 Lia Gentil
Lia Gentil Guy Grenier2
Guy Grenier2 Henri Dorvil
Henri Dorvil Marie-Josée Fleury
Marie-Josée Fleury- 1Department of Psychiatry, McGill University, Montreal, QC, Canada
- 2Research Center, Douglas Mental Health University Institute, Montreal, QC, Canada
- 3School of Social Work, Université du Québec à Montréal, Montreal, QC, Canada
Quality of life (QOL) is a key indicator in mental health planning, program evaluation, and evaluation of patient outcomes. Yet few studies have focused on QOL in homeless populations. More specifically, research has yet to identify profiles of homeless individuals based on their QOL using cluster analysis. This study developed a typology of QOL for a sample of 455 homeless individuals recruited from 27 community and public organizations in Quebec (Canada). The typology was developed based on QOL scores, as well as sociodemographic, clinical, and service use variables. Study participants had to be at least 18 years old, with current or previous experience of homelessness. A questionnaire including socio-demographics, residential history, service utilization, and health-related variables was administered. Four clusters were identified using a two-step cluster analysis. QOL was highest in the cluster consisting of older women with low functional disability, and relatively few episodes of homelessness. The second cluster with high QOL scores included individuals living in temporary housing with relatively few mental health or substance use disorders (SUDs). The third cluster with low QOL included middle-aged women living in temporary housing, with criminal records, personality disorders, and SUDs. QOL was also lower in the fourth cluster composed of individuals with multiple homeless episodes and complex health problems as well as high overall service use. Findings reinforced the importance of disseminating specific programs adapted to the diverse profiles of homeless individuals, with a view toward increasing their QOL.
Introduction
Quality of life (QOL) is one of the most important indicators in mental health planning, program evaluation, and assessment of patient outcomes (1). QOL is a heterogeneous concept that encompasses many areas of objective and subjective well-being (2). Objective QOL includes aspects of the physical environment and social functioning (2), whereas subjective QOL (SQOL) relates more to individual preferences, opinions, and life satisfaction (3). Research on QOL has been conducted with patients affected by mental health disorders (MHDs) (4–7); while studies on QOL and homelessness have focused on veterans (8–10), newly housed individuals who were previously homeless (11, 12), or homeless individuals with MHDs or substance use disorders (SUDs) (13, 14). However, few studies have focused on QOL in homeless populations.
QOL in homelessness may be linked to multiple variables including sociodemographic characteristics, clinical, and health care service use variables. Some studies have reported higher QOL among older homeless women (12, 13, 15); whereas having a criminal record has been found to negatively affect QOL (16). Compared with individuals who have experienced multiple episodes of homelessness, those experiencing a first homeless episode had higher QOL (12). Fewer days of homelessness were also associated with higher QOL (17). Individuals living in permanent supported housing such as Housing First (HF) programs, which integrate financial subsidies, case management, and a harm reduction philosophy tailored to individual needs, had higher levels of QOL compared with control groups consisting of emergency shelter users, or those residing in temporary housing or various forms of independent housing viewed as inadequate (18–20). In terms of clinical variables, homeless individuals with common MHDs (e.g., depression), serious MHDs (e.g., psychosis), SUDs, and personality disorders reported low QOL scores (13, 17, 21), similar to results for homeless individuals with high functional disabilities (22). While suicidal behaviors associated with MHDs and SUDs (23–25), and physical illnesses were also found to be prevalent in homeless populations (e.g., diabetes, cardiovascular disease) (26, 27), research has yet to investigate possible associations between these conditions and QOL. Regarding service use, one study found that being enrolled in outpatient services produced improved QOL scores in a homeless sample (28), while another identified improved QOL after enrolment in medical, employment or public support programs (17, 19). While homeless individuals with MHDs, SUDs or physical illnesses have tended to be high emergency room (ER) users, defined as four or more ER visits in a single year (29, 30) no study has identified associations between high ER use and QOL.
Cluster analysis is a useful method for establishing typologies (31), and may be used to investigate QOL among individuals experiencing homelessness. General profiles have been developed using cluster analysis among homeless individuals with both common and serious MHDs (32–34), co-occurring MHDs/SUDs (35), or physical illnesses (36), as well as among patients with serious MHDs using psychiatric services (33) and those using shelters over a multiple-year period (37–41). However, no known study has used cluster analysis to identify profiles of homeless individuals based on their QOL. Moreover, few cluster analyses in homelessness have taken into account the possible effects of sociodemographic characteristics such as criminal record, episodes of homelessness, and different types of accommodation on QOL. As well, clinical variables such as suicidal ideation or functional disability, and overall service use have hardly been considered in typologies of homelessness. The availability of a QOL typology based on sociodemographic, clinical, and service use variables for homeless populations would provide critical information and a deeper understanding that could inform the development of housing policies and services that capture the unique characteristics and needs of each group. Accordingly, the objective of this study was to build a typology based on QOL, sociodemographic and clinical variables, and service use for a sample of 455 homeless individuals in Quebec who were living in different types of accommodation.
Materials and Methods
Study Setting and Data Collection
The study was conducted in the two major urban areas of Quebec: Montreal and Quebec City. Montreal had the largest homeless population (N = 3,016), as well as 2,017 available beds (71% of the provincial total) in emergency shelters and transitional housing, while Quebec City had 262 beds (15%) (42). Recruitment was conducted in 27 public organizations, mainly community organizations (22 from Montreal and five from Quebec City). Twenty of these organizations offered housing resources; five with emergency shelters (29 beds per organization, on average); 12 with temporary housing resources (average 20 beds per organization), and three with permanent supported housing (total: 173 beds). The seven organizations without a housing component provided other essential services including food banks, day centers, leisure activities; employment or housing services, and financial or material support.
Eligibility requirements for participation in the study included current or previous experience of homelessness and age requirements (18 or older). No interested participant was excluded from the study, if eligible; but interviews sometimes had to be delayed for participants who were intoxicated or otherwise indisposed at recruitment time. Posters were displayed in common areas of the selected organizations. The project coordinator also recruited participants directly while present in sites where homeless people congregate, such as nearby cafés. Finally, researchers held information meetings with housing staff and enlisted their help with recruitment. There were four housing conditions: emergency shelters (overnight accommodation), temporary housing (3–12 month residency), and permanent housing (1 year to indefinite stay), either with financial and case manager support (Housing First), or without this support. Homeless individuals invited to participate in the study included 46 users of emergency shelters, 243 residents in temporary housing, 156 residents in permanent housing with support, and 52 permanent housing residents without support, for a total of 497 invited study participants.
Data were collected between January and September 2017 by trained interviewers. Interviews were conducted in the selected organizations, at participant apartments, or in quiet corners of local cafés or fast foods restaurants. Interviews usually took place on the same day, or day following initial contact, and averaged 90 min in duration. All study participants signed a consent form before undergoing an interview, and were told that their responses would remain confidential. The research ethics board of the Douglas Mental Health University Institute approved the multisite study protocol.
Variables and Instruments
The questionnaire included socio-demographic information, as well as questions on residential history, service utilization, and clinical variables. The dependent variable, QOL, was measured using the Satisfaction with Life Domains Scale (SLDS), a frequently used instrument for QOL assessments in various fields. The SLDS was published initially by Baker and Intagliata in 1982 (43), and a French translation developed and validated (Cronbach Alpha = 0.92) by Caron (44). The SLDS assesses 20 domains of life satisfaction. As well, five stylized faces were used to represent a range of emotional states, from the saddest face (score = 1), to the happiest face (score = 5). Study participants were directed to select the face that corresponded to their current emotional state (43).
Table 1 presents all variables included in the study and the instruments used. Variables were based on the literature, and included socio-demographics: age, sex, criminal record, homelessness episodes, and type of accommodation; clinical variables: MHDs, SUDs, number of physical illnesses, suicidal ideation, and functional disability; and service use variables: has a family physician and frequency of the following services: community services (e.g., soup kitchen, day center, employment support program, support group, women's center); public services (local community service center; addiction rehabilitation center, hospital or other); and emergency room (ER).
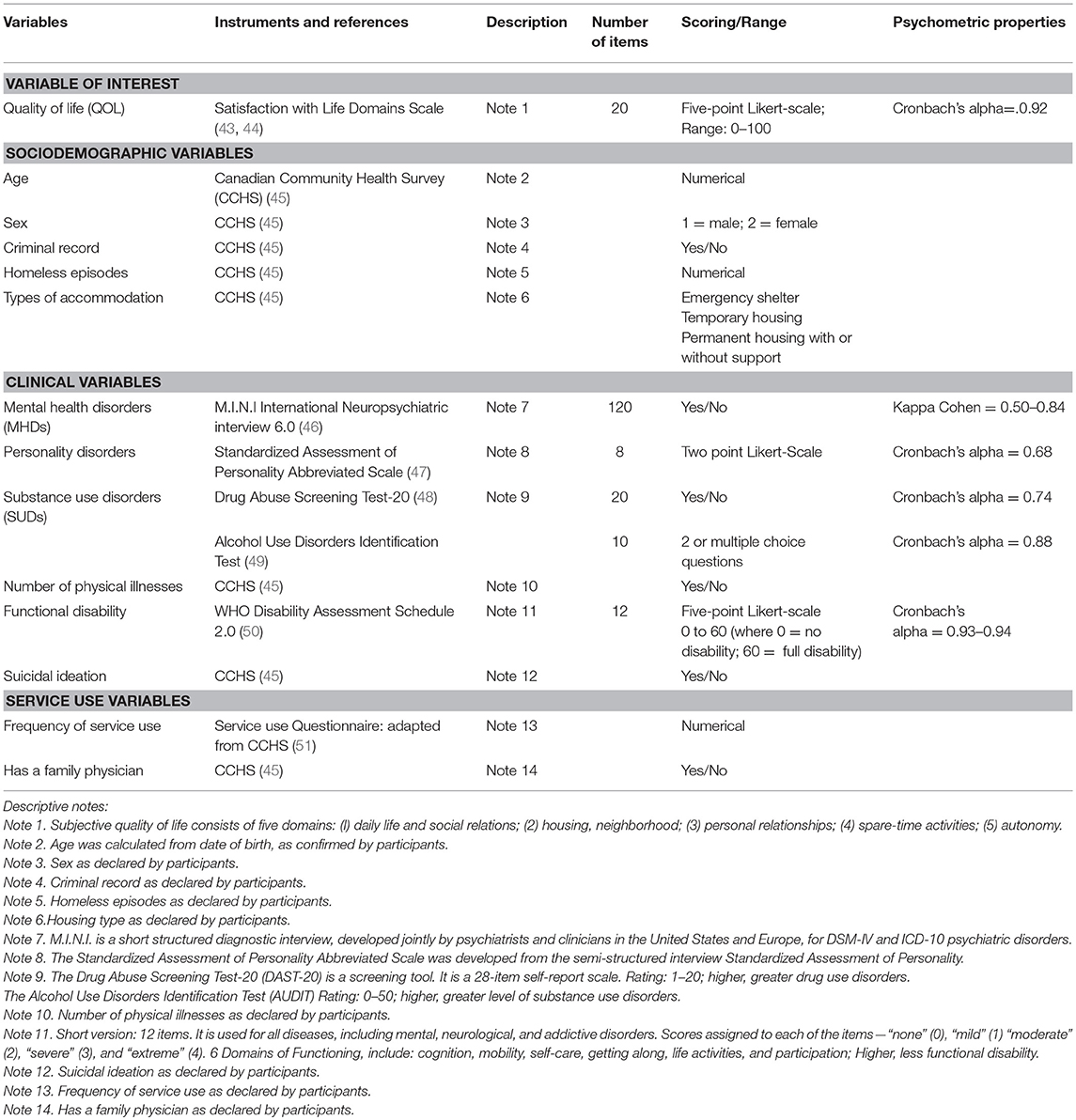
Table 1. Variables and instruments.
Analyses
After cleaning the database for missing values and outliers, univariate analyses comprised of frequency distributions for categorical variables, and mean values with standard deviations for continuous variables were carried out, followed by Cluster verification analyses. Missing values (<5%) were randomly distributed and treated using the Expectation Maximization method. Clustering of participants was computed with the SPSS Statistics 24.0 package Two Step Cluster Analysis. QOL was the variable of interest. The choice of variables was based on their relevance to the homeless population according to the literature. Variables were organized as continuous or categorical variables. Categorical variables were entered in the program first, followed by continuous variables. The Log-likelihood method was used to determine inter-subject distance. Participant clusters were identified using Schwartz Bayesian criteria, with the final number of clusters set at four, according to their overall contributions to inter-Cluster homogeneity. An analysis of variance was also performed to test whether differences among profiles were statistically significant on QOL scores, followed by post hoc tests using the Bonferroni correction. Comparison analyses were run to assess statistical differences between clusters for each variable, using the Chi-square test for categorical variables, and ANOVA t-test for continuous variables.
Results
The final sample consisted of 455 participants, of the 497 invited, for an overall response rate of 92%. Response rates for the four housing groups were: 94% (n = 229/243) for temporary housing; 90% (n = 140/156) for permanent housing with support; 79% (n = 41/52) for permanent housing without support; and 98% (n = 45/46) for homeless individuals using emergency shelters. Sample characteristics are presented in Table 2. Regarding sociodemographic variables, 60% of the sample were men, and 52% were 50 years of age, or older. Almost half had experienced a single homeless episode (46%), and 50% resided in temporary housing. In terms of clinical variables, 67% of participants reported personality disorders, 42% common MHDs (e.g., depression, anxiety), 39% SUDs, and 26% serious MHDs (e.g., schizophrenia, bipolar disorders). The mean for functional disability was 21, or moderate, on a 60-point scale. Concerning source of healthcare, 42% had a family physician. Participants had used community services an average of 72.5 times in the previous 12 months, public services 6.2 times, and the ER 1.9 times. Finally, the global mean score for QOL was 70.3/100.
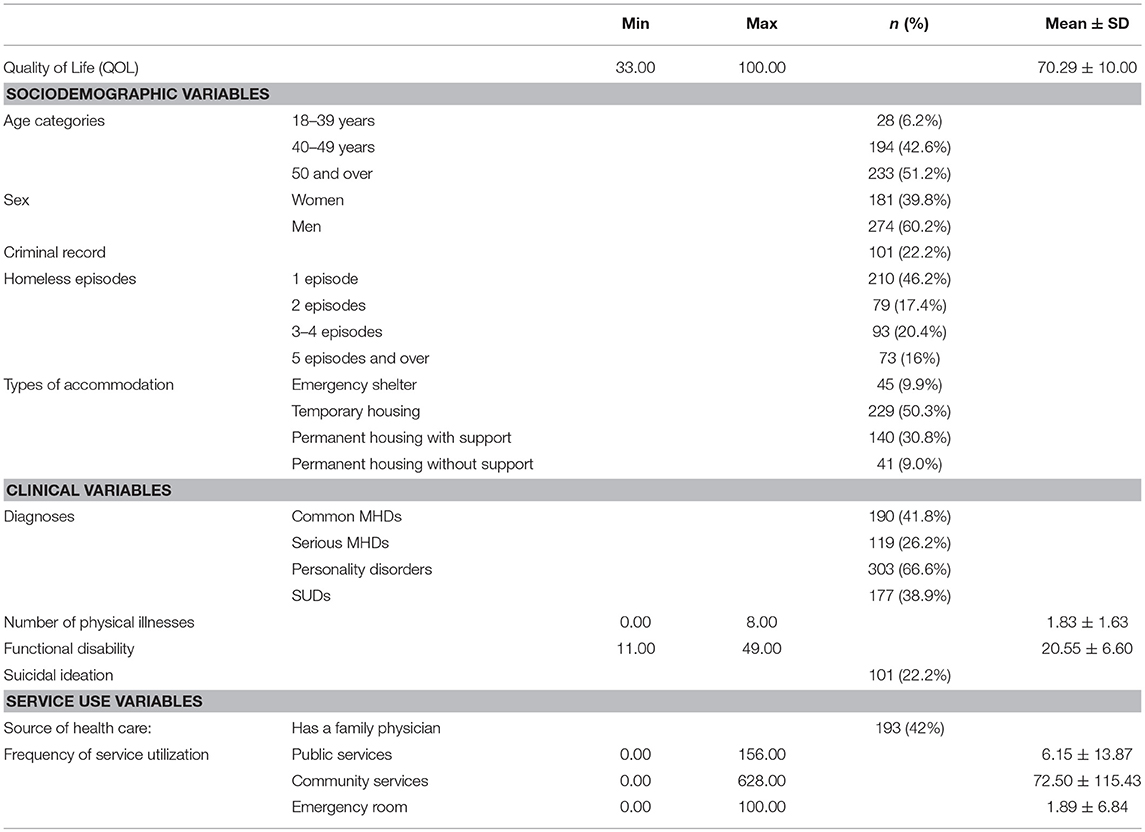
Table 2. Participant characteristics.
Table 3 presents the four clusters identified in the sample based on QOL. Cluster 1 was composed of 128 participants (28% of total sample) with a mean overall score for QOL of 75.8 (SD = 10.7), ranking first of the four clusters. Cluster 2 consisted of 120 individuals (26% of total sample), had the lowest overall mean QOL score (mean = 66.0; SD = 11.0). Cluster 3 included 142 individuals (31% of sample) ranked second on QOL (mean = 70.4, SD = 3.1). Finally, Cluster 4 presented 65 participants (14% of total sample), ranked third on QOL (mean = 67.1; SD = 11.4). Analysis of variance comparing QOL scores among the four clusters revealed significant differences: F(3, 454) = 26.54, p < 0.000. Post hoc tests using the Bonferroni correction revealed higher mean scores on QOL for Cluster 1 than for the other three Clusters (p < 0.000). Cluster 2 had lower scores than Cluster 3 (p < 0.001). Finally, the comparison between the mean scores for QOL for other Clusters (2 vs. 4, and 3 vs. 4) were non-significant (Tables 3, 4).
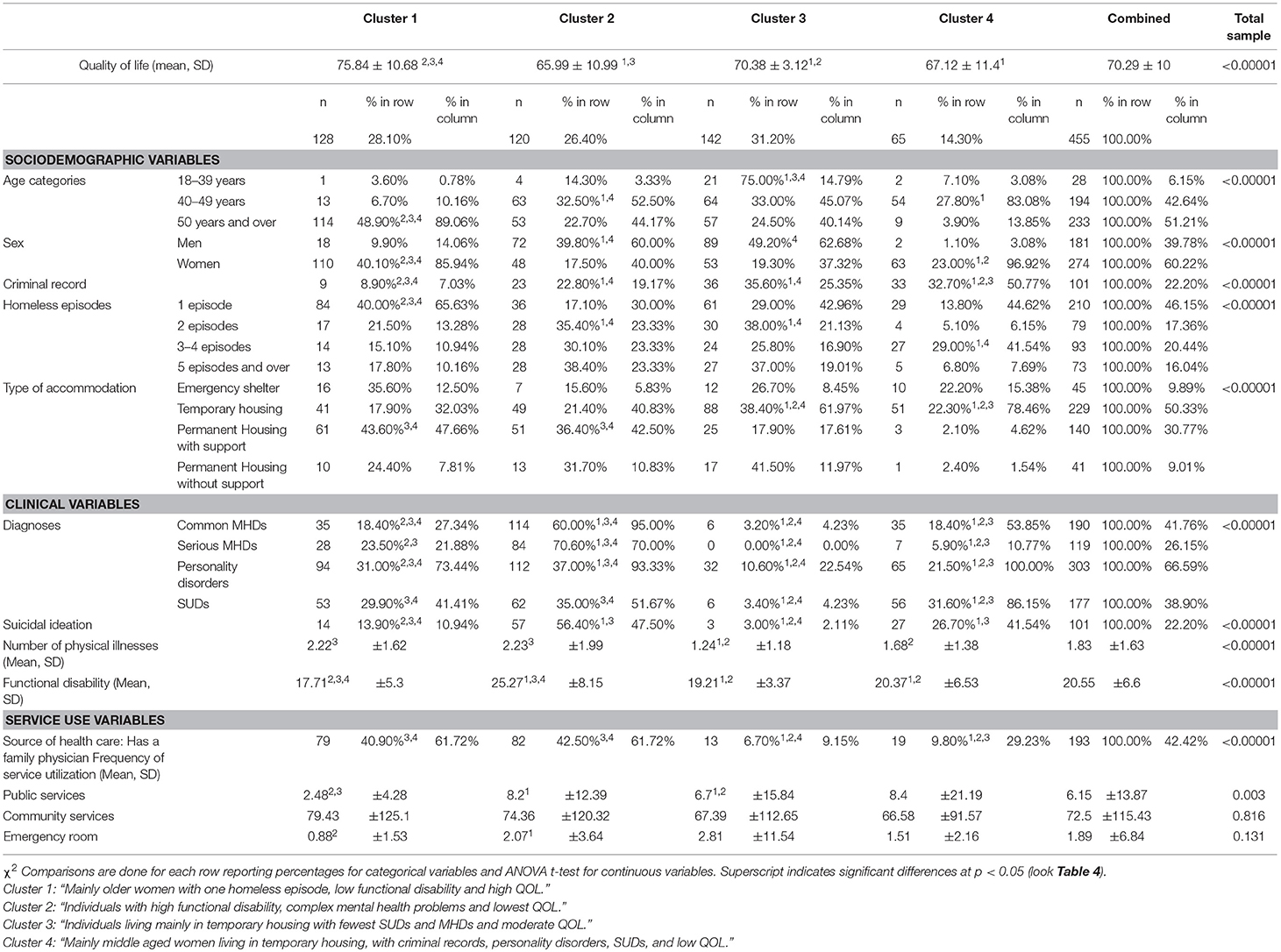
Table 3. Cluster analysis and comparison between clusters.
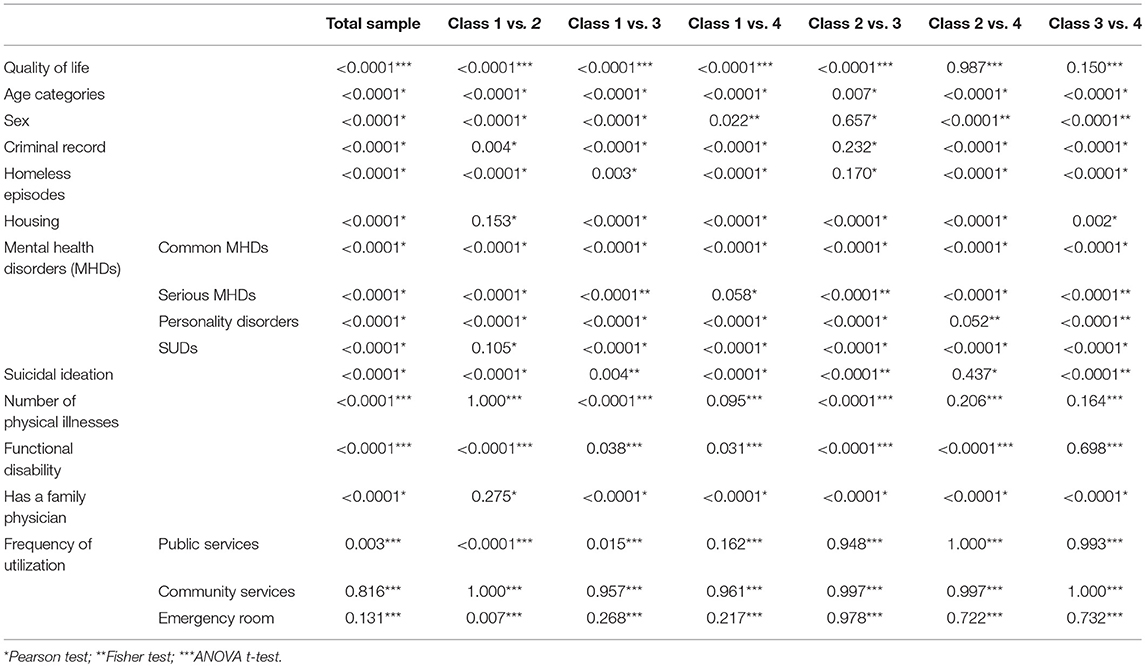
Table 4. Comparison tests between classes and variables.
Tests confirming the cluster analysis indicated that socio-demographic variables (age, sex, criminal record, homeless episodes, type of accommodation), clinical variables (suicidal ideation, number of physical illnesses, and functional disability), and frequency of services use (public services) differed significantly across clusters (Table 3). Cluster 1 included predominantly women 50 years old and over, who had experienced one episode of homelessness. Cluster 1 also had the lowest proportion of individuals with criminal records and the lowest functional disability scores. As compared with those in Clusters 3 and 4, more Cluster 1 participants resided in permanent housing with support; they reported a greater number of physical illnesses, but more often had a family physician. Compared with Clusters 2 and 3, Cluster 1 participants also made less use of public services. Finally, compared with Cluster 2, Cluster 1 participants reported lower ER use. Cluster 1 was labeled: “Mainly older women with one homeless episode, low functional disability and high QOL”
Cluster 2 had the highest proportions of individuals with MHDs (both common and serious MDs) and suicidal ideation, as well as higher functional disability scores than individuals in the other three clusters. As opposed to both Clusters 1 and 4, Cluster 2 had a higher proportion of individuals with two episodes of homeless, and more with five homeless episodes and over. Compared to Clusters 3 and 4, Cluster 2 also had a higher proportion of individuals with a family physician, and more residing in permanent housing with support. Finally, compared with Cluster 1, Cluster 2 individuals used public services with greater frequency. Cluster 2 was labeled: “Individuals with higher functional disability, complex mental health problems and lowest QOL.”
Cluster 3 mainly consisted of individuals residing in temporary housing who had the lowest proportion of SUDs, MHDs (both common and serious MDs), personality disorders, and suicidal ideation among the 4 clusters. As compared with Clusters 1, Cluster 3 had a higher proportion of individuals with a criminal record and with two homeless episodes. Individuals from Cluster 3 were also less affected by physical illnesses. Fewer had a family physician compared with individuals in Clusters 1 and 2. Cluster 3 was labeled: “Individuals living mainly in temporary housing with fewest SUDs and MHDs and moderate QOL.”
Finally, Cluster 4 had a higher proportion of women between 40 and 49 years of age, who had experienced one homeless episode. More had a criminal record, resided in temporary housing, and had personality disorders and SUDs as compared with individuals in the other three clusters. Cluster 4 was labeled: “Mainly middle aged women living in temporary housing, with criminal records, personality disorders, SUDs, and low QOL.”
Discussion
This study developed a typology for a sample of homeless individuals on the basis of QOL in relation to sociodemographic, clinical, and service use characteristics. Four clusters were identified, each with distinct features. Mean QOL scores varied from 66.0 to 75.8 (M = 70.3), which was lower than QOL scores for the general population in a Quebec epidemiological area, at 78 (52).
Our results showed marked differences among the four clusters in terms of sex, age, presence or absence of a criminal record, episodes of homelessness, and residence in temporary vs. permanent housing, number of physical illnesses, MHDs, or SUDs, as well as sources of health care and frequency of public service use in the previous year.
Cluster 1 differed from other clusters in terms of mean QOL, but also on sociodemographic and clinical characteristics. Cluster 1 mainly included older women who had experienced one episode of homelessness; they had the lowest scores on disability and criminal record as well the highest QOL. These results seem to confirm that high QOL among homeless individuals was associated with older age and female gender, as identified in previous research (53). Moreover, this cluster with the higher QOL also included those less affected by functional disability, which suggests that functional disability negatively influenced QOL (22).
Cluster 1 showed very marked differences from Cluster 2, which had the lowest QOL in relation to socio-demographics (sex, age, criminal record number of homeless episodes), and clinical variables (both common and serious MHDs, personality disorders, suicidal ideation, and functional disability) and on the frequency of public service use. Cluster 2 mainly consisted of individuals with a high prevalence of MHDs (common, serious, personality disorders), and functional disability. MHDs have been associated with lower QOL (14, 17). Previous studies also found that the presence of MHDs was associated with increased access to public health services; including primary care (54). The presence of multiple MHDs among homeless individuals also increases the risk of suicide (24). As well, functional disability, higher in Cluster 2, is a frequent result of both medical and psychiatric conditions, creating barriers to employment, and perpetuating the cycle of homelessness (55). A US study estimated that 37% of homeless individuals have a functional disability as compared with 25% of individuals living in poverty, and 15% of the general population (56). The fact that Cluster 2 individuals resided mainly in permanent supported housing, as in Cluster 1, seemed to indicate that QOL was not automatically associated with type of accommodation in homelessness. Similarly, QOL was not automatically associated with a regular source of health care, as the two clusters with higher (Cluster 1) vs. lower (Cluster 2) QOL reported similar proportions of individuals with a family physician.
Cluster 3 was second in terms of QOL, with moderate scores. Cluster 3 was mainly composed of individuals with few MHDs and SUDs who residing in temporary housing. The higher QOL than reported in Cluster 3 may have been due to the very low numbers of MHDs, SUDs, physical illnesses and suicidal ideation in this cluster. Individuals with MHDs or SUDs tend to report low QOL scores (13, 17, 21, 22). The low prevalence of MHDs and SUDs may also explain the low use of healthcare resources, such as family physicians and public services, in this cluster.
QOL scores for Clusters 3 and 4 showed no significant differences. These Clusters were similar in terms of the number of physical illnesses, levels of functional disability, and frequency of service utilization. However, major differences emerged on other variables between Clusters 3 and 4, the later consisting mainly of women greatly affected by personality disorders, SUDs, common and serious MHDs and suicidal ideation. The prevalence of common MHDs, and personality disorders was higher in women than men (57). Among women, MHDs, SUDs as well as violence are main causes of homeless (58). A systematic review of the literature on homeless women veterans also revealed that women were more likely to be affected by MHDs than men (59), and were more often involved in the justice system, in addition to having relatively higher rates of MHDs and SUDs (57).
Clusters 2 and 4 accounted for the lowest QOL scores, with no significant differences between them. These clusters were similarly and strongly characterized by high rates of personality disorders, SUDs, common MHDs, suicidal ideation, and high functional disability among their respective constituents. MHDs and SUDs have been identified in association with poor QOL, with a correspondingly high negative impact on family relationships and on employment status (17, 60, 61). Individuals in the two clusters also had similarly high rates of public services use, which suggests that frequency of service use was more related to clinical variables than socio-demographic variables or type of housing.
Finally, compared with Cluster 1, Cluster 4 consisted almost exclusively of middle aged women living in temporary housing, who had low QOL scores. As well, all Cluster 4 participants had a disproportionately high prevalence of personality disorders and SUDs, which is interesting as individuals with dual diagnoses are known to be high service users (62). Cluster 4 also had a disproportionate number of individuals with SUDs and criminal records. These results were similar to results of other studies underlining that SUDs increased vulnerability among homeless women, making them more prone to participate in drug-related crimes (63, 64).
Strengths and Limitations
This first study to profile QOL in a homeless sample included individuals living in different types of accommodation (emergency shelter, temporary housing, and permanent housing with and without support). In addition, the participation rate (92%) in this study was very high; only 42 of the 497 participants invited to the study refused to participate. Moreover, this study provided highly relevant insights into different aspects of homelessness and their associations with QOL, identifying sociodemographic, clinical, and service use characteristics affecting QOL in homelessness.
This study had also limitations that should be noted. The main limitation concerned the modest number of variables that could be introduced into the cluster analysis. Second, due to the convenience sampling, our results may not be generalizable. Third, our results emanating from data collected in Quebec may not be generalizable to other jurisdictions. Fourth, the study used cross-sectional and self-reported data. A longitudinal study could have better highlighted the causal relationships between QOL and the selected independent variables. Fifth, some housing groups, such as emergency shelters, were less represented than others in this study. Finally, while the sample was more evenly distributed in terms of sex, there were relatively fewer young people than those in older age categories.
Conclusion
The use of cluster analysis provides insight into the differences among homeless individuals in terms of QOL, taking into account sociodemographic, clinical, and service use variables. A better understanding of QOL in different homeless groups may help inform policy and service planning, while better responding to the need for client-focused healthcare that is sensitive to group differences. Our results suggest that older age may have a positive influence on QOL in women, while clinical characteristics, such as MHDs, SUDs, and high functional disability scores may influence QOL negatively, as the two clusters where individuals were more affected by complex mental health problems revealed the lowest QOL scores. Moreover, type of accommodation, having a family physician, and frequency of service utilization seemed not to have a direct impact on QOL. Temporary and permanent housing may both positively influence QOL but only among individuals without complex health problems.
Our findings reinforce the importance of disseminating specific programs adapted to the diverse profiles within homeless populations, with a view toward increasing their QOL. For Cluster 1, use of a family physician may be sufficient to meet the needs of that fairly functional clientele; whereas in Cluster 3, strategies such as the deployment of outreach workers may be needed to encourage service use. Programs that promote social integration may influence QOL in Cluster 4, as this group included a high proportion of women with criminal records and SUDs. Finally, assertive community treatment should be considered as an effective strategy for Cluster 2 individuals affected by both multiple MHDs and high functional disability.
Author Contributions
LG, GG, and M-JF: study design and analyses, interpretation of data, and preparation of manuscript. J-MB: data analysis. HD: revision of manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are grateful for the support of the Social Sciences and Humanities Research Council of Canada (SSHRC) (Grant number # 435-2016-0761), and thank the individuals who participated in the research, including the advisory committee, network respondents, and the research team. We are especially grateful to Daniela Perrottet and Judith Sabetti for their assistance.
References
1. Martin AJ, Stockler M. Quality-of-life assessment in health care research and practice. Eval Health Prof. (1998) 21:141–56. doi: 10.1177/016327879802100202
2. Awad AG, Voruganti LN. Measuring quality of life in patients with schizophrenia: an update. Pharmacoeconomics (2012) 30:183–95. doi: 10.2165/11594470-000000000-00000
3. Sirgy MJ, Michalos AC, Ferriss AL, Easterlin RA, Patrick D, Pavot W. The qualityity-of-life (QOL) research movement: past, present, and future. Soc Indic Res. (2006) 76:343–466. doi: 10.1007/s11205-005-2877-8
4. Fleury MJ, Grenier G, Bamvita JM, Tremblay J, Schmitz N, Caron J. Predictors of quality of life in a longitudinal study of users with severe mental disorders. Health Qual Life Outcomes (2013) 11:92. doi: 10.1186/1477-7525-11-92
5. Strine TW, Kroenke K, Dhingra S, Balluz LS, Gonzalez O, Berry JT, et al. The associations between depression, health-related quality of life, social support, life satisfaction, and disability on community-dwelling U.S. adults. J Nerv Ment Dis. (2009) 197:61–4. doi: 10.1097/NMD.0b013e3181924ad8
6. Caron J, Mercier C, Diaz P, Martin A. Socio-demographic and clinical predictors of quality of life in patients with schizophrenia or schizo-affective disorder. Psychiatry Res. (2005) 137:203–13. doi: 10.1016/j.psychres.2005.07.002
7. Fleury MJ, Grenier G, Bamvita JM. Predictive typology of subjective quality of life among participants with severe mental disorders after a five-year follow-up: a longitudinal two-step cluster analysis. Health Qual Life Outcomes (2015) 13:150. doi: 10.1186/s12955-015-0346-x
8. O'Connell MJ, Kasprow W, Rosenheck R. Rates and risk factors for homelessness after successful housing in a sample of formerly homeless veterans. Psychiatr Serv. (2008) 59:268–75. doi: 10.1176/ps.2008.59.3.268
9. O'Connell MJ, Kasprow W, Rosenheck R. Direct placement versus multistage models of supported housing in a population of veterans who are homeless. Psychol Serv. (2009) 6:190–201. doi: 10.1037/a0014921
10. Tsai J, Kaspow W, Rosenheck RA Exiting homelessness without a voucher: a comparison of independently housed and other homeless veterans. Psychol Serv. (2011) 8:114–22. doi: 10.1037/a0023189
11. Caton CLM, Dominguez B, Schanzer B, Hasin DS, Shrout PE, Felix A, et al. Risk factors for long-term homelessness: findings from a longitudinal study of first-time homeless single adults. Am J Public Health (2005) 95:1753–9. doi: 10.2105/AJPH.2005.063321
12. Wolf J, Burnam A, Koegel P, Sullivan MS. Changes in subjective quality of life among homeless adults who obtain housing: a prospective examination. Soc Psychiatry Psychiatr Epidemiol. (2001) 36:391–8. doi: 10.1007/s001270170029
13. Gilmer TP, Stefanic A, Ettner SL, Mannig WG, Tsemberis S. Effect of full-service partnerships on homeless, use and cost of mental health services, and quality of life among adults with serious mental illness. Arch. Gen. Psychiatry (2010) 67:645–52. doi: 10.1001/archgenpsychiatry.2010.56
14. Hwang S, Aubry T, Palepu A, Farrell S, Nisenbaum R, Hubley A, et al. The health and housing in transition study: a longitudinal study of the health of homeless and vulnerably housed adults in three Canadian cities. Int J Public Health (2011) 56:609–23. doi: 10.1007/s00038-011-0283-3
15. Hubley AM, Russell LB, Palepu A, Hwang SW. Subjective quality of life among individuals who are homeless: a review of current knowledge. Soc Indic Res. (2014) 115:509–24. doi: 10.1007/s11205-012-9998-7
16. Lam JA, Rosenheck R. The effect of victimization on clinical outcomes of homeless persons with serious mental illness. Psychiatr Serv. (1998) 49:678–83. doi: 10.1176/ps.49.5.678
17. Lam JA, Rosenheck RA. Correlates of improvement in quality of life among homeless persons with serious mental illness. Psychiatr Serv. (2000) 51:116–8. doi: 10.1176/ps.51.1.116
18. Tsemberis S, Gulcur L, Nakae M. Housing first, consumer choice, and harm reduction for homeless individuals with a dual diagnosis. Am J Public Health (2004) 94:651–6. doi: 10.2105/AJPH.94.4.651
19. Hwang S, Gogosis E, Chambers C, Dunn J, Hoch J, Aubry T. Health status, quality of life, residential stability, substance use, and health care utilization among adults applying to a supportive housing program. J Urban Health (2011) 88:1076–90. doi: 10.1007/s11524-011-9592-3
20. Ministère de la Santé et des Services Sociaux. Ensemble, Pour éviter la rue et en sortir. Politique nationale de lutte à l'itinérance. Quebec City, QC (2014).
21. Sullivan G, Burnam A, Koegel P, Hollenberg J. Quality of life of homeless persons with mental illness: results from the course-of-homelessness study. Psychiatr Serv. (2000) 51:1135–41. doi: 10.1176/appi.ps.51.9.1135
22. van der Plas AGM, Hoek HW, van Hoeken D, Valencia E, van Hemert AM. Perceptions of quality of life and disability in homeless persons with schizophrenia and persons with schizophrenia living in non-institutional housing. Int J Soc Psychiatry (2012) 58:629–34. doi: 10.1177/0020764011419056
23. Cheung AM, Hwang SW. Risk of death among homeless women: a cohort study and review of the literature. CMAJ (2004) 170:1243–7. doi: 10.1503/cmaj.1031167
24. Christensen RC, Garces LK. Where is the research on homeless persons and suicide? Psych Serv. (2006) 57:447. doi: 10.1176/ps.2006.57.4.447
25. Filtzpatrick IJ, Lagory M, Ritchey F. Just thinking about it: social capital and suicide ideation among homeless persons. J Health Psychol. (2007) 12:750–60. doi: 10.1177/1359105307080604
26. Oliveira LP, Pereira ML, Azevedo A, Lunet N. Risk factors for cardiovascular disease among the homeless and in the general population of the city of Porto, Portugal. Cad Saude Publica (2012) 28:1517–29. doi: 10.1590/S0102-311X2012000800010
27. Fazel S, Geddes JR, Kushel M. The health of homeless people in high-income countries: descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet (2014) 384:1529–40. doi: 10.1016/S0140-6736(14)61132-6
28. Lehman AF, Dixon LB, Kernan E, DeForge B, Postrado LT. A randomized trial of assertive community treatment for homeless persons with severe mental illness. Arch Gen Psychiatry (1997) 54:1038–43. doi: 10.1001/archpsyc.1997.01830230076011
29. Cheung A, Somers JM, Moniruzzaman A, Patterson M, Frankish CJ, Krausz M, et al. Emergency department use and hospitalizations among homeless adults with substance dependence and mental disorders. Addict Sci Clin Pract. (2015) 10:17. doi: 10.1186/s13722-015-0038-1
30. Zhang L, Norena M, Gadermann A, Hubley A, Russell L, Aubry T, et al. Concurrent disorders and health care utilization among homeless and vulnerably housed persons in canada. J Dual Diagn. (2018) 14:21–31. doi: 10.1080/15504263.2017.1392055
31. Herman SE, Mowbray CT. Client typology based on functioning level assessments: utility for service planning and monitoring. J Ment Health Adm. (1991) 18:101–15. doi: 10.1007/BF02518604
32. Bonin JP, Fournier L, Blais R. A typology of mentally disordered users of resources for homeless people: towards better planning of mental health services. Adm Policy Ment Health (2009) 36:223–35. doi: 10.1007/s10488-009-0206-2
33. Mowbray CT, Bybee D, Cohen E. Describing the homeless mentally ill: cluster analysis results. Am J Community Psychol. (1993) 21:67–93. doi: 10.1007/BF00938208
34. Wuerker AK, Keenan CK. Patterns of psychiatric service use by homeless mentally ill clients. Psychiatr Q. (1997) 68:101–16. doi: 10.1023/A:1025449504221
35. Adlaf EM, Zdanowicz YM. A cluster-analytic study of substance problems and mental health among street youths. Am J Drug Alcohol Abuse (1999) 25:639–60. doi: 10.1081/ADA-100101884
36. Goldstein G, Luther JF, Jacoby AM, Haas GL, Gordon AJ. A Taxonomy of medical comorbidity for veterans who are homeless. J Health Care Poor Underserved (2008) 19:991–1005. doi: 10.1353/hpu.0.0040
37. Aubry T, Farrell S, Hwang SW, Calhoun M. Identifying the patterns of emergency shelter stays of single individuals in canadian cities of different sizes. Housing Stud. (2013) 28:910–27. doi: 10.1080/02673037.2013.773585
38. Kuhn R, Culhane DP. Applying cluster analysis to test a typology of homelessness by pattern of shelter utilization: results from the analysis of administrative data. Am J Community Psychol. (1998) 26:207–232. doi: 10.1023/A:1022176402357
39. Cherry A. Combining the cluster and discriminant analysis to develop a social bond typology of runaway youth. Res Soc Work Pract. (1993) 3:175–90. doi: 10.1177/104973159300300204
40. Zide MR, Cherry AL. A typology of runaway youths: an empirically based definition. CASW (1992) 9:155–68. doi: 10.1007/BF00755230
41. Culhane DP, Metraux S, Park JM, Schretzman M, Valente J. Testing a typology of family homelessness based on patterns of public shelter utilization in four U.S. jurisdictions: implications for policy and program planning. Hous Policy Debate (2007) 18:1–28. doi: 10.1080/10511482.2007.9521591
42. Statistics Canada Statistics Canada. Homeless Shelter Capacity, Bed and Shelter Counts for Emergency Shelters, Transitional Housing and Violence Against Women Shelters for Canada and Provinces, Employment and Social Development Canada Annual (Number). Table 14-10-0353-01.
43. Baker F, Intagliata J. Quality of life in the evaluation of community support systems. Eval Program Plann. (1982) 5:69–79. doi: 10.1016/0149-7189(82)90059-3
44. Caron J, Mercier C, Tempier R. Validation of satisfaction with life domains scale in Quebec. Sante Ment Que (1997) 22:195–217. doi: 10.7202/032422ar
45. Statiscs Canada. Canadian community health survey: mental health and well-being. The Daily. (2003, September 3).
46. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry (1998) 59 (Suppl. 20):22–3; quiz 34–57.
47. Moran P, Leese M, Lee T, Walters P, Thornicroft G, Mann A. Standardised assessment of personality - abbreviated scale (SAPAS): preliminary validation of a brief screen for personality disorder. Br J Psychiatry (2003) 183:228–32. doi: 10.1192/bjp.183.3.228
48. Skinner HA. The drug abuse screening test. Addict Behav. (1982) 7:363–71. doi: 10.1016/0306-4603(82)90005-3
49. Bohn MJ, Babor TF, Kranzler HR. The alcohol use disorders identification test (AUDIT): validation of a screening instrument for use in medical settings. J Stud Alcohol Drugs (1995) 56:423–32. doi: 10.15288/jsa.1995.56.423
50. Üstü B, Chatterji S, Kostanjsek N, Rehm J, Kennedy C, Epping-Jordan J, et al. Developing the World Health Organization disability assessment schedule 2.0. Bull World Health Organization (2010) 88:815–23. doi: 10.2471/BLT.09.067231
51. Gravel R, Beland Y. The Canadian Community Health Survey: mental health and well-being. Can J Psychiatry (2005) 50:573–9. doi: 10.1177/070674370505001002
52. Caron J, Cargo M, Daniel M, Liu A. Predictors of quality of life in montreal, canada: a longitudinal study. Community Ment Health J. (2018) doi: 10.1007/s10597-018-0340-y. [Epub ahead of print].
53. LaGory M, Fitzpatrick K, Ritchey F. Life chances and choices: assessing quality of life among the homeless. Sociol Q. (2001) 42:633–51. doi: 10.1111/j.1533-8525.2001.tb01783.x
54. Kushel MB, Vittinghoff E, Haas JS. Factors associated with the health care utilization of homeless persons. JAMA (2001) 285:200–6. doi: 10.1001/jama.285.2.200
55. National Health Care for the Homeless Council. Disability, Employment and Homelessness. 2011 Policy Statement. Available online at: http://www.nhchc.org/wp-content/uploads/2011/09/disability2011_-final.pdf (Accessed August 10, 2012).
56. O'Connell JJ, Zevin BD, Quick PD, Anderson SF, Perret YM, Dalton M, et al. Documenting Disability: Simple Strategies for Medical Providers. Nashville, TN: Health Care for the Homeless Clinicians' Network, National Health Care for the Homeless Council (2007). Available online at: http://www.nhchc.org/wp-content/uploads/2012/02/DocumentingDisability2007.pdf
57. Finlay AK, Binswanger A, Smelson D, Sawh L, McGuire J, Rosenthal J, et al. Sex differences in mental health and substance use disorders and treatment entry among justice-involved Veterans in the Veterans Health Administration. Med Care (2015) 53 (4 Suppl. 1):S105–11. doi: 10.1097/MLR.0000000000000271
58. Finfgeld-Connett D. Becoming homeless, being homeless, and resolving homelessness among women. Issues Ment Health Nurs. (2010) 31:461–9. doi: 10.3109/01612840903586404
59. Byrne T, Montgomery AT, Dichter ME. Homelessness among female veterans: a systematic review of the literature. Women Health (2013) 53:572–96. doi: 10.1080/03630242.2013.817504
60. National Coalition for the Homeless. Substance Abuse and Homelessness (2009). Avalaible online at http://www.nationalhomeless.org/factsheets/addiction.pdf
61. O'Brien KK, Schuttke A, Alhakeem A, Donnelly-Swift E, Keogh C, O'Carroll A, et al. Health, perceived quality of life and health services use among homeless illicit drug users. Drug Alcohol Depend. (2015) 154:139–45. doi: 10.1016/j.drugalcdep.2015.06.033
62. McGovern MP, Lambert-Harris C, Gotham HJ, Claus RE, Xie H. Dual diagnosis capability in mental health and addiction treatment services: an assessment of programs across multiple state systems. Adm Policy Ment Health (2014) 41:205–14. doi: 10.1007/s10488-012-0449-1
63. Fries L, Fedok G, Kubiak SP. Role of gender, substance use, and serious mental illness in anticipated postjail homelessness. Social Work Res. (2014) 38:107–116. doi: 10.1093/swr/svu014
Keywords: quality of life, homeless, cluster analysis, mental health disorders, substance use disorders, type of accommodation, health care service use variables
Citation: Gentil L, Grenier G, Bamvita J-M, Dorvil H and Fleury M-J (2019) Profiles of Quality of Life in a Homeless Population. Front. Psychiatry 10:10. doi: 10.3389/fpsyt.2019.00010
Received: 24 August 2018; Accepted: 09 January 2019;
Published: 30 January 2019.
Edited by:
Matthias Jaeger, Psychiatrie Baselland, SwitzerlandReviewed by:
Susanne Jaeger, ZfP Südwürttemberg, GermanyAndreas Hoell, Central Institute for Mental Health, Germany
David Briner, Independent researcher, Zurich, Switzerland
Copyright © 2019 Gentil, Grenier, Bamvita, Dorvil and Fleury. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie-Josée Fleury, ZmxlbWFyQGRvdWdsYXMubWNnaWxsLmNh