
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Psychiatry, 23 July 2019
Sec. Child and Adolescent Psychiatry
Volume 10 - 2019 | https://doi.org/10.3389/fpsyt.2019.00512
This article is part of the Research TopicPsychopathology Among Youth in the 21st Century: Examining Influences from Culture, Society and Technology View all 21 articles
 John Chee Meng Wong1*†
John Chee Meng Wong1*† Michelle Jing Si Wan2†
Michelle Jing Si Wan2† Leoniek Kroneman3
Leoniek Kroneman3 Takahiro A. Kato4T. Wing Lo5
Takahiro A. Kato4T. Wing Lo5 Paul Wai-Ching Wong6
Paul Wai-Ching Wong6 Gloria Hongyee Chan7
Gloria Hongyee Chan7Hikikomori, which originated in Japan, refers to the condition where youths withdraw into the home and do not participate in society for an extended period of time. Recent updates on hikikomori presentation within the region were exchanged at a Hikikomori Round Table and Regional Symposium (HRTRS) discussion late 2017, leading to this perspective paper. Hikikomori presents as an overall homogeneous construct, while diversity in clinical presentation exists across East Asian countries. We examined the various presentations, risk factors, theoretical frameworks, and classification issues about hikikomori. In particular, specific risk factors have emerged to some degree across the region, while some are more locale specific. We propose that hikikomori youths have differential onset and developmental patterns, potentially resulting in heterogeneous presentation. We briefly summarized existing interventions in the East Asian region. Intervention strategies need to be tailored to different subtypes. A multicomponent approach would address complexity, multifactorial onset, and development of the condition. The HRTRS presented to participating countries the opportunity to collectively work toward a more universal definition of the hikikomori condition and explored innovative ways to shape existing service structures. Opportunities for participating countries described pertain to early detection of cases, adoption of assessment tools, and improved intervention services.
Youths who experience prolonged social withdrawal and retreat into homebound states have been referred to as hikikomori (Japan), hidden youth (China, Hong Kong, and Singapore), or socially withdrawn youth (South Korea and Hong Kong). They cause significant social and health concerns, with associated intervention complexities and poorly understood psychopathology, inviting controversy among social work agencies and policy makers (1).
At the Hikikomori Round Table and Regional Symposium (HRTRS) hosted by the National University of Singapore in November 2017, researchers and clinicians from Japan, Hong Kong, South Korea, China, and Singapore convened to share findings toward progressive understanding of the phenomenon.
The HRTRS aimed to describe varying cultural and regional presentations of hikikomori, highlight evidence-based interventions to map out a consensus toward clinical definition, and discuss appropriate sociopolitical responses for the East Asian countries represented. Although the condition has been ubiquitously reported globally, including several European countries, India, and the US (2–6), this article focuses on East Asia where the phenomenon is better differentiated and described. The present article aims to overview similarities and differences in identification, intervention, and support strategies to summarize opportunities in the region.
Prevalence estimates are only available for Japan and Hong Kong (7, 8). For Japan, the lifetime prevalence rate of social withdrawal of 6 months or more was 1.2% (based on face-to-face survey), while for Hong Kong, it was 1.9% (based on telephone survey). Some argue that the hikikomori condition is becoming more prevalent. If so, it is not known whether this surge is due to increased awareness, improved identification of cases, or causes such as financial circumstance or increased internet usage. In particular, increased internet usage, online gaming, and consequently, the rise of internet-associated addictions may play an important part in the rising rates of social withdrawal (9). Online food delivery and shopping platforms that provide resources and services to the doorstep may further facilitate social withdrawal and disengagement.
During the HRTRS, a broad definition was used to accommodate regional differences. Hikikomori is a condition where socially withdrawn youths aged 12–30 years isolated at home for 3–6 months or more, may experience distress, impaired daily functioning, or psychiatric comorbidity. This definition implies that not all those with hikikomori are dysfunctional, and not all those with hikikomori perceive themselves as being dysfunctional. Existing assessment tools include screening questionnaires, such as a self-report Hikikomori screening questionnaire (HQ-25) validated in a Japanese sample (10), and a proposed diagnostic interview tool (6). In addition, research has included social interaction models and biomarkers (11, 12), tools not yet applicable to clinical assessments in distinguishing subtypes of hikikomori.
Hikikomori presents with different stage, duration, and degree of social withdrawal that may be due to differential developmental course of the condition. A Hong Kong study showed that self-reports of self-efficacy, self-esteem, subcultural identity, and empowerment were initially low in youths with 3 to 24 months of social withdrawal but improved beyond 24 months. This positive trend may be due to formation of a subcultural identity within the online community that allowed youths to realize their full potential. Moreover, prolonged social withdrawal was associated with improved physical, social, and psychological quality of life over time (13). Retrospective viewpoints of formerly withdrawn youth suggest that initial phases of social withdrawal may confer a private status that blinds them to the dangers of social skill deterioration and increased apathy, submersed in this state over time (14). These findings await replication in other regions. A cross-national study of 36 socially withdrawn males with an average duration of 2.1 years showed high levels of loneliness and moderate functional impairment (6), but the sample size did not allow for analyses by duration of social withdrawal. In addition, youths often show fluctuations in the degree of withdrawal in all regions (15). This varies from exclusive seclusion in one’s bedroom, to youths with no contact with others outside the nuclear family, to youths who infrequently leave home for sustenance.
Variance in duration and form of social withdrawal moderate the corresponding impact on the individual, family, and society. While some hikikomori may not experience a decrease in quality of life, negative behavioral and social consequences may arise from complications associated with a sedentary lifestyle. In Asian societies that emphasize individual industrialism and regular routines, disrupted dietary routines and sleep diurnal reversal patterns are frowned upon, compounded by negative impacts on physical health (12). Adverse social impacts on families include social distancing between family members, escalating to marital and parent–child conflict, sibling rivalry, loss of youth’s potential earnings, and depleting parents’ savings. Socioeconomic costs include reduced available human capital and possibly negative impacts on population growth.
Hikikomori carries high psychiatric comorbidity across Asian populations. A Japanese study showed 80% of help-seeking hikikomori met the criteria for a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision diagnosis (16), including avoidant personality, social anxiety disorder, and major depression. In addition, autistic spectrum disorders and prodromal states of schizophrenia may also demonstrate overlapping symptomatology (3, 6).
In order to further our understanding of the hikikomori phenomenon, a typology distinguishing primary versus secondary hikikomori has been proposed. Suwa and Suzuki (17) and Li and Wong (4) propose a distinction between primary versus secondary hikikomori. Primary hikikomori has no evident psychiatric disorder, while secondary hikikomori has social withdrawal attributable to the presence of psychiatric disorders. This classification of hikikomori is theoretical, while there is little empirical evidence for such a distinction (18). Existing literature indicates substantial numbers of secondary hikikomori in the respective studied populations. However, this may be ascribed to the fact that mental health and social services remain their main receptor platforms and treatment centers. In contrast, primary hikikomori may chiefly be identified through novel research studies designed to capture this elusive group. Furthermore, the primary hikikomori concept remains poorly defined and unstandardized across studies and countries. For instance, all socially withdrawn youths in South Korea are considered primary hikikomori, while Japan includes those with or without psychiatric comorbidities. This alludes to directional uncertainty on whether prolonged social withdrawal is caused by, correlated with, or causes psychiatric disorders.
Another theoretical framework describes socially withdrawn youths as a function of different interactions between individual, family, school, and social factors (4) via different types of social withdrawal processes. Some youths may lack autonomy due to overprotective parenting and financial overdependence. Others may experience existential uncertainty due to discrepancy between parental expectations for achievement and their prospective outcomes. However, no studies to date have examined these underlying mechanisms.
The best-known risk factors for hikikomori are the presence of a psychiatric disorder, developmental disorder, substance-related or behavioral addictive disorders (including Internet and gaming misuse), and poor psychosocial contexts (5, 16, 19). Various risk factors that emerge from the literature are universal among the East Asian regions, including male gender, insecure attachment (20), and psychiatric conditions. Conversely, other risk factors achieve less consensus. Studies on clinically detected hikikomori in Japan, for example, demonstrate that high educational status of families, especially fathers, is reported to increase the risk of hikikomori (21). However, it has been suggested that these studies of clinically detected hikikomori may not represent hikikomori receiving assistance from nonprofit organizations or no assistance at all (22). Hikikomori in Hong Kong detected through social service platforms, for instance, emerges in diversified contexts including low socioeconomic status (SES) families with single parents. However, 80% of cases from Hong Kong emerge from middle to high SES families, mirroring trends observed in Japan.
In countries with high costs of living such as Hong Kong and Singapore, a family with high SES may accommodate financial burden of the hikikomori individual. For anomalies with low SES, several clinicians at the HRTRS anecdotally hypothesized that they may possess specific attributes, such as high cognitive function or remote earning capabilities. Furthermore, low familial support and maternal mental disorder were also positively associated with hikikomori (21).
Dependent behavior described as “amae” in Japanese parent–child relationships has been hypothesized to play a role in developing social withdrawal (23) by normalizing and encouraging the acceptance of their socially withdrawn child (HRTRS) (24) staying at home. These mechanisms await further investigation in the various regions. East Asian parenting styles tend to embody the mother–child relationship as interdependent cooperation, in contrast to the focus on evolving independence and autonomy in Western regions (25). In Korea, the youth culture incorporates a strong sense of cohesion and engagement through social gatherings. When individuals are isolated for more than 6 months, it is perceived as a sign of mental illness. Lastly, preliminary studies in Japan and Hong Kong have begun investigating physiological biomarkers and physical health parameters, respectively, that may eventually contribute to early identification (11, 12).
Furthermore, studies point to the overlap between social withdrawal and Internet and gaming addiction [e.g. Refs. (18, 26)]. Benarous and colleagues, for instance, describe how avoidance and social withdrawal as a persistent maladaptive reaction in a patient with an anxious–avoidant insecure attachment plays a key role in the emergence and persistence of Internet gaming disorder. Lastly, the stigma surrounding mental illness diagnoses may result in preference for hikikomori labeling to mask psychiatric conditions.
Table 1 shows inter-regional presentations of the hikikomori phenomenon, elucidating heterogeneity across regions. The infrastructure to address social or mental health issues determines main modes of identification for the autonomous regions and, in turn, the locale-specific hallmarks of the hikikomori condition. However, regardless of the identification method, hikikomori youths are a heterogeneous population due to differing causes unique to the specific youth.
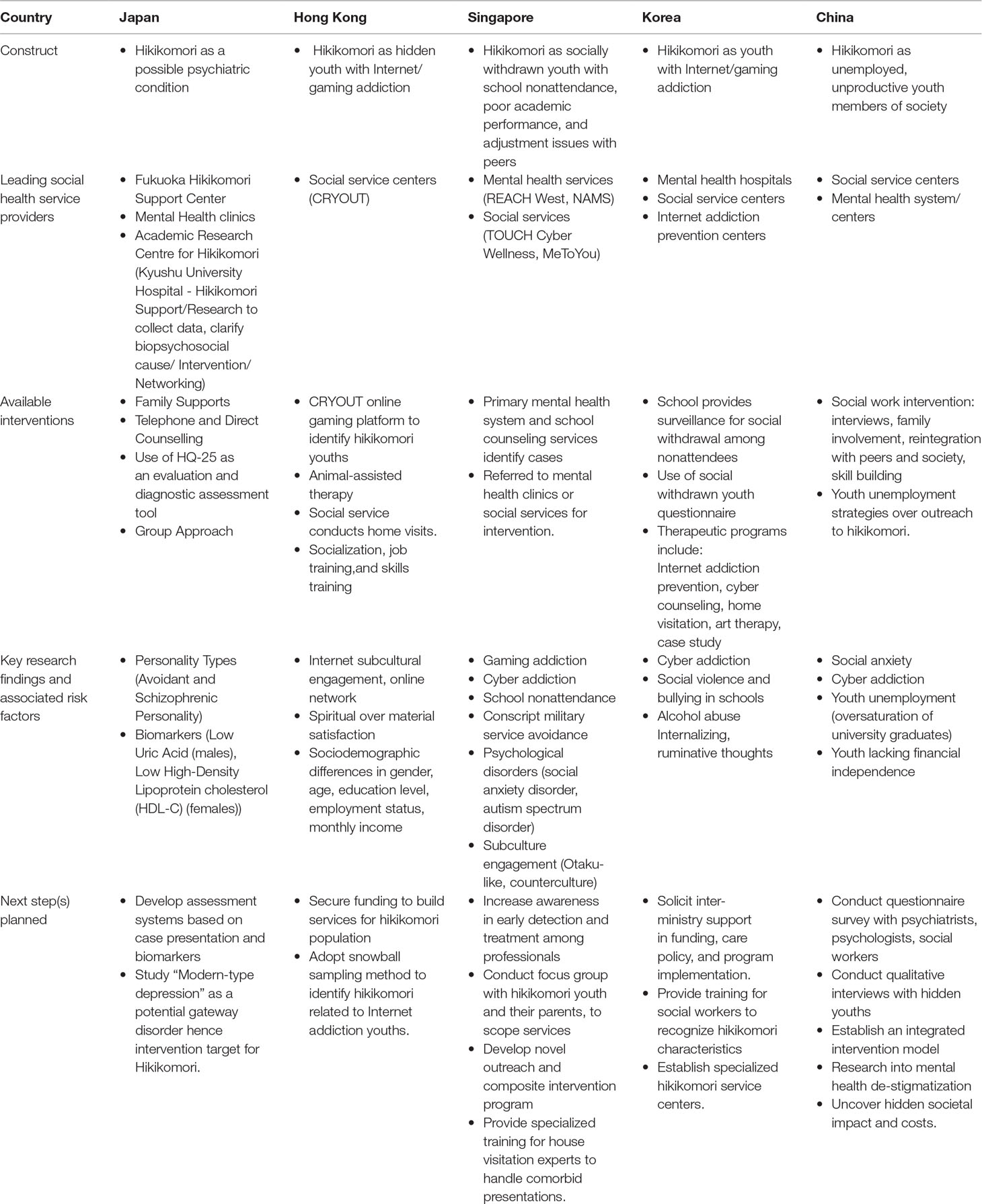
Table 1 Cross-regional presentation of hikikomori phenomenon.
Various healthcare interventions including family, individual, and group counseling or therapy, clinical psychological assessment, and medication or hospitalization exist for hikikomori in various countries. In addition, support and management services including group and interest activities, socialization and skills training, parenting advice, and community education may also be offered (27). Different interventions exist in disparate East Asian regions (refer to Table 1). These include home visits, befriending, psychodynamic therapy, parent support groups, Internet addiction programs, art therapy, cyber counseling, e-mentoring, family therapy, pharmacotherapy, animal-assisted therapy (AAT), and halfway homes. Specialized services catered to the hikikomori population exist in Japan and Hong Kong. Interventions are offered through specialized centers (Japan), general (psychiatric) hospitals (China and Singapore), schools (Singapore), government agencies (South Korea) or voluntary welfare organizations, and social agencies (Hong Kong, Singapore, and Japan). Interventions are often administered by social workers and mental health professionals. In China, apart from social work intervention (28, 29), ideological and moral education have also been advocated (30). Currently, referrals are based on condition presentation and location of identification. For instance, a socially withdrawn youth replying to a question in an online game receives cyber counseling, school nonattenders receive intervention through governmental agencies, and parents of socially withdrawn children mostly turn to psychiatric hospitals.
To date, published evidence on treatments for this group is scarce. In their review, Li and Wong (4) identified one empirical evaluation of an intervention specifically targeted at the hikikomori condition, involving a home visitation program conducted in Korea (19). More recently, Wong and colleagues (31) examined the effectiveness of a multicomponent program with animal-assisted therapy (AAT) for socially withdrawn youth in Hong Kong. Program evaluation indicated enhanced self-esteem and perceived employability, and reduced social anxiety. The AAT component did not significantly add to program outcomes but appeared effective in promoting enrolment. During the HRTRS, various strategies to attract and incentivize youth into accepting social and therapeutic interventions were discussed. These include online treatments, potentially incorporated into online gaming, and messaging platforms in Hong Kong’s programs. However, the efficacy of these pilot interventions has yet to be assessed. In a cross-national study of 36 socially withdrawn males, a consistent preference for treatment delivered in person over tele-psychiatry was expressed (6). Although social media advertising has demonstrated nominal capacity to detect hikikomori (32), the potential for effective online interventions to bridge the therapeutic gap remains unclear.
In line with other mental health conditions and drawing from the various presentations, intervention strategies evidently need to be tailored to heterogeneous hikikomori subtypes. A multicomponent approach would address complexity, multifactorial onset, and development of the condition. This multicomponent approach should always include youth empowerment and family interventions, whereas AAT should be second-line treatment. For instance, the most severe cases of exclusive seclusion at home may require intensive home visits, coupled with AAT. Alternatively, youths experiencing withdrawal as a transitory state may respond to interventions targeting school resumption and reemployment. In addition, interventions may differ depending on withdrawal duration. Earlier intervention is advantageous to directly address youths with impaired daily functioning. The optimal time frame for intervention appears to be after 3 months of withdrawal, before youths are officially characterized as hikikomori (withdrawal >6 months). At this interval, the joys of regained autonomy have faded, and youths begin to realize the downside but have yet to regain renewed “self-efficacy” and a new sense of hikikomori identity cultivated by a prolonged state of social withdrawal—typically after 2 years.
Challenges across countries concern the difficulty of case detection due to its hidden nature (32) and that youths may not pathologize this state. Another closely related challenge relates to motivating hikikomori youth to access services or treatment and to return to society. The fragmented knowledge of the condition also hampers optimal intervention. The heterogeneity in presentation, developmental pathways, risk and protective factors, and underlying mechanisms, within regions and across regions, have led to a wide range of services currently being offered, often of unknown efficacy.
The components of challenges at the societal or country level include recognizing burden of care on family and society and the role of authorities or policy makers. As the individual is nested in an ecological social system, the involvement of peers and family is essential to scaffold intervention. Authorities and policy makers may prioritize service planning and implementation by reinforcing case detection by effective gatekeepers. State policy and funding should also focus on awareness, advocacy, and fostering interorganizational collaboration.
The HRTRS presented an opportunity to collectively work toward a more universal definition of the hikikomori condition and explore innovative ways to shape existing service structures. These opportunities pertain to early detection of cases, adoption of assessment tools, and improved intervention services.
Development of opportunities is critical for early detection in the respective regions, through evolving the existing service structures to fit the needs of their youths. For example, primary and secondary school attendance is compulsory and tracked in Singapore. Prolonged absence from school without medical reason could trigger a home visit by a trained social worker. In Hong Kong, it may be helpful to raise awareness to recognize hikikomori symptoms among general practitioners, teachers, and parents, since hikikomori is currently mainly detected through online gaming platforms.
Next, standardization of screening and assessment tools would align primary evaluation within a validated diagnostic framework. We recommend to adopt the HQ-25 screening instrument, as it is theoretically grounded, easy to administer, and shows encouraging psychometric properties (10). We propose that a common method of identification would allow construction of a pathway to justify combinations of recommended interventions. These interventions would directly target affirmed symptomology and causes specific to the hikikomori individual.
As hikikomori is a multifaceted condition, an intervention model that integrates various possible factors affecting the individual could structure and direct intervention. Each country has differing approaches to case identification but may additionally adopt aspects of intervention from other regions to construct a complete biopsychosocial intervention. For example, Singapore may consider adapting AAT into their programs for hikikomori with low motivation and severe withdrawal. For Japan, which has strengths in biological identification and psychiatric and social services, they may consider working toward a more integrated and unified approach. Through a shared information network on research protocol and standardized outcome measurements, different countries may create their own integrated intervention model specific to local needs.
Furthermore, it may be beneficial for regions to examine innovative treatment approaches. The use of augmented reality games to draw socially withdrawn youths out of their rooms and into the real world (33, 34) has recently been suggested. One potential development may include introducing gaming stations at therapy centers and devising activities that encourage offline cooperation and interaction. Another potential avenue pertains to integrating therapeutic gaming with exposure therapy strategies by introducing hikikomori to virtual reality experiences, then shared virtual reality environments, before resocialization into society (9).
The lack of large-scale standardized research has previously been highlighted by multiple authors (4, 35). Future studies should include structured psychiatric assessments to investigate primary hikikomori and associated psychosocial comorbidities to better delineate the cause–effect relationship and intervention touch points for improved outcomes. Furthermore, the debate underlying hikikomori classification is between one camp that contends that it deserves a stand-alone diagnosis in the Diagnostic and Statistical Manual of Mental Disorders versus another that argues hikikomori is simply a secondary effect of other psychiatric conditions. Select studies currently differentiate between onset of other psychiatric conditions before, during, and after hikikomori onset (7). This operational method could be used to differentiate primary and secondary hikikomori and align existing and future literature in streamlining manifestation of psychiatric comorbidity. This would better define case selection for cluster analysis of treatment outcomes and comparison across countries.
In addition, the examination and detection of precursors in large-scale longitudinal epidemiological studies will further enhance early intervention opportunities to prevent withdrawal or limit withdrawal duration. Future studies should also examine Internet and gaming addictions in relation to the hikikomori condition. These collective efforts will further our understanding of this complex phenomenon and consequently improve services provided to prevent or mitigate youth from prolonged social withdrawal.
JW and MW organized the HRTRS and collated all discussions. MW and LK wrote the manuscript. TK, PW, WL, and GC contributed their insights to the HRTRS and the manuscript. All authors contributed to manuscript revision and read and approved the submitted version.
The Round Table and Regional Symposium have been partly funded by the NUS Mind Science Center, National University of Singapore. No other sources of funding have been received for this event.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank all researcher and clinician attendees of the Hikikomori Round Table and Regional Symposium (HRTRS) from Japan, Hong Kong, South Korea, China, and Singapore for their content presentation and contribution of insights. We would also like to acknowledge Ms Rachael Lee Zhi Yi and Mr Jonathan Wong Yao Zhang, for their contributions.
2. Chauliac N, Couillet A, Faivre S, Brochard N, Terra JL. Characteristics of socially withdrawn youth in France: a retrospective study. Int J Soc Psychiatry (2017) 63(4):339–44. doi: 10.1177/0020764017704474
3. Kato TA, Kanba S, Teo AR. Hikikomori: experience in Japan and international relevance. World Psychiatry (2018) 17(1):105–6. doi: 10.1002/wps.20497
4. Li TMH, Wong PWC. Editorial Commentary: pathological social withdrawal during in adolescence: a culture-specific or a global phenomenon? J Child Psychol Psychiatry (2015) 56(10):1039–41. doi: 10.1111/jcpp.12440
5. Malagón-Amor A, Córcoles-Martínez D, Martín-López LM, Pérez-Solà V. Hikikomori in Spain: a descriptive study. Int J Soc Psychiatry (2015) 61(5):475–83. doi: 10.1177/0020764014553003
6. Teo AR, Fetters MD, Stufflebam K, Tateno M, Balhara Y, Choi TY, et al. Identification of the hikikomori syndrome of social withdrawal: psychosocial features and treatment preferences in four countries. Int J Soc Psychiatry (2015) 61(1):64–72. doi: 10.1177/0020764014535758
7. Koyama A, Miyake Y, Kawakami N, Tsuchiya M, Tachimori H, Takeshima T. Lifetime prevalence, psychiatric comorbidity and demographic correlates of “hikikomori” in a community population in Japan. Psychiatry Res (2010) 176(1):69–74. doi: 10.1016/j.psychres.2008.10.019
8. Wong PWC, Li TMH, Chan M, Law YW, Chau M, Cheng C, et al. The prevalence and correlates of severe social withdrawal (hikikomori) in Hong Kong: a cross-sectional telephone-based survey study. Int J Soc Psychiatry (2014) 61(4):330–42. doi: 10.1177/0020764014543711
9. Hussain WMHW. Augmented reality games (ARG) and Pokémon go: preventing hikikomori in Malaysia. Int J Civ Eng Technol (2018) 9(5):1128–35. http://www.iaeme.com/ijciet/issues.asp?JType=IJCIET&VType=9&IType=5
10. Teo AR, Chen JI, Kubo H, Katsuki R, Sato-Kasai M, Shimokawa N, et al. Development and validation of the 25-item Hikikomori Questionnaire (HQ-25). Psychiatry Clin Neurosci (2018). 72(10):780–8. doi: 10.1111/pcn.12691
11. Hayakawa K, Kato TA, Watabe M, Teo AR, Horikawa H, Kuwano N, et al. Blood biomarkers of Hikikomori, a severe social withdrawal syndrome. Sci Rep (2018) 8(1):2884. doi: 10.1038/s41598-018-21260-w
12. Yuen JW, Yan YK, Wong VC, Tam WW, So KW, Chien WT. A physical health profile of youths living with a “Hikikomori” lifestyle. Int J Environ Res Public Health (2018) 15(2):315. doi: 10.3390/ijerph15020315
13. Chan HY, Lo TW. Quality of life of the hidden youth in Hong Kong. Appl Res Qual Life (2014a) 9(4):951–69. doi: 10.1007/s11482-013-9279-x
14. Li TM, Liu L, Wong PW. Withdrawal experience and possible way-outs from withdrawal behavior in young people. Qual Soc Work (2018) 17(4):537–55. 1473325016688369. doi: 10.1177/1473325016688369
15. Round Table and Regional Symposium Hikikomori – Hidden Youth Syndrome. Regional technical Report. (2017). NUS Mind-Science Centre, National University of Singapore.
16. Kondo N, Sakai M, Kuroda Y, Kiyota Y, Kitabata Y, Kurosawa M. General condition of Hikikomori (prolonged social withdrawal) in Japan: psychiatric diagnosis and outcome in mental health welfare centres. Int J Soc Psychiatry (2013) 59(1):79–86. doi: 10.1177/0020764011423611
17. Suwa M, Suzuki K. The phenomenon of “hikikomori” (social withdrawal) and the socio-cultural situation in Japan today. J Psychopathol (2013) 19:191–8. https://pdfs.semanticscholar.org/98f2/467ed738530f738605da9b5aa5b20251fb86.pdf
18. Stip E, Thibault A, Beauchamp-Chatel A, Kisely S. Internet addiction, hikikomori syndrome, and the prodromal phase of psychosis. Front Psychiatry (2016) 7:6. doi: 10.3389/fpsyt.2016.00006
19. Lee YS, Lee JY, Choi TY, Choi JT. Home visitation program for detecting, evaluating and treating socially withdrawn youth in Korea. Psychiatry Clin Neurosci (2013) 67(4):193–202. doi: 10.1111/pcn.12043
20. Krieg A, Dickie JR. Attachment and hikikomori: a psychosocial developmental model. Int J Soc Psychiatry (2013) 59:61–72. doi: 10.1177/0020764011423182
21. Umeda M, Kawakami N. Association of childhood family environments with the risk of social withdrawal (‘hikikomori’) in the community population in Japan. Psychiatry Clin Neurosci (2012) 66(2):121–9. doi: 10.1111/j.1440-1819.2011.02292.x
22. Tajan N. Social withdrawal and psychiatry: A comprehensive review of Hikikomori. Neuropsychiatr Enfance Adolesc (2015) 63(5):324–31. doi: 10.1016/j.neurenf.2015.03.008
23. Kato TA, Hashimoto R, Hayakawa K, Kubo H, Watabe M, Teo AR, et al. Multidimensional anatomy of ‘modern type depression’ in Japan: A proposal for a different diagnostic approach to depression beyond the DSM-5 . Psychiatry Clin Neurosci (2016) 70(1):7–23. doi: 10.1111/pcn.12360
24. Kato TA, Tateno M, Shinfuku N, Fujisawa D, Teo AR, Sartorius N, et al. Does the ‘hikikomori’ syndrome of social withdrawal exist outside Japan? A preliminary international investigation. Soc Psychiatry Psychiatr Epidemiol (2012) 47:1061–75. doi: 10.1007/s00127-011-0411-7
26. Benarous X, Morales P, Mayer H, Iancu C, Edel Y, Cohen D. Internet gaming disorder in adolescents with psychiatric disorder: two case reports using a developmental framework. Front Psychiatry (2019) 10:336. doi: 10.3389/fpsyt.2019.00336
27. Chan GHY, Lo TW. Hidden youth services: what Hong Kong can learn from Japan. Child Youth Serv Rev (2014b) 42:118–26. doi: 10.1016/j.childyouth.2014.03.021
28. Wang Y. Use of social work in the counselling of hidden youth. J Guangdong Youth Vocat Coll (2016) 30(4).
29. Yang Z. Exploration of the syndrome of hidden youth and its help-seeking path. China Youth Study (2012).
30. Zhang H-M, Liu L-Q. Hidden youth: Special target of ideological and moral education. China Constr Educ (2008) 10(10).
31. Wong PWC, Yu RWM, Li TMH, Lai SLH, Ng HYH, Fan WTH. Efficacy of a multicomponent intervention with animal-assisted therapy for socially withdrawn youth in Hong Kong. Soc Anim (2017), 1–14. doi: 10.1163/15685306-12341462
32. Liu LL, Li TM, Teo AR, Kato TA, Wong PW. Harnessing social media to explore youth social withdrawal in three major cities in China: Cross-Sectional Web Survey. JMIR Ment health (2018) 5(2):1–10. doi: 10.2196/mental.8509
33. Kato TA, Teo AR, Tateno M, Watabe M, Kubo H, Kanba S. Can Pokémon GO rescue shut-ins (hikikomori) from their isolated world? Psychiatry Clin Neurosci (2017a) 71(1):75–6. doi: 10.1111/pcn.12481
34. Kato TA, Shinfuku N, Sartorius N, Kanba S. Loneliness and single-person households: issues of Kodoku-Shi and Hikikomori in Japan. Mental Health and Illness in the City (2017b), 1–15. doi: 10.1007/978-981-10-0752-1_9-1
Keywords: hikikomori, social withdrawal, youth, Asia, challenges, opportunities
Citation: Wong JCM, Wan MJS, Kroneman L, Kato TA, Lo TW, Wong PW-C and Chan GH (2019) Hikikomori Phenomenon in East Asia: Regional Perspectives, Challenges, and Opportunities for Social Health Agencies. Front. Psychiatry 10:512. doi: 10.3389/fpsyt.2019.00512
Received: 23 November 2018; Accepted: 28 June 2019;
Published: 23 July 2019.
Edited by:
Lee Elizabeth Wachtel, Kennedy Krieger Institute, United StatesReviewed by:
Xavier Benarous, Hôpital Pitié-Salpêtrière, France Assistance Publique Hopitaux De Paris, FranceCopyright © 2019 Wong, Wan, Kroneman, Kato, Lo, Wong and Chan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: John C.M. Wong, cGNtd2NtakBudXMuZWR1LnNn
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.