). Among these measures, there are non-pharmaceutical interventions, a critical part of current public health measures addressing the pandemic (2–4). These interventions aim at protecting people by physically distancing those with confirmed and suspected COVID-19 or potentially carrying the virus from the general population (2). Such interventions include physical distancing, quarantining, mandatory or voluntary isolation, closing national borders and other travel-related restrictions, closing schools and workplaces, and canceling social gathering events (2).
The rapid spread of the disease, along with the public health measures taken to reduce its progression, present a challenge to mental health services around the world, both in terms of a potential higher demand and difficulties in providing onsite services (5). In this scenario, telemedicine services provide a vital asset for mental health care (6). Telemedicine is defined as the use of telecommunication technologies to provide remote health care (7). The COVID-19 pandemic has created the need to expand telepsychiatry care; in fact, telepsychiatry use among mental health professionals has increased worldwide (8, 9). Unfortunately, these services are limited in various countries, and not all health care services around the globe might be ready to cope with this public health demand (10). Also, mental health care professionals and service providers may have feelings of apprehension or ill-preparedness when facing the sudden need to set up telepsychiatry services and/or to provide mental health care primarily via this approach (10). At the same time, not all services count with local guidelines for telepsychiatry (11), and available guidelines may not be transferable to different social and cultural contexts. Moreover, not all available guidelines may have contemplated the particular circumstances imposed by the current COVID-19 pandemic. The present project was set to assist with this situation, with the goal of creating a practical and clinically useful protocol for mental health care that would cater to most clinical and cultural contexts, assisting mental health care providers around the world.
Methods
The project sought to take advantage of the knowledge and experience of psychiatrists from a wide range of countries, connected by the Early Career Psychiatrists Section of the World Psychiatric Association (12). A panel of 16 psychiatrists from 15 different countries covering all WHO regions was convened. The study used a combination of a modified Delphi technique, called reactive Delphi, and strategies drawn from the consensus development conference method (13–15) (Tables 1, 2).
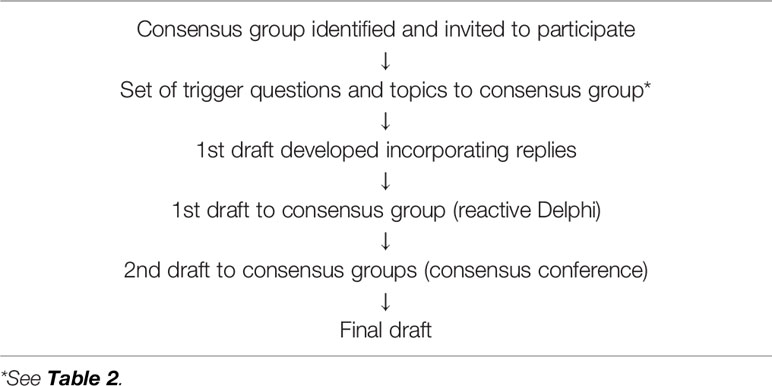
Table 1 Protocol development pathway.
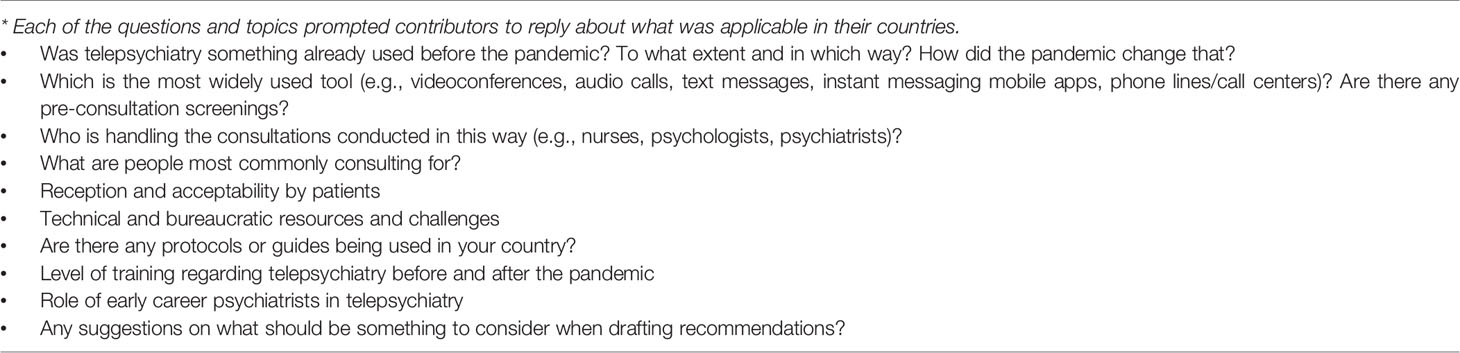
Table 2 Trigger questions and topics.
All participants were provided with a set of trigger questions and topics via the social network messaging application WhatsApp® and prompted to reply about what was applicable in their countries (Table 2). All answers were collected by the lead (RRam) and co-lead (LO) authors and entered into an Excel spreadsheet. Informed by these answers, RR developed a first draft of the protocol with the support of LO and then shared it with all participants as a Google® document, who were asked to provide feedback using a reactive Delphi Technique (14, 15). All feedback was incorporated into a second draft and then shared and discussed with all participants using the Zoom® platform and strategies drawn from the consensus development conference method (13). The final draft was unanimously accepted by all participants (Table 1). Group discussions were accompanied with a review of the emerging scientific literature about COVID-19 and its impact on mental health, as available in online journals and databases. Also, the answers provided to the trigger questions and topics informed the development of other manuscripts published (11) and to be published in the near future.
This study did not involve the management of sensitive data; all of the authors participated voluntarily, and their contributions reflect their own views and not necessarily those from their institutions. Due to the nature of this study, prior assessment by an Institutional Review Board was not necessary.
Results
The consensus group was composed of 16 participants representing countries from all WHO regions: African Region, Region of the Americas, South-East Asia Region, European Region, Eastern Mediterranean Region, and the Western Pacific Region. These were representatives from lower middle income (Egypt, India, Indonesia, Nigeria, and Tunisia), upper middle income (Brazil, Colombia, Iran, Kosovo, and Lebanon), and high income countries (Italy, New Zealand, Portugal, Spain, and United States of America).
Delivery Platform
There are some contexts where video conferencing is available for specialists and the population. However, while it would be ideal for everybody to have access to the tools and the necessary digital literacy to liaise with mental health providers online, this is not always the case. An actual means available for the wider population and mental health care providers in most contexts involve phone calls (landline or mobile), primarily via telephone hotlines. The following protocol was created with this limitation in mind. Still, whenever possible, video conferencing should also be made available to the public.
Resources Required
We recommend mental health departments to provide an entry point to mental health care via telephone hotlines or helplines. But before making this service widely available, these departments should first organize the necessary resources, including human resources. This organization should include securing the contact information of, and/or an open line of communication with, available hospitals, ambulance services, and any other potentially necessary resource (e.g., hotlines for people experiencing intimate partner violence). Depending on availability, this organization should also include securing up-to-date information about COVID-19, public health measures, essential services, and any financial assistance available to the population in times of quarantine. It should also include setting up a filing system for records, if these were to be used.
The service would require, ideally, a coordination team, a technical support team, and mental health care providers (from here on referred to as providers). The coordination team should be responsible for ensuring resources, both material and human resources, including technical support. In case that not all members of the providers team were mental health specialists, the protocol we are presenting offers a guide for when to refer the call to these specialists. All providers should possess the appropriate and necessary competencies in terms of mental health care. In regard to the provision of telemental health care, it might be necessary to organize brief training at the service, either through professional associations, by inviting national or international consultants, or even through active learning under a self-training scheme. There may be contexts where it would be the same providers who are in charge of coordinating the service. Still, it is advisable for them to organize first the necessary resources, according to the service capabilities.
Care Provision
Providers should be aware that telepsychiatry carries some additional challenges in regard to establishing rapport. This is due to the loss of nonverbal cues during the interaction, the lack of physical closeness, and, in cases where it is conducted via video conferencing, the artificiality of eye contact through a screen (16). Providers should demonstrate a high tone of professionalism in their verbal communication, maintaining an attitude of active, empathic, and non-judgmental listening. They should act as if they were, in fact, face-to-face with the caller, being mindful of their background and self-presentation, and trying to avoid multitasking and getting distracted during the conversation.
When contacted for the first time, providers should conduct an immediate assessment and intervention, tailored to each person’s needs to the best of the provider’s capabilities. Table 3 shows a suggested guideline for conducting this initial assessment. After greeting the caller and introducing themselves, providers would set the frame of the consultation, assuring callers about its confidentiality, and obtain their informed consent. Providers will then ask for a name and contact information, the latter due to the possibility of having the call dropped out in the middle of a conversation; however, providers should be open to the possibility of callers not willing to share that information through telecommunication means. The initial assessment will then move to explore four areas: the caller’s current living conditions, the presence and quality of any psychological distress, COVID-19 diagnosis and misinformation about it, and the caller’s medical history. This assessment could also include the administration of screening scales, such as the Patient Health Questionnaire 9-item Depression scale (PHQ-9) and the 7-item Generalized Anxiety Disorder scale (GAD-7), two validated and widely used depression and anxiety measures (17, 18).
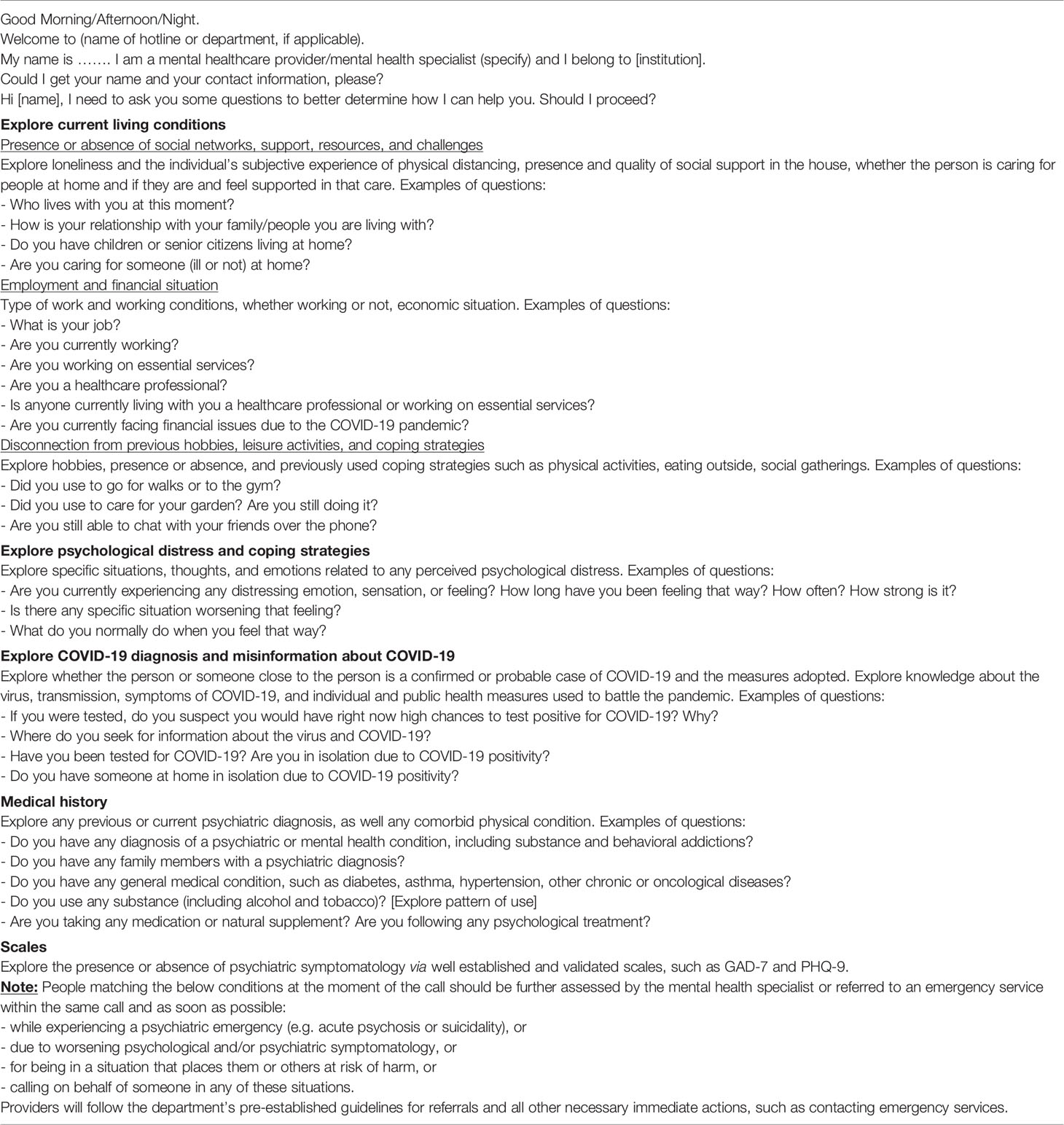
Table 3 Semi-structured outline of an initial assessment.
As an outcome of this initial assessment, callers will then be matched to one of three potential lines of intervention (Table 4). Most people contacting the department will likely match either the first or the second-line interventions (Table 5). First-line interventions aim to provide trustworthy and appropriate information, reduce the distress associated with the pandemic and manage its emotional impact, and assist in the process of complying with public health measures of physical distancing. Providers who are not mental health specialists should be able to provide first-line interventions. Second-line interventions aim at providing the necessary support to people who are facing situations of particular distress or may be more susceptible to the mental health impact of the pandemic. Second-line interventions will require contact with a mental health specialist, whether during the same call or by referral to a scheduled one. Close monitoring via follow up calls and further communication should be scheduled with this population. People experiencing a psychiatric emergency or a situation that places them or others at risk of harm require third-line interventions, which include immediate contact with a mental health specialist or an emergency service.
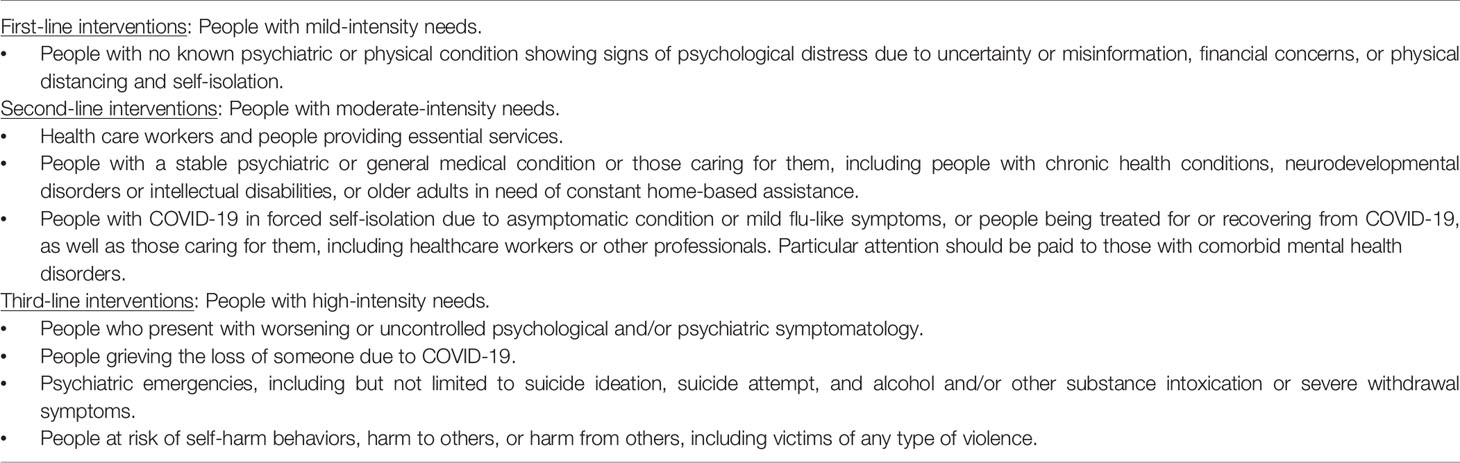
Table 4 Target population and matching interventions.
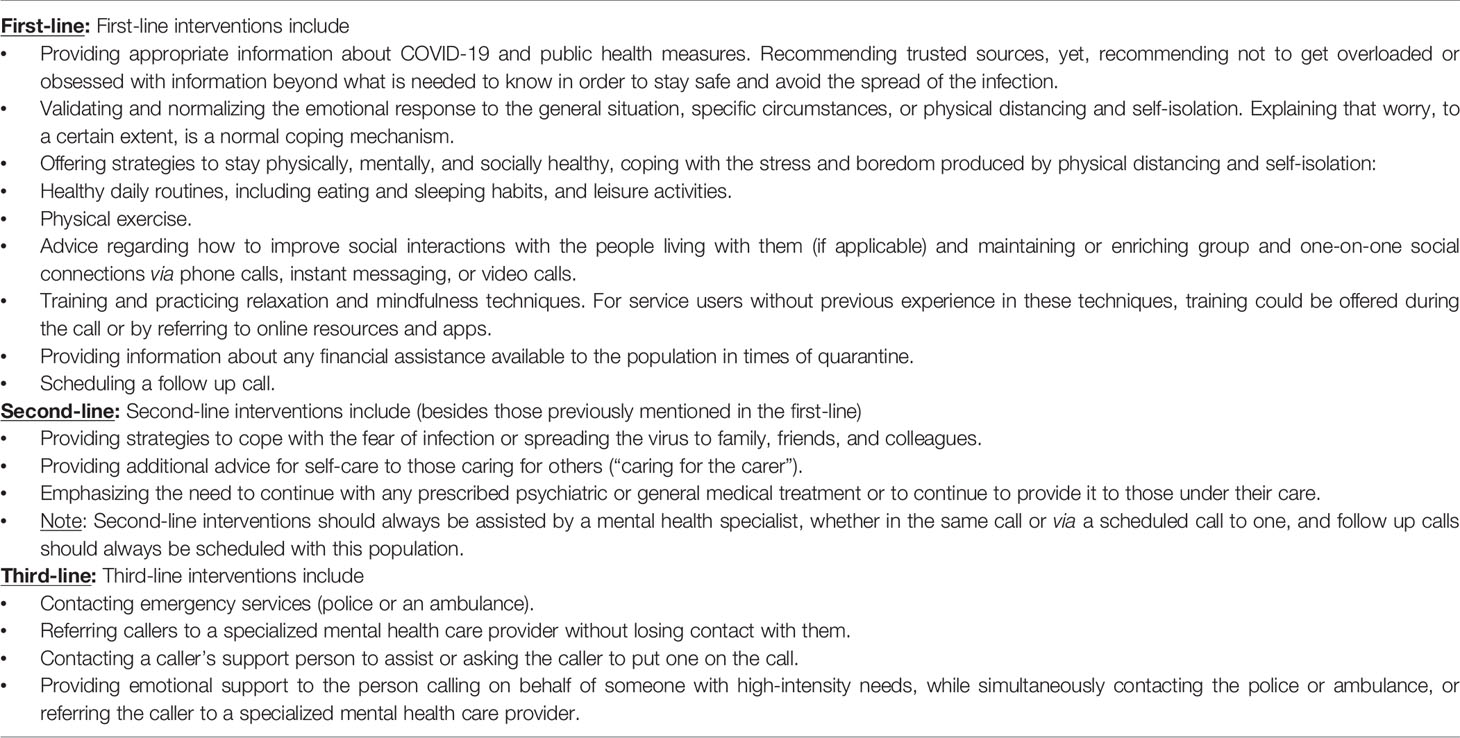
Table 5 First, second, and third-line interventions.
All interventions should follow the criteria of appropriateness and evidence-based efficacy. It is highly recommended for providers to review and follow, according to the provider’s and service capabilities, the best practice guidelines provided by either local or international entities, e.g., those published by the American Psychiatric Association and the American Telemedicine Association (19), and other researchers (20). Finally, as much as with face-to-face consultations, cultural responsiveness is an essential component of telepsychiatry. All providers should be sensitive to the caller’s cultural identity and cultural conceptualisation of distress, as well as the impact of cultural features on the caller-provider relationship (DSM-5) (21). There is one extra component that needs to be taken into account, that is, the influence of the service user’s cultural background on the use of the provided service (22, 23). Providers should assess callers and communities’ acceptability of this service, adapt and respond to this assessment, and continuously monitor changes.
Discussion
The rapid progression of COVID-19 and the non-pharmacological interventions adopted to reduce the spread of the virus have led to increasing difficulties in the provision of mental health care. As a result, telemedicine has become a pivotal tool in the task of ensuring the continuous provision of mental health care for the population. It is extremely important for mental health services around the globe to prepare and take action (24); the protocol here outlined can assist them with both.
The strength of this protocol lies in its practicality, clinical usefulness, and wide transferability, resulting from the diversity of the consensus group that developed it. Country representatives from a wide range of social, cultural, and economic contexts contributed to the development of this protocol. As such, it represents a valuable tool with a likely wide transferability across different regions and contexts. Nevertheless, it should be acknowledged that there is a potentially high degree of resource allocation needed to apply these recommendations, which may indeed limit its transferability to some contexts. Therefore, further studies are recommended to ensure a match between the here proposed protocol and country/context-specific conditions or to guide all necessary adjustments before it is implemented locally. Moreover, both these studies and/or the implementation of the present protocol in any mental health service should abide by specific local health regulations and the institutions’ ethics committees.
Still, the proposed protocol could help mental health providers to identify and address the mental health impact of physical distancing and misinformation during the COVID-19 pandemic, two key issues highlighted in the literature (25). Furthermore, mental health departments should also acknowledge the impact of physical distancing and provide adequate mental health support (26). This support may prove a valuable resource in assisting people to comply with prescribed physical distancing measures, and thus with the battle against the pandemic (27, 28). The WHO has called people to resort only to official sources when seeking information about COVID-19 (29). Mental health departments should support this call and combat misinformation, but they should also provide people with strategies to avoid a hyperconsumption of information (30, 31). These are all points addressed in the recommended protocol and should be acknowledged when developing local adaptations.
The literature also suggests that it may prove beneficial to develop targeted telepsychiatry interventions for different populations during the pandemic (32). Particular attention should be paid to older adults, children, and those caring for them (33–35). Similarly, healthcare professionals require special consideration (30, 36, 37). The proposed protocol would allow mental health departments to identify and support these and other particularly vulnerable populations, such as those with a pre-existing or emerging mental health disorder (5, 38) and those in situations of domestic or intrafamilial violence, which may dramatically increase during the quarantine (39). It is highly recommended for local adaptions of this protocol also to identify and cater for different populations within each specific context in case these were not contemplated in the present protocol.
As suggested by other authors (6, 26, 40), telemedicine services should be formally provided as a crucial component of the public health response to the ongoing COVID-19 pandemic. The adoption and expansion of telepsychiatry in mental health care would simultaneously improve access to this care and decongest those mental health care services already working at capacity. The proposed protocol can support mental health departments to provide care in non-urgent situations that do not necessarily require a face-to-face interaction, minimizing the risk of contagion between members of the population and the health care workforce. It can also help with redirecting and maximizing the use of available resources, including specialized mental health care professionals. But further research is needed on its use and applicability to local healthcare systems, services, and resources during the pandemic.
The mental health impact of the COVID-19 pandemic has forced mental health services around the world to adapt. The adoption of this protocol can complement existing guidelines during the pandemic in those contexts where telepsychiatry was well established already, but most importantly, it can also provide a starting point to those where telepsychiatry has played a marginal role until now. These are particularly difficult moments in time. However, they also offer the opportunity to advance the way in which mental health services worldwide support the population, and this protocol also highlights the importance of acknowledging and harvesting the knowledge and expertise of early career psychiatrists around the globe in that task.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Author Contributions
RRam developed the trigger questions and topics and wrote the first draft of recommendations and article with the support from LO. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organisation. Operational considerations for case management of COVID-19 in health facility and community. Interim guidance (2020). Available at: https://apps.who.int/iris/bitstream/handle/10665/331492/WHO-2019-nCoV-HCF_operations-2020.1-eng.pdf (Accessed 16 April 2020).
2. European Centre for Disease Prevention and Control. Guidelines for the use of non-pharmaceutical measures to delay and mitigate the impact of 2019-nCoV. Stockholm: ECDC Press (2020).
3. Markel H, Lipman HB, Navarro JA, Sloan A, Michalsen JR, Stern AM, et al. Nonpharmaceutical interventions implemented by US cities during the 1918–1919 influenza pandemic. JAMA (2007) 298:644–54. doi: 10.1001/jama.298.6.644
4. Morse SS. Pandemic influenza: studying the lessons of history. Proc Natl Acad Sci USA (2007) 104(18):7313–4. doi: 10.1073/pnas.0702659104
5. Li W, Yang Y, Liu ZH, Zhao YJ, Zhang Q, Zhang L, et al. Progression of mental health services during the COVID-19 outbreak in China. Int J Biol Sci (2020) 16(10):1732–8. doi: 10.7150/ijbs.45120
6. Chauhan V, Galwankar S, Arquilla B, Garg M, Di Somma S, El-Menyar A, et al. Novel coronavirus (COVID-19): Leveraging telemedicine to optimize care while minimizing exposures and viral transmission. J Emerg Trauma Shock 2020 (2020) 13(1):20–4. doi: 10.4103/JETS.JETS_32_20
7. Perednia DA, Allen A. Telemedicine technology and clinical applications. JAMA (1995) 273(6):483–8. doi: 10.1001/jama.273.6.483
8. Corruble E. A viewpoint from Paris on the COVID-19 pandemic: a necessary turn to telepsychiatry. J Clin Psychiatry (2020) 8(3):20com13361. doi: 10.4088/JCP.20com13361
9. Zhou X, Snoswell CL, Harding LE, Bambling M, Edirippulige S, Bai X, et al. The role of telehealth in reducing the mental health burden from COVID-19. Telemed J E Health (2020) 26(4):377–9. doi: 10.1089/tmj.2020.0068
10. Pereira-Sanchez V, Adiukwu F, El Hayek S, Gashi Bytyçi D, Gonzalez-Diaz JM, Kudva Kundadak G, et al. Early career psychiatrists’ perspectives on the mental health impact and care of the COVID-19 pandemic across the world. Lancet Psychiatry (2020) 7(6):E29–30. doi: 10.1016/S2215-0366(20)30153-X
11. Ramalho R, Adiukwu F, Gashi Bytyçi D, El Hayek S, Gonzalez-Diaz JM, Larnaout A, et al. Telepsychiatry and healthcare access inequities during the COVID-19 pandemic. Asian J Psychiatr (2020) 53:102234. doi: 10.1016/j.ajp.2020.102234
12. Pinto da Costa M. Early career psychiatrists–history, 2020 and beyond. World Psychiatry (2020) 19(1):127–8. doi: 10.1002/wps.20712
13. Halcomb E, Davidson P, Hardaker L. Using the consensus development conference method in healthcare research. Nurse Res 2008; (2008) 16(1):56–71. doi: 10.7748/nr2008.10.16.1.56.c6753
14. Delbecq AL, van de Ven AH, Gustafson DH. Group techniques for program planning. A guide to nominal group and Delphi processes. 1st ed. Illinois: Scott, Forseman & Co. Glenview (1975).
15. McKenna HP. The Delphi technique: a worthwhile research approach for nursing? J Adv Nurs (1994) 19(6):1221–5. doi: 10.1111/j.1365-2648.1994.tb01207.x
16. Cowan KE, McKean AJ, Gentry MT, Hilty DM. Barriers to use of telepsychiatry: clinicians as gatekeepers. Mayo Clin Proc (2019) 94(12):2510–23. doi: 10.1016/j.mayocp.2019.04.018
17. Kroenke K, Spitzer RL, Williams JB. The PHQ-9. Validity of a brief depression severity measure. J Gen Intern Med (2001) 16(9):606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
18. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med (2006) 166(10):1092–7. doi: 10.1001/archinte.166.10.1092
19. American Psychiatric Association. Telepsychiatry practice guidelines (2020). Available at: https://www.psychiatry.org/psychiatrists/practice/telepsychiatry/toolkit/practice-guidelines (Accessed 16 April 2020).
20. Manfrida G, Albertini V, Eisenberg E. Connected: recommendations and techniques in order to employ internet tools for the enhancement of online therapeutic relationships. Experiences from Italy. Contemp Fam Ther (2017) 39(4):314–28. doi: 10.1007/s10591-017-9439-5
21. American Psychiatrist Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, VA: APA Press (2013).
22. Acharibasam JW, Wynn R. The importance of cultural awareness when planning and implementing telepsychiatric services. Rural Remote Health (2018) 18(3):4724. doi: 10.22605/RRH4724
23. Shore JH, Savin DM, Novins D, Manson SM. Cultural aspects of telepsychiatry. J Telemed Telecare (2006) 12(3):116–21. doi: 10.1258/135763306776738602
24. Ransing R, Adiukwu F, Pereira-Sanchez V, Ramalho R, Orsolini L, Schuh Teixera AL, et al. Mental health interventions during the COVID-19 Pandemic: a conceptual framework by early career psychiatrists. AJP (2020) 51:102085. doi: 10.1016/j.ajp.2020.102085
25. Brooks S, Webster R, Smith L, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet (2020) 395(10227):912–20. doi: 10.1016/S0140-6736(20)30460-8
26. Dong L, Bouey J. Public mental health crisis during COVID-19 pandemic, China. Emerg Infect Dis (2020) 26(7):1616–8. doi: 10.3201/eid2607.200407
27. Galea S, Merchant RM, Lurie N. The mental health consequences of COVID-19 and physical distancing: the need for prevention and early intervention. JAMA Intern Med (2020) 180(6):817–8. doi: 10.1001/jamainternmed.2020.1562
28. Venkatesh A, Edirappuli S. Social distancing in COVID-19: what are the mental health implications? BMJ (2020) 369:m1379. doi: 10.1136/bmj.m1379
29. World Health Organization. Mental health and psychosocial considerations during the COVID-19 outbreak (2020). Available at: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf?sfvrsn=6d3578af_8&fbclid=IwAR2pnbOkm351iO6cLEFLAqfWzj36HfczasuLxEx4uy_oAHS4T1z5QYKN7lc (Accessed 16 April 2020).
30. Bao Y, Sun Y, Meng S, Shi J, Lu L. 2019-nCoV epidemic: address mental health care to empower society. Lancet (2020) 395(10224):e37–8. doi: 10.1016/S0140-6736(20)30309-3
31. Gao J, Zheng P, Jia Y, Chen H, Mao Y, Chen S, et al. Mental health problems and social media exposure during COVID-19 outbreak. PloS One (2020) 15(4):e0231924. doi: 10.1371/journal.pone.0231924
32. Jung SJ, Jun JY. Mental health and psychological intervention amid COVID-19 outbreak: perspectives from South Korea. Yonsei Med J (2020) 61(4):271–2. doi: 10.3349/ymj.2020.61.4.271
33. Lima CKT, de Medeiros Carvalho PM, Lima IDAS, de Oliveira Nunes JVA, Saraiva JS, de Souza RI, et al. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res (2020) 287:112915. doi: 10.1016/j.psychres.2020.112915
34. Liu JJ, Bao Y, Huang X, Shi J, Lu L. Mental health considerations for children quarantined because of COVID-19. Lancet Child Adolesc Health (2020) 4(5):347–9. doi: 10.1016/S2352-4642(20)30096-1. pii: S2352-4642(20)30096-1.
35. Yang Y, Li W, Zhang Q, Zhang L, Cheung T, Xiang YT. Mental health services for older adults in China during the COVID-19 outbreak. Lancet Psychiat (2020) 7(4):e19. doi: 10.1016/S2215-0366(20)30079-1
36. Chen Q, Liang M, Li Y, Guo J, Fei D, Wang L, et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiat (2020) 7(4):e15–6. doi: 10.1016/S2215-0366(20)30078-X
37. Xiang YT, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry (2020) 7(3):228–9. doi: 10.1016/S2215-0366(20)30046-8
38. Zhang J, Wu W, Zhao X, Zhang W. Recommended psychological crisis intervention response to the 2019 novel coronavirus pneumonia outbreak in China: a model of West China Hospital. Precis Clin Med (2020) 3(1):3–8. doi: 10.1093/pcmedi/pbaa006
39. Alves PMR, de Oliveira CJB, de Oliveira TRN, Barbosa KB, Marcene HC, de Oliveira SV. COVID-19: isolations, quarantines and domestic violence in rural areas. Sci Med J (2020) 2(1):44–5. doi: 10.28991/SciMedJ-2020-0201-7
Keywords: COVID-19, Coronavirus disease, mental health, protocol, psychiatry, telemedicine, telemental health, telepsychiatry
Citation: Ramalho R, Adiukwu F, Gashi Bytyçi D, El Hayek S, Gonzalez-Diaz JM, Larnaout A, Grandinetti P, Nofal M, Pereira-Sanchez V, Pinto da Costa M, Ransing R, Teixeira ALS, Shalbafan M, Soler-Vidal J, Syarif Z and Orsolini L (2020) Telepsychiatry During the COVID-19 Pandemic: Development of a Protocol for Telemental Health Care. Front. Psychiatry 11:552450. doi: 10.3389/fpsyt.2020.552450
Received: 17 April 2020; Accepted: 31 August 2020;
Published: 23 September 2020.
Edited by:
Darren C. Treadway, Daemen College, Untied StatesReviewed by:
Anke Maatz, University of Zurich, SwitzerlandLucas Borrione, Fundação Faculdade de Medicina, Brazil
Copyright © 2020 Ramalho, Adiukwu, Gashi Bytyçi, El Hayek, Gonzalez-Diaz, Larnaout, Grandinetti, Nofal, Pereira-Sanchez, Pinto da Costa, Ransing, Teixeira, Shalbafan, Soler-Vidal, Syarif and Orsolini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rodrigo Ramalho, r.ramalho@auckland.ac.nz