 Daniel Schöttle1*
Daniel Schöttle1* Friederike Ruppelt1Benno G. Schimmelmann2,3Anne Karow1Alexandra Bussopulos1Jürgen Gallinat4Klaus Wiedemann5
Friederike Ruppelt1Benno G. Schimmelmann2,3Anne Karow1Alexandra Bussopulos1Jürgen Gallinat4Klaus Wiedemann5 Daniel Luedecke1Anja Christine Rohenkohl1Christian G. Huber4Thomas Bock1Martin Lambert1
Daniel Luedecke1Anja Christine Rohenkohl1Christian G. Huber4Thomas Bock1Martin Lambert1- 1Psychosis Centre, Department of Psychiatry and Psychotherapy, University Centre of Psychosocial Medicine, Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 2University Hospital of Child and Adolescent Psychiatry, University of Bern, Bern, Switzerland
- 3University Hospital of Child and Adolescent Psychiatry, University Centre of Psychosocial Medicine, Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 4Department of Adult Psychiatry, Universitäre Psychiatrische Kliniken Basel (UPK), University of Basel, Basel, Switzerland
- 5Department of Psychiatry and Psychotherapy, University Centre of Psychosocial Medicine, Medical Center Hamburg-Eppendorf, Hamburg, Germany
Objective: The ACCESS treatment model offers assertive community treatment (ACT) embedded in an integrated care program to patients with severe psychotic disorders. Compared to standard care, it proved to be more effective in terms of service disengagement and other outcomes in patients with psychotic disorders over 12, 24, and 48 months. Many patients with severe mental disorders experience involuntary admissions which can be potentially traumatic. In this study, we assessed the effect of ACT on reducing involuntary admissions over an observation period of 4 years.
Method: One hundred seventy-one patients treated in ACCESS were included in this study. The primary outcome was rate of involuntary admissions during 48 months. Secondary outcomes were differences between those with and without involuntary admissions in the 2 years prior to ACCESS regarding change of psychopathology, severity of illness, psychosocial functioning, quality of life, satisfaction with care, medication non-adherence, and service-disengagement.
Results: Of 171 patients, 58 patients (33.9%) were involuntarily admitted to hospital in the past 2 years before entry. During the 4 years of treatment, 16 patients (9.4%) were involuntarily admitted to hospital which was a significantly lower rate compared to the 2 years before inclusion in ACCESS (p < .001). Comparing the two groups, larger improvements in severity of illness (p = .004) and functional status (p = .043) were detected in the group with no history of involuntary admissions. At 4-year follow-up, of the remaining patients, 69.2% (n = 81) were full adherent (p < .001), compared to 18.9% (n = 31) at baseline with no differences between the two groups over the study period (p = .25). Over 4 years, only 13 patients (13.2%) were service-disengaged due to non-practical reasons.
Conclusions: In this long-term study, we were able to demonstrate a reduction in involuntary admissions in four treatment years compared to the 2 years prior to admission to the ACCESS model in patients with severe and mostly multiphase schizophrenia spectrum disorders and affective disorders with psychotic features. This may help prevent patients from suffering from a potentially traumatic experience during treatment in the psychiatric system.
Clinical Trial Registration:www.ClinicalTrials.gov, identifier NCT01888627.
Introduction
With the progressive deinstitutionalization of psychiatric care, outpatient care has changed significantly in recent decades. The treatment of patients with the most severe forms of mental disorders, such as psychotic disorders (1, 2), is still demanding. Patients often remain very susceptible to future recurrences after a first episode and experience persistent or even increasing difficulties in symptoms and functioning, even when they are not acutely ill (2, 3). Schizophrenia spectrum and bipolar disorders (especially with comorbid substance use disorders) are associated with one of the highest risks of involuntary hospitalization for patients (4, 5). Compulsorily admitted patients often lack insight into their disorders and the need for treatment (6).
In addition, patients with schizophrenia spectrum or bipolar disorders often experience other forms of coercive treatment, such as seclusion, mechanical restraint, or coercive medication, or more subtle forms, such as informal coercion (7–9). Therapeutic staff have to deal with the difficult ethical and clinical task of patient care on the one hand, and with respect for patients’ autonomy in trying to maintain a good therapeutic relationship between these conflicting requirements on the other. Therapeutic self-understanding does not include the use of institutional violence, sometimes necessary to prevent patients from harming themselves or others (10). Even when coercive measures are used to regain patients’ autonomy and enable individuals to recover from a severe psychotic episode—for example, coercive treatment of patients is often experienced negatively and may be traumatic (11–13). A negative attitude and acceptance of future psychiatric care, unfavorable treatment courses with high relapse rates, and subsequent involuntary admissions as well as rejection of inpatient and outpatient treatment may possibly develop as negative consequences of such a loss of existential autonomy and coercion (10, 13–19). In addition, the experience and/or use of violence in a psychiatric treatment environment can be potentially negative and even traumatic for therapeutic personnel (20). Apart from those who perceive their coercive treatment as negative, there are a considerable number of patients who consider it to be justified retrospectively. Patients’ perceptions of coercive experiences depend, among other things, on when patients are asked about a coercive event, the therapeutic relationship, how coercive measures are communicated to patients, and as how fair and effective they are experienced (12, 21–26). Studies with results on long-term outcomes on other variables such as treatment discontinuation, symptomatology, and functional status are sparse and have shown heterogeneous findings.
In recent years, various outpatient care models have been developed for patients with severe mental illnesses (SMI), which are adapted to their complex treatment needs and generally show positive effects. Most of them comprise multiprofessional teams and individualized, flexible, and domestic treatments such as assertive community treatment (ACT), flexible ACT (FACT), and intensive case management (ICM) (27–35). There are also other approaches, such as the Crisis Resolution Team, which offer temporary treatment (36).
Most study care models are diagnosis-specific and do not provide continuous and unlimited treatment for patients with severe mental disorders (32).
Because patients with SMI have high rates of withdrawal, non-adherence, involuntary admission, and often chronic disease progression, specific, timely, and permanent treatment may be required for patients with psychotic disorders beyond early detection of new episodes and pure crisis management (33, 37). In addition, treatment must overcome structural barriers and fragmentation of treatment systems to ensure therapeutic continuity. The therapeutic alliance depends, among other things, on continuous confidence-building and long-term treatment. Since the therapeutic relationship is one of the most effective factors for successful treatment, this must be ensured (38). In 2006, our group designed and evaluated a diagnosis-specific integrated treatment model with ACT (the ACCESS model) specializing in psychotic disorders (rather than critically ill patients in general), with a focus on maintaining a continuous therapeutic relationship, low-threshold psychotherapy, and family involvement and embedding the ACT team in an integrated care program that allows for need-adapted, time-unlimited treatment (27, 39). Under real-life conditions, the effectiveness of the program was continuously evaluated, and the results were published in various studies (27, 29, 39–49). The evidence of a reduction in involuntary admissions or the use of coercive measures in intensive care models is difficult to compare and ambiguous due to methodological differences in treatment systems used. It is known that unfavorable therapeutic conditions such as high barriers to access to psychiatric care, the availability of home treatment, or crisis intervention teams have an impact on the rate of involuntary admissions (50–52). In addition, involuntary admissions often take place in hours outside regular outpatient services (50–52). Early detection of an emerging episode to prevent a new crisis or rapid worsening of symptoms, combined with early involvement of family members or friends in the home environment, may be key elements of assertive outreach treatment. Although this could theoretically lead to prevention of involuntary admission due to early and rapid treatment, assertive outreach teams also attract critically ill patients who not only have a higher chance of involuntarily being admitted to hospitals but who are better able to recognize the need for treatment that, conversely, can increase or have no effect on the rate of (involuntary) admission (36, 53–56).
Although intensive treatment models can have positive effects on, amongst others, symptomatology, relapses, and hospital stay, there are few studies that assess their direct effects on involuntary admissions with heterogeneous outcomes, partly due to methodological differences, differences between national legislations, and model adherence in the implementation of assertive outreach structures (29, 49, 55, 57–61).
In our present study, we report the frequency of involuntary admission of 171 patients with severe psychotic disorders during 4 years of treatment compared to 2 years of treatment before admission to ACCESS. In addition, we performed outcome comparisons between a group that had involuntary admission and a group that had not been involuntarily admitted to hospital in the last 2 years prior to ACCESS in terms of outcome variables such as course of psychopathology, severity of disease, functional status, quality of life, and satisfaction with treatment. We assume that the rate of involuntary admissions would decrease compared to the 2 years prior to admission over an extended period of 4 years of treatment and that both groups would show similar improvements throughout the study period.
Methods
Context, Sample, and Inclusion and Exclusion Criteria
The Psychosis Center of the University Hospital Hamburg-Eppendorf is responsible for the treatment of adult patients with severe schizophrenia spectrum disorders (SSD) or bipolar disorder (BD) in an urban catchment area of 300,000 inhabitants.
The ACCESS model is described in detail elsewhere (27) (29). The main features of the integrated care concept, including details on ACT, inclusion and exclusion criteria, and assessments, are presented in Table 1 and Table 2. From May 2007 to March 2012, 171 patients with SSD and BD and severe mental illness were included within the ACCESS model. Of these, 171 patients who were followed-up for 4 years were analyzed. All treated patients (N = 171) participated in the clinical routine assessments. The study was conducted in accordance with the latest version of the Helsinki Declaration, and written informed consent of the participants was obtained. All patients treated in the ACCESS model agreed that their data could be used in the ACCESS-II study whenever they were sufficiently stable, and the ability to consent was determined by a counseling psychiatrist. The ethics committee of the Hamburg Medical Association approved the observational study (registration number: PV4059). The study was registered at ClinicalTrials.gov (NCT0188868627).
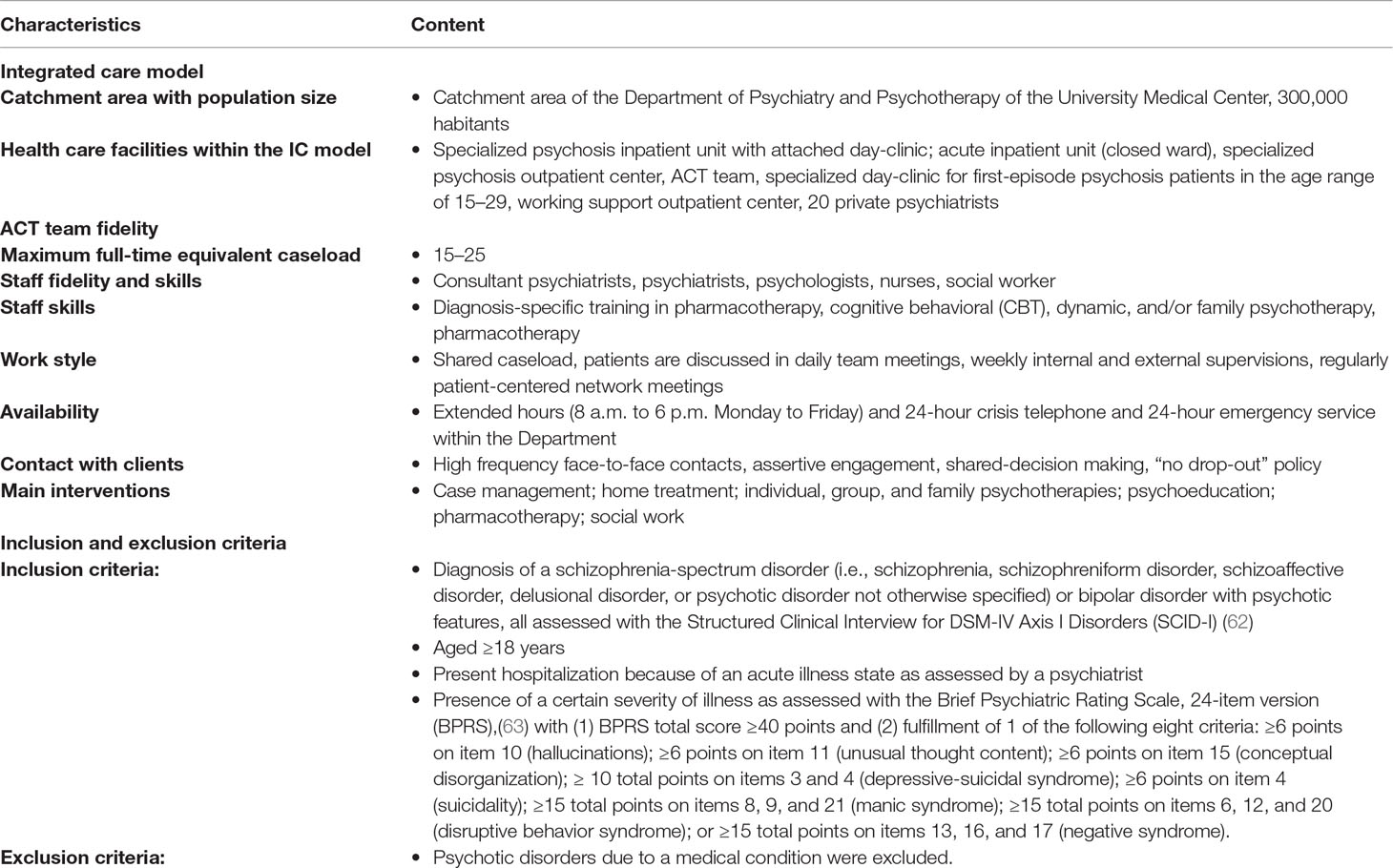
Table 1 Characteristics of the ACCESS treatment and inclusion/exclusion criteria.
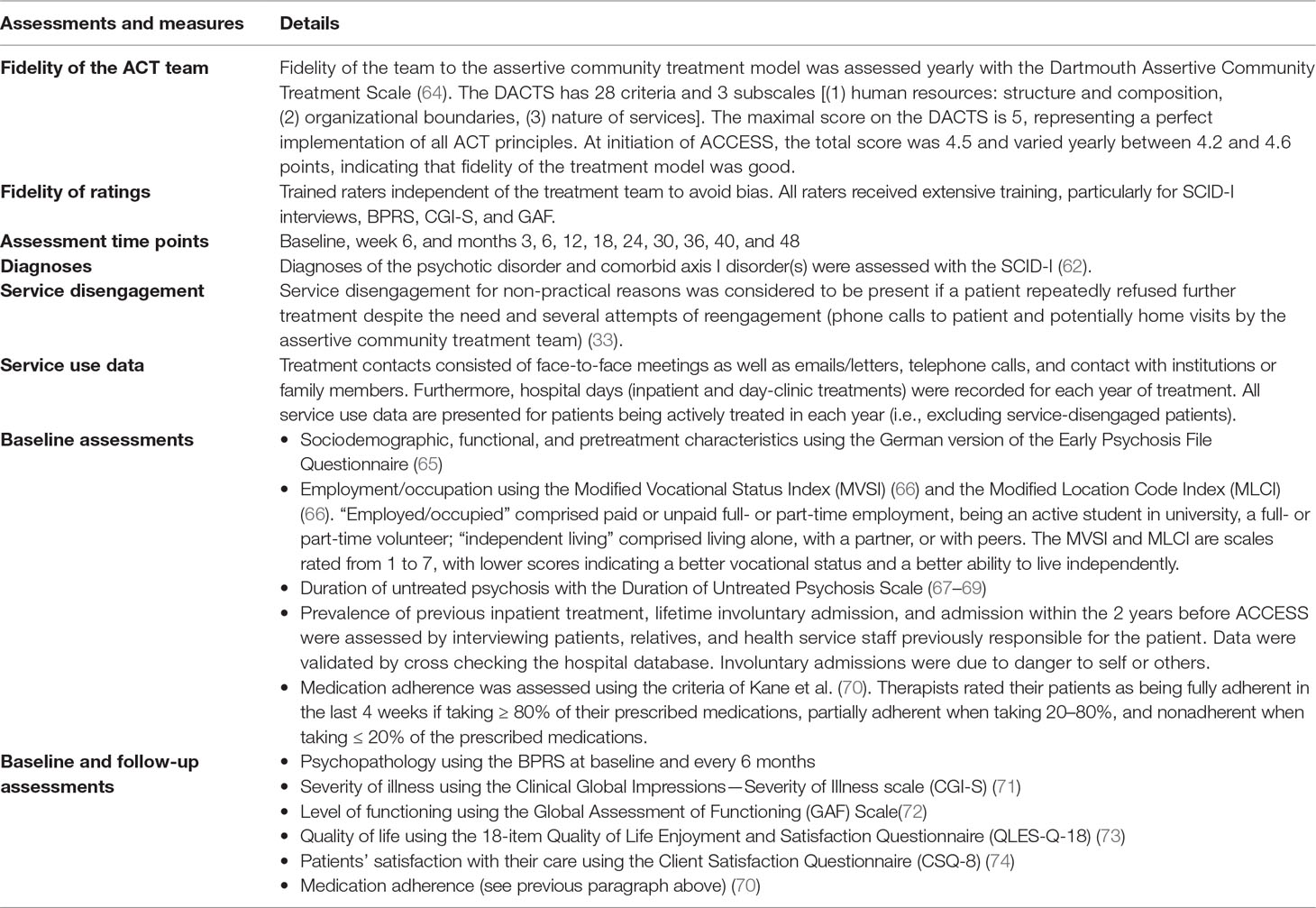
Table 2 Assessments and measures.
To evaluate involuntary admissions before and after inclusion in the ACCESS program, we used a pre-post-mirror comparison design. We decided to evaluate a longer observation period of 4 years in order to better detect differences between the time before and after admission and between the two groups. Involuntary admissions were assessed 2 years before admission and during the 4-year observation period. Involuntary treatment included compulsory admission based on (1) the “Hamburger PsychischKrankenGesetz” (HambPsych KG; §12 and §9) with patients who meet the criteria of acute risk to themselves or others from a mental disorder initiated by a physician or psychiatric hospital ordered by law, or (2) the Bürgerliches Gesetzbuch (BGB) with compulsory admission initiated by a parent or guardian under §1906. While both actions require a very acute symptomatology, compulsory admissions of the second type cannot be performed if there is solely a danger for others. Both actions, which lead to involuntary admissions to hospitals, require the opinion of a psychiatrist and must be approved by a judge.
Statistical Analysis
Descriptive baseline differences between diagnostic groups were assessed via independent-samples t-tests for continuous dependent variables. Categorical variables were assessed with chi-square tests. To compare baseline with the 48-month follow-up for the binary outcomes (e.g., involuntary admissions), we used McNemar’s test. We evaluated the changes from baseline (admission to ACCESS treatment) via mixed-model repeated measures, considering the follow-up times as repeated measures, the patients as the random effect, the group (with vs. without involuntary admissions 2 years before baseline) and time as fixed effects, and the baseline values of the dependent variable as covariates. Outcomes were changes from baseline for BPRS total score, CGI-S score, GAF, Q-LES-Q-18, and CSQ-P. We examined the interaction between time and group. If the interaction was not significant, the interaction term was eliminated from the model. We used the baseline values of the dependent variables (BPRS total score, CGI-Severity score, GAF, Q-LES-Q-18, CSQ-8 P) as covariates to minimize variance (75). The main effects (F), significance levels (p), and estimated marginal means (EMM) and 95%-confidence intervals (CI) are reported. The level of significance was set at p < .05, two-sided. Statistical analyses were performed using SPSS version 20.0 (IBM Corp, 2011).
Results
Baseline Characteristics
One hundred and seventy-one patients with SSD or BD (42.7% male; mean age = 42.3 years; SD 13.4) were treated in the ACCESS model and participated in the ACCESS-II study. Baseline details are displayed in Table 3.
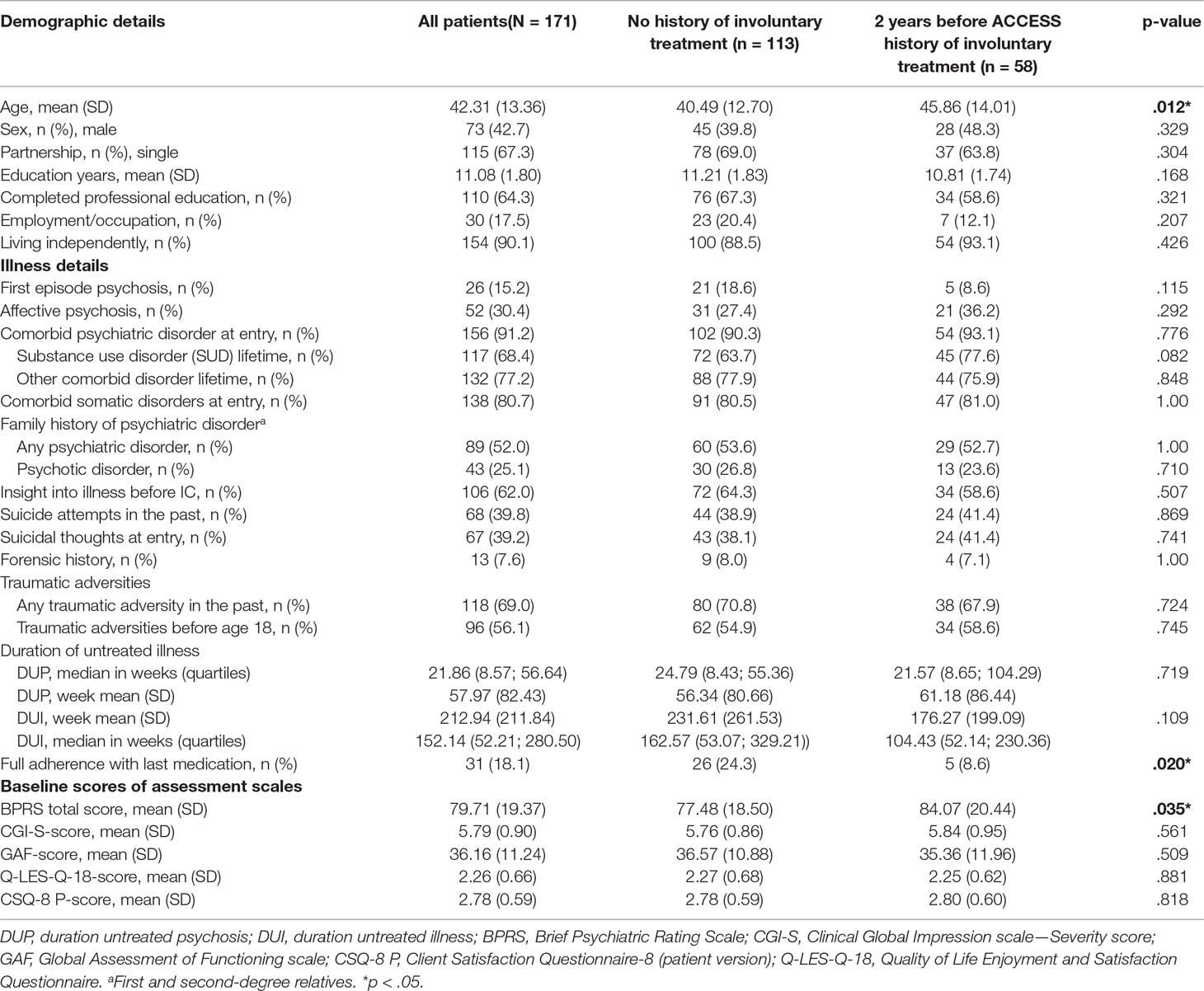
Table 3 Baseline variables.
Of all 171 patients, 23 (13%) did not have any psychiatric inpatient treatment before inclusion in the ACCESS model. Furthermore, as 141 (85%) of the patients already had multiple episodes of their illness, we assume that most of them had contact to the treatment system and had been treated with different forms of psychopharmacological and psychotherapeutic interventions. However, we could not assess this question in detail, as detailed data on prior outpatient treatment were not available.
Patients with both schizophrenia-spectrum disorders (n = 147) and BD (n = 24) were severely ill (high CGI-S and BPRS scores and low GAF scores). Quality of life and satisfaction with care before entry into the ACCESS treatment model were low; 58 patients (34%) had involuntary admissions to inpatient treatment in the past 2 years before inclusion in ACCESS, and only 18.1% (n = 31) were adherent to their most recent medication. Patients with a recent history of involuntary admissions were significantly older (45.9 vs. 40.5 years; p = 0.012), less adherent (8.6 vs. 24.3%; p = 0.02) with the last medication, and had higher scores on the BPRS Scale (84.1 vs. 77.5; p = 0.035) than the patient group without involuntary admissions.
Rates of Involuntary Admissions During 4 Years of Treatment
Of those being involuntarily treated in the past 2 years before entry, 47 patients had a SSD (32.0% of the whole SSD-group) and 11 patients were diagnosed with a BD with psychotic symptoms (45.8% of the whole BD-group) (p = .184). During the 4 years of treatment, 16 patients (9.4%) were involuntarily admitted to hospital which was a significantly lower rate (58 patients; 34%) compared to the 2 years before inclusion in ACCESS (p < .001). Of those being involuntarily admitted during 4 years of treatment, 14 patients had a diagnosis of a SSD (9.5% of the whole SSD-group) and 2 patients had BD with psychotic symptoms (8.3% of the whole BD-group).
Clinical Course of Patients With and Without Involuntary Admissions in the 2 Years Prior to ACCESS
All follow-up assessments during the 4 years indicated significantly improved psychopathology, illness severity, global functioning, and quality of life in patients (Table 4). Comparing the two groups, larger improvements in severity of illness (p = .004) and functional status (p = .043) were detected in the group with no history of involuntary admissions 2 years before ACCESS, compared to the group without involuntary admissions, between baseline and year 4. No significant differences were found on the course of psychopathology and quality of life. Regarding satisfaction with treatment, the CSQ-8 scores indicated a significantly better than baseline satisfaction with care, with a mean rating of “good” at 12- and 24- and 48-month follow-ups with no differences between the groups.
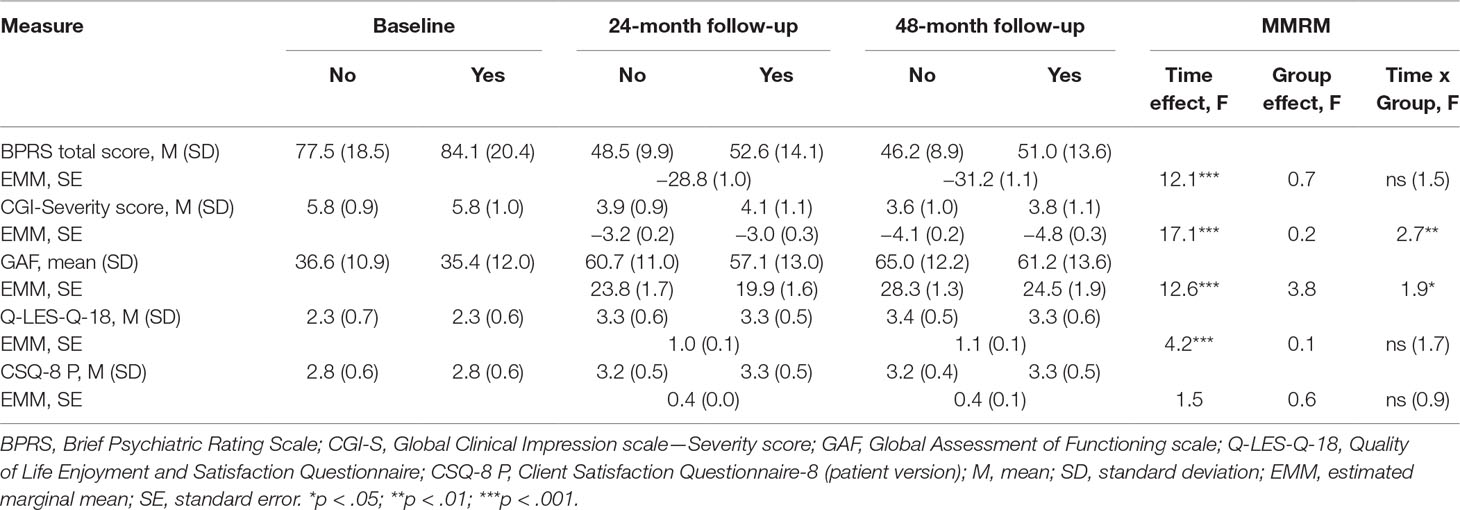
Table 4 Course of illness over 4 years.
At 48-month follow-up, of the remaining patients, 69.2% (n = 81) were full adherent (McNemar’s test, p < .001), compared to 18.9% (n = 31) at baseline with no differences between the two groups over the study period (p = 0.25).
Furthermore, in the whole group, significantly more patients were employed/occupied after 48 months (n = 35; McNemar’s test, p = 0.036), while rates of living independently remained stable (n = 88, p = .332). There were no significant differences between the two groups regarding both variables.
Service-Disengagement
Over the 48-month treatment period, 13 patients (13.2%) were service-disengaged after a median of 79.1 weeks (quartiles 36.9–150.6) due to non-practical reasons (refused treatment contact, disengaged from study despite several attempts to engage them). Of these 13 patients, 8 (61.5%) had an involuntary admission in the 2 years before ACCESS and 3 (23.1%) during the ACCESS treatment. Furthermore, 41 patients (24.0%) dropped out of the study due to practical reasons [moved out of catchment area: 15 patients (36.6%); moved to sheltered housing: 13 patients (31.7%); transition to other service: 10 patients (24.4%); change of health insurance company: 1 patient (2.4%); change of diagnosis: 2 patients (4.9%) after a median duration of treatment of 91.4 weeks (quartiles 40.9-130.1)]. Of these 41 patients, 13 (31.7%) had an involuntary admission in the 2 years before ACCESS and 10 (24.4%) during the ACCESS treatment.
Discussion
The ACCESS model provides treatment as a temporally unlimited care model and is delivered to a sample of critically ill patients, especially with recurring SSD and BD with complex treatment needs.
In this study, we focused (1) on the rates of involuntary admissions during long-term treatment and (2) on whether those with or without involuntary admissions prior to ACCESS differ in other outcome parameters such as symptomatic progression, functional status, quality of life, and satisfaction with treatment. In addition, we analyzed differences on employment and living standards.
We were able to show that the rate of involuntary admissions decreased significantly during ACCESS treatment over 4 years. While in the 2 years prior to ACCESS one in three patients experienced involuntary admission, the rates were reduced to 9.4% over 4 years of treatment. Most patients involuntarily admitted to hospital were diagnosed with SSD, which is consistent with other studies showing that patients with SSD belong to a high-risk group for involuntary admissions. Compared to the group of patients with SSD, the rates of those with BD have decreased significantly compared to the 2 years prior to ACCESS treatment, so it appears that these patients benefit particularly from the need-adapted and fast-response treatment system that offers high-frequency home treatment, including psychotherapy and early family involvement. Our results are consistent with other studies showing a reduction of coercive measures during intensive outpatient treatment (29, 49) (58, 61), but the results of other studies are heterogeneous (56, 60). These are due to methodological differences, e.g., different treatment approaches/systems, different national legislations, patient characteristics, follow-up time, model fidelity, and therefore difficult to compare. Nevertheless, the CRT in the study by Johnson et al. did not lead to a reduction in involuntary detentions, and no difference in coercive measures was found in the OPUS study, in which ACT was offered, and compared with usual treatment (55, 59). The availability of low-threshold and high-frequency outpatient treatment and crisis resolution teams led to a reduction in involuntary admissions in the study by Juckel et al. (52, 62). On the other hand, there are studies showing an increase in the frequency of involuntary hospital admissions (56, 60), probably due to the group of patients (1) in which mainly seriously ill patients at high risk of involuntary admission are treated and (2) in which those who would normally not reached by the psychiatric treatment network can be identified and then treated, often with a first compulsory hospital treatment. In addition, there is a group of patients who would not have entered the psychiatric treatment system under “treatment as usual” circumstances and who are difficult to treat even in intensive care approaches, but who are nevertheless contacted by assertive outreach teams and then voluntarily admitted to hospital.
Although causal attributions are not possible due to the absence of a control group, we assume that some factors contribute to the observed significant decreases in compulsory hospital admissions for patients with complex treatment needs, high co-morbidity rates, and high chances of treatment discontinuation and non-adherence (49).
It can only be assumed which of the factors are related to the reductions of admissions. We believe that treatment should be offered openly and need-adapted with a small enough case load per case manager to allow for multiple outpatient contacts per week. The treatment team should be committed to psychotherapy and family involvement and should be recovery oriented. The most important points are the therapeutic alliance and the ability to intervene early, both factors being related to the high-intensity and ongoing treatment.
Although we lack specific empirical evidence from our data, continuous treatment seems especially important with a high number of treatment contacts, leading to a well-established treatment alliance between patients and their therapists, the low-threshold availability of the assertive outreach team, with rapid detection and response to emerging crises, is among the key elements of ACCESS that in our view contribute to reducing involuntary admissions in our patients. In addition, the early and intensive involvement of family members and other key individuals, as well as the recovery-oriented psychotherapeutic approach, may further have contributed to promoting treatment engagement. Other factors mentioned in the study by Burns et al., which do not explicitly contribute to a reduction in compulsory admission but in number of inpatients days, can also be found in our treatment approach: regular home visits, a high proportion of home contacts, smaller patient-to-therapist ratio, responsibility for health and social affairs, and multidisciplinary teams (76).
Confirming the results of our previous study, the psychopathology of the patients, the severity of the disease, the functioning, and the quality of life improved overall during the 4-year treatment period (29, 49). Although difficult to compare with each other because of differences in sample composition and the offered care model itself, other trials have shown that intensive treatment can improve and stabilize patients with severe mental illness—as long as it is actively and continuously offered (75, 77). We cannot deduce causality from our non-randomized single-group design, but we believe it is worth providing affordable and flexible but highly specific long-term care for patients with first and multiple episode psychosis (78). The group with involuntary admissions prior to ACCESS had fewer improvements in severity and functional status than the other patients. The only fundamental difference we found was that these patients were older, had higher baseline values on the BPRS scale, and had lower adherence rates to their previous medication. Non- or partial adherence with psychopharmacological treatment is one of the major risk factors for relapses (79, 80), which significantly reduces patients’ psychosocial and occupational functioning and negatively affects their quality of life (79, 81, 82). Psychopharmacological treatment, as an integral part of an integrated framework for social and psychological care, can help to overcome these impairments and is highly effective (83). Non-adherence with treatment is, however, particularly frequently observed in patients with schizophrenia (80, 84, 85) with a significantly increased risk of relapse (86). Even small gaps in medication intake can have a negative impact on the outcome, since discontinuation of medication for only 1 to 10 days in a period of 1 year (partial adherence) was associated with a significantly increased risk of hospitalization with a quota ratio of 1.98 (87). Partial adherence, such as intermittent medication intake, also leads to a 3-fold higher relapse risk in stable patients (88). Adherence rates increased significantly during treatment, and we found no persistent differences in medication use between the two groups.
Quality of life was not significantly influenced by previous involuntary admissions, a finding also found in other studies (89, 90). In the study by Ohlenschlaeger et al., the patients in integrated treatment, who are not directly comparable to our study due to the focus on patients of the first episode, showed a better quality of life compared to other treatment models (91).
Satisfaction with the treatment was also “good” in all patients without group differences. Treatment satisfaction is influenced by many factors but seems to be more related to the subjectively perceived degree of coercion during admission and treatment than to the objective (documented) extent of coercive measures (92). We did not measure levels of perceived coercion, but it is interesting in the context of intensive assertive outreach treatment that, among other factors, viewing the hospital as ineffective and other treatments as more appropriate and involving patients in the decision-making and treating them with respect may reduce perceived coercion (93). As our treatment model involves patients intensively in decision-making, this could have influenced ratings of satisfaction with treatment.
The disengagement rate of services over 48 months remained very low over the 4 years at 13.2%, which was slightly higher than in the previous 4-year study (8.7% disengagement rate). Insofar, in the years since the beginning of ACCESS, we had a constant afflux of patients. Therefore, the team increased from one multiprofessional team consisting of 4 full-time team members in 2007 treating 64 patients to 10.7 full-time team members in the year 2019, who work in 3 multiprofessional teams treating 228 patients. We were creating new small teams to achieve that every team member knows each patient and to make sure that personal treatment continuation is guaranteed.
Strengths and Limitations
Due to the observational, non-randomized study design, more severely ill patients with higher rates of comorbidities were included, who probably would not have provided consent to participation in a (randomized) controlled trial. During such a long follow-up period, it was possible to assess the long-term effects of continuous treatment beyond the initial course of illness. The biggest limitation, of course, is the lack of a control group in the ACCESS-II study. Therefore, a direct causal effect of the treatment program on the results of the key outcome parameters cannot be drawn. Instead, other factors may also be responsible for the positive results found in patients treated in the ACCESS model over 4 years. Therefore, the descriptive results must be interpreted with cautions. We decided, after a prospectively controlled study confirmed the superiority of the ACCESS model over standard treatment over a period of 1 year, that only an observational and uncontrolled long-term study can be considered ethical. Another unavoidable limitation was the non-blind assessment of patients. Although we have used external advisors to ensure the quality of evaluation, we probably could not completely avoid a social desirability bias and thus positive evaluations of psychopathology. One major outcome—the rate of involuntary admissions—was not influenced by social desirability or nonblind assessments. However, patients who dropped out due to non-practical reasons could have impaired the beneficial results since it is not known whether they would have been involuntarily admitted during the observation period. This cannot be ruled out, but it seems unreasonable because they dropped out after having been in treatment for almost 2 years. Since the sample size of the involuntary treatment group is rather small, analyses of differences between the two groups may be underestimated. In addition, we did not include homeless people, so the sample is not fully representative and is limited by the exclusion of homeless people. These were treated elsewhere by definition of the catchment area. In addition, we cannot exclude the possibility that other important confounding factors were not assessed, including the specific impact of different psychopharmacological treatments. In our treatment model, patients are actively engaged to participate in treatment decisions, and dose-reductions are facilitated in close consultation with the therapist. Therefore, it is not likely that the results are due to general increases in doses of outpatient medication.
Conclusion
In this long-term study, we were able to demonstrate a reduction in involuntary admissions in four treatment years compared to the 2 years prior to admission to the ACCESS model in patients with severe and mostly multi-episode SSD and affective disorders with psychotic features. This may help prevent patients from suffering from a potentially traumatic experience during treatment in the psychiatric system. The ACCESS model, which was offered in a timely and unlimited manner, provided results related to several clinically important outcome parameters, with low disengagement and significantly improved medication adherence rates. We hypothesize some factors to explain these positive outcomes. Psychosis-specific ACT, embedded in an integrated care system that offers a wide range of treatment options for psychotic disorders and comorbidities flexibly and rapidly, with a focus on recovery-oriented psychotherapy and family involvement, could have contributed to strengthening the therapeutic alliance that, together with the above-mentioned treatment system, could serve as a protective factor. Treatment should be offered on a need-adapted basis with a low caseload to allow a high frequency of contacts. While the results are promising, to draw causal conclusions, stronger evidence including a long-term RCT would be required. Nevertheless, our study adds important knowledge that there is an association of intensive and ongoing home treatment and a significant reduction of involuntary admissions during long-term treatment of patients with severe mental illness.
Data Availability Statement
The full dataset of the analysis is not publicly available due to the rules of data protection of our hospital.
Ethics Statement
The ethics committee of the Hamburg Medical Association approved the observational study (registration number: PV4059). The study was registered under ClinicalTrials.gov (NCT0188868627).
Author Contributions
Conceptualization: DS, FR, TB, AK, ML; data curation: FR; data analyses: FR; investigation: DS, FR, AB, JG, KW, TB, AK, ML; methodology: BS, FR, project administration: JG, AK, ML; supervision: ML; writing original draft: DS, FR, AK, ML; writing, review and editing: DS, ML, FR, AB, JG, KW, AR, CH, TB, AK; contribution: all authors contributed to manuscript revision, read and approved the submitted version.
Conflict of Interest
DS has been a consultant and/or advisor to or has received honoraria from Astra Zeneca, Otsuka Pharma GmbH, Lundbeck GmbH, Janssen Cilag and Shire.BS has been a consultant and/or advisor to or has received honoraria from Shire, Takeda, Novartis and Medice.TB has received honoraria from Astra Zeneca.ML has held lectures for AstraZeneca, Bristol-Myers Squibb, Lilly Deutschland GmbH, Janssen Cilag GmbH, Lundbeck GmbH, Otsuka Pharma GmbH, Roche Deutschland Holding GmbH, Sanovi Aventis; Grants: AstraZeneca, Bristol-Myers Squibb, Lilly Deutschland GmbH, Janssen Cilag GmbH, Lundbeck, Sanovi Aventis; Consultancy: AstraZeneca, Lilly Deutschland GmbH, Janssen Cilag GmbH, Roche Deutschland Holding GmbH, Trommsdorff GmbH & Co. KG. AK has been consultant and/or advisor to or has received honoraria from: AstraZeneca, Bristol-Myers Squibb, Lilly Deutschland GmbH, Janssen Cilag GmbH, Lundbeck GmbH, Otsuka Pharma GmbH, Roche Deutschland Holding GmbH.JG has received research funding from the German Federal Ministry of Education and Research, German Science Foundation, and speaker fees from Lundbeck, Janssen-Cilag, Lilly and Otsuka.CH serves in the cariprazine advisory board for Recordati AG and has received travel grants from Recordati AG, Servier (Suisse) S.A., and Janssen-Cilag AG, Switzerland.KW has been a consultant and received honoraria for lectures from Janssen GmbH, Lundbeck GmbH and Otsuka Pharma GmbH. DL has served as speaker for Janssen Cilag.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors express their gratitude to all participating patients and private psychiatrists who were involved in the ACCESS program.
References
1. NICE. Psychosis and schizophrenia in adults: NICE Guideline. In: Excellence NIfHaC. London, UK: National Institute for Health and Care Excellence (UK) (2014).
2. Austin SF, Mors O, Secher RG, Hjorthoj CR, Albert N, Bertelsen M, et al. Predictors of recovery in first episode psychosis: the OPUS cohort at 10 year follow-up. Schizophr Res (2013) 150(1):163–8. doi: 10.1016/j.schres.2013.07.031
3. Hafner H, Maurer K, An der Heiden W. Schizophrenia—a disorder in its own right?: results from 25 years of the ABC study. Nervenarzt (2013) 84(9):1093–46–103. doi: 10.1007/s00115-013-3788-6
4. Rosca P, Bauer A, Grinshpoon A, Khawaled R, Mester R, Ponizovsky AM. Rehospitalizations among psychiatric patients whose first admission was involuntary: a 10-year follow-up. Israel J Psychiatr Relat Sci (2006) 43(1):57–64.
5. Opsal A, Clausen T, Kristensen O, Elvik I, Joa I, Larsen TK. Involuntary hospitalization of first-episode psychosis with substance abuse during a 2-year follow-up. Acta Psychiatr Scand (2011) 124(3):198–204. doi: 10.1111/j.1600-0447.2011.01700.x
6. McEvoy JP, Applebaum PS, Apperson LJ, Geller JL, Freter S. Why must some schizophrenic patients be involuntarily committed? The role of insight. Compr Psychiatry (1989) 30(1):13–7. doi: 10.1016/0010-440X(89)90113-2
7. Jaeger M, Ketteler D, Rabenschlag F, Theodoridou A. Informal coercion in acute inpatient setting—knowledge and attitudes held by mental health professionals. Psychiatr Res (2014) 220(3):1007–11. doi: 10.1016/j.psychres.2014.08.014
8. Elmer T, Rabenschlag F, Schori D, Zuaboni G, Kozel B, Jaeger S, et al. Informal coercion as a neglected form of communication in psychiatric settings in Germany and Switzerland. Psychiatr Res (2018) 262:400–6. doi: 10.1016/j.psychres.2017.09.014
9. Fiorillo A, Giacco D, De Rosa C, Kallert T, Katsakou C, Onchev G, et al. Patient characteristics and symptoms associated with perceived coercion during hospital treatment. Acta Psychiatr Scand (2012) 125(6):460–7. doi: 10.1111/j.1600-0447.2011.01809.x
10. Theodoridou A, Schlatter F, Ajdacic V, Rossler W, Jager M. Therapeutic relationship in the context of perceived coercion in a psychiatric population. Psychiatr Res (2012) 200(2-3):939–44. doi: 10.1016/j.psychres.2012.04.012
11. Langle G, Bayer W. Compulsory psychiatric treatment and the patients’ perspective. Psychiatr Prax (2007) 34 Suppl 2:S203–7. doi: 10.1055/s-2006-952008
12. Katsakou C, Priebe S. Outcomes of involuntary hospital admission—a review. Acta Psychiatr Scand (2006) 114(4):232–41. doi: 10.1111/j.1600-0447.2006.00823.x
13. Frueh BC, Knapp RG, Cusack KJ, Grubaugh AL, Sauvageot JA, Cousins VC, et al. Patients’ reports of traumatic or harmful experiences within the psychiatric setting. Psychiatr Serv (2005) 56(9):1123–33. doi: 10.1176/appi.ps.56.9.1123
14. Katsakou C, Priebe S. Patient’s experiences of involuntary hospital admission and treatment: a review of qualitative studies. Epidemiol Psichiatr Soc (2007) 16(2):172–8. doi: 10.1017/S1121189X00004802
15. Priebe S, Katsakou C, Glockner M, Dembinskas A, Fiorillo A, Karastergiou A, et al. Patients’ views of involuntary hospital admission after 1 and 3 months: prospective study in 11 European countries. Br J Psychiatry (2010) 196(3):179–85. doi: 10.1192/bjp.bp.109.068916
16. Luciano M, Sampogna G, Del Vecchio V, Pingani L, Palumbo C, De Rosa C, et al. Use of coercive measures in mental health practice and its impact on outcome: a critical review. Expert Rev Neurother (2014) 14(2):131–41. doi: 10.1586/14737175.2014.874286
17. Swartz MS, Swanson JW, Hannon MJ. Does fear of coercion keep people away from mental health treatment? Evidence from a survey of persons with schizophrenia and mental health professionals. Behav Sci Law (2003) 21(4):459–72. doi: 10.1002/bsl.539
18. Xu Z, Muller M, Lay B, Oexle N, Drack T, Bleiker M, et al. Involuntary hospitalization, stigma stress and suicidality: a longitudinal study. Soc Psychiatr Psychiatr Epidemiol (2018) 53(3):309–12. doi: 10.1007/s00127-018-1489-y
19. Kortrijk HE, Staring AB, van Baars AW, Mulder CL. Involuntary admission may support treatment outcome and motivation in patients receiving assertive community treatment. Soc Psychiatr Psychiatr Epidemiol (2010) 45(2):245–52. doi: 10.1007/s00127-009-0061-1
20. Virtanen M, Vahtera J, Batty GD, Tuisku K, Pentti J, Oksanen T, et al. Overcrowding in psychiatric wards and physical assaults on staff: data-linked longitudinal study. Br J Psychiatry (2011) 198(2):149–55. doi: 10.1192/bjp.bp.110.082388
21. Giacco D, Fiorillo A, Del Vecchio V, Kallert T, Onchev G, Raboch J, et al. Caregivers’ appraisals of patients’ involuntary hospital treatment: European multicentre study. Br J Psychiatry (2012) 201(6):486–91. doi: 10.1192/bjp.bp.112.112813
22. Wullschleger A, Vandamme A, Ried J, Pluta M, Montag C, Mahler L. Standardized debriefing of coercive measures on psychiatric acute wards: a pilot study. Psychiatr Prax (2019) 46(3):128–134. doi: 10.1055/a-0651-6812.
23. Kallert TW, Katsakou C, Adamowski T, Dembinskas A, Fiorillo A, Kjellin L, et al. Coerced hospital admission and symptom change—a prospective observational multi-centre study. PloS One (2011) 6(11):e28191. doi: 10.1371/journal.pone.0028191
24. Steinert T, Birk M, Flammer E, Bergk J. Subjective distress after seclusion or mechanical restraint: one-year follow-up of a randomized controlled study. Psychiatr Serv (2013) 64(10):1012–7. doi: 10.1176/appi.ps.201200315
25. Jaeger M, Rossler W. Enhancement of outpatient treatment adherence: patients’ perceptions of coercion, fairness and effectiveness. Psychiatry Res (2010) 180(1):48–53. doi: 10.1016/j.psychres.2009.09.011
26. Mielau J, Altunbay J, Lehmann A, Bermpohl F, Heinz A, Montag C. The influence of coercive measures on patients’ stances towards psychiatric institutions. Intl J Psychiatry Clin Pract (2018) 22(2):115–22. doi: 10.1080/13651501.2017.1383437
27. Lambert M, Bock T, Schottle D, Golks D, Meister K, Rietschel L, et al. Assertive community treatment as part of integrated care versus standard care: a 12-month trial in patients with first- and multiple-episode schizophrenia spectrum disorders treated with quetiapine immediate release (ACCESS trial). J Clin Psychiatry (2010) 71(10):1313–23. doi: 10.4088/JCP.09m05113yel
28. Marshall M, Lockwood A. WITHDRAWN: assertive community treatment for people with severe mental disorders. Cochrane Database Syst Rev (2011) (4):CD001089. doi: 10.1002/14651858.CD001089.pub2
29. Schottle D, Schimmelmann BG, Karow A, Ruppelt F, Sauerbier AL, Bussopulos A, et al. Effectiveness of integrated care including therapeutic assertive community treatment in severe schizophrenia spectrum and bipolar I disorders: the 24-month follow-up ACCESS II study. J Clin Psychiatry (2014) 75(12):1371–9. doi: 10.4088/JCP.13m08817
30. Stein LI, Test MA. Alternative to mental hospital treatment. I. Conceptual model, treatment program, and clinical evaluation. Arch Gen Psychiatry (1980) 37(4):392–7. doi: 10.1001/archpsyc.1980.01780170034003
31. Sytema S, Wunderink L, Bloemers W, Roorda L, Wiersma D. Assertive community treatment in the Netherlands: a randomized controlled trial. Acta Psychiatr Scand (2007) 116(2):105–12. doi: 10.1111/j.1600-0447.2007.01021.x
32. Schottle D, Karow A, Schimmelmann BG, Lambert M. Integrated care in patients with schizophrenia: results of trials published between 2011 and 2013 focusing on effectiveness and efficiency. Curr Opin Psychiatry (2013) 26(4):384–408. doi: 10.1097/YCO.0b013e328361ec3b
33. Conus P, Lambert M, Cotton S, Bonsack C, McGorry PD, Schimmelmann BG. Rate and predictors of service disengagement in an epidemiological first-episode psychosis cohort. Schizophr Res (2010) 118(1–3):256–63. doi: 10.1016/j.schres.2010.01.032
34. Dieterich M, Irving CB, Park B, Marshall M. Intensive case management for severe mental illness. Cochrane Database of Syst Rev (2010) (10):1465–1858. doi: 10.1002/14651858.CD007906.pub2
35. van Veldhuizen JR. FACT: a Dutch version of ACT. Community. Ment Health J (2007) 43(4):421–33. doi: 10.1007/s10597-007-9089-4
36. Wheeler C, Lloyd-Evans B, Churchard A, Fitzgerald C, Fullarton K, Mosse L, et al. Implementation of the Crisis Resolution Team model in adult mental health settings: a systematic review. BMC Psychiatry (2015) 15(1):74. doi: 10.1186/s12888-015-0441-x
37. Stowkowy J, Addington D, Liu L, Hollowell B, Addington J. Predictors of disengagement from treatment in an early psychosis program. Schizophr Res (2012) 136(1-3):7–12. doi: 10.1016/j.schres.2012.01.027
38. Priebe S, McCabe R. Therapeutic relationships in psychiatry: the basis of therapy or therapy in itself? Int Rev Psychiatry (2008) 20(6):521–6. doi: 10.1080/09540260802565257
39. Karow A, Reimer J, Konig HH, Heider D, Bock T, Huber C, et al. Cost-effectiveness of 12-month therapeutic assertive community treatment as part of integrated care versus standard care in patients with schizophrenia treated with quetiapine immediate release (ACCESS trial). J Clin Psychiatry (2012) 73(3):e402–8. doi: 10.4088/JCP.11m06875
40. Lambert M, Schöttle D, Bock T, Schulte-Markwort M, Naber D, Karow A. Hamburger Modell der integrierten Versorgung von schwer erkrankten Psychosepatienten. Psychotherapeut (2014) 59(2):95–9. doi: 10.1007/s00278-014-1034-8
41. Karow A, Bock T, Daubmann A, Meigel-Schleiff C, Lange B, Lange M, et al. The Hamburg-model of integrated care for patients with psychosis: part 2. Results of the clinical course over 2- and 4-years of treatment. Psychiatr Prax (2014) 41(5):266–73. doi: 10.1055/s-0033-1349496
42. Lambert M, Bock T, Daubmann A, Meigel-Schleiff C, Lange B, Lange M, et al. The Hamburg-model of integrated care for patients with psychosis: part 1. Rationale, treatment concept and results of the pre-study. Psychiatr Prax (2014) 41(5):257–65. doi: 10.1055/s-0033-1349497
43. Lambert M, Ruppelt F, Siem AK, Rohenkohl AC, Kraft V, Luedecke D, et al. Comorbidity of chronic somatic diseases in patients with psychotic disorders and their influence on 4-year outcomes of integrated care treatment (ACCESS II study). Schizophr Res (2018) 193:377–83. doi: 10.1016/j.schres.2017.07.036
44. Lambert M, Schottle D, Ruppelt F, Ludecke D, Sarikaya G, Schulte-Markwort M, et al. Integrated care for patients with first and multiple episodes of severe psychotic illnesses: 3-year results of the Hamburg model. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz (2015) 58(4-5):408–19. doi: 10.1007/s00103-015-2123-8
45. Lambert M, Schottle D, Ruppelt F, Rohenkohl A, Sengutta M, Luedecke D, et al. Early detection and integrated care for adolescents and young adults with psychotic disorders: the ACCESS III study. Acta Psychiatr Scand (2017) 136(2):188–200. doi: 10.1111/acps.12762
46. Lambert M, Schottle D, Sengutta M, Ludecke D, Nawara AL, Galling B, et al. Early detection and integrated care in adolescents and young adults with severe psychotic illnesses. Psychiatr Prax (2015) 42 Suppl 1:S49–53. doi: 10.1055/s-0034-1387652
47. Lambert M, Schottle D, Sengutta M, Ruppelt F, Rohenkohl A, Luedecke D, et al. Early detection and integrated care for adolescents and young adults with severe psychotic disorders: rationales and design of the Integrated Care in Early Psychosis Study (ACCESS III). Early Interv Psychiatry (2018) 12(1):96–106. doi: 10.1111/eip.12361
48. Schottle D, Ruppelt F, Karow A, Lambert M. Home treatment—a treatment model of integrated care in Hamburg. Psychother Psychosom Med Psychol (2015) 65(3-4):140–5. doi: 10.1055/s-0034-1390424
49. Schottle D, Schimmelmann BG, Ruppelt F, Bussopulos A, Frieling M, Nika E, et al. Effectiveness of integrated care including therapeutic assertive community treatment in severe schizophrenia-spectrum and bipolar I disorders: Four-year follow-up of the ACCESS II study. PloS One (2018) 13(2):e0192929. doi: 10.1371/journal.pone.0192929
50. McGarvey EL, Leon-Verdin M, Wanchek TN, Bonnie RJ. Decisions to initiate involuntary commitment: the role of intensive community services and other factors. Psychiatr Serv (2013) 64(2):120–6. doi: 10.1176/appi.ps.000692012
51. Lorant V, Depuydt C, Gillain B, Guillet A, Dubois V. Involuntary commitment in psychiatric care: what drives the decision? Soc Psychiatr Psychiatr Epidemiol (2007) 42(5):360–5. doi: 10.1007/s00127-007-0175-2
52. Juckel G, Haussleiter I. Involuntary Admissions in Accordance to the Mental Health Act (PsychKG)—what are the strongest predictors? Psychiatr Prax (2015) 42(3):133–9. doi: 10.1055/s-0034-1369866
53. Killaspy H, Kingett S, Bebbington P, Blizard R, Johnson S, Nolan F, et al. Randomised evaluation of assertive community treatment: 3-year outcomes. Br J Psychiatry (2009) 195(1):81–2. doi: 10.1192/bjp.bp.108.059303
54. Cotton MA, Johnson S, Bindman J, Sandor A, White IR, Thornicroft G, et al. An investigation of factors associated with psychiatric hospital admission despite the presence of crisis resolution teams. BMC Psychiatry (2007) 7:52. doi: 10.1186/1471-244X-7-52
55. Johnson S, Nolan F, Hoult J, White IR, Bebbington P, Sandor A, et al. Outcomes of crises before and after introduction of a crisis resolution team. Br J Psychiatry (2005) 187:68–75. doi: 10.1192/bjp.187.1.68
56. Keown P, Tacchi MJ, Niemiec S, Hughes J. Changes to mental healthcare for working age adults: impact of a crisis team and an assertive outreach team. Psychiatr Bull (2018) 31(8):288–92. doi: 10.1192/pb.bp.106.012054
57. Kalisova L, Raboch J, Nawka A, Sampogna G, Cihal L, Kallert TW, et al. Do patient and ward-related characteristics influence the use of coercive measures? Results from the EUNOMIA international study. Soc Psychiatr Psychiatr Epidemiol (2014) 49(10):1619–29. doi: 10.1007/s00127-014-0872-6
58. Wullschleger A, Berg J, Bermpohl F, Montag C. Can “Model projects of need-adapted care” reduce involuntary hospital treatment and the use of coercive measures? Front Psychiatry (2018) 9:168. doi: 10.3389/fpsyt.2018.00168
59. Ohlenschlaeger J, Nordentoft M, Thorup A, Jeppesen P, Petersen L, Christensen TO, et al. Effect of integrated treatment on the use of coercive measures in first-episode schizophrenia-spectrum disorder. A randomized clinical trial. Intl J Law Psychiatry (2008) 31(1):72–6. doi: 10.1016/j.ijlp.2007.11.003
60. Tyrer P, Gordon F, Nourmand S, Lawrence M, Curran C, Southgate D, et al. Controlled comparison of two crisis resolution and home treatment teams. Psychiatrist (2018) 34(2):50–4. doi: 10.1192/pb.bp.108.023077
61. Berghofer A, Hubmann S, Birker T, Hejnal T, Fischer F. Evaluation of quality indicators of integrated care in a regional psychiatry budget—a pre-post comparison by secondary data analysis. Int J Integr Care (2016) 16(4):17. doi: 10.5334/ijic.2479
62. First MB, Spitzer RL, Miriam G, Williams JBW. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition. (SCID-I/P). New York: Biometrics Research, New York State Psychiatric Institute; (2002).
63. Overall J, Gorham D. The brief psychiatric rating scale. Psychol Rep (1962) 10:799–812. doi: 10.2466/pr0.1962.10.3.799
64. Teague GB, Bond GR, Drake RE. Program fidelity in assertive community treatment: development and use of a measure. Am J Orthopsychiatry (1998) 68(2):216–32. doi: 10.1037/h0080331
65. Lambert M, Conus P, Cotton S, Robinson J, McGorry PD, Schimmelmann BG. Prevalence, predictors, and consequences of long-term refusal of antipsychotic treatment in first-episode psychosis. J Clin Psychopharmacol (2010) 30(5):565–72. doi: 10.1097/JCP.0b013e3181f058a0
66. Tohen M, Hennen J, Zarate CM Jr., Baldessarini RJ, Strakowski SM, Stoll AL, et al. Two-year syndromal and functional recovery in 219 cases of first-episode major affective disorder with psychotic features. Am J Psychiatry (2000) 157(2):220–8. doi: 10.1176/appi.ajp.157.2.220
67. McGorry PD, Copolov DL, Singh BS. Royal Park Multidiagnostic Instrument for Psychosis: part I. Rationale and review. Schizophr Bull (1990) 16(3):501–15. doi: 10.1093/schbul/16.3.501
68. McGorry PD, Singh BS, Copolov DL, Kaplan I, Dossetor CR, van Riel RJ. Royal Park Multidiagnostic Instrument for Psychosis: part II. Development, reliability, and validity. Schizophr Bull (1990) 16(3):517–36. doi: 10.1093/schbul/16.3.517
69. Schimmelmann BG, Huber CG, Lambert M, Cotton S, McGorry PD, Conus P. Impact of duration of untreated psychosis on pre-treatment, baseline, and outcome characteristics in an epidemiological first-episode psychosis cohort. J Psychiatr Res (2008) 42(12):982–90. doi: 10.1016/j.jpsychires.2007.12.001
70. Kane JM, Leucht S, Carpenter D, Docherty JP. The expert consensus guideline series. Optimizing pharmacologic treatment of psychotic disorders. Introduction: methods, commentary, and summary. J Clin Psychiatry (2003) 64 Suppl 12:5–19.
71. Guy W. Clinical Global Impression. In: Guy, W, and Rockville, M, editors. National Institute for Mental Health. MD: US Department of Heath, Education, and Welfare Public Health Service Alcohol, Drug Abuse, and Mental Health Administration. (1976). doi: 10.1037/t48216-000
72. American Psychiatric Association DI. In: Association, A, editor. Diagnostic and Statistical Manual of Mental Disorders, DSM IV., APA. Washington, DC: American Psychiatric Association and Task Force on DSM IV (1994).
73. Ritsner M, Kurs R, Gibel A, Ratner Y, Endicott J. Validity of an abbreviated quality of life enjoyment and satisfaction questionnaire (Q-LES-Q-18) for schizophrenia, schizoaffective, and mood disorder patients. Qual Life Res (2005) 14(7):1693–703. doi: 10.1007/s11136-005-2816-9
74. Nguyen TD, Attkisson CC, Stegner BL. Assessment of patient satisfaction: development and refinement of a service evaluation questionnaire. Eval Program Plann (1983) 6(3-4):299–313. doi: 10.1016/0149-7189(83)90010-1
75. Bertelsen M, Jeppesen P, Petersen L, Thorup A, Ohlenschlaeger J, le Quach P, et al. Five-year follow-up of a randomized multicenter trial of intensive early intervention vs standard treatment for patients with a first episode of psychotic illness: the OPUS trial. Arch Gen Psychiatry (2008) 65(7):762–71. doi: 10.1001/archpsyc.65.7.762
76. Burns T, Fioritti A, Holloway F, Malm U, Rossler W. Case management and assertive community treatment in Europe. Psychiatr Serv (2001) 52(5):631–6. doi: 10.1176/appi.ps.52.5.631
77. Secher RG, Hjorthoj CR, Austin SF, Thorup A, Jeppesen P, Mors O, et al. Ten-year follow-up of the OPUS specialized early intervention trial for patients with a first episode of psychosis. Schizophr Bull (2015) 41(3):617–26. doi: 10.1093/schbul/sbu155
78. Craig TK, Garety P, Power P, Rahaman N, Colbert S, Fornells-Ambrojo M, et al. The Lambeth Early Onset (LEO) Team: randomised controlled trial of the effectiveness of specialised care for early psychosis. BMJ (2004) 329(7474):1067. doi: 10.1136/bmj.38246.594873.7C
79. Lindenmayer JP, Liu-Seifert H, Kulkarni PM, Kinon BJ, Stauffer V, Edwards SE, et al. Medication nonadherence and treatment outcome in patients with schizophrenia or schizoaffective disorder with suboptimal prior response. J Clin Psychiatry (2009) 70(7):990–6. doi: 10.4088/JCP.08m04221
80. Kane JM, Kishimoto T, Correll CU. Non-adherence to medication in patients with psychotic disorders: epidemiology, contributing factors and management strategies. World Psychiatry (2013) 12(3):216–26. doi: 10.1002/wps.20060
81. Szkultecka-Debek M, Miernik K, Stelmachowski J, Jakovljevic M, Jukic V, Aadamsoo K, et al. Schizophrenia causes significant burden to patients’ and caregivers’ lives. Psychiatr Danub (2016) 28(2):104–10.
82. Suzuki T, Uchida H, Takeuchi H, Tsuboi T, Hirano J, Mimura M. A review on schizophrenia and relapse—a quest for user-friendly psychopharmacotherapy. Hum Psychopharmacol (2014) 29(5):414–26. doi: 10.1002/hup.2421
83. Kahn RS, Sommer IE, Murray RM, Meyer-Lindenberg A, Weinberger DR, Cannon TD, et al. Schizophrenia. Nat Rev Dis Primers (2015) 1:15067. doi: 10.1038/nrdp.2015.67
84. Perkins DO. Predictors of noncompliance in patients with schizophrenia. J Clin Psychiatry (2002) 63(12):1121–8. doi: 10.4088/JCP.v63n1206
85. Lacro JP, Dunn LB, Dolder CR, Leckband SG, Jeste DV. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry (2002) 63(10):892–909. doi: 10.4088/JCP.v63n1007
86. Carbon M, Correll CU. Clinical predictors of therapeutic response to antipsychotics in schizophrenia. Dialogues Clin Neurosci (2014) 16(4):505–24.
87. Weiden PJ, Kozma C, Grogg A, Locklear J. Partial compliance and risk of rehospitalization among California Medicaid patients with schizophrenia. Psychiatr Serv (2004) 55(8):886–91. doi: 10.1176/appi.ps.55.8.886
88. De Hert M, Sermon J, Geerts P, Vansteelandt K, Peuskens J, Detraux J. The use of continuous treatment versus placebo or intermittent treatment strategies in stabilized patients with schizophrenia: a systematic review and meta-analysis of randomized controlled trials with first- and second-generation antipsychotics. CNS Drugs (2015) 29(8):637–58. doi: 10.1007/s40263-015-0269-4
89. Kohigashi M, Kitabayashi Y, Okamura A, Nakamura M, Hoshiyama A, Kunizawa M, et al. Relationship between patients’ quality of life and coercion in psychiatric acute wards. Psychiatr Res (2013) 208(1):88–90. doi: 10.1016/j.psychres.2012.09.040
90. Shannon S, Roche E, Madigan K, Renwick LJ, Dolan C, Devitt P, et al. Quality of life and functioning one year after experiencing accumulated coercive events during psychiatric admission. Psychiatr Serv (2015) 66(8):883–7. doi: 10.1176/appi.ps.201400212
91. Ohlenschlaeger J, Thorup A, Petersen L, Jeppesen P, Koster A, Munkner R, et al. Intensive treatment models and coercion. Nord J Psychiatry (2007) 61(5):369–78. doi: 10.1080/08039480701644652
92. Katsakou C, Bowers L, Amos T, Morriss R, Rose D, Wykes T, et al. Coercion and treatment satisfaction among involuntary patients. Psychiatr Serv (2010) 61(3):286–92. doi: 10.1176/ps.2010.61.3.286
Keywords: psychosis, involuntary admissions, coercive, multiple episodes, follow-up
Citation: Schöttle D, Ruppelt F, Schimmelmann BG, Karow A, Bussopulos A, Gallinat J, Wiedemann K, Luedecke D, Rohenkohl AC, Huber CG, Bock T and Lambert M (2019) Reduction of Involuntary Admissions in Patients With Severe Psychotic Disorders Treated in the ACCESS Integrated Care Model Including Therapeutic Assertive Community Treatment. Front. Psychiatry 10:736. doi: 10.3389/fpsyt.2019.00736
Received: 25 April 2019; Accepted: 13 September 2019;
Published: 24 October 2019.
Edited by:
Andres Ricardo Schneeberger, Albert Einstein College of Medicine, United StatesReviewed by:
Domenico Giacco, Queen Mary University of London, United KingdomMaaike Van Vugt, Trimbos Institute, Netherlands
Copyright © 2019 Schöttle, Ruppelt, Schimmelmann, Karow, Bussopulos, Gallinat, Wiedemann, Luedecke, Rohenkohl, Huber, Bock and Lambert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Schöttle, ZC5zY2hvZXR0bGVAdWtlLmRl