 Arianna Giorgetti1,2
Arianna Giorgetti1,2 Francesco Paolo Busardò3*Roberta Tittarelli4
Francesco Paolo Busardò3*Roberta Tittarelli4 Volker Auwärter2,5
Volker Auwärter2,5 Raffaele Giorgetti3
Raffaele Giorgetti3- 1Legal Medicine and Toxicology, University-Hospital of Padova, Padova, Italy
- 2Institute of Forensic Medicine, Forensic Toxicology, Medical Center, University of Freiburg, Freiburg, Germany
- 3Section of Legal Medicine, Department of Excellence SBSP, University Politecnica delle Marche of Ancona, Ancona, Italy
- 4Unit of Forensic Toxicology, SAIMLAL Department, Sapienza University of Rome, Rome, Italy
- 5Faculty of Medicine, University of Freiburg, Freiburg, Germany
Background: Synthetic cannabinoid receptor agonists (SCRAs) have become the largest group of new psychoactive substances monitored by the European Union Early Warning System. Despite the wide diffusion on the market, data regarding effects, toxicities, and mechanisms as well as toxic/lethal doses are still scarce.
Methods: A comprehensive literature search for articles published up to January 2019 was performed in multiple electronic databases. Only cases of death in which toxicological analyses revealed the presence of SCRAs in blood or urine and at least an external examination was performed, including those occurred in emergency departments, were included.
Results: Of 380 studies identified, 354 were excluded, while 8 additional manuscripts were included through the screening of relevant references cited in the selected articles. A total number of 34 manuscripts (8 case series and 26 case reports) were included.
Conclusions: Typical toxic ranges for SCRAs have not been so far identified, and the results of toxicological analyses should be interpreted with caution. In death cases involving SCRAs, a thorough post-mortem examination is a prerequisite to assess the role of the substance use in the deceased and to identify a probable mechanism of death. Even after a comprehensive analysis of clinical, circumstantial, toxicological, and autoptic data, the cause and manner of death remain unclear in some cases.
Introduction
Synthetic cannabinoids or synthetic cannabinoid receptor agonists (SCRAs) are a heterogeneous group of compounds designed to mimic the effects of delta-9-tetrahydrocannabinol (Δ9-THC) by binding to the cannabinoid receptors CB1 and CB2. In contrast to Δ9-THC, a partial agonist at the CB1 and CB2 receptors, most of the SCRAs marketed so far are full agonists at these receptors and additionally show much higher potency (1, 2). Since their first detection in herbal blends in 2008 (3, 4), they have become the largest group of new psychoactive substances (NPS), with 190 compounds reported to the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) until the end of 2018 and an extraordinary dynamic market (5), even though there has been a relative reduction of the rate of new compounds per year (5). It was initially claimed that SCRAs could be “safe” alternatives to marijuana, due to similarities of their pharmacological profile to Δ9-THC and other phytocannabinoids, and lots of compounds binding to the cannabinoid receptors have been synthesized and evaluated regarding their binding affinities and activity in animal or cell models since then (6). However, a huge number of in-vitro and in-vivo studies, reports, and alerts have highlighted severe adverse events and enhanced toxicity (2, 7, 8) prompting the United States Drug Enforcement Administration to classify some of these compounds as Schedule I substances. Signs and symptoms of SCRAs consumption include psychomotor agitation, euphoria, anxiety, confusion, and psychosis on the one side, sedation and loss of consciousness on the other (9, 10). Adverse cardiac effects are among the most frequently encountered adverse reactions after SCRA intake. Particularly, both tachycardia (more frequently) and bradycardia have been reported. Gastro-intestinal symptoms with nausea and vomiting are also common. Moreover, rhabdomyolysis, hyperthermia, and hypothermia, seizures, respiratory depression, nephro- and hepatotoxicity were described in combination with SCRA intake (11, 12). Some of these effects might be mediated also by interference with other neurotransmitter pathways, since certain SCRAs can also bind to glutamatergic, serotonin (5-HT), opioid, and both adrenergic and cholinergic receptors and to calcium, sodium, potassium channels (13).
Several cases of intoxication have been reported caused by, e.g., MDMB-CHMICA and AB-CHMINACA, which can cause severe symptoms requiring hospitalization and prolonged recovery time (14). Other compounds, such as Cumyl-PEGACLONE, have been suggested as “relatively safe” due to the low number of poisonings despite the abundant presence in herbal blends (25–30% of tested products) and their widespread use (prevalence of 29% in samples positive for SCRAs, including testing for driving under the influence, insult, and threat, criminal offenses). Moreover, the role of the SCRA was deemed minor or contributory in the majority of death cases (15).
Despite the wide diffusion in the market, data regarding effects, toxicities, and mechanisms as well as toxic/lethal doses are still scarce, making SCRAs one of the most “unpredictable” classes of substances (16). Moreover, only few studies regarding the time of detectability, the diffusion in tissues, and the post-mortem distribution of the drugs can be retrieved in the literature. The limited knowledge regarding the pharmacodynamics and pharmacokinetics of SCRAs contributes to the difficulties of the interpretation of toxicological results. Furthermore, several aspects, such as interactions among SCRAs or in the combination with other drugs, are difficult to assess in cases of SCRA-related deaths.
To our knowledge, there are no previous detailed review papers, which report fatalities caused by the misuse of synthetic cannabinoids providing circumstantial, analytical data, and complete results of post-mortem examination.
The aim of the present study is to offer an overview of thoroughly investigated fatalities involving SCRAs, considering not only analytical results, but also an in-depth analysis on investigative data, analytical methods, and macro and microscopic findings.
Materials and Methods
Literature Search and Inclusion/Exclusion Criteria
In February 2019 a literature search for articles published until January 2019 was performed in electronic databases (Pubmed, Scopus), using the following research terms: “synthetic cannabinoids” AND (death OR fatal OR fatalities OR autopsy OR forensic OR post-mortem). Search was done in English language and duplicates were manually deleted. Titles and abstracts were screened and only cases of death, in which toxicological analyses revealed at least one SCRA in blood or urine, and at least an external examination was performed were included. Patients rushed to the emergency department and subsequently died were also included in the selected cases.
Exclusion criteria were: irretrievability of a full-text; off-topic articles (e.g., death cases in which other NPS, but no SCRAs, were detected); in vitro/animal model studies; herbal blends analyses; non-fatal cases of intoxication; books/reviews not including unpublished cases of death due to SCRAs; autopsy/external examination not performed.
Data Extraction
An electronic database with the selected papers was built in Excel ® (Microsoft Office, 2006). For each included manuscript, authors, title, journal, year, and type of publication (e.g., case report, case series), number of death cases and type of involved SCRA were extracted.
A separate database was built with the retrieved papers and, for each death case, the following information was extracted:
● type of victim, referring to age and sex;
● concentrations of SCRA retrieved during toxicological analyses in central and peripheral blood, urine, and tissues;
● other substances detected in blood;
● circumstantial data (and whatever relevant emerged during the death scene investigation), with particular reference to a history of drug abuse and to the availability of herbal blends/paraphernalia at the scene,
● post-mortem gross and microscopic findings;
● cause, manner, and suggested mechanism of death;
● post-mortem interval (PMI)
● role of the SCRA as described by the authors.
Data Analysis/Interpretation
Only a descriptive statistic was applied. For each death case, two independent observers assigned a Toxicological Significance Score (TSS) to the involved SC, in accordance to the methodology proposed by Elliott et al. (17). When no agreement was achieved, a third person was consulted. This rating was compared with the likely role in death assigned by the authors.
Information related to toxicological analytical methodology (linearity, calibration curve, accuracy, precision, limit of detection/quantification, matrix effect), in accordance with what suggested by Welter-Luedeke and Maurer (18) were also noted and taken into consideration when evaluating the single cases.
Results
Literature Review
The literature search resulted in 380 sources after elimination of duplicates. Of these, 354 were excluded applying the criteria listed in “Materials and Methods,” while 8 additional manuscripts were included through the screening of references cited in the selected articles. Details of the literature search are listed in Figure 1.
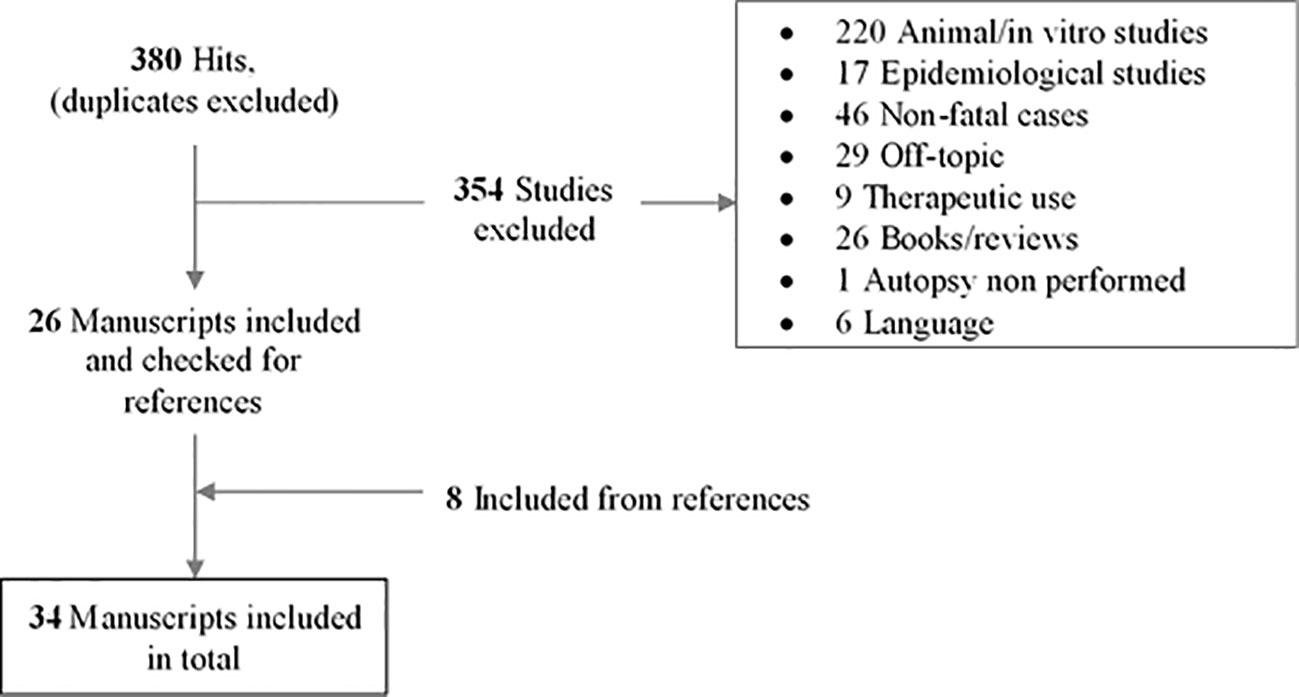
Figure 1 Flow diagram of study identification, screening, and selection.
Finally, a total of 34 manuscripts were included (authors, title, journal, date of publication, and involved SCRAs are shown in Table 1), corresponding to 74 published cases. Of the 34 manuscripts, 8 consisted in case series and 26 in case reports, including articles only providing new analytical data on previously reported death cases (Table 1). Tables 2 and 3 both refer to the single cases. Particularly, Table 2 displays the epidemiology of the victim, the involved SCRA(s), other substances detected, anamnestic/circumstantial, and clinical data, macroscopic and microscopic features, cause, and suggested mechanism of death, toxicological significance score, and role of SCRA as suggested by the authors of the paper. In Table 3, concentrations in peripheral, central blood, urine, and tissues, together with the PMI are shown.
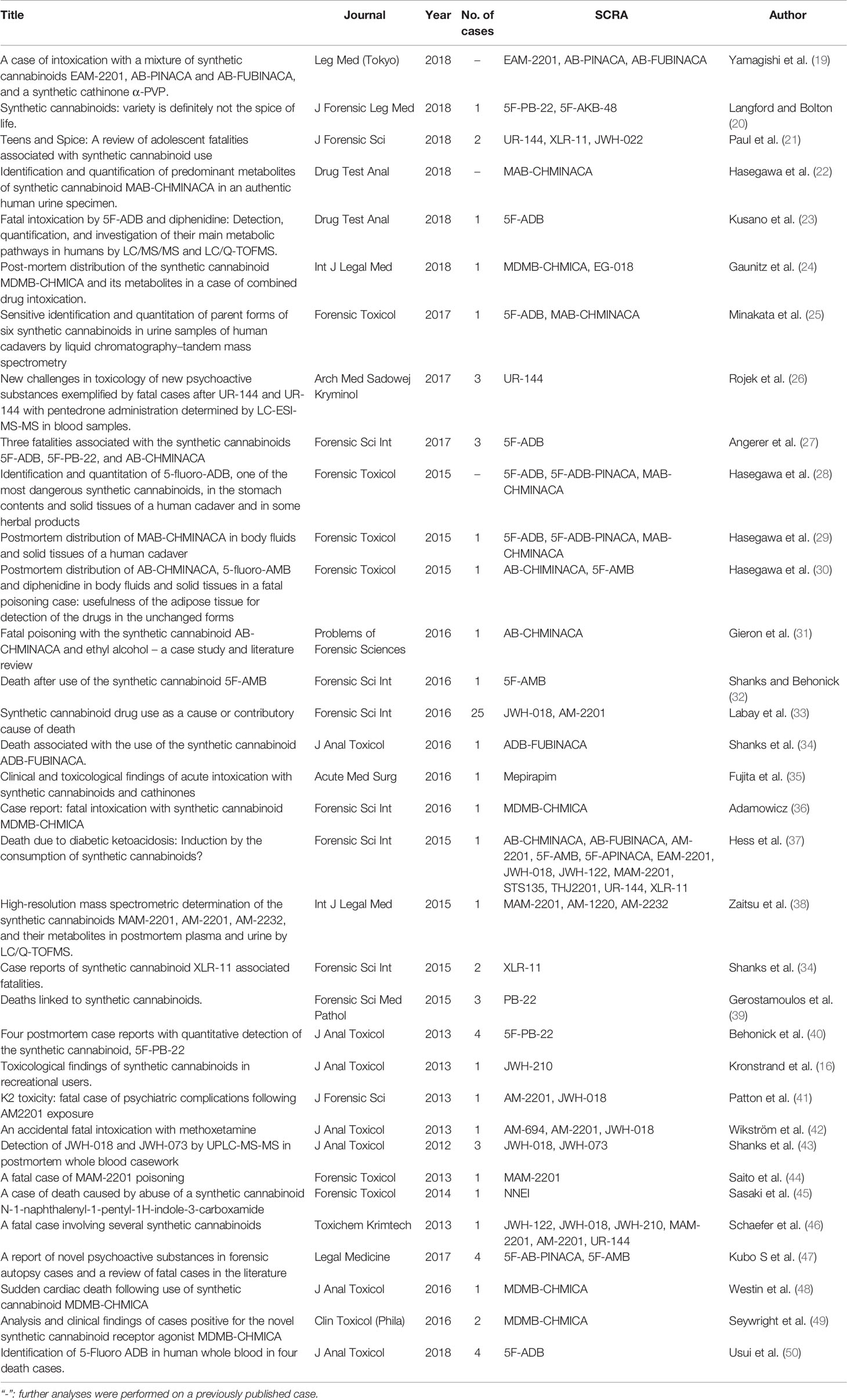
Table 1 Characteristics of the included studies: authors, titles, journal, and year of publication, number of cases reported and type of SCRAs involved (semisystematic names).

Table 2 Results of the literature revision for each case.
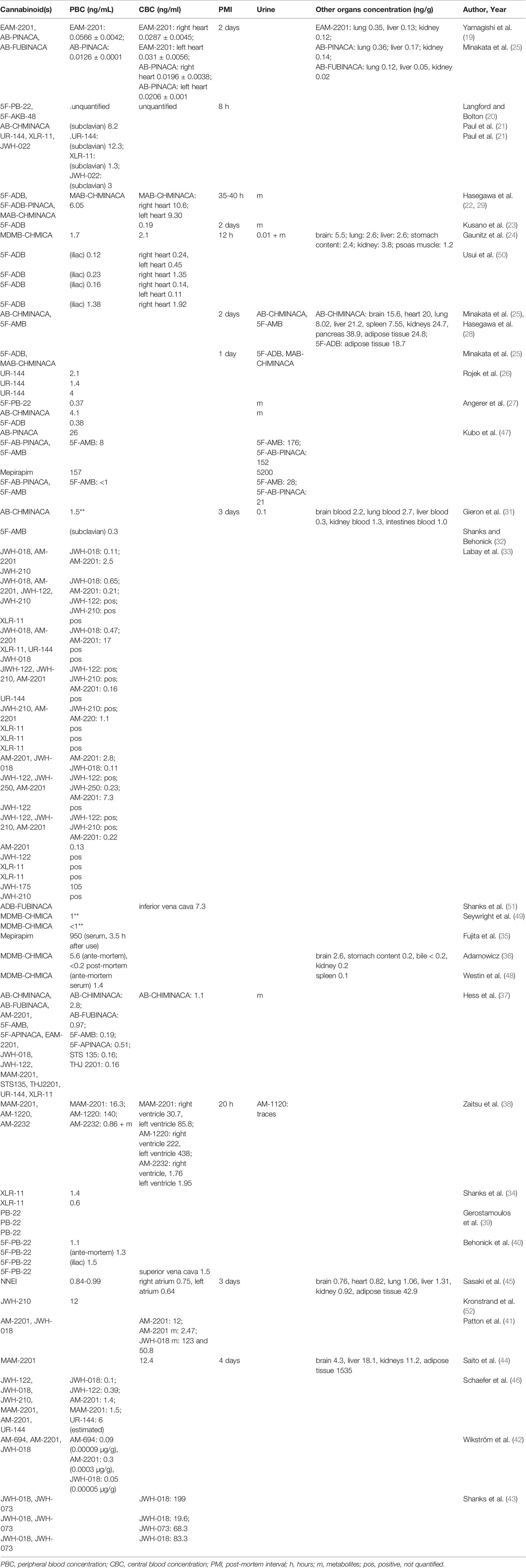
Table 3 Post-mortem concentrations in peripheral blood (PBC), central blood (CBC) and other tissues.
Analytical Issues
Sample preparation and extraction procedures varied widely: liquid-liquid extraction was the most frequently used, though solid-phase extraction (24, 44, 47, 53) and QuEChERS dispersive solid-phase extraction (29, 30, 35, 50) were also reported. Only in a minority of the cases, the standard addition method was employed for quantification (19, 23, 28, 30). In two cases, liquid chromatography quadrupole time-of-flight mass spectrometry (LC-QToF-MS) was used to detected and quantitate parent compounds and/or metabolites in blood and ante-mortem serum (38, 48).
Overall, 31 SCRAs (EAM-2201, AB-PINACA, 5F-PB-22, 5F-AKB-48, 5F-ADB, AB-CHMINACA, UR-144, XLR-11, JWH-022, MAB-CHMINACA, MDMB-CHMICA, 5F-AMB, Mepirapim, JWH-018, AM-2201, JWH-210, JWH-122, JWH-250, JWH-175, ADB-FUBINACA, AB-FUBINACA, 5F-APINACA, MAM-2201, STS135, THJ 2201, AM-1220, AM-2232, PB-22, NNEI, AM-604, and JWH-073) were detected, some being more frequently identified in the revised cases, such as 5F-ADB, XLR-11, AM-2201, AB-CHMINACA, and JWH-018.
Even if reported with lower rates, 5F-PB-22, UR-144 were also common. XLR-11 was mostly reported in 2016, while 5F-ADB showed a peak in 2017 and 2018. However, a clear trend cannot be determined on the sole basis of this data.
While some laboratories applied national or international validation guidelines, such as those of the German Society of Toxicological and Forensic Chemistry (GTFCh), “in house” methods have also been adopted, stating overall good results (31, 32, 43). Analytical details were not always given and not all of the above-mentioned parameters, especially matrix-effects, were systematically assessed (19, 27, 31, 37, 38, 41, 44, 52).
According to previously published cases (33, 43), concentrations of SCRAs in post-mortem cases covered a wide range, from 0.01 (19) to 199 ng/mL (43), although lower concentrations, in the range 0.5 to 2.5 ng/ml, were most frequently encountered.
Peripheral blood was analyzed in 53 cases out of 74 (72%). In 8 cases (11%) only heart blood concentrations were stated, while both peripheral and central concentrations were published in 10 cases (14%). Other biological matrices, apart from urine, were quantitatively analyzed in only 8 cases (11%) (Table 3). Other substances were found in 44 out of 74 cases (59%).
As regard other xenobiotics detected, ethanol was detected in 13 cases (17%), though levels ≥ 1.5 g/L were found only in 6. A co-consumption of NPS, as synthetic cathinones (pentedrone, α-PVP, DL-4662), hallucinogens (6-APB, 6-MAPB, methoxetamine), anesthetics (diphenidine), and synthetic opioids (AH-7921) was seen in 11 cases (15%). Common drugs of abuse detected included antidepressive/neuroleptics/antipsychotics (quetiapine, trimipramine, olanzapine, sodium valproate, mirtazapine, amitriptyline, phenytoin, paroxetine, aripiprazole, citalopram, fluoxetine, haloperidol, trazodone, venlafaxine, pregabalin, topiramate) (12/74, 16.2%), cannabinoids (10/74, 13%), amphetamines, benzodiazepines (both 6/74, 8%) and opioids (5/74, 7%).
Case Reports
The age of the deceased ranged from 14 to 61 (19). Mean age was 32, median 29. The 38.5% belonged to the 20 to 29 decades. Teenagers were also represented (15.4%) (Figure 2). With reference to the gender of the victims, 88.1% were male and 11.9% were female. A past use of drugs and/or alcohol was reported in 18 out of 74 cases (24%), while poor mental health was only reported in 5 cases (7%).
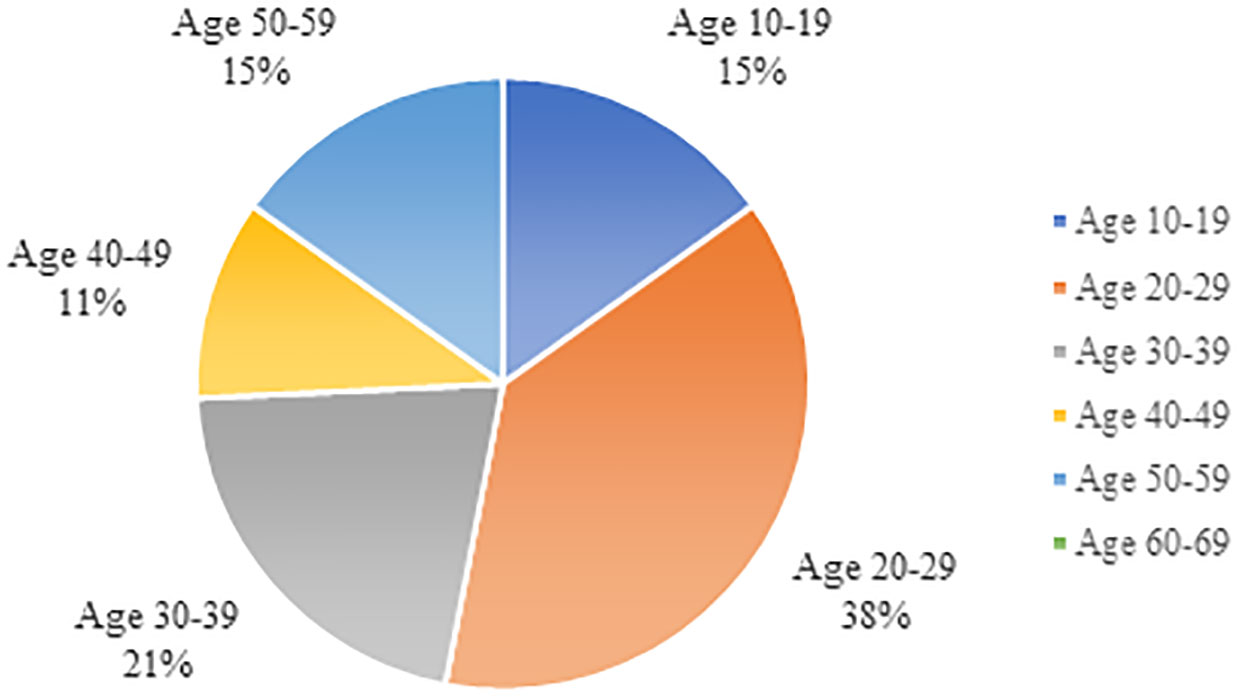
Figure 2 Age distribution among the cases reported in the literature.
Herbal blends, smoking devices (e.g., pipes) and other paraphernalia were found during the death scene investigation (DSI) in 30 of 74 cases (41%) and were variably labeled as “Aladdin platinum/limited,” “Herbal incense, the super lemon,” “F1,” “Hammer Head,” “Magic Gold,” “Desert Premium Potpourri,” “AL 37,” “AP 31,” “Strongman,” “GM sapphire,” “Heart Shot Black,” “Apollo,” “Mocarz,” “Smoke XXX. A potent potpourri,” “Mad Hatter Incense,” “Fairy evolution,” “Mary Joy Annihilation,” “Passion Flower Herb – Zonk,” “Stoner Pot-Pourri K11,” “Supanova Pot-Pourri,” “K2 Cherry,” “Space Cade Flight Risk,” “Game over,” “Orange Flame,” “Legal Phunk,” “Mojo.” Clinical data was available in 15 cases (20%) and mostly included the detection of cardiac arrest/asystolia/fibrillation at the arrival to an Emergency Department.
Results of post-mortem examination, as for macroscopical or gross findings, were available in 55 cases (74%), including those cases in which only a short referral to “unremarkable findings” was reported. In most cases in which a SC was later discovered during toxicological analysis, the post-mortem examination had revealed only non-specific signs of intoxication, such as pulmonary edema and congestion, brain edema, hemolysis, and signs of aspiration (34, 40). In some cases, stomach and gastroduodenal erosions (20, 35), abundant hypostasis coupled to petechiae (27, 29, 37) and intracutaneous skin bleedings (vibices) (30) were reported. Lastly, cardiac abnormalities, such as cardiomegaly (33, 43), dilatative or hypertrophic cardiomyopathy (21), stenosis due to atherosclerosis (33, 46) or acute thrombosis of the coronary arteries were seen (32).
Histological data, as a specific result of a microscopical analysis, was clearly described only in 13 cases (18%).
Cause of death was stated in all but 4 cases (5%). Cardiac arrhythmias and cardio-circulatory acute effects were listed in 17 cases (23%) as cause of death or as underlying mechanisms in a group of mono and poly-drug intoxications, involving both teenagers and adults (20, 21, 35, 40, 48). A number of death cases were associated with excited delirium and police restraints (33), as well as fall from height, either due to drug-induced psychosis or reduced awareness with accidental falling (24, 26). Behavioral effects could also lead to suicide (26), self-inflicted self-injuries (41) and further consumption of other drugs (26, 55). Respiratory depression (27), especially in the setting of mixed intake of xenobiotics (33, 51), and asphyxia due to aspiration of gastric content in a state of coma (22, 27, 28) were also declared.
Manner of death was mostly accidental or not given and 4 cases of suicide (5%) were recognized.
Post-mortem interval (PMI) was stated in 11 cases (15%) and ranged from 8 hours to 4 days (Table 3).
Discussion
The systematic review of the literature has resulted in an unexpectedly high number of cases of death involving SCRAs. Though, given the widespread use of the compounds, similar fatalities might be under-reported (publication bias) or under-recognized as a result of the challenges of post-mortem analyses. Indeed, the delay in developing and updating analytical methodologies affects the capability of many laboratories to detect and report cases of SCRA-related death, particularly when novel compounds which just entered the market are involved (55). Accordingly, the results here presented cannot be taken to estimate the prevalence.
Circumstantial Data
In almost the totality of cases, a possible involvement of SCRAs was suggested by either a past history of drug/alcohol abuse, by witnesses' statements of partying or smoking shortly before collapse, or by the DSI, which revealed paraphernalia and herbal residues. Depending on the market availability, it emerged that the content of such packages varied over time (31, 36, 55). Thus, it must be kept in mind that the product names do not validly predict the ingested substances.
Although e-cigarettes and e-liquids represent an innovative and attractive way to consume SCRAs (56, 57), no vaping liquids were reported in the circumstantial data of the reviewed death cases. The link between e-cigarettes and SCRA consumption might be less familiar and known to the investigators, possibly resulting in such liquids not being systematically seized and/or analyzed. When such paraphernalia are found, an analysis of vaping liquids collected at the DSI should be strongly encouraged.
SCRAs are not detected by common immunoassays and require a target analysis, which is usually only requested by authorities and conducted when a suspicion is raised, due to analytical limitations and economic reasons (21). This factor could lead to a failure to recognize such cases and consequently to a massive underestimation of the number of death cases involving SCRAs. This underlines the importance of an appropriate awareness and of an in-depth experience in forensic toxicology during DSI and when interviewing witnesses.
Analytical Issues
The data extracted from the revision of the literature regarding toxicological analyses once again highlights the role of liquid chromatography-mass spectrometry (LC-MS/MS) for the quantification of SCRAs in biological specimens, although a singular preferred method for sample extraction is not known, given the variety of chemical differences among analytes (52). The use of standard addition methods, as recently suggested in a series of intoxications (58) is limited, possibly due to the low amount of post-mortem blood collected at the autopsy.
Only a small number of SCRAs emerged from the literature review, compared to the quantity of compounds included in the NPS category. We do not believe that this is a bias due to an attention to recent molecules, since the follow-up period ended in 2019 and more recent molecules, such as SCRAS bearing a γ-carbolinone core, were not found. This observation could be on the contrary related to difficulties in detecting SCRAs in the absence of a dedicated and updated method. The main challenge in forensic toxicology from an analytical point of view resides indeed in keeping methods updated, in order to detect novelties as soon as they are involved in death cases. Although there was a decrease in the last years, the frequent emergence of novel compounds might lead to missing relevant analytes. This was clearly demonstrated by cases where re-analysis of samples with novel and more sensitive methods allowed for identification of substances previously undetected (19, 22, 25). Very sensitive methods are needed in blood, given the low concentrations reported in the literature (52) and urine analysis can reveal a previous intake even when nothing is detected in blood (22, 23).
Once a new methodology for the analysis of biological specimens has been established, even in case reports, a so-called short validation, including selectivity, linearity, accuracy, precision, and matrix effect, is strongly recommended even if not always performed or published (59). In the case described by Langford et al., for example, the analyses were granted by a private licensed forensic laboratory, and no information was disclosed due to alleged “competition and market issues” (20). The absence of a clearly stated methodology and validation process questions the reliability of the analytical results and limits the comparability of the data. The validation could be further hampered by the lack of material for re-analysis and/or by the lack of isotopically labeled standards (27, 33). Lack of material represents a serious limitation particularly in the case of measured concentrations being far above the linear range of the calibration, even though results might be estimated by extrapolation (27, 38, 43). It has to be underlined that the vast majority of the methods for SCRAs quantification were validated in serum and not in post-mortem blood.
When evaluating the concentrations, several aspects need to be considered, including site of sampling, post-mortem interval, possible tolerance of the user, co-consumption of other drugs, potency of the compounds, chemical characteristics, and time delay between intake and death.
Some compounds, such as 5F-ADB, are known to be particularly unstable (29) and this could explain the extremely low concentrations of the highly potent SCRAs in our review (27). Rapid degradation due to pyrolysis, ante-mortem drug metabolism, as well as post-mortem redistribution and degradation (due to remaining esterase activity) were considered as further main factors for reduced concentrations and should be considered for all SCRAs, though with different weighting (19, 23, 44).
When compared to others SCRAs, mean concentrations were relatively higher for AB-CHMINACA, despite its high potency (21, 27). This could be due to the narrow time interval between drug smoking and death, approximately an hour in the case described by Paul et al. (21), or to a high tolerance of the subject implying high doses (21).
Concerning post-mortem redistribution (PMR), disparities among central and peripheral blood levels were mostly slight (19, 45) (PMI: 2 days). A 1.2 quotient of central/peripheral blood (C/P ratio) was found in a case of MDMB-CHMICA 12 h after death, and this result was interpreted as not indicative of PMR (24). Similarly, concentrations were in the same range in all tissues in a case described by Yamagishi et al. (19). On the contrary, cardiac blood levels strongly exceeded the peripheral ones in the case of Zaitsu et al. (38) for MAM-2201, AM-1220, and AM-2232 (PMI: 20 h), where left and right ventricle blood levels were 2 to 5 and 1.5 to 2 times higher than femoral blood concentrations. Quantification employed LC-QTOF, a full validation was not performed and concentrations of some analytes were far above the highest calibration point. Nevertheless, C/P ratios appear to tend to values above 1 especially in the case of short time intervals between smoking and death (in this case 1.5 h). A death shortly after smoking, with high concentrations of SCRAs in lungs being released to the surrounding vessels and tissues could explain the higher levels in the blood of the left ventricle (60), although the authors suggested a myocardial accumulation instead (38). C/P ratios of 1.75 to 1.54 were also seen by Hasegawa et al. (29) (PMI: 2 days).
Divergences among compounds suggest that the chemical characteristics (e.g., greater or lower lipophilicity) as well as the pattern of use should be considered when hypothesizing PMR (45). Ingestion and smoking probably result in higher concentrations in stomach content and lungs, respectively. This could lead to a release into nearby vessels of the central compartment. Since femoral blood levels increase mostly due to release/redistribution from fat and muscle tissues, an inversed central/peripheral ratio would suggest a greater lipophilicity of the compound and/or chronic accumulation of SCRAs in deep compartments. However, the scarce information regarding time between last consumption and death as well as the PMI complicates the situation. Stability and matrix effects additionally limit the capability of drawing valid conclusions based on blood concentrations.
The distribution of SCRAs in tissues varied widely. Concentrations in tissues have been assessed only in a minority of cases and results may strongly depend on the employed methods of analysis, the description of which is beyond the scope of this article. Given the rarity of this type of measurement, which afford a time-demanding standard addition method (19), the available data regarding tissue distribution does not allow for general conclusions. However, they can be used to evaluate the specific case and might allow identifying potential sites of accumulation. For example, extremely high levels in the adipose tissue were seen for MAM-2201 (124 fold higher than blood concentration), leading to the suggestion of fatty tissue as a suitable target specimen for analysis (PMI: 4 days) (44). High adipose levels were also found for NNEI (45) (PMI 3 days) and might be interpreted as a result of continued substance use. According to Kusano et al. (23) adipose tissues are a suitable matrix for the detection of the parent compound, while other tissues (with higher esterase activity) could contain higher levels of metabolites.
High levels in liver and kidney tissue could be found in the case of more hydrophilic compounds (e.g., MAB-CHMINACA; PMI: 2–3 days) (29), especially when the interval between intake and death was short. In these cases, an accumulation in fatty tissue might not have occurred yet, requiring longer time (24, 29). Brain concentrations were high for MDMB-CHMICA in a case described by Gaunitz et al. (PMI: 12 h) and this allowed to confirm that the victim was under the effect of cannabinoids at the moment of death (24). High concentrations in lungs were also reported, pointing towards an intake through smoking.
In summary, blood and tissue concentrations should always be interpreted with caution, due to the multiple factors which have to be taken into account (e.g., PMR, PMI, active metabolites, stability, chemical characteristics, plasma/blood ratio, tolerance etc.) (61).
Pathology and Histopathology
The un-specificity of gross pathological findings heightens the risk of missing deaths involving SCRAs. Vomiting and aspiration of gastric content are highly suggestive for drug-induced coma or loss of consciousness in otherwise healthy and young subjects (22, 29). This was also seen in a case in which, originally, only urine was found positive for SCRAs, and further analyses demonstrated high blood concentrations of MAB-CHMINACA (22, 29). It should always be kept in mind that acute gastrointestinal bleedings could be due to several diseases and factors, such as Mallory-Weiss disease or hypothermia, and an accurate differential diagnosis remains fundamental before attributing such findings directly to SCRA consumption. For example, erosions seen in the case described by Langford and Bolton (20), could have been the result of ethanol intake, which was in his fatal ranges (3.11 g/L).
Bleedings and abundant hypostasis could raise the suspicion for a recent intake of SCRAs. In 2018, fatal and life-threatening bleedings were connected to superwarfarin-type drugs such as brodifacoum added to products allegedly containing SCRAs as reported by the Centers for Disease Control and Prevention (CDC), which released a health advisory. Long-acting anticoagulant rodenticides (LAARs) were occasionally found as adulterants in herbal blends (62). A case of death connected to anticoagulants is described in the literature (63), even though the case was not included in the review, since the past use of SCRAs emerged only from circumstantial data (thus, the paper did not fit into the inclusion criteria). It is not clear if hemolysis, abundant hypostasis, and intracutaneous or soft tissue bleedings can be caused by such adulterants or represent a hematological effect, maybe liver-mediated, of SCRAs themselves (40). As LAARs are usually not detected by urine screening analyses, highly sensitive LC-MS/MS methods are required for their detection (62).
The interpretation of cardio-vascular findings is discussed in the following subsection.
Cause and Mechanism of Death, TSS
Several preclinical studies and case reports addressed the increased cardiovascular risk related to SCRAs use, though scientific evidence is still limited (14, 64–68). This was reflected by our literature review, since abnormal findings in heart were seen and death related to acute cardiovascular arrest or collapse certified. However, it could be unclear if these deaths are actually related to SCRAs or not (69). Marijuana exerts some cardiovascular effects, acutely resulting in increased catecholamine release and, consequently, increased heart rate and vasodilation, with orthostatic hypotension (68). Cannabis is told either to exert negligible effects on blood pressure or an increase in blood pressure, and might increase the risk of myocardial infarction, particularly in predisposed subjects (68, 70–72). SCRAs, being more potent cannabinoid receptor agonists, have been linked to the occurring of myocardial infarction (64) even in the absence of coronary artery disease, and of arrhythmia-related sudden cardiac death (65–67). Sasaki et al. (45) found signs of hypertension and aging in a 20-year-old victim, coupled to myocardial suffering, and thus hypothesized a cardio-circulatory hyperactivity due to prolonged SCRA use. The diversity of potential injury mechanisms (between myocardial infarction and arrhythmia) may explain why in some cases band necrosis proved a myocardial damage (21, 45), while in others neither macroscopic nor microscopic signs were noted (20, 21, 35).
In the cases where post-mortem examination failed to identify signs of heart diseases, the attribution of cardiac death to the SCRA was mostly based on circumstantial data, e.g., the victim reported having smoked shortly before dying and/or a sudden collapse after smoking occurred (20, 35, 40). In a similar case, the possible role of SCRAs was confirmed by a serum sample collected only 2 h after a sudden collapse with asystolia, revealing 1.4 ng/mL of MDMB-CHMICA (48).
Moreover, asystole was initially noted in a case of death where, after resuscitation, a multi-organ failure finally led to cardiac arrest (36).
Atherosclerotic disease and other cardiac abnormalities, such as cardiomegaly and dilatative cardiomyopathy, pose an additional challenge to the assessment of the role of SCRAs in death cases (50, 61). In fact, drugs can either exacerbate a pre-existing condition, or be considered an irrelevant finding (33). In a case described by Tse et al. (64) a triple-vessel coronary thrombosis was found and death was attributed to myocardial infarction with a possible contributory role of SCRAs, despite the absence of analytical confirmation. In a case involving ADB-FUBINACA, Shanks et al. (51) concluded that, due to occurrence of behavioral effects followed by a sudden death, a SCRA-induced dysrhythmia contributed to the death, notwithstanding the presence of a potentially fatal thrombolytic occlusion. Similarly, a contributory role was stated by Tse et al. (64) despite morphological findings which could have explained the death by themselves. These cases demonstrate that it can be difficult to assess the cardiac effects of SCRAs, particularly in the presence of findings potentially constituting a cause of death on their own. In such cases, a TSS of “1,” which does not exclude a partial contribution, seems to be appropriate (17).
In cases of polydrug abuse, the evaluation of role cannot leave aside concentrations of xenobiotics, leading to attribution of different TSS on a case-by-case basis, e.g., TSS U with 3 g/L of ethanol, positive unquantified SCRAs and suspected arrhythmias (20) vs TSS 3 with 1.8 g/L ethanol, 1.5 ng/mL AB-CHMINACA and acute cardiorespiratory depression (50).
Coma/somnolence can lead to death directly, through vomiting/aspiration or indirectly due to environmental exposure and hypothermia (54). In a case presented by Kronstrand et al. (52), death occurred due to “hypothermia and SCRA use,” despite the absence of typical hypothermia-related signs such as freeze-erythema and Wischnewsky spots (52). Hypothermia after the use of SCRAs was seen in experimental studies on animals (e.g., male rats and monkeys) (73, 74) and has been partially related to the effects of cannabinoids on dopamine receptors (75), but has not been confirmed in humans yet. However, in a case described by Adamowicz (36) a cadaveric temperature of 35.1°C was measured, despite the victim was at home and the measurement took place only 30 minutes after the sudden collapse. This finding would be in line with the animal experimental data regarding the effect of SCRAs on body temperature and highlights the need to evaluate body and ambient temperatures in cases of death possibly related to such compounds. An “intoxicated-state” was also considered as the underlying mechanism of a death due to ketoacidosis, even though an AB-CHMINACA-induced hyperglycemia was also possible (37).
A behavioral contribution of SCRAs to the death appears to be an additional source of concern. Anxiety and psychosis might be also explained by the affinity of SCRAs to dopaminergic (D2), serotoninergic (5-HT2A) or glutamatergic (NMDA) receptors (76, 77). In a case described by Labay et al. (33), the victim fell from a high building after feeling sick and vomiting several times and was found intoxicated with MDEA, MDA, and JWH-175. While psychiatric consequences of SCRAs intake are clear in the absence of other drugs (41), the evaluation of role in polydrug consumption is puzzling, as in the case of low levels of both SCRAs and phenytoin, which can induce psychosis (78). Data on toxic/fatal levels might lack for NPS (e.g., for co-consumption of pentedrone resulting in behavioral abnormalities) (26) and even therapeutic or negligible levels of common drugs of abuse could assume relevance in combination with SCRAs. The influence of SCRAs on non-cannabinoid receptors and on serotonin, dopamine, catecholamine levels further complicate potential interpretations. In such cases of polydrug abuse, it is possible that the death would not have occurred without SCRA consumption, although no direct causality can be established. A TSS of “1” (“i” indicating the indirect role) is suggested due to the presence of multiple drugs with unknown contributory role, despite behavioral toxicity being an important risk factor for fatal outcome (33).
On the other hand, in the first case reported by Rojek et al. (26), the victim jumped from a building after a reported “loss of control” and no other drug was detected. Thus, notwithstanding the behavioral toxicity and the indirect mechanism, a contribution to death is likely (TSS of “3” was assigned).
Finally, cases of acute liver and/or kidney failure have been described (40, 55).
In general, if only toxicological results are listed in the absence of macroscopical and microscopical data, uncertainties regarding the role of the substance increase, as in the case reported by Kusano et al. (23). However, the mechanism of death could remain unclear, despite having a more complete data set (40) and the agreement between independent reviewers judging the very same pieces of information could be weak (e.g., unanimous agreement in 2 cases out of 25 submitted to multiple evaluations) (33, 40). Thus, a multidisciplinary evaluation should be recommended for each case, in order to possibly limit such uncertainties.
Most of the publications identified a possible contributory role of SCRAs, even in the absence of findings clearly pointing towards a drug-related death (32, 34, 39, 45, 48). In the present review, a TSS of 3 was assigned when no competitive cause was seen, and the hypothesized mechanism of death was in line with the most frequently reported SCRA toxicities. Affinity and activity of new compounds are often unknown, and unexpectedly severe or idiosyncratic effects may occur (19). Given the uncertainty regarding toxic levels and toxic effects, even when the mechanism of death remains unclear and/or other substances might have played role, the possibility of a contribution of SCRAs should not be ignored, and a TSS of “2” justified.
The likelihood of a high significance score is greater when multiple compounds with potentially synergic effects are detected, despite low concentrations of each single compound (19).
On the contrary, even though SCRAs could exacerbate an intoxication due to alcohol or other drugs, in cases with relatively very low SCRA concentrations or with concentrations of the competitive drug above the toxic threshold, a TSS of “1” is suggested. This does not necessarily mean that the SCRA has not exerted any negative effect, and the stability of the analyte of interest should further be considered as a cause of low concentrations.
TSS was rated “U” in cases with lack of sufficient data, as for example in the case described by Langford and Bolton (20), where high alcohol concentrations were retrieved, and no quantification of SCRAs was possible, or in the case of Minakata et al. (25) and Kusano et al. (23), where the effects of the other substance detected was difficult to assess.
Limitations
There are several limitations in this study. First of all, despite the extensive research involving multiple databases, the process of inferring scientific evidence is strongly limited by the possibility of under-reporting of similar cases and by the necessity of establishing a temporal limit for the review. Thus, the information presented have to be regarded as incomplete. Secondly, no weighting of selected articles regarding their quality was undertaken. A third significant limitation resides in establishing the TSS (16) of the selected cases, since the TSS is so far a non-validated scale. However, given the lack of criteria for establishing the role of substance(s) in death cases, the TSS appeared to be a flexible and easy-to-use tool to assign a contributory weight to SCRAs, and thus to evaluate and compare different cases. In order to avoid misinterpretations and to appreciate the point of view of the authors of the manuscripts, in each death case the role of the substance was also supplied in their own words. Finally, only death cases in which at least one SCRA was analytically confirmed, and in which an autopsy was presumably performed, were included. The authors are aware that this could have resulted in a partial loss of information, but on the other hand our aim was to possibly achieve a higher level of evidence.
Conclusions
Several mechanisms could lead to death after SCRAs consumption, and behavioral risks as well as cardiovascular effects or central nervous system depression appear to play important roles. Given the limited pharmacodynamic and pharmacokinetic data and the overlap between fatal and non-fatal concentrations, typical toxic ranges for SCRAs have not been identified so far. The results of toxicological analyses should be interpreted with caution, considering the many confounding and influencing factors, particularly regarding the reliability of LC-MS/MS methods validated insufficiently or validated only in serum. Furthermore, pattern of consumption (e.g., occasional v. chronic) and tolerance of the subject should be estimated or evaluated on a case by case basis.
A complete and accurate post-mortem examination is a fundamental part in the evaluation of death cases involving SCRAs, since a comprehensive and multi-disciplinary evaluation of clinical, circumstantial, toxicological, and autoptic data is the only possibility to assess the toxicological significance of a substance and to tentatively identify a plausible mechanism of death, which could remain unclear despite an in-depth analysis of all data available.
Author Contributions
All authors materially participated in the article preparation and have approved the final article.
Funding
Role of funding source: The study was supported by Presidency of the Ministers Council, Department of Antidrug Policy.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Atwood BK, Huffman J, Straiker A, Mackie K. JWH018, a common constituent of ‘Spice' herbal blends, is a potent and efficacious cannabinoid CB1 receptor agonist. Br J Pharmacol (2010) 160(3):585–93. doi: 10.1111/j.1476-5381.2009.00582.x
2. Fantegrossi WE, Moran JH, Radominska-Pandya A, Prather PL. Distinct pharmacology and metabolism of K2 synthetic cannabinoids compared to Δ(9)-THC: mechanism underlying greater toxicity? Life Sci (2014) 97:45–54. doi: 10.1016/j.lfs.2013.09.017
3. Auwärter V, Dresen S, Weinmann W, Müller M, Pütz M, Ferreirós N. ‘Spice' and other herbal blends: harmless incense or cannabinoid designer drugs? J Mass. Spectrom. (2009) 44:832–7. doi: 10.1002/jms.1558
4. Uchiyama N, Kikura-Hanajiri R, Kawahara N, Goda Y. Identification of a cannabimimetic indole as a designer drug in a herbal product. Forensic Toxicol (2009) 27:61–6. doi: 10.1007/s11419-009-0069-y
5. EMCDDA. European Drug Report 2019: Trends and Developments. Publications Office of the European Union, Luxembourg. Available from: http://www.emcdda.europa.eu/system/files/publications/11364/20191724_TDAT19001ENNPDF.pdf.
6. Huffman JW, Dai D, Martin BR, Compton DR. Design, synthesis and pharmacology of cannabimimetic indoles. Bioorg Med Chem Lett (1994) 4:563–6. doi: 10.1016/S0960-894X(01)80155-4
7. Kasper AM, Ridpath AD, Gerona RR, Cox R, Galli R, Kyle PB, et al. Severe illness associated with reported use of synthetic cannabinoids: a public health investigation (Mississippi, 2015). Clin Toxicol (Phila) (2015) 57:10–8. doi: 10.1080/15563650.2018.1485927
8. Adams AJ, Banister SD, Irizarry L, Trecki J, Schwartz M, Gerona R. “Zombie” outbreak caused by the synthetic cannabinoid AMB-FUBINACA in New York. New Engl J Med (2017) 376:235–42. doi: 10.1056/nejmoa1610300
9. Hermanns-Clausen M, Kneisel S, Szabo B, Auwärter V. Acute toxicity due to the confirmed consumption of synthetic cannabinoids: clinical and laboratory findings. Addiction. (2013) 108:534–44. doi: 10.1111/j.1360-0443.2012.04078.x
10. Barceló B, Pichini S, López-Corominas V, Gomila I, Yates C, Busardò FP, et al. Acute intoxication caused by synthetic cannabinoids 5F-ADB and MMB-2201: A case series. Forensic Sci Int (2017) 273:e10–4. doi: 10.1016/j.forsciint.2017.01.020
11. Cooper ZD. Adverse effects of synthetic cannabinoids: management of acute toxicity and withdrawal. Curr Psychiatry Rep (2016) 18:52. doi: 10.1007/s11920-016-0694-1
12. Solimini R, Busardò FP, Rotolo MC, Ricci S, Mastrobattista L, Mortali C, et al. Hepatotoxicity associated to synthetic cannabinoids use. Eur Rev Med Pharmacol Sci (2017) 21:1–6.
13. Pertwee RG, Howlett AC, Abood ME, Alexander SPH, Di Marzo V, Elphick MR, et al. International union of basic and clinical pharmacology. LXXIX. Cannabinoid receptors and their ligands: beyond CB1 and CB2. Pharmacol Rev (2010) 62(4):588–631. doi: 10.1124/pr.110.003004
14. Hermanns-Clausen M, Müller D, Kithinji J, Angerer V, Franz F, Eyer F, et al. Acute side effects after consumption of the new synthetic cannabinoids AB-CHMINACA and MDMB-CHMICA. Clin Toxicol (Phila) (2017) 56:404–11. doi: 10.1080/15563650.2017.1393082
15. Halter S, Angerer V, Röhrich J, Groth O, Roider G, Hermanns-Clausen M, et al. Cumyl-PEGACLONE: a comparatively safe new synthetic cannabinoid receptor agonist entering the NPS market? Drug Test Anal (2019) 11:347–9. doi: 10.1002/dta.2545
16. Kronstrand R, Guerrieri D, Vikingsson S, Wohlfarth A, Gréen H. Fatal poisonings associated with new psychoactive substances. Handb Exp Pharmacol (2018) 252:495–541. doi: 10.1007/164_2018_110
17. Elliott S, Sedefov R, Evans-Brown M. Assessing the toxicological significance of new psychoactive substances in fatalities. Drug Test Anal (2018) 10:120–6. doi: 10.1002/dta.2225
18. Welter-Luedeke J, Maurer HH. Relevance of published blood concentrations of new psychoactive substance for rational case interpretation. WIREs Forensic Sci (2019) 1:e1174. doi: 10.1002/wfs2.1174
19. Yamagishi I, Minakata K, Nozawa H, Hasegawa K, Suzuki M, Kitamoto T, et al. A case of intoxication with a mixture of synthetic cannabinoids EAM-2201, AB-PINACA and AB-FUBINACA, and a synthetic cathinone α-PVP. Leg Med (Tokyo) (2018) 35:44–9. doi: 10.1016/j.legalmed.2018.08.004
20. Langford AM, Bolton JR. Synthetic cannabinoids: variety is definitely not the spice of life. J. Forensic Leg Med (2018) 59:36–8. doi: 10.1016/j.jflm.2018.07.012
21. Paul ABM, Simms L, Amini S, Paul AE. Teens and Spice: a review of adolescent fatalities associated with synthetic cannabinoid use. J Forensic Sci (2018) 63:1321–4. doi: 10.1111/1556-4029.13704
22. Hasegawa K, Minakata K, Gonmori K, Nozawa H, Yamagishi I, Watanabe K, et al. Identification and quantification of predominant metabolites of synthetic cannabinoid MAB-CHMINACA in an authentic human urine specimen. Drug Test Anal (2018) 10:365–71. doi: 10.1002/dta.2220
23. Kusano M, Zaitsu K, Taki K, Hisatsune K, Nakajima J, Moriyasu T, et al. Fatal intoxication by 5F–ADB and diphenidine: detection, quantification, and investigation of their main metabolic pathways in humans by LC/MS/MS and LC/Q-TOFMS. Drug Test Anal (2018) 10:284–93. doi: 10.1002/dta.2215
24. Gaunitz F, Lehmann S, Thomas A, Thevis M, Rothschild MA, Mercer-Chalmers-Bender K. Post-mortem distribution of the synthetic cannabinoid MDMB-CHMICA and its metabolites in a case of combined drug intoxication. Int J Leg Med (2018) 133:973. doi: 10.1007/s00414-018-1976-4
25. Minakata K, Yamagishi I, Nozawa H, Hasegawa K, Suzuki M, Gonmori K, et al. Sensitive identification and quantitation of parent forms of six synthetic cannabinoids in urine samples of human cadavers by liquid chromatography–tandem mass spectrometry. Forensic Toxicol (2017) 35:275–83. doi: 10.1007/s11419-017-0354-0
26. Rojek S, Korczyńska-Albert M, Kulikowska J, Klys M. New challenges in toxicology of new psychoactive substances exemplified by fatal cases after UR-144 and UR-144 with pentedrone administration determined by LC-ESI-MS-MS in blood samples. Arch Med Sadowej Kryminol (2017) 67:104–20. doi: 10.5114/amsik.2017.71452
27. Angerer V, Jacobi S, Franz F, Auwärter V, Pietsch J. Three fatalities associated with the synthetic cannabinoids 5F-ADB, 5F-PB-22, and AB-CHMINACA. Forensic Sci Int (2017) 281:e9–e15. doi: 10.1016/j.forsciint.2017.10.042
28. Hasegawa K, Wurita A, Minakata K, Gonmori K, Yamagishi I, Nozawa H, et al. Identification and quantitation of 5-fluoro-ADB, one of the most dangerous synthetic cannabinoids, in the stomach contents and solid tissues of a human cadaver and in some herbal products. Forensic Toxicol (2015a) 33:112–21. doi: 10.1007/s11419-014-0259-0
29. Hasegawa K, Wurita A, Minakata K, Gonmori K, Nozawa H, Yamagishi I, et al. Postmortem distribution of MAB-CHMINACA in body fluids and solid tissues of a human cadaver. Forensic Toxicol (2015b) 33:380–7. doi: 10.1007/s11419-015-0272-y
30. Hasegawa K, Wurita A, Minakata K, Gonmori K, Nozawa H, Yamagishi I, et al. Postmortem distribution of AB-CHMINACA, 5-fluoro-AMB, and diphenidine in body fluids and solid tissues in a fatal poisoning case: usefulness of adipose tissue for detection of the drugs in unchanged forms. Forensic Toxicol (2015c) 33:45–53. doi: 10.1007/s11419-014-0245-6
31. Gieron J, Adamowicz P. Fatal poisoning with the synthetic cannabinoid AB-CHMINACA and ethyl alcohol – A case study and literature review. Z Zagadnien Nauk Sadowych (2017) 106:482–95.
32. Shanks KG, Behonick GS. Death after use of the synthetic cannabinoid 5F-AMB. Forensic Sci Int (2016) 262:e21–4. doi: 10.1016/j.forsciint.2016.03.004
33. Labay LM, Caruso JL, Gilson TP, Phipps RJ, Knight LD, Lemos NP, et al. Synthetic cannabinoid drug use as a cause or contributory cause of death. Forensic Sci Int (2016) 260:31–9. doi: 10.1016/j.forsciint.2015.12.046
34. Shanks KG, Winston D, Heidingsfelder J, Behonick G. Case reports of synthetic cannabinoid XLR-11 associated fatalities. Forensic Sci Int (2015) 252:e6–9. doi: 10.1016/j.forsciint.2015.04.021
35. Fujita Y, Koeda A, Fujino Y, Onodera M, Kikuchi S, Niitsu H, et al. Clinical and toxicological findings of acute intoxication with synthetic cannabinoids and cathinones. Acute Med Surg (2016) 3:230–6. doi: 10.1002/ams2.182
36. Adamowicz P. Fatal intoxication with synthetic cannabinoid MDMB-CHMICA. Forensic Sci Int (2016) 261:e5–e10. doi: 10.1016/j.forsciint.2016.02.024
37. Hess C, Stockhausen S, Kernbach-Wighton G, Madea B. Death due to diabetic ketoacidosis: Induction by the consumption of synthetic cannabinoids? Forensic Sci Int (2015) 257:e6–e11. doi: 10.1016/j.forsciint.2015.08.012
38. Zaitsu K, Nakayama H, Yamanaka M, Hisatsune K, Taki K, Asano T, et al. High-resolution mass spectrometric determination of the synthetic cannabinoids MAM-2201, AM-2201, AM-2232, and their metabolites in postmortem plasma and urine by LC/Q-TOFMS. Int J Legal Med (2015) 129:1233–45. doi: 10.1007/s00414-015-1294-z
39. Gerostamoulos D, Drummer OH, Woodford NW. Deaths linked to synthetic cannabinoids. Forensic Sci Med Pathol (2015) 11:478. doi: 10.1007/s12024-015-9669-5
40. Behonick G, Shanks KG, Firchau DJ, Mathur G, Lynch CF, Nashelsky M, et al. Four postmortem case reports with quantitative detection of the synthetic cannabinoid, 5F-PB-22. J Anal Toxicol (2014) 38:559–62. doi: 10.1093/jat/bku048
41. Patton AL, Chimalakonda KC, Moran CL, McCain KR, Radominska-Pandya A, James LP, et al. K2 toxicity: fatal case of psychiatric complications following AM2201 exposure. J Forensic Sci (2013) 58:1676–80. doi: 10.1111/1556-4029.12216
42. Wikström M, Thelander G, Dahlgren M, Kronstrand R. An accidental fatal intoxication with methoxetamine. J Anal Toxicol (2013) 37:43–6. doi: 10.1093/jat/bks086
43. Shanks KG, Dahn T, Terrell AR. Detection of JWH-018 and JWH-073 by UPLC–MS-MS in postmortem whole blood casework. J Anal Toxicol (2012) 36:145–52. doi: 10.1093/jat/bks013
44. Saito T, Namera A, Miura N, Ohta S, Miyazaki S, Osawa M, et al. A fatal case of MAM-2201 poisoning. Forensic Toxicol (2013) 31:333–7. doi: 10.1007/s11419-013-0190-9
45. Sasaki C, Saito T, Shinozuka T, Irie W, Murakami C, Maeda K, et al. A case of death caused by abuse of a synthetic cannabinoid N-1-naphthalenyl-1-pentyl-1H-indole-3-carboxamide. Forensic Toxicol (2015) 33:165–9. doi: 10.1007/s11419-014-0246-5
46. Schaefer S, Peters B, Bregel D, Kneisel S, Auwärter V, Schmidt PH, et al. A fatal case involving several synthetic cannabinoids. Toxichem Krimtech (2013) 80:248–51.
47. Kubo SI, Waters B, Hara K, Fukunaga T, Ikematsu K. A report of novel psychoactive substances in forensic autopsy cases and a review of fatal cases in the literature. Leg Med (Tokyo) (2017) 26:79–85. doi: 10.1016/j.legalmed.2017.03.008
48. Westin AA, Frost J, Brede WR, Gundersen PO, Einvik S, Aarset H, et al. Sudden cardiac death following use of the synthetic cannabinoid MDMB-CHMICA. J Anal Toxicol (2016) 40:86–7. doi: 10.1093/jat/bkv110
49. Seywright A, Torrance HJ, Wylie FM, McKeown DA, Lowe DJ, Stevenson R. Analysis and clinical findings of cases positive for the novel synthetic cannabinoid receptor agonist MDMB-CHMICA. Clin Toxicol (Phila) (2016) 54:632–7. doi: 10.1080/15563650.2016.1186805
50. Usui K, Fujita Y, Kamijo Y, Kokaji T, Funayama M. Identification of 5-Fluoro ADB in human whole blood in four death cases. J Anal Toxicol (2018) 42:e21–5. doi: 10.1093/jat/bkx088
51. Shanks KG, Clark W, Behonick G. Death associated with the use of the synthetic cannabinoid ADB-FUBINACA. J Anal Toxicol (2016) 40:236–9. doi: 10.1093/jat/bkv142
52. Kronstrand R, Roman M, Andersson M, Eklund A. Toxicological findings of synthetic cannabinoids in recreational users. J Anal Toxicol (2013) 37:534–41. doi: 10.1093/jat/bkt068
53. Reidy L, Seither J, Boland D. Identification of synthetic cannabinoid 5-Fluoro-ADB in human performance and postmortem case samples: a case series. J Forensic Toxicol Pharmacol (2018) 7:2. doi: 10.4172/2325-9841.1000162
54. White CM. The pharmacologic and clinical effects of illicit synthetic cannabinoids. J Clin Pharmacol (2017) 57:297–304. doi: 10.1002/jcph.827
55. Trecki J, Gerona RR, Schwartz MD. Synthetic cannabinoid-related illnesses and deaths. N Engl J Med (2015) 373:103–7. doi: 10.1056/NEJMp1505328
56. Angerer V, Florian F, Moosmann B, Bisel P, Auwärter V. 5-F-Cumyl-PINACA in “e-liquids” for electronic cigarettes: comprehensive characterization of a new type of synthetic cannabinoid in a trendy product including investigations on the in vitro and in vivo phase I metabolism of 5F-Cumyl-PINACA and its non-fluorinated analog Cumyl-PINACA. Forensic Toxicol (2015) 37:186–96. doi: 10.1007/s11419-018-0451-8
57. Lefever TW, Marusich JA, Thomas BF, Barrus DG, Peiper NC, Kevin RC, et al. Vaping synthetic cannabinoids: a novel preclinical model of e-cigarette use in mice. Subst Abuse (2017) 11:1178221817701739. doi: 10.1177/1178221817701739
58. Giorgetti A, Mogler L, Halter S, Haschimi B, Alt A, Rentsch D, et al. Four cases of death involving the novel synthetic cannabinoid 5F-Cumyl-PEGACLONE. Forensic Toxicol (2019). doi: 10.1007/s11419-019-00514-w
59. Peters FT, Drummer OH, Musshoff F. Validation of new methods. Forensic Sci Int (2007) 165:216–24. doi: 10.1016/j.forsciint.2006.05.021
60. Moriya F, Hashimoto Y. Redistribution of basic drugs into cardiac blood from surrounding tissues during early-stages postmortem. J Forensic Sci (1999) 44:10–6. doi: 10.1520/jfs14405j
61. Angerer V, Franz F, Schwarze B, Moosmann B, Auwärter V. Reply to “Sudden cardiac death following use of the synthetic cannabinoid MDMB-CHMICA”. J Anal Toxicol (2016) 40:240–2. doi: 10.1093/jat/bkw004
62. Arepally GM, Ortel TL. Bad weed: synthetic cannabinoid–associated coagulopathy. Blood (2019) 133:902–5. doi: 10.1182/blood-2018-11-876839
63. Kelkar AH, Smith NA, Martial A, Moole H, Tarantino MD, Roberts JC. An outbreak of synthetic cannabinoid–associated coagulopathy in Illinois. New Engl J Med (2018) 379:1216–23. doi: 10.1056/NEJMoa1807652
64. Tse R, Kodur S, Squires B, Collins N. Sudden cardiac death complicating acute myocardial infarction following synthetic cannabinoid use. Intern Med J (2014) 44:934–6. doi: 10.1111/imj.12521
65. Ibrahim S, Al-Saffar F, Wannenburg T. A unique case of cardiac arrest following K2 abuse. Case Rep Cardiol (2014) 2014:120607. doi: 10.1155/2014/120607
66. Mir A, Obafemi A, Young A, Kane C. Myocardial infarction associated with use of the synthetic cannabinoid K2. Pediatrics (2011) 128:e1622–7. doi: 10.1542/peds.2010-3823
67. Davis C, Boddington D. Teenage cardiac arrest following abuse of synthetic cannabis. Hear Lung Circ (2015) 24:e162–3. doi: 10.1016/j.hlc.2015.04.176
68. Pacher P, Steffens S, Haskó G, Schindler TH, Kunos G. Cardiovascular effects of marijuana and synthetic cannabinoids: the good, the bad, and the ugly. Nat Rev Cardiol (2018) 15:151–66. doi: 10.1038/nrcardio.2017.130
69. Hoyte CO, Jacob J, Monte AA, Al-Jumaan M, Bronstein AC. Heard KJ. A characterization of synthetic cannabinoid exposures reported to the National Poison Data System in 2010. Ann Emerg Med (2012) 60:435–8. doi: 10.1016/j.annemergmed.2012.03.007
70. Aryana A, Williams MA. Marijuana as a trigger of cardiovascular events: speculation or scientific certainty? Int J Cardiol (2007) 118:141–4. doi: 10.1016/j.ijcard.2006.08.001
71. Alshaarawy O, Elbaz HA. Cannabis use and blood pressure levels: United States National Health and Nutrition Examination Survey, 2005-2012. J Hypertens (2016) 34(8):1507–12. doi: 10.1097/HJH.0000000000000990
72. Vidot DC, Powers M, Gonzalez R, Jayaweera DT, Roy S, Dong C, et al. Blood pressure and marijuana use: results from a decade of NHANES data. Am J Health Behav (2019) 43(5):887–97. doi: 10.5993/AJHB.43.5.2
73. Schindler CW, Gramling BR, Justinova Z, Thorndike EB, Baumann MH. Synthetic cannabinoids found in “spice” products alter body temperature and cardiovascular parameters in conscious male rats. Drug Alcohol Depend (2017) 179:387–94. doi: 10.1016/j.drugalcdep.2017.07.029
74. Rodriguez JS, McMahon LR. JWH-018 in rhesus monkeys: differential antagonism of discriminative stimulus, rate-decreasing, and hypothermic effects. Eur J Pharmacol (2014) 740:151–9. doi: 10.1016/j.ejphar.2014.06.023
75. Nava F, Carta G, Gessa GL. Permissive role of dopamine D(2) receptors in the hypothermia induced by delta(9)-tetrahydrocannabinol in rats. Pharmacol Biochem Behav (2000) 66(1):183–7. doi: 10.1038/sj.bjp.0703413
76. Castaneto MS, Gorelick DA, Desrosiers NA, Hartman RL, Pirard S, Huestis MA. Synthetic cannabinoids: epidemiology, pharmacodynamics, and clinical implications. Drug Alcohol Depend (2014) 144:12–41. doi: 10.1016/j.drugalcdep.2014.08.005
77. Fantegrossi WE, Wilson CD, Berquist MD. Pro-psychotic effects of synthetic cannabinoids: interactions with central dopamine, serotonin, and glutamate systems. Drug Metab Rev (2018) 50(1):65–73. doi: 10.1080/03602532.2018.1428343
Keywords: forensic toxicology, novel psychoactive substances, synthetic cannabinoids, post-mortem examination, toxicological significance score
Citation: Giorgetti A, Busardò FP, Tittarelli R, Auwärter V and Giorgetti R (2020) Post-Mortem Toxicology: A Systematic Review of Death Cases Involving Synthetic Cannabinoid Receptor Agonists. Front. Psychiatry 11:464. doi: 10.3389/fpsyt.2020.00464
Received: 08 January 2020; Accepted: 06 May 2020;
Published: 25 May 2020.
Edited by:
Marc N. Potenza, Yale University, United StatesReviewed by:
John Martin Corkery, University of Hertfordshire, United KingdomFabrizio Schifano, University of Hertfordshire, United Kingdom
Copyright © 2020 Giorgetti, Busardò, Tittarelli, Auwärter and Giorgetti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Paolo Busardò, ZnJhLmJ1c2FyZG9AbGliZXJvLml0