
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 28 July 2020
Sec. Child and Adolescent Psychiatry
Volume 11 - 2020 | https://doi.org/10.3389/fpsyt.2020.00747
 Elise Riquin1,2,3*
Elise Riquin1,2,3* Philippe Duverger1,3Cindy Cariou1Magalie Barth4
Philippe Duverger1,3Cindy Cariou1Magalie Barth4 Clément Prouteau4
Clément Prouteau4 Patrick Van Bogaert5
Patrick Van Bogaert5 Dominique Bonneau2,4Arnaud Roy3,6
Dominique Bonneau2,4Arnaud Roy3,6Mitochondrial diseases (MDs) are a group of clinically heterogeneous genetic disorders that arise as the result of dysfunctional mitochondria. Only few medical articles deal with neuropsychological or psychiatric aspects of MDs.
Aim: The present article aims to provide a systematic review of neuropsychological and psychiatric aspects of MDs.
Methods: In order to identify all studies dealing with psychiatric and neuropsychological aspects of MDs in children and adolescents, we performed a search in the medical literature between April 2009 and April 2019 using PubMed, Cochrane, and Web of Science and we defined inclusion and exclusion criteria.
Results: We found only seven studies that satisfy the inclusion requirements and criteria. The main psychiatric aspects reported in MDs were depressive and behavioral disorders. With regard to the neuropsychological aspects of MDs, developmental analyses showed an overall deterioration and developmental delay.
Interpretation: Children and adolescents with MDs may present psychiatric symptoms and neuropsychological impairment. A more systematic investigation of psychiatric and neuropsychological features of MDs is needed to foster a better understanding of the phenotype of these diseases and their links with the genotype, which may have significant implications for the developmental trajectories of patients.
Mitochondrial diseases (MDs) are a group of clinically heterogeneous genetic disorders that arise as the result of dysfunctional mitochondria (1). The forms of MDs affecting children (<16 years old) have an estimated prevalence ranging from 5 to 15 cases per 100,000 individuals (1). MDs can be caused either by mutations in the mitochondrial DNA (mtDNA) or in genes from the nuclear genome encoding for mitochondrial proteins (2). Many MDs often involve multiple organ systems and typically affect organs that require the greatest amount of energy (i.e. brain, heart, muscles, kidney) (3–5). The main central nervous system (CNS) symptoms of MDs include epilepsy, hearing loss, visual impairment, intellectual disability, fluctuating encephalopathy, stroke-like episodes, ataxia, and spasticity.
Brain dysfunction in MDs can also result in neuropsychological or psychiatric disturbances including mood or behavior disorders, but few articles deal with this aspect of MDs (6, 7). Cognitive impairment is a common feature in adults presenting with mitochondrial encephalopathy, such as MELAS (mitochondrial encephalopathy lactic acidosis, and stroke-like episodes) (8) and psychiatric symptoms are associated with MDs in up to 70% of the adult population (9, 10). Along the same lines, a recent article suggested that mitochondrial activity could regulate the availability in neurons of GABA, an inhibitory neurotransmitter, leading to social deficits that can be rescued by the modulation of GABA level (11).
In contrast, only few articles have dealt with the neuropsychological and psychiatric features of children and adolescents with MDs (12–15). It is, however, crucial to consider this aspect of MDs in the pediatric population because the disease occurs in developing brains and may have not only a significant impact on developmental trajectories, but also may lead to psychological disturbances affecting quality of life.
This review follows the 2019 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements for performing a systematic review (16). As a first step, studies dealing with neuropsychological and psychiatric features of children and adolescents with MD were identified thanks to a computerized search in PubMed, Cochrane, and Web of Science using the following keywords: (mitochondrial disorder OR mitochondria OR mitochondrial cytopathy OR mitochondrial disease) AND (psychiatry OR psychiatric OR mental illness OR mental disorders OR major depression OR anxiety OR bipolar disorder OR schizophrenia OR psychosis OR neuropsychology OR cognitive OR executive function OR development OR IQ OR memory OR language OR learning abilities) AND (children OR adolescent OR pediatrics).
All articles found were registered using the bibliographic management software EndNote. Duplicates were checked not only digitally, but also manually in order to remove duplicates that could have been missed by the software.
In a second step, the articles previously found were selected using inclusion and exclusion criteria. Inclusion criteria included: 1) articles published in English; 2) articles reporting prospective and retrospective studies; 3) articles reporting longitudinal and cross-sectional studies; 4) articles reporting studies with an experimental group of children and/or adolescents with MD, and 5) articles published between April 2009 and April 2019.
Articles reporting results from adults, literature reviews, and case reports were excluded.
During the review phase of the articles, data was summarized by a primary reviewer (ER) who completed a data abstraction form. Then, a secondary reviewer (CC) checked the accuracy and completeness of the primary review. Finally, two other reviewers independently assessed the eligibility of the study for inclusion and unresolved disagreements between reviewers were adjudicated by a third reviewer (MB). The kappa coefficient, measuring the interrater reliability, was 0.84. Our local research ethics committee did not consider that its approval was needed for this systematic review.
The PRISMA flow diagram of this bibliographic search is shown in Figure 1.
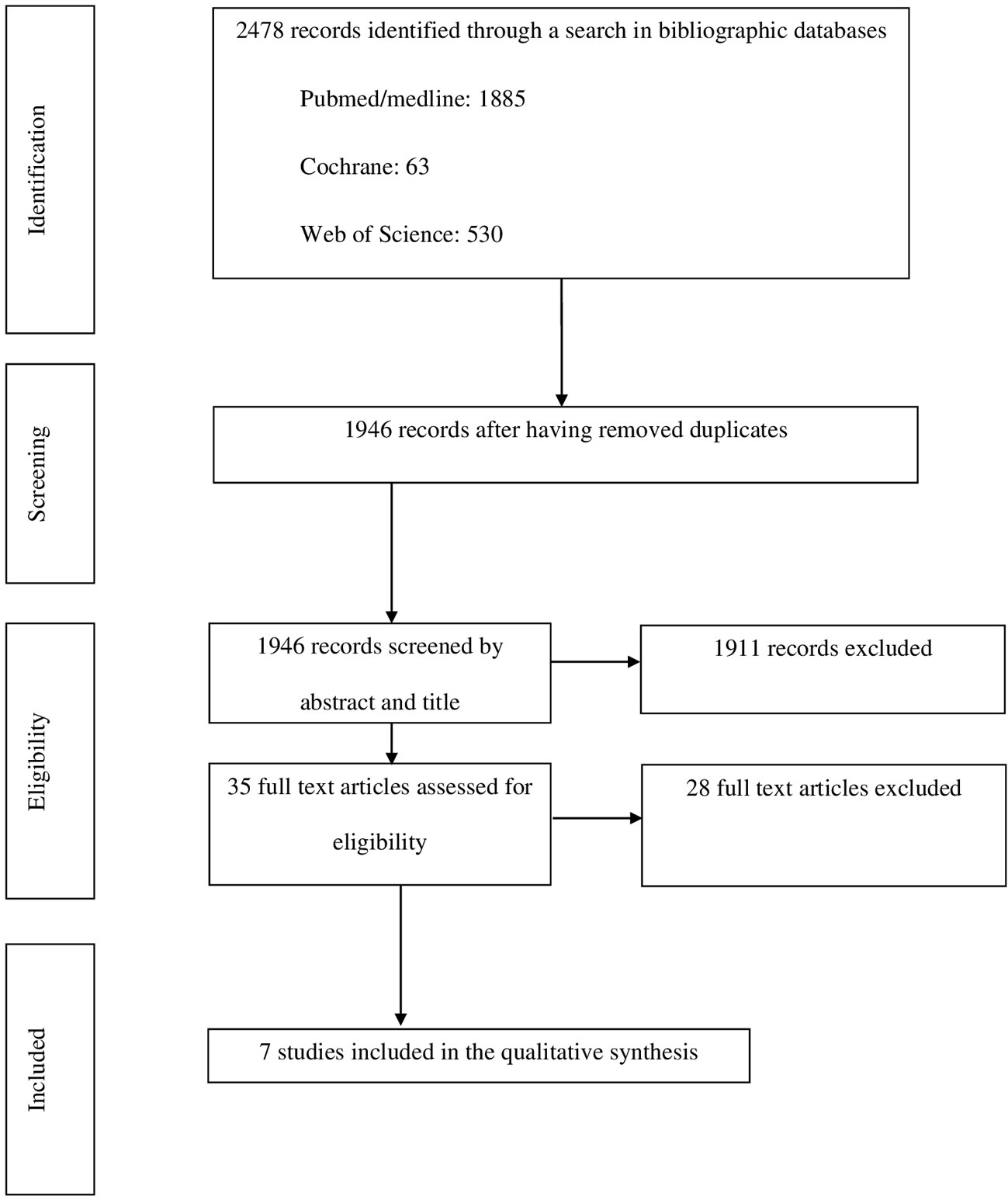
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
A total of 1,946 articles were retrieved during the first step of the review but only seven met the inclusion and exclusion criteria (Table 1). Two of these articles reported retrospective studies (21, 23), four reported prospective studies (17–20), and one reported a longitudinal study (22). The number of children included in these studies ranged from 14 (20) to 112 individuals (18). Two studies were carried out in the Netherlands (17, 19), two in the Republic of Korea (21, 22), two in the USA (20, 23), and one in the UK (18). Quantitative data obtained from psychometric tests were available in only six of these studies (Table 1) (19–23).
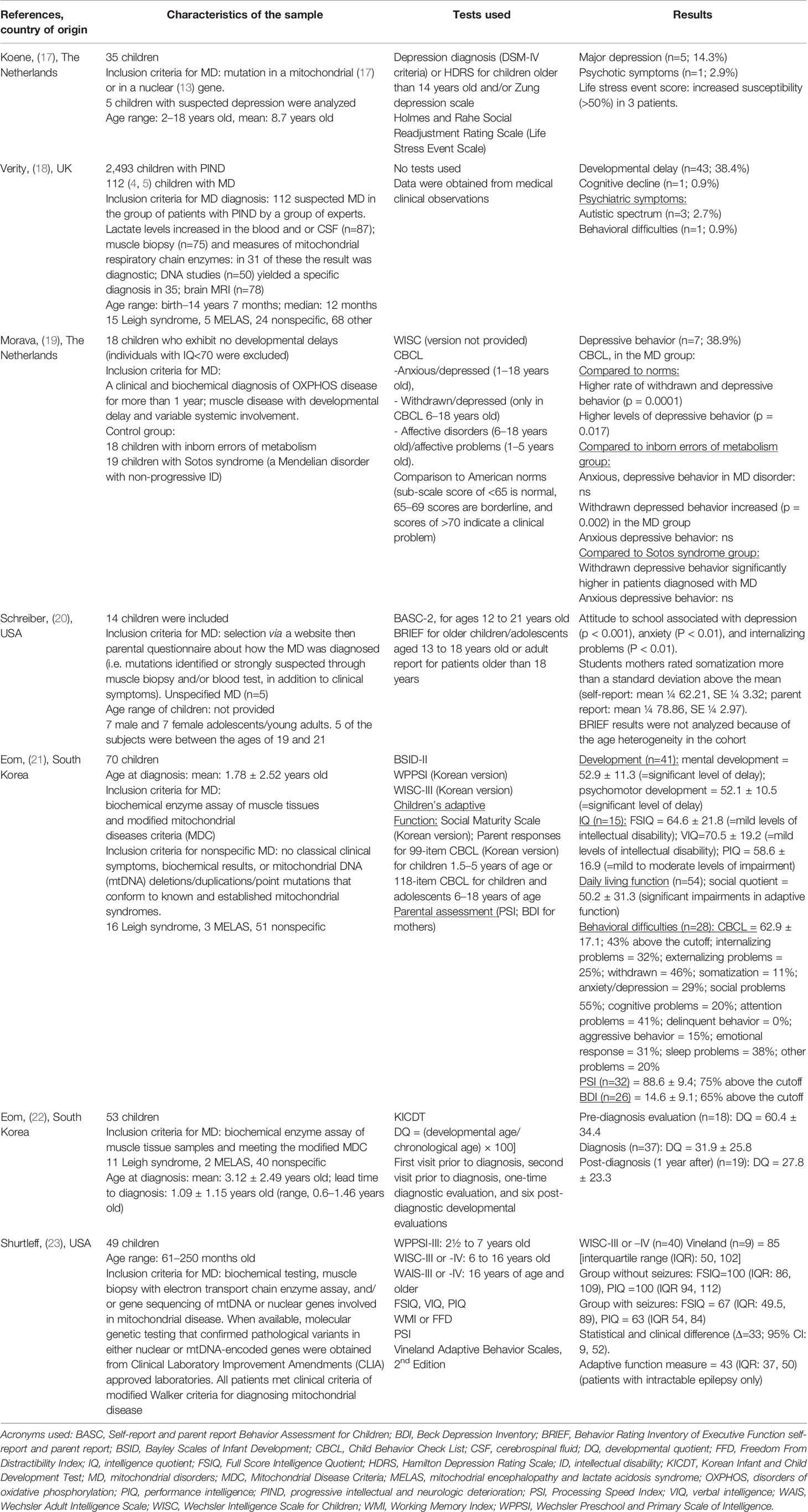
Table 1 Main results of the studies included in the literature review.
Psychiatric disorders were analyzed in four articles, (17–19, 21) but only three of them (17, 19, 21) used rating scales to objectively assess them. The scales used in these studies were the Hamilton Depression Rating Scale (HDRS), the Zung depression scale (17), the Holmes and Rahe Social Readjustment Rating Scale (17), and the child behavior checklist (CBCL) (19, 21). These studies, the main results of which are shown in Table 1, primarily demonstrated the high prevalence of depressive symptoms and behavioral disorders, such as withdrawal, social problems, attention deficit, sleep disorders, and emotional response in children with MDs.
In the study performed by Eom et al. (21), 28 children with behavioral disorders were tested using the CBCL. The most severe features reported in this study were withdrawal, social problems, attention deficit, sleep disorders, and emotional response. In addition, a high level of parental stress was also reported. Similarly, almost 65% of the mothers from this study exhibited significant levels of depression.
Morava et al. (19) evaluated the psychological characteristics of 18 Dutch children with MDs who exhibited no developmental delays. In this study, a significantly high rate of withdrawal and depressive behavior was observed in the MD group in comparison to not only the normal population, but also to children affected with other forms of inborn errors of metabolism and to children with Sotos syndrome.
When comparing both these groups, the authors aimed to check whether factors such as the stress of being diagnosed with such conditions, fatigue, and discomfort were major determinants of the depressive behavior. This study showed a strikingly high incidence of depressive behavior in children with MDs, but the occurrence of depression was not significantly correlated with the degree of mitochondrial dysfunction and the clinical severity of the disease or, more specifically, with muscle involvement or severe CNS involvement. According to the authors, this lack of correlation supported the hypothesis that depressive behavior could be genetically determined, as shown in multiple studies (24), and that abnormal cerebral energy metabolism could be a risk factor for mood disorders.
In another study conducted in the Netherlands, Koene et al. (17) found that 5 children with MD out of 35 (14.3%) demonstrated major depressive behavior.
In a study conducted in the UK, Verity et al. (18) focused on the clinical presentation, the way the diagnosis was made, and the epidemiology of MD in children who exhibited progressive intellectual and neurological deterioration. The methodology was based on the British Pediatric Surveillance Unit (BPSU) card, which asks pediatricians to report children presenting progressive intellectual and neurological deterioration (PIND). The data reported by clinicians were classified and analyzed by an expert group. In this study, 3 children out of 112 had autistic spectrum disorder (2.7%) and 1 had behavioral difficulties (without specificities) (0.9%). In this study, however, no specific scales rating the psychiatric disorders were used.
The neuropsychological profiles of children and adolescents with MDs has been analyzed in five studies (18, 20–23), the main results of which are shown in Table 1. However, only four of these studies used specific scales to evaluate the neuropsychological profiles of affected children.
Regarding intelligence, there was a substantial heterogeneity among juvenile patients with MDs with mild levels of intellectual disability and a Full Scale Intelligence Quotient (FSIQ) ranging from 64.6 to 100 in non-epileptic children (21, 23). By contrast, the cognitive profile appeared to be more affected in individuals with seizures and early onset of the disease (23).
In the study by Eom et al. (21), which included 70 children, several neuropsychological scales were used but not all measures were complete for all patients due to the limited functioning of some individuals. The results for 41 patients showed a significant level of mental and psychomotor developmental delay. Due to limited function, the intellectual quotient (IQ) measurement was performed for only 15 individuals and showed mild levels of intellectual disability and mild to moderate levels of impairment. Regarding overall development, children with MD showed an overall developmental delay and had consistently varying signs of cognitive decline.
Verity et al. (18) found that 43 children with MDs among 112 showed developmental delay (38.4%), one of them having a cognitive decline (0.9%). In this study, however, no specific scales were used and the data was only obtained from clinical observations.
In the study by Eom et al. (22), which included 53 children, the developmental function was evaluated at nine different time points (two points before diagnosis, one at the time of diagnosis, and six during the post-diagnosis phase) using the developmental quotient (DQ) from the Korean infant and child development test (KICDT), which assesses developmental age rather than chronological age. The overall DQ calculated for these 53 children showed a decline from the pre-diagnostic period to the post-diagnostic periods, suggesting an overall deterioration. However, even if declining patterns were consistently present, the characteristics of developmental deterioration were disparate. The authors described five phases: 1) pre-diagnostic initial decline phase; 2) pre-diagnostic accelerated decline phase; 3) post-diagnostic alleviated phase; 4) post-diagnostic reaccelerated decline phase; and 5) post-diagnostic stagnant phase. This study showed that diffuse brain atrophy, the clinical rating provided by the physician, and the age at which the first symptoms significantly affected the developmental level and decline. However, no significant effect was noted according to the type of syndrome and the severity of epilepsy, suggesting that these aspects may not directly reflect the developmental condition of the patients. The authors stressed some limitations in their study such as a preliminary study with a small number of patients, and the overall cohort that was not followed up consistently as they reviewed the data retrospectively.
Schreiber et al. (20) studied 14 children using the Behavior Rating Inventory of Executive Function® (BRIEF®) scale to evaluate their behavior and executive functions. Unfortunately, the results were not significant because the age of participants in the cohort was too heterogeneous.
In this systematic review, we found only three articles dealing with the psychiatric features of children and adolescents affected by MDs and only five articles reporting their neuropsychological outcomes. These studies were conducted in only five countries (Table 1) and their methodologies were heterogeneous. For example, some studies took all the children in the sample into account (19–23) whereas others only analyzed the individuals who had psychiatric and behavior issues or had progressive intellectual and neurologic deterioration (17, 18). In two studies (17, 18), no specific psychometric scales were used and in another (20), data were not collected for all individuals in the sample.
The main psychiatric features affecting children and adolescents with MDs include depressive (14.3 to 38.9%) and behavioral disorders, such as withdrawal, social problems, attention deficit, sleep disorders, and emotional response (0.9 to 43%). This supports the fact that, even in children, mood disorders can be associated with abnormal cerebral energy metabolism (19). Koene et al. (17) stated that depression could affect 14.3% of their study group of patients with MDs in comparison to 3 to 4% of the adolescents from the general population. However, in this study, only on children with a history of depression were evaluated and not all the 35 children of their sample because many children were either too young or too severely affected. The authors therefore argued that the depression rate in children with MDs was probably underestimated (17). The prevalence of depression in MDs is similar to other chronic neurodegenerative disorders, although slightly higher, suggesting that the expression of major depression in these disorders is mostly dependent on the age of onset and clinical severity of the condition and regulated by the coping mechanism of the child and the family (25). Koene et al. (17) proposed the abnormal energy metabolism of the central nervous system as the underlying cause of the mood disorder in pediatric patients. Schreiber et al. (20) added that the etiology of depression and anxiety in young students with MDs is likely complex and may involve the biological and genetic substrates of these diseases. It is also well established that MDs lead to severe disabilities in most pediatric patients, significantly affecting their quality of life (26) and mood. In fact, having a chronic disease is a risk factor of depression (27–29). In the study by Verity et al. (18), the limitation is due to the fact that data were only obtained through clinical observations. The description of psychiatric symptoms is also very vague as “behavioral difficulties.” Moreover, this study was aimed to analyze children with progressive intellectual and neurological deterioration and not to take into account children with stable conditions. In addition, this study relied on information obtained from hospital records and on the diagnosis evaluation by pediatricians for children with developmental delay or autistic spectrum disorders. In the study by Eom et al. (21), the patient sample size was small and the data were collected retrospectively.
Anglin et al. (9) described cases of adults with MDs that was diagnosed many years after the onset of the psychiatric symptoms, which occurred during childhood or adolescence. These observations suggest that psychiatric symptoms could have been considered as early signs of the disease and could have led to an earlier diagnosis, especially if there were linked with other symptoms, such as a cognitive decline (30). The majority of cases in the literature had personal and family histories of multiple medical symptoms, including muscle weakness, hearing loss, fatigue, dysphagia, constipation, type 2 diabetes mellitus, migraines, and stroke-like episodes. From a psychiatric perspective, several patients had atypical aspects to their presentation and did not conform to strict DSM-IV diagnostic categories (9).
Beyond mood disorders, some authors described psychotic symptoms in adult populations (9) and Satogami (31) reported a case of Leigh syndrome who survived past adolescence and presented schizophrenia-like symptoms, including persecutory delusions and auditory hallucinations.
In addition, and in connection with analyses of adult populations, Rosebush (10) suggested that there could be a difference between sexes in the timing of onset of the psychiatric manifestations of inherited MDs, with girls potentially having earlier onset of the psychiatric manifestations.
The treatment of psychiatric illness in patients with MDs can be associated with resistance to treatment and even clinical deterioration. With some reported exceptions (32, 33), many psychotropic agents, including both typical and atypical anti-psychotic agents, selective serotonin reuptake inhibitors (SSRIs), and tricyclic antidepressants, have been found to impair mitochondrial function, generally through inhibition of complex I of the mitochondrial respiratory chain (10, 34). Nevertheless, it is challenging to delineate whether mitochondrial dysfunction occurs secondary to pharmaceutical treatment or whether it is a result of the underlying disease process itself (34). Therefore, intensive research is needed in psychiatric disorders to avoid malfunctioning of the mitochondria (35). In addition, as shown before, a very high proportion of patients is supposed to receive antiepileptic medications and could suffer from the side effects of antiepileptic treatment (decrease of vigilance, attention disorders, speech difficulties…). In this vulnerable population, additional iatrogenic symptoms should be carefully looked for and monitored over time.
Regarding the neuropsychological consequences of MDs in the pediatric population, the evaluation of intellectual abilities is not consensual. Overall, the studies showed that many affected children have psychomotor and mental developmental delays (21) but the results of cognitive function evaluations are heterogeneous (20). The studies analyzed herein have many limitations. In the study by Eom et al. (22), the analyzes were retrospective and included an insufficient number of individuals to draw relevant conclusions. Moreover, this study presented only the pre-diagnostic neuropsychological profiles of the children together with comorbidities in their mothers. In addition, direct measurement of quality of life or long-term follow-up results were not provided.
The studies suggest deterioration of the DQ with a decline from the pre-diagnostic through the post-diagnostic periods (22). When such deterioration occurs, it may be either very quick and sudden, causing death or leading to a vegetative state, or slow and progressive (36). According to Shurtleff et al. (23), an early diagnosis of MD is essential to try to limit the cognitive loss with a more effective control of seizures. However, Shurtleff et al. (23) reported on only intelligence and adaptive functioning without distinction between the different types of MDs.
In the children and adolescents population, the difficulties, and in particular the psychiatric symptoms, must be identified and analyzed in a developmental logic. The disorders presented at a young age will have very different consequences from those presented in adult population, particularly in terms of learning abilities, but also quality of life. The issues of care and diagnosis are therefore particularly not the same as adult population. Future studies on neuropsychological and psychiatric features of MDs in children and adolescents should focus on the cognitive profiles and executive functions for which data are lacking. Executive functions are cognitive processes that assist the child in adapting their behavior to a specific purpose in a specific environment using reasoning, planning, and problem solving. Frontal-subcortical circuits are the effector mechanisms of executive functions and mature progressively throughout childhood and adolescence (37). Executive control function should be evaluated in children with MDs (20), considering that abnormal presence of intra-cerebral metabolites, such as lactate, could disrupt the development and the functioning of frontal-subcortical networks (20). Furthermore, the presence of these metabolites could also cause psychiatric symptoms, in particular in zones such as the caudate nucleus, the cingulate cortex, and the hippocampus with regard to depression and anxiety (38, 39). There is therefore a real interest in studying the association between neuropsychological aspects, executive functions, and psychiatric symptoms in children with MDs (40) The executive functions comprise all the processes that help to monitor and regulate cognitive processes during complex tasks and include planning, self-regulation, behavior organization, cognitive flexibility, working memory, error detection and correction, inhibition, sustained attention, and resistance to interference (41). Disorders of executive functions are also linked to anxiety and depression in children and adults (40, 42). Future studies should aim to understand the mechanisms underlying clinical symptoms in MDs in children and the adolescents by focusing on the analysis of the psychiatric profile and, more specifically, the anxiety and the depression and the neuropsychological profile through the dysexecutive syndrome hypothesis.
This systematic review shows that children and adolescents affected with MDs may have psychiatric symptoms and neuropsychological impairment that are similar to those observed in adults highlighting the importance of considering them as key clinical signs for the diagnosis of MDs in pediatric practice. It seems of interest to better know the phenotype in children and adolescents and highlights the developmental specificities in MD diseases.
All datasets presented in this study are included in the article/supplementary material.
Design of the study: ER, CC, MB, AR. Data analysis: ER, CC, CP, AR. Article writing and revising: ER, PD, CC, MB, CP, PB, DB, AR. Revision of the manuscript: ER, PD, CC, MB, CP, PB, DB, AR.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank the University of Angers and the Enjeu[x] program for their financial support.
1. Gorman GS, Chinnery PF, DiMauro S, Hirano M, Koga Y, McFarland R, et al. Mitochondrial diseases. Nat Rev Dis Primer (2016) 2:16080. doi: 10.1038/nrdp.2016.80
2. Chinnery PF. Mitochondrial Disorders Overview. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJ, Stephens K, et al. editors. GeneReviews®. Seattle (WA): University of Washington, Seattle (1993). [cité 3 mars 2020]. Disponible sur: http://www.ncbi.nlm.nih.gov/books/NBK1224/.
3. Finsterer J. Mitochondriopathies. Eur J Neurol (2004) 11(3):163–86. doi: 10.1046/j.1351-5101.2003.00728.x
4. McFarland R, Taylor RW, Turnbull DM. A neurological perspective on mitochondrial disease. Lancet Neurol (2010) 9(8):829–40. doi: 10.1016/S1474-4422(10)70116-2
5. van Adel BA, Tarnopolsky MA. Metabolic myopathies: update 2009. J Clin Neuromuscul Dis (2009) 10(3):97–121. doi: 10.1097/CND.0b013e3181903126
6. Koene S, Jansen M, Verhaak CM, De Vrueh RLA, De Groot IJM, Smeitink JAM. Towards the harmonization of outcome measures in children with mitochondrial disorders. Dev Med Child Neurol (2013) 55(8):698–706. doi: 10.1111/dmcn.12119
7. Bosbach S, Kornblum C, Schröder R, Wagner M. Executive and visuospatial deficits in patients with chronic progressive external ophthalmoplegia and Kearns-Sayre syndrome. Brain J Neurol (2003) 126(Pt 5):1231–40. doi: 10.1093/brain/awg101
8. Yatsuga S, Povalko N, Nishioka J, Katayama K, Kakimoto N, Matsuishi T, et al. MELAS: a nationwide prospective cohort study of 96 patients in Japan. Biochim Biophys Acta (2012) 1820(5):619–24. doi: 10.1016/j.bbagen.2011.03.015
9. Anglin RE, Tarnopolsky MA, Mazurek MF, Rosebush PI. The psychiatric presentation of mitochondrial disorders in adults. J Neuropsychiatry Clin Neurosci (2012) 24(4):394–409. doi: 10.1176/appi.neuropsych.11110345
10. Rosebush PI, Anglin RE, Rasmussen S, Mazurek MF. Mental illness in patients with inherited mitochondrial disorders. Schizophr Res (2017) 187:33–7. doi: 10.1016/j.schres.2017.05.010
11. Kanellopoulos AK, Mariano V, Spinazzi M, Woo YJ, McLean C, Pech U, et al. Aralar Sequesters GABA into Hyperactive Mitochondria, Causing Social Behavior Deficits. Cell (2020) 180(6):1178–97. doi: 10.1016/j.cell.2020.02.044
12. Finsterer J. Central nervous system manifestations of mitochondrial disorders. Acta Neurol Scandinavica (2006) 114(4):217–38. doi: 10.1111/j.1600-0404.2006.00671.x
13. Finsterer J. Mitochondrial disorders, cognitive impairment and dementia. J Neurol Sci (2009) 283(1–2):143–8. doi: 10.1016/j.jns.2009.02.347
14. Finsterer J. Cognitive dysfunction in mitochondrial disorders. Acta Neurol Scand (2012) 126, 1:1–11. doi: 10.1111/j.1600-0404.2012.01649.x
15. Anglin RE, Garside SL, Tarnopolsky MA, Mazurek MF, Rosebush PI. The psychiatric manifestations of mitochondrial disorders: a case and review of the literature. J Clin Psychiatry (2012) 73(4):506–12. doi: 10.4088/JCP.11r07237
16. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev (2015) 4:1. doi: 10.1186/2046-4053-4-1
17. Koene S, Kozicz TL, Rodenburg RJT, Verhaak CM, de Vries MC, Wortmann S, et al. Major depression in adolescent children consecutively diagnosed with mitochondrial disorder. J Affect Disord (2009) 114(1–3):327–32. doi: 10.1016/j.jad.2008.06.023
18. Verity CM, Winstone AM, Stellitano L, Krishnakumar D, Will R, McFarland R. The clinical presentation of mitochondrial diseases in children with progressive intellectual and neurological deterioration: a national, prospective, population-based study. Dev Med Child Neurol (2010) 52(5):434–40. doi: 10.1111/j.1469-8749.2009.03463.x
19. Morava E, Gardeitchik T, Kozicz T, de Boer L, Koene S, de Vries MC, et al. Depressive behaviour in children diagnosed with a mitochondrial disorder. Mitochondrion (2010) 10(5):528–33. doi: 10.1016/j.mito.2010.05.011
20. Schreiber H. Pilot study on executive function and adaptive skills in adolescents and young adults with mitochondrial disease. J Child Neurol (2012) 27(12):1506–16. doi: 10.1177/0883073812442589
21. Eom S, Lee Y-M. Preliminary Study of Neurodevelopmental Outcomes and Parenting Stress in Pediatric Mitochondrial Disease. Pediatr Neurol (2017) 71:43–9. doi: 10.1016/j.pediatrneurol.2017.01.019
22. Eom S, Lee Y-M. Long-term Developmental Trends of Pediatric Mitochondrial Diseases: The Five Stages of Developmental Decline. Front Neurol (2017) 8:208. doi: 10.3389/fneur.2017.00208
23. Shurtleff H, Barry D, Chanprasert S, Firman T, Warner M, Saneto RP. Cognitive characteristics of mitochondrial diseases in children. Epilepsy Behav EB (2018) 88:235–43. doi: 10.1016/j.yebeh.2018.09.013
24. Major Depressive Disorder Working Group of the Psychiatric GWAS Consortium, Ripke S, Wray NR, Lewis CM, Hamilton SP, Weissman MM, et al. A mega-analysis of genome-wide association studies for major depressive disorder. Mol Psychiatry (2013) 18(4):497–511. doi: 10.1038/mp.2012.21
25. Fitzpatrick C, Barry C, Garvey C. Psychiatric Disorder Among Boys with Duchenne Muscular Dystrophy. Dev Med Child Neurol (1986) 28(5):589–95. doi: 10.1111/j.1469-8749.1986.tb03900.x
26. Smeitink JA, Zeviani M, Turnbull DM, Jacobs HT. Mitochondrial medicine: a metabolic perspective on the pathology of oxidative phosphorylation disorders. Cell Metab (2006) 3(1):9–13. doi: 10.1016/j.cmet.2005.12.001
27. Cadman D, Boyle M, Szatmari P, Offord DR. Chronic illness, disability, and mental and social well-being: findings of the Ontario Child Health Study. Pediatrics (1987) 79(5):805–13.
28. Gortmaker SL, Walker DK, Weitzman M, Sobol AM. Chronic conditions, socioeconomic risks, and behavioral problems in children and adolescents. Pediatrics (1990) 85(3):267–76.
29. Wallander JL, Thompson RJ, Alriksson-Schmidt A. (2003). Psychosocial Adjustment of Children with Chronic Physical Conditions. In: Roberts MC, editor Handbook of pediatric psychology, New York: Guilford Press.
30. Ozelle R, Doudard A, Bodin A-L, Gueden S, Duverger P, Riquin E. [Organic troubles with psychiatric symptoms: What is the appropriate childhood and adolescence psychiatric care? Reflections on disimmune encephalitis cases]. Arch Pediatr Organe Off Soc Francaise Pediatr (2017) 24(5):483–91. doi: 10.1016/j.arcped.2017.02.030
31. Satogami K, Takahashi S, Kose A, Shinosaki K. Schizophrenia-like symptoms in a patient with Leigh syndrome. Asian J Psychiatry (2017) 25:249–50. doi: 10.1016/j.ajp.2016.12.012
32. Bachmann RF, Wang Y, Yuan P, Zhou R, Li X, Alesci S, et al. Common effects of lithium and valproate on mitochondrial functions: protection against methamphetamine-induced mitochondrial damage. Int J Neuropsychopharmacol (2009) 12(6):805–22. doi: 10.1017/S1461145708009802
33. Villa RF, Ferrari F, Gorini A, Brunello N, Tascedda F. Effect of desipramine and fluoxetine on energy metabolism of cerebral mitochondria. Neuroscience (2016) 330:326–34. doi: 10.1016/j.neuroscience.2016.05.051
34. Chan ST, McCarthy MJ, Vawter MP. Psychiatric drugs impact mitochondrial function in brain and other tissues. Schizophr Res (2020) 217:136–47. doi: 10.1016/j.schres.2019.09.007
35. Ben-Shachar D, Ene HM. Mitochondrial Targeted Therapies: Where Do We Stand in Mental Disorders? Biol Psychiatry (2018) 83(9):770–9. doi: 10.1016/j.biopsych.2017.08.007
36. Nissenkorn A, Zeharia A, Lev D, Watemberg N, Fattal-Valevski A, Barash V, et al. Neurologic Presentations of Mitochondrial Disorders. J Child Neurol (2000) 15(1):44–8. doi: 10.1177/088307380001500110
37. Roy A, Lodenos V, Le Gall D, Roulin J-L. Le syndrome dysexécutifs chez l’enfant : Entre avancées scientifiques et questionnements. ANAE (2017) 29(146):27–38.
38. Anglin RE, Rosebush PI, Noseworthy MD, Tarnopolsky M, Weber AM, Soreni N, et al. Metabolite measurements in the caudate nucleus, anterior cingulate cortex and hippocampus among patients with mitochondrial disorders: a case–control study using proton magnetic resonance spectroscopy. CMAJ Open (2013) 1(1):E48–55. doi: 10.9778/cmajo.20120020
39. Anglin RE, Rosebush PI, Noseworthy MD, Tarnopolsky M, Mazurek MF. Psychiatric symptoms correlate with metabolic indices in the hippocampus and cingulate in patients with mitochondrial disorders. Transl Psychiatry (2012) 2:e187. doi: 10.1038/tp.2012.107
40. Gohier B, Ferracci L, Surguladze SA, Lawrence E, El Hage W, Kefi MZ, et al. Cognitive inhibition and working memory in unipolar depression. J Affect Disord (2009) 116(1–2):100–5. doi: 10.1016/j.jad.2008.10.028
41. Torres Nupan MM, Velez Van Meerbeke A, López Cabra CA, Herrera Gomez PM. Cognitive and Behavioral Disorders in Children with Neurofibromatosis Type 1. Front Pediatr (2017) 5:227. doi: 10.3389/fped.2017.00227
Keywords: mitochondrial diseases, children, adolescent, neuropsychological profile, psychiatric profile
Citation: Riquin E, Duverger P, Cariou C, Barth M, Prouteau C, Van Bogaert P, Bonneau D and Roy A (2020) Neuropsychological and Psychiatric Features of Children and Adolescents Affected With Mitochondrial Diseases: A Systematic Review. Front. Psychiatry 11:747. doi: 10.3389/fpsyt.2020.00747
Received: 07 May 2020; Accepted: 16 July 2020;
Published: 28 July 2020.
Edited by:
David Cohen, Université Pierre et Marie Curie, FranceReviewed by:
Roberto Canitano, Siena University Hospital, ItalyCopyright © 2020 Riquin, Duverger, Cariou, Barth, Prouteau, Van Bogaert, Bonneau and Roy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elise Riquin, ZWxpc2UucmlxdWluQGNodS1hbmdlcnMuZnI=; orcid.org/0000-0002-5956-3014
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.