 Michele Fornaro1,2*
Michele Fornaro1,2* Andrea Fusco1
Andrea Fusco1 Stefano Novello1Pierluigi Mosca1
Stefano Novello1Pierluigi Mosca1 Annalisa Anastasia2Antonella De Blasio1Felice Iasevoli1
Annalisa Anastasia2Antonella De Blasio1Felice Iasevoli1 Andrea de Bartolomeis1
Andrea de Bartolomeis1- 1Laboratory of Molecular and Translational Psychiatry, Unit of Treatment-Resistant Psychosis, Section of Psychiatry, University of Naples Federico II, Naples, Italy
- 2Polyedra Research Group, Teramo, Italy
Objective: Treatment-resistant depression (TRD) and treatment-resistant bipolar depression (TRBD) poses a significant clinical and societal burden, relying on different operational definitions and treatment approaches. The detection of clinical predictors of resistance is elusive, soliciting clinical subtyping of the depressive episodes, which represents the goal of the present study.
Methods: A hundred and thirty-one depressed outpatients underwent psychopathological evaluation using major rating tools, including the Hamilton Rating Scale for Depression, which served for subsequent principal component analysis, followed-up by cluster analysis, with the ultimate goal to fetch different clinical subtypes of depression.
Results: The cluster analysis identified two clinically interpretable, yet distinctive, groups among 53 bipolar (resistant cases = 15, or 28.3%) and 78 unipolar (resistant cases = 20, or 25.6%) patients. Among the MDD patients, cluster “1” included the following components: “Psychic symptoms, depressed mood, suicide, guilty, insomnia” and “genitourinary, gastrointestinal, weight loss, insight”. Altogether, with broadly defined “mixed features,” this latter cluster correctly predicted treatment outcome in 80.8% cases of MDD. The same “broadly-defined” mixed features of depression (namely, the standard Diagnostic and Statistical Manual for Mental Disorders, Fifth Edition—DSM-5—specifier plus increased energy, psychomotor activity, irritability) correctly classified 71.7% of BD cases, either as TRBD or not.
Limitations: Small sample size and high rate of comorbidity.
Conclusions: Although relying on different operational criteria and treatment history, TRD and TRBD seem to be consistently predicted by broadly defined mixed features among different clinical subtypes of depression, either unipolar or bipolar cases. If replicated by upcoming studies to encompass also biological and neuropsychological measures, the present study may aid in precision medicine and informed pharmacotherapy.
Introduction
Almost half of the patients suffering from a major depressive episode (MDE) fail to achieve a response, despite sequential combination or augmentation treatment strategies, irrespective of the operational definition adopted for treatment-resistant depression (TRD) (1, 2). The rates of treatment-resistant bipolar depression (TRBD) within the course of bipolar disorder (BD) can even exceed those documented for major depressive disorder (MDD) and present a differential pattern of response to different medications, indeed (3). Both TRD (4) and TRBD (5, 6) pose a significant clinical and societal burden, soliciting the assessment of putative predictors using clinical, neuropsychological, neuroimaging, and genetic measures (7, 8). However, the general failure to find sensitive and specific predictors of treatment response in MDD and BD, either current- of future-state markers (9), is in part, due to the heterogeneity of these conditions, which range from biologically determined to event-dependent conditions (10). The initial hype about digital phenotyping has been tempered by increasing awareness of the significant technical and analytical difficulties hindering translational change (11, 12) most likely due to differential neurobiology underpinning MDD (13, 14) and BD (15–17). To date, no single biological marker stood-out in selecting the best initial antidepressant treatment for a given individual, despite promising evidence coming from recent pharmacogenomics studies (18). Clinical risk stratification models for TRD, incorporating baseline sociodemographic and clinical features (19), preceded algorithm-based approaches proposed for TRBD (20). For MDD, a cluster of variables including marital status, insomnia, psychosocial impact, trauma, education, energy, disorder recurrence, comorbidity, race, and severity of current MDE resulted in a positive predictive value of TRD =.61 and a negative predictive value =.69, consistently across males and females and primary- vs. specialty care settings (19). Over the past decade, findings from the Group for the Study of Resistant Depression (GSRD), a multinational European research consortium, pointed toward strong effects of clinical variables on treatment outcome of MDD (21), as well as specific genetic signature (22). This is particularly relevant considering that, when considered separately, the potential predictors of TRD usually showed odd ratios (ORs) around 1.5, and thus, were not applicable as univocal hints in the clinical setting (23, 24). Nonetheless, four potent clinical predictors of TRD emerged in a validation study that showed a collective predictive accuracy of 87%. These latter include symptom severity, suicidal risk, comorbid anxiety disorder, and the lifetime number of MDE episodes (25–27). Overall, symptom severity, suicidal risk, higher number of lifetime of MDEs, and comorbid anxiety disorder were consistently replicated as the most prominent risk factors for different stages of TRD in large-sampled studies (28).
Machine learning approaches may, however, further increase the detection of TRD (29, 30), as reinforced by the 2019 report by the GSRD study group for TRD (22).
Concerning BD, clinical predictors of “full clinical recovery” include outpatient treatment and more extended periods of lifetime mania (31). In contrast, higher baseline severity scores, presence of MDEs in the previous year, poor social functioning predict failure to achieve remission or recovery in BD (32). Among other clinical hallmarks, earlier (hypo-)manic or mixed recurrence, including sub-threshold manic symptoms and the proportion of days spent with an elevated mood in the preceding year, predict TRBD (33). The conceptualization of TRBD is more articulated than one of TRD, due to the differential natural and pharmacological course of BD and the controversial role of the antidepressants in BD (2). While drug resistance or worsening in MDD has been associated with mixed features and other bipolarity hints (34), relatively little is known about the impact of mixed features in bipolar depression and subsequence failure to respond. However, side-by-side comparisons of unipolar vs. bipolar MDEs relying on a relatively limited-range of retrospective data, suggesting that TDR represents a distinct psychopathological condition and not necessarily a prodromal state of BD (35).
The aim of the present exploratory-hypothesis generating study is to assess multiple clinical predictors of treatment resistance comparing unipolar vs. bipolar patients across different clinical subtypes of current MDE. To the best of our knowledge, the present data-driven study is the first of its kind to a side-by-side comparison of a range of putative clinical predictors of treatment resistance across different clinical subtypes of depression, either unipolar or bipolar major depression.
Methods
Participants
A hundred and thirty-one outpatients, both sexes, 18–65 years old, consecutively enrolled in a non-interventional study at a tertiary care unit of the Department of Psychiatry of the Federico II University of Naples, Italy, between May 3, 2017, and June 17, 2019. All patients met the Diagnostic and Statistical Manual for Mental Disorders, Fifth Edition (DSM-5) (36) criteria for a current MDE, either in the course of MDD or BD. Six experienced psychiatrists (MF, AF, SN, AA, ABl, PM) made the clinical diagnoses. Eligible patients signed a valid written informed consent after the study procedures had fully explained by the appointed principal investigator (MF). The protocol of the study was approved by the local I.R.B. on May 2nd, 2017, according to the 1964 Declaration of Helsinki and its subsequent amendments (37). Exclusion criteria were the lack of valid informed consent, untreated thyroid disease, schizophrenia, severe brain syndrome, or other organic conditions, potentially hampering the validity of the consent.
Evaluation Procedure and Operational Definitions
The participating outpatients were rated according to the Hamilton Rating Scale for Depression, 17-item version scale (HAM-D-17) (38), Young Mania Rating Scale (YMRS) (39), and Temperament Evaluation of Memphis, Pisa, Paris, and San Diego, 110-item version (TEMPS-110) (40). The following clinical variables were recorded: age, sex, duration of the untreated illness (DUI), family history for header MDD or BD, lifetime suicidal behavior, significant psychiatric and medical comorbidities, and essential current and lifetime psychiatric treatment. The DUI was defined as the “time interval between the first lifetime onset of symptoms of depression, not necessarily reaching the diagnostic threshed set by the DSM-5: at least five symptoms of depression, and the first adequate treatment” (41). TRD was defined as “failure of two or more consecutive trials with antidepressants” (2). TRBD was defined as a lack of response to treatment to at least two previously established treatments for bipolar depression (e.g., olanzapine/fluoxetine combination, brexpiprazole, cariprazine, quetiapine, aripiprazole). TRBD could, however, have been exposed to at least one mood stabilizer drug plus an antidepressant in case of the previous failure to “adequate” trials for acute bipolar depression, especially whenever such therapy had been started elsewhere before seeking our consultation or in the presence of significant comorbidities (e.g., anxiety or obsessive–compulsive disorders).
Finally, the mixed features of the current MDE reflected the DSM-5 specifier. Besides, the “overlapping” symptoms otherwise excluded by the DSM-5 for a DSM-5-defined MDE with mixed features, i.e., “irritability,” “distractibility,” “impulsivity,” “mood lability,” and “psychomotor agitation,” were nonetheless recorded given their clinical relevance (42).
Statistical Analysis
The statistical analysis was performed using IBM™ SPSS™ Statistics™ v.25.0.0 for Windows™ (43), adopting alpha.05, two-tailed. Non-parametric distributions were transformed as necessary. The interrater reliability for the analysis using Cohen's k statistics was ascertained for consistency issues. Descriptive statistics followed by principal component analysis (PCA) and by two-step cluster analysis were carried-out for MDD and BD patients, separately. Patients recorded as TRD or TRBD were considered as “cases”; those without a history of treatment resistance were deemed as “controls.” Oblique rotation solution (Promax) was performed by calculating the coefficient for each pair of variables, and multi-collinearity was excluded; coefficient ≤.3 were suppressed. We assumed the conservative loadings >.3 to be significant. The Kaiser–Meyer–Olkin measure of sampling adequacy resulted in.65, indicating an acceptable sample size, with Bartlett's test of sphericity scoring lower than.05. To determinate the component number, we considered only eigenvalues > 1. For readers' convenience, an eigenvalue of 1 would explain as much variance as the one explained by a single variable.
In plain, the PCA aimed to extract the psychopathological components captured by the HAM-D scale, while the cluster analysis carried aimed at discriminate the cases at study based on the PCA-fetched components. The generated clusters of depressions were compared against each other using descriptive statistics and binary logistic regression analysis.
Results
Demographic and Clinical Variables Across Different Clinical Subtypes of Depression
A summary of the essential clinical and demographic features of the included sample has been reported in Table 1. Essential current and lifetime pharmacological history are presented in Table 2, while Table 3 provides the core rating tools and predominant affective temperament. Among other clinical variables, mixed, anxious, and psychotic features of current MDE were statistically more frequent among BD patients compared to the MDD counterpart.
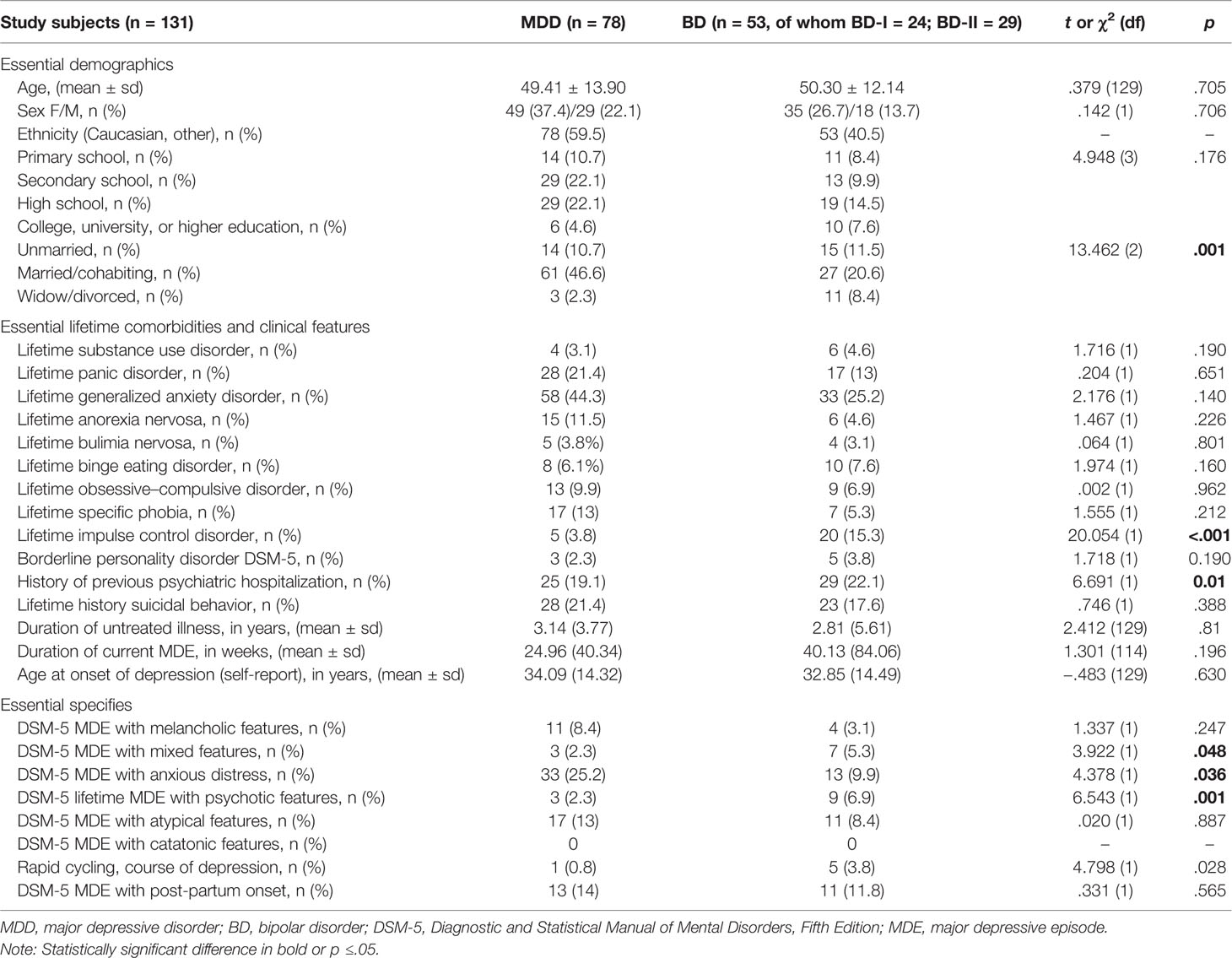
Table 1 Essential clinical and demographics across unipolar and bipolar cases.
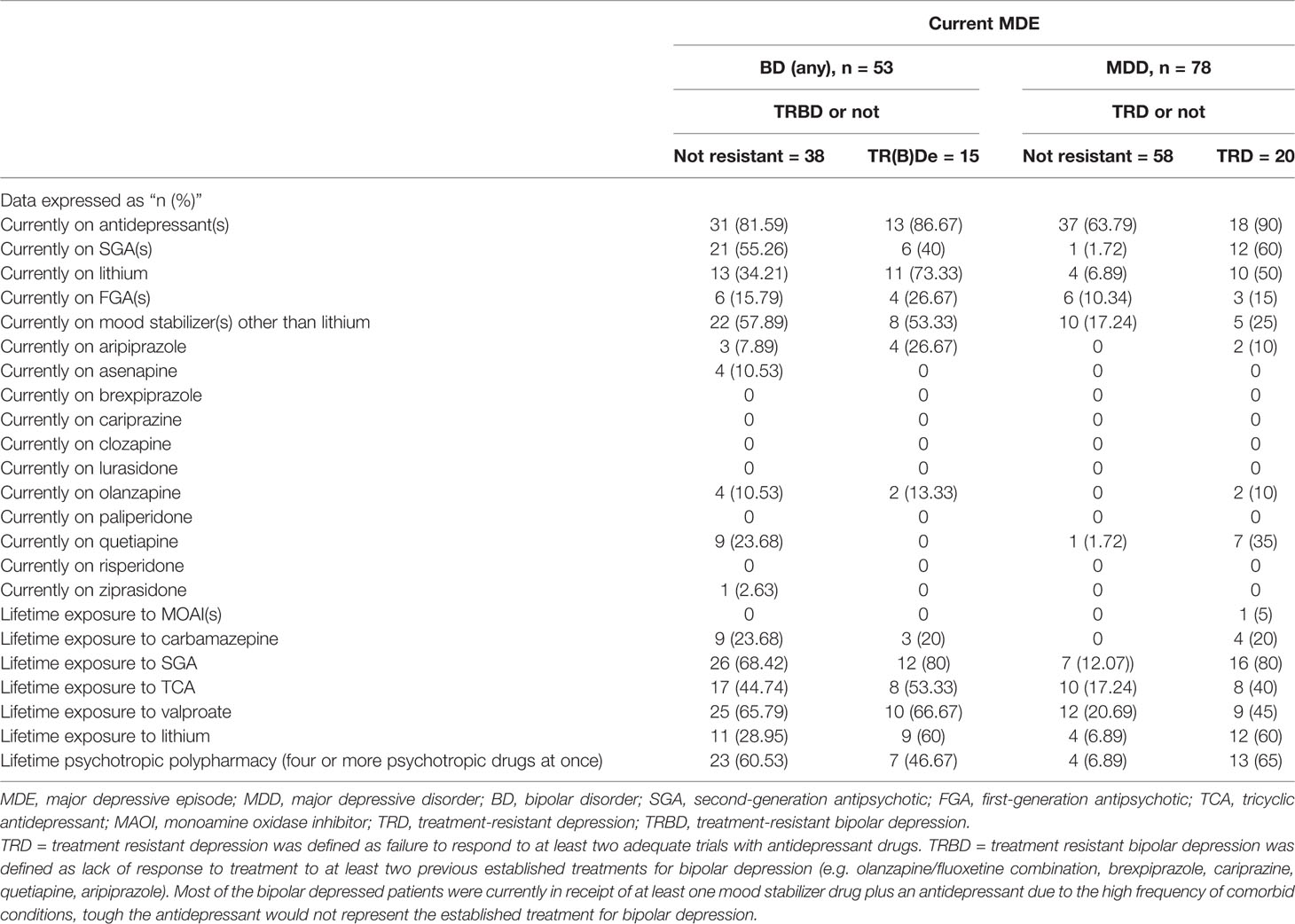
Table 2 Essential pharmacological treatment history across the included cases.
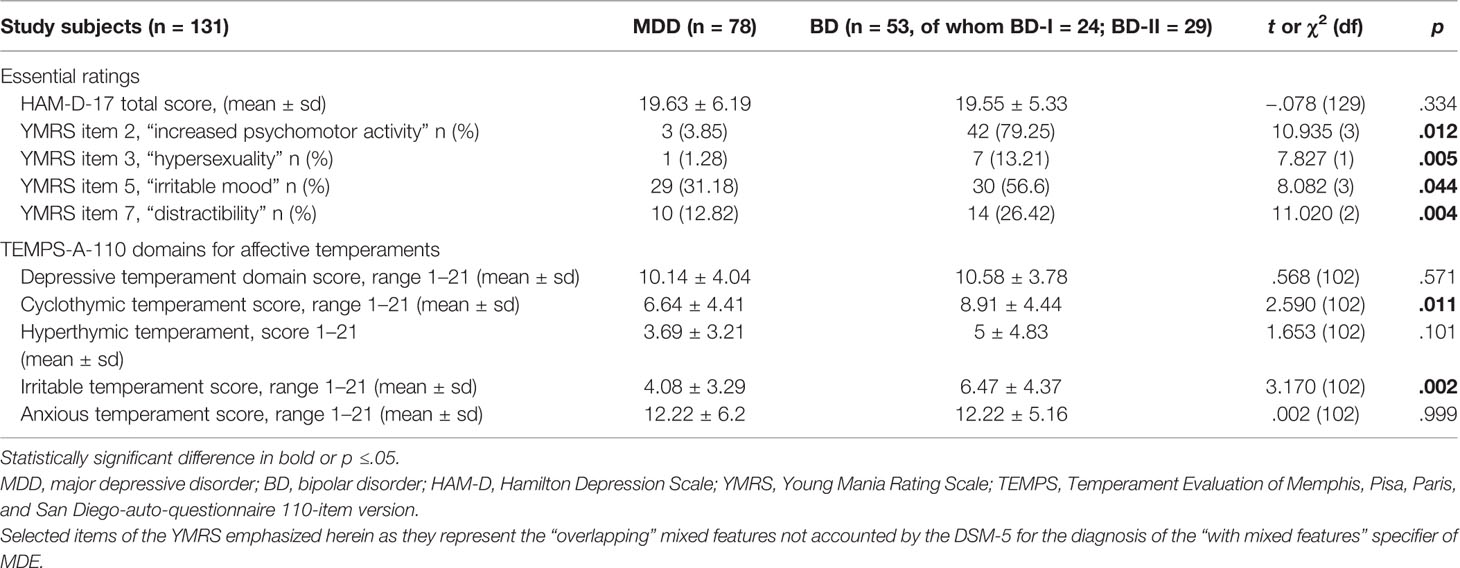
Table 3 Rating and temperamental profile of MDD and BD patients.
Principal Component and Cluster Analysis Statistics
PCA was performed on the items of the HAM-D-17 to characterize the sample at the report better, discriminating between unipolar and bipolar cases of depression. Two-step cluster analysis of cases based on the three components generated by the PCA led to two clinically interpretable clusters, both in the MDD (Table 4) and the BD (Table 5) group. Notably, the fetched clusters comprised different component-items from the original HAM-D scale across the BD and the MDD groups, as detailed in Tables 4 and 5, also reporting the proportion of resistant cases across different clusters, respectively.
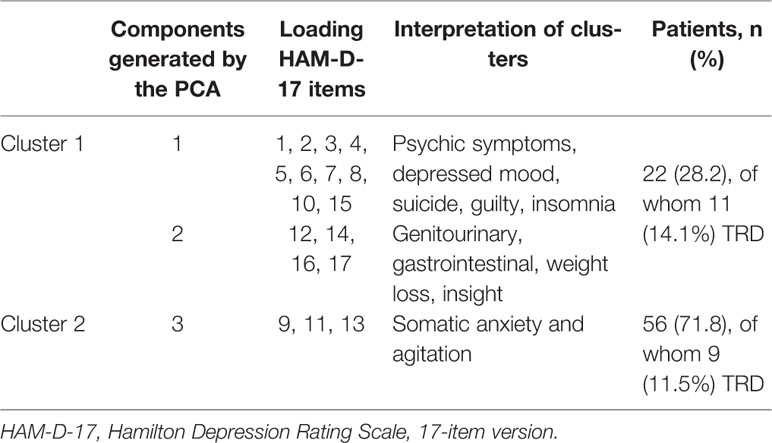
Table 4 Clusters and their characterization generated by two-step cluster analysis based on the three components obtained upon principal component analysis (PCA) on MDD patients.
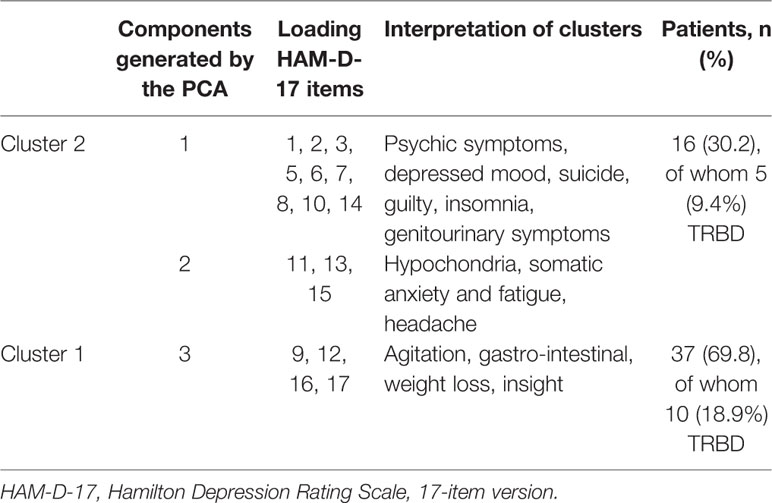
Table 5 Clusters and their characterization generated by two-step cluster analysis based on the three components obtained upon Principal Component Analysis (PCA) on BD patient.
Prediction of Treatment Resistance Based on Clinical Subtyping of Depression and Mixed Features Across Unipolar and Bipolar Clusters
Overall, the clinical subtypes of depression fetched by cluster analysis failed to allow a conclusive distinction between resistant vs. non-resistant cases (please refer to Tables 4 and 5 for details).
The presence of DSM-5-defined mixed features among MDD and BD cases was inversely related to the resistance outcome. In contrast, the presence of the “overlapping” symptoms of depression among MDD and BD—excluded by the DSM-5 specifiers of mixed depression—such as “distractibility,” “impulsivity,” “increased psychomotor activity,” and “hypersexuality,” predicted higher rates of treatment resistance, consistently in the MDD and the BD groups. Such “permissive” criteria for mixed depression, already outlined by the 1978 Research Diagnostic Criteria (44), consistently predicted treatment resistance both in the MDD and the BD groups even in the presence of different operational definitions and pharmacological courses differed between TRD and TRBD cases. Please refer to Table 6 for details. Finally, in the MDD group, the DSM-5 mixed features and the broadly defined mixed features were endorsed by 1.5% and 6.1% of cluster 1 patients, and 0.8% and 6.1% of cluster 2 patients, respectively. In the BD group, group the DSM-5 mixed features and the broadly defined mixed features were disclosed by 7.6% and 12.2% of cluster 1 patients, and 0.8% and 1.5% of cluster two patients, respectively.
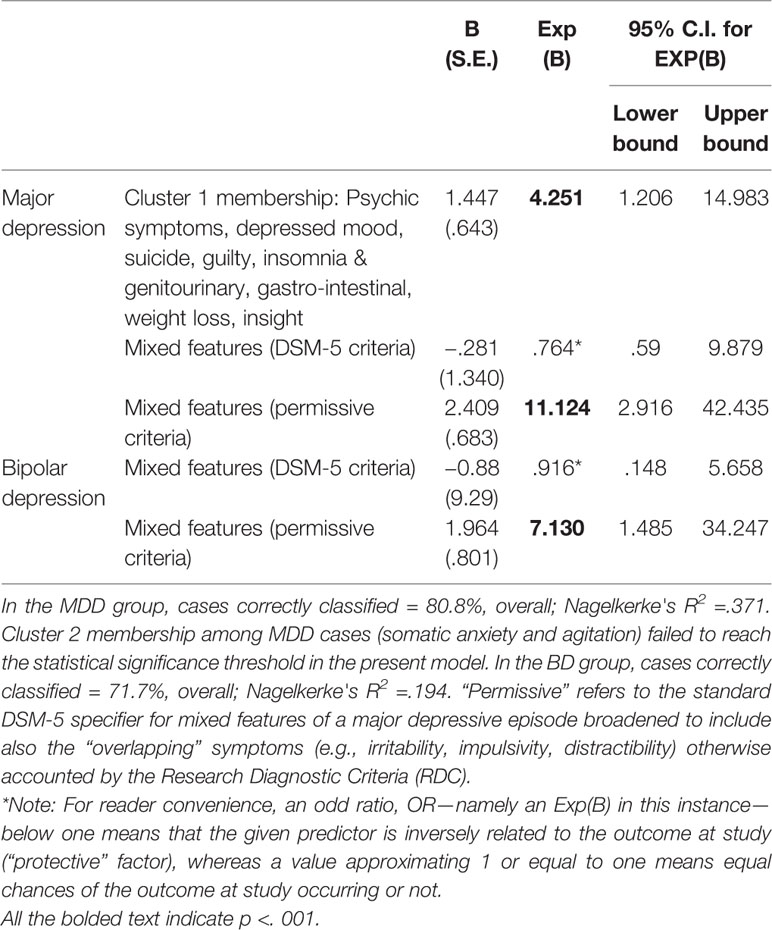
Table 6 Binary logistic regression, significant predictors only.
Discussion
Consistent with our hypothesis, the propensity toward TRD may vary across different clinical subtypes of depression. Cluster 1 membership among MDD cases, including the core depressive symptoms, psychomotor retardation, suicidal behavior (ideation or attempt), and somatic-anxiety (namely, gastrointestinal, indigestion, cardiovascular, palpitations, headaches, respiratory, and genitourinary symptoms), predicted TRD in half of such cases (14.1% of 28.2% of cluster 1 MDD patients). This is in line with previous evidence which, albeit failing to discriminate across different clinical subtypes of depression, highlighted the role of suicidal behavior—even those of mild to moderate intensity (27)—anxiety (25), and severity of the current MDE in the prediction of the treatment outcome (26, 28), as well as the impact of psychotic features of depression in the prediction of subsequent TRD (45). This is also in line with previous evidence involving patients diagnosed using the codes provided by the Fourth Edition of the Manual (DSM-IV) (46), yet failing to adopt a data-generated clustering of psychopathology (47). However, it must be noticed that the clustering had a poor predictive value overall in the MDD group and no significant predictive value for TRBD cases. Similarly, the affective temperaments measured by means of the TEMPS had no discriminative value for treatment resistance, neither in the MDD, neither in the BD subgroups, in line with previous reports comparing unipolar and bipolar cases (48).
On the other side, the present study highlights the impact of mixed features of depression, broadly defined to encompass also the not overlapping symptoms otherwise excluded by the DSM-5. Mixed features of depression were somewhat similar in terms of frequency among different data-generated subtypes of depression, in the MDD and the BD groups. Overall, mixed features consistently predicted treatment resistance among BD and MDD cases across different clinical subtypes of depression, especially when these latter included “excitement” symptoms among MDD patients. Indeed, mixed features of depression have been suggested to represent hallmarks of bipolarity among DSM-defined cases of BD, which may, on turn, be prone to treatment failure with standard MDD medications (49). In particular, MDD patients may require strategies other than the two “adequate” trials with antidepressants before receiving a diagnosis of treatment resistance in the presence of mixed features, especially when these latter encompass the “excitement” overlapping symptoms. In the MDD group, patients without broadly-defined mixed features, or DSM-5 defined mixed features of depression neither, may be more likely to respond to standard antidepressant care, thus endorsing lower rates of TRD. Stating the categorical nature of the operational definitions adopted by the present study for TRD or TRBD, it cannot be excluded, however, that the propensity for treatment resistance may span across a linear gradient ranging from almost neutral risk (OR =.916; C.I. =.148–5.658 in BD patients with narrowly-defined mixed features of depression) toward a 7-fold increased odd (OR = 7.130; C.I. = 1.485–34.247) in the BD group endorsing broadly-defined mixed features. Moreover, since the DSM-5-defined mixed features had negligible predictive value for treatment resistance, the use of the sole boundary-defined mixed features proposed by the DSM-5 itself may lead to improper pharmacological management of depression (50).
The categories proposed the DSM consist of “ideal types,” abstractions from reality, which we can use to assess empirical observations but which are not themselves, empirical facts. This latter concept, which is central to Jaspers' thinking in his textbook “General Psychopathology” (51), was derived from the work of Max Weber (52). While the ideal types may aid in discriminating depression from, say mania, the most common clinical presentations are an admixture of both conditions (53). From this perspective, we remark the relevance of the present study, although its preliminary nature solicits for additional research on the matter. However, more sensible operational definitions for TRD, especially in BD, are warranted (Fornaro M. et al., submitted for publication).
There several limitations of the present study, which was conducted in a tertiary care outpatient setting that needs to be accounted for in the interpretation of the results. The sample size is a relatively small one, with no longitudinal follow-up or systematic stratification of pharmacological history across different classes of antidepressants, titration modality. No stratification according to the predominant mood polarity or polarity index of BD was reported. Recall bias may have hampered the validity of some diagnoses, including general medical comorbidities (which may have nonetheless affected the propensity of treatment response). Specifically, those BD patients who were also in receipt of antidepressant(s) drugs beyond the mood stabilizer(s) need to be further stratified by upcoming studies in order to better account for several comorbidities (e.g., obsessive–compulsive disorder) that may have led to pseudo-resistance in some cases. However, per study-protocol, even those BD patients who were currently in receipt of antidepressant(s) at the time of the assessment had already failed at least two adequate courses with established treatments for acute bipolar depression (e.g., the atypical antipsychotic quetiapine, or the olanzapine/fluoxetine combination). Besides, there was no virtually no record of the psychosocial or neuro-modulatory interventions, any correlation measures with neither neuroimaging, molecular nor genetic marker. Yet, neuro-modulatory interventions such as electroconvulsive therapy represent consolidated treatment avenues for TRD (54). Besides, the psychopathological clustering of depression based entirely on the sole HAM-D, which may not be sufficient to catch the complexity of depression exhaustively.
However, stating the data-generating hypothesis of the present preliminary report, we further reinforce the need for upcoming studies to replicate the present results across different clinical subtypes of depression and a large number of putative biological and neuropsychological measures.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
Ethics Statement
The studies involving human participants were reviewed and approved by Federico II University of Naples. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MF and AF conceived the study and extensively edited the main-text and its attachments together with SN, ABl, AA, PM, FI, and ABa. Finally, all the co-authors contributed substantially to the present piece of work.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Malhi G, Parker G, Crawford J, Wilhelm K, Mitchell P. Treatment-resistant depression: resistant to definition? Acta Psychiatr Scand (2005) 112(4):302–9. doi: 10.1111/j.1600-0447.2005.00602.x
2. McIntyre RS, Filteau M-J, Martin L, Patry S, Carvalho A, Cha DS, et al. Treatment-resistant depression: definitions, review of the evidence, and algorithmic approach. J Affect Disord (2014) 156:1–7. doi: 10.1016/j.jad.2013.10.043
3. Hui Poon S, Sim K, Baldessarini RJ. Pharmacological approaches for treatment-resistant bipolar disorder. Curr Neuropharmacol (2015) 13: (5):592–604. doi: 10.2174/1570159X13666150630171954
4. Mrazek DA, Hornberger JC, Altar CA, Degtiar I. A review of the clinical, economic, and societal burden of treatment-resistant depression: 1996–2013. Psychiatr Serv (2014) 65(8):977–87. doi: 10.1176/appi.ps.201300059
5. Sylvia LG, Shelton RC, Kemp DE, Bernstein EE, Friedman ES, Brody BD, et al. Medical burden in bipolar disorder: findings from the Clinical and Health Outcomes Initiative in Comparative Effectiveness for Bipolar Disorder study (Bipolar CHOICE). Bipolar Disord (2015) 17(2):212–23. doi: 10.1111/bdi.12243
6. Greenberg PE, Birnbaum HG. The economic burden of depression in the US: societal and patient perspectives. Expert Opin Pharmacother (2005) 6(3):369–76. doi: 10.1517/14656566.6.3.369
7. Johnston KM, Powell LC, Anderson IM, Szabo S, Cline S. The burden of treatment-resistant depression: A systematic review of the economic and quality of life literature. J Affect Disord (2019) 242:195–210. doi: 10.1016/j.jad.2018.06.045
8. Kemp AH, Gordon E, Rush AJ, Williams LM. Improving the prediction of treatment response in depression: integration of clinical, cognitive, psychophysiological, neuroimaging, and genetic measures. CNS Spectrums (2008) 13: (12):1066–86. doi: 10.1017/S1092852900017120
9. Vergunst FK, Fekadu A, Wooderson SC, Tunnard CS, Rane LJ, Markopoulou K, et al. Longitudinal course of symptom severity and fluctuation in patients with treatment-resistant unipolar and bipolar depression. Psychiatry Res (2013) 207(3):143–9. doi: 10.1016/j.psychres.2013.03.022
10. Kim Y-K. Major Depressive Disorder: Current Advances and Paradigm Shifts. Psychiatry Invest (2020) 17(3):179–80. doi: 10.30773/pi.2019.0092
11. Sanches M, Quevedo J, Soares JC. Treatment Resistance in Bipolar Disorders. In: Treatment Resistance in Psychiatry. New York, USA (2019). p. 139–50.
12. Bennabi D, Aouizerate B, El-Hage W, Doumy O, Moliere F, Courtet, et al. Risk factors for treatment resistance in unipolar depression: a systematic review. J Affect Disord (2015) 171:137–41. doi: 10.1016/j.jad.2014.09.020
13. Coplan JD, Gopinath S, Abdallah CG, Berry BR. A neurobiological hypothesis of treatment-resistant depression–mechanisms for selective serotonin reuptake inhibitor non-efficacy. Front Behav Neurosci (2014) 8:189. doi: 10.3389/fnbeh.2014.00189
14. Caraci F, Calabrese F, Molteni R, Bartova L, Dold M, Leggio GM, et al. International union of basic and clinical pharmacology CIV: The neurobiology of treatment-resistant depression: From antidepressant classifications to novel pharmacological targets. Pharmacol Rev (2018) 70(3):475–504. doi: 10.1124/pr.117.014977
15. Muneer A. The neurobiology of bipolar disorder: an integrated approach. Chonnam Med J (2016) 52(1):18–37. doi: 10.4068/cmj.2016.52.1.18
16. Andreazza AC, Young LT. The neurobiology of bipolar disorder: identifying targets for specific agents and synergies for combination treatment. Int J Neuropsychopharmacol (2014) 17(7):1039–52. doi: 10.1017/S1461145713000096
17. Harrison PJ, Geddes JR, Tunbridge EM. The emerging neurobiology of bipolar disorder. Trends Neurosci (2018) 41(1):18–30. doi: 10.1016/j.tins.2017.10.006
18. Mrazek DA, Lerman CJJ. Facilitating clinical implementation of pharmacogenomics. JAMA (2011) 306: (3):304–5. doi: 10.1001/jama.2011.1010
19. Perlis RH. A clinical risk stratification tool for predicting treatment resistance in major depressive disorder. Biol Psychiatry (2013) 74(1):7–14. doi: 10.1016/j.biopsych.2012.12.007
20. Hidalgo-Mazzei D, Berk M, Cipriani A, Cleare AJ, Di Florio A, Dietch D, et al. Treatment-resistant and multi-therapy-resistant criteria for bipolar depression: consensus definition. Br J Psychiatry (2019) 214(1):27–35. doi: 10.1192/bjp.2018.257
21. Schosser A, Serretti A, Souery D, Mendlewicz J, Zohar J, Montgomery S, et al. European Group for the Study of Resistant Depression (GSRD)—where have we gone so far: review of clinical and genetic findings. Eur Neuropsychopharmacol (2012) 22(7):453–68. doi: 10.1016/j.euroneuro.2012.02.006
22. Bartova L, Dold M, Kautzky A, Fabbri C, Spies M, Serretti A, et al. Results of the European Group for the study of resistant depression (GSRD)—basis for further research and clinical practice. World J Biol Psychiatry (2019) 20(6):427–48. doi: 10.1080/15622975.2019.1635270
23. Souery D, Oswald, Massat I, Bailer U, Bollen J, Demyttenaere K, et al. Clinical factors associated with treatment resistance in major depressive disorder: results from a European multicenter study. J Clin Psychiatry (2007) 68(7):1062–70. doi: 10.4088/JCP.v68n0713
24. Gratten J, Wray NR, Keller MC, Visscher PM. Large-scale genomics unveils the genetic architecture of psychiatric disorders. Nat Neurosci (2014) 17(6):782. doi: 10.1038/nn.3708
25. Dold M, Bartova L, Souery D, Mendlewicz J, Serretti A, Porcelli S, et al. Clinical characteristics and treatment outcomes of patients with major depressive disorder and comorbid anxiety disorders-results from a European multicenter study. J Psychiatr Res (2017) 91:1–13. doi: 10.1016/j.jpsychires.2017.02.020
26. Kautzky A, Baldinger-Melich, Kranz GS, Vanicek T, Souery D, Montgomery S, et al. A New Prediction Model for Evaluating Treatment-Resistant Depression. J Clin Psychiatry (2017) 78(2):215–22. doi: 10.4088/JCP.15m10381
27. Dold M, Bartova L, Fugger G, Kautzky A, Souery D, Mendlewicz J, et al. Major depression and the degree of suicidality: results of the European Group for the Study of Resistant Depression (GSRD). Int J Neuropsychopharmacol (2018) 21(6):539–49. doi: 10.1093/ijnp/pyy009
28. Kautzky A, Dold M, Bartova L, Spies M, Kranz GS, Souery D, et al. Clinical factors predicting treatment resistant depression: affirmative results from the European multicenter study. Acta Psychiatr Scand (2019) 139(1):78–88. doi: 10.1111/acps.12959
29. Pigoni A, Delvecchio G, Madonna D, Bressi C, Soares J, Brambilla. Can Machine Learning help us in dealing with Treatment Resistant Depression? A review. J Affect Disord (2019) 259:21–6. doi: 10.1016/j.jad.2019.08.009
30. Kautzky A, Dold M, Bartova L, Spies M, Vanicek T, Souery D, et al. Refining Prediction in Treatment-Resistant Depression: Results of Machine Learning Analyses in the TRD III Sample. J Clin Psychiatry (2018) 79(1). doi: 10.4088/JCP.16m11385
31. Dikeos D, Badr MG, Yang F, Pesek MB, Fábián Z, Tapia-Paniagua G, et al. Twelve-month prospective, multinational, observational study of factors associated with recovery from mania in bipolar disorder in patients treated with atypical antipsychotics. World J Biol Psychiatry (2010) 11(4):667–76. doi: 10.3109/15622970903544638
32. Haro J, Reed C, Gonzalez-Pinto A, Novick D, Bertsch J, Vieta E. 2-Year course of bipolar disorder type I patients in outpatient care: factors associated with remission and functional recovery. Eur Neuropsychopharmacol (2011) 21(4):287–93. doi: 10.1016/j.euroneuro.2010.08.001
33. Perlis RH, Ostacher MJ, Patel JK, Marangell LB, Zhang H, Wisniewski SR, et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry (2006) 163(2):217–24. doi: 10.1176/appi.ajp.163.2.217
34. Perugi G, Pacchiarotti I, Mainardi C, Verdolini N, Menculini G, Barbuti M, et al. Patterns of response to antidepressants in major depressive disorder: Drug resistance or worsening of depression are associated with a bipolar diathesis. Eur Neuropsychopharmacol (2019) 29(7):825–34. doi: 10.1016/j.euroneuro.2019.06.001
35. Nuñez NA, Comai S, Dumitrescu E, Ghabrash MF, Tabaka J, Saint-Laurent M, et al. Psychopathological and sociodemographic features in treatment-resistant unipolar depression versus bipolar depression: a comparative study. BMC Psychiatry (2018) 18(1):68. doi: 10.1186/s12888-018-1641-y
36. APA. Diagnostic and statistical manual of mental disorders (DSM-5®). Association AP, editor. Washington D.C: American Psychiatric Publishing (2013).
37. WMA. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA (2013) 310(20):2191–4. doi: 10.1001/jama.2013.281053
38. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56
39. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry (1978) 133(5):429–35. doi: 10.1192/bjp.133.5.429
40. Akiskal HS, Akiskal KK, Haykal RF, Manning JS, Connor PD. TEMPS-A: progress towards validation of a self-rated clinical version of the Temperament Evaluation of the Memphis, Pisa, Paris, and San Diego Autoquestionnaire. J Affect Disord (2005) 85: (1-2):3–16. doi: 10.1016/j.jad.2004.12.001
41. Dell'Osso B, Altamura AC. Duration of untreated psychosis and duration of untreated illness: new vistas. CNS Spectr (2010) 15(4):238–46. doi: 10.1017/S1092852900000079
42. Perugi G, Angst J, Azorin J-M, Bowden CL, Mosolov S, Reis J, et al. Mixed features in patients with a major depressive episode: the BRIDGE-II-MIX study. J Clin Psychiat (2015) 76: (3):e351–8. doi: 10.4088/JCP.14m09092
44. Spitzer RL, Endicott J, Robins E. Research diagnostic criteria: rationale and reliability. Arch Gen Psychiatry (1978) 35: (6):773–82. doi: 10.1001/archpsyc.1978.01770300115013
45. Dold M, Bartova L, Kautzky A, Porcelli S, Montgomery S, Zohar J, et al. Psychotic Features in Patients With Major Depressive Disorder: A Report From the European Group for the Study of Resistant Depression. J Clin Psychiatry (2019) 80(1). doi: 10.4088/JCP.17m12090
46. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). Washington D.C: A.P. Association (2010).
47. Arnow BA, Blasey C, Williams LM, Palmer DM, Rekshan W, Schatzberg AF, et al. Depression subtypes in predicting antidepressant response: a report from the iSPOT-D trial. Am J Psychiatry (2015) 172: (8):743–50. doi: 10.1176/appi.ajp.2015.14020181
48. Zaninotto L, Souery D, Calati R, Di Nicola M, Montgomery S, Kasper S, et al. Temperament and character profiles in bipolar I, bipolar II and major depressive disorder: Impact over illness course, comorbidity pattern and psychopathological features of depression. J Affect Disord (2015) 184:51–9. doi: 10.1016/j.jad.2015.05.036
49. Zaninotto L, Souery D, Calati R, Scudellari, Janiri L, Montgomery S, et al. Mixed, melancholic, and anxious features in depression: a cross-sectional study of sociodemographic and clinical correlates. Ann Clin Psychiatry (2014) 26(4):243–53.
50. Malhi GS, Das, Mannie Z, Irwin L. Treatment-resistant depression: problematic illness or a problem in our approach? Br J Psychiatry (2019) 214(1):1–3. doi: 10.1192/bjp.2018.246
53. Ghaemi SN. Feeling and time: the phenomenology of mood disorders, depressive realism, and existential psychotherapy. Schizophr Bull (2006) 33(1):122–30. doi: 10.1093/schbul/sbl061
Keywords: treatment-resistance, depression, bipolar disorder, mixed states, mixed features
Citation: Fornaro M, Fusco A, Novello S, Mosca P, Anastasia A, De Blasio A, Iasevoli F and de Bartolomeis A (2020) Predictors of Treatment Resistance Across Different Clinical Subtypes of Depression: Comparison of Unipolar vs. Bipolar Cases. Front. Psychiatry 11:438. doi: 10.3389/fpsyt.2020.00438
Received: 08 January 2020; Accepted: 28 April 2020;
Published: 15 May 2020.
Edited by:
Brisa Fernandes, University of Texas Health Science Center at Houston, United StatesReviewed by:
Massimo Pasquini, Sapienza University of Rome, ItalyLucie Bartova, Medical University of Vienna, Austria
Copyright © 2020 Fornaro, Fusco, Novello, Mosca, Anastasia, De Blasio, Iasevoli and de Bartolomeis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michele Fornaro, ZG90dC5mb3JuYXJvQGdtYWlsLmNvbQ==