 Suzette Brémault-Phillips
Suzette Brémault-Phillips Ashley Pike
Ashley Pike Francesca Scarcella
Francesca Scarcella Terry Cherwick
Terry Cherwick- 1Department of Occupational Therapy, Faculty of Rehabilitation Medicine, University of Alberta, Edmonton, AB, Canada
- 2Royal Canadian Chaplain Service, Department of National Defence, Edmonton, AB, Canada
Introduction: Moral injury (MI) results when military personnel are exposed to morally injurious events that conflict with their values and beliefs. Given the complexity of MI and its physical, emotional, social, and spiritual impact, a holistic approach is needed. While the biopsychosocial aspects of MI are more commonly addressed, less is known of the spiritual dimension and how to incorporate it into treatment that facilitates restoration of one’s core self and mending of relationships with self, others, and the sacred/Transcendent. The purpose of this study was to gain a greater understanding of the relationship between spirituality/religion (S/R) and MI as experienced by military members and veterans and to consider how S/R might be better integrated into prevention and treatment strategies.
Methods: A mini-review of peer-reviewed articles published between January 2000 and April 2018 regarding the relationship between spirituality and MI among military personnel and veterans was conducted.
Results: Twenty-five articles were included in the final review. Five themes were identified and explored, including i) Spirituality: A potential cause of and protective factor against MI, ii) Self and identity: Lost and found, iii) Meaning-making: What once was and now is, iv) Spirituality as a facilitator of treatment for MI, and v) Faith communities: Possible sources of fragmentation or healing.
Discussion: Findings identified a cyclical relationship between S/R and MI, whereby S/R can both mitigate and exacerbate MI, as well as be affected by it. Seen as a type of S/R struggle, the use of S/R-specific strategies [e.g., forgiveness, review of S/R beliefs, engagement in S/R practices, and (re)connection with S/R communities], integration of S/R perspectives into general interventions, and help from chaplains may support healing, self-regulation, and mending of relationships, moral emotions, and social connection. Further research is yet needed, however, regarding i) S/R orienting systems, interventions, practices, and rituals/ceremonies that might protect against and treat MI; ii) features of individuals who do/do not experience MI; iii) S/R assessment tools and interventions; and iv) ways to maximize the positive contributions of faith communities.
Introduction
Exposure to morally injurious experiences (MIEs) (1–9) that occur in the course of military service can be mentally and spiritually distressing (1, 10). MIEs, experiences that cannot be justified within a member’s personal and moral beliefs, can leave military members struggling to reconcile seemingly irreconcilable discrepancies between their lived experience, beliefs, values, and worldview(s) (11–14). Occurring in the course of military service, missions, disaster relief efforts, stateside and/or training accidents, drone warfare, or military sexual trauma, exposure to MIEs can be life-altering. Serious psychological problems such as posttraumatic stress disorder (PTSD) and moral injury (MI) can arise (11, 15), leaving military members contending with intrusive thoughts, impulsivity, suicidal ideation, sleep disturbances, or substance use; avoiding experiential triggers; and engaging in maladaptive coping, aggressive, self-harming, self-handicapping, or demoralizing behaviors, all of which can be debilitating (11, 13, 16). More fundamentally, individuals can be impacted at the deepest level of their being (17) and spirit (18). As a result, consideration of the spiritual dimension is needed when trying to understand the impact of exposure to MIEs and prevention and treatment of MI.
The Human Spirit
The human spirit is “the essential core of the individual, the deepest part of the self” (p. 58) (15). More than characteristics and roles associated with one’s identity (15), the human spirit is a motivating force directed toward realizing higher-order goals and aspirations that grow out of the essential self (19). When exposed to MIEs, a person’s core self, ideals, and perceptions of reality can be shattered and their spirit “broken,” leaving them spiritually and existentially struggling.
Moral Injury: A Form of Spiritual/Religious Struggle
MI, described as one of several types of S/R struggles (20–24), is associated with questions, disorientation, and tensions about matters of deepest significance that arise within oneself, with other people, and/or with the sacred or Transcendent (15, 25–27). Positively associated with depressive symptoms and negatively with happiness, S/R struggles can impact psychological well-being and health, and cause significant distress (20, 27, 28) and decline (29–31). When a person is unable to resolve S/R struggles, one can experience compromised psychological, social, physical, and spiritual functioning; poor recovery from MI; increased mental health symptoms; and greater risk of mortality. Disconnection from self, others, and the sacred/Transcendent can also occur (22, 26, 31–33). Longer periods of S/R struggle tend to create greater risk (21, 26, 32, 34–38).
Spiritual/Religious Struggles: Potential for Growth and Resilience
An association between S/R struggles and growth is found in the literature (29–31). Rosner and Powell (2006) reported that there is limited empirical evidence that posttraumatic or adversarial growth occurs due to war, and a paucity of evidence that “adversarial growth” during and after war is specifically due to traumatic events (39). More recently, however, exposure to MIEs has been associated with S/R growth, with some veterans reportedly experiencing renewed faith and more frequent use of prayer as a means of protection (40). S/R commitment, life sanctification, support, and hope have been identified as significant buffers against unhappiness, depressive symptoms, and S/R struggles (28). The most significant growth seems to be related to existential and S/R matters (30, 41, 42).
Growth and resilience related to S/R struggles (including recovery, resistance, and reconfiguration) (43) may be predicated on numerous factors. These include a person’s ability to accept the reality of situations, access supports, draw on S/R resources, make meaning of experiences, (re)affirm a sense of purpose, and (re)engage in positive problem-solving actions (41, 42, 44, 45). Further, a person’s history of S/R struggles seems to be an important factor to consider as those with a lifetime history of S/R struggles appear to have lower levels of well-being. One’s standing on the Big Five and religiousness also seems to be a contributing factor, with higher Neuroticism and Openness, and lower Agreeableness and Conscientiousness, being associated with higher lifetime frequency of S/R struggles and degree of current S/R struggles (27). Identifying those at greater risk of S/R struggles based on their history, personality traits, and religiousness, and facilitating their growth and development, may be beneficial for mitigating the impact of MIEs and development of MI.
This article examines peer-reviewed literature on spirituality as it relates to MI among military personnel and veterans, and its role in the prevention of and recovery from MI. While two scoping reviews have explicitly explored spirituality and MI [Carey et. al.’s review focused on MI, spiritual care, and the role of chaplains (46), and Haight et al.’s review focused on social work research (47)], no review to date has looked more specifically at how MI affects the human person—particularly the spirit (or spiritual) dimension of the self and the importance of using a holistic, biopsychosocial–spiritual model when addressing MI. Spirituality and S/R issues, isolated as key aspects of MI (1), warrant further examination regarding their association with MI.
Materials and Methods
The search, selection, and critical assessment of English-language, peer-reviewed manuscripts published between January 2000 and April 2018 were performed independently and blindly by two authors according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (48). Conducted on January 21, 2017, and repeated on April 22, 2018 to identify new articles published between January 2017 and April 2018, the database searches used SocIndex, MEDLINE (with EBSCO), PsycINFO, Web of Science, and Cumulative Index to Nursing & Allied Health Literature (CINAHL). Keywords included the following: “Moral injur*,” “moral emotions, transgressive acts, morals”; military personnel or naval medicine or military medicine or war or aerospace medicine or soldier* or sailor* or air men or air man or airmen or airman or armed forces or air force or military or naval or coast guard* or submariner* or infantr* or marine corps or marines or army or special forces or warfight* or warfare or land mine* or machine gun* or “United States Department of Veterans Affairs” or Veterans or Veterans Health or army or soldier (49) and spiritual* or faith or theolog* or Muslim or “Bapti* or Buddhis* or religi* or Christian* or Judaism or “belief system*” or meaningful* (50) (Figure 1). A manual search of the literature and reference lists was also performed. Data charting utilized data extraction categories suggested by Arksey and O’Malley (51, 52). Concept charting allowed for identification and tracking of overlapping concepts and presenting themes. Discrepancies between authors were resolved through discussion and by consensus.
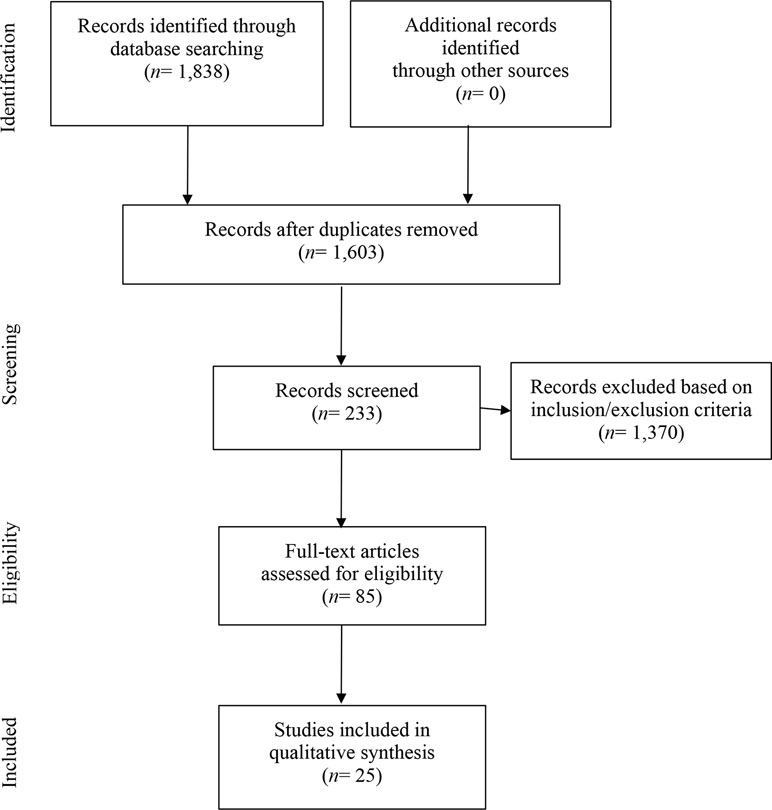
Figure 1 Flowchart of the systematic search. PRISMA flowchart from (82).
Results
Table 1 presents the studies included in the review, author(s), year of publication, study type, population, and study objectives. The following themes regarding MI and spirituality were identified in the course of the review: i) Spirituality: A potential cause of and protective factor against MI, ii) Self and identity: Lost and found, iii) Meaning-making: What once was and now is, iv) Spirituality as a facilitator of treatment for MI, and v) Faith communities: Possible sources of fragmentation or healing. As for populations represented in the articles, 18 of the 25 articles focused on military populations, 2 considered military members and the role of social work, 3 explored military healthcare/religious professionals, 1 focused on individuals including military personnel experiencing moral stress, and 1 included the development of MI and treatment options as it relates to social work practice in morally complex environments including with military personnel. What follows is a description of the key findings.
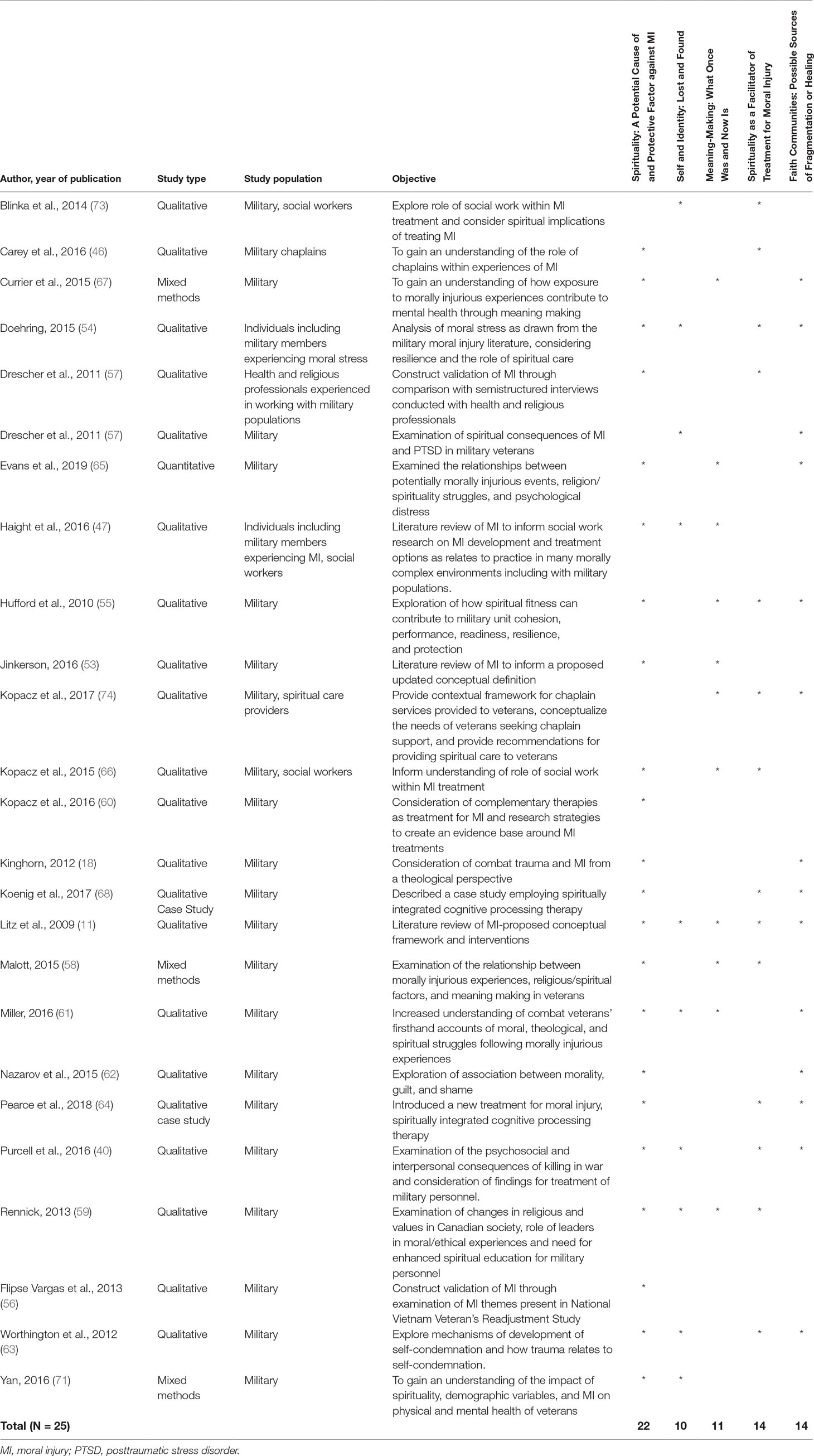
Table 1 Results of peer-reviewed publications on spirituality and moral injury among military personnel (from January 2000 to April 2018).
Moral Injury and Spirituality: Descriptive Summary of the Studies
Spirituality: A Potential Cause of and Protective Factor Against Moral Injury
The literature reflects a close association between MI and spirituality (11, 18, 46, 53–65), with spirituality being described as underlying MI and MI having an equally salient impact on spirituality (55, 58, 61–68). A person’s spiritual worldview contributes to the development of MI, with rigid religious principles and expectations potentially enhancing guilt and self-condemnation following exposure to an MIE (63, 66). Hufford et al. suggested that those who are religious may experience greater distress and may be at greater risk of MI due to existential questioning of a Divine being and a “shattering [of] deeply held spiritual beliefs” (p. 76) (55). Currier et al. (67) noted that insult to one’s religious framework or spiritual belief system may result in distress (40, 55, 61, 62, 67, 69). Interviews with combat veterans considering experiences of MI identified loss, questioning, and disillusionment of faith/a higher power as postdeployment experiences (61). As MI can significantly damage the way a person’s values, beliefs, and spirituality guide daily behaviors, consideration of spiritual or theological perspectives may enhance current psychological and medical understandings of MI (18, 54).
Spirituality is also identified both as a protective factor against MI (55, 58, 70, 71) and as a means of coping with MIEs. Hufford and colleagues suggest that spiritual resilience might provide protection from MI in wartime experiences (55). Malott’s (58) survey of 140 Iraq and Afghanistan veterans found that veterans who utilized daily spiritual practices had increased religious coping abilities and levels of forgiveness (58). Further, military personnel whose spirituality was more refined were found to more readily incorporate MIEs into their spiritual framework, potentially reducing the risk of MI (58). Finally, studies suggest that drawing on spiritual practices and Chaplain services during deployment can support spiritual beliefs and offer understanding and context to MIEs (55, 59).
Self and Identity: Lost and Found
A loss of innocence, self, and soul during and following deployment has been reported by veterans (61). Cognitive dissonance that arises from discrepancies between an individual’s moral belief system, self-concept, actions, and experiences when exposed to MIEs (11, 59, 72) can disrupt a person’s ability to align their personal sense of right and wrong with that of society (11, 40, 47, 54) and create “maladaptive moral intuitions” of oneself (p. 644) (54). As spirituality enables people to make meaning of events, helping military members “cognitive[ly] [reframe] events as implicitly spiritual experiences” (p. 78) (55) may minimize the risk of MI. In the course of recovery from MI, efforts can be made to help members gain greater self-understanding, self-acceptance, and self-worth through self-reflection (69).
Meaning-Making: What Once Was and Now Is
Exposure to MIEs can compromise an individual’s sense of identity, self-worth, and orienting systems, leaving one struggling to find meaning (11, 13, 47, 54, 58, 59, 61, 69, 71, 72). Feelings of unease, self-condemnation, and distress can quickly surface (47, 58, 67). Currier and colleagues found that exposure to more traumatic MIEs is negatively correlated with a person’s ability to make meaning of trauma (67), be that meaning made of the MIE, the impact of the MIE on meaning systems, or attributions of the MIE (11, 47, 53, 55, 59–61, 65, 67, 58, 73). From a syndrome perspective of MI (53), perceived loss of life meaning has been identified as a core symptom within the spiritual conflict domain (61). Deriving meaning from an MIE has enabled veterans to alleviate stress, restore meaning, realign previously established moral frameworks, and influence the likelihood of developing MI (53, 55, 59). Consideration of the MIE and the meaning a member attributes to it is essential when seeking resolution for MI (11), something that Kopacz and colleagues (60) suggest pastoral care can help military personnel with.
Spirituality as a Facilitator of Treatment for Moral Injury
The literature outlines treatment strategies required for the prevention and resolution of MI (1, 11, 74, 75). Specific spiritual interventions may be key to alleviating symptoms, reestablishing a stable framework of beliefs, values, and moral code (11, 54), and reestablishing relationships with self, others, the world, and the sacred or Transcendent. This may involve education, modified exposure, self-forgiveness, dialogue with a benevolent moral authority, reparation and forgiveness, (re)connection and (re)engagement with an S/R community, and integration throughout life (1, 11, 74, 76). Spirituality, which is identified as a treatment modality for MI (p. 704) (77), may enhance recovery and healing (11, 40, 46, 54, 55, 58–60, 63, 64, 68, 72, 73, 78).
S/R practices can be incorporated throughout the course of military service. During deployment and prior to returning home, S/R practices and rituals/ceremonies aimed at cleansing, purification, healing, and restoration of relationships with self, others, and the gods/Transcendent have been noted to foster cohesion among military members (55) and facilitate healing and transition to postservice activities. S/R principles and practices—specifically confession and forgiveness from a higher power—are noted to support self-forgiveness (63), which has been identified as a critical component of recovery from MI (11, 63). Further, Drescher et al. (29) highlighted numerous specific S/R intervention strategies: i) forgiveness to facilitate repair of relationships; ii) review of S/R beliefs and engagement in S/R practices that temper anger, rage, and a desire for revenge; iii) prayer and meditation to reduce stress; and iv) (re)connections with S/R communities to reduce isolation, establish social supports, encourage a healthy lifestyle, and facilitate recovery. The following S/R practices can also be incorporated into general interventions (17): i) self-regulation (e.g., through prayer, meditation, yoga, mindfulness, and breathing), ii) self-concept (i.e., enhancing self-awareness through journaling, alignment with a benevolent moral authority), iii) concept of the world (e.g., contributing to making the world a better place through acts of community services, e.g., working at a food bank, soup kitchen, or house-building initiatives), iv) moral emotions (e.g., virtuous living, cultivating a grateful attitude, acceptance, joy), and v) social connection.
Integration of S/R perspectives into general strategies used to treat PTSD and MI is also noted in the literature. This includes the use of spiritual dialogue (77), imagination, and spiritually oriented/integrated cognitive processing therapy (68). Specific spiritually integrated mindfulness, theological reflexivity, and compassion training could be employed to promote recovery and strengthen spiritual fitness and resilience (54, 55). Spiritual-strengthening and meaning-making groups are also suggested (58), as are arts and literature groups to explore S/R and moral dimensions of MIEs (66). Several articles highlighted the importance of chaplains, and pastoral and spiritual care services as a resource for addressing MI (46, 58, 59, 79).
Faith Communities: Possible Sources of Fragmentation or Healing
S/R communities can be invaluable resources for military personnel and veterans recovering from MI. Faith-based communities can provide a place and space for members to connect; engage; practice patience, kindness, and forgiveness; spiritually integrate; and reconstruct meaning and purpose (11, 13, 18, 54, 61–65, 40, 68, 73). Conversely, some individuals may experience difficulty engaging in S/R communities due to feelings of guilt, shame, and perceived or real judgment. This can regrettably exacerbate MI symptoms (61, 67). Ideally, however, community can surround military members and veterans struggling with MI so that they can find healing and a renewed sense of meaning and growth.
Discussion
This mini-review, which aimed to explore the relationship between spirituality and MI, identified a cyclical relationship between MI and spirituality such that S/R was found to serve as both a risk factor for and a protective factor against MI; it can also be directly influenced by MIEs. As a result, consideration of S/R factors, in addition to biopsychosocial elements, is essential when trying to better understand, prevent, and treat MI experienced by military members and veterans.
This review emphasizes the importance of utilizing a holistic biopsychosocial–spiritual approach that leverages S/R resources for the benefit of those who experience S/R struggles such as MI (80) (e.g., the Canadian Model of Occupational Performance and Engagement) (81). Biopsychosocial models more widely used in modern healthcare (46) may be better able to meet the existential and spiritual needs of military members by integrating S/R resources, practices, and tools. This is becoming all the more important as military service becomes increasingly complex and members are impacted at the deepest level of their being (17) and spirit (18) by MIEs not only in the course of missions and disaster relief efforts, but also due to stateside and/or training accidents, drone warfare, and military sexual trauma.
There is growing support for the use of spirituality as both a treatment component of MI and way of addressing the varying values, beliefs, and spiritual needs of military personnel and veterans (11, 40, 46, 54, 55, 57, 59, 60, 63, 64, 72, 76, 79). Helping military personnel and veterans maintain a stable meaning system, ascribe spiritual meaning to MIEs, and access opportunities to discuss moral dilemmas may reduce the risk of developing MI (11, 43, 47, 53, 55, 59–61, 76, 79). This may be facilitated through supportive, nonjudgmental groups and faith communities and engagement in S/R practices and rituals prior to, during, and following military service.
While some evidence exists regarding the relationship between spirituality and MI, further research is yet needed regarding the following: i) how specific S/R orienting systems, interventions, practices, and rituals/ceremonies might protect against and treat MI; ii) features of individuals who do/do not experience MI; iii) S/R assessment tools and interventions, and key time points for their administration; and iv) ways to maximize the positive contributions of faith communities. More robust evidence is also needed to enable the confident use of S/R interventions as it applies to MI in relation to the self, identity, meaning making, S/R struggles, growth, and resilience. Finally, while research has been conducted regarding the way in which S/R may be supportive of members and veterans struggling with MI, further research into supports that social/cultural environments may be able to offer is also warranted.
Limitations
The scope of the review was restricted to a limited number of indexed peer-reviewed studies that focused on the S/R dimension of MI and were found in the five databases searched. While the search strategy reduced the risk of publication bias, some studies and salient work may have been overlooked. The findings are not generalizable to other groups experiencing MI beyond military personnel and veterans. Further, the subjective nature of concepts presented raises the possibility that personal bias informed thematic findings. To help offset this, the review was conducted by two blind reviewers, reflexivity occurred throughout the research process, and concepts were linked to concrete definitions.
Conclusion
Spirituality underlies many of the experiences of MI, including changes in identity, meaning making, social supports, and MI symptoms. The findings of this mini-review highlight the need to consider a person’s spiritual fitness and health throughout military service and during treatment of MI and examine how spirituality can be fostered to help build resilience and reduce the risk of MI (17). While acknowledging the limited quality of evidence, encouraging military members and veterans to draw on S/R resources and practices may be a salve to psychospiritual distress. Integration of spirituality as a bona fide modality seems timely. Although much of the literature agreed that spirituality is important for the treatment of MI, more research is needed to understand how to effectively incorporate it into treatment to facilitate healing of MI among military members and veterans.
Author Contributions
FS and SB-P collected the materials and resources needed for this review. SB-P, FS, and AP analyzed the data. FS and SB-P wrote this article, AP and TC provided subject matter expertise and reviewed and revised each draft of the manuscript.
Funding
This work was supported by Veterans Affairs Canada, contract number OX170116741401P, and the Royal Canadian Chaplain Service, Department of National Defence. The funding sources had no involvement in the planning, conduction, or evaluation of this study.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to acknowledge all military members, veterans, and their families who give of themselves in service to their country. We would also like to acknowledge those committed to helping members and veterans recover and continue to grow and thrive.
References
1. Nash WP, Litz BT. Moral Injury: a mechanism for war-related psychological trauma in military family members. Clin Child Fam Psychol Rev (2013) 16(4):365–75. doi: 10.1007/s10567-013-0146-y
2. Thompson MM, Gignac M. The experience of Canadian Forces augmentees. In: The human in command: peace support operations. Amsterdam, NL: Mets en Schilt (2002). p. 235–63.
3. Thomson MH, Adams BD, Sartori JA. Moral and ethical decision making in Canadian Forces Operations (No. 7703-13). In: Moral and ethical decision making in Canadian Forces Operations. Toronto: Defence R&D Canada (2006).
4. Thomson MH, Adams BD, Tario CD, Brown AL, Thompson M. Collaborative team decision-making in a realistic CF training scenario. Draft Report, Toronto: Defence R&D Canada (2008).
5. Grossman D. On killing: the psychological cost of learning to kill in war and society. Boston: Little, Brown (1996).
6. Kilner PG. The military ethicist’s role in preventing and treating combat- related, perpetration-induced psychological trauma. Draft report, Joint Services Conference on Professional Ethics. Virginia: Springfield (2005). Available at: http://isme.tamu.edu/JSCOPE05/Kilner05.html
7. Kilner P. Military leaders’ obligation to justify killing in war. Mil Rev (2002) 82(2):24. Available at: http://cgsc.contentdm.oclc.org/cdm/singleitem/collection/p124201coll1/id/232/rec/4
8. Kulka RA, Schlenger WE, Fairbank JA, Hough RL, Jordan BK, Marmar CR, et al. Trauma and the Vietnam war generation: report of findings from the National Vietnam Veterans Readjustment Study. Philadelphia, PA: Brunner/Mazel (1990).
9. Maguen S, Lucenko BA, Reger MA, Gahm GA, Litz BT, Seal KH, et al. The impact of reported direct and indirect killing on mental health symptoms in Iraq war veterans. J Trauma Stress (2010) 23(1):86–90. doi: 10.1002/jts.20434
10. Bryan CJ, Bryan AO, Anestis MD, Anestis JC, Green BA, Etienne N, et al. Measuring moral injury: psychometric properties of the Moral Injury Events Scale in two military samples. Assessment (2016) 23(5):557–70. doi: 10.1177/1073191115590855
11. Litz BT, Stein N, Delaney E, Lebowitz L, Nash WP, Silva C, et al. Moral injury and moral repair in war veterans: a preliminary model and intervention strategy. Clin Psychol Rev (2009) 29:695–706. doi: 10.1016/j.cpr.2009.07.003
12. Callaway KL, Spates RC. Moral injury in military members and veterans. In: Oxford Handbooks Online. Online: Oxford University Press (2016). doi: 10.1093/oxfordhb/9780199935291.013.69
13. Drescher K, Foy DW. When they come home: posttraumatic stress, moral injury, and spiritual consequences for veterans. Reflective Pract (2008) 28:85–102. Available from http://journals.sfu.ca/rpfs/index.php/rpfs/article/view/158/157
14. Park J. A profile of the Canadian Forces. Perspect Labour Income (2008) 9(7):17–30. Catalogue: 75-001-X200810713214.
15. Pargament KI, Sweeney PJ. Building spiritual fitness in the Army: an innovative approach to a vital aspect of human development. Am Psychol (2011) 66(1):58–64. doi: 10.1037/a0021657
16. Frankfurt S. Frazier P. A review of research on moral injury in combat veterans. Mil Psychol (2016) 28(5):318–30. doi: 10.1037/mil0000132
18. Kinghorn W. Combat trauma and moral fragmentation: a theological account of moral injury. J Soc Christ Ethics (2012) 2:57. doi: 10.1353/sce.2012.0041
20. Stauner N, Exline JJ, Pargament KI. Religious and spiritual struggles as concerns for health and well-being. HORIZONTE-Revista de Estudos de Teologia e Ciências da Religião (2016) 14(41):48–75. doi: 10.5752/P.2175-5841.2016v14n41p48
21. Exline JJ, Pargament KI, Grubbs JB, Yali AM. The Religious and spiritual struggles scale: development and initial validation. Psycholog Relig Spiritual (2014) 6(3):208. doi: 10.1037/a0036465
22. Pargament KI, Magyar-Russell GM, Murray-Swank NA. The sacred and the search for significance: religion as a unique process. J Soc Iss (2005) 61(4):665–87. doi: 10.1111/j.1540-4560.2005.00426.x
23. Mahoney PK. Spirituality: discovering and conserving the sacred. In: Snyder CR, Shane JL, editors. Handbook of Positive Psychology. Oxford (England): Oxford University Press (2002). p. 646–59.
24. Trevino KM, Pargament KI, Cotton S, Leonard AC, Hahn J, Caprini-Faigin CA, et al. Religious coping and physiological, psychological, social, and spiritual outcomes in patients with HIV/AIDS: cross-sectional and longitudinal findings. AIDS Behav (2010) 14(2):379–89. doi: 10.1007/s10461-007-9332-6
25. Exline JJ, Rose E. Religious and spiritual struggles. In: Handbook of the psychology of religion and spirituality., vol. 2. New York, NY: Guilford Press (2005). p. 380–98.
26. Pargament KI, Murray-Swank NA, Magyar GM, Ano GG. Spiritual struggle: a phenomenon of interest to psychology and religion. In: Judeo-Christian perspectives on psychology: human nature, motivation, and change. Washington DC: American Psychological Association (2005). p. 245–68. doi: 10.1037/10859-013
27. Wilt JA, Grubbs JB, Pargament KI, Exline JJ. Religious and spiritual struggles, past and present: relations to the big five and well-being. Int J Psychol Relig (2017) 27(1):51–64. doi: 10.1080/10508619.2016.1183251
28. Abu-Raiya H, Pargament KI, Krause N. Religion as problem, religion as solution: religious buffers of the links between religious/spiritual struggles and well-being/mental health. Qual Life Res (2016) 25(5):1265–74. doi: 10.1007/s11136-015-1163-8
29. Drescher KD, Smith MW, Foy DW. Spirituality and readjustment following war-zone experiences. In Routledge psychosocial stress series. Combat stress injury: Theory, research, and management. New York, NY: Routledge/Taylor & Francis Group (2007). p. 295–310.
30. Calhoun LG, Tedeschi RG. The foundations of posttraumatic growth: an expanded framework. In: Handbook of posttraumatic growth. New York, NY: Psychology Press (2014). p. 17–37. doi: 10.4324/9781315805597
31. Pargament KI, Wong S, Exline JJ. Wholeness and holiness: the spiritual dimension of eudaimonics. In: Vittersø J. Handbook of eudaimonic well-being, international handbooks of quality-of-life. Switzerland: Springer International Publishing (2016). p. 379–94. doi: 10.1007/978-3-319-42445-3_25
32. Pargament KI, Trevino K. Spiritual struggles as a fork in the road to healthy living. Hum Dev (2006) 27:5–13.
33. Pargament KI, Mahoney A. Sacred matters: sanctifications as a vital topic for the psychology of religion. Int J Psychol Relig (2005) 15(3):179–98. doi: 10.1207/s15327582ijpr1503_1
34. Bryant AN, Astin HS. The correlates of spiritual struggle during the college years. J Higher Educ (2008) 79(1):1–27. doi: 10.1353/jhe.2008.0000
35. Fontana A RR. The role of loss of meaning in the pursuit of treatment for posttraumatic stress disorder. J Trauma Stress (2005) 18(2):133–6. doi: 10.1002/jts.20014
36. Grubbs JB, Wilt J, Stauner N, Exline JJ, Pargament KI. Self, struggle, and soul: linking personality, self-concept, and religious/spiritual struggle. Pers Individ Dif (2016) 1(101):144–52. doi: 10.1016/j.paid.2016.05.365
37. Pargament KI, Desai KM, McConnell KM. Spirituality: a pathway to posttraumatic growth or decline? In: Calhoun LG, Tedeschi RG, editors Handbook of posttraumatic growth. Lawrence Erlbaum (2006). p. 121–37.
38. Pargament KI, Ano GG. Spiritual resources and struggles in coping with medical illness. South Med J (2006) 99(10):1161–2. doi: 10.1097/01.smj.0000242847.40214.b6
39. Rosner R, Powell S. Posttraumatic growth after war. In: Handbook of posttraumatic growth: research and practice. Mahwah, NJ: Lawrence Erlbaum Associates Publishers (2006). p. 197–213.
40. Purcell N, Maguen S, Koenig CJ. Veterans’ perspectives on the psychosocial impact of killing in war. Couns Psychol (2016) 44(7):1062–99. doi: 10.1177/0011000016666156
41. Lepore SJ, Revenson TA. Resilience and posttraumatic growth: recovery, resistance, and reconfiguration. In: Handbook of posttraumatic growth: research & practice. Mahwah, NJ: Lawrence Erlbaum Associates Publishers (2006). p. 197–213.
42. Pargament KI. Spiritually integrated psychotherapy: understanding and addressing the sacred. New York, NY: Guilford Press (2007).
43. Currier JM, Drescher KD, Holland JM, Lisman R, Foy DW. Spirituality, forgiveness, and quality of life: testing a mediational model with military veterans with PTSD. Int J Psychol Relig (2016) 26(2):167–79. doi: 10.1080/10508619.2015.1019793
45. Park CL. Religion and meaning. Handbook of the psychology of religion and spirituality. Guildford Press (2013). p. 357–79.
46. Carey LB, Hodgson TJ, Krikheli L, Soh RY, Armour A, Singh TK, et al. Moral injury, spiritual care and the role of chaplains: an exploratory scoping review of literature and resources. J Relig Health (2016) 55(4):1218–45. doi: 10.1007/s10943-016-0231-x
47. Haight W, Sugrue E, Calhoun M, Black J. A scoping study of moral injury: identifying directions for social work research. Child Youth Serv Rev (2016) 70:190–200. doi: 10.1016/j.childyouth.2016.09.026
48. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med (2009) 6(7):e1000100. doi: 10.1371/journal.pmed.1000100
49. Campbell S. Filter to Retrieve Studies Related to Military Medicine from the Ovid MEDLINE Database. John W. Scott Health Sciences Library, University of Alberta. (2015). Available at http://guides.library.ualberta.ca/ld.php?content_id=14872980
50. Campbell S. Filter to Retrieve Studies Related to Faith and Religion from the OVID MEDLINE Database. John W. Scott Health Sciences Library, University of Alberta. (2015). Available from http://guides.library.ualberta.ca/ld.php?content_id=14026257
51. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol (2005) 8(1):19–32. doi: 10.1080/1364557032000119616
52. Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci (2010) 5:69–77. doi: 10.1186/1748-5908-5-69
53. Jinkerson JD. Defining and assessing moral injury: a syndrome perspective. Traumatology (2016) 22(2):122–30. doi: 10.1037/trm0000069
54. Doehring C. Resilience as the relational ability to spiritually integrate moral stress. Pastoral Psychol (2015) 64(5):635–49. doi: 10.1007/s11089-015-0643-7
55. Hufford DJ, Fritts MJ, Rhodes JE. Spiritual fitness. Mil Med (2010) 175(suppl 8):73–87. doi: 10.7205/MILMED-D-10-00075
56. Flipse Vargas A, Hanson T, Kraus D, Drescher K, Foy D. Moral injury themes in combat veterans’ narrative responses from the National Vietnam Veterans’ Readjustment Study. Traumatology (2013) 19(3):243–50. doi: 10.1177/1534765613476099
57. Drescher KD, Foy DW, Kelly C, Leshner A, Schutz K, Litz B. An exploration of the viability and usefulness of the construct of moral injury in war veterans. Traumatology (2011) 17(1):8–13. doi: 10.1177/1534765610395615
58. Malott JD. Morally injurious experiences, meaning, and spiritual functioning in Iraq and Afghanistan veterans. Fuller Theological Seminary, School of Psychology. Ann Arbor, MI: Proquest LLC (2015).
59. Rennick JB. Canadian values and military operations in the twenty-first century. Armed Forces Soc (2013) 39(3):511–30. doi: 10.1177/0095327X12441326
60. Kopacz MS, Connery AL, Bishop TM, Bryan CJ, Drescher KD, Currier JM, et al. Moral injury: a new challenge for complementary and alternative medicine. Complement Ther Med (2016) 24:29–33. doi: 10.1016/j.ctim.2015.11.003
61. Miller Brian P. Exploring moral injury in combat veterans: a qualitative study of four combat veteran interviews (thesis) (2016). https://www.researchgate.net/publication/295920131_Exploring_Moral_Injury_in_Combat_Veterans_A_Qualitative_Study_of_Four_Combat_Veteran_Interviews
62. Nazarov A, Jetly R, McNeely H, Kiang M, Lanius R, McKinnon MC. Role of morality in the experience of guilt and shame within the armed forces. Acta Psychiatr Scand (2015) 132(1):4–19. doi: 10.1111/acps.12406
63. Worthington EL, Langberg DM. Religious considerations and self-forgiveness in treating complex trauma and moral injury in present and former soldiers. J Psychol Theol (2012) 40(4):274–88. doi: 10.1177/009164711204000403
64. Pearce M, Haynes K, Rivera NR, Koenig HG. Spiritually integrated cognitive processing therapy: a new treatment for post-traumatic stress disorder that targets moral injury. Glob Adv Health Med (2018) 7:2164956118759939. doi: 10.1177/2164956118759939
65. Evans WR, Stanley MA, Barrera TL, Exline JJ, Pargament KI, Teng EJ. Morally injurious events and psychological distress among veterans: examining the mediating role of religious and spiritual struggles. Psychol Trauma (2019) 10(30):360–67. doi: 10.1037/tra0000347
66. Kopacz MS, Simons KV, Chitaphong K. Moral injury: an emerging clinical construct with implications for social work education. J Relig Spiritual Soc Work (2015) 34(3):252–64. doi: 10.1080/15426432.2015.1045681
67. Currier JM, Holland JM, Malott J. Moral injury, meaning making, and mental health in returning veterans. J Clin Psychol (2015) 71(3):229–40. doi: 10.1002/jclp.22134
68. Koenig HG, Boucher NA, Oliver RJP, Youssef N, Mooney SR, Currier JM, et al. Rationale for spiritually oriented cognitive processing therapy for moral injury in active duty military and veterans with posttraumatic stress disorder. J Nerv Ment Dis (2017) 205(2):147–53. doi: 10.1097/NMD.0000000000000554
69. Worthington EL Jr., Langberg D. Religious considerations and self-forgiveness in treating complex trauma and moral injury in present and former soldiers. J Psychol Theol (2012) 40(4):274–88. doi: 10.1177/009164711204000403
70. Government of Canada. Canadian Forces Joint Publication (CFJP) 1.0—Military Personnel Management Doctrine (2008). Canada: Department of National Defence. Available at http://publications.gc.ca/collections/collection_2010/forces/D2-252-100-2008-eng.pdf. doi: B-GL-005-100/FP-001
71. Yan GW. The invisible wound: moral injury and its impact on the health of Operation Enduring Freedom/Operation Iraqi Freedom veterans. Mil Med (2016) 181(5):451–8. doi: 10.7205/MILMED-D-15-00103
72. Blinka D, Wilson Harris H. Moral injury in warriors and veterans: the challenge to social work. Social Work Christ (2016) 43(3):7–27. Available at: https://www.researchgate.net/publication/307601841_Moral_Injury_in_Warriors_and_Veterans_The_Challenge_to_Social_Work
73. Kopacz MS, O’Reilly LM, Van Inwagen CC, Bleck-Doran TL, Smith WD, Cornell N. Understanding the role of chaplains in veteran suicide prevention efforts: a discussion paper. Online Access: Sage Open (2014) 4(4):2158244014553589. doi: 10.1177/2158244014553589
74. Litz BT, Lebowitz L, Gray MJ, Nash WP. Adaptive disclosure: a new treatment for military trauma, loss, and moral injury. New York, NY: Guilford Publications (2017).
76. Keenan MJ, Lumley VA, Schneider RB. A group therapy approach to treating combat posttraumatic stress disorder: interpersonal reconnection through letter writing. Psychotherapy (2014) 51(4):546. doi: 10.1037/a0036025
77. Nash WP, Silva C, Litz B. The historic origins of military and veteran mental health stigma and the stress injury model as a means to reduce it. Psychiatr Ann (2009) 39(8):789. doi: 10.3928/00485713-20090728-05
78. Kent DD, David WF, Caroline K, Anna L, Kerrie S, Brett L. An exploration of the viability and usefulness of the construct of moral injury in war veterans. Traumatology (2011) 1:8. doi: 10.1177/1534765610395615
79. Kopacz MS, McCarten JM, Pollitt MJ. VHA chaplaincy contact with veterans at increased risk of suicide. South Med J (2014) 107(10):661–4. doi: 10.14423/SMJ.0000000000000182
80. Sulmasy DP. A biopsychosocial-spiritual model for the care of patients at the end of life. Gerontologist (2002) 42(suppl 3):24–33. doi: 10.1093/geront/42.suppl_3.24
81. Polatajko HJ, Townsend EA, Craik J. Canadian model of occupational performance and engagement (CMOP-E). In: Enabling occupation II: advancing an occupational therapy vision of health, well-being, & justice through occupation. CAOT Publications ACE (2007). p. 22–36.
Keywords: moral injury, military, veterans, spirituality, self, identity, biopsychosocial–spiritual approach
Citation: Brémault-Phillips S, Pike A, Scarcella F and Cherwick T (2019) Spirituality and Moral Injury Among Military Personnel: A Mini-Review. Front. Psychiatry 10:276. doi: 10.3389/fpsyt.2019.00276
Received: 02 September 2018; Accepted: 10 April 2019;
Published: 29 April 2019.
Edited by:
Harold G. Koenig, Duke University Medical Center, United StatesReviewed by:
Nathan Boucher, Duke University, United StatesMichelle Pearce, University of Maryland, United States
Copyright © 2019 Brémault-Phillips, Pike, Scarcella and Cherwick. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suzette Brémault-Phillips, c3V6ZXR0ZS5icmVtYXVsdC1waGlsbGlwc0B1YWxiZXJ0YS5jYQ==