 Cosme Alvarado-Esquivel
Cosme Alvarado-Esquivel Sergio Estrada-Martínez
Sergio Estrada-Martínez Alma Rosa Pérez-Alamos
Alma Rosa Pérez-Alamos- 1Faculty of Medicine and Nutrition, Juárez University of Durango State, Durango, Mexico
- 2Institute for Scientific Research “Dr. Roberto Rivera Damm,” Juárez University of Durango State, Durango, Mexico
Background and Aims: Infection with the parasite Toxoplasma gondii has been associated with bipolar disorder in several countries other than Mexico. Therefore, we sought to determine the association between seropositivity to T. gondii and bipolar disorder in a Mexican population.
Methods: We performed an age- and gender-matched case–control study of 66 patients with bipolar disorder (WHO International Classification of Diseases, 10th Revision code: F31) and 396 subjects without this disorder from the general population. Anti-Toxoplasma immunoglobulin G (IgG) and IgM antibodies were determined using commercially available enzyme-linked immunoassays.
Results: Six (9.1%) of the 66 patients with bipolar disorder and 22 (5.6%) of the 396 controls had anti–T. gondii IgG antibodies (odds ratio [OR] = 1.7; 95% confidence interval [CI] = 0.66–4.36; P = 0.26). Stratification by gender and age did not show a difference in seroprevalence between cases and controls. The frequency of high (> 150 international units/ml) anti–T. gondii IgG levels was similar in cases (n = 2) and in controls (n = 12) (OR = 1.0; 95% CI = 0.21–4.57; P = 1.00). Stratification by International Classification of Diseases, 10th Revision F31 codes showed that patients with F31.3 code had a higher seroprevalence of T. gondii infection than their age- and gender-matched controls (OR = 16.4; 95% CI = 1.25–215.09; P = 0.04). None of the six anti–T. gondii IgG–seropositive patients with bipolar disorder and 4 (18.2%) of the 22 anti–T. gondii IgG–seropositive controls had anti–T. gondii IgM antibodies (P = 0.54).
Conclusions: Our results suggest that T. gondii seropositivity is not associated with bipolar disorder in general. However, a specific type of bipolar disorder (F31.3) might be associated with T. gondii seropositivity. Further research to elucidate the role of T. gondii infection in bipolar disorder is needed.
Introduction
Toxoplasma gondii is one of the most successful intracellular parasites with strategies to avoid destruction by the host and to obtain lifelong survival (1). This pathogen that infects over one-third of the global human population invades and chronically persists in the central nervous system of the infected host (2). Most human infections are mild or asymptomatic; however, T. gondii infection can result in life-threatening disease in immunocompromised individuals (3). Primary infection with T. gondii in pregnant women may cause abortions and central nervous and eye disease in the fetus leading to disability (4). Chronic infection in the brain correlates with changes in neuronal architecture, neurochemistry, and behavior suggesting that chronic infection is not without consequence (5). Prevalence of infection with T. gondii has been found higher in psychiatric patients than in controls (6–8). Infections with T. gondii have been associated with suicide attempts (9–11), mixed anxiety and depressive disorder (12), schizophrenia (13–15), depression (16), and obsessive–compulsive disorder (13). There is increasing evidence of an association between infection with T. gondii and bipolar disorder. Studies in several countries have found a higher seroprevalence of T. gondii infection in patients suffering from bipolar disorder than in controls (17–22). In contrast, no association between maternal infection with T. gondii and risk of bipolar disorder in offspring was found (23, 24). Bipolar disorder is a public health problem around the worldwide, and about 1% of the population suffers from this disease (25, 26). To the best of our knowledge, the association between T. gondii infection and bipolar disorder has not been studied in Mexican populations. Therefore, we sought to determine the association between seropositivity to T. gondii infection and bipolar disorder in Durango City, Mexico.
Materials and Methods
Study Design and Population
Through an age- and gender-matched case–control study design, we studied 66 psychiatric patients suffering from bipolar disorder attended in a public hospital of mental health (Hospital of Mental Health “Dr. Miguel Vallebueno” of the Secretary of Health) in the northern Mexican city of Durango and 396 control subjects without bipolar disorder from the general population of the same city. Inclusion criteria for enrollment of cases were (1) patients suffering from bipolar disorder diagnosed in the Hospital of Mental Health “Dr. Miguel Vallebueno”; (2) 18 years or older; and (3) who voluntarily accepted to participate in the survey. Bipolar disorder was diagnosed by psychiatrists and was classified according to the classification of mental and behavioral disorders of the International Classification of Diseases, 10th Revision (ICD-10) (https://www.icd10data.com/ICD10CM/Codes/F01-F99/F30-F39/F31-). Bipolar disorder has the ICD-10 code F31. Blood sampling of subjects was performed at the time that corresponds to the most recent diagnostic ICD-10 code F31. Of the 66 patients with bipolar disorder, 33 (50.0%) were females and 33 (50.0%) were males. Their mean age was 40.05 ± 14.48 (range, 20–76) years. Control subjects were obtained from the general population of Durango City, selected at random, and matched with cases for gender and age (± 2 years). Inclusion criteria for enrollment of controls were (1) subjects of the general population of Durango City without bipolar disorder; (2) 18 years or older; and (3) who voluntarily accepted to participate in the survey. Of the 396 controls, 198 (50.0%) were females and 198 (50.0%) were males. Mean age in controls subjects was 40.05 ± 14.39 (range, 20–77) years. Age and gender in cases were similar to those in controls (P = 0.99, and P = 1.0, respectively). The socioeconomic status of participants was not included in the matching of cases and controls because this characteristic has not been impacting on the seroprevalence of T. gondii infection in the region.
Laboratory Tests for Detection of Anti–T. Gondii Immunoglobulin G and Immunoglobulin M Antibodies
Each participant provided a blood sample. After centrifugation of blood samples, serum samples were obtained and kept frozen at −20°C until analyzed. Serum samples of participants were analyzed for detection of anti–T. gondii immunoglobulin G (IgG) antibodies with the commercially available enzyme immunoassay (EIA) kit “Toxoplasma IgG” (Diagnostic Automation/Cortez Diagnostics Inc., Woodland Hills, CA, USA). This assay has a cutoff of ≥8 international units (IU)/ml of anti–T. gondii IgG antibody. Serum samples of participants who were seropositive for anti–T. gondii IgG antibodies were further examined for detection of anti–T. gondii IgM antibodies by the commercially available EIA “Toxoplasma IgM” kit (Diagnostic Automation/Cortez Diagnostics Inc.). All IgG and IgM assays were performed according to the instructions of the manufacturer.
Statistical Analysis
Statistical analysis of the data was performed with the aid of the software Epi Info version 7 and the SPSS version 15.0 (SPSS Inc., Chicago, IL). We calculated the sample size using the following values: a reference seroprevalence of T. gondii infection of 6.1% (27) as the expected frequency of exposure in controls, a power of 80%, a confidence level of 95%, a 1:6 proportion of cases and controls, and an odds ratio (OR) of 3.5. We used this high OR because some population groups in Durango City (12, 15) have about threefold or fourfold higher seroprevalences of T. gondii infection than the 6.1% seroprevalence found in the general population in the same city (27). However, using these values, an association can be detected even below a 3.5 OR. The result of the sample size calculation was 54 cases and 320 controls. The Student t test was used to compare the ages among cases and controls. We used the two-tailed Pearson χ2 test or the Fisher exact test (when values were small) to determine the association of T. gondii infection and bipolar disorder. In addition, we calculated the OR and 95% confidence interval (CI), and statistical significance was set at P < 0.05.
Ethical Aspects
This project was approved by the Ethics Committee of the General Hospital of the Secretary of Health in Durango City, Mexico. Subjects were invited to voluntarily participate in the study, and they were informed about the purpose and procedures of this survey. A written informed consent was obtained from each participant.
Results
Six (9.1%) of the 66 patients with bipolar disorder and 22 (5.6%) of the 396 controls had anti–T. gondii IgG antibodies. The difference in seroprevalence of T. gondii infection between cases and controls was not statistically significant (OR = 1.7; 95% CI = 0.66–4.36; P = 0.26). Further analysis with stratification by sex and age did not show a difference in seroprevalence between cases and controls (Table 1). Of the six anti–T. gondii IgG–positive cases, two (33.3%) had IgG levels higher than 150 IU/ml, two (33.3%) between 100 and 150 IU/ml, and two (33.3%) between 8 and 99 IU/ml. On the other hand, of the 22 anti–T. gondii IgG–positive controls, 12 (54.5%) had IgG levels higher than 150 IU/ml, two (9.1%) between 100 and 150 IU/ml, and 8 (36.4%) between 8 and 99 IU/ml. The frequency of high (> 150 IU/ml) anti–T. gondii IgG levels was similar in cases and controls (OR = 1.0; 95% CI = 0.21–4.57; P = 1.00).
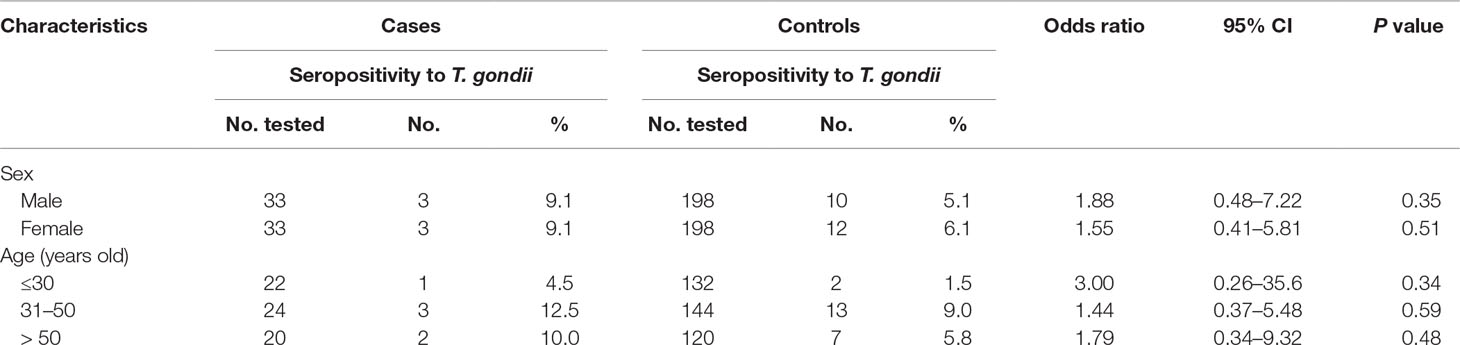
Table 1 Stratification by sex and age in cases and controls and seropositivity rates to Toxoplasma gondii.
Stratification by ICD-10 F31 diagnosis groups showed that patients suffering from bipolar disorder, with current episode depressed, of mild or moderate severity (F31.3) had a higher seroprevalence of anti–T. gondii IgG antibodies than their age- and gender-matched controls (OR = 16.4; 95% CI = 1.25–215.09; P = 0.04) (Table 2). All but one of the patients had only one psychiatric illness (bipolar disorder). One patient had two psychiatric illnesses: bipolar disorder and schizoaffective disorder.
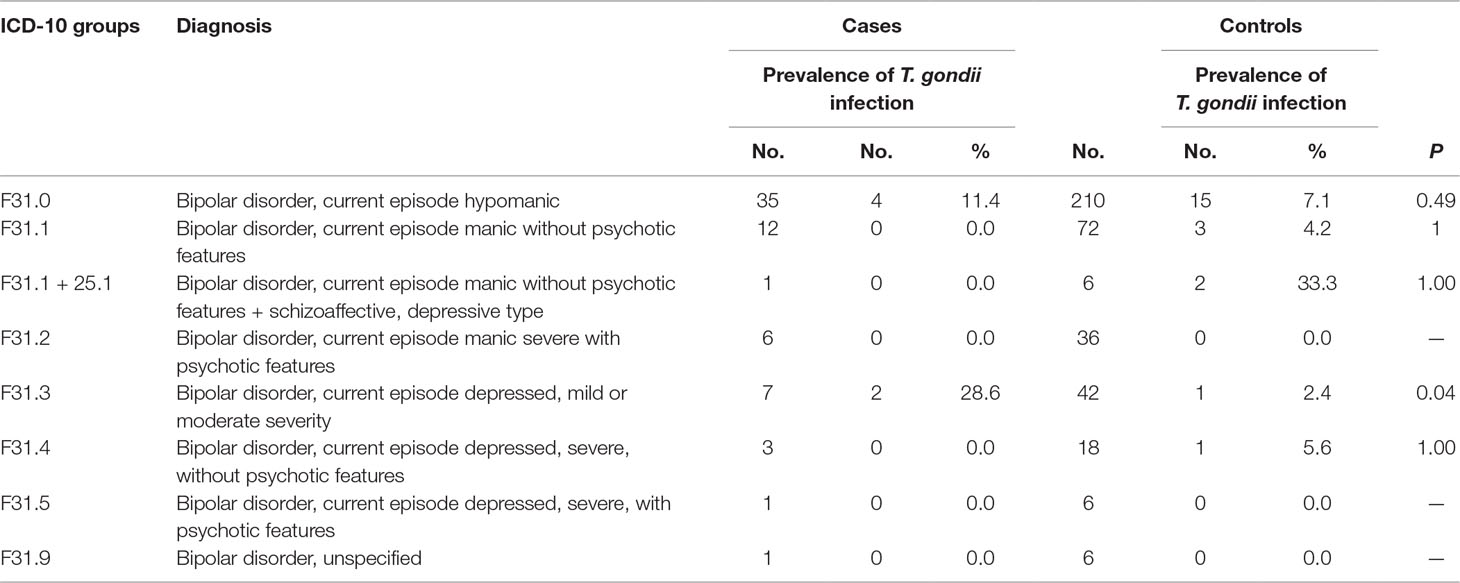
Table 2 Comparison of Toxoplasma gondii seropositivity rates in cases and controls according to International Classification of Diseases, 10th Revision (ICD-10) diagnosis groups.
Concerning anti–T. gondii IgM seropositivity, none of the six anti–T. gondii IgG–seropositive patients with bipolar disorder had anti–T. gondii IgM antibodies. In contrast, anti–T. gondii IgM antibodies were found in 4 (18.2%) of the 22 anti–T. gondii IgG–seropositive controls. No statistically significant difference in anti–T. gondii IgM seropositivity rates in cases and in controls was found (P = 0.54).
Discussion
After infection, T. gondii disseminates to a large variety of organs in the body including brain (28). Studies in several countries other than Mexico have reported an association between seropositivity to T. gondii and bipolar disorder. However, we are not aware of any study about this association in Mexico. Therefore, we performed this case-control study to determine whether seropositivity to T. gondii is associated with bipolar disorder in a group of patients in the northern Mexican city of Durango. We found that patients suffering from bipolar disorder had a similar seroprevalence of T. gondii infection to age- and gender-matched control subjects. We did not find a difference in IgG or IgM seropositivity rates among cases and controls. In addition, the frequency of high levels of anti–T. gondii IgG antibodies was similar in cases and controls. Therefore, our results based on IgG and IgM seroprevalence and IgG serointensity suggest that T. gondii infection is not associated with bipolar disorder in patients in Durango, Mexico, in general. The seroprevalence (9.1%) found in patients with bipolar disorders is comparable with the seroprevalences of T. gondii infection reported in general population (6.1%) (27) and blood donors (7.1%) in the same Durango City (29). Furthermore, the seroprevalence found in patients suffering from bipolar disorder is lower than seroprevalences reported in high-risk population groups including waste pickers (21.1%) (30), schizophrenic patients (20%) (15), and inmates (21.1%) (31) also in the same Durango City. This comparison further supports the lack of association of T. gondii infection and bipolar disorder in our setting. However, we found an association between T. gondii seropositivity and patients suffering from bipolar disorder, with current episode depressed, of mild or moderate severity (F31.3). This association should be interpreted with caution since the 95% CI obtained was very wide. The sample size of patients with this code was very small, and further studies with large sample sizes of these patients to elucidate the association should be conducted. It is not clear why T. gondii infection was not associated with bipolar disorder in this study in general. In fact, the lack of association between T. gondii infection and bipolar disorder found in the current study was unexpected. Other studies have reported a higher seroprevalence of T. gondii infection in patients suffering from bipolar disorder than in control subjects. These findings have been reported in Saudi Arabia (19), France (20, 32), the United States (22), and Ethiopia (17). In a meta-analysis of 50 studies about the association of seroprevalence of T. gondii infection and psychiatric disorders, researchers found a significant OR with IgG antibodies in bipolar disorder (13). We are not aware of a previous age-and gender-matched case–control study that reported a lack of association between T. gondii infection and bipolar disorder. Differences in the association between T. gondii infection and bipolar disorder among the studies could be explained by differences in the characteristics of the patients studied including severity and duration of the disease, presence of concomitant psychiatric disease as schizophrenia, or duration of the infection (acute or chronic). All T. gondii–seropositive patients in our study had latent infection, and it is not clear whether clinical features of bipolar disorder might be associated only with acute T. gondii infection or chronic infection or both. We studied only patients attended in a public hospital, whereas other researchers have studied a population-based sample of subjects (22).
The present study has some limitations: the study population of patients with bipolar disorder was enrolled in only a psychiatric hospital, we studied only adult patients, and the sample size of specific ICD-10 F31 diagnosis groups was small. Additional studies to assess the association between T. gondii seropositivity and bipolar disorder should enroll not only adults but also younger patients in several hospitals and include a large sample size of patients with ICD-10 F31 diagnosis codes. Our study was performed in a low T. gondii seroprevalence population, and this condition may help to identify only clear associations when using small sample sizes, as we found in previous studies of 50 schizophrenic patients (15) and 65 patients with mixed anxiety and depressive disorder (12). However, it is possible that using a larger sample size may help to identify an association between T. gondii infection and bipolar disorder in our region.
Conclusions
Our results suggest that T. gondii seropositivity is not associated with bipolar disorder in general. This finding conflicts with those reported in previous studies. However, a specific type of bipolar disorder (F31.3) might be associated with T. gondii seropositivity. Further research to elucidate the role of T. gondii infection in bipolar disorder is needed. Data of the present study can be useful for further research to determine the association between T. gondii infection and bipolar disorder using a meta-analysis design.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the General Hospital of the Secretary of Health in Durango City, Mexico. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CA-E conceived and designed the study, obtained blood samples, performed laboratory tests and data analysis, and wrote the manuscript. SE-M performed the statistical analysis and reviewed the manuscript. AP-A obtained blood samples, summited questionnaires, and reviewed the manuscript.
Funding
This study was financially supported by the Secretary of Public Education, Mexico (grant no. DSA/103.5/14/11311).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Zhu W, Li J, Pappoe F, Shen J, Yu L. Strategies developed by toxoplasma gondii to survive in the host. Int J Bipolar Disord (2019) 10:899. doi: 10.3389/fmicb.2019.00899
2. Schlüter D, Barragan A. Advances and challenges in understanding cerebral toxoplasmosis. Front Microbiol (2019) 10:242. doi: 10.3389/fimmu.2019.00242
3. Lima TS, Lodoen MB. Mechanisms of human innate immune evasion by toxoplasma gondii. Front Cell Infect Microbiol (2019) 9:103. doi: 10.3389/fcimb.2019.00103
4. Fallahi S, Rostami A, Nourollahpour Shiadeh M, Behniafar H, Paktinat S. An updated literature review on maternal-fetal and reproductive disorders of Toxoplasma gondii infection. J Microsc Ultrastruct (2018) 47(3):133–40. doi: 10.1016/j.jogoh.2017.12.003
5. Sinai AP, Watts EA, Dhara A, Murphy RD, Gentry MS, Patwardhan A. Reexamining chronic toxoplasma gondii infection: surprising activity for a “dormant” parasite. Curr Clin Microbiol Rep (2016) 3(4):175–85. doi: 10.1007/s40588-016-0045-3
6. Cong W, Dong W, Bai L, Wang XY, Ni XT, Qian AD, et al. Seroprevalence and associated risk factors of Toxoplasma gondii infection in psychiatric patients: a case-control study in eastern China. Epidemiol Infect (2015) 143(14):3103–9. doi: 10.1017/S0950268814003835
7. James BO, Agbonile IO, Okolo M, Lawani AO, Omoaregba JO. Prevalence of Toxoplasma gondii infection among individuals with severe mental illness in Nigeria: a case control study. Psychiatry Res (2013) 107(4):189–93. doi: 10.1179/2047773213Y.0000000093
8. Alvarado-Esquivel C, Alanis-Quiñones OP, Arreola-Valenzuela MA, Rodríguez-Briones A, Piedra-Nevarez LJ, Duran-Morales E, et al. Seroepidemiology of Toxoplasma gondii infection in psychiatric inpatients in a northern Mexican city. BMC Infect Dis (2006) 19:6:178. doi: 10.1186/1471-2334-6-178
9. Bak J, Shim SH, Kwon YJ, Lee HY, Kim JS, Yoon H, et al. The association between suicide attempts and toxoplasma gondii infection. Clin Psychopharmacol Neurosci (2018) 16(1):95–102. doi: 10.9758/cpn.2018.16.1.95
10. Alvarado-Esquivel C, Sánchez-Anguiano LF, Arnaud-Gil CA, López-Longoria JC, Molina-Espinoza LF, Estrada-Martínez S, et al. Toxoplasma gondii infection and suicide attempts: a case-control study in psychiatric outpatients. J Parasitol (2013) 201(11):948–52. doi: 10.1097/NMD.0000000000000037
11. Ling VJ, Lester D, Mortensen PB, Langenberg PW, Postolache TT. Toxoplasma gondii seropositivity and suicide rates in women. J Parasitol (2011) 199(7):440–4. doi: 10.1097/NMD.0b013e318221416e
12. Alvarado-Esquivel C, Sanchez-Anguiano LF, Hernandez-Tinoco J, Berumen-Segovia LO, Torres-Prieto YE, Estrada-Martinez S, et al. Toxoplasma gondii infection and mixed anxiety and depressive disorder: a case-control seroprevalence study in durango, mexico. J Gynecol Obstet Hum Reprod (2016) 8(7):519–23. doi: 10.14740/jocmr2576w
13. Sutterland AL, Fond G, Kuin A, Koeter MW, Lutter R, van Gool T, et al. Beyond the association. Toxoplasma gondii in schizophrenia, bipolar disorder, and addiction: systematic review and meta-analysis. Acta Psychiatr Scand (2015) 132(3):161–79. doi: 10.1111/acps.12423
14. Omar A, Bakar OC, Adam NF, Osman H, Osman A, Suleiman AH, et al. Seropositivity and serointensity of Toxoplasma gondii antibodies and DNA among patients with schizophrenia. Parasite Immunol (2015) 53(1):29–34. doi: 10.3347/kjp.2015.53.1.29
15. Alvarado-Esquivel C, Urbina-Álvarez JD, Estrada-Martínez S, Torres-Castorena A, Molotla-de-León G, Liesenfeld O, et al. Toxoplasma gondii infection and schizophrenia: a case control study in a low Toxoplasma seroprevalence Mexican population. Pathog Glob Health (2011) 60(2):151–5. doi: 10.1016/j.parint.2010.12.003
16. Alvarado-Esquivel C, Sánchez-Anguiano LF, Hernández-Tinoco J, Berumen-Segovia LO, Torres-Prieto YE, Estrada-Martínez S, et al. Toxoplasma gondii infection and depression: a case-control seroprevalence study. Eur J Microbiol Immunol (Bp) (2016) 6(2):85–9. doi: 10.1556/1886.2016.00010
17. Tedla Y, Shibre T, Ali O, Tadele G, Woldeamanuel Y, Asrat D, et al. Serum antibodies to Toxoplasma gondii and Herpesvidae family viruses in individuals with schizophrenia and bipolar disorder: a case-control study. Ethiop Med J (2011) 49(3):211–20.
18. Chen X, Chen B, Hou X, Zheng C, Yang X, Ke J, et al. Association between Toxoplasma gondii infection and psychiatric disorders in Zhejiang, Southeastern China. Acta Trop (2019) 192:82–6. doi: 10.1016/j.actatropica.2019.02.001
19. Afifi MA, Jiman-Fatani AA, Al-Rabia MW, Al-Hussainy NH, El Saadany S, Mayah W. More than an association: latent toxoplasmosis might provoke a local oxidative stress that triggers the development of bipolar disorder. J Nerv Ment Dis (2018) 6(3):139–44. doi: 10.4103/JMAU.JMAU_22_18
20. Oliveira J, Kazma R, Le Floch E, Bennabi M, Hamdani N, Bengoufa D, et al. Toxoplasma gondii exposure may modulate the influence of TLR2 genetic variation on bipolar disorder: a gene-environment interaction study. J Affect Disord (2016) 4(1):11. doi: 10.1186/s40345-016-0052-6
21. Hamdani N, Bengoufa D, Godin O, Doukhan R, Le Guen E, Daban-Huard C, et al. Immunoglobulin sub-class distribution in bipolar disorder and schizophrenia: potential relationship with latent Toxoplasma Gondii infection. BMC Psychiatry (2018) 18(1):239. doi: 10.1186/s12888-018-1821-9
22. Pearce BD, Kruszon-Moran D, Jones JL. The relationship between Toxoplasma gondii infection and mood disorders in the third National Health and Nutrition Survey. Biol Psychiatry (2012) 72(4):290–5. doi: 10.1016/j.biopsych.2012.01.003
23. Mortensen PB, Pedersen CB, McGrath JJ, Hougaard DM, Nørgaard-Petersen B, Mors O, et al. Neonatal antibodies to infectious agents and risk of bipolar disorder: a population-based case-control study. Bipolar Disord (2011) 13(7-8):624–9. doi: 10.1111/j.1399-5618.2011.00962.x
24. Freedman D, Bao Y, Shen L, Schaefer CA, Brown AS. Maternal T. gondii, offspring bipolar disorder and neurocognition. Soc Psychiatry Psychiatr Epidemiol (2016) 243:382–9. doi: 10.1016/j.psychres.2016.06.057
25. Esan O, Esan A. Epidemiology and burden of bipolar disorder in Africa: a systematic review of data from Africa. Zoonoses Public Health (2016) 51(1):93–100. doi: 10.1007/s00127-015-1091-5
26. Mcdonald KC, Bulloch AG, Duffy A, Bresee L, Williams JV, Lavorato DH, et al. Prevalence of Bipolar I and II Disorder in Canada. Can J Psychiatry (2015) 60(3):151–6. doi: 10.1177/070674371506000310
27. Alvarado-Esquivel C, Estrada-Martínez S, Pizarro-Villalobos H, Arce-Quiñones M, Liesenfeld O, Dubey JP. Seroepidemiology of Toxoplasma gondii infection in general population in a northern Mexican city. Korean J Parasitol (2011) 97(1):40–3. doi: 10.1645/GE-2612.1
28. Harker KS, Ueno N, Lodoen MB. Toxoplasma gondii dissemination: a parasite's journey through the infected host. Parasitol Int (2015) 37(3):141–9. doi: 10.1111/pim.12163
29. Alvarado-Esquivel C, Mercado-Suarez MF, Rodríguez-Briones A, Fallad-Torres L, Ayala-Ayala JO, Nevarez-Piedra LJ, et al. Seroepidemiology of infection with Toxoplasma gondii in healthy blood donors of Durango, Mexico. BMC Infect Dis (2007) 7:75. doi: 10.1186/1471-2334-7-75
30. Alvarado-Esquivel C, Liesenfeld O, Márquez-Conde JA, Cisneros-Camacho A, Estrada-Martínez S, Martínez-García SA, et al. Seroepidemiology of infection with Toxoplasma gondii in waste pickers and waste workers in Durango, Mexico. Acta Psychiatr Scand (2008) 55(6):306–12. doi: 10.1111/j.1863-2378.2008.01133.x
31. Alvarado-Esquivel C, Hernández-Tinoco J, Sánchez-Anguiano LF, Ramos-Nevárez A, Cerrillo-Soto SM, Sáenz-Soto L, et al. High seroprevalence of Toxoplasma gondii infection in inmates: a case control study in Durango City, Mexico. Eur J Microbiol Immunol (Bp) (2014) 4(1):76–82. doi: 10.1556/EuJMI.4.2014.1.7
Keywords: Toxoplasma gondii, seroprevalence, bipolar disorder, psychiatric patients, case–control study
Citation: Alvarado-Esquivel C, Estrada-Martínez S and Pérez-Alamos AR (2019) A Case–Control Seroprevalence Study on the Association Between Toxoplasma gondii Infection and Bipolar Disorder. Front. Psychiatry 10:766. doi: 10.3389/fpsyt.2019.00766
Received: 29 May 2019; Accepted: 24 September 2019;
Published: 25 October 2019.
Edited by:
Bradley D. Pearce, Emory University, United StatesReviewed by:
Michael Joseph McCarthy, University of California, San Diego, United StatesJu Wang, Tianjin Medical University, China
Copyright © 2019 Alvarado-Esquivel, Estrada-Martínez and Pérez-Alamos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cosme Alvarado-Esquivel, YWx2YXJhZG9jb3NtZUB5YWhvby5jb20=