 Shauna L. Mc Gee
Shauna L. Mc Gee Jan Höltge
Jan Höltge Andreas Maercker
Andreas Maercker Myriam V. Thoma
Myriam V. Thoma- 1Psychopathology and Clinical Intervention, Institute of Psychology, University of Zürich, Zurich, Switzerland
- 2University Research Priority Program ‘Dynamics of Healthy Aging', University of Zürich, Zurich, Switzerland
Background: Trauma, stress, and adversity are well-known for having lasting negative effects on health. Yet, not all individuals go on to develop psychopathology or impaired health. However, little is known about the underlying mechanisms which influence the development of stress-related resilience. Sense of coherence-revised (SOC-R) may play a role in this process, as it is formed through overcoming stress or adversity. It may also influence the steeling effect, which suggests that previous exposure to moderate adversity increases resilience to later adversities.
Objectives: This study aimed to examine the mediating and moderating roles of SOC-R in the relationship between stress or adversity, and psychological health and well-being. It further aimed to investigate the role of SOC-R in steeling processes.
Methods: The study used a longitudinal design, with data collection at baseline and one-year follow-up. Participants included (N = 238) Swiss older adults (Mage = 68.3 years). Standardized questionnaires assessed early-life adversity, recent chronic stress, SOC-R, and current health and well-being. Mediation and moderation analyses examined the mechanisms underpinning stress-related resilience and curvilinear associations assessed steeling.
Results: Results showed that the Manageability subscale of SOC-R significantly moderated the relationship between chronic stress and general mental health (b = 0.04, 95% CI [0.007, 0.082], t = 2.32, p < 0.05). Furthermore, SOC-R significantly mediated the relationship for general mental health (GMH) and satisfaction with life (SWL) with childhood emotional neglect (GMH: b = −0.056, 95% BCa CI [−0.126, −0.002]; SWL: b = −0.043, 95% BCa CI [−0.088, −0.004]), childhood physical neglect (GMH: b = −0.100, 95% BCa CI [−0.232, −0.002]; SWL: b = −0.081, 95% BCa CI [−0.181, −0.002]), and chronic stress (GMH: b = −0.052, 95% BCa CI [−0.100, −0.001]; SWL: b = −0.055, 95% BCa CI [−0.097, −0.020]). No curvilinear associations were observed between stress or adversity and SOC-R.
Conclusions: This study expands on the limited research on stress-related resilience by examining the role of SOC-R in the interactions between adversity, stress, and health. Future research should examine SOC-R in samples with a greater range and different types of adversity. Overall, findings suggest that SOC-R is an important mechanism underpinning the development of stress-related resilience.
Introduction
Trauma, adversity, and stress exposure can have lasting negative effects on psychological health and well-being. In particular, early-life adversity (such as trauma, maltreatment, or neglect) has been shown to lead to long-term health-related problems and the development of mental health disorders (1, 2). For instance, a large-scale study by the World Health Organization (WHO) examined the prevalence of mental health disorders across 21 countries. Findings revealed that 38.8% of participants had experienced some form of early-life adversity, such as maltreatment and neglect, family violence, or physical abuse. It further revealed that such experiences of early-life adversity accounted for 29.8% of psychological disorders in adulthood (3). In addition, stress exposure is also associated with long-term negative outcomes, with chronic stress in particular being detrimental to health. Continuous or repeated exposure to stress can result in cumulative adverse effects on physiological health (4, 5). This “wear and tear” on the body has been shown to lead to an increased susceptibility to the development of stress-related mental health problems, such as depression, anxiety, and post-traumatic stress disorder (6, 7). However, while stress or adversity can lead to long-term negative outcomes, not all individuals go on to develop psychopathology or impaired physical health.
Many individuals are able to adapt to stress or adversity and maintain good health and quality of life (8, 9). Such heterogeneity in response to stress or adversity can be explained by the concept of “resilience.” Resilience refers to the ability to adapt to experiences of stress or adversity and maintain a stable trajectory of healthy psychosocial and physical functioning (10). For example, with regard to chronic stress, a study by Sharpley et al. (11) examined the relationship between chronic stress, resilience, and depression in 104 cancer patients. Results indicated that at low to moderate levels of chronic stress, individuals showed higher levels of resilience and lower levels of depression. In relation to early-life adversity, one notable example of longer-term outcomes of trauma and adversity is the recent longitudinal project by Maercker and colleagues. This research examined psychopathological and resilient outcomes in an adult sample of former indentured child laborers in Switzerland (i.e., the so-called Verdingkinder). Many former Verdingkinder experienced high levels of exposure to trauma and maltreatment in childhood, including physical, emotional, and sexual abuse, as well as physical and emotional neglect (1, 12). Findings showed that some former Verdingkinder had developed mental health disorders in later life: 23% major depressive disorder, 26.3% posttraumatic stress disorder, and 7.8% generalized anxiety disorder (13, 14). Nevertheless, despite the experiences of early-life trauma and adversity, results showed that many former Verdingkinder had no mental health disorders and some also showed indications of resilience in later life (15).
Despite the increasing research interest on resilience in the aftermath of stress or adversity, there is a lack of information on the underlying mechanisms which influence the development of this stress-related resilience. The interplay between risk and resilience factors needs to be further explored in order to better understand resilience processes and interindividual differences in psychological health and well-being. One factor which may play an important role in the development of stress-related resilience is the recently revised Sense of Coherence (SOC-R) concept. The SOC-R concept and scale was developed by Bachem and Maercker (16) as a revision of the original Sense of Coherence (SOC), which had shown conflicting results with regard to its psychometric properties (17–19). The original SOC refers to a way of viewing the world which facilitates successful coping with stressors and is comprised of three components: (1) Comprehensibility, that stimuli are perceived as structured, predictable, and explicable; (2) Manageability, that adequate resources are available to meet demands; and (3) Meaningfulness, that demands are viewed as worth investing in and engaging with (20, 21). While the revised SOC-R concept builds on Antonovsky's research, it assumes a more neutral position on the predictability of events and instead focuses on dealing with the ambiguity of life experiences (16).
SOC-R refers to an individual's ability to integrate and balance both positive and negative experiences in order to maintain and develop health and well-being (16). This ability is proposed to develop through the successful coping with and overcoming of experiences of stress or adversity (21). It may therefore be considered an indicator of stress-related resilience aspects. Similar to the original SOC, the SOC-R concept and scale is comprised of three theoretical dimensions and also includes the manageability dimension: (1) Manageability, the ability to come to terms and deal with difficult situations. However, two new dimensions were developed to reflect the revised concept: (2) Reflection, the ability to consider different perspectives and understand connections, and (3) Balance, the ability to balance positive and negative experiences and feelings (16). Regarding the theoretical assumptions of SOC-R, it is suggested that through these three aspects of SOC-R, individuals are able to mobilize available and appropriate resources in order to cope with stressors and adversity. Furthermore, SOC-R is assumed to be relatively stable later in life and a strong SOC-R is assumed to facilitate healthy aging through the maintenance of psychological health and well-being (16, 22).
Initial research with the SOC-R examined its role in overcoming minor adversities (in the form of daily hassles), as well as major adversities (16). Participants included a bereaved sample (n = 334) and a control sample from the general population (n = 157). Results of this study indicated that SOC-R may be a useful coping mechanism for both minor adversities and extreme stressors. This study also compared the original SOC and SOC-R. With regard to total scores, lower SOC-R was observed in the bereaved sample in comparison to the general population sample. These results were consistent with the findings for the original SOC scale. In addition, construct validity was improved in the SOC-R scale, as SOC-R showed lower correlations than the original SOC with measures of psychological well-being, such as optimism, neuroticism, and self-efficacy (16). These initial findings suggested that the SOC-R scale may be a suitable alternative to the original SOC scale. Further studies have examined the moderating role of SOC-R on the association between adversity health outcomes. One such study examined the influence of SOC-R on the relationship between early-life adversity (in the form of emotional neglect) and mental health in later life (23). Results showed that SOC-R significantly moderated this relationship and acted as a buffer against the negative effects of emotional neglect, with stronger SOC-R associated with better mental health. A more recent study also investigated the interaction between SOC-R and value orientations in predicting posttraumatic growth in bereaved parents (24). Results found a significant interaction between SOC-R and the value self-transcendence, with stronger SOC-R associated with higher levels of posttraumatic growth.
The above research suggests that the strength of an individual's SOC-R can influence their ability to cope with stress or adversity, with stronger SOC-R associated with better outcomes. However, thus far no research exists on the potential mediating role of SOC-R. Previous research with the original SOC construct has shown that SOC can mediate the relationship between adversity and health. For instance, a study with N = 193 participants from the general population found that the relationship between adversity (as indicated by worry, anxiety, and stress) and psychological well-being (as indicated by satisfaction with life) was best explained through the significant mediation of SOC (25). Additionally, a more recent longitudinal study examined the mediating role of SOC in N = 162 cancer patients. Results showed that following a diagnosis of breast cancer, SOC significantly mediated the change in health-related quality of life over a 6-month period, as indicated by factors such as global quality of life and cognitive, social, and emotional functioning (26). Based on these findings, it is anticipated that SOC-R would also act as a mediator between stress or adversity and indicators of psychological health and well-being. However, the mediating role of SOC-R remains unclear and further research is needed in this area.
Furthermore, as the development of SOC-R is closely linked to the experiences of stress or adversity, the strength and influence of SOC-R may therefore differ depending on the type and severity of the adversity, as well as the stage in the lifespan at which it occurs (23, 27). The majority of the research on SOC-R to-date has focused on early-life adversity and event-specific adversity (e.g., bereavement). Research is therefore needed to examine the role of SOC-R with different types and severities of adversity.
Related to severity is the concept of “steeling.” The steeling effect suggests that previous exposure to some or moderate amounts of stress or adversity can strengthen an individual by increasing their resilience and resistance to later stress (28). In comparison, extreme stress or adversity may be too overwhelming to facilitate successful coping, and minimal stress or adversity may not be sufficiently challenging to necessitate the development of coping abilities. Moderate stress or adversity is therefore proposed to be more beneficial than extreme or even minimal stress or adversity (28, 29). Thus, in accordance with the steeling effect, a non-linear, quadratic (i.e., U-shaped) relationship should exist between stress or adversity and well-being (29). Studies have therefore focused on testing the steeling effect theory by assessing curvilinear (i.e., non-linear) rather than linear models of adversity. Results have demonstrated curvilinear relationships between different types of stress or adversity and indicators of health and well-being. For example, some studies have shown optimal health outcomes at moderate levels of early-life adversity [e.g., 30], lifetime adversity [e.g., 31], and perceived stress [e.g., 32]. In addition, a recent study examined the underlying factors involved in steeling by investigating the relationship between early-life adversity, mental health, and successful aging (33). Findings supported the steeling effect and showed optimal levels of successful aging at moderate levels of early-life adversity and that mental health was a significant mediator of this relationship. These studies provide initial evidence for a steeling effect. However, it is a relatively new and emerging area of resilience research and little is known about the underlying mechanisms which may influence the steeling effect. Given the function of SOC-R in overcoming stress or adversity, it may also play a role in steeling processes. Further research is required to clarify the role of SOC-R in the development of stress-related resilience and, in turn, its influence on health and well-being.
Therefore, to address the gaps identified in the literature, the main aim of the current study was to examine the potential mediating and moderating roles of SOC-R in the relationship between stress or adversity and indicators of psychological health and well-being. As recommended by Fossion et al. (27) and Mc Gee et al. (23), and to build on the existing research with SOC-R, the current study assessed two types of stress or adversity, occurring at different stages in the lifespan: early-life adversity (i.e., childhood trauma and maltreatment) and recent chronic stress. Related to this main aim, two hypotheses were tested: First, based on the theoretical assumptions of SOC-R and the existing empirical evidence, it was hypothesized that SOC-R would significantly moderate the relationship between stress or adversity and indicators of psychological health and well-being (i.e., general mental health, satisfaction with life). It was expected that individuals with a strong SOC-R would show better psychological health than individuals with weaker SOC-R, even with high levels of stress or adversity. Second, it was hypothesized that SOC-R would significantly mediate the relationship between stress or adversity and indicators of psychological health and well-being (i.e., general mental health, satisfaction with life). Finally, an additional aim of this study was to conduct an exploratory analysis to investigate the steeling effect and the role of SOC-R in steeling processes. It was therefore expected that moderate levels of stress or adversity would be associated with stronger SOC-R, which in turn would lead to optimal psychological health and well-being (i.e., general mental health, satisfaction with life).
Materials and Methods
Study Design and Procedure
The current study was part of an overarching, longitudinal research project on the steeling effect (“Healthy Aging Against the Odds—Mechanisms behind the Steeling Effect”). A quantitative survey composed of standardized questionnaires was used in this study to assess positive and negative experiences, stress or adversity, current health and well-being, and resilience-related resources. The study was organized and conducted in the University of Zurich and was conducted with the informed consent of all participants in accordance with the Declaration of Helsinki. The protocol was approved by the Swiss ethics committee of the Canton of Zurich (ID 2015-00135) and the Ethics Committee of the Faculty of Arts and Social Sciences in the University of Zurich, Switzerland.
Participants
Eligible participants were those who met the following inclusion criteria: adults aged 50 years or older, and native Swiss-German speakers. G*Power software was initially used to calculate the statistical power analysis. In addition, empirical research recommendations for mediation and moderation analyses were also taken into consideration in determining the required sample size. A minimum sample of N = 224 was required in order to detect small to medium effect sizes, with a significance level of p = 0.05, and statistical power (1-β) of 0.80 (34–36).
Measures
Sense of Coherence Scale—Revised [SOC-R; 16]
The SOC-R scale assesses an individual's ability to perceive and integrate both positive and negative life experiences in order to maintain and develop health (16). As SOC-R is assumed to develop within the context of adversity, it was used in the current study as an indicator of a stress-related resilience resource. The SOC-R scale is comprised of 13 items rated on a five-point Likert scale and yields a single score. The three dimensions which comprise the scale are: Manageability (e.g., “One can always find a way to cope with painful things in life”), Balance (e.g., “In my thoughts and actions I take into account that things often have two sides: good and bad ones”), and Reflection (e.g., “Normally I can consider a situation from various perspectives”). It is available in German and English, and results from the German version show high internal consistency of between α = 0.75 and 0.81 for the total scale, and sufficient internal consistency of between α = 0.54 and 0.77 for the subscales (16, 23). The SOC-R scale has also been shown to have high test-retest reliability, with an r = 0.85 over a 1-month period, and r = 0.74 over an interval of 15 months (16).
Childhood Trauma Questionnaire [CTQ; 37]
The CTQ measures trauma and adversity experienced early in life. It is comprised of 28 items rated on a five-point Likert scale. It is composed of the following five subscales, with each subscale assessed by 5 items: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. It also includes a three-item minimization-denial scale to detect false-negative trauma reports. The German version shows sufficient internal consistency across all subscales, with a Cronbach's alpha of between α = 0.55 and 0.96 (38, 39).
Screening Scale of Chronic Stress [SSCS; 40]
The SSCS is a screening subscale of the Trier Inventory for the Assessment of Chronic Stress (TICS) and measures perceived stress over the previous 3-month period. It assesses five domains of stress: chronic worrying, work-related overload, social overload, excessive demands, and lack of social recognition. It consists of 12 items rated on a five-point Likert scale and yields a single score. The German version shows high internal consistency of α = 0.87 (41).
36-Item Short Form Health Survey Version 2 [SF-36 V2; 42, 43]
The SF-36 measures current mental and physical health. It consists of 36 items and is comprised of eight subscales which combine to form the two distinct component summary scores for mental and physical health. The physical component consists of four subscales: physical functioning, role-physical, bodily pain, and general health; and the mental component consists of four subscales: vitality, social functioning, role-emotional, and mental health (43). To calculate the component summary scores, population- and gender-specific norms for means, standard deviations, and factors loadings are used. As country-specific norms are currently unavailable for Switzerland, German norms were used in the current study (44, 45). The mental health component was used in the current study as an indicator of psychological health. The German version shows high internal consistency across the eight subscales, with a Cronbach's alpha of between α = 0.81 and 0.94 (43).
Satisfaction With Life Scale [SWLS; 46]
The SWLS measures subjective well-being in relation to global life satisfaction (47). It consists of five items rated on a seven-point Likert scale and yields a single score. The German version shows high internal consistency of α = 0.92 (48).
Procedure
A longitudinal study was conducted in the German-speaking regions of Switzerland. The study consisted of two assessment time points: baseline assessment at T1 (summer 2016) and a follow-up assessment 12 months later at T2 (summer 2017). Study participants were recruited using advertisements on websites, in newspapers and magazines, posted flyers, and radio interviews with the authors. Participants were also recruited through the University Research Priority Program “Dynamics of Healthy Aging” in the University of Zurich. The survey was available as an online survey or in pen-and-paper format. Individuals who were interested in taking part contacted the research team and were either emailed a link to the online survey or were posted a pen-and-paper survey package. A study incentive was provided at each assessment point, with participants who completed the survey being entered into a raffle for 10 shopping vouchers.
The online survey was programmed using Unipark software (49). After following the link to the online survey, participants were provided with the study information sheet and then the informed consent form. Participants provided informed consent online by ticking the corresponding box to indicate their consent to participate in the study. Only if they provided informed consent could participants go on to complete the questionnaires. The pen-and-paper survey package also contained an information sheet, an informed consent form, and the questionnaire survey, as well as a free-post return envelope. At T2, participants were provided with either the online survey link or the pen-and-paper survey package depending on their preference at T1. Both survey formats were randomized at the scale level for each participant in order to avoid sequence and order effects. All assessment instruments were repeated at T2, except for the CTQ. As the CTQ assessed trauma and adversity experienced in childhood, this data was collected at baseline (T1) and the scale was then removed from the survey at T2 to reduce participant burden. Only data for which informed consent had been provided was included in the dataset and analyses.
Statistical Analysis
IBM Statistical Package for Social Sciences (SPSS) version 25.0 and PROCESS version 3.0 macro for SPSS were used to analyze the data (50, 51). For each instrument, less than 1% missing values were observed. Little's missing completely at random (MCAR) test suggested that most of the values were MCAR and were therefore replaced using the Expectation-Maximization algorithm (52, 53). For values not missing at random, the means on the subscale level were calculated for each participant.
The mediating and moderating roles of SOC-R were examined in the relationship between past and recent adversity and psychological health and well-being. According to the conceptual framework for longitudinal research proposed by Collins (54), the theoretical model of the anticipated change should be considered in the operationalization of the statistical model. Regarding the current study, according to the theoretical assumptions of SOC-R, SOC-R should be relatively stable later in life (16, 20). Therefore, as the current sample consisted mainly of adults and older adults, it was anticipated that SOC-R would not change significantly over the two assessment points. A paired-samples t-test was conducted to test this assumption. In line with the theoretical assumption, the results showed that SOC-R scores did not differ significantly [t(237) = 1.61, p = 0.11; r = 0.10] at T1 (M = 50.61, SD = 5.72) and T2 (M = 50.12, SD = 5.62). Therefore, baseline SOC-R was used for the longitudinal mediation and moderation analyses with the CTQ subscales. In order to examine the influence of more recent stress, T2 variables were assessed with chronic stress as the predictor.
Mediation analyses (model 4) and moderation analyses (model 1) were conducted using the PROCESS version 3.0 macro for SPSS (50). Socio-demographic variables (i.e., age and education) which showed significant correlations with the predictor and outcomes variables were included as covariates in these analyses to control for potential confounding. Where effects were not observed for total SOC-R, analyses were conducted with the SOC-R subscale level in order to probe potential underlying effects from the dimensions which comprise and ultimately influence SOC-R. Regarding the moderation analyses, a “regions of significance” analysis was also conducted using the Johnson-Neyman procedure (55). This procedure provides additional information on the significance regions for the effect of the predictor (early-life adversity and chronic stress) on the outcome (general mental health and satisfaction with life) at specific values of a continuous moderator (SOC-R). In addition, in order to investigate the role of SOC-R in steeling processes curvilinear (i.e., non-linear) associations, specifically quadratic relationships, must be assessed. To examine these potential curvilinear relationships, the linear stress and adversity terms must first be controlled for by including these variables as covariates in the model. The quadratic (i.e., squared) terms for early-life adversity (CTQ2) and chronic stress (SSCS2) were then implemented into the mediation model (29, 56). Within this model, a steeling effect is indicated by a significant relationship between the quadratic adversity and stress terms and the mediator (i.e., SOC-R), and with the health and well-being indicators of general mental health and satisfaction with life.
Results
Sample Characteristics
A total of 337 participants were recruited at T1. From this, 260 participants completed both assessments (T1 and T2) and 77 participants dropped out after T1. Participants who completed both T1 and T2 assessments showed a higher SOC-R score (M = 50.5, SD = 5.79), than those who dropped out after T1 (M = 48.6, SD = 6.93). An independent samples t-test showed that this difference, 1.93, BCa 95% CI [0.217, 3.64], was significant t(328) = 2.44, p = 0.03, with a small effect size (r = 0.13). From the 260 participants at T2, n = 17 participants were excluded from the analyses due to data missing at the total scale or subscale level and a further n = 5 multivariate outliers were removed. The final sample consisted of N = 238 participants, with a mean age of 68.31 years (SD = 8.96, age range = 50–92 years). The sample was comprised of 175 females (73.5%) and 63 males (26.5%). The online survey was completed by 160 participants (67.2%, Mage = 65.94 years, SD = 8.27) and the pen-and-paper survey was completed by 78 participants (32.8%, Mage = 73.17 years, SD = 8.39). The majority of participants indicated that vocational training (33.2%) was their highest level of education, followed by university-level education at university of applied sciences (18.5%) and university (16.0%). Regarding employment status, 110 participants (46.2%) were retired, 65 (27.3%) were employed, 38 (16.0%) were involved in voluntary activities, and 7 (2.9%) were unemployed. Regarding relationship status, the majority of participants were married (35.3%), followed by widowed (16.4%), and divorced (15.5%). See Table 1 for an overview of the sample characteristics. With regard to early-life adversity, participants reported higher levels of emotional neglect (M = 13.60; SD = 5.55) and emotional abuse (M = 10.43; SD = 5.49), followed by physical neglect (M = 8.41; SD = 3.12), physical abuse (M = 7.15; SD = 3.43), and sexual abuse (M = 7.08; SD = 3.76). However, levels of experienced early-life adversity were low for most categories, with a high percentage of participants reporting none to low levels of adversity: sexual abuse (73.9%, n = 176), physical abuse (84.5%, n = 201), physical neglect (71.4%, n = 170), emotional abuse (70.2%, n = 167), and emotional neglect (59.7%, n = 142).
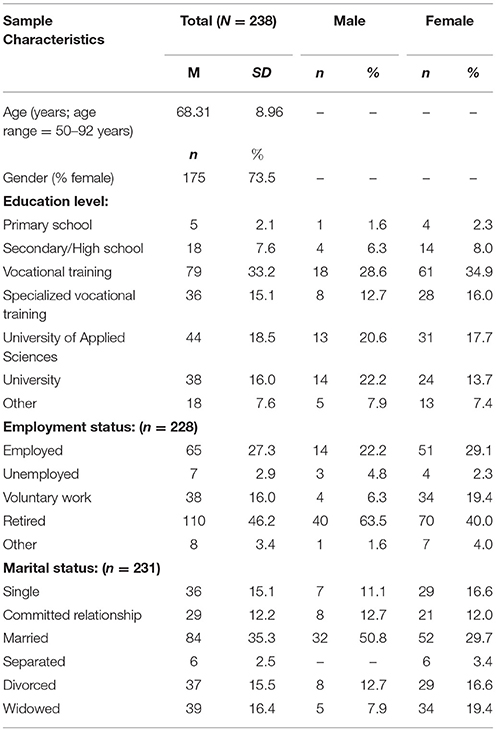
Table 1. Sample characteristics.
Moderation Analysis
Moderation analyses were conducted to examine the influence of SOC-R on the strength of the relationship between different indicators of stress or adversity (i.e., early-life adversity, chronic stress) and current psychological health and well-being (i.e., general mental health, satisfaction with life). With regard to early-life adversity, no significant interaction effects were observed at the SOC-R total or subscale level for the CTQ subscales (physical, sexual, emotional abuse, and physical or emotional neglect).
Regarding chronic stress, no significant interaction effects were shown for total SOC-R. However, on the subscale level, a significant interaction effect was observed for general mental health and the manageability subscale of SOC-R (b = 0.04, 95% CI [0.007, 0.082], t = 2.32, p < 0.05). This suggests that the manageability dimension of SOC-R significantly moderates the relationship between chronic stress and general mental health (see Table 2 for the predictors of general mental health and the interaction effect).
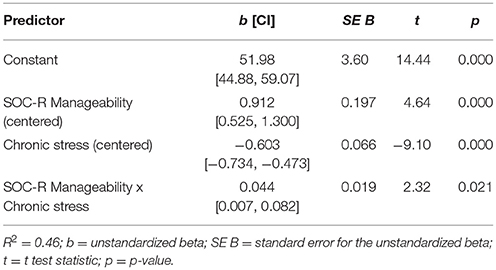
Table 2. Predictors of general mental health and the significant interaction effect, with SOC-R Manageability as the moderator.
Additionally, a significant negative relationship was observed between chronic stress and general mental health at low (b = −0.696, 95% CI [−0.842, −0.551], t = −9.43, p < 0.01); mean (b = −0.607, 95% CI [−0.738, −0.477], t = −9.19, p < 0.01); and high levels of manageability (b = −0.519, 95% CI [−0.674, −0.363], t = −6.58, p < 0.01). High and low levels refer to one standard deviation above and below the mean of the moderator (i.e., SOC-R Manageability). However, the decrease in effect (i.e., b-values) suggested a buffering effect of manageability. Supporting this, results of the Johnson-Neyman procedure showed that as manageability increased, the strength of the relationship between chronic stress and general mental health changed from a strong negative effect (b = −0.963) to a small negative effect (b = −0.341). This indicates that the stronger the manageability, the weaker is the negative effect of chronic stress on general mental health. Visual inspection of the interaction plot also indicated a buffering effect. Individuals with a higher level of manageability had higher scores of general mental health across all levels of chronic stress in comparison to individuals with mean and low levels of manageability. This difference was particularly evident when levels of chronic stress were high. See Figure 1 for the graph of the significant moderation and interaction effects.
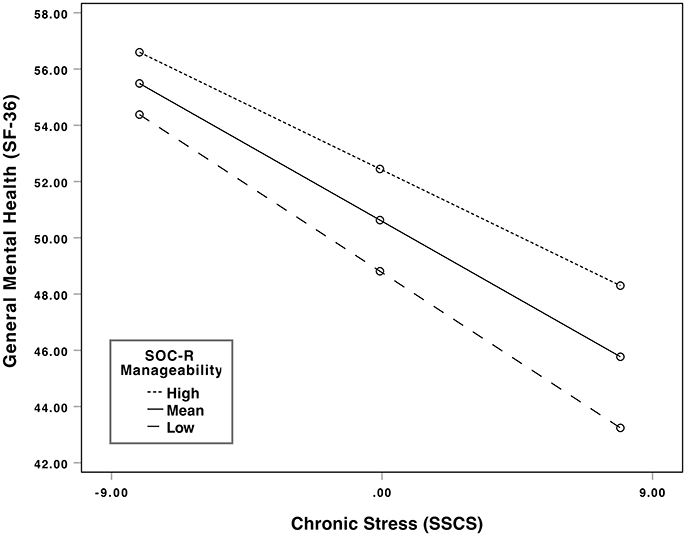
Figure 1. Significant interaction between chronic stress and general mental health at different levels of the moderator (SOC-R manageability). High and low levels refer to one standard deviation above and below the mean of the moderator (i.e., SOC-R Manageability).
Mediation Analysis
Mediation analyses investigated whether SOC-R acts as a mediator of the relationship between stress or adversity (i.e., early-life adversity, chronic stress) and current psychological health and well-being (i.e., general mental health, satisfaction with life). With regard to early-life adversity, a significant indirect effect was observed for the CTQ subscales emotional neglect and physical neglect, for both general mental health and satisfaction with life. No significant indirect effects were observed for the abuse subscales of the CTQ (emotional, physical, sexual abuse). With regard to chronic stress, a significant indirect effect was also observed for both general mental health and satisfaction with life.
CTQ: Emotional Neglect
Regarding emotional neglect, a significant negative total effect was initially observed (b = −0.309, 95% CI [−0.524, −0.094], t = −2.83, p < 0.01), explaining 4.23% of the variance in general mental health. However, when SOC-R was included as a mediator in the model, a significant direct effect emerged, explaining a greater percentage of the variance (9.11%). A significant indirect effect was also observed, indicating that SOC-R significantly mediated the relationship between emotional neglect and general mental health. See Figure 2A for the full mediation model.
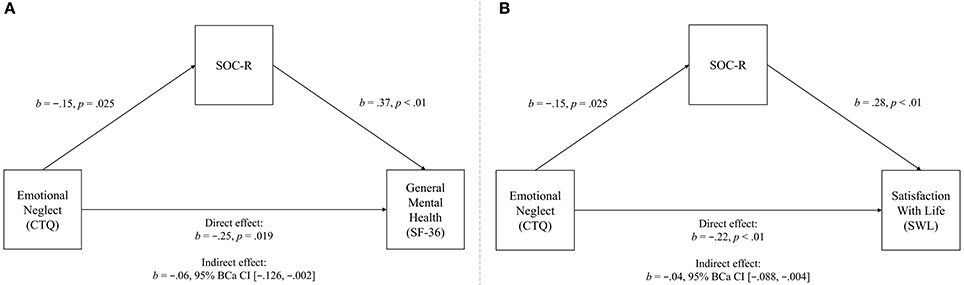
Figure 2. Mediation model of the relationships between emotional neglect (predictor) and general mental health (outcome variable, A), and satisfaction with life (outcome variable, B), significantly mediated by SOC-R (mediator).
Similarly, a significant negative total effect was initially observed for satisfaction with life (b = −0.259, 95% CI [−0.388, −0.129], t = −3.93, p < 0.01), explaining 8.67% of the variance. However, when SOC-R was included as a mediator in the model, a significant direct effect emerged, explaining a greater percentage of the variance (16.13%). A significant indirect effect was also observed, indicating that SOC-R significantly mediated the relationship between emotional neglect and satisfaction with life. See Figure 2B for the full mediation model.
CTQ: Physical Neglect
Regarding physical neglect, a significant negative total effect was initially observed (b = −0.746, 95% CI [−1.125, −0.367], t = −3.88, p < 0.01), explaining 6.92% of the variance in general mental health. However, when SOC-R was included as a mediator in the model, a significant direct effect emerged, explaining a greater percentage of the variance (11.32%). A significant indirect effect was also observed, indicating that SOC-R significantly mediated the relationship between physical neglect and general mental health. See Figure 3A for the full mediation model.
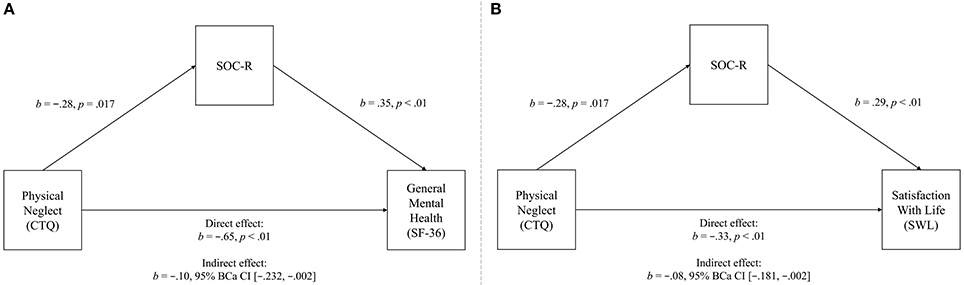
Figure 3. Mediation model of the relationships between physical neglect (predictor) and general mental health (outcome variable, A), and satisfaction with life (outcome variable, B), significantly mediated by SOC-R (mediator).
In addition, a significant negative total effect was initially observed for satisfaction with life (b = −0.407, 95% CI [−0.640, −0.173], t = −3.43, p < 0.01), explaining 7.31% of the variance. However, when SOC-R was included as a mediator in the model, a significant direct effect emerged, explaining a greater percentage of the variance (14.93%). A significant indirect effect was also observed, indicating that SOC-R significantly mediated the relationship between physical neglect and satisfaction with life. See Figure 3B for the full mediation model.
SSCS: Chronic Stress
Regarding chronic stress, a significant negative total effect was initially observed (b = −0.756, 95% CI [−0.880, −0.632], t = −12.04, p < 0.01), explaining 39.38% of the variance in general mental health. However, when SOC-R was included as a mediator in the model, a significant direct effect emerged, explaining a greater percentage of the variance (41.45%). A significant indirect effect was also observed, indicating that SOC-R significantly mediated the relationship between chronic stress and general mental health. See Figure 4A for the full mediation model.
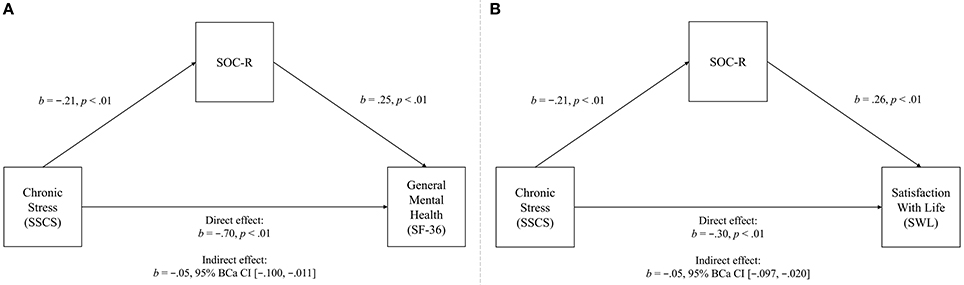
Figure 4. Mediation model of the relationships between chronic stress (predictor) and general mental health (outcome variable, A), and satisfaction with life (outcome variable, B), significantly mediated by SOC-R (mediator).
A significant negative total effect was also initially observed for satisfaction with life (b = −0.359, 95% CI [−0.443, −0.275], t = −8.38, p < 0.01), explaining 26.01% of the variance. However, when SOC-R was included as a mediator in the model, a significant direct effect emerged, explaining a greater percentage of the variance (31.93%). A significant indirect effect was also observed, indicating that SOC-R significantly mediated the relationship between chronic stress and satisfaction with life. See Figure 4B for the full mediation model.
Steeling Effect
Additionally, to examine the role of SOC-R in steeling processes, the quadratic terms for early-life adversity (CTQ2) and chronic stress (SSCS2) were implemented in the mediation model to assess potential curvilinear relationships (29). To detect evidence of steeling, a curvilinear relationship should exist between adversity and stress and SOC-R, and between adversity and stress and the health and well-being outcomes (i.e., general mental health, satisfaction with life). However, results showed no significant indirect effects through SOC-R, and no significant quadratic relationships were observed between adversity and stress and SOC-R. This suggests that highest level of SOC-R was not shown in participants with moderate levels of adversity or stress, and that SOC-R did not significantly mediate the curvilinear relationship between adversity and stress and the indicators of psychological health and well-being.
Discussion
The purpose of the current study was to examine the moderating and mediating roles of SOC-R in the development of stress-related resilience, and to investigate its potential role in steeling processes. Results showed that the Manageability subscale of SOC-R significantly moderated the relationship between chronic stress and psychological health. Results further showed that SOC-R was a significant mediator of the relationship between certain early-life adversities (i.e., physical and emotional neglect), as well as chronic stress, and psychological health and well-being. Finally, results revealed no curvilinear relationships between adversity or stress and SOC-R, indicating no evidence for a steeling effect.
Regarding moderation, total SOC-R was not shown to moderate the relationship between early-life adversity and health or well-being. This finding is in contrast to previous research, which examined the moderating role of SOC-R in a Swiss sample (23). Findings showed that total SOC-R moderated the relationship between emotional neglect in childhood and current mental health (23). One explanation may be that the sample in the current study was somewhat older than in the previous study by Mc Gee et al. (23). It may be that with increasing age, the focus of health-related resources, such as SOC-R, shifts toward more immediate health concerns such as physical or functional health (57). In relation to the original SOC, studies often found a weaker relationship with physical health in comparison with mental health (58). For example, recent research by Gison et al. (59) examined the predictive effect of SOC on psychological and physical outcomes in participants with Parkinson's Disease. Results showed that SOC was predictive of health-related quality of life and emotional distress, but not physical disability. However, the influence of SOC-R on physical health has not yet been assessed and future research is required to further examine this relationship across various age groups with a diversity of physical health statuses.
SOC-R (total) was also not found to moderate chronic stress and health or well-being. However, the Manageability subscale was shown to be a significant moderator. This would tentatively suggest partial support for the first hypothesis (i.e., that SOC-R would significantly moderate the relationship between stress or adversity and indicators of psychological health and well-being). Individuals with strong Manageability showed better general mental health scores than individuals with weaker Manageability, even when levels of chronic stress were high. Furthermore, similar to the moderation results of the study by Mc Gee et al. (23), a buffering effect was observed so that as Manageability increased, the negative effect of chronic stress on general mental health decreased. The Manageability dimension of SOC-R refers to the ability to come to terms and deal with difficult situations (16). These findings may therefore indicate that the ability to manage stress over prolonged periods is an important aspect of successful coping, over and above the influence of the Reflection or Balance dimensions. In support of this, the importance of Manageability for coping was highlighted in the initial evaluation study of SOC-R by Bachem and Maercker (16). Results found that the Manageability dimension explained the largest proportion of variance in the bereaved sample. Bereavement is a major adversity, which would (similar to a chronic stressor) require long-term coping management abilities.
With regard to mediation, SOC-R (total) was shown to be a significant mediator for some types of early-life adversity and chronic stress. While no significant mediations were observed with the abuse subscales (of early-life adversity), this is not entirely unexpected, given the low number of reported physical and sexual abuse in the general population sample. In line with previous general population studies in Germany [see Glaesmer (60)], experiences of neglect were more prevalent in the current study than experiences of abuse. However, in support of the second hypotheses (i.e., that SOC-R would significantly mediate the relationship between stress or adversity and indicators of psychological health and well-being), the results suggest that SOC-R was a significant mediator for general mental health and satisfaction with life, in relation to childhood physical neglect, childhood emotional neglect, and recent chronic stress. Although no previous research exists on the mediating role of SOC-R, findings are consistent with and expand upon the empirical research indicating a mediating influence with the original SOC (58, 61). The finding that SOC-R may explain the relationship between stress or adversity and psychological health and well-being also supports the assumption that SOC-R may be an integral mechanism underpinning the development of stress-related resilience.
In contrast to expectations, results did not support a steeling effect (i.e., that moderate levels of stress or adversity would be associated with stronger SOC-R, which in turn would lead to optimal psychological health and well-being). This is also inconsistent with recent research, which found significant curvilinear relationships between early-life adversity and quality of life outcomes, including general mental health (33). This may suggest that moderate levels of adversity are not “optimal” for the development of a strong SOC-R. However, another explanation may be due to differences in the adversity indicator, as the operationalization of early-life adversity in the study by Höltge et al. (33) differed to that in the current study. Nevertheless, before definitive conclusions can be drawn, further research is required to assess SOC-R and the steeling effect in larger, representative samples, with a greater range of adversity. Although a steeling effect was also not observed for chronic stress, this was consistent with previous research. Similar to the current study, research by Dooley et al. (62) found evidence of a linear relationship (i.e., as in the mediation analysis of the current study) but not a curvilinear (steeling) relationship between chronic stress and well-being. One explanation may be that prolonged stress experiences have often been shown to lead to increased sensitization to later stress rather than an increased resistance to later stress (4, 7, 28. Nevertheless, these findings highlight the importance of considering the type and severity of the stressor and adversity in the interplay between risk and resilience factors, and the resulting resilience or psychopathology (23, 27).
Limitations and Future Directions
Directions for future research can be identified by addressing some limitations of the current study. First, the retrospective nature of the study design may have led to recall bias, particularly in relation to the more distant experiences of early-life adversity (63). Similarly, the use of self-report assessments may also have led to biased reporting. To more accurately capture the influence of stress or adversity exposure, future research should use prospective, longitudinal designs, and include objective measures of stress or adversity, such as cortisol activity in response to stress-tests [e.g., 32]. Another limitation of this study was the low levels of adversity, particularly early-life adversity, in the current sample. For instance, in relation to early-life adversity, the large-scale, cross-national study by Kessler et al. (3) found that in a sample of n = 20,652 participants from high-income countries (from the same World Bank classification as Switzerland), 38.4% reported having experienced childhood adversity. Furthermore, in relation to childhood sexual abuse, a recent nationally-representative survey of N = 6,787 adolescents was conducted in Switzerland (64). Results showed that 40.2% (n = 1,282) of girls and 17.2% (n = 610) of boys reported having experienced at least one form of child sexual abuse. While the prevalence of adversities was generally lower in the current study, the highest reported adversities were emotional and physical neglect. However, this may be expected in a general population sample and the lower levels of adversity in the other categories may explain the lack of significant results. Related to this is self-selection bias, which may have influenced the composition of the sample, as individuals who experienced less adversity may be more likely to choose to participate in the study (65). Similarly, differences observed in SOC-R between participants and drop-outs may indicate a selection bias. Those who dropped out after T1 showed a significantly lower SOC-R score than those who completed both assessment points. It may be that individuals with a higher SOC-R are more likely to initially volunteer to take part in a study and to persevere with it at T2. To improve confidence in the findings, future research should replicate these analyses using different sampling techniques in both clinical and non-clinical samples with a greater range of SOC-R, as well as stressor and adversity severities.
Another limitation is the relatively small sample size, which may restrict the generalization of results to the general population. Nevertheless, research from large-scale studies on resilience support the finding that resilience can buffer the negative effects of stress or adversity. For instance, a recent study with a representative German community sample (N = 2,508) found that resilient coping was not only associated with lower levels of distress, but also buffered the negative effects of childhood adversities on distress (66). Comparable results were shown in the population-based, longitudinal study: the Virginia Adult Twin Studies of Psychiatric and Substance Use Disorders. Results from N = 7,463 participants showed that high levels of resilience at baseline buffered against the development of psychopathology, even in the presence of high levels of stressful life events (67). Similarly, a longitudinal Swedish cohort study of N = 237,879 participants found that participants with lower stress resilience to chronic stress showed an increased risk of stroke (68). However, SOC-R has yet to be assessed as an indicator of stress-related resilience aspects on such a large scale. Therefore, to increase confidence in the results, it is recommended that future research assess the buffering effect of SOC-R with a large sample size. Furthermore, another sample-related limitation is the broad age range (50–92 years) used in the current study, which may have masked specific age group effects or patterns in SOC-R (69). Future studies could also examine SOC-R across different age groups.
In addition, studies should investigate the different types of adversity (e.g., acute versus chronic stress, cumulative lifetime adversity, event-specific adversities), which may influence the strength of SOC-R and in turn, its impact on health and well-being (16, 23). Finally, the current study investigated the role of SOC-R in steeling processes using a simple mediation model of curvilinear associations. However, SOC-R is assumed to promote the development of stress-related resilience through the appropriate use of resources (16, 22). Future studies may therefore benefit from including resources into the model with SOC-R, such as in the form of moderated mediation (29). This is supported by a review of studies on resilience in stress-related disorders (70). Thirteen studies were included which investigated predictors of resilient outcomes following stress exposure. Results indicated that resilience is a dynamic process, involving the interaction of multiple separate resilience-related factors (70). Similarly, in relation to resilience in older adults, research has shown that that a combination of mental, social, and physical factors is important for resilience. In particular, a recent review identified optimism, adaptive coping, positive emotions, social support, and social connectedness as important factors in the maintenance of high levels of resilience in older adulthood (71). In relation to future moderation and mediation analyses with SOC-R, as indication for which resources to include, studies can also draw on previous research by Mc Gee et al. (23), which examined convergent and discriminant correlations between SOC-R and related psychological concepts. Similar to the recommendations by MacLeod et al. (71), results showed moderate to strong correlations between SOC-R and a number of resources, including general self-efficacy, social support, and optimism.
Conclusion
By investigating the moderating and mediating roles of SOC-R, the current study provides a meaningful contribution to the research on stress-related resilience. It addresses a gap in the literature, as it is the first study to examine the mediating role of SOC-R in the relationship between stress or adversity and health and well-being. It also builds on previous studies by assessing chronic stress, as well as early-life adversity. While evidence of a steeling effect was not observed, the results suggest that SOC-R may still be a crucial underlying mechanism in the development of resilience. In conclusion, the findings suggest that in overcoming stress or adversity, an individual's SOC-R (and the strength of their SOC-R) plays an important role in fostering resilience and in turn, psychological health and well-being.
Author Contributions
All authors made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; and final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This work was supported by the Swiss Government Excellence Scholarship (ESKAS-Nr. 2016.0109) which funded the first author's (SM) position.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling Editor declared a shared affiliation, though no other collaboration, with the authors.
Acknowledgments
During the work on their dissertations, SM and JH were pre-doctoral fellows of LIFE (International Max Planck Research School on the Life Course; participating institutions: MPI for Human Development, Humboldt-Universität zu Berlin, Freie Universität Berlin, University of Michigan, University of Virginia, University of Zurich). This study was supported by the University Research Priority Program (URPP) Dynamics of Healthy Aging at the University of Zurich, and the Jacobs Foundation.
References
1. Krammer S, Kleim B, Simmen-Janevska K, Maercker A. Childhood trauma and complex posttraumatic stress disorder symptoms in older adults: a study of direct effects and social-interpersonal factors as potential mediators. J Dissoc. (2016) 17:593–607. doi: 10.1080/15299732.2014.991861
2. McCrory C, Dooley C, Layte R, Kenny RA. The lasting legacy of childhood adversity for disease risk in later life. Health Psychol. (2015) 34:687–96. doi: 10.1037/hea0000147
3. Kessler RC, McLaughlin KA, Greif Green J, Gruber MJ, Sampson NA, Zaslavsky AM, et al. Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. Br J Psychiatry (2010) 197:378–85. doi: 10.1192/bjp.bp.110.080499
4. Juster R-P, McEwen BS, Lupien SJ. Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci Biobehav Rev. (2010) 35:2–16. doi: 10.1016/j.neubiorev.2009.10.002
5. McEwen BS. Stressed or stressed out: what is the difference? J Psychiatry Neurosci. (2005) 30:315–8.
6. Davis MT, Holmes SE, Pietrzak RH, Esterlis I. Neurobiology of chronic stress-related psychiatric disorders: evidence from molecular imaging studies. Chronic Stress (2017) 1:1–21. doi: 10.1177/2470547017710916
7. McEwen BS. Protection and damage from acute and chronic stress: Allostasis and allostatic overload and relevance to the pathophysiology of psychiatric disorders. Ann NY Acad Sci. (2004) 1032:1–7. doi: 10.1196/annals.1314.001
8. Huber M, Knottnerus JA, Green L, van der Horst H, Jadad AR, Kromhout D, Smid H. How should we define health? Br Med J. (2011) 343:d4163. doi: 10.1136/bmj.d4163
9. Maercker A, Gäbler I, O'Neill J, Schützwohl M, Müller M. Long-term trajectories of PTSD or resilience in former East German political prisoners. Torture (2013) 23:15–27. doi: 10.5167uzh-71813
10. Bonanno GA, Westphal M, Mancini AD. Resilience to loss and potential trauma. Ann Rev Clin Psychol. (2011) 7:511–35. doi: 10.1146/annurev-clinpsy-032210-104526
11. Sharpley CF, Christie DRH, Bitsika V, Agnew LL, Andronicos NM, McMillan ME, et al. Limitations in the inverse association between psychological resilience and depression in prostate cancer patients experiencing chronic physiological stress. Psycho-Oncology (2017) 27:223–8. doi: 10.1002/pon.4496
12. Maercker A, Simmen-Janevska K. Psychische Folgestörungen der Verdingung im Alter [Psychological sequelae of indentured child labour in old age]. In: Furrer M, Heininger K, Huonker T, Jenzer S, Praz A, editors. Fremdplatzierung von Kindern und Jugendlichen in der Schweiz 1850-1980 [Placement of children and adolescents in Switzerland 1850-1980] Basel: Schwabe (2014). pp. 373–85.
13. Krammer S, Simmen-Janevska K, Maercker A. In Richtung “Komplexe PTBS”: Die deutsche Version des Trauma Symptom Inventory (TSI) zur Erfassung komplexer Traumafolgen [Towards ‘Complex PTSD': German translation of the Trauma Symptom Inventory (TSI) for the assessment of complex trauma sequelae]. Psychother Psychos Med Psychol. (2013) 63:318–26. doi: 10.1055/s-0032-1327752
14. Kuhlman KR, Maercker A, Bachem R, Simmen-Janevska K, Burri A. Developmental and contextual factors in the role of severe childhood trauma in geriatric depression: the sample case of former indentured child labourers. Child Abuse Negl. (2013) 37:969–78. doi: 10.1016/j.chiabu.2013.04.013
15. Maercker A, Hilpert P, Burri A. Childhood trauma and resilience in old age: applying a context model of resilience to a sample of former indentured child laborers. Aging Mental Health (2016) 20:616–26. doi: 10.1080/13607863.2015.1033677
16. Bachem R, Maercker A. Development and psychometric evaluation of a revised sense of coherence scale. EurJ Psychol Assess. (2016) 34:206–15. doi: 10.1027/1015-5759/a000323
17. Grødal K, Innstrand ST, Bauer GF, Haugan G, Rannestad T, André B. Validation of the Norwegian version of the work-related sense of coherence scale. Scand J Public Health. (2017). doi: 10.1177/1403494817725466. [Epub ahead of print].
18. Gruszczynska E. What is measured by the orientation to life questionnaire? Construct validity of the instrument for the Sense of Coherence measurement. Polish Psychol. Bull. (2006) 37:74–83.
19. Saravia JC, Iberico C, Yearwood K. Validation of sense of coherence (SOC) 13-item scale in a Peruvian sample. J Behav Health Soc Issues (2015) 6:35–44. doi: 10.5460/jbhsi.v6.2.43847
20. Antonovsky A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well. San Francisco, CA: Jossey-Bass (1987).
21. Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med. (1993) 36:725–33. doi: 10.1016/0277-9536(93)90033-Z
22. Antonovsky A. The salutogenic model as a theory to guide health promotion. Health Promot Int. (1996) 11:11–8. doi: 10.1093/heapro/11.1.11
23. Mc Gee SL, Höltge J, Maercker A, Thoma MV. Evaluation of the revised Sense of Coherence scale in a sample of older adults: a means to assess resilience aspects. Aging Mental Health (2017). doi: 10.1080/13607863.2017.1364348. [Epub ahead of print].
24. Xiu D, Mc Gee SL, Maercker A. Sense of coherence and posttraumatic growth: The moderating role of value orientation in Chinese and Swiss bereaved parents. J Loss Trauma (2018) 23:259–70. doi: 10.1080/15325024.2018.1436120
25. Gana K. Is sense of coherence a mediator between adversity and psychological well-being in adults? Stress Health (2001) 17:77–83. doi: 10.1002/smi.882
26. Rohani C, Abedi H-A, Sundberg K, Langius-Eklöf A. Sense of coherence as a mediator of health-related quality of life dimensions in patients with breast cancer: a longitudinal study with prospective design. Health Qual Life Outcomes (2015) 13:195. doi: 10.1186/s12955-015-0392-4
27. Fossion P, Leys C, Kempenaers C, Braun S, Verbanck P, Linkowski P. Disentangling sense of coherence and resilience in case of multiple traumas. J Affect Disord. (2014) 160:21–6. doi: 10.1016/j.jad.2014.02.029
28. Rutter M. Resilience as a dynamic concept. Dev Psychopathol. (2012) 24:335–44. doi: 10.1017/S0954579412000028
29. Liu RT. A developmentally informed perspective on the relation between stress and psychopathology: when the problem with stress is that there is not enough. J Abnorm Psychol. (2015) 124:80–92. doi: 10.1037/abn0000043
30. Edge MD, Ramel W, Drabant EM, Kuo JR, Parker KJ, Gross JJ. For better or worse? Stress inoculation effects for implicit but not explicit anxiety. Depress Anxiety (2009) 26:831–7. doi: 10.1002/da.20592
31. Seery MD, Leo RJ, Lupien SP, Kondrak CL, Almonte JL. An upside to adversity? Moderate cumulative lifetime adversity is associated with resilient responses in the face of controlled stressors. Psychol Sci. (2013) 24:1181–9. doi: 10.1177/0956797612469210
32. Hagan MJ, Roubinov DS, Purdom Marreiro CL, Luecken LJ. Childhood interparental conflict and HPA axis activity in young adulthood: examining nonlinear relations. Dev Psychobiol. (2014) 56:871–80. doi: 10.1002/dev.21157
33. Höltge J, Mc Gee SL, Thoma MV. The curvilinear relationship of early-life adversity and successful aging: the mediating role of mental health. Aging Mental Health (2018). doi: 10.1080/13607863.2018.1433635. [Epub ahead of print].
34. Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods (2007) 39:175–91. doi: 10.3758/BF03193146
35. Fritz MS, MacKinnon DP. Required sample size to detect the mediated effect. Psychol Sci. (2007) 18:233–9. doi: 10.1111/j.1467-9280.2007.01882.x
36. Maxwell SE. Sample size and multiple regression analysis. Psychol Methods (2000) 5:434–58. doi: 10.1037/1082-989X.5.4.434
37. Bernstein D, Fink L. Childhood Trauma Questionnaire: A Retrospective Self-Report. San Antonio, TX: Psychological Corp. (1998).
38. Klinitzke G, Romppel M, Häuser W, Brähler E, Glaesmer H. The German Version of the Childhood Trauma Questionnaire (CTQ) - psychometric characteristics in a representative sample of the general population. Psychother Psychos Med Psychol. (2011) 62:47–51. doi: 10.1055/s-0031-1295495
39. Wingenfeld K, Spitzer C, Mensebach C, Grabe HJ, Hill A, Gast U, et al. Die deutsche Version des Childhood Trauma Questionnaire (CTQ): Erste Befunde zu den psychometrischen Kennwerten [The German version of the Childhood Trauma Questionnaire (CTQ): First findings on the psychometric characteristics]. Psychother Psychos Med Psychol. (2010) 60:442–50. doi: 10.1055/s-0030-1247564
40. Schulz P, Schlotz W. Trierer Inventar zur Erfassung von chronischem Streß (TICS): Skalenkonstruktion, teststatistische Überprüfung und Validierung der Skala Arbeitsüberlastung [The Trier Inventory for the Assessment of Chronic Stress (TICS): Scale construction, statistical testing, and validation of the scale work overload]. Diagnostica (1999) 45:8–19. doi: 10.1026/0012-1924.45.1.8
41. Schulz P, Schlotz W, Becker P. (2004). TICS - Trierer Inventar zum Chronischen Stress (Screening-Skala zum Chronischen Stress (SSCS); Trierer Inventar zur Erfassung von chronischem Stress) [TICS - Trierer Inventory for Chronic Stress (Screening Scale for Chronic Stress (SSCS); Trierer Inventory for the Detection of Chronic Stress]. PSYNDEX Tests Review. Göttingen: Hogrefe.
42. Bullinger M, Kirchberger I, Ware J. Der deutsche SF-36 Health Survey Übersetzung und psychometrische Testung eines krankheitsübergreifenden Instruments zur Erfassung der gesundheitsbezogenen Lebensqualität. [The German SF-36 health survey translation and psychometric testing of a generic instrument for the assessment of health-related quality of life]. J Public Health (1995) 3:21–36. doi: 10.1007/BF02959944
43. Morfeld M, Bullinger M, Nantke J, Brähler E. Die Version 2.0 des SF-36 Health Survey - Ergebnisse einer bevölkerungsrepräsentativen Studie [The version 2.0 of the SF-36 health survey: results of a population-representative study]. Sozial Pravent. (2005) 50:292–300. doi: 10.1007/s00038-005-4090-6
44. Ellert U, Kurth B-M. Methodische Betrachtungen zu den Summenscores des SF-36 anhand der erwachsenen bundesdeutschen Bevölkerung [Methodological views on the SF-36 summary scores based on the adult German population]. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz (2004) 47:1027–32. doi: 10.1007/s00103-004-0933-1
45. Ellert U, Kurth B-M. Gesundheitsbezogene Lebensqualität bei Erwachsenen in Deutschland [Health related quality of life in adults in Germany: results of the German Health Interview and Examination Survey for Adults (DEGS1)]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz (2013) 56:643–9. doi: 10.1007/s00103-013-1700-y
46. Schumacher J. SWLS – Satisfaction with Life Scale. In: J. Schumacher A, Klaiberg E, Braehler editors. Diagnostische Verfahren zu Lebensqualität und Wohlbefinden [Diagnostic Procedures for Quality of Life and Well-Being] Goettingen: Hogrefe (2003). pp. 305–9.
47. Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Person Assess. (1985) 49:71–5. doi: 10.1207/s15327752jpa4901_13
48. Glaesmer H, Grande G, Brähler E, Roth M. The German version of the satisfaction with life scale – psychometric properties and population based norms. Eur J Psychol Assess. (2011) 27:127–32. doi: 10.1027/1015-5759/a000058
49. Unipark and QuestBack. Unipark EFS Survey Software [Computer software]. Germany: Globalpark AG, Hürth. Available online at: http://www.unipark.com/de/
50. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. 2nd ed. New York, NY: The Guildford Press (2018).
51. IBM Corp. (2017). IBM SPSS Statistics for Macintosh, Version 25.0. Released 2017. Armonk NY: IBM Corp.
52. Dempster AP, Laird NM, Rubin DB. Maximum likelihood from incomplete data via the EM algorithm. J R Stat Soc B (1977) 39:1–38.
53. Little RJA. A test of missing completely at random for multivariate data with missing values. J Am Stat Assoc. (1988) 83:1198–202. doi: 10.2307/2290157
54. Collins LM. Analysis of longitudinal data: The integration of theoretical model temporal design and statistical model. Ann Rev Psychol. (2006) 57:505–28. doi: 10.1146/annurev.psych.57.102904.190146
55. Johnson PO, Neyman J. Tests of certain linear hypotheses and their application to some educational problems. Stat Res Mem. (1936) 1:57–93.
56. Cohen J, Cohen P, West SG, Aiken LS. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences. New York, NY: Routledge (2013).
57. Carpentieri JD, Elliott J, Brett CE, Deary IJ. Adapting to aging: older people talk about their use of selection, optimization, and compensation to maximize well-being in the context of physical decline. J Gerontol. (2017) 72:351–61. doi: 10.1093/geronb/gbw132
58. Eriksson M, Lindström B. Antonovsky's sense of coherence scale and the relation with health: A systematic review. J Epidemiol Commun Health (2006) 60:376–81. doi: 10.1136/jech.2005.041616
59. Gison A, Rizza F, Bonassi S, Dall'Armi V, Lisi S, Giaquinto S. (2014). The sense-of-coherence predicts health-related quality of life and emotional distress but not disability in Parkinson's disease. BMC Neurol. 14:193. doi: 10.1186/s12883-014-0193-0
60. Glaesmer H. Assessing childhood maltreatment on the population level in Germany: findings and methodological challenges. Child Adolesc Psychiatry Mental Health (2016) 10:15. doi: 10.1186/s13034-016-0104-9
61. Eriksson M, Lindström B. Antonovsky's sense of coherence scale and its relation with quality of life: a systematic review. J Epidemiol Commun Health (2007) 61:938–44. doi: 10.1136/jech.2006.056028
62. Dooley LN, Slavich GM, Moreno PI, Bower JE. Strength through adversity: moderate lifetime stress exposure is associated with psychological resilience in breast cancer survivors. Stress Health (2017) 33:549–57. doi: 10.1002/smi.2739
63. Church C, Andreassen OA, Lorentzen S, Melle I, Aas M. Childhood trauma and minimization/denial in people with and without a severe mental disorder. Front Psychol. (2017) 8:1276. doi: 10.3389/fpsyg.2017.01276
64. Mohler-Kuo M, Landolt MA, Maier T, Meidert U, Schönbucher V, Schnyder U. Child sexual abuse revisited: A population-based cross-sectional study among Swiss adolescents. J Adolesc Health (2014) 54:304–11.e1. doi: 10.1016/j.jadohealth.2013.08.020
65. Frissen A, Lieverse R, Drukker M, van Winkel R, Delespaul P, GROUP Investigators Childhood trauma and childhood urbanicity in relation to psychotic disorder. Soc Psychiatry Psychiatr Epidemiol. (2015) 50:1481–8. doi: 10.1007/s00127-015-1049-7
66. Beutel ME, Tibubos AN, Klein EM, Schmutzer G, Reiner I, Kocalevent R-D, et al. Childhood adversities and distress – The role of resilience in a representative sample. PLoS ONE (2017) 12:e0173826. doi: 10.1371/journal.pone.0173826
67. Sheerin CM, Lind MJ, Brown EA, Gardner CO, Kendler KS, Amstadter AB. The impact of resilience and subsequent stressful life events on MDD and GAD. Depress Anxiety (2018) 35:140–7. doi: 10.1002/da.22700
68. Bergh C, Udumyan R, Fall K, Nilsagård Y, Appelros P, Montgomery S. Stress resilience in male adolescents and subsequent stroke risk: cohort study. J Neurol Neurosurg Psychiatry (2014) 85:1331–6. doi: 10.1136/jnnp-2013-307485
70. Kalisch R, Baker DG, Basten U, Boks MP, Bonanno GA, Brummelman E, et al. The resilience framework as a strategy to combat stress-related disorders. Nat Hum Behav. (2017) 1:784–90. doi: 10.1038/s41562-017-0200-8
Keywords: sense of coherence-revised, stress-related resilience, resilience mechanisms, psychological health, mediating factor
Citation: Mc Gee SL, Höltge J, Maercker A and Thoma MV (2018) Sense of Coherence and Stress-Related Resilience: Investigating the Mediating and Moderating Mechanisms in the Development of Resilience Following Stress or Adversity. Front. Psychiatry 9:378. doi: 10.3389/fpsyt.2018.00378
Received: 24 May 2018; Accepted: 30 July 2018;
Published: 21 August 2018.
Edited by:
Ulrich Schnyder, Universität Zürich, SwitzerlandReviewed by:
Tom Sensky, Imperial College London, United KingdomRonny Westerman, Bundesinstitut für Bevölkerungsforschung, Germany
Copyright © 2018 Mc Gee, Höltge, Maercker and Thoma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shauna L. Mc Gee, cy5tY2dlZUBwc3ljaG9sb2dpZS51emguY2g=