 Isabelle Häberling1
Isabelle Häberling1 Gregor Berger1*
Gregor Berger1* Klaus Schmeck2
Klaus Schmeck2 Ulrike Held3
Ulrike Held3 Susanne Walitza1 on behalf of The Omega-3 Study Team
Susanne Walitza1 on behalf of The Omega-3 Study Team- 1Research Department of Child and Adolescent Psychiatry, University Hospital of Psychiatry Zurich of the University of Zurich, Zurich, Switzerland
- 2Research Department of Child and Adolescent Psychiatry, Psychiatric University Hospitals Basel, University of Basel, Basel, Switzerland
- 3Epidemiology, Biostatistics and Prevention Institute, University of Zurich, Zurich, Switzerland
Background: Depressive disorders in childhood and adolescence are a major health problem and often follow a chronic course with severe consequences in later life. Depressive disorders cause the highest burden of disease in this age group across all medical conditions. Treatment adherence is usually very poor, and the use of antidepressant drugs is heavily debated, as suicidal ideations may increase, in particular in the early phase of treatment. Omega-3 fatty acids rich in eicosapentaenoic acid have shown some promising results in over a dozen small scale randomized controlled trials (RCTs) in adult major depressive disorders, with only very few published RCTs in children and adolescents. High-quality phase III RCTs are missing.
Methods and Design: The omega-3-pMDD trial is a carefully designed phase III RCT to assess the efficacy and safety of omega-3 fatty acids in the early course of pediatric major depressive disorder (MDD). The study is designed as a multi-center, double-blinded, placebo-controlled, randomized clinical trial enrolling 220 patients aged 8 to 17 years meeting DSM-IV criteria for major depressive disorder of at least moderate symptom severity. After a single-blinded placebo-lead-in phase (7 to 10 days) patients are randomly assigned to omega-3 fatty acids or placebo over 36 weeks. Primary outcomes are changes in depression severity, as well as remission and recovery rates. Secondary outcome measures include the omega-3 index and inflammatory parameters as predictors of response. Data analysis will be performed in the intention-to-treat sample using a (generalized) linear random intercept regression model. Through sampling of blood, hair, saliva, and urine, further putative biological markers for depression and omega-3 fatty response will be investigated.
Discussion: This trial addresses if omega-3 fatty acids play a role in the pathogenesis of pediatric MDDs and have antidepressant properties, in particular in clinically depressed children and adolescents with a pre-existing omega-3 fatty acid deficiency, increased markers of oxidative stress, and/or markers of (low grade) inflammation.
Ethics and Dissemination: The study was approved by the local ethics committees. The results will be published in peer-reviewed journals irrespective of specific outcomes.
Clinical Trial Registration: www.ClinicalTrials.gov, identifier NCT03167307.
Introduction
Prevalence rates of major depressive disorders (MDDs) are low in prepubertal children, but increase substantially throughout adolescence. In a recent representative survey of over 10,000 adolescents aged 13 to 18 years, lifetime and 12-month prevalence were estimated at 11.0% and 7.5%, respectively (1). Females have a three times higher risk than males to undergo a first depressive episode between the ages of 12 and 17 years (2). About 20% of childhood-onset MDD will recover within 3 months and about 60% within 9 months, which puts the mean length of childhood onset MDD to about 9 months (3). A more recent survey estimated the mean duration of an episode to be about 27 weeks (1), but with high individual variability (4). An early onset of the disease is a risk factor for chronic and recurrent forms of depression in adulthood with more than half experiencing a first relapse within five years (5). MDD is associated with difficulties in relationships, impaired school and work functioning, conduct problems, and an increased risk of substance abuse (2,, 7). Additionally, depressive disorders are major contributors to the burden of suicide and poor long-term health later in life (8, 9).
Depressive disorders are often not recognized by professionals (10) and only about a quarter receive appropriate treatment (11). These findings are alarming given that MDD is the leading cause of disability between 10 and 24 year olds (12).
Omega-3 Fatty Acids and Depression
The dramatic change in human life style, in particular in dietary habits, might be one of the reasons for the raise of civilization diseases, such as obesity, cardiovascular diseases, cancer, inflammatory, and autoimmune diseases, but also mental disorders such as depression, given that in modern societies the nutritional environment does not match the human genetic constitution (13). The modern Western dietary habits have changed in an unprecedented way since the industrial revolution with a dramatic shift from a balanced omega-3 to omega-6 ratio towards an excessive intake of omega-6 fatty acids. Nowadays, there are hardly any processed foods without an excess of omega-6 fatty acids due to the widespread industrial use of vegetable oils (e.g. sunflower oil). Furthermore, the intake of fish and other sources of omega-3 long chained polyunsaturated fatty acids (LC-PUFAs) have decreased, in particular in urban areas.
Epidemiological studies provide some evidence that high intake of fish seems to be a protective factor against the development of MDD (14), in particular in females (15). Case-control studies confirm that a high fish intake reduces the relative risk for child and adolescent depression (16). Reduced levels of omega-3 fatty acids in red blood cells of depressed patients provide further evidence supporting a link between altered PUFA metabolism and depression (17). Interestingly, such a reduction in PUFAs is only found in patients experiencing a current depressive episode, but not in remitted patients (18, 19), suggesting a direct and reversible relationship between omega-3 fatty acids deficiency and depression.
Meta analyses summarizing the results of various randomized placebo-controlled clinical trials on the efficacy of omega-3 fatty acids treatment in MDD reported standardized mean differences ranging from 0.11 to 0.56 (an overview of all RCTs is given in SI Table 1), reaching different conclusions of the clinical significance of omega-3 fatty acids as an antidepressant (AD) treatment (20–30). A recent rigorous Cochrane review encompassing 20 RCTs in MDD suggests a small-to-modest benefit for depressive symptomology with an SMD = −0.32 (27). Some of the inconsistencies between studies may also be explained by methodological differences, such as the inclusion/exclusion criteria, study subgroup selection, and choice of drug composition. For example, omega-3 fatty acids have only been found to be effective in populations with a clinical diagnosis of depression, but not in subclinical depressed individuals (23, 28). In addition, formulations rich in eicosapentaenoic acid (EPA) seem to be more effective than formulations rich in docosahexaenoic acid (DHA) (26), although it is unclear whether the effects depend on a specific ratio of EPA to DHA (24) or solely on a higher EPA dose irrespective of the DHA content (28, 29). Furthermore, omega-3 fatty acids might be especially effective in depressed patients with no comorbid disorders (30), and some studies have shown that it is also effective as an augmentation to another AD therapy, possibly even more so (28, 29, 31). Nearly all meta-analyses come to the conclusion that, at present, we do not have sufficient evidence to support or rule out that omega-3 PUFAs are potential treatments for MDD or could reduce dosages of selective serotonin reuptake inhibitors (SSRI) medication in MDD. Adequately powered RCTs are, therefore, warranted.
Evidence in Children and Adolescents
In contrast to the abundance of studies conducted in adults, the evidence of a link between omega-3 fatty acids and depression in children and adolescents is relatively sparse. In a Japanese study including 6,700 adolescents aged 12 to 15 years daily fish intake was inversely associated with depressive symptoms, but only in college boys and not girls (16). Red blood cell fatty acid levels have also been shown to be lower in depressed adolescents than in healthy controls (32) although the highest effects were found in other fatty acids than EPA or DHA.
The few randomized controlled trials conducted in minors showed at least partly encouraging results (see SI Table 1). In a small study including 20 depressed children aged 6 to 12 years, omega-3 fatty acid supplementation showed a large advantage over placebo (33). Given the small sample size, though, these results need to be interpreted with caution. Similarly, an RCT including 23 young adults around 20 years of age also showed significant reduction in depression severity after 3 weeks of omega-3 fatty acids treatment (34). In another small scale study including 35 patients with half of them getting a daily dose of 2,400 mg omega-3 fatty acids and the other half getting the same amount of omega-6 fatty acids (35), a significant treatment effect was found for patients with a major depressive disorder. Patients with a mixed anxiety depressive disorder, however, did not benefit from the omega-3 fatty acid treatment. The largest study to date included 72 youth with pediatric depression aged 7 to 14 years which underwent omega-3 monotherapy, individual-family psychoeducational psychotherapy (PEP) or combinations, respectively, for a trial duration of 12 weeks (36). Omega-3 treatment showed a small to medium effect compared to placebo. In an interesting study including 14 adolescents with SSRI resistant MDD, half of the patients received a very high dose of 16.2 g omega-3 fatty acids per day and the other half a low dose of 2.4 g per day over 10 weeks (37). In the high-dose group, 100% of patients showed symptoms remissions compared to 40% in the low dose group. In contrast though, no beneficial effects of omega-3 fatty acids were found in an RCT including 51 adolescents with MDD who were treated for a period of 10 weeks (38). In summary, preliminary data point towards beneficial effects of omega-3 fatty acids on pediatric depression but large-scale studies are needed to validate these results.
Omega-3 Fatty Acids, Depression, and Cognition
Cognitive deficits are often observed in depressed individuals reflected in reduced concentration, attention, and impairments in executive and memory functions, among others (39). Even more so, residual cognitive deficits may persist after remission of the depressive episode affecting academic performance (40). The role of omega 3 fatty acids in improving cognitive functions has been extensively studied in a variety of populations ranging from infants to the elderly, and from healthy individuals to patients with psychiatric, neurodegenerative or neurodevelopment disorders. For example, omega 3 fatty acids supplementation has been shown to improve depressive symptoms and verbal fluency in elderly with mild cognitive impairments (41), although the effects might depend also on genetic variations of the patients (42). However, other studies reported no or only small beneficial effects (43, 44), or only on specific cognitive subdomains such as reaction time (45).
The evidence of a beneficial effect of omega-3 fatty acids on cognition in children and adolescents remains inconclusive. In a Danish study assessing the impact of a healthy diet on school performance in third and fourth grade children, the dietary intervention improved school performance and reading comprehension. Post hoc analysis revealed that about 20% of the intervention effect might be attributed to an increase in EPA and DHA levels due to the intake of fish (46). Similarly, end-term grades and vocabulary were found to be higher in the group of 700 Dutch high school students who met the national guidelines of fish consumption compared to the group who never ate fish (47). In healthy adolescents aged 13 to 15 years, the blood level ratio between omega-3 and omega-6 correlated with scores on the letter Digit Substitution Test, indicating a higher information processing speed (48).
A recent meta-analysis confirmed a beneficial effect of omega-3 fatty acids in infants up to 18 months of age but not in children or adults (49), although the inclusion of a wide range of assessment instruments and age stages might raise questions regarding the validity of the result (50). Even if omega-3 fatty acids might not improve cognition in healthy developing children, they might alleviate cognitive deficits in adolescents with psychiatric disorders. For example, omega-3 fatty acid supplementation for 16 weeks improved working memory but no other cognitive functions in children diagnosed with attention-deficit/hyperactivity disorder (ADHD) (51). Similarly, the level of DHA was lower in ADHD children with learning difficulties than in those without, and higher DHA levels predicted better word reading skills (52). In a recent meta-analysis Chang and colleagues (53) concluded that omega-3 fatty acids supplementation improves cognitive functioning associated with attention in ADHD children. Surprisingly, only one study to date assessed directly whether omega-3 fatty acid supplementation will not only improve mood symptoms in pediatric depression but also associated cognitive deficits. Vesco and colleagues (54) found improved executive functioning after a 12-week omega-3 fatty acid intervention. It remains to be established whether omega-3 fatty acids have beneficial effects on other cognitive domains that are often affected in pediatric depression, such as working memory or attention. Given the high prevalence of cognitive deficits in depressed youth and their impact on academic performance and school work, more studies using a set of different cognitive tests are necessary to evaluate differential effects of omega-3 fatty acids on cognitive functioning in depressed children and youth.
Biological Mechanism
Preclinical and clinical data point toward several mechanisms that most likely act in concert (55). For example, omega-3 fatty acids have shown to attenuate the exaggerated, persistent elevation of the stress response in animal models with depressive features (56–58) and humans (59, 60). Several lines of evidence support an altered immune-modulation in the pathophysiology of depression. Inflammatory mediators, like cytokines, play an important role in the stress system by influencing the activity of the hypothalamic pituitary adrenal (HPA) axis (61). Chronic stress, elicits a neuroinflammatory response, releasing inflammatory mediators, such as interleukin-1β (IL-1β) and tumor necrosis factor-α (TNF-α) (62), two cytokines that are inhibited by omega-3 fatty acids. Chronic stress also alters activation of the immune system in the periphery, which might account for the state of chronic inflammation observed in depressed patients (63). Omega-6 fatty acids such as arachidonic acid (AA) and omega-3 fatty acids such as EPA and DHA are both converted in bioactive molecules, also called eicosanoids. The eicosanoids derived from omega-3 and omega-6 fatty acids have partially opposing functions, with the first ones being mainly pro-inflammatory and the latter ones acting anti-inflammatory (64, 65). Both compete with each other for incorporation into cell membrane phospholipids (66–68). Omega-3 fatty acids inhibit the release of pro-inflammatory cytokines, such as IL-1β, IL-2, IL-6, interferon-γ, and TNFα (69). Given the link between depression and an increased production of pro-inflammatory cytokines (70), this inhibition might explain some of the AD effects of omega-3 fatty acids. Furthermore, cytokines also lower neurotransmitter precursor availability, and neurotransmitter metabolism (71), which might be important in the pathogenesis of mood disorders.
Omega-3 fatty acids are also crucially important for brain development. Myelination and synaptic pruning are core processes during normal pubertal brain development (72). The regulation of PUFA metabolism is crucial for both processes (73, 74). Of particular interest is a preclinical study investigating cognition and behavior across different developmental stages in rats. Omega-3 fatty acids deficient diets across consecutive generations produced a modality-selective and task-dependent impairment in cognitive and motivated behavior in adolescent rats distinct from the deficits observed in adult rats (75, 76). Omega-3 fatty acids supplementation was able to attenuate such depression-like animal behaviors during critical periods of brain development (77). Furthermore, omega-3 fatty acids have a preventive and neurotrophic effect against structural hippocampal alterations in animal models with depression- and anxiety-like behaviors (78–81). In addition, supplementation with omega-3 fatty acids might increase synaptic plasticity through an increase of brain-derived neurotrophic factor (BDNF), acting neuroprotective (71). Omega-3 fatty acids might ameliorate symptoms of depression through the protection of cells and their positive effects on neurogenesis, and counteract the shrinkage of the hippocampus (82). Omega-3 fatty acids deprived rats also provide evidence for an increase in serotonin 2 (5-HT2) and a decrease in dopamine 2 (D2) receptor density in the frontal cortex, as well as an increased serotonin turnover in the prefrontal cortex and decreased midbrain tryptophan hydroxylase-2 expression (83–89). In humans, omega-3 intake is associated with an increase in cerebrospinal fluid 5-5-hydroxyindoleacetic acid (5-HIAA) release (90, 91).
Omega-3 fatty acids are essential components of intracellular und neuronal cell membranes, affecting cell membrane integrity and fluidity (69, 92, 93). Through their effect on the efficiency of membrane functioning, omega-3 fatty acids play a role in a variety of biological mechanisms, such as enzyme and receptor activity, ion channels functioning, and the production and activity of neurotransmitters (85, 94). An increase in membrane fluidity results in a more flexible membrane and facilitates transmission (95).
While supplementation of omega-3 fatty aims to increase concentrations of fatty acids and their derived bioactive lipids that are available to the organism, omega-3 fatty acid metabolism depends on a variety of factors, including genetic variations. Therefore, omega-3 fatty concentrations will be monitored over the course of the study with blood sampling procedures carried out at baseline, after 3 months, and at the end of the study. Remaining blood is stored in a biobank allowing for further analyses of various parameters associated with omega-3 fatty acid balance and depression as well as the impact of genetic makeups on fatty acid metabolism.
The Omega-3-pMDD Trial: Rationale
As summarized above, there is growing evidence for the efficacy of omega-3 fatty acids as a treatment for major depression, in particular in pediatric populations. The generalizability of the results, though, is hampered by the conduction of small-scale studies, which do not allow for an accurate estimation of effect sizes. Therefore, the implementation of a well-designed large-scale clinical trial is warranted.
The present omega-3-pMDD trial recruits 220 patients with clinically diagnosed pediatric depression to assess the efficacy and safety of omega-3 fatty acids treatment. Given the knowledge gained from trials conducted in adults, formula rich in EPA will be used. In addition, comorbid disorders are assessed systematically for each patient, and concomitant medication is recorded throughout the 36-week trial. In case no concomitant medication is given, the efficacy of omega-3 fatty acid supplementation as a first line treatment is evaluated. However, ethical considerations do not allow for all patients to be treated solely with omega-3 fatty acids or placebo over a period of 36 weeks. In cases of severe or treatment resistant depression, additional pharmacological therapies might be indicated. In a recent survey, 40% of 85,000 depressed adolescents received AD medication during the course of their illness (96). This number appears relatively high given the major concern of increased suicidal ideations in the first weeks of treatment, which has been linked to the intake of ADs in minors (97, 98). In 2004, the advisory board of the Food and Drug Administration (FDA) decided to issue a black box warning indicating an increased risk of suicidal ideation in children receiving AD medication, especially SSRIs. Although further meta-analyses debated the increase of suicidal ideation after use of these drugs (99), it has contributed to a lot of insecurity in affected individuals and their families, as well as in the professional community (100).
When we designed the Omega-3 pMDD study, we evaluated several possible study designs. If we had decided to do a pure augmentation trial, the likelihood to lose those families opposed to AD medication (quite common in pediatric populations) would have been large. If we had decided to do a pure monotherapy omega-3 PUFAs RCT, we were concerned that clinicians would only refer less severe cases raising the risk of a ceiling effect due to the natural recovery rates of less severely depressed patients. Furthermore, omega-3 fatty acids seem to have better efficacy in severely depressed patients (23), potentially because more severe states of depression may be associated with stronger inflammatory processes. Both options were therefore considered less favorable to investigate the primary aim that omega-3 PUFAs have AD properties in moderately to severely depressed children and adolescents. For all these reasons, we decided that concomitant treatment with AD medication is permitted to not compromise the representativeness of the sample and to ensure that patients receive the optimal therapy for their disorder. Our design will allow us to directly compare the effects of omega-3 fatty acids as a monotherapy as well as adjunct to other AD drugs. In addition, statistical methods including multiple imputations in those who are put on ADs will be employed to control for the effects of AD medications on the trials’ results. Without controlling for AD use, we would run the risk to compare omega-3 fatty acids with ADs instead of placebo. In the proposed additional intention-to-treat analysis, we will consider the start of AD medication as a dropout criterion and impute the consecutive assessment time points of the main outcome measurements based on the values of those subjects that are not put on an AD. By considering the beginning of an AD as a treatment failure, we minimize the risk to mask a positive effect of omega-3 fatty acid supplementation by starting ADs more frequently or earlier in the placebo arm than in the omega-3 fatty acid arm. With this unique und novel way of analyzing the primary outcome data, the omega-3-pMDD trial aims to answer a wide range of questions regarding the treatment with omega-3 fatty acids, such as their efficacy and safety, the influence of omega-3 fatty acid supplementation on cognitive deficits associated with depression, and the emergence of putative biomarkers for omega-3 fatty acid treatment with and without the confounding effects of ADs.
Methods and Analysis
Study Overview
The Omega-3-pMDD study is a Swiss multicenter, randomized, double blind, placebo controlled clinical trial, enrolling a sample of 220 individuals aged 8 to 17 years who have a present primary diagnosis of a major depressive disorder of at least moderate symptom severity. The study design incorporates a 7- to 10-day lead in phase and a 36-week double blind placebo-controlled treatment phase. The study was approved by the local ethics committees and the regulatory affairs and is registered at ClinicalTrials.gov protocol No NCT03167307. The primary outcome is changes in the Children’s Depression Rating Scale (CDRS-R) total score (101, 102). The categorical co-primary outcome includes response rates at 6 weeks and remission rates at 12 and 36 weeks, and rates of recovery defined by the absence of major depression for > 4 months at 36 weeks. Secondary outcome measures are a variety of psychopathological, neuropsychological, and biological measures, including questionnaires, cognitive testing, and biological markers. In addition, potential response predictors are assessed, such as inflammatory mediators in serum, red blood cell acids, and bioactive lipid mediators.
Interventions
Intervention Group
The active treatment consists of a daily dose of 1,000 mg EPA/500 mg DHA in the over 13 years old. Meta-analyses in adults have shown that only drugs containing an EPA content over 60% are effective in the treatment of depressive disorders (24). Furthermore, according to the meta-analysis conducted by Grosso and colleagues (103), the optimal daily dose of omega-3 fatty acids is about 1.8 g, which is very close to the 1.5 g administered in the current trial. In children under 13 years old, half the dose is administered resulting in 500-mg EPA/250 mg DHA per day, which is a similar daily dose to the one used in the trial of prepubertal children conducted by Nemets and colleagues (33).
Control Group
The control group receives placebo capsules containing mostly medium chain triglycerides (MCT), because they do not contain any unsaturated fatty acids, and in these small quantities, they do not have any pharmacological effect. A major concern is that omega-3 fatty acids capsules could be “unblinded” because of the fishy taste. Therefore, a small amount of fish oil is added to the placebo capsules to mimic the taste, preventing guessing of the treatment arm (104). Capsules are especially manufactured so that they can easily be swallowed by children. In addition, they will contain natural orange flavor for a pleasant odor when opening the bottle and so optimizing compliance.
Concomitant Interventions
The background treatment across both groups is standardized based on the evidence and consensus-based German S3 Guidelines for the treatment of depression in children and adolescents (105). The core element is based on the cognitive behavioral therapy (CBT) method that includes individual CBT as well as psycho-educational family sessions. All participant sites are trained accordingly. In severe or treatment resistant cases of depression, the prescription of AD drugs might be indicated by experienced senior clinicians of the participating centers. Medicated patients can still participate in the trial. However, the start time and dose of the AD medication are recorded and are taken into account in the statistical analyses, as described further below.
Participants and Recruitment Methods
Participant Eligibility
Table 1 displays the inclusion and exclusion criteria used in the trial and their corresponding rationale. Given that omega-3 fatty acids were shown to be mainly efficient in clinically diagnosed patients (23), diagnosis criteria for major depressive disorder are carefully assessed to ensure that all patients fulfill the diagnosis of a major depressive disorder (MDD) according to DSM-IV. In addition, the severity of the symptoms needs to be of at least moderate severity, as measured by a revised Children’s Depression Rating Scale (CDRS-R) total score of ≥40. Patients with the primary diagnosis of schizophrenia, bipolar affective disorder, substance use dependency, pervasive developmental disorders (autism), neurological conditions or the diagnosis of an eating disorder within the last 6 months are excluded from the trial. Other comorbid disorders, such as attention deficit disorders, anxiety disorder or conduct disorders, are not considered to be a reason for exclusion of the trial, but are recorded as pre-specified comorbidities to allow the identification of clinical subgroups which might differ in their treatment response. Furthermore, routine laboratory blood testing is performed before the intervention time to ensure the well-being of the patients and to detect any medical problems. Given the ongoing debate whether omega-3 fatty intake might increase bleeding time (106), coagulation parameters will be assessed and in case of clinically significant values patients will not be able to take part in the trial.
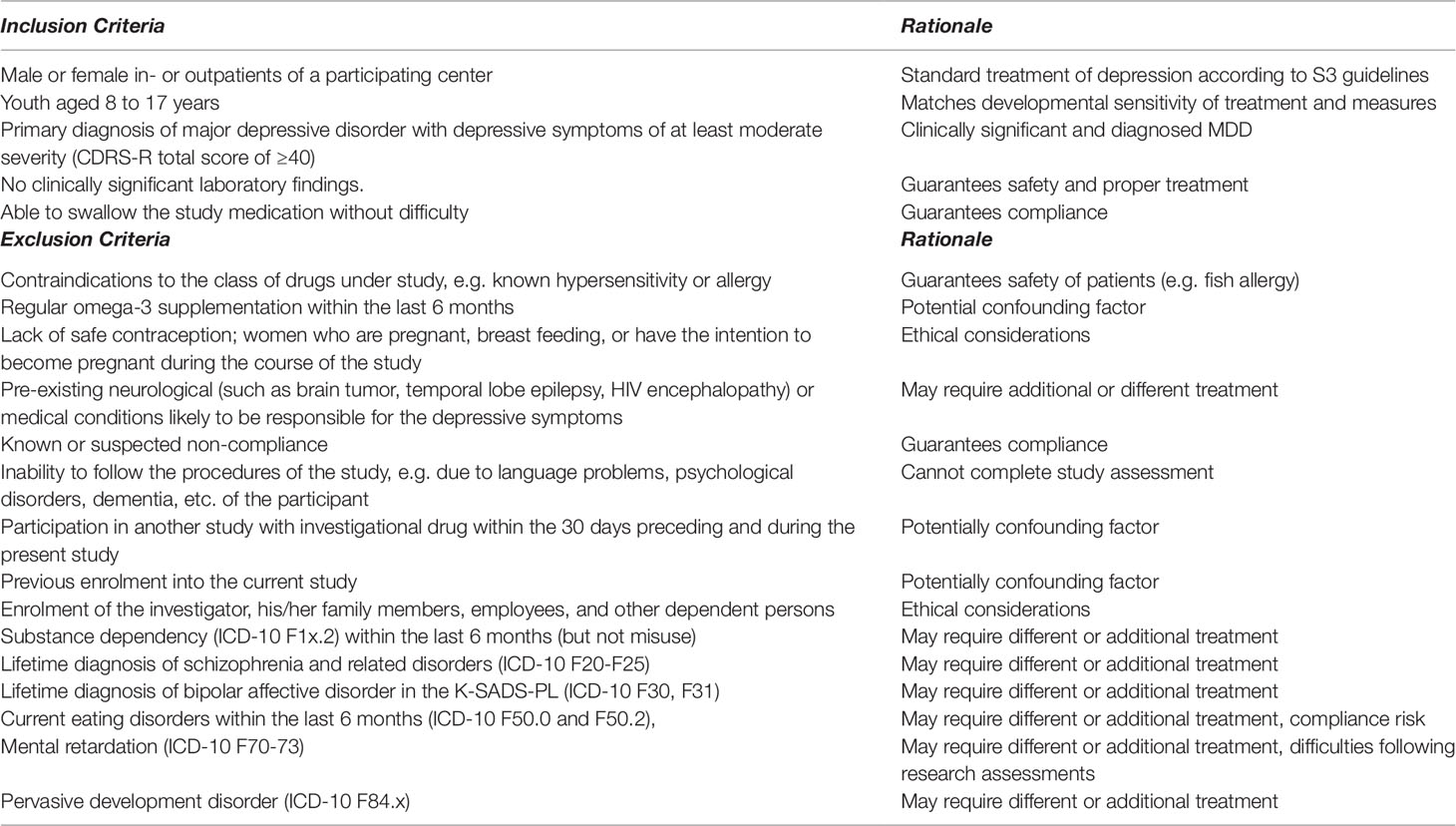
Table 1 Inclusion and exclusion criteria Omega-3-pMDD trial.
Recruitment
Children and adolescents meeting criteria for clinical depression are recruited from mental health in- and outpatient services in the German speaking part of Switzerland. In all participating centers, the study team performs annual workshops introducing the study. Patients and their families are only contacted directly by the investigators once clinicians have explored their willingness to be informed about the study. Thereafter, the first visit is scheduled during which patients and their families are informed about the nature and course of the study, and the study information and informed consent are handed out. The study team answers all questions, and the families are advised not to sign immediately but to think it over for at least another day before enrolling. Once the patients and their legal guardian have signed, the consent form appointments for the first week are scheduled.
Research assessments are carried out by the central study team, which will visit patients and their families in the participating centers or at their homes. All research psychologists will complete training courses for the clinical interviews and the cognitive tests prior to visiting patients. Scoring of clinical interviews will be tested using video footage of patients being assessed. Furthermore, all new staff members will be directly observed in their first research assessments, and symptoms will be scored simultaneously by other researchers until a good agreement is reached. To ensure the reliability of the data and to detect any inconsistencies in assessments, weekly research meetings will be held, during which symptom ratings and fulfillment of diagnostic criteria are discussed with senior clinicians (GB, SW).
Stratification and Randomization
The data are stratified by sex (male, female), age group (≥ 13 years old, < 13 years old), center, and whether the patient belongs to an in- or outpatient unit. In addition, the value of the high sensitive C-reactive protein (hsCRP) forms another stratification parameter (low < 1 mg/L; average 1.0–3.0 mg/L; high > 3.0 mg/L). Previous studies in adults (107, 108) and adolescents (109) have shown serum hsCRP to be an independent risk factor in depressive disorders, highlighting the role of low grade inflammation in the pathogenesis of mood disorders. Given the anti-inflammatory mechanisms of omega-3 fatty acids, a balanced allocation of patients with and without low-grade inflammation in the treatment arms are warranted. Randomization is carried out using the in-built functions of the clinical trial software SecuTrial®. SecuTrial® assigns the patient to the subgroup which leads to least imbalance within all strata. The software then provides a randomization number from a list implemented previously by a data administrator not otherwise involved in the study. Given that not always the next randomization number is selected by the computer, the study team is unable to guess what the next number will be. The research psychologist hands out the correct trial medication, which are stored in identical bottles and with the number as only identification.
Assessments
Primary Outcome Assessments/Parameters
The primary outcome is change in the total score of the Children’s Depression Rating Scale- revised (CDRS-R), measured on a continuous scale. Co-primary categorical outcomes are response rate to treatment at week 6, remission rate at weeks 12, 24, and 36, and recovery rate at 36 weeks. The CDRS-R is a 17-item scale and quantifies childhood (102) and adolescent (110) depressive symptoms with a total score of ≥40 indicating moderate to severe depression and has been extensively used in research (111). The scale is also evaluated in German (112). Response is defined as a 30% decrease in the total CDRS-R scores (113), whereas a score ≤28 is being used to define remission. Recovery is defined as the absence of the diagnosis of MDD for > 4 months, and is established with the semi-structured interview Kiddie Schedule for Affective Disorders and Schizophrenia — Present and Lifetime Version (K-SADS-PL) (114). The K-SADS-PL is a diagnostic interview designed to assess current and past DSM-IV diagnoses in children and adolescents, by interviewing the parent(s) and child. The section for diagnosing the presence of a current major depressive disorder confirms the presence of a MDD at baseline and determines recovery status of a study participant at each assessment time point. In addition, the K-SADS-PL is also used to assess comorbid disorders and to ensure inclusion and exclusion criteria are met.
Secondary Outcome Assessments/Parameters
Secondary outcome assessments consist of a variety of questionnaires, rating scales, and neuropsychological tests, as summarized in Table 2. Depression severity is additionally assessed through a self-report questionnaire, the Depression Inventory for Children and Adolescents (DIKJ) (115). Suicidal ideation is assessed using the Suicidal Ideation Questionnaire (118) with adolescents over 13 years also filling in the Beck’s hopelessness Scale (116). Anxiety levels are assessed through the Beck’s anxiety inventory (117), and emotional instability as well as other borderline traits are rated by parents and patients over 13 years of age using the German versions of the IES-27 (124). Stress is monitored with the Perceived Stress Scale (PSS) (121), while the Connor Davidson Resilience Scale (120) is used to estimate resilience. Sleep quality is assessed using the Insomnia Severity Index (119). Parents and patients rate quality of life with the Kidscreen (132) with parents and patients over the age of 11 years also rating behavioral problems using the Strength and Difficulty Questionnaire (SDQ) (123). In addition, childhood maltreatment is assessed with the Childhood Trauma Questionnaire (CTQ) (138) while victimization in the school environment is assessed with the Olweus Bullying Questionnaire (OBQ) (139).
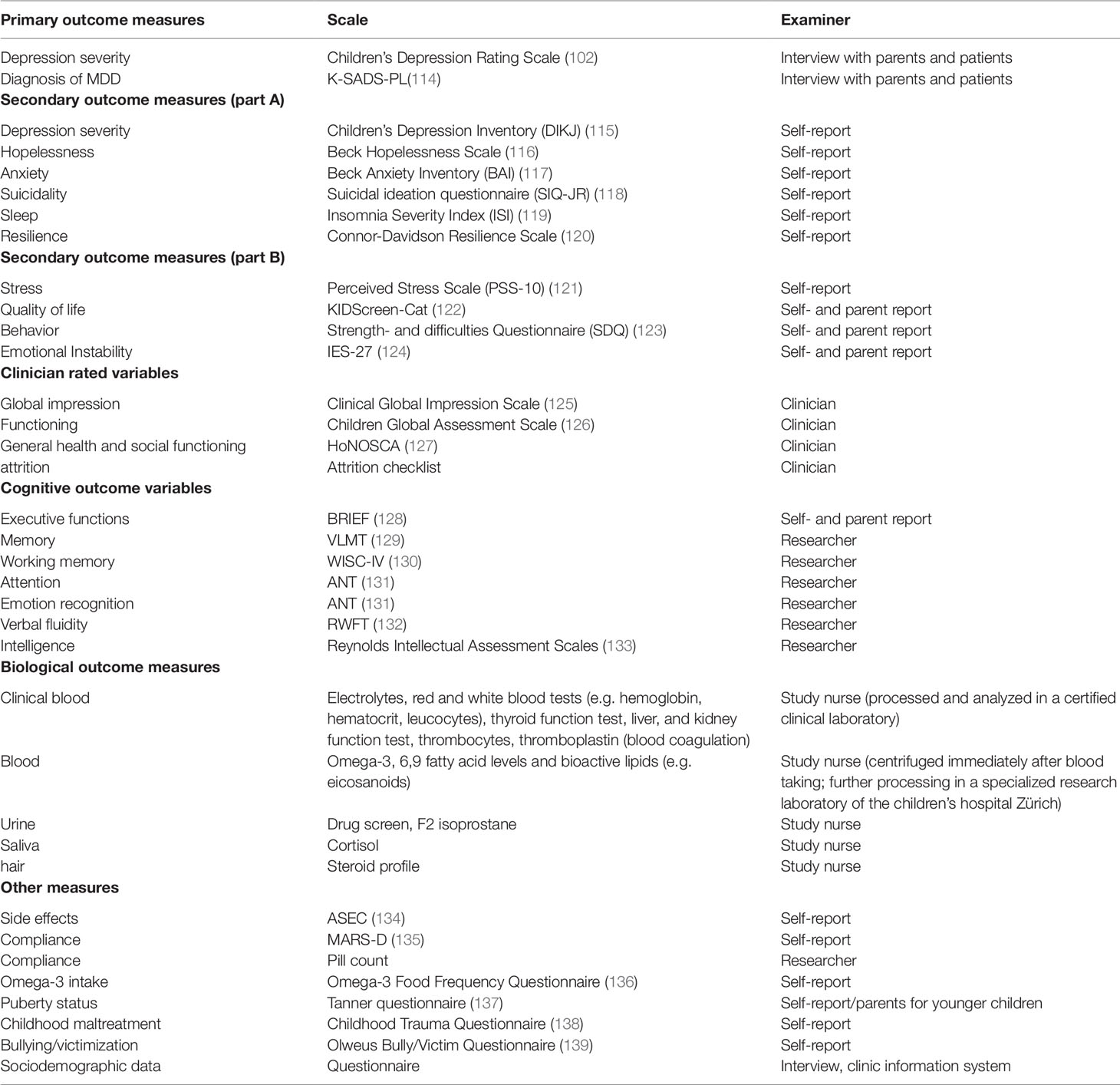
Table 2 Outcome measures Omega-3-pMDD trial.
Clinician-Rated Scales
In addition to self- and parent-rated instruments, clinicians treating the patients are asked to fill in three short rating scales. Clinicians rate symptom severity and global improvement on the Clinical Global impression scale (CGI-S/I) (125) and global functioning on the Children’s Global Assessment of functioning (CGAS) scale (126). In addition, behavior, impairment, symptom severity, and social functioning are scored on the Health of the Nation Outcome Scale for Children and Adolescents (HoNOSCA) (127). Furthermore, clinicians indicate how many minutes they spent treating the patient between study assessments.
Cognitive Assessments
The level of cognitive functioning is assessed using a variety of standardized neuropsychological tests. Different episodic memory parameters are assessed with the Verbal Memory Learning Test (VMLT) (129), while working memory is tested with the Digit Span Forward and Backward of the Wechsler Intelligence Test for Children (WISC IV) (130). The Regensburger Word Fluency Test measures verbal fluency as a function of divergent thinking (132). The ability to shift attention and inhibit responses is assessed with the Shifting Visual Attention Test of the computerized Amsterdam Neuropsychological Test battery (131). Included in the same test battery is also the Identifying Facial Emotions test which assesses the ability of a subject to recognize emotions displayed in faces. In addition, executive functioning is assessed with the Behavior Rating Inventory of Executive Function (BRIEF) (128, 140), in which parents and patients over the age of 11 years rate the level of impairment of executive functioning in daily life. And finally, intellectual abilities are assessed with the Reynolds Intellectual Assessment Scale (RIAS) (133).
Biological Assessments
Blood is drawn three times during the course of the study, at baseline, 12 weeks, and at 36 weeks, respectively. At baseline, routine laboratory parameters are assessed to ensure that the patients are healthy and do not need any immediate medical attention. The remaining blood is stored for PUFAs (omega-3, -6, and -9 and trans fatty acids), bioactive lipids (e.g., eicosanoids, hydroxy metabolites, E-series resolvins), immune parameters (including but not restricted to interferon-γ, IL-1α, IL-1RA, IL-5, Il-6, IL-10, IL12p40, IL-15, IL-18, and TNF-α, as well as leptin and adiponetin), and for the tissue repository. Since multiple studies are currently investigating biomarkers in MDD, serum, lymphocytes, erythrocyte, platelets, and DNA will be stored after the end of the study to measure potential novel biomarkers. Genetic and epigenetic markers of interest (e.g. FADS haplotypes) include but are not restricted to genes relevant for bioactive lipid metabolism. In addition to the blood sample, patients are asked to provide 3 cm of hair in order to assess the steroid profile, including cortisol, testosterone, progesterone, dehydroepiandrosterone, and estradiol levels at 6 weeks and 9 months. Furthermore, saliva (cortisol, melatonin) and urine (drug screen, F2 isoprostane as a marker of lipid oxidation) are sampled. Biological samples are stored in a biobank for use in future research if patients and their parents agree to sign an additional consent form.
Compliance, Safety, and Other Measures
Compliance is monitored with the Medication Adherence Reporting Scale (MARS-D) (135). In addition, returned capsules are counted at each study visit. Potential side effects are assessed with a modified version of the Antidepressant Side Effect Checklist (ASEC) at each visit (134). The daily nutritional intake of omega-3 fatty acid is estimated with an adapted version of the Omega-3 Food Frequency Questionnaire (136), three times during the course of the trial.
Study Schedule
A flowchart of the study schedule is depicted in Figure 1. After the consent process, patients and their families undergo a screening interview in order to assess inclusion criteria, such as the diagnosis and severity of the depressive disorder and exclusion criteria, such as comorbidities that might prevent participation. Sociodemographic data and information about medical and family history and current medication use is also collected. If a patient is considered eligible for the trial, he or she enters the 7 to 10 days single blinded placebo lead-in phase. All patients receive placebo capsules for at least 7 days prior to randomization in order to assess any difficulties in swallowing the medication and measure compliance. Furthermore, the lead-in phase allows the identification of fast placebo responders. The baseline visit takes place at the end of the placebo lead-in phase, during which the CDRS and the subscale depressive disorder of the K-SADS-PL will be administered for a second time. If the patient still fulfills the diagnosis of a major depressive disorder with at least moderate severity, and no other exclusion criteria have emerged, the patient is randomized. Four follow-up assessments at 6, 12, 24, and 36 weeks are performed, consisting mainly out of the same measurements taken during the lead-in phase. Only four follow-up measurements are scheduled given that the number of research assessments has been identified as a predictor for placebo response (141, 142). The timing of the assessments was based on the design of the “Treatment for Adolescents with Depression” study (143), allowing us to make direct comparisons of illness trajectories between the trials. Intelligence is assessed only once at the 6-week appointment, and hair sample are taken at the 6-week appointment and at the end of the trial. Unused study drugs are counted at each appointment with compliance rates below 60% resulting in the discontinuation of the trial.
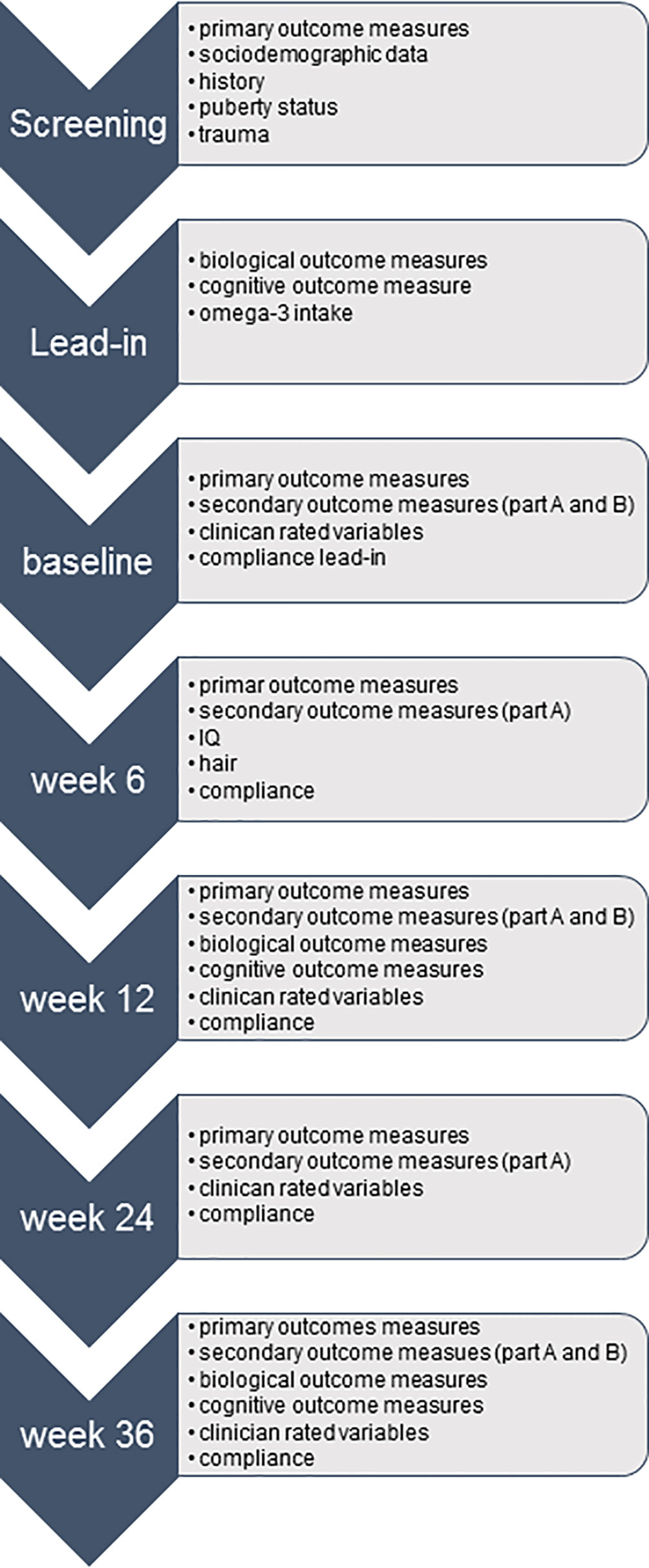
Figure 1 Flowchart study schedule Omega-3-pMDD trial.
Participants’ Compensation
There is only a small compensation for participation with patients receiving a voucher of about 20 CHF three times during the course of the study. Additional travelling costs (i.e., train fares) are recompensed.
Data Management and Analytic Approach
Data Acquisition and Security
All data collected for the Omega-3-pMDD study are entered into electronic case report forms hosted on a secure server of the Clinical Trials Centre of the University Hospital of Zurich. Each participant is assigned a study ID at enrolment, which is subsequently used to enter data into the clinical trial software SecuTrial® (www.secutrial.com). All data that are not entered directly by the patients or their parents are entered twice by two different investigators with another investigator checking the consistency of the double data entry and resolving all conflict. In addition, data quality is ensured through regular on-site monitoring by the Clinical Trials Centre of the University Hospital of Zürich. Data security, on the other hand, is guaranteed by encrypted communication and stringent firewall settings. Automated backups are made every 24 h to guarantee that no data are lost. Confidentiality of the data will be granted at all times.
Sample Size
Our power calculation was based on the available meta-analysis at the time of grant submission. The available meta-analyses provided an expected SMD of omega-3 PUFAs between 0.28 and 0.56 mainly based on adult omega-3 intervention trials (22, 24–26,). However, at this time point no studies in pediatric MDD were published, except one very small (n = 20) pilot study in childhood depression showing a large effect size (SMD = 1.4) (33). Because of the confounding factor of concomitant AD therapy and an expected high placebo response in pediatric populations, we introduced a range of measures, such as a placebo-lead in phase and conservative expected difference effect size between active and placebo. We used the following assumptions for our power calculation: Cohen’s d as effect size, calculated as difference between means in the two treatment groups divided by their pooled standard deviation, was considered to be 0.4, and with a significance level alpha of 5% and a power of 80%, 100 patients per group would be necessary to detect the clinically relevant difference with a two-sample, two-sided t-test, resulting in 200 patients in total. With an anticipated dropout rate of 10% within the first six weeks after randomization (the time point of the first follow up assessment), the number of patients for this study would be 220. The study is sufficiently powered to address also the co-primary endpoint according to the following considerations: the proportion of patients with clinically relevant improvement in the group of patients receiving omega-3 is P(omega-3) = 0.60, and the corresponding proportion of patients in the placebo group is P(placebo) = 0.40. With a significance level of 0.05 for a two-tailed chi-squared test and an anticipated power of 80%, 97 patients per treatment group would be needed. With an anticipated dropout rate of 10%, 220 patients would be sufficient to address this clinically relevant endpoint.
Based on the preliminary analysis of the baseline data of the on-going trial, 2/3 of the patients are AD free at the time of randomization, with most of them still being AD free after the first follow-up. A sample size of n = 74 per treatment arm in this subgroup of AD-free participants will enable us to detect a moderate SMD of 0.54 using a two-group t test for the CRSR-R total score with a 0.05 two-sided significance level and a 90% power. The entire ITT sample (also encompassing the third with pre-existing AD treatment) will even enable us to detect small effect sizes between active/placebo. Meta-analyses of omega- 3 PUFA supplementation in depression suggest that omega-3 PUFA augmentation trials show an even larger effect size compared to omega-3 monotherapy RCTs (31, 144, 145), in particular if EPA rich formulations or pure EPA is considered (146).
Statistical Analysis
Descriptive statistics include mean and standard deviation for continuous variables, as well as number and percentages of total for categorical variables. Ordinal scaled variables will be reported as median and interquartile range. Descriptive statistics will be reported within treatment groups.
Primary analysis is performed based on the intention to treat (ITT) principle, i.e. including all randomized patients. For the continuous primary outcome (total CDRS-R score), we will apply a linear random intercept regression model. For the co-primary endpoint, i.e., the binary outcome measure for treatment response, we will apply a logistic regression model, and treatment group as independent variable will be used. Results will be presented as effect estimates — beta-coefficients or odds ratios — with 95% confidence intervals for primary and co-primary endpoints, respectively.
However, the analysis of treatment efficacy of the omega-3 fatty acids needs to address that some study participants already receive ADs prior to study inclusion or will be put on ADs in the due course of the study. The additional use of ADs might not be uniformly distributed between the two treatment arms, which might introduce biased results if not accounted for. To account for this major confounding factor, we propose to use two different analytic approaches. (1) We will perform an additional ITT analysis of the primary and secondary outcomes defining the beginning of an AD as a treatment failure and include treatment failure/additional use of AD as time-dependent covariate in the random effects model. (2) Using 20-fold multiple imputation, depression scores that a patient would have had without AD prescriptions are estimated, based on consecutive data of subjects without AD, and on earlier observations in the same subjects. To address that the missingness generating mechanism is considered to be “missing not at random” (MNAR), the “drawn indicator method” proposed by Jolani et al. (147) will be applied. A subsequent sensitivity analysis of the results will reveal the dependence of the results on specific assumptions in the two different analytic approaches.
A pre-specified subgroup analysis will address whether there is a differential treatment effect between patients with or without the pre-specified variable (e.g. AD therapy at baseline). If there is evidence for an interaction (as quantified with the p-value of the corresponding interaction test), the treatment effect will also be reported in those subgroups.
Furthermore, we’ll run following analyses to investigate the impact of AD use based on a priori working hypotheses: Firstly, we will test differences in novel AD prescriptions between the treatment groups by means of the two proportions z-Test using the ITT sample (assuming that ADs are more frequently prescribed in the placebo arm). We will also calculate retention rates between the two groups by means of the two proportions z-Test prior of “dropping out” those subjects put on ADs (assuming that the retention rate is longer in the active compared to the placebo arm).
Further analyses on primary and secondary outcome measures will be run as detailed in the study protocol, which is available on the clinical.trials.gov website.
Safety Considerations
Omega-3 fatty acids are usually well-tolerated, but according to a recent meta-analysis by Chang et al. (148), they might elicit mild adverse effects such as gastrointestinal symptoms in some patients. In a meta-analysis including 148 omega-3 fatty acid studies with dosage up to 6 g per day, 6.6% of the active group relative to 4.3% in the placebo group reported gastrointestinal complaints. Only one study reported an increase in bleeding time (64). Thus, any medical conditions experienced during the trial are recorded. In addition, patients fill in the ASEC at each visit to measure other putative side effects. No doses changes of active/placebo are permitted during the trial, but patients and their families are informed of the voluntary nature of the study and that consent can be rescinded anytime. While no serious side effects are expected due to omega-3 fatty acids intake, the current patient population warrants for a tight safety control due to the risk of suicide. Therefore, suicidal tendencies will be closely monitored by the study team by asking directly about suicidal ideations during the clinical interviews in addition to the administration of the Suicidal Ideation Questionnaire (SIQ-Jr). Furthermore, a data monitoring committee (DMC) is set up consisting of an expert in child and adolescent psychiatry, an expert in ethical considerations, and an expert in biostatistics. All members have access to the unblinded data due to permissions associated with their study function in the database SecuTrial. In case of a serious adverse event, the members of the DMC are automatically notified through an inbuilt function of the software in order for them to continuously monitor the safety of the patients. Furthermore, after 60 enrolled patients, an interims analysis on the safety of the treatment is was performed by a member of the DMC.
Publication and Dissemination
The main outcome of the trial is published irrespective of the results. A publications committee establishes publication guidelines and coordinates the publication of secondary outcome measures, also giving recommendations to the timing of different abstracts, reviewing all publications for their appropriateness and scientific merit. No later than five years after closure of the data base, a completely de-identified data set will be provided for sharing purposes.
Discussion
This paper describes the design and methodology for a clinical trial evaluating the efficacy and safety of omega-3 fatty acids as a treatment for pediatric depression. It is paramount for children and adolescents suffering from mental problems to receive appropriate treatment. However, affected families often don’t seek help because of the stigma associated with mental illness and psychiatric treatments (149). Being open to novel treatments such as omega-3 fatty acids that are closely linked to lifestyle, food, and general well-being may indirectly encourage affected families to seek help sooner. If omega-3 fatty acids prove to be beneficial, they might serve as a benign well-accepted first step in a comprehensive treatment plan. On the other hand, if omega-3 fatty acids prove to be ineffective, the results are as important given the risks associated with delaying other effective treatments due to an unjustified supplementation of omega-3 fatty acids. Therefore, this well-designed large-scale clinical trial will provide important information on the optimal management and treatment of pediatric depression.
In our study design, we permit concomitant AD medication, to ensure the representativeness of our sample and the inclusion of more severely depressed patients. However, we will study the confounding effects by running subgroup analyses and statistically controlling for use of AD drugs. We believe that the abovementioned measures and the large sample size will allow us to address both the question if omega-3 fatty acids are effective as a first-line treatment, as well as to address the question of augmenting a pre-existing AD treatment with omega-3 PUFAs will further improve treatment outcomes.
The long study duration of 36 weeks allows studying the trajectory of a variety of psychopathological and cognitive symptoms associated with depression. Patients fill in a full range of questionnaires ranging from anxiety and emotional instability to sleep disturbances1 to dietary omega-3 fatty intake. This allows the characterization of symptoms that are affected by omega-3 fatty acid intake and the establishment of subgroups of patients profiting the most from the treatment. Pre-treatment blood levels of omega-3, 6, and 9 fatty acids are used to predict treatment response, and a variety of biological parameters are assessed in order to enhance our understanding of the biological mechanism associated with depression and the effects of omega-3 fatty acids on the brain. This is especially important given the on-going brain development in minors and the severe impacts of pediatric depression on brain structure and function (150). The establishment of a biobank creates a database of a highly unique sample that allows for further studying of the underlying biological mechanisms of pediatric depression. Therefore, this trial will advance our understanding of the pathogenesis of depression in minors and will provide a valuable contribution to the best treatment options of this severely affected patient group.
The Omega-3 Study Team
The Omega-3 Study Team contributed with implementation of the design with following roles: Sponsorinvestigator of the trial is GB (Department of Child and Adolescent Psychiatry, University Hospital of Psychiatry, University of Zurich, Neumünsterallee 9, 8032 Zurich, Switzerland; gregor. YmVyZ2VyQHB1ay56aC5jaA==; +41 43 499 2626). Chief investigators are SW and KS. IH is study coordinator. Principal investigators and research psychologist from the clinical sites are as follows: Principal Investigator Zurich: SW; Research psychologists: Noemi Baumgartner, Sophie Emery, Mona Albermann, and Kristin Nalani (Department of Child and Adolescent Psychiatry, University Hospital of Zurich); Principal Investigator Basel: KS; Investigators and research psychologists: Oliver Pick, Alain Di Gallo, and Michael Strumberger (Department of Child and Adolescent Psychiatry, Psychiatric University Hospitals Basel); Principal Investigator Basel-Stadt: Brigitte Contin; Investigator: Stefan Müller (Child and Adolescent Psychiatric Services Baselland); Principal Investigator: Silke Bachmann; Investigators: Lars Wöckel, and Simone Heitzer (Clienia Littenheid); Principal Investigator: Bruno Rhiner; Investigators: Amir Yamini (Child and Adolescent Psychiatric Services Thurgau); Principal Investigator: Suzanne Erb; Investigators: Michael Schmid (Child and Adolescent Psychiatric Services St. Gallen); Principal Investigator: Ulrich Müller-Knapp; Investigator: Ioannis Christodoulakis (Klinik Sonnenhof). UH and Burkhardt Seifert (retired) are statistical consultants. Renate Drechsler is head of the neuropsychology department and Edna Grünblatt head of the department for translational molecular psychiatry (Department of Child and Adolescent Psychiatry, University Hospital of Zurich). Martin Hersberger is head of the division of Clinical Chemistry and Biochemistry at the University Children’s Hospital Zürichand his PhD student Ivan Hartling of the division of Clinical Chemistry and Biochemistry who will analyze the bioactive lipids; Romuald Brunner (University of Heidelberg), Jürgen Drewe (University of Basel), and Julia Braun (Epidemiology, Biostatistics, and Prevention Institute, University of Zürich) are members of the Data Monitoring Committee. Jenny Peterson, Clinical Trials Pharmacy (Kantonsapotheke) Zürich, responsible for the packaging, handling, and quality of the study medication.
Author Contributions
GB conceived of the study. GB, SW, KS, and IH devised the study design. UH lent statistical support.
Funding
This research was funded as an investigator initiated clinical trial by the Swiss National Foundation (SNF grant 33IC30_166826). Furthermore, the Thalmann Foundation (University of Basel) supports an embedded sleep add on project, the Ebnet Foundation supports an additional PhD project in collaboration with the ETH Zürich investigating the influence of diet on depression and treatment response to omega-3 fatty acids. The Research Department of Child and Adolescent Psychiatry, University Hospital of Psychiatry Zurich of the University of Zurich further provides infrastructure and administrative staff support. Burgerstein, Antistress AG, Rapperswil-Jona (SG, Switzerland) provided the study medication (active and placebo). No additional industrial funding is provided throughout the study.
Conflict of Interest
The company that provided the study medication (Burgerstein, Antistress AG, Rapperswil-Jona (SG, Switzerland) provides no direct financial support towards the RCT. Burgerstein, Antistress AG has no influence on the design or analysis of the trial or publication of any results in relation to the study. The lead authors declare following conflict of interests: IH: no conflict of interest; GB: GB was supported by the Swiss National Science Foundation, the Stanley Foundation, the Gertrud Thalmann Fonds, and the Ebnet Foundation and has received speaker honoraria from Lundbeck, Opopharma, Antistress AG (Burgerstein) in the last 5 years; KS: In the last 5 years KS has received royalties from Springer, Hogrefe, and Schattauer. Since 2014, KS received no honoraria from pharmaceutical or other industrial companies. His work was supported in the last 5 years by the Swiss National Science Foundation (SNF), Swiss Ministry of Justice, University of St. Gallen, Botnar Foundation, and Gertrud Thalmann Fonds. UH: no conflict of interest. SW: SW has received in the last 5 years royalties from Thieme Hogrefe, Kohlhammer, Springer, Beltz. SW received lecture honoraria from Opopharma in the last 5 years. Her work was supported in the last 5 years by the Swiss National Science Foundation (SNF), diff. EU FP7s, HSM Hochspezialisierte Medizin of the Kanton Zurich, Switzerland, Bfarm Germany, ZInEP, Hartmann Müller Stiftung, Olga Mayenfisch, Gertrud Thalmann Fonds. Outside professional activities and interests are declared under the link of the University of Zurich.
Acknowledgments
We would like to thank all the researchers and clinicians working on the project. Special thanks belongs to the patients and their families for participating in our research.
Footnotes
- ^ An add-on study under supervision of Prof. Christian Cajochen and Prof. Klaus Schmeck will investigate the effects of omega-3 fatty acids supplementation on sleep and physical activity in a subgroup of the depressed patients.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00863/full#supplementary-material
References
1. Avenevoli S, Swendsen J, He JP, Burstein M, Merikangas KR. Major depression in the national comorbidity survey-adolescent supplement: prevalence, correlates, and treatment. J Am Acad Child Adolesc Psychiatry (2015) 5437-44(1):e32. doi: 10.1016/j.jaac.2014.10.010
2. Breslau J, Gilman SE, Stein BD, Ruder T, Gmelin T, Miller E. Sex differences in recent first-onset depression in an epidemiological sample of adolescents. Transl Psychiatry (2017) 7(5):e1139. doi: 10.1038/tp.2017.105
3. Kovacs M. Presentation and course of major depressive disorder during childhood and later years of the life span. J Am Acad Child Adolesc Psychiatry (1996) 35(6):705–15. doi: 10.1097/00004583-199606000-00010
4. Kaminski KM, Garber J. Depressive spectrum disorders in high-risk adolescents: episode duration and predictors of time to recovery. J Am Acad Child Adolesc Psychiatry (2002) 41(4):410–8. doi: 10.1097/00004583-200204000-00013
5. Lewinsohn PM, Rohde P, Seeley JR, Klein DN, Gotlib IH. Natural course of adolescent major depressive disorder in a community sample: predictors of recurrence in young adults. Am J Psychiatry (2000) 157(10):1584–91. doi: 10.1176/appi.ajp.157.10.1584
6. Fergusson DM, Woodward LJ. Mental health, educational, and social role outcomes of adolescents with depression. Arch Gen Psychiatry (2002) 59(3):225–31. doi: 10.1001/archpsyc.59.3.225
7. Korczak DJ, Goldstein BI. Childhood onset major depressive disorder: course of illness and psychiatric comorbidity in a community sample. J Pediatr (2009) 155(1):118–23. doi: 10.1016/j.jpeds.2009.01.061
8. Ferrari AJ, Norman RE, Freedman G, Baxter AJ, Pirkis JE, Harris MG, et al. The burden attributable to mental and substance use disorders as risk factors for suicide: findings from the Global Burden of Disease Study 2010. PloS One (2014) 9(4):e91936. doi: 10.1371/journal.pone.0091936
9. Richardson LP, Ludman E, McCauley E, Lindenbaum J, Larison C, Zhou C, et al. Collaborative care for adolescents with depression in primary care: a randomized clinical trial. JAMA (2014) 312(8):809–16. doi: 10.1001/jama.2014.9259
10. Scott EG, Luxmore B, Alexander H, Fenn RL, Christopher NC. Screening for adolescent depression in a pediatric emergency department. Acad Emerg Med (2006) 13(5):537–42. doi: 10.1197/j.aem.2005.11.085
11. Ghio L, Gotelli S, Marcenaro M, Amore M, Natta W. Duration of untreated illness and outcomes in unipolar depression: a systematic review and meta-analysis. J Affect Disord (2014), 152–4:45–51. doi: 10.1016/j.jad.2013.10.002
12. Gore FM, Bloem PJ, Patton GC, Ferguson J, Joseph V, Coffey C, et al. Global burden of disease in young people aged 10-24 years: a systematic analysis. Lancet (2011) 377(9783):2093–102. doi: 10.1016/S0140-6736(11)60512-6
13. Simopoulos AP. Evolutionary aspects of diet: the omega-6/omega-3 ratio and the brain. Mol Neurobiol (2011) 44(2):203–15. doi: 10.1007/s12035-010-8162-0
14. Hibbeln JR. Fish consumption and major depression. Lancet (1998) 351(9110):1213. doi: 10.1016/S0140-6736(05)79168-6
15. Timonen M, Horrobin D, Jokelainen J, Laitinen J, Herva A, Rasanen P. Fish consumption and depression: the Northern Finland 1966 birth cohort study. J Affect Disord (2004) 82(3):447–52. doi: 10.1016/j.jad.2004.02.002
16. Murakami K, Miyake Y, Sasaki S, Tanaka K, Arakawa M. Fish and n-3 polyunsaturated fatty acid intake and depressive symptoms: Ryukyus Child Health Study. Pediatrics (2010) 126(3):e623–630. doi: 10.1542/peds.2009-3277
17. Lin PY, Huang SY, Su KP. A meta-analytic review of polyunsaturated fatty acid compositions in patients with depression. Biol Psychiatry (2010) 68(2):140–7. doi: 10.1016/j.biopsych.2010.03.018
18. Carney RM, Steinmeyer BC, Freedland KE, Rubin EH, Rich MW, Harris WS. Baseline blood levels of omega-3 and depression remission: a secondary analysis of data from a placebo-controlled trial of omega-3 supplements. J Clin Psychiatry (2016) 77(2):e138–143. doi: 10.4088/JCP.14m09660
19. Thesing CS, Bot M, Milaneschi Y, Giltay EJ, Penninx B. Omega-3 and omega-6 fatty acid levels in depressive and anxiety disorders. Psychoneuroendocrinology (2018) 87:53–62. doi: 10.1016/j.psyneuen.2017.10.005
20. Appleton KM, Hayward RC, Gunnell D, Peters TJ, Rogers PJ, Kessler D, et al. Effects of n-3 long-chain polyunsaturated fatty acids on depressed mood: systematic review of published trials. Am J Clin Nutr (2006) 84(6):1308–16. doi: 10.1093/ajcn/84.6.1308
21. Lin PY, Su KP. A meta-analytic review of double-blind, placebo-controlled trials of antidepressant efficacy of omega-3 fatty acids. J Clin Psychiatry (2007) 68(7):1056–61. doi: 10.4088/jcp.v68n0712
22. Martins JG. EPA but not DHA appears to be responsible for the efficacy of omega-3 long chain polyunsaturated fatty acid supplementation in depression: evidence from a meta-analysis of randomized controlled trials. J Am Coll Nutr (2009) 28(5):525–42. doi: 10.1080/07315724.2009.10719785
23. Appleton KM, Rogers PJ, Ness AR. Updated systematic review and meta-analysis of the effects of n-3 long-chain polyunsaturated fatty acids on depressed mood. Am J Clin Nutr (2010) 91(3):757–70. doi: 10.3945/ajcn.2009.28313
24. Sublette ME, Ellis SP, Geant AL, Mann JJ. Meta-analysis of the effects of eicosapentaenoic acid (EPA) in clinical trials in depression. J Clin Psychiatry (2011a) 72(12):1577–84. doi: 10.4088/JCP.10m06634
25. Bloch MH, Hannestad J. Omega-3 fatty acids for the treatment of depression: systematic review and meta-analysis. Mol Psychiatry (2012) 17(12):1272–82. doi: 10.1038/mp.2011.100
26. Grosso G, Pajak A, Marventano S, Castellano S, Galvano F, Bucolo C, et al. Role of omega-3 fatty acids in the treatment of depressive disorders: a comprehensive meta-analysis of randomized clinical trials. PloS One (2014b) 9(5):e96905. doi: 10.1371/journal.pone.0096905
27. Appleton KM, Sallis HM, Perry R, Ness AR, Churchill R. omega-3 Fatty acids for major depressive disorder in adults: an abridged Cochrane review. BMJ Open (2016) 6(3):e010172. doi: 10.1136/bmjopen-2015-010172
28. Hallahan B, Ryan T, Hibbeln JR, Murray IT, Glynn S, Ramsden CE, et al. Efficacy of omega-3 highly unsaturated fatty acids in the treatment of depression. Br J Psychiatry (2016b) 209(3):192–201. doi: 10.1192/bjp.bp.114.160242
29. Mocking RJ, Harmsen I, Assies J, Koeter MW, Ruhe HG, Schene AH. Meta-analysis and meta-regression of omega-3 polyunsaturated fatty acid supplementation for major depressive disorder. Transl Psychiatry (2016a) 6:e756. doi: 10.1038/tp.2016.29
30. Schefft C, Kilarski LL, Bschor T, Kohler S. Efficacy of adding nutritional supplements in unipolar depression: a systematic review and meta-analysis. Eur Neuropsychopharmacol (2017) 27(11):1090–109. doi: 10.1016/j.euroneuro.2017.07.004
31. Jazayeri S, Tehrani-Doost M, Keshavarz SA, Hosseini M, Djazayery A, Amini H, et al. Comparison of therapeutic effects of omega-3 fatty acid eicosapentaenoic acid and fluoxetine, separately and in combination, in major depressive disorder. Aust N Z J Psychiatry (2008) 42(3):192–8. doi: 10.1080/00048670701827275
32. Pottala JV, Talley JA, Churchill SW, Lynch DA, von Schacky C, Harris WS. Red blood cell fatty acids are associated with depression in a case-control study of adolescents. Prostaglandins Leukot Essent Fatty Acids (2012) 86(4-5):161–5. doi: 10.1016/j.plefa.2012.03.002
33. Nemets H, Nemets B, Apter A, Bracha Z, Belmaker RH. Omega-3 treatment of childhood depression: a controlled, double-blind pilot study. Am J Psychiatry (2006) 163(6):1098–100. doi: 10.1176/ajp.2006.163.6.1098
34. Ginty AT, Conklin SM. Short-term supplementation of acute long-chain omega-3 polyunsaturated fatty acids may alter depression status and decrease symptomology among young adults with depression: A preliminary randomized and placebo controlled trial. Psychiatry Res (2015) 229(1-2):485–9. doi: 10.1016/j.psychres.2015.05.072
35. Trebaticka J, Hradecna Z, Bohmer F, Vavakova M, Waczulikova I, Garaiova I, et al. Emulsified omega-3 fatty-acids modulate the symptoms of depressive disorder in children and adolescents: a pilot study. Child Adolesc Psychiatry Ment Health (2017) 11:30. doi: 10.1186/s13034-017-0167-2
36. Fristad MA, Vesco AT, Young AS, Healy KZ, Nader ES, Gardner W, et al. Pilot randomized controlled trial of Omega-3 and individual-family psychoeducational psychotherapy for children and adolescents with depression. J Clin Child Adolesc Psychol (2019) 48(sup1):S105–18. doi: 10.1080/15374416.2016.1233500
37. McNamara RK, Strimpfel J, Jandacek R, Rider T, Tso P, Welge JA, et al. Detection and treatment of long-chain omega-3 fatty acid deficiency in adolescents with SSRI-resistant major depressive disorder. Pharma Nutr (2014) 2(2):38–46. doi: 10.1016/j.phanu.2014.02.002
38. Gabbay V, Freed RD, Alonso CM, Senger S, Stadterman J, Davison BA, et al. A double-blind placebo-controlled trial of Omega-3 fatty acids as a monotherapy for adolescent depression. J Clin Psychiatry (2018) 79(4). doi: 10.4088/JCP.17m11596
39. Bortolato B, Miskowiak KW, Kohler CA, Maes M, Fernandes BS, Berk M, et al. Cognitive remission: a novel objective for the treatment of major depression? BMC Med (2016) 14:9. doi: 10.1186/s12916-016-0560-3
40. MacQueen GM, Memedovich KA. Cognitive dysfunction in major depression and bipolar disorder: Assessment and treatment options. Psychiatry Clin Neurosci (2017) 71(1):18–27. doi: 10.1111/pcn.12463
41. Sinn N, Milte CM, Street SJ, Buckley JD, Coates AM, Petkov J, et al. Effects of n-3 fatty acids, EPA v. DHA, on depressive symptoms, quality of life, memory and executive function in older adults with mild cognitive impairment: a 6-month randomised controlled trial. Br J Nutr (2012) 107(11):1682–93. doi: 10.1017/S0007114511004788
42. Samieri C, Feart C, Proust-Lima C, Peuchant E, Dartigues JF, Amieva H, et al. omega-3 fatty acids and cognitive decline: modulation by ApoEepsilon4 allele and depression. Neurobiol Aging (2011) 322317(12):e2313–2322. doi: 10.1016/j.neurobiolaging.2010.03.020
43. Antypa N, Van der Does AJ, Smelt AH, Rogers RD. Omega-3 fatty acids (fish-oil) and depression-related cognition in healthy volunteers. J Psychopharmacol (2009) 23(7):831–40. doi: 10.1177/0269881108092120
44. Mazereeuw G, Herrmann N, Oh PI, Ma DW, Wang CT, Kiss A, et al. Omega-3 fatty acids, depressive symptoms, and cognitive performance in patients with coronary artery disease: analyses from a randomized, double-blind, placebo-controlled trial. J Clin Psychopharmacol (2016) 36(5):436–44. doi: 10.1097/JCP.0000000000000565
45. Fontani G, Corradeschi F, Felici A, Alfatti F, Migliorini S, Lodi L. Cognitive and physiological effects of Omega-3 polyunsaturated fatty acid supplementation in healthy subjects. Eur J Clin Invest (2005) 35(11):691–9. doi: 10.1111/j.1365-2362.2005.01570.x
46. Sorensen LB, Damsgaard CT, Dalskov SM, Petersen RA, Egelund N, Dyssegaard CB, et al. Diet-induced changes in iron and n-3 fatty acid status and associations with cognitive performance in 8-11-year-old Danish children: secondary analyses of the optimal well-being, development and health for Danish children through a healthy new Nordic diet school meal study. Br J Nutr (2015) 114(10):1623–37. doi: 10.1017/S0007114515003323
47. de Groot RH, Ouwehand C, Jolles J. Eating the right amount of fish: inverted U-shape association between fish consumption and cognitive performance and academic achievement in Dutch adolescents. Prostaglandins Leukot Essent Fatty Acids (2012) 86(3):113–7. doi: 10.1016/j.plefa.2012.01.002
48. van der Wurff IS, von Schacky C, Berge K, Zeegers MP, Kirschner PA, de Groot RH. Association between blood Omega-3 index and cognition in typically developing Dutch adolescents. Nutrients (2016) 8(1). doi: 10.3390/nu8010013
49. Jiao J, Li Q, Chu J, Zeng W, Yang M, Zhu S. Effect of n-3 PUFA supplementation on cognitive function throughout the life span from infancy to old age: a systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr (2014) 100(6):1422–36. doi: 10.3945/ajcn.114.095315
50. Nelson EB, Van Elswyk ME. Limitations of the review and meta-analysis of the role of n-3 long-chain PUFA supplementation and cognitive function. Am J Clin Nutr (2015) 101(6):1305–6. doi: 10.3945/ajcn.115.107078
51. Widenhorn-Muller K, Schwanda S, Scholz E, Spitzer M, Bode H. Effect of supplementation with long-chain omega-3 polyunsaturated fatty acids on behavior and cognition in children with attention deficit/hyperactivity disorder (ADHD): a randomized placebo-controlled intervention trial. Prostaglandins Leukot Essent Fatty Acids (2014) 91(1-2):49–60. doi: 10.1016/j.plefa.2014.04.004
52. Milte CM, Sinn N, Buckley JD, Coates AM, Young RM, Howe PR. Polyunsaturated fatty acids, cognition and literacy in children with ADHD with and without learning difficulties. J Child Health Care (2011) 15(4):299–311. doi: 10.1177/1367493511403953
53. Chang JP, Su KP, Mondelli V, Pariante CM. Omega-3 polyunsaturated fatty acids in youths with attention deficit hyperactivity disorder: a systematic review and meta-analysis of clinical trials and biological studies. Neuropsychopharmacology (2018b) 43(3):534–45. doi: 10.1038/npp.2017.160
54. Vesco AT, Young AS, Arnold LE, Fristad MA. Omega-3 supplementation associated with improved parent-rated executive function in youth with mood disorders: secondary analyses of the omega 3 and therapy (OATS) trials. J Child Psychol Psychiatry (2018) 59(6):628–36. doi: 10.1111/jcpp.12830
55. Grosso G, Galvano F, Marventano S, Malaguarnera M, Bucolo C, Drago F, et al. Omega-3 fatty acids and depression: scientific evidence and biological mechanisms. Oxid Med Cell Longev (2014a) 2014:313570. doi: 10.1155/2014/313570
56. Song C, Li X, Kang Z, Kadotomi Y. Omega-3 fatty acid ethyl-eicosapentaenoate attenuates IL-1beta-induced changes in dopamine and metabolites in the shell of the nucleus accumbens: involved with PLA2 activity and corticosterone secretion. Neuropsychopharmacology (2007) 32(3):736–44. doi: 10.1038/sj.npp.1301117
57. Goshen I, Kreisel T, Ben-Menachem-Zidon O, Licht T, Weidenfeld J, Ben-Hur T, et al. Brain interleukin-1 mediates chronic stress-induced depression in mice via adrenocortical activation and hippocampal neurogenesis suppression. Mol Psychiatry (2008) 13(7):717–28. doi: 10.1038/sj.mp.4002055
58. Larrieu T, Hilal ML, Fourrier C, De Smedt-Peyrusse V, Sans N, Capuron L, et al. Nutritional omega-3 modulates neuronal morphology in the prefrontal cortex along with depression-related behaviour through corticosterone secretion. Transl Psychiatry (2014) 4:e437. doi: 10.1038/tp.2014.77
59. Mocking RJ, Ruhe HG, Assies J, Lok A, Koeter MW, Visser I. Relationship between the hypothalamic-pituitary-adrenal-axis and fatty acid metabolism in recurrent depression. Psychoneuroendocrinology (2013) 38(9):1607–17. doi: 10.1016/j.psyneuen.2013.01.013
60. Mocking RJ, Verburg HF, Westerink AM, Assies J, Vaz FM, Koeter MW, et al. Fatty acid metabolism and its longitudinal relationship with the hypothalamic-pituitary-adrenal axis in major depression: associations with prospective antidepressant response. Psychoneuroendocrinology (2015) 59:1–13. doi: 10.1016/j.psyneuen.2015.04.027
61. Logan AC. Omega-3 fatty acids and major depression: a primer for the mental health professional. Lipids Health Dis (2004) 3:25. doi: 10.1186/1476-511X-3-25
62. Krishnan V, Nestler EJ. Linking molecules to mood: new insight into the biology of depression. Am J Psychiatry (2010) 167(11):1305–20. doi: 10.1176/appi.ajp.2009.10030434
63. Wager-Smith K, Markou A. Depression: a repair response to stress-induced neuronal microdamage that can grade into a chronic neuroinflammatory condition? Neurosci Biobehav Rev (2011) 35(3):742–64. doi: 10.1016/j.neubiorev.2010.09.010
64. DeFilippis AP, Sperling LS. Understanding omega-3’s. Am Heart J (2006) 151(3):564–70. doi: 10.1016/j.ahj.2005.03.051
65. Owen C, Rees AM, Parker G. The role of fatty acids in the development and treatment of mood disorders. Curr Opin Psychiatry (2008) 21(1):19–24. doi: 10.1097/YCO.0b013e3282f29841
66. Maes M, Mihaylova I, Kubera M, Bosmans E. Why fish oils may not always be adequate treatments for depression or other inflammatory illnesses: docosahexaenoic acid, an omega-3 polyunsaturated fatty acid, induces a Th-1-like immune response. Neuro Endocrinol Lett (2007) 28(6):875–80.
67. Muller N, Myint AM, Schwarz MJ. The impact of neuroimmune dysregulation on neuroprotection and neurotoxicity in psychiatric disorders–relation to drug treatment. Dialogues Clin Neurosci (2009) 11(3):319–32.
68. Freeman MP, Rapaport MH. Omega-3 fatty acids and depression: from cellular mechanisms to clinical care. J Clin Psychiatry (2011) 72(2):258–9. doi: 10.4088/JCP.11ac06830
69. Parker G, Gibson NA, Brotchie H, Heruc G, Rees AM, Hadzi-Pavlovic D. Omega-3 fatty acids and mood disorders. Am J Psychiatry (2006) 163(6):969–78. doi: 10.1176/ajp.2006.163.6.969
70. Suarez EC, Krishnan RR, Lewis JG. The relation of severity of depressive symptoms to monocyte-associated proinflammatory cytokines and chemokines in apparently healthy men. Psychosom Med (2003) 65(3):362–8. doi: 10.1097/01.psy.0000035719.79068.2b
71. Logan AC. Neurobehavioral aspects of omega-3 fatty acids: possible mechanisms and therapeutic value in major depression. Altern Med Rev (2003) 8(4):410–25.
72. Bremner JD, Narayan M, Anderson ER, Staib LH, Miller HL, Charney DS. Hippocampal volume reduction in major depression. Am J Psychiatry (2000) 157(1):115–8. doi: 10.1176/ajp.157.1.115
73. McNamara RK, Carlson SE. Role of omega-3 fatty acids in brain development and function: potential implications for the pathogenesis and prevention of psychopathology. Prostaglandins Leukot Essent Fatty Acids (2006) 75(4-5):329–49. doi: 10.1016/j.plefa.2006.07.010
74. McNamara RK, Vannest JJ, Valentine CJ. Role of perinatal long-chain omega-3 fatty acids in cortical circuit maturation: mechanisms and implications for psychopathology. World J Psychiatry (2015) 5(1):15–34. doi: 10.5498/wjp.v5.i1.15
75. Bourre JM. Roles of unsaturated fatty acids (especially omega-3 fatty acids) in the brain at various ages and during ageing. J Nutr Health Aging (2004) 8(3):163–74.
76. Janssen CI, Kiliaan AJ. Long-chain polyunsaturated fatty acids (LCPUFA) from genesis to senescence: the influence of LCPUFA on neural development, aging, and neurodegeneration. Prog Lipid Res (2014) 53:1–17. doi: 10.1016/j.plipres.2013.10.002
77. Pudell C, Vicente BA, Delattre AM, Carabelli B, Mori MA, Suchecki D, et al. Fish oil improves anxiety-like, depressive-like and cognitive behaviors in olfactory bulbectomised rats. Eur J Neurosci (2014) 39(2):266–74. doi: 10.1111/ejn.12406
78. Carlezon WA Jr., Mague SD, Parow AM, Stoll AL, Cohen BM, Renshaw PF. Antidepressant-like effects of uridine and omega-3 fatty acids are potentiated by combined treatment in rats. Biol Psychiatry (2005) 57(4):343–50. doi: 10.1016/j.biopsych.2004.11.038
79. Huang SY, Yang HT, Chiu CC, Pariante CM, Su KP. Omega-3 fatty acids on the forced-swimming test. J Psychiatr Res (2008) 42(1):58–63. doi: 10.1016/j.jpsychires.2006.09.004
80. Song C, Zhang XY, Manku M. Increased phospholipase A2 activity and inflammatory response but decreased nerve growth factor expression in the olfactory bulbectomized rat model of depression: effects of chronic ethyl-eicosapentaenoate treatment. J Neurosci (2009) 29(1):14–22. doi: 10.1523/JNEUROSCI.3569-08.2009
81. Song C, Wang H. Cytokines mediated inflammation and decreased neurogenesis in animal models of depression. Prog Neuropsychopharmacol Biol Psychiatry (2011) 35(3):760–8. doi: 10.1016/j.pnpbp.2010.06.020
82. Bartl J, Walitza S, Grunblatt E. Enhancement of cell viability after treatment with polyunsaturated fatty acids. Neurosci Lett (2014) 559:56–60. doi: 10.1016/j.neulet.2013.11.023
83. Delion S, Chalon S, Guilloteau D, Besnard JC, Durand G. alpha-Linolenic acid dietary deficiency alters age-related changes of dopaminergic and serotoninergic neurotransmission in the rat frontal cortex. J Neurochem (1996) 66(4):1582–91. doi: 10.1046/j.1471-4159.1996.66041582.x
84. Delion S, Chalon S, Guilloteau D, Lejeune B, Besnard JC, Durand G. Age-related changes in phospholipid fatty acid composition and monoaminergic neurotransmission in the hippocampus of rats fed a balanced or an n-3 polyunsaturated fatty acid-deficient diet. J Lipid Res (1997) 38(4):680–9.
85. Zimmer L, Delion-Vancassel S, Durand G, Guilloteau D, Bodard S, Besnard JC, et al. Modification of dopamine neurotransmission in the nucleus accumbens of rats deficient in n-3 polyunsaturated fatty acids. J Lipid Res (2000) 41(1):32–40. http://www.jlr.org/content/41/1/32.long
86. Song C, Horrobin D. Omega-3 fatty acid ethyl-eicosapentaenoate, but not soybean oil, attenuates memory impairment induced by central IL-1beta administration. J Lipid Res (2004) 45(6):1112–21. doi: 10.1194/jlr.M300526-JLR200
87. Yao JK, Magan S, Sonel AF, Gurklis JA, Sanders R, Reddy RD. Effects of omega-3 fatty acid on platelet serotonin responsivity in patients with schizophrenia. Prostaglandins Leukot Essent Fatty Acids (2004) 71(3):171–6. doi: 10.1016/j.plefa.2004.03.011
88. Chalon S. Omega-3 fatty acids and monoamine neurotransmission. Prostaglandins Leukot Essent Fatty Acids (2006) 75(4-5):259–69. doi: 10.1016/j.plefa.2006.07.005
89. McNamara RK, Able J, Liu Y, Jandacek R, Rider T, Tso P, et al. Omega-3 fatty acid deficiency during perinatal development increases serotonin turnover in the prefrontal cortex and decreases midbrain tryptophan hydroxylase-2 expression in adult female rats: dissociation from estrogenic effects. J Psychiatr Res (2009) 43(6):656–63. doi: 10.1016/j.jpsychires.2008.09.011
90. Hibbeln JR, Linnoila M, Umhau JC, Rawlings R, George DT, Salem N Jr. Essential fatty acids predict metabolites of serotonin and dopamine in cerebrospinal fluid among healthy control subjects, and early- and late-onset alcoholics. Biol Psychiatry (1998a) 44(4):235–42. doi: 10.1016/s0006-3223(98)00141-3
91. Hibbeln JR, Umhau JC, Linnoila M, George DT, Ragan PW, Shoaf SE, et al. A replication study of violent and nonviolent subjects: cerebrospinal fluid metabolites of serotonin and dopamine are predicted by plasma essential fatty acids. Biol Psychiatry (1998b) 44(4):243–9. doi: 10.1016/s0006-3223(98)00143-7
92. Litman BJ, Niu SL, Polozova A, Mitchell DC. The role of docosahexaenoic acid containing phospholipids in modulating G protein-coupled signaling pathways: visual transduction. J Mol Neurosci (2001) 16(2-3):237–42. doi: 10.1385/JMN:16:2-3:237discussion279-284.
93. Grossfield A, Feller SE, Pitman MC. A role for direct interactions in the modulation of rhodopsin by omega-3 polyunsaturated lipids. Proc Natl Acad Sci U.S.A. (2006) 103(13):4888–93. doi: 10.1073/pnas.0508352103
94. Bowen RA, Clandinin MT. Dietary low linolenic acid compared with docosahexaenoic acid alter synaptic plasma membrane phospholipid fatty acid composition and sodium-potassium ATPase kinetics in developing rats. J Neurochem (2002) 83(4):764–74. doi: 10.1046/j.1471-4159.2002.01156.x
95. Said T, Tremblay-Mercier J, Berrougui H, Rat P, Khalil A. Effects of vegetable oils on biochemical and biophysical properties of membrane retinal pigment epithelium cells. Can J Physiol Pharmacol (2013) 91(10):812–7. doi: 10.1139/cjpp-2013-0036
96. Joyce NR, Schuler MS, Hadland SE, Hatfield LA. Variation in the 12-month treatment trajectories of children and adolescents after a diagnosis of depression. JAMA Pediatr (2018) 172(1):49–56. doi: 10.1001/jamapediatrics.2017.3808
97. Newman TB. A black-box warning for antidepressants in children? N Engl J Med (2004) 351(16):1595–8. doi: 10.1056/NEJMp048279
98. Sharma T, Guski LS, Freund N, Gotzsche PC. Suicidality and aggression during antidepressant treatment: systematic review and meta-analyses based on clinical study reports. BMJ (2016) 352:i65. doi: 10.1136/bmj.i65
99. Gibbons RD, Brown CH, Hur K, Davis J, Mann JJ. Suicidal thoughts and behavior with antidepressant treatment: reanalysis of the randomized placebo-controlled studies of fluoxetine and venlafaxine. Arch Gen Psychiatry (2012) 69(6):580–7. doi: 10.1001/archgenpsychiatry.2011.2048
100. Barry CL, Busch SH. News coverage of FDA warnings on pediatric antidepressant use and suicidality. Pediatrics (2010) 125(1):88–95. doi: 10.1542/peds.2009-0792
101. Poznanski EO, Cook SC, Carroll BJ. A depression rating scale for children. Pediatrics (1979) 64(4):442–50.
102. Poznanski E, Mokros H. Children’s Depression Rating Scale-Revised (CDRS-R). Los Angeles:WPS (1996).
103. Grosso G, Micek A, Marventano S, Castellano S, Mistretta A, Pajak A, et al. Dietary n-3 PUFA, fish consumption and depression: a systematic review and meta-analysis of observational studies. J Affect Disord (2016) 205:269–81. doi: 10.1016/j.jad.2016.08.011
104. Damico KE, Stoll AL, Marangell LB, Cohen BM. How blind is double-blind? A study of fish oil versus placebo. Prostaglandins Leukot Essent Fatty Acids (2002) 66(4):393–5. doi: 10.1054/plef.2002.0364
105. DGPPN, BÄK, KBV, AWMF, AkdÄ, BPtK, , et al. (Hrsg) für die Leitliniengruppe Unipolare Depression*. S3-Leitlinie/Nationale VersorgungsLeitlinie Unipolare Depression - Langfassung, 1. Auflage. Version 5 (2009). doi: 10.6101/AZQ/000239
106. Jeansen S, Witkamp RF, Garthoff JA, van Helvoort A, Calder PC. Fish oil LC-PUFAs do not affect blood coagulation parameters and bleeding manifestations: analysis of 8 clinical studies with selected patient groups on omega-3-enriched medical nutrition. Clin Nutr (2018) 37(3):948–57. doi: 10.1016/j.clnu.2017.03.027
107. Pasco JA, Nicholson GC, Williams LJ, Jacka FN, Henry MJ, Kotowicz MA. Association of high-sensitivity C-reactive protein with de novo major depression. Br J Psychiatry (2010) 197(5):372–7. doi: 10.1192/bjp.bp.109.076430
108. Azar R, Nolan RP, Stewart DE. Listening to the heart-brain talk: persistent depressive symptoms are associated with hsCRP in apparently healthy individuals at high risk for coronary artery disease. Eur J Prev Cardiol (2012) 19(4):857–63. doi: 10.1177/1741826711415720
109. Duivis HE, Kupper N, Vermunt JK, Penninx BW, Bosch NM, Riese H, et al. Depression trajectories, inflammation, and lifestyle factors in adolescence: The TRacking Adolescents’ Individual Lives Survey. Health Psychol (2015) 34(11):1047–57. doi: 10.1037/hea0000210
110. Plener PL, Grieb J, Sprober N, Straub J, Schneider A, Keller F, et al. Convergence of children’s depression rating scale-revised scores and clinical diagnosis in rating adolescent depressive symptomatology. Ment Illn (2012) 4(1):e7. doi: 10.4081/mi.2012.e7
111. March JS, Silva S, Petrycki S, Curry J, Wells K, Fairbank J, et al. The Treatment for Adolescents With Depression Study (TADS): long-term effectiveness and safety outcomes. Arch Gen Psychiatry (2007) 64(10):1132–43. doi: 10.1001/archpsyc.64.10.1132
112. Keller F, Grieb J, Ernst M, Sprober N, Fegert JM, Kolch M. [Children’s Depression Rating Scale-Revised (CDRS-R): development of a German version and psychometric properties in a clinical sample]. Z Kinder Jugendpsychiatr Psychother (2011) 39(3):179–85. doi: 10.1024/1422-4917/a000090
113. Emslie GJ, Heiligenstein JH, Wagner KD, Hoog SL, Ernest DE, Brown E, et al. Fluoxetine for acute treatment of depression in children and adolescents: a placebo-controlled, randomized clinical trial. J Am Acad Child Adolesc Psychiatry (2002) 41(10):1205–15. doi: 10.1097/00004583-200210000-00010
114. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry (1997) 36(7):980–8. doi: 10.1097/00004583-199707000-00021
115. Stiensmeier-Pelster JM, Schürmann M, Duda K. Depressions-Inventar für Kinder und Jugendliche (DIKJ). Handanweisung (2., überarb. und neunormierte Auflage). Göttingen:Hogrefe (2000).
116. Beck AT, Weissman A, Lester D, Trexler L. The measurement of pessimism: the hopelessness scale. J Consult Clin Psychol (1974) 42(6):861–5. doi: 10.1037/h0037562
117. Leyfer OT, Ruberg JL, Woodruff-Borden J. Examination of the utility of the Beck Anxiety Inventory and its factors as a screener for anxiety disorders. J Anxiety Disord (2006) 20(4):444–58. doi: 10.1016/j.janxdis.2005.05.004
118. Reynolds W. SIQ, Suicidal Ideation Questionnaire: Professional Manual. Florida: Psychological Assessment Resources (1998).
119. Bastien CH, Vallieres A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med (2001) 2(4):297–307. doi: 10.1016/s1389-9457(00)00065-4
120. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety (2003) 18(2):76–82. doi: 10.1002/da.10113
121. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav (1983) 24(4):385–96.
122. Ravens-Sieberer U, Gosch A, Rajmil L, Erhart M, Bruil J, Power M, et al. The KIDSCREEN-52 quality of life measure for children and adolescents: psychometric results from a cross-cultural survey in 13 European countries. Value Health (2008) 11(4):645–58. doi: 10.1111/j.1524-4733.2007.00291.x
123. Goodman R, Meltzer H, Bailey V. The strengths and difficulties questionnaire: a pilot study on the validity of the self-report version. Eur Child Adolesc Psychiatry (1998) 7(3):125–30. doi: 10.1007/s007870050057
124. Kröger C, del Pozo MA, Kosfelder J, Allroggen M, Grabowski G, Legenbauer T. Erfassung von Impulsivität und emotionaler Dysregulation bei Jugendlichen mit Borderline-Persönlichkeitsstörung. Diagnostica (2017) 63(4):297–308. doi: 10.1026/0012-1924/a000184
125. Guy W. Clinical Global Impression (CGI) Scale, Modified. Washington DC:American Psychiatric Association (2000).
126. Schaffer D, Gould MS, Brasic J, Ambrosini P, Fisher P, Bird H, et al. A children’s global assessment scale (CGAS). Arch Gen Psychiatry (1983) 40:1228–31. doi: 10.1001/archpsyc.1983.01790100074010
127. Gowers SG, Harrington RC, Whitton A, Lelliott P, Beevor A, Wing J, et al. Brief scale for measuring the outcomes of emotional and behavioural disorders in children. Health of the Nation Outcome Scales for children and Adolescents (HoNOSCA). Br J Psychiatry (1999) 174:413–6. doi: 10.1192/bjp.174.5.413
128. Gioia GA, Isquith PK, Guy SC, Kenworthy L. BRIEF: Behavior rating inventory of executive function. Lutz, FL:Psychological Assessment Resources (2000).
129. Helmstadter C, Lendt M, Lux S. Verbaler Lern- und Merkfähigkeitstest: VLMT, Manual. Gottingen:Beltz Test GmbH (2001).
130. Wechsler D. Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV). San Antonio, TX:The Psychological Corporation (2003).
131. de Sonneville L. Amsterdam Neuropsychological Tasks: A computer-aided assessment program. Cogn Ergon Clin Asses Comput Assist Learn: Comput In Psychol (1999) 6:187–203.
132. Aschenbrenner S, Tucha O, Lange KW. Regensuberger Wortflüssigkeits-Test: RWT. Göttingen:Hogrefe (2000).
133. Reynolds R, Kamphaus C. Reynolds Intellectual Assessment Scales and Reynolds Intellectual Screening Test Professional Manual. Lutz, FL.: Psychological Assessment Resources (2003).
134. Hodgson K, Uher R, Crawford AA, Lewis G, O’Donovan MC, Keers R, et al. Genetic predictors of antidepressant side effects: a grouped candidate gene approach in the Genome-Based Therapeutic Drugs for Depression (GENDEP) study. J Psychopharmacol (2014) 28(2):142–50. doi: 10.1177/0269881113517957
135. Mahler C, Hermann K, Horne R, Ludt S, Haefeli WE, Szecsenyi J, et al. Assessing reported adherence to pharmacological treatment recommendations. Translation and evaluation of the Medication Adherence Report Scale (MARS) in Germany. J Eval Clin Pract (2010) 16(3):574–9. doi: 10.1111/j.1365-2753.2009.01169.x
136. Sublette ME, Segal-Isaacson CJ, Cooper TB, Fekri S, Vanegas N, Galfalvy HC, et al. Validation of a food frequency questionnaire to assess intake of n-3 polyunsaturated fatty acids in subjects with and without major depressive disorder. J Am Diet Assoc (2011b) 111(1):117–123 e111-112. doi: 10.1016/j.jada.2010.10.007
137. Marshall WA, Tanner JM.Variations in the pattern of pubertal changes in boys. Arch Dis Child (1970) 45(239):13–23. doi: 10.1136/adc.45.239.13
138. Bernstein DP, Ahluvalia T, Pogge D, Handelsman L. Validity of the Childhood Trauma Questionnaire in an adolescent psychiatric population. J Am Acad Child Adolesc Psychiatry (1997) 36(3):340–8. doi: 10.1097/00004583-199703000-00012
139. Olweus D. The Revised Olweus Bully/Victim Questionnaire. Bergern, Norway:Mimeo, Research Center of Health Promotion (HEMIL), University of Bergen (1996).
140. Drechsler R, Steinhausen H-C. Verhaltensinventar zur Beurteilung exekutiver Funktionen BRIEF. Deutschsprachige Adaption des Behavior Rating Inventory of Executive Function. Bern:Verlag Hans Huber (2013).
141. Bridge JA, Birmaher B, Iyengar S, Barbe RP, Brent DA.Placebo response in randomized controlled trials of antidepressants for pediatric major depressive disorder. Am J Psychiatry (2009) 166(1):42–9. doi: 10.1176/appi.ajp.2008.08020247
142. Parellada M, Moreno C, Moreno M, Espliego A, de Portugal E, Arango C. Placebo effect in child and adolescent psychiatric trials. Eur Neuropsychopharmacol (2012) 22(11):787–99. doi: 10.1016/j.euroneuro.2011.09.007
143. Treatment for Adolescents With Depression Study, T..Treatment for Adolescents With Depression Study (TADS): rationale, design, and methods. J Am Acad Child Adolesc Psychiatry (2003) 42(5):531–42. doi: 10.1097/01.CHI.0000046839.90931.0D
144. Hallahan B, Ryan T, Hibbeln JR, Murray IT, Glynn S, Ramsden CE, et al. Efficacy of omega-3 highly unsaturated fatty acids in the treatment of depression. Br J psychiatry: J Ment Sci (2016a) 209(3):192–201. doi: 10.1192/bjp.bp.114.160242
145. Mocking RJT, Harmsen I, Assies J, Koeter MWJ, Ruhe HG, Schene AH.Meta-analysis and meta-regression of omega-3 polyunsaturated fatty acid supplementation for major depressive disorder. Trans Psychiatry (2016b) 6:e756. doi: 10.1038/tp.2016.29
146. Liao Y, Xie B, Zhang H, He Q, Guo L, Subramaniapillai M.Efficacy of omega-3 PUFAs in depression: a meta-analysis. Trans Psychiatry (2019) 9(1):190. doi: 10.1038/s41398-019-0515-5
147. Jolani S, Frank LE, van Buuren S.Dual imputation model for incomplete longitudinal data. Br J Math Stat Psychol (2014) 67(2):197–212. doi: 10.1111/bmsp.12021
148. Chang CH, Tseng PT, Chen NY, Lin PC, Lin PY, Chang JP, et al. Safety and tolerability of prescription omega-3 fatty acids: a systematic review and meta-analysis of randomized controlled trials. Prostaglandins Leukot Essent Fatty Acids (2018a) 129:1–12. doi: 10.1016/j.plefa.2018.01.001
149. Corrigan PW, Morris SB, Michaels PJ, Rafacz JD, Rusch N. Challenging the public stigma of mental illness: a meta-analysis of outcome studies. Psychiatr Serv (2012) 63(10):963–73. doi: 10.1176/appi.ps.201100529
Keywords: omega-3 fatty acids, clinical trial protocol, randomized controlled trial, pediatric depression, treatment of depression
Citation: Häberling I, Berger G, Schmeck K, Held U and Walitza S (2019) Omega-3 Fatty Acids as a Treatment for Pediatric Depression. A Phase III, 36 Weeks, Multi-Center, Double-Blind, Placebo-Controlled Randomized Superiority Study. Front. Psychiatry 10:863. doi: 10.3389/fpsyt.2019.00863
Received: 16 July 2019; Accepted: 04 November 2019;
Published: 27 November 2019.
Edited by:
Amit Anand, Case Western Reserve University, United StatesReviewed by:
Khemraj Hirani, University of Miami, United StatesSerafim Carvalho, Cooperativa de Ensino Superior Politécnico e Universitário, Portugal
Copyright © 2019 Häberling, Berger, Schmeck, Held and Walitza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gregor Berger, Z3JlZ29yLmJlcmdlckBwdWsuemguY2g=