
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol., 06 August 2019
Sec. Exercise Physiology
Volume 10 - 2019 | https://doi.org/10.3389/fphys.2019.01013
This article is part of the Research TopicChildren's Exercise PhysiologyView all 29 articles
 Braulio Henrique Magnani Branco1,2*
Braulio Henrique Magnani Branco1,2* Débora Valladares1,2Fabiano Mendes de Oliveira2Isabelle Zanquetta Carvalho2Déborah Cristina Marques2Andressa Alves Coelho2Leonardo Pestillo de Oliveira2Sônia Maria Marques Gomes Bertolini1,2
Débora Valladares1,2Fabiano Mendes de Oliveira2Isabelle Zanquetta Carvalho2Déborah Cristina Marques2Andressa Alves Coelho2Leonardo Pestillo de Oliveira2Sônia Maria Marques Gomes Bertolini1,2The main objective of this study was to investigate the effects of the order of physical exercises on body composition, physical fitness, and cardiometabolic risk in adolescents participating in an interdisciplinary program focusing on the treatment of obesity. The final 12-week analyses involved 33 female adolescents who were split into two groups of concurrent training (CT): resistance plus aerobic training and aerobic plus resistance training, with equalization performed in all physical exercises. The only difference between the two groups was the order in which the exercises were performed. The results showed reductions in fat mass, body fat, and waist circumference, as well as increases in musculoskeletal mass and resting metabolic rate (p < 0.05) following the multiprofessional intervention period. However, no significant differences were observed in regard to body mass, body mass index, neck circumference, or arm circumference (p > 0.05). Maximal isometric strength and maximal oxygen consumption showed significant increases after the intervention period (p < 0.05). There were reductions in insulin, HOMA-IR, total cholesterol, triglycerides, and low-density lipoproteins (p < 0.05), and an interaction within the resistance plus aerobic training group showed lower values for triglycerides when compared to itself (p = 0.002). No difference was found in fasting glycemia for either group (p > 0.05). It is worth noting that the equalization training variables presented no differences between the two groups (p > 0.05). Based on these results, both CT methods were found to be effective in promoting health parameters in overweight and obese female adolescents, and triglyceride values decreased more in the resistance plus aerobic group. Future studies with larger samples and feeding control should be conducted to confirm or refute our findings.
Obesity is substantially associated with increased caloric intake, low levels of physical activity, and reduced energy expenditure (Blüher, 2019). The literature has indicated that, by 2015, more than 100 million children and adolescents worldwide were classified as obese in both developed and developing countries (Lee and Yoon, 2018). Furthermore, obesity in adolescence exponentially increases the risks of developing other diseases, including diabetes mellitus and hypertension and other cardiovascular diseases in adulthood (Ho et al., 2019).
Currently, the scientific literature still lacks controlled studies seeking to identify the effects of physical exercise (PE) intensity on weight loss in adolescents since most studies present a low volume of interventions (Stoner et al., 2019). Therefore, consensus among researchers regarding the most efficient physical training method for reducing body fat (BF) in adolescents is lacking. Among the recommended strategies, multiprofessional intervention has been noted for the treatment of obesity (Branco et al., 2018).
In addition, Petridou et al. (2019) indicated that resistance exercises (RE) are relevant for the treatment of obesity due to increased resting metabolic rate (RMR) and fat-free mass, which consequently increase the day-to-day energy expenditure. The same authors suggested that aerobic exercises (AE) should be incorporated in weight-loss programs since, depending on volume and intensity, the energy expenditure during the session may be greater than that in resistance training (RT), especially when the resting intervals are very long.
Recently, Branco et al. (2018) compared the effects of two different concurrent training methods on body composition, physical fitness, and cardiometabolic risk of obese adolescents. The two physical-training protocols were similar in volume, intensity, and types of exercises. The only difference was the means by which the exercises were performed, i.e., one group used body weight and the other group used machines, and when possible, the exercises were equalized by the primary muscle groups involved in achieving the activity. The results of all analyzed variables were similar since the volume, intensity, and exercises performed were equalized.
Consistent with Kang and Ratamess (2014) regarding the choice of the protocol used to conduct concurrent training, AE or RE at the beginning or end of the session will depend on the first objective of physical training for athletes of different modalities. However, this condition is recommended for athletes but not for sedentary individuals or for the treatment of certain chronic diseases. The same authors noted that the choice of the order of PE within the same training session can be organized according to the specificity of the modality, i.e., for athletes with aerobic resistance modalities, performing aerobic training first to increase the quality of their training is recommended. However, for athletes seeking muscular hypertrophy, it is recommended that RE be performed at the beginning of the training session for the same reason mentioned above. The World Health Organization [WHO], (2010) suggested that children and adolescents need to improve cardiorespiratory fitness and muscular endurance and strength. Thus, a strategy that may be used is concurrent training (Coffey and Hawley, 2017). Furthermore, Vilaça et al. (2011) emphasized that a combination of AE and RE (regardless of order) is beneficial for reducing BF and increasing energy expenditure during and after PE sessions.
To the best of the author’s knowledge, the chronic physiological and metabolic responses under the order of concurrent training in obese sedentary adolescents are unknown. Regardless of the order of the execution of PE, there is no consensus or indication regarding which model/order of PE should be followed in order to enhance improvement in components related to physical fitness in terms of health. Considering these aspects, the identification of physiological and metabolic responses during respective intervention models could direct the interventions and even prevent paradigms or concepts based on the common sense of health professionals, especially those involved in prescribing PE. Therefore, the aim of the present study was to investigate the effects of the order of physical exercises on body composition, physical fitness, and cardiometabolic risk in female adolescents participating in an interdisciplinary program focusing on the treatment of obesity. Regarding the hypothesis, it is believed that the responses observed in the different parameters analyzed will be similar since only the order of the exercises was changed.
A total of 44 female adolescents were recruited according to the following established inclusion criteria: (1) age between 13 and 17 years; (2) overweight or obesity according to the cutoff ranges established by Cole and Lobstein (2012); and (3) availability to participate in multiprofessional interventions 3× per week during the evening for a period of 12 weeks. The exclusion criteria were as follows: (1) participating in sports practices systematized outside of school, (2) orthopedic, cardiovascular, or cognitive deficits that impede practicing PE, (3) some type of restrictive diet, i.e., low-carb, low-fat or hypocaloric, (4) the use of a psychotropic or appetite-regulating medicine, and (5) completion of less than 75% of the multiprofessional interventions during the 12-week intervention. It is emphasized that the adolescents were encouraged to be more physically active during the intervention (outside the university setting). In relation to the variables, a sample size with nine participants in each group intervention was enough to detect eventual changes in dependent variables, with standard deviation smaller when compared to previous study, with 80% confidence (Branco et al., 2018). The details of the process are provided in Figure 1, which depicts the flowchart for the present study.
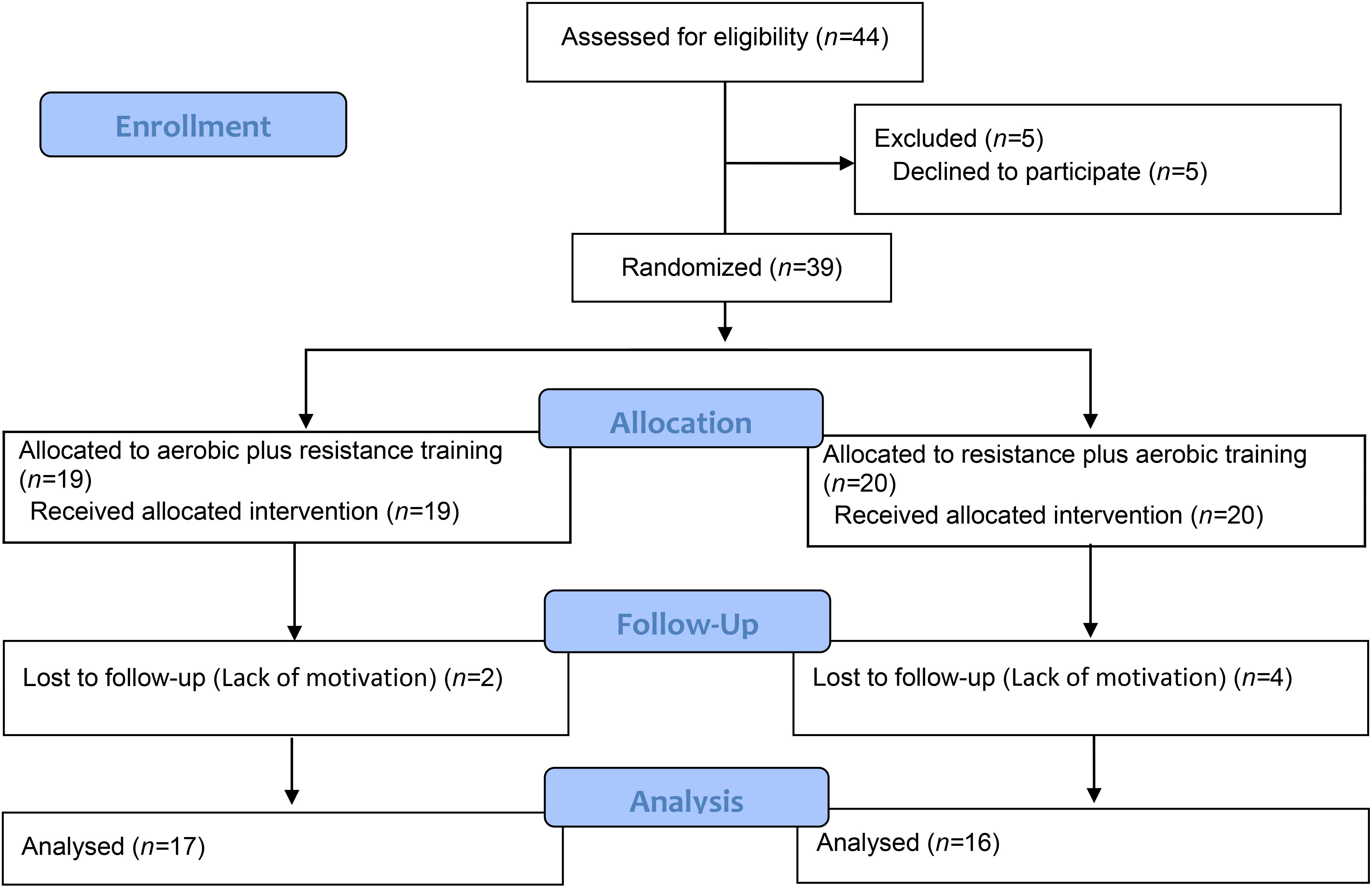
Figure 1. The flowchart of the present study.
This study was approved by the Committee for Ethics in Research of the University Center of Maringá (UniCesumar) through the opinion n° 2,505,200/2018. The research followed all recommendations proposed by resolution 466/2012 of the Ministry of Health of the Brazilian Government and the Declaration of Helsinki. All parents or guardians of the adolescents were informed in detail about the purposes of the study and subsequently signed an informed consent form. In addition, the adolescents signed a consent term agreeing to participate.
This study adopted an experimental, longitudinal, parallel-group, and repeated-measures design. Previously, the adolescents were randomly allocated to one of the following two experimental groups: G1 = aerobic plus resistance group or G2 = resistance plus aerobic group. The only distinction between the groups was the order of performing the activities, i.e., G1 performed AE followed by RE, whereas G2 performed the activities in the inverse order, i.e., RE followed by AE. The details of the aerobic and resistance exercises in regard of volume and intensity are presented in the discussion below. The participants performed the interventions three times a week for 12 weeks guided by a team of professionals in physical education, nutrition, and psychology. PE was performed 3× per week divided into training A and B, as theoretical and practical classes related to nutrition were conducted 2× per week, and cognitive-behavioral therapy was provided 1× per week over the course of the 12-week intervention. On the first day of evaluations, the adolescents underwent a medical consultation involving the following: (a) anamnesis, (b) measurement of resting blood pressure, (c) pulmonary and cardiac auscultation, (d) completion of the International Physical Activity Questionnaire (IPAQ), and (e) release for venous blood collection. On the second day, the following were performed: (a) venous blood collection following ∼ 12 h of fasting, (b) body composition assessment, (c) anthropometry, and (d) explanation and collection of food records. On the third day, physical tests were performed in the following order: (a) maximal isometric handgrip test (MIHT), (b) maximal isometric lumbar-traction strength (MILTS), (c) maximal isometric lower-body strength (MILBT) and (d) aerobic fitness. The 3 days of evaluations were separated by a 48-h interval. Considering that the interventions were performed on Mondays, Wednesdays, and Fridays, the evaluations began on the same days, and re-evaluations were conducted after the weekend. The girls rested for 2 days, and the process followed the same days of evaluation in the beginning of this study.
The training sessions were divided into two mesocycles performed in circuit form with series A and B. The two series were performed alternately to promote the physiological recovery of the muscle groups previously worked. The training schedule was divided into two mesocycles of 6 weeks duration each. Regarding the exercises, we chose to perform PE without repetition counting and to control the exercises by timing the activities. During the first mesocycle, the effort: pause ratio was 30″ by 30″, while for the second mesocycle, the effort: pause ratio was 40″ by 20″ using a 1:1 ratio between the concentric and eccentric phases. In addition, before the session, the adolescents performed a 10-min warm-up as follows: light walking and stretching of the main muscle groups (with low muscle tension). To periodize the training, promote anatomical adaptation, and reduce any lesions, the intensity of the sessions was controlled by the Borg (1982), which includes values of 6 arbitrary units (a.u.) up to 20 a.u., i.e., from very easy to exhausting. Table 1 shows the AE performed by both experimental groups.
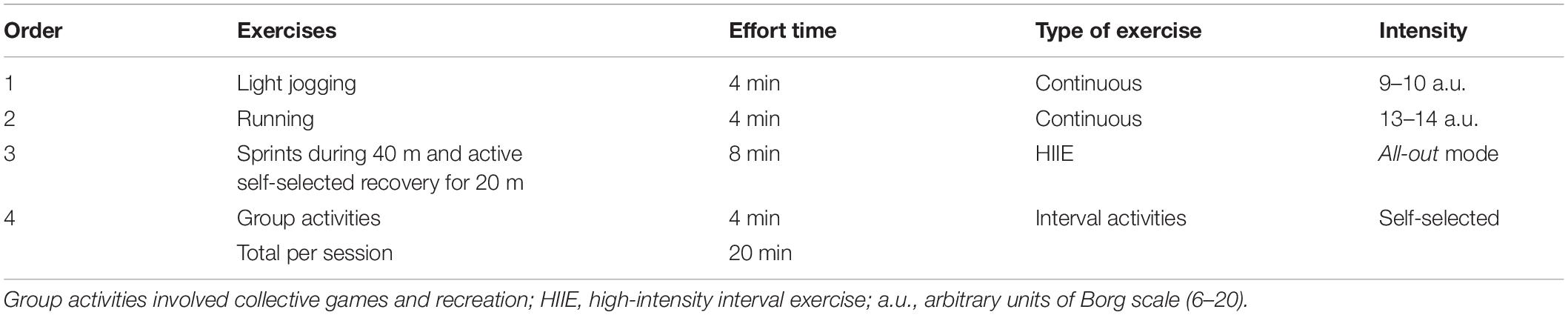
Table 1. Systematization of aerobic training during 12 weeks of intervention.
Table 2 shows the intensity of the resistance efforts during the 12-week intervention.
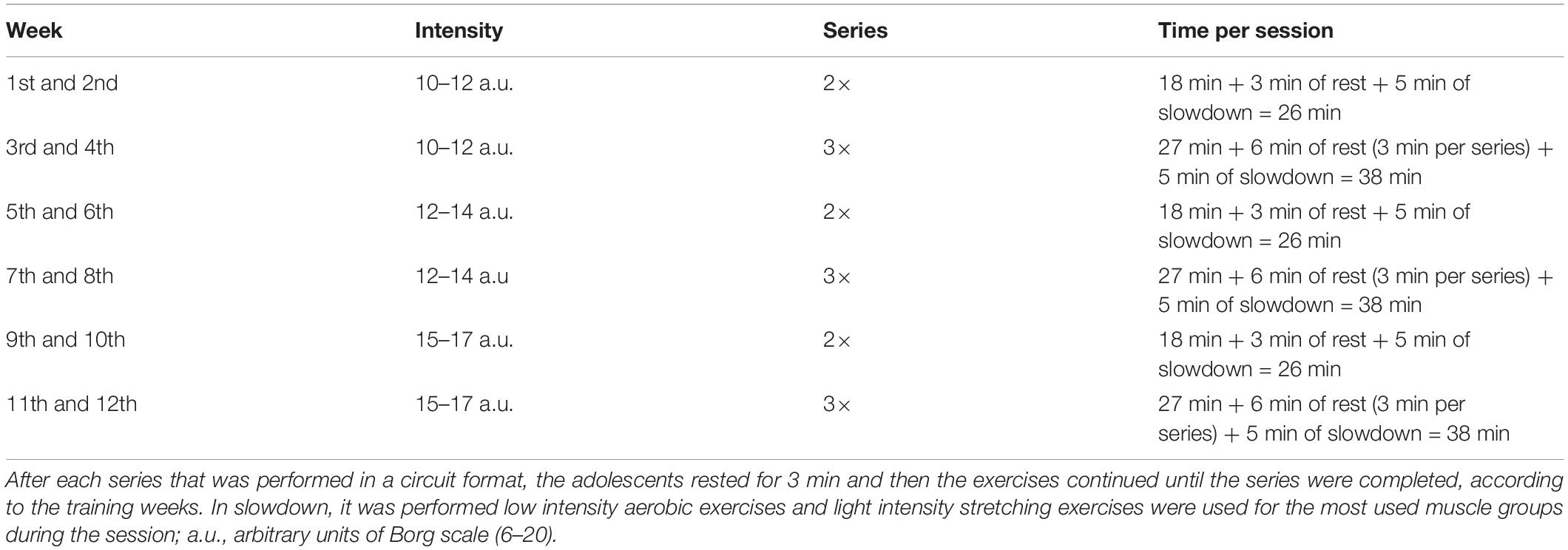
Table 2. Intensity of the resisted efforts during the 12 weeks of intervention.
Table 3 presents the training program groups A and B performed during the first and second RT mesocycles.
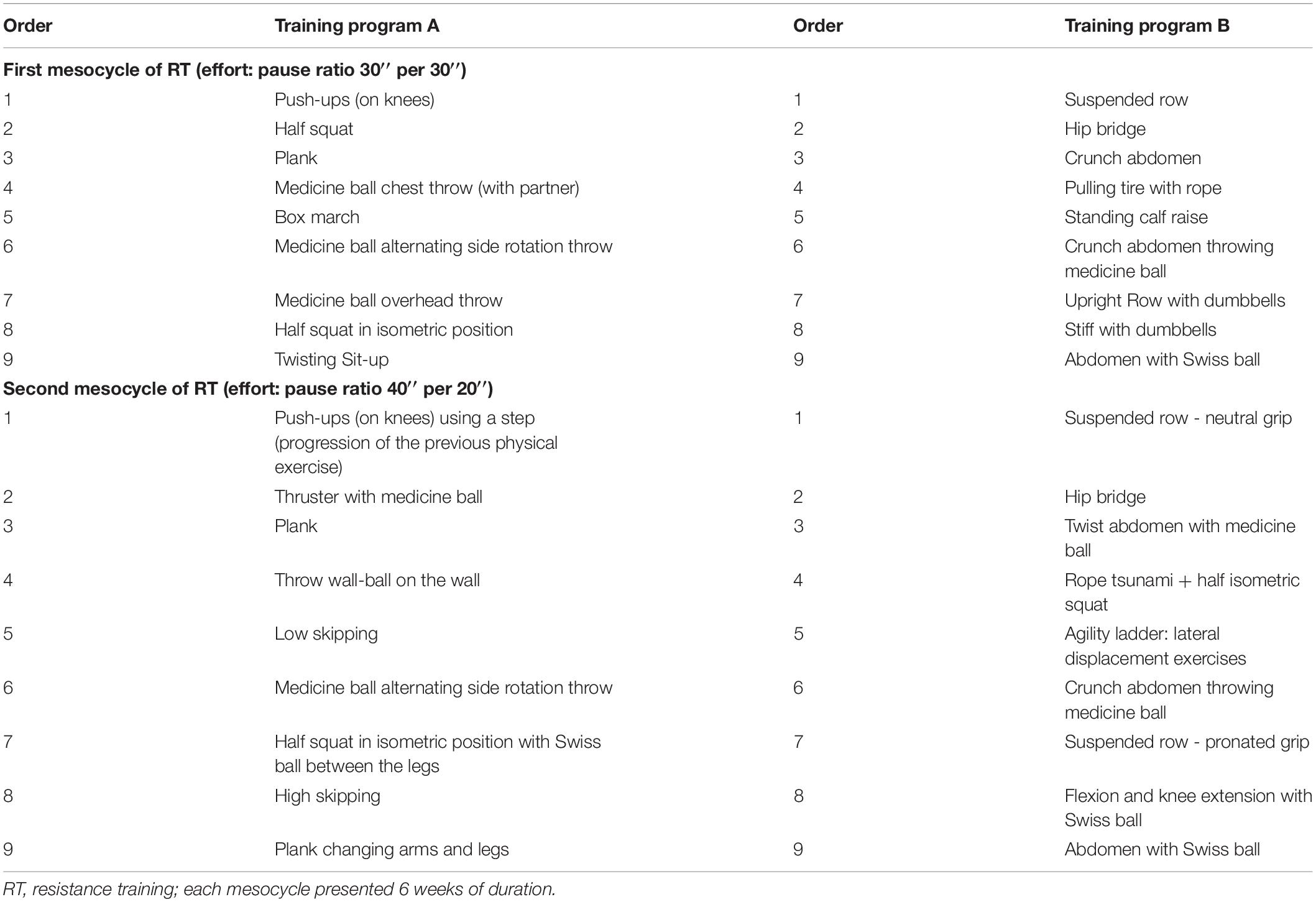
Table 3. First and second mesocycle of resistance training of both experimental groups.
To monitor the physical training sessions, several non-invasive and practical instruments were used by the physical trainer. Prior to each training session, the rating of the perceived recovery (RPR) scale as proposed by Laurent et al. (2011), the rating of perceived exertion (RPE session) as proposed by Foster et al. (2001), and the internal training load (ITL) were assessed according to the considerations proposed by Nakamura et al. (2010). The RPR indicates the recovery status and is used before each training session. The scale comprises numerical values ranging from 0 a.u. (very poor recovery/extremely tired) to 10 a.u. (very good recovery/extremely well-disposed). The RPE session was applied 30 min after the end of the training sessions. This scale comprises values ranging from 0 a.u. (extremely light effort) to 10 a.u. (extremely heavy stress). The ITL was calculated by multiplying the value of the RPE by the duration of the training session in minutes. The girls were familiarized with the scales before and during interventions. The scales were administered to the girls, and explanations were provided during the theoretical classes and before the PE sessions.
The IPAQ questionnaire adapted for adolescents was used to identify the levels of physical activity before and after the interdisciplinary interventions and to determine whether the adolescents had already engaged in other moderate/intense physical activities before starting the program (Guedes et al., 2005).
The nutritional interventions aimed to guide the adolescents in nutritional aspects such as: (a) introduction to healthy eating: food manufacturers, regulators, energy, and the food pyramid, (b) frequency and portioning of food, (c) soluble and insoluble fibers, (d) the importance of fiber consumption, (e) a list of food replacements, according to the food groups, (f) pre- and post-physical activity feeding, (g) minimally processed, processed, and ultra-processed foods, (h) amounts of sugar, salt, and fat in foods, (i) how to read and interpret food labels, (j) diet and “light” foods, (k) eating disorders, (l) the dangers of “fad diets”, and (m) ingesting food for health and quality of life using food re-education as an instrument. Those responsible were advised to note, in specific forms, all foods and beverages consumed throughout the day, and also to record the size of portions consumed; the name of the preparations, their ingredients, and the method preparation. They were also instructed to note details such as the addition of salt, sugar, oil, sauces, etc., and whether the food or drink consumed was regular, diet, or light. For the best estimation of the portion size, they used home measurements (Slater et al., 2002). The classes, which were conducted by means of theoretical activities and practical dialogues, lasted approximately 1 h and took place 2× per week. A 3-day food recall was applied on two non-consecutive days of the week and on 1 day at the end of the week. All data were tabulated using the program Avanutri (Avanutri Equipamentos de Avaliação Ltda, Três Rios, Brazil). Another point that needs to be highlighted was the absence of feeding control. It was suggested that the teenagers change their dietary habits according to theoretical and practical classes on nutrition and psychological interventions. However, a control of percentages of macronutrient ingestion or the quality of the food consumed was not performed during this study. Finally, the kilocalories/day ingested by the adolescents were calculated, and the values pre- and post-intervention were compared. The intervention model and food-recall analysis procedures were the same as those performed in the study conducted by Branco et al. (2018).
The primary themes of the psychological intervention were cognitive and behavioral strategies used to improve the quality of food consumption among the adolescents, including self-monitoring, control of anxiety, negative feelings, and health education. The activities also aimed to reduce negative emotions regarding the participants’ relationships with food consumption and strategies used to improve the assessment of body self-image. Psychological intervention was divided into four large groups of subjects, and a cognitive-behavioral methodology in a group setting was used once a week for 1 h.
Discussions about food re-education explored the eating habits of the participants and their families.
Self-monitoring is an important variable to be discussed in the behavioral treatment of obesity. The meetings held with this theme were conducted with the following characteristics: group activities to increase mutual knowledge and foster interaction among the participants, discussions about the advantages of having a healthy lifestyle for the whole family and alluding to the practice of exercise and its advantages.
The purpose was to promote reflection on anxiety and to explore the fears, difficulties, and expectations of the participants. The purpose of the meetings with this theme was to discuss issues related to the acquisition of behaviors considered healthy and to reduce the negative feelings related to anxiety, as well as to promote the participants’ self-knowledge so that they could reflect on positive and negative thoughts that permeate their daily lives.
The purpose of the meetings was to raise awareness about issues related to the reality of the group, for example, to demystify beliefs, prejudices, and stereotypes associated with obesity. The interventions followed the model proposed by Branco et al. (2018).
Prior to all activities, the adolescents consulted with a medical team. They were interviewed following a structured anamnesis to investigate their clinical history, previous and current pathologies, and their use of medications. In addition, pulmonary and cardiac auscultation and blood pressure measurements were performed according to the 7th Brazilian Guideline of Arterial Hypertension (Malachias et al., 2016).
The adolescents arrived at the biochemistry laboratory of the teaching institution after fasting for approximately 12 h. After local asepsis of the arm, a puncture was performed on the antecubital veins of the evaluated adolescents. All analyses were performed by a biomedical team blinded to the details of the interventions, i.e., the team did not have access to the intervention model realized by the adolescents during the 12-week intervention. All analyses were performed in triplicate using Siemens reagents (Frimley, Camberley, United Kingdom) in accordance with the manufacturer’s specifications. Subsequently, the samples were centrifuged at 3,600 rpm for 11 min at a controlled temperature (24°C) for the separation of the serum and plasma. Vacuum tubes (Becton Dickinson Vacutainer®, Plymouth, United Kingdom) were used for all collections, namely a tube with potassium fluoride and ethylenediaminetetraacetic acid (EDTA) was used for the analysis of the fasting plasma glucose level, and a clot activator tube (silica) was used for the analysis of the insulin, total cholesterol (TC), high-density lipoprotein (HDL-c), low-density lipoprotein (LDL-c), and triglyceride (TG) serum levels. For the biochemical analyses, Siemens equipment (Advia 1800 Chemistry Analyzer®, Siemens Healthcare Diagnostics, Illinois, United States) was used. The formula HOMA-IR = fasting glucose (nmol/L) ∗fasting insulin test (HOMA-IR) was used to calculate the homeostasis model assessment (HOMA) to evaluate insulin resistance [μU/mL)/22.5] according to Matthews et al. (1985).
Electrical bioimpedance (BIA) was conducted using the eight-tailed InBody four-quadrupole multifrequencial apparatus (model 570® Body Composition Analyzers, Seoul, South Korea). On the first day of evaluations, all participants received an informative document containing the protocol used to perform the assessment, including (a) 12-h fasting, (b) no moderate or vigorous physical exercise within the 24 h preceding the test, (c) urination and evacuation for the evaluation, (d) the absence of metallic objects during the evaluation, (e) postponement of the assessment in menstruating participants until after their period, (f) at least 8 h of sleep, and (g) no ingestion of caffeinated beverages or foods during the 12 h prior to the measurement (Heyward, 2001; Branco et al., 2018b). The following BIA variables were evaluated: body weight, body mass index (BMI), musculoskeletal mass (MME), fat mass (FM), %BF, and RMR.
Stature was measured by an electronic scale with a stadiometer (Filizola®, São Paulo, Brazil) with a capacity of 200 kg, with a measuring capacity of 2 m and accuracy of 0.1 cm. Waist (WC), relaxed right arm (AC), and neck (NC) circumferences were measured following the protocol proposed by Heyward (2001). An extensible measuring tape of the WISO brand (model T87-2®, Florianopolis, Santa Catarina, Brazil) was used with a measuring capacity of 2 m and precision within 0.1 cm.
Before the measurements were obtained, all adolescents were familiarized with the MIHS, MILTS, MILBS and aerobic fitness tests (Branco et al., 2018a).
A Jamar dynamometer (Asimow Engineering, Los Angeles, CA, United States) was used to evaluate MIHS. The teenager remained standing while holding the device close to her body with her arm extended with a neutral grip. Following a signal by the evaluator, the adolescent squeezed the dynamometer as hard as possible while maintaining the isometric contraction for 3 to 5 s. The measurement was performed with both hands. It was used the sum of right and left hand (sum of maximum isometric handgrip strength of right and left hand – SMIHS, in the statistical analysis), for After three attempts on each side, the maximum isometric strength of the handgrip of the right and left hands was recorded. A 60-s interval separated each attempt (Branco et al., 2018a).
A Kratos dynamometer (Kratos Industrial Equipment, Model DS®, São Paulo, Brazil) was used to evaluate MILTS. The teenager walked with both feet on the device with her knees extended, trunk flexed approximately 120°, head and neck aligned with the trunk, and fingers (holding the bar) positioned in front of the patella bone. The maximum contraction over 3 to 5 s was recorded, and the highest value of the measurement after three attempts with 60 s of rest between attempts was recorded (Branco et al., 2018a).
To evaluate the maximal isometric strength of the lower limbs, a Kratos dynamometer also used (the same equipment of evaluation of MILTS). The teenager stood on a platform with her knees bent at approximately 120° and trunk upright while holding the traction bar lined up in the inguinal fold. Following the evaluator’s signal, the adolescent performed the maximum isometric contraction for 3 to 5 s, and the highest measured value after three attempts with 60-s resting intervals was recorded (Branco et al., 2018a).
To measure aerobic fitness, the maximal oxygen consumption (VO2max) test, which was proposed by Léger and Lambert (1982), was used. This test has 21 stages; the initial velocity is 8.5 km/h, which increases by 0.5 km/h per stage. The VO2max was calculated by the following equation:
where X = velocity in the stage reached, and A = age in years.
Previously, the normality of the data was tested using the Shapiro–Wilk test. Similarly, the homogeneity of the data was tested by Levene’s test. After confirming normality and homogeneity, the data were expressed as the mean and (±) standard deviation. Mauchly’s test of sphericity was used to test as well as the Greenhouse-Geisser correction, if necessary. A two-way mixed-measures analysis of variance (ANOVA) was used to compare the groups and phases (pre- and post-intervention). Bonferroni post hoc test was used when a significant difference was found. A significance level of 5% was adopted for all analyses. In addition, the effect size was calculated using Cohen’s d (1992) as follows: 0.20 (small effect), 0.50 (moderate effect), and 0.80 (large effect). Furthermore, the partial eta-squared: ηp2 was calculated with the following classification: 0.10 (small effect), 0.25 (moderate effect), and 0.40 (large effect), according to Cohen (1992). All statistical analyses were performed using the statistical package SPSS 22.0 (IBM, Inc., United States).
Information regarding age, body weight, and stature is provided in Table 4.
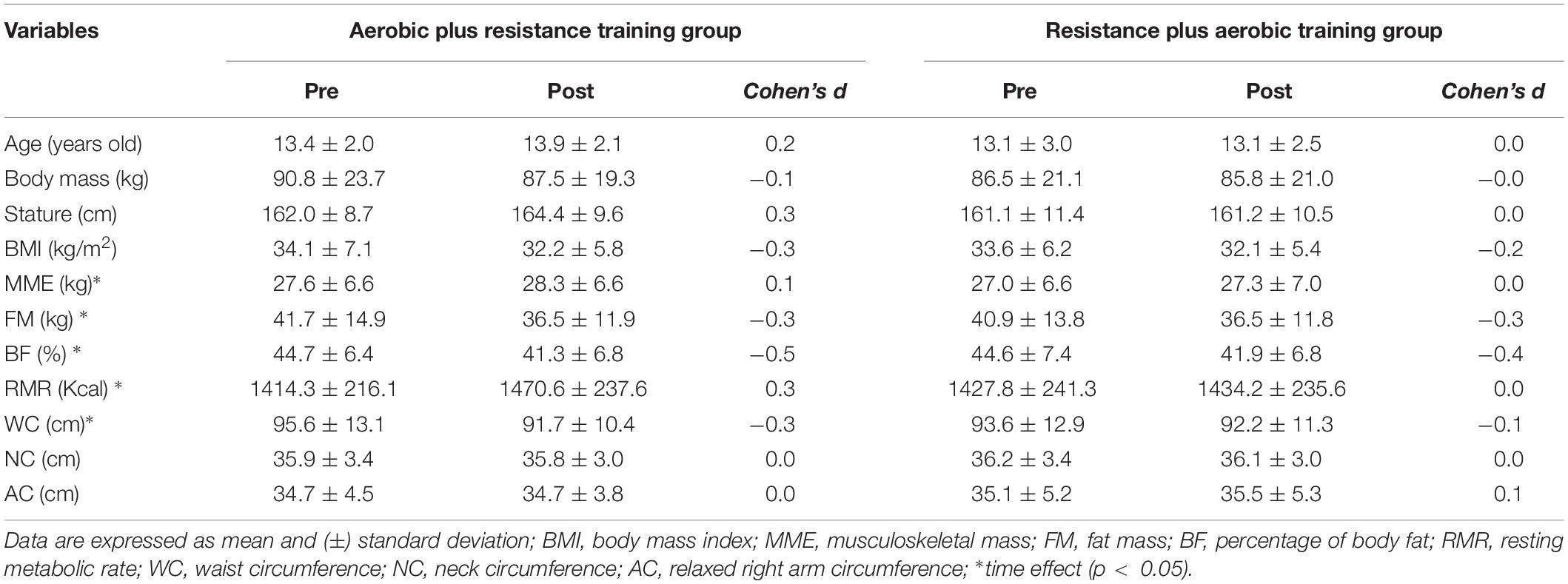
Table 4. Body composition and anthropometric measurements of female of adolescents participating in the study.
For the IPAQ, no significant differences were observed in the level of physical activity among the adolescents after the 12-week multiprofessional intervention (p > 0.05). The only difference observed was an increase in the level of physical activity performed on Mondays, Wednesdays, and Fridays. However, this result was expected since the adolescents participated in the activities 3× per week during the 12-week intervention.
For the RPE, ITL, and RPR, no significant differences were identified during the same microcycles and mesocycles of training performed by the adolescents (p > 0.05). These responses suggest that both training groups were similarly equalized in recovery, volume, and intensity.
For the caloric intake in kcal, no significant differences were observed before and after the 12-week intervention (p > 0.05). These responses suggest that the 12-week nutritional intervention is incipient for promoting significant changes in caloric intake.
Table 5 presents the body composition and anthropometric measurements of the adolescents participating in the interdisciplinary project for the treatment of obesity before and after the 12-week intervention.
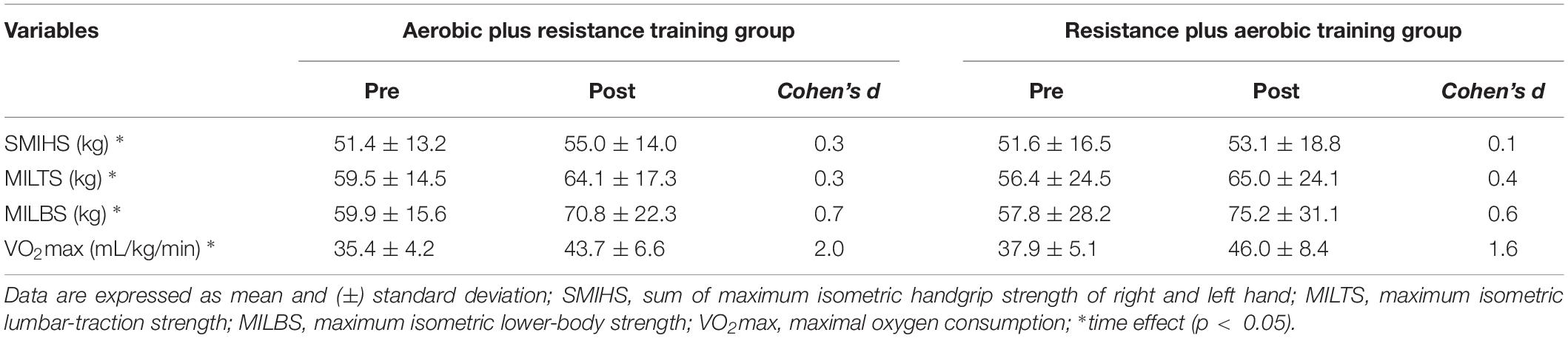
Table 5. Physical tests of female of adolescents participating in the study.
Age, body weight, stature, BMI, CN, and AC did not show group, time or interaction effects. However, specifically regarding MME [F(1,31) = 5.71, p = 0.02, ηp2 = 0.15, small] and RMR [F(1,31) = 5.06, p = 0.03, ηp2 = 0.14, small] a time effect was identified, with higher values after the intervention period when compared to the pre-intervention values, while FM [F(1,31) = 7.79, p = 0.008, ηp2 = 0.20, small],%BF [F(1,31) = 19.43, p = 0.001, ηp2 = 0.38, medium] and WC [F(1,31) = 11.28, p = 0.002, ηp2 = 0.28, medium] showed significantly lower values after the intervention period.
Table 5 shows the physical tests performed by the adolescents participating in the interdisciplinary project for the treatment of obesity before and after the 12-week intervention.
For MIHS [F(1,31) = 4.13, p = 0.05, ηp2 = 0.11, small], MILTS [F(1,31) = 6.18, p = 0.01, ηp2 = 0.16, small], MILBS [F(1,31) = 13.49, p = 0.0008, ηp2 = 0.30, medium] and VO2max [F(1,31) = 116.35, p < 0.001, ηp2 = 0.79, large] a time effect was identified, with higher values after the intervention period when compared to the pre-intervention values.
Table 6 shows the biochemical examination results of the adolescents participating in the interdisciplinary project for the treatment of obesity before and after the 12-week intervention.
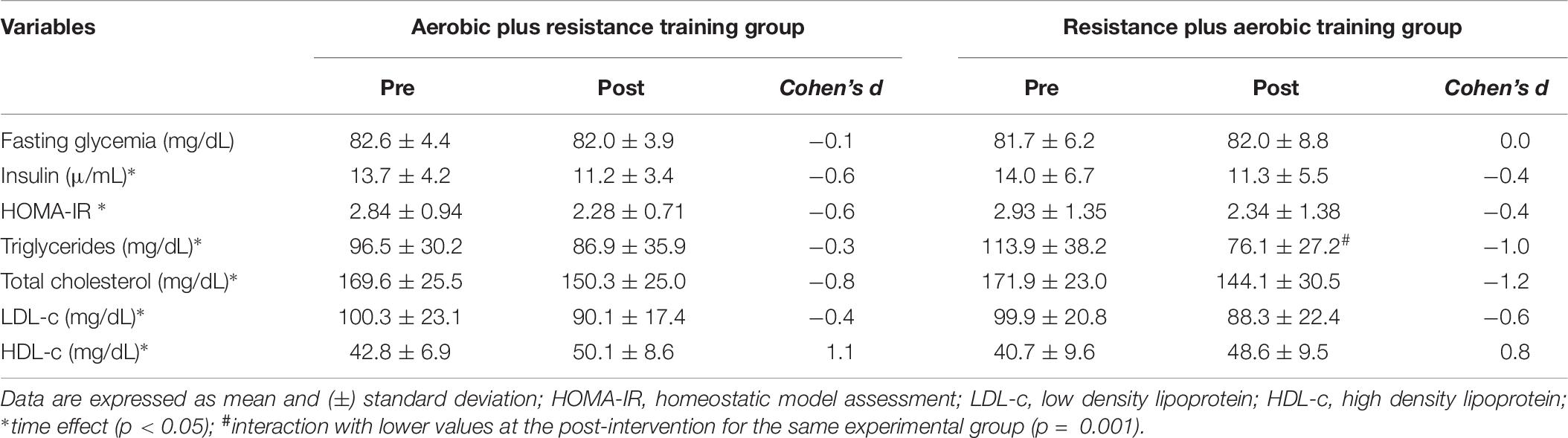
Table 6. Hormonal and biochemical tests of female of adolescents participating in the study.
Fasting glycemia levels, did not show group, time or interaction effects. Regarding insulin [F(1,25) = 9.67, p = 0.004, ηp2 = 0.28, medium], HOMA-IR, [F(1,25) = 6.44, p = 0.01, ηp2 = 0.22, small], TG [F(1,25) = 12.12, p = 0.001, ηp2 = 0.33, medium], TC [F(1,25) = 22.59, p = 0.000, ηp2 = 0.47, large] and LDL-c [F(1,24) = 1.56, p = 0.003, ηp2 = 0.06, small] a time effect was identified, with lower values after the intervention period when compared to the pre-intervention values. In addition, it was observed an interaction effect for TG [F(1,25) = 4.29, p = 0.048, ηp2 = 0.15, small] with lower values in the resistance plus aerobic group in post-intervention period when compared to the pre-intervention values (p = 0.002). Besides, for HDL-c [F(1,25) = 29.43, p < 0.001, ηp2 = 0.54, large] a time effect was identified, with higher values after the intervention period when compared to the pre-intervention values.
The main results of the present study indicated the following differences after 12 weeks in the two intervention groups: (a) increase in MME and RMR, (b) reduction in FM, %BF, and WC, (c) increase in MIHS, MILTS, and MILBT, (d) increase in VO2max, (e) reduction in insulin, HOMA-IR, TG, TC, and LDL-c levels, and (f) increase in HDL-c. In addition, an interaction was detected with lower values of TG in the resistance plus aerobic group after the intervention period. However, no differences were observed in fasting glycemia levels in the two experimental groups after the 12 weeks. As a result, the study’s hypothesis was confirmed.
In the condition that the concurrent protocols are somehow equalized, the training responses have a tendency to be similar (Branco et al., 2018). The findings of the present study indicate that MME increased significantly after 12 weeks of concurrent training concomitant with multiprofessional care in obese adolescents. Thus, muscle hypertrophy is intimately associated with the optimal volume and intensity of RE (Schoenfeld, 2010). A study conducted by Branco et al. (2018) did not identify muscle hypertrophy after 12 weeks of concurrent training in obese male adolescents. However, the volume of the resistance exercises conducted by Branco et al. (2018) was relatively lower than that in the present study. Regarding this discrepancy, Figueiredo et al. (2018) noted that volume can be considered the most effective variable in RE for muscle hypertrophy. However, in a letter to the editor, Souza et al. (2018) explained that RE is very complex, and due to methodological differences among scientific studies, determining the decisive variables for establishing what volume is critical for muscle hypertrophy is impossible. In light of these different findings and because scientific studies sometimes employ different intervention models with dissimilar body-composition analyses, it is believed that the key to the process of muscle hypertrophy is the optimal interdependence of volume and intensity based on the uniqueness of individuals. Thus, the differences observed between the study conducted by Branco et al. (2018) and the present study may be related to the higher volume of RE performed by the adolescents in this study.
Considering absolute FM and BF, significant reductions were identified after 12 weeks. However, it is suggested that the reduction in %BF is mainly related to the increase in energy expenditure resulting from the concurrent training practiced since no significant differences in caloric intake were detected during the 12-week period. In addition, no differences among IPAQ responses were identified during the 12-week intervention. Branco et al. (2018) identified no alterations in caloric intake inferred from food records for 2 days during the week and one weekend day and IPAQ responses over the course of 12-week multiprofessional interventions that focused on reducing body fat and cardiometabolic risk and improving the components of physical fitness related to health in adolescents. Despite the limitations of overestimation or underestimation during the completion of food records and the IPAQ, especially by adolescents, considering the above-mentioned aspects is recommended to determine whether the reduction in absolute and relative fat is closely linked to an increase in energy expenditure resulting from physical exercises performed daily for a duration of ∼60 min, reaching ∼180 min weekly. Thus, Donnelly et al. (2004) suggested that the addition of regular physical exercise over the medium and long term can result in additional energy expenditure (between 1000 and 2000 kcal per week depending on volume and intensity). However, regarding energy expended to be converted to reduce body fat, it cannot be compensated by increasing daily caloric consumption.
Well-controlled studies indicate that an elevation in RMR is closely related to increased levels of physical activity if dietary restrictions with a negative energy balance are not incorporated (Stiegler and Cunliffe, 2006). Thus, overall, the gain of MME directly affect elevation in the RMR (Stiegler and Cunliffe, 2006). However, studies in the literature note that MME accounts for only 20% of oxygen consumption at basal conditions (Brozek and Grande, 1955; Durnin and Passmore, 1967; Wahrlich and Anjos, 2001). Thus, importantly, the energy expenditure of the MME represents only 13 kcal/kg/day (McClave and Snider, 2001). Consequently, the increase in MME has a very low impact on the total energy expenditure/day of individuals. Therefore, it is essential to increase the performance of structured and unstructured physical activities and decrease the time spent performing low-intensity activities to increase energy expenditure throughout the day.
Regarding WC, significant reductions were identified after the multiprofessional intervention period. Branco et al. (2018) also identified a reduction in WC in overweight or obese adolescents after a 12-week intervention. Reduction in WC has a considerable impact on reduction in cardiometabolic risk (Freedman et al., 1999). As a result, despite the significant reduction in WC in the two intervention groups, the values are considered high (Patnaik et al., 2017). However, NC and AC did not exhibit significant differences, which is likely due to the short duration of the 12-week intervention. These two measures, NC and AC, have been associated with cardiometabolic risk (Jaiswal et al., 2017; Patnaik et al., 2017). Thus, both anthropometric measures can also be used in clinical practice for the evaluation of adolescents with overweight or obesity. From this perspective, Patnaik et al. (2017) identified that WC and NC are strongly correlated (r = 0.69), suggesting that both may be used to identify possible conditions related to cardiometabolic risk. In addition, Jaiswal et al. (2017) reported accuracy between 0.92 and 0.98 of the ROC curve of the association between arm circumference and overweight in children and adolescents. In summary, it has been identified that 12 weeks of multiprofessional interventions are insufficient to reduce WC and AC. These responses can be interrelated with a higher deposition of fat mass in WC compared to NC and AC. Thereby, NC and AC can be used to verify the applicability of these measures in longer-term obesity-treatment interventions.
Regarding the variables of health-related physical fitness, significant improvements were observed in MIHS, MILTS, MILBT, and VO2max in the two experimental groups, results that were expected. A relevant point highlighted by Nardo Júnior et al. (2018) discuss that success criteria for the multiprofessional treatment of obesity. The physical fitness variable selected in the study as substantial was aerobic fitness. Improvement in cardiorespiratory fitness reduces risks associated with morbidity and mortality and is considered a key component of the cardiovascular health of adolescents (Nardo Júnior et al., 2018).
Fasting glycemia did not show significant changes in either experimental group after the intervention period. However, the values found in the adolescents before and after the respective time were well below (from 81.7 to 82.6 mg/dL) the cutoff points proposed by the American Diabetes Association, i.e., < 100 mg/dL after fasting for 8 h (American Diabetes Association [ADA], 2018). Nevertheless, significant reductions were observed in the fasting insulin levels in both experimental groups. Thus, it was verified that physical exercise activates the insulin-signaling pathways, facilitating the process of glucose diffusion via GLUT-4 (Röhling et al., 2016). Therefore, considering the mechanisms occurring via GLUT-4, by performing exercise, sensitivity to insulin action is increased and lower levels of insulin release are required for glucose uptake. In regard to lipid profiles, significant reductions in TG, total cholesterol, and LDL-c levels and an elevation in HDL-c were identified in both experimental groups. A systematic review and meta-analysis published by García-Hermoso et al. (2018) identified that concurrent training tends to be more effective for the treatment of variables associated with the lipid profile, particularly in pediatric obesity. A substantial difference was observed for TG levels in this study, and decreases in TG are closely linked to reductions in cardiovascular diseases (Keech and Jenkins, 2017). TG decreases may be associated with PE and suggest changes in feeding during the interdisciplinary intervention (Hartley et al., 2016; Surampudi et al., 2016); such dietary changes may be related to the increased consumption of fibers and omega-3 (Surampudi et al., 2016; Siscovick et al., 2017). However, this is only a hypothesis since feeding control was not conducted during the 12-week interdisciplinary interventions. Considering that, in the present study, the authors did not control food intake over the course of the intervention, it is not possible to confirm that one model is better than the other to further reduce TG levels. Therefore, the differences between the groups can be attributed to a spurious relationship because other variables can influence the responses that are interrelated. Acute studies have identified similar global responses between the order of exercise during concurrent training (Coffey and Hawley, 2017). Nevertheless, in accordance with the author’s knowledge, these are still incipient studies that tested the responses among these biochemical and hormonal variables in order to verify the effectiveness of the order of the concurrent training on these variables. In this way, new longitudinal studies that include food control can be tested to verify the responses between the order of exercise.
Finally, considering that the two models of intervention resulted in similar responses, the choice of the order may be suggested by adolescents in order to maintain adherence, enjoyment, and satisfaction and to reduce dropouts. In addition, another point that can be highlighted is the low cost of the materials needed to conduct the PE routine and to control volume, intensity, and recovery. In light of these, this methodology may be replicated in larger studies in different contexts, e.g., activities against the school shift, sports centers, clubs, and basic health units, among others. Accordingly, this methodology may represent a strategy for health promotion that costs less, considering that the materials are cost effective.
Two limitations may be highlighted: (a) the lack of controlled feeding during the 12-week intervention, and (b) the utilization of perceptual effort and recovery scales in order to quantify training load and recovery, respectively. Despite this, Haddad et al. (2017) suggested that RPE presents good reliability for monitoring training load in teenagers. The same approach was used by Branco et al. (2018) with the purpose of monitoring the training load with PE sessions. Thus, it is believed that familiarization can be incorporated to minimize eventual errors in the utilization of perceptual scales.
Based on the results presented, the two models of concurrent training within a multiprofessional context focusing on the treatment of obesity positively impacted the body composition and anthropometric variables, reduced FM, %BF, and WC, and elevated MME and RMR. Moreover, regardless of the order in which the concurrent exercise was performed, physical fitness related to health presented significant improvements in maximum isometric strength and cardiopulmonary fitness tests. Finally, in regard to glycemic and lipid profiles, reductions in insulin, HOMA-IR, triglycerides, total cholesterol, and LDL-c and increases in HDL-c were observed in the two experimental groups.
The datasets generated for this study are available on request to the corresponding author.
This study was approved by the Committee of Ethics in Research of the University Center of Maringá (UniCesumar) through the opinion n 2,505,200/2018.
BB, DV, IC, LdO, and SB contributed to conception and design of the study. BB, FdO, DM, and AC organized the database. BB performed the statistical analysis. BB, DV, FdO, IC, DM, AC, LdO, and SB wrote the first draft of the manuscript. BB, IC, LdO, and SB wrote the sections of the manuscript. All authors contributed to the manuscript revision, and read and approved the submitted version.
This work was funded by ICETI – Instituto Cesumar de Ciência, Tecnologia e Inovação (Cesumar Institute of Science, Technology and Innovation).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
American Diabetes Association [ADA], (2018). Classification and diagnosis of diabetes: standards of medical care in diabetes-2018. Diabetes Care 41(Suppl. 1), S13–S27. doi: 10.2337/dc18-S002
Blüher, M. (2019). Obesity: global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 15, 288–298. doi: 10.1038/s41574-019-0176-8
Borg, G. A. (1982). Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 14, 377–381. doi: 10.1249/00005768-198205000-00012
Branco, B. H. M., Bernuci, M. P., Marques, D. C., Carvalho, I. Z., Barrero, C. A. L., De Oliveira, F. M., et al. (2018b). Proposal of a normative table for body fat percentages of Brazilian young adults through bioimpedanciometry. J. Exerc. Rehabil. 14, 974–979. doi: 10.12965/jer.1836400.200
Branco, B. H. M., Andreato, L. V., Ribeiro, E. D., Oliveira, H. G., Almeida, F. N., and Junior, N. N. (2018a). Development of tables for classifying judo athletes according to maximal isometric strength and muscular power, and comparisons between athletes at different competitive levels. Sports Sci. Health 14, 607–614. doi: 10.1007/s11332-018-0469-7
Branco, B. H. M., Carvalho, I. Z., Oliveira, H. G., Fanhani, A. P., Santos, M. C. M., Oliveira, L. P., et al. (2018). Effects of 2 types of resistance training models on obese adolescents’ body composition, cardiometabolic risk, and physical fitness. J. Strength Cond. Res. doi: 10.1519/JSC.0000000000002877 [Epub ahead of print].
Brozek, J., and Grande, F. (1955). Body composition and basal metabolism in man: correlation analysis versus physiological approach. Hum. Biol. 27, 22–31.
Coffey, V. G., and Hawley, J. A. (2017). Concurrent exercise training: do opposites distract? J. Physiol. 595, 2883–2896. doi: 10.1113/JP272270
Cole, T. J., and Lobstein, T. (2012). Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 7, 284–294. doi: 10.1111/j.2047-6310.2012.00064.x
Donnelly, J. E., Smith, B., Jacobsen, D. J., Kirk, E., DuBose, K., Hyder, M., et al. (2004). The role of exercise for weight loss and maintenance. Best Pract. Res. Clin. Gastroenterol. 18, 1009–1029. doi: 10.1016/j.bpg.2004.06.022
Figueiredo, V. C., De Salles, B. F., and Trajano, G. S. (2018). Volume for muscle hypertrophy and health outcomes: the most effective variable in resistance training. Sports Med. 48, 499–505. doi: 10.1007/s40279-017-0793-0
Foster, C., Florhaug, J. A., Franklin, J., Gottschall, L., Hrovatin, L. A., Parker, S., et al. (2001). A new approach to monitoring exercise training. J. Strength Cond. Res. 15, 109–115.
Freedman, D. S., Serdula, M. K., Srinivasan, S. R., and Berenson, G. S. (1999). relation of circumferences and skinfold thicknesses to lipid and insulin concentrations in children and adolescents: the bogalusa heart study. Am. J. Clin. Nutr. 69, 308–317. doi: 10.1093/AJCN/69.2.308
García-Hermoso, A., Ramírez-Vélez, R., Ramírez-Campillo, R., Peterson, M. D., and Martínez-Vizcaíno, V. (2018). Concurrent aerobic plus resistance exercise versus aerobic exercise alone to improve health outcomes in pediatric obesity: a systematic review and meta-analysis. Br. J. Sports Med. 52, 161–166. doi: 10.1136/bjsports-2016-096605
Guedes, D. P., Lopes, C. C., and Guedes, J. E. R. P. (2005). Reproducibility and validity of the international physical activity questionnaire in adolescents. Rev. Bras. Med. Esporte 11, 151–158. doi: 10.1590/S1517-86922005000200011
Haddad, M., Stylianides, G., Djaoui, L., Dellal, A., and Chamari, K. (2017). Session-RPE method for training load monitoring: validity, ecological usefulness, and influencing factors. Front. Neurosci. 11:612. doi: 10.3389/fnins.2017.00612
Hartley, L., May, M. D., Loveman, E., Colquitt, J. L., and Rees, K. (2016). Dietary fibre for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 7:CD011472. doi: 10.1002/14651858.CD011472.PUB2
Heyward, V. (2001). ASEP methods recommendation: body composition assessment. J. Exerc. Physiol. Online 4, 1–12.
Ho, H. C. H., Maddaloni, E., and Buzzetti, R. (2019). Risk factors and predictive biomarkers of early cardiovascular disease in obese youth. Diabetes Metab. Res. Rev. 35:e3134. doi: 10.1002/dmrr.3134
Jaiswal, M., Bansal, R., and Agarwal, A. (2017). Role of mid-upper arm circumference for determining overweight and obesity in children and adolescents. J. Clin. Diagn. Res. 11:SC05. doi: 10.7860/JCDR/2017/27442.10422
Kang, J., and Ratamess, N. (2014). Which comes first? resistance before aerobic exercise or vice versa? ACSMs Health Fit. J. 18, 9–14. doi: 10.1249/FIT.0000000000000004
Keech, A. C., and Jenkins, A. J. (2017). Triglyceride-lowering trials. Curr. Opin. Lipidol. 28, 477–487. doi: 10.1097/MOL.0000000000000465
Laurent, C. M., Green, J. M., Bishop, P. A., Sjökvist, J., Schumacker, R. E., Richardson, M. T., et al. (2011). A practical approach to monitoring recovery: development of a perceived recovery status scale. J. Strength Cond. Res. 25, 620–628. doi: 10.1519/JSC.0b013e3181c69ec6
Lee, E. Y., and Yoon, K. H. (2018). Epidemic obesity in children and adolescents: risk factors and prevention. Front. Med. 12, 658–666. doi: 10.1007/s11684-018-0640-1
Léger, L. A., and Lambert, J. (1982). A maximal multistage 20-m shuttle run test to predict VO2max. Eur. J. Appl. Physiol. 49, 01–12. doi: 10.1007/BF00428958
Malachias, M. V. B., Souza, W. K. S. B., Plavnik, F. L., Rodrigues, C. I. S., Brandão, A. A., Neves, M. F. T., et al. (2016). VII Diretrizes brasileiras de hipertensão arterial. Arq. Bras. Cardiol. 107, 31–83. doi: 10.5935/abc.20160153
Matthews, D. R., Hosker, J. P., Rudenski, A. S., Naylor, B. A., Treacher, D. F., and Turner, R. C. (1985). Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412–419. doi: 10.1007/BF00280883
McClave, S. A., and Snider, H. L. (2001). Dissecting the energy needs of the body. Curr. Opin. Clin. Nutr. Metab. Care 4, 143–147. doi: 10.1097/00075197-200103000-00011
Nakamura, F. Y., Moreira, A., and Aoki, M. S. (2010). Training load monitoring: is the session rating of perceived exertion a reliable method? R. da Educação Física/UEM. 21, 1–11. doi: 10.4025/reveducfis.v21i1.6713
Nardo Júnior, N., Bianchini, J. A. A., da Silva, D. F., Ferraro, Z. M., Lopera, C. A., and Antonini, V. D. S. (2018). Building a response criterion for pediatric multidisciplinary obesity intervention success based on combined benefits. Eur. J. Pediatr. 177, 1–12. doi: 10.1007/s00431-018-3115-0
Patnaik, L., Pattnaik, S., Rao, E. V., and Sahu, T. (2017). Validating neck circumference and waist circumference as anthropometric measures of overweight/obesity in adolescents. Indian J. Pediatr. 54, 377–380. doi: 10.1007/s13312-017-1110-6
Petridou, A., Siopi, A., and Mougios, V. (2019). Exercise in the management of obesity. Metabolism 92, 163–169. doi: 10.1016/j.metabol.2018.10.009
Röhling, M., Herder, C., Stemper, T., and Müssig, K. (2016). Influence of acute and chronic exercise on glucose uptake. J. Diabetes Res. 2868652, 1–33. doi: 10.1155/2016/2868652
Schoenfeld, B. J. (2010). The mechanisms of muscle hypertrophy and their application to resistance training. J. Strength Cond. Res. 24, 2857–2872. doi: 10.1519/JSC.0b013e3181e840f3
Siscovick, D. S., Barringer, T. A., Fretts, A. M., Wu, J. H., Lichtenstein, A. H., Costello, R. B., et al. (2017). Omega-3 polyunsaturated fatty acid (fish oil) supplementation and the prevention of clinical cardiovascular disease: a science advisory from the american heart association. Circulation 135, e867–e884. doi: 10.1161/CIR.0000000000000482
Slater, B., Philippi, S. T., Fisberg, R. M., and Latorre, M. R. (2002). Validation of a semiquantitative adolescent food frequency questionnaire applied at a public school in São paulo. Brazil. Eur. J. Clin. Nutr. 57, 629–635. doi: 10.1038/sj.ejcn.1601588
Souza, D. C., Viana, R. B., Coswig, V. S., Fisher, J. P., Steele, J., and Gentil, P. (2018). Comment on: volume for muscle hypertrophy and health outcomes: the most effective variable in resistance training. Sports Med. 48, 1281–1284. doi: 10.1007/s40279-018-0865-9
Stiegler, P., and Cunliffe, A. (2006). The role of diet and exercise for the maintenance of fat-free mass and resting metabolic rate during weight loss. Sports Med. 36, 239–262. doi: 10.2165/00007256-200636030-00005
Stoner, L., Beets, M. W., Brazendale, K., Moore, J. B., and Weaver, R. G. (2019). Exercise dose and weight loss in adolescents with overweight–obesity: a meta-regression. Sports Med. 49, 83–94. doi: 10.1007/s40279-018-01040-2
Surampudi, P., Enkhmaa, B., Anuurad, E., and Berglund, L. (2016). Lipid lowering with soluble dietary fiber. Curr. Atheroscler. Rep. 18:75. doi: 10.1007/S11883-016-0624-Z
Vilaça, J., Bottaro, M., and Santos, C. (2011). Energy expenditure combining strength and aerobic training. J. Hum. Kinet. 29A, 21–25. doi: 10.2478/v10078-011-0054-5
Wahrlich, V., and Anjos, L. A. D. (2001). Aspectos históricos e metodológicos da medição e estimativa da taxa metabólica basal: uma revisão da literatura. Cad. Saúde Pública 17, 801–817. doi: 10.1590/s0102-311x2001000400015
Keywords: adolescent health, cardiometabolic risk in childhood, childhood obesity, exercise physiology, health promotion, interdisciplinary research
Citation: Branco BHM, Valladares D, de Oliveira FM, Carvalho IZ, Marques DC, Coelho AA, de Oliveira LP and Bertolini SMMG (2019) Effects of the Order of Physical Exercises on Body Composition, Physical Fitness, and Cardiometabolic Risk in Adolescents Participating in an Interdisciplinary Program Focusing on the Treatment of Obesity. Front. Physiol. 10:1013. doi: 10.3389/fphys.2019.01013
Received: 20 April 2019; Accepted: 23 July 2019;
Published: 06 August 2019.
Edited by:
Luca Paolo Ardigò, University of Verona, ItalyReviewed by:
Dale R. Wagner, Utah State University, United StatesCopyright © 2019 Branco, Valladares, de Oliveira, Carvalho, Marques, Coelho, de Oliveira and Bertolini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Braulio Henrique Magnani Branco, YnJhdWxpb21hZ25hbmlAbGl2ZS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.