 Roman Schleifer
Roman Schleifer Alex Gamma
Alex Gamma Ingeborg Warnke
Ingeborg Warnke Mounira Jabat
Mounira Jabat Wulf Rössler
Wulf Rössler Michael Liebrenz
Michael Liebrenz- 1Institute of Forensic Medicine, Department of Forensic Psychiatry, University of Bern, Bern, Switzerland
- 2Department of Psychiatry, Psychotherapy and Psychosomatics, Psychiatric Hospital, University of Zurich, Zurich, Switzerland
Objective: To evaluate perceived needs and difficulties related to instruments for assessing work ability in individuals with mental disorders.
Method: We conducted an online survey of 104 German-speaking medico-legal experts (forensic psychiatric and psychology experts, insurance physicians) and therapists.
Results: The large majority of respondents reported they would welcome a standardized, structured instrument for the assessment of work ability. High predictiveness, inter-rater agreement, comprehensibility for laymen, and symptom validity were desired in roughly equal measure as the main characteristic of such an instrument. More women than men, and more medico-legal experts than therapists, considered symptom validation as always necessary. Pain, personality, and affective disorders were perceived to be the most difficult disorders in the context of work ability assessments.
Conclusion: Our survey documents professionals' wish for a structured assessment of work ability in both medico-legal and therapeutic settings.
Introduction
In the past decades, most OECD member states have seen a substantial rise in spending on disability benefits, with mental disorders accounting for at least 30–45% of claims (1). In most social security systems, the assessment of work ability and of the resulting claim is based on a medical examination (2). While the validity and reliability of such examinations are crucial quality criteria, there is evidence for inhomogeneity of expert decisions and consequent inequality of claimants before the law (3, 4). The current use of unstructured and non-validated procedures further provokes inaccurate assessments of claimants' personal resources, potential for rehabilitation, and social and occupational outcomes (5, 6). In Switzerland, similar criticism has also arisen from within the medical community, as well as from politicians and the general public. For example, current assessment procedures have been likened to a lottery, where the quality of assessment is largely a matter of chance, due to the random assignment of claimants to experts and to alleged substantial differences in expert competence (7–10).
The insufficient reliability of psychiatric assessments has also been discussed in other German-speaking countries (11, 12), with references to the discourse in Switzerland (13) and attempts to improve education by establishing uniform quality criteria (14).
Standardization of assessments is one way to improve their homogeneity and comprehensiveness. A first step toward this goal are guidelines specifying formal criteria for structuring assessment procedures. A further gain should result from the use of standardized, structured instruments for assessing work ability (15, 16).
In German-speaking countries, the de facto standard tool for work ability assessment in psychiatric patients is the Mini-ICF-APP (17, 18), which contains components of the WHO's International Classification of Functioning, Disability and Health (ICF). It is, however, not validated for the insurance medical setting. As far as we know, among the many existing instruments, none are validated and specific to mental disorders in such a setting (19, 20). Thus there appears to be a lack of validated structured instruments for the expert assessment of work ability in individuals affected by mental disorders (19).
The present study is part of a project to develop such an instrument called REAcT (= “Risikoeinschätzung für Einschränkungen der beruflichen Aktivität und Teilhabe,” or, in English: “Risk assessment for restrictions of work activity and participation”). Phase one of the development consisted in an evaluation of perceived needs and difficulties in this area of testing. In particular, we were interested to see whether the lack of standardized tools would emerge as an actual need in the reports of medical professionals. Responses were collected in an online survey distributed among German-speaking therapists and medico-legal experts. Its results are reported here in a largely descriptive manner.
Materials and Methods
Survey and Sample
Survey questions were formulated based on the authors' interest, in particular the ongoing development of REAcT. The survey was hosted online by “Research Electronic Database Capture” (REDCap) (21). In June 2017, a link to the survey was distributed to German-speaking therapists and medico-legal experts (forensic psychologists and psychiatrists, and insurance physicians) via a mailing list for announcements of continuing education events, and leaflets were distributed at such events over the past 5 years. The mailing list consisted of 400, mostly Swiss and some German, recipients, including all members of the Swiss Society of Forensic Psychiatry. Initial recipients were encouraged to recruit further respondents. Data was gathered for 4 months. No systematic attempt at sampling representative sections of a larger population was made.
The survey contained 58 questions: 1 item each for age and gender, 2 items about respondents' medical certification, 2 items about continuing education/additional training, 1 item about area of work, 1 item about the number of completed professional assessments of work ability, 7 items about perceived needs for a standardized instrument for work ability assessment, 2 items about respondents' current use of standardized instruments, 1 item about the perceived difficulty of assessing work ability in different psychiatric disorders, 1 item about the estimated agreement among experts for these disorders, and 39 items about specific aspects of the REAcT questionnaire (these are not part of the present report). The questionnaire as used in this study (19 items) can be found in the Appendix at the end of the manuscript.
Bern's cantonal ethics committee filed a letter of non-competence stating no objection (Req-2017-00278).
Statistics
Frequency data was analyzed using χ2-tests, while Kruskal-Wallis tests were used for comparing continuous and ordinal data across groups. The Kruskal-Wallis test is a multisample generalization of the two-sample Wilcoxon (Mann-Whitney) rank-sum test and yields the same statistical inference (p-value) in the two-group case. It avoids the assumption of normality of the data.
Some categorical data (Figures 2–4) is visualized using “spine plots” (22), which, like stacked bar charts, show the proportion of various categories among two or more groups, but additionally encode the number of subjects per category or group in the width of the bars. Thus, it becomes easy to see whether, for example, one group was much smaller than its comparison group, and the size of its category proportions correspondingly less trustworthy. Analyses were performed in R 3.3.3 for Mac.
Results
Sample
By the end of the data acquisition period, N = 104 responses had been collected. About two thirds of the questions had complete data, the rest had 5 missing values each. The mean age of the sample was 45 years, and 39% of respondents were women. There was no statistically significant age difference between the sexes [H(1) = 0.15, p = 0.22]. Sixty-Nine percent of participants were physicians (a breakdown into specialties is reported in the next section). Forty percent of participants were medico-legal experts, 55% were therapists involved with work-disabled psychiatric patients, and 5% of the data was missing. Medico-legal experts were defined as respondents with certified training in insurance-medical assessment.
The sex distribution among professional groups was almost identical: 39% of medico-legal experts were women Vs. 40% of therapists [ = 0.04, p = 0.85].
Table 1 Lists the Characteristics of the Sample.
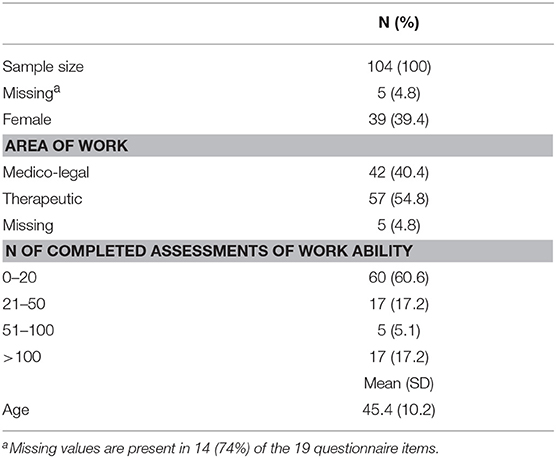
Table 1. Sample description.
Certification in Medical Specialty
Sixty-Nine percent of the sample had a certification in some field of medical specialization. Sixty-one percent were specialized in (adult) psychiatry and psychotherapy, Two percent in child and adolescent psychiatry and psychotherapy, another Two percent in internal medicine, one percent in psychosomatic medicine and Eleven percent in other fields, including cardiology, sexual therapy, and neurology.
Further Education
Of our respondents, 42% had received further education in the area of insurance medicine; 23% had attained the title of Certified Medical Expert in Swiss Insurance Medicine (SIM); 15% had become certified forensic psychiatrists and psychotherapists SGFP (Swiss Society for Forensic Psychiatry); 5% had attained the title of Certified Medical Examiner SGV (Swiss Society of Insurance Physicians); 2% were certified physicians for social insurance medicine (“RAD physicians”) and 7% gave various other answers, each of which appeared only once.
Area of Work
In all, 49% of respondents worked in a clinic, day clinic or outpatient clinic, 34% were practitioners, 21% worked at a medical assessment center, 2% worked in an insurance company and 13% gave various other answers, only one of which occurred more than once.
Number of Assessments Completed
The total number of completed assessments of work ability was less than 21 in 61% of participants, 21 to 50 in 17% of participants, 51-100 in 5%, and more than 100 in 17%. Using a somewhat arbitrary cut-off of 20 lifetime assessments, we considered a total of roughly 40% of experts “experienced.”
Currently Used Instruments for Work Ability Assessment
In their own work, 37% of respondents already used a standardized instrument for work ability assessment. A further 30% used the Mini-ICF-APP (23), 13% used the GAF (Global Assessment of Functioning scale), 2% used ICF-CorSets, and 6% reported other instruments: 1 person listed the IFAP-1(16), while all other entries referred to tests not specific to work ability assessment [e.g., HAM-D (Hamilton Scale for depression), SCL-90R (Symptom Complaint List−90 Revised), WAIS-IV (Wechsler Adult Intelligence Scale Version IV) etc].
Need for Standardized Assessment Instrument
Figure 1 shows that the vast majority of respondents would welcome a standardized, structured tool for work ability assessment (top two panels).
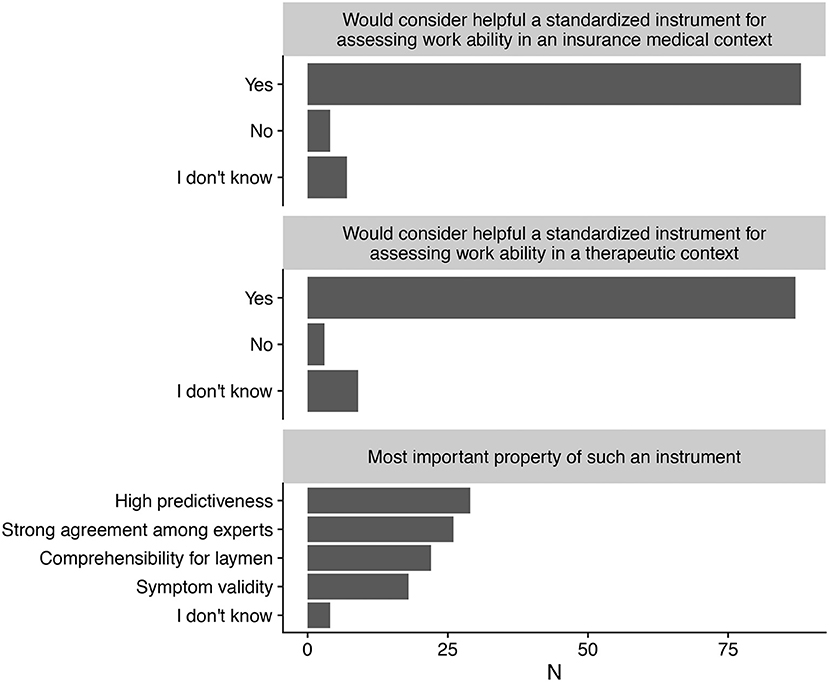
Figure 1. Desirability of a structured, standardized assessment of work ability in an insurance medical (Top) and therapeutic (Middle) context, as well as most important property expected of such an instrument (Bottom).
Preferred Form of Instrument
Half of respondents said they would prefer an online instrument, 37% preferred a paper version, while 13% had no preference.
Preferred Type of Rating
In all, 59% of respondents preferred an informant-rating scale (for use by the expert), 13% preferred a self-rating scale (for use by the patient), while 29% were uncommitted.
Preferred Property of Instrument
Responses on the most important and desirable feature of such a new tool were fairly evenly distributed: predictiveness, inter-expert agreement, comprehensibility for laymen, and symptom validity all received between 20 and 30% of the responses (bottom panel).
Medico-legal experts and therapists did not differ appreciably in their responses, except perhaps for a smaller proportion of medico-legal experts emphasizing an instrument's comprehensibility for laymen.
Importance of Symptom Validity Tests
The most frequent view (44%) on the importance of symptom validity tests was that they should only be administered when the expert had reason to suspect that a claimant's reports on complaints might not be truthful. The view that they are always necessary was about half as frequent (23%). A surprisingly high proportion (25%) of participants expressed no opinion.
Medico-legal experts were less likely than therapists to find symptom validation never necessary (0 vs. 3.5%) or only when requested (2.4 vs. 7.0%). Also, they were much less likely to give “I don't know” as an answer (9.5 vs. 36.8%; Figure 2). The overall group test yielded χ2(4) = 14.93, p = 0.005.
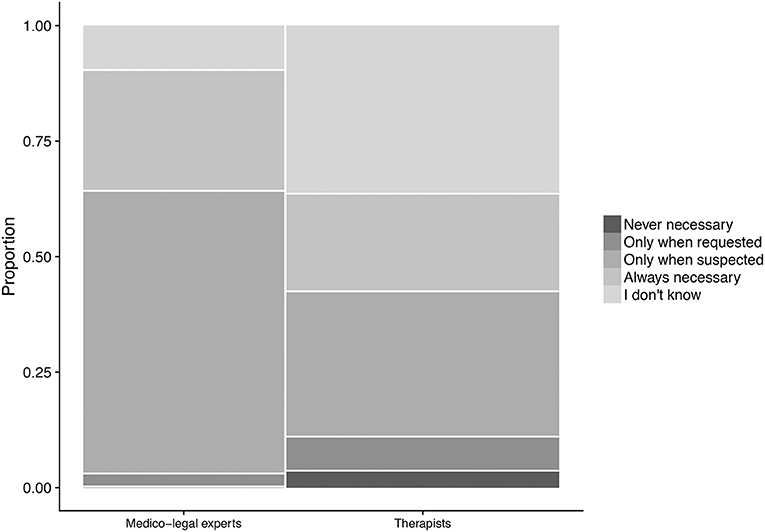
Figure 2. Perceived necessity of symptom validation, broken down by area of work. The width of the categories represents the frequency of the corresponding response in the total sample.
Moreso than men, women favored the strict necessity of symptom validation (60.9 vs. 39.1%), whereas the small proportion (2.0%) of respondents finding it never necessary consisted exclusively of men. The overall group test yielded χ = 8.54, p = 0.07.
Perceived Difficulty of Assessing Various Mental Disorders
For each of six categories of psychiatric disorders (affective, psychotic, substance use, pain, personality, developmental), participants were asked to rate whether or not they considered it to be the most difficult disorder to assess for work ability, and how likely they considered different experts to agree on such assessments.
Respondents sometimes nominated more than one disorder as being the most difficult to assess, which led to the number of nominations exceeding the number of respondents. This was unexpected, as we assumed asking for the one most difficult among a group of disorders would elicit only one answer per person. However, given this de facto multiple-response format, disorders in descending order of difficulty were: pain (78 nominations), personality (63 nominations), affective (27 nominations), substance use (20 nominations), developmental (8 nominations), and psychotic (4 nominations).
Expected Expert Agreement on Various Mental Disorders
We found that the more a disorder was considered difficult to assess, the less respondents expected expert agreement on such assessments. This effect was clearest in the case of affective disorders (Figure 3), where the overall group test yielded χ = 15.28, p = 0.009.
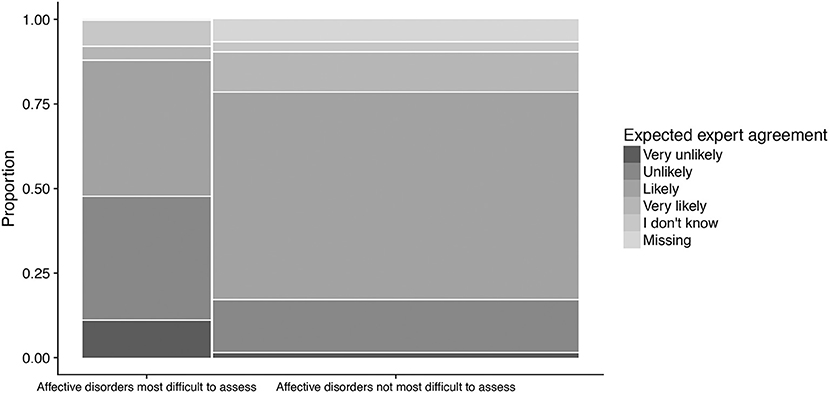
Figure 3. Expected expert agreement on work ability assessments of affective disorders, as a function of perceived difficulty of such assessments. Respondents considering affective disorders as most difficult to assess tended to find expert agreement more unlikely than respondents who did not. The width of the categories represents the frequency of the corresponding response in the total sample.
Among those finding affective disorders the most difficult to assess (N = 27), medico-legal experts tended to expect less agreement than therapists (Figure 4). More of them considered an agreement ‘very unlikely' (23.1 vs. 0%) or ‘unlikely' (46.2 vs. 28.6%), while comparatively fewer expected agreement to be “likely” (23.1 vs. 57.1%) or “very likely” (0 vs. 7.1%). The overall group test yielded = 6.64, p = 0.16.
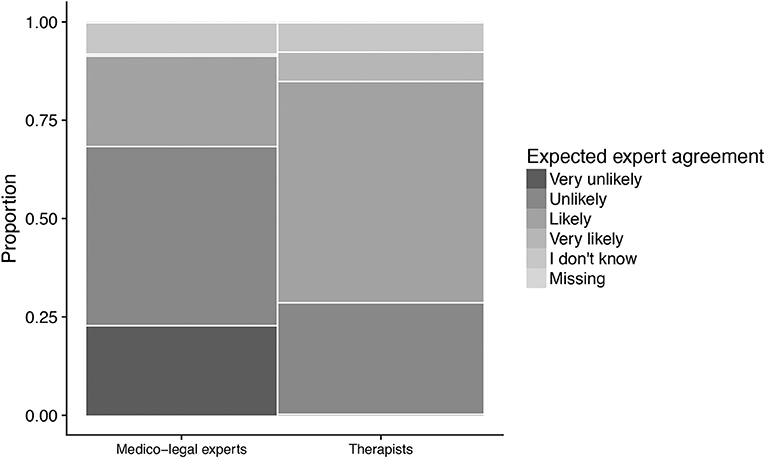
Figure 4. Expected expert agreement in work ability assessments for affective disorders, by area of work. Only those considering affective disorder most difficult to assess are shown (N = 27). Medico-legal experts tended to be more skeptical about expected agreement than therapists. The width of the categories represents the frequency of the corresponding response in the sample.
Men tended to expect less expert agreement than women (15.8 vs. 0% for “very unlikely,” 0 vs. 12.5% for “very likely”). The overall group test yielded = 4.07, p = 0.40. However, due to the small sample size, these test result can be assumed to be somewhat unreliable.
Discussion
Our survey among 104 German-speaking professionals documented the wish for a standardized, structured instrument to assess work ability. Respondents were overwhelmingly in favor of such a tool both in an insurance medical and therapeutic setting. However, roughly equal proportions (~20–30%) of participants named four characteristics as the most desirable property of the instrument: high predictiveness, high inter-rater agreement, high comprehensibility for laymen, and high symptom validity. While this flat distribution may reflect a diversity of informed opinion, it may also be the case (as one reviewer suggested) that these concepts were somewhat foreign to respondents, introducing unsystematic variation into their answers.
Symptom validity, the truthfulness of a claimant's report of complaints, was rated as more important by women than men, and by medico-legal experts compared with therapists. The explanation of the sex difference, if it is a real effect, is not obvious to us. One plausible idea is that the higher levels of conscientiousness found in women (24) may make them consider it more of a duty (than men would) to first rule out malingering before proceeding further. The finding regarding medico-legal experts, on the other hand, may simply reflect the perception that malingering is more frequent in a medico-legal than in a clinical setting (25). Further, there might have been a lack of understanding of the concept of symptom validity in therapists, contributing to lower importance ratings. In any case, the between-group heterogeneity in importance given to symptom validation should be considered in the development of the REAcT and other instruments, e.g., by instructing users to pay special attention to symptom validation in order to achieve robustly high rates of this practice across all groups.
Asking respondents about which of six categories of psychiatric disorders was most difficult to assess for work ability yielded the following ranking by decreasing difficulty: pain disorder, personality disorders, affective disorders, substance use disorders, developmental disorders, and psychosis. This rank order is partly reflected in Swiss federal court rulings, which are more complex for pain and affective disorders and involve special legislation (26).
Not surprisingly, more difficult disorders were expected by participants to lead to lower expert agreement in assessing work ability. This effect was most pronounced for affective disorders. This finding is consistent with the majority of participants wishing for a standardized and structured assessment tool, as such a tool would be expected to reduce assessment difficulty and consequently lead to higher inter-rater agreement, i.e., higher reliability.
Our study had a number of limitations: First, the sample was small and statistical power correspondingly low. Second, due to the non-random distribution of the survey, including snowball sampling, it is not known to what extent current results are generalizable to a larger population. Third, we had no control over possibly untruthful survey responses.
In conclusion, the results of our survey document professionals' wish for a structured, standardized instrument to assess work ability in both insurance medical and therapeutic settings. This study was the first part of a project that aims at the development of such an instrument.
Author Contributions
All authors were responsible for conceiving and designing the study and contributed to data interpretation. AG and IW conducted the data analysis. RS and ML were responsible for data acquisition and contributed to its interpretation. RS, AG, and ML wrote the manuscript, and all co-authors revised its content. All authors approved the final version of the manuscript and agree to be held accountable for all aspects of the work.
Conflict of Interest Statement
WR has been the chief editor of the present journal (Frontiers in Psychiatry–Public Mental Health) for the past 4 years. He was not involved in any aspect of the processing of this manuscript.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Dominique Rubi for implementing the survey on REDCap.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2018.00453/full#supplementary-material
References
2. Anner J, Kunz R, Boer Wd. Reporting about disability evaluation in European countries. Disabil Rehabilit. (2013) 36:848–54. doi: 10.1186/1471-2458-12-1088
3. Schandelmaier S, Fischer K, Mager R, Hoffmann-Richter U, Leibold A, Bachmann MS, et al. Evaluation of work capacity in Switzerland: a survey among psychiatrists about practice and problems. Swiss Med Wkly. (2013) 143:w13890. doi: 10.4414/smw.2013.13890
4. Patel B, Buschbacher R, Crawford J. National variability in permanent partial impairment ratings. Am J Phys Med Rehabil. (2003) 82:302–6. doi: 10.1097/01.PHM.0000057225.83490.32
5. Ebner G, Dittmann V, Mager R, Stieglitz R-D, Träbert S, Bührlen B, Herdt J. Erhebung der formalen Qualität psychiatrischer Gutachten. Federal Social Insurance Office (2012). Available online at: https://www.bsvlive.admin.ch/praxis/forschung/publikationen/index.html?lang=de&download=NHzLpZig7t,lnp6I0NTU042l2Z6ln1acy4Zn4Z2qZpnO2Yuq2Z6gpJCEdH59hGym162dpYbUzd,Gpd6emK2Oz9aGodetmqaN19XI2IdvoaCUZ,s-.pdf
6. Spanjer J, Krol B, Brouwer S, Groothoff JW. Sources of variation in work disability assessment. Work (2010) 37:405–11. doi: 10.3233/WOR-2010-1094
7. Müller R, Basler P. IV-Rente als ≪Lotterie≫: grosse unterschiede je nach Gutachter. Schweizer Radio und Fernsehen SRF (2016) Available online at: https://www.srf.ch/news/schweiz/iv-rente-als-lotterie-grosse-unterschiede-je-nach-gutachter [Accessed December 18, 2017].
8. Föhn M. Spielt die IV falsch Lotto? Beobachter (2014) Available online at: https://www.beobachter.ch/ahviv/gutachten-spielt-die-iv-falsch-lotto [Accessed December 18, 2017]
9. Bloom D. Thousands of disability benefit tests branded 'unacceptable‘ under the government's own quality control scheme. Mirror (2017) Available online at: https://www.mirror.co.uk/news/politics/thousands-disability-benefit-tests-branded-11641747
10. Mason R. Inquiry into disability benefits “deluged” by tales of despair. The Guardian (2017) Available online at: https://www.theguardian.com/society/2017/nov/27/inquiry-into-disability-benefits-deluged-by-tales-of-despair
11. Dickmann JRM, Broocks A. Das psychiatrische gutachten im rentenverfahren-wie reliabel? Fortschr Neurol Psychiatr. (2007) 75:397–401. doi: 10.1055/s-2006-944303
12. Gehrke J, Müller-Garnn A. Die Nachvollziehbarkeit von Gutachten. Ergebnisse einer Analyse von Gutachtenmängeln. Das Gesundheitswesen (2014) 76:A57. doi: 10.1055/s-0034-1386907
13. Czypionka T, Lappöhn S, Pohl A, Röhrling G. Invaliditätspension aufgrund psychischer Erkrankungen. Institute for Advanced Studies (2016). Available online at: http://irihs.ihs.ac.at/3886/
14. Müller JL, Saimeh N. Standards nichtstrafrechtlicher psychiatrischer Begutachtung. Forensische Psychiatr Psychol Kriminol. (2014) 8:41–8. doi: 10.1007/s11757-013-0250-3
15. Barth J, de Boer WEL, Busse JW, Hoving JL, Kedzia S, Couban R, et al. Inter-rater agreement in evaluation of disability: systematic review of reproducibility studies. BMJ (2017) 356:j14. doi: 10.1136/bmj.j14
16. Bachmann M, de Boer W, Schandelmaier S, Leibold A, Marelli R, Jeger J, et al. Use of a structured functional evaluation process for independent medical evaluations of claimants presenting with disabling mental illness: rationale and design for a multi-center reliability study. BMC Psychiatry (2016) 16:271. doi: 10.1016/j.socscimed.2010.10.022
17. Baron S, Linden M. Disorders of Functions and disorders of capacity in relation to sick leave in mental disorders. Int J Soc Psychiatry (2009) 55:57–63. doi: 10.1177/0020764008091660
18. Linden M, Baron S, Muschalla B, Ostholt-Corsten M. Fähigkeitsbeeinträchtigungen bei psychischen Erkankungen: Diagmostik, Therapie und sozialmedizinische Beurteilung in Anlehnung an das Mini-ICF-APP. Göttingen: Hogrefe (2015).
19. Canela C, Schleifer R, Dube A, Hengartner M, Ebner G, Seifritz E, Liebrenz M. Funktionsbeschreibung in der Begutachtung der Arbeitsfähigkeit – Was ist „evidence-based“? Psychiat Prax. (2016) 43:74–81. doi: 10.1055/s-0035-1552762
20. Schleifer R, Liebrenz M. Beurteilung der beruflichen und ausserberuflichen Leistungsfähigkeit im Rahmen der psychiatrischen Begutachtung. Schweizer Zeitschrift Psychiatrie Neurol. (2017) 3:40–46. Available online at: https://www.rosenfluh.ch/media/psychiatrie-neurologie/2017/03/Beurteilung-der-beruflichen-und-ausserberuflichen-Leistungsfaehigkeit-im-Rahmen-der-psychiatrischen-Begutachtung.pdf
21. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:77–381. doi: 10.1016/j.jbi.2008.08.010
22. Cox NJ. Speaking stata: spineplots and their kin. Stata J. (2008) 8:105–121. Available online at: https://www.stata-journal.com/sjpdf.html?articlenum=gr0031
23. Molodynski A, Linden M, Juckel G, Yeeles K, Anerson C, Vazquez-Montes M, et al. The reliability, validity, and applicability of an English language version of the Mini-ICF-APP. Soc Psychiatry Psychiatr Epidemiol. (2013) 48:1347–54. doi: 10.1007/s00127-012-0604-8
24. Schmitt DP, Realo A, Voracek M, Allik J. Why Can't a man be more like a woman? sex differences in big five personality traits across 55 cultures. J Personal Soc Psychol. (2008) 94:168–82. doi: 10.1037/0022-3514.94.1.168
25. Dandachi-Fitzgerald B, Ponds RWHM, Merten T. Symptom validity and neuropsychological assessment: a survey of practices and beliefs of neuropsychologists in six European countries. Archi Clin Neuropsychol. (2013) 28:771–83. doi: 10.1093/arclin/14.6.511
Keywords: work ability, assessment, psychiatry, rehabilitation, online survey
Citation: Schleifer R, Gamma A, Warnke I, Jabat M, Rössler W and Liebrenz M (2018) Online Survey of Medical and Psychological Professionals on Structured Instruments for the Assessment of Work Ability in Psychiatric Patients. Front. Psychiatry 9:453. doi: 10.3389/fpsyt.2018.00453
Received: 08 March 2018; Accepted: 31 August 2018;
Published: 25 September 2018.
Edited by:
Yasser Khazaal, Université de Genève, SwitzerlandReviewed by:
Stefanie Kristiane Gairing, Universitäre Psychiatrische Kliniken Basel, SwitzerlandValentino Pomini, Université de Lausanne, Switzerland
Copyright © 2018 Schleifer, Gamma, Warnke, Jabat, Rössler and Liebrenz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roman Schleifer, Um9tYW4uU2NobGVpZmVyQGZwZC51bmliZS5jaA==