 Zhang Wan-Tong1,2,3†
Zhang Wan-Tong1,2,3† Zhu Bao-Chen4†
Zhu Bao-Chen4† Liu Zhao5†
Liu Zhao5† Wang Xu-Jie1,2,3
Wang Xu-Jie1,2,3 Gao Rui1,2,3Xiao Ning2Tang Wei3Wu Yu-Fei3Phoebe Miles6Weng Wei-Liang1,2*Lin Hao-Xiang7
Gao Rui1,2,3Xiao Ning2Tang Wei3Wu Yu-Fei3Phoebe Miles6Weng Wei-Liang1,2*Lin Hao-Xiang7 Li Qiu-Yan2,3,8*
Li Qiu-Yan2,3,8*- 1Institute of Clinical Pharmacology, Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, China
- 2National Clinical Research Center for Chinese Medicine Cardiology, Beijing, China
- 3NMPA Key Laboratory for Clinical Research and Evaluation of Traditional Chinese Medicine, Beijing, China
- 4Department of Pharmacy, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China
- 5Tobacco Medicine and Tobacco Cessation Center, China-Japan Friendship Hospital, Beijing, China
- 6Faculty of Humanities and Social Sciences, University of Nottingham, Ningbo, China
- 7Department of Social Medicine and Health Education, School of Public Health, Peking University Health Science Center, Beijing, China
- 8Stroke Center, Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, China
Background: No effective medication is available for symptomatic bradyarrhythmia, particularly in low socioeconomic status (SES) population.
Objective: To explore the safety and efficacy of Yuanjiang decoction, a traditional Chinese medicinal prescription, for symptomatic bradyarrhythmia on a compassionate-use basis.
Methods: This compassionate-use study was conducted in Beijing, China between January 2019 and January 2020. Eligible participants were recruited and treated with Yuanjiang decoction (composed of 6 Chinese herbal medicines), 200 ml twice daily for 16 weeks. Analyses were done with the intention-to-treat (ITT) approach. The primary outcome measure was the proportion of participants who achieved a favorable treatment outcome at 16 weeks.
Results: As of January 2020, 184 patients were included. After 16-weeks treatment, 12 participants were lost to contact while 21 participants were terminated from this study, with a drop-out rate of 17.93%. The most common treatment-related adverse events were xerostomia (6.52%), constipation (6.45%) and sleepiness (3.26%). The proportion of participants with favorable treatment outcome was 65.22% at 4 weeks, 59.78% at 8 weeks (OR: 1.11, 95% CI: 0.71–1.73), 61.41% at 12 weeks (OR: 1.16, 95% CI: 0.92–1.45) and 60.87% at 16 weeks (OR: 1.15, 95% CI: 0.98–1.35). In the multifactor regression analysis, the favorable treatment outcome at 16 weeks was significantly associated with completing at least 8 weeks treatment (OR: 2.053, 95% CI: 1.064–3.560), while unfavorable treatment outcome was significantly associated with an atrioventricular block (OR: 0.255, 95% CI: 0.083–0.784), current smoking (OR: 0.343, 95% CI: 0.027–0.487), and syncope in the month before treatment (OR: 0.321, 95%CI: 0.114–0.904).
Conclusion: This compassionate-use study showed encouraging outcomes of treatment with Yuanjiang decoction, without serious adverse events. This study identified several key factors that may affect outcomes. These findings helped inform the design and assess the feasibility of a large-scale randomized clinical trial.
Introduction
Bradyarrhythmia is a severe cardiac arrhythmia in clinical practice, characterized by slow heart rate and hemodynamic disorders which can result in blood insufficiency. The causes of bradyarrhythmia mainly include sinus-node dysfunction, atrioventricular-conduction disturbances and intraventricular block (Honarbakhsh et al., 2018). In severe cases, bradyarrhythmia can cause circulatory disturbance and endanger life.
The prevalence of bradyarrhythmia is rapidly increasing, owing to an ageing population (Ma et al., 2020). Despite its significance, only limited pharmaceutical interventions, such as atropine and isoproterenol, can be used to increase heart rate in the short-term. More importantly, there are no approved medications currently available for long-term use (Neumar et al., 2010). In the absence of proven effective medication, clinically significant bradyarrhythmia with typical symptoms requires pacemaker implantation (Epstein et al., 2013). The number of pacemaker implantations in China has greatly increased from 25,000 in 2007 to 73,000 in 2016 (Hua and Zhang, 2018). However, the quality of life in patients with pacemaker implantation is severely affected due to a high incidence of complications such as heart failure and infection (Johansen et al., 2011; Gillam et al., 2018), life-long follow-up demand (Mond and Proclemer, 2011) and its high cost (Clémenty et al., 2018). Therefore, many individuals refuse or cannot afford to pacemaker implantation, especially in low socioeconomic status (SES) population (Clémenty et al., 2019). This population is at the greatest risk for severe complications, and there is an urgent need to find out an alternative option for them.
Traditional Chinese medicine has a long history of treating bradyarrhythmia, which may have begun as early as 2,000 years ago (Chan, 2005). In recent years, several clinical trials demonstrated TCM, including Shenxian-Shengmai oral solution (Gao et al., 2019), Shensong Yangxin capsule (Liu et al., 2014), and Xinbao pill (Hu et al., 2020) has potential therapeutic effects for patients with bradyarrhythmia, without the need for pacemaker implantation. To date, no effective treatment is available for those who need pacemaker implantation but cannot afford the high cost.
As such, to provide an alternative option for symptomatic bradyarrhythmia patients requiring pacemaker implantation, we proposed an innovative herb formula, Yuanjiang decoction. This proposal is based upon the herb properties (Liu et al., 2018), recommendations from existing studies and guidelines (Yang et al., 1992; Wen et al., 2007; Cao et al., 2020), and our clinical practice experience (Li et al., 2017). This decoction consists of 6 herbs, including Alpinia officinarum Hance (Family: Zingiberaceae, Plant part: Rhizome), 12 g; Zingiber officinale Roscoe (Family: Zingiberaceae, Plant part: Rhizome), 6 g; Cinnamomum verum J.Presl (Family: Lauraceae, Plant part: Cortex), 6 g; Piper longum L. (Family: Piperaceae, Plant part: Fructus), 12 g; Corydalis yanhusuo (Family: Papaveraceae, Plant part: Rhizome), 15 g; Curcuma aromatica Salisb. (Family: Zingiberaceae, Plant part: Radix), 12 g. Yuanjiang decoction appears to have a favorable clinical safety profile, as reported based on our clinical practice experience (Liu and Weng, 2020). Moreover, previous studies have shown potential therapeutic efficacy in non-clinical models (Zhang et al., 2018). In this report, we describe the outcomes in a cohort of patients with low SES treated for symptomatic bradyarrhythmia with Yuanjiang decoction on a compassionate-use basis, in order to inform the design and assess the feasibility of a large-scale randomized clinical trial.
Methods
Study Design
We conducted a prospective pilot trial of compassionate use of Yuanjiang decoction for symptomatic bradyarrhythmia among low SES patients between January 2019 and January 2020 in Beijing, China. The protocol of this study is shown in Supplementary Appendix SA. This study was reviewed and approved by the institutional review board of Xiyuan Hospital of China Academy of Chinese Medical Sciences before the start of the study (No. 2018XLA035-2) and registered in Chinese Clinical Trial Registry (No. ChiCTR-1800018464).
As this was a compassionate-use study, the Xiyuan Hospital of China Academy of Chinese Medical Sciences established a specific Data and Safety Monitoring Board (DSMB) to monitor the study once per month and received summaries of study conduct, safety, and efficacy.
Participants
Eligible participants were recruited via trial sites, local newspapers, community events, websites, and recommendations from other medical institutions. Participants were included if they met all the following inclusion criteria: 1) aged 18–90 years; 2) documented symptomatic bradyarrhythmia; 3) Class I indications of permanent pacemaker implantation; 4) low SES and cannot afford pacemaker implantation due to inadequate finance; 5) voluntary participation in this trial and able to provide informed consent. Also, females were required to have a negative urine pregnancy test before starting treatment.
Participants were excluded if they met any of the following criteria: 1) pregnant or lactating; 2) allergic predisposition and drug allergy to the 6 herbs in the decoction; 3) comorbidities including severe liver disease, severe renal dysfunction, persistent atrial fibrillation, acute myocardial infarction, stroke, hematopoietic system abnormalities and mental illness in the past 3 months; 4) drug-induced transient secondary bradyarrhythmia; 5) athletes with low heart rate but normal sinoatrial node function, without bradyarrhythmia-related symptoms; 6) participation in other clinical trials in the last month; 7) taking any Chinese medicinal herbs in the last month.
The trial adhered to the Declaration of Helsinki. All participants signed informed consent and received financial compensation for trial participation time and travel expenses.
Compassionate Use and Ethical Consideration
Compassionate use is a treatment option that allows for exceptional use of unapproved drugs to treat patients with life-threatening or severe disease (Zhang et al., 2018). For the protection of the participants, at the request of the DSMB, the analysis of the primary outcome was completed once a month. The participants who showed syncope during the treatment with heart rate less than 30 bpm were terminated from this study and referred for further treatment, if appropriate.
Another important ethical consideration was that currently, as there are no alternative approved medications for this condition, there cannot be a non-treatment control group for apparent ethical reasons. Therefore, we did not define a control group in this study.
Procedures
All participants received 16 weeks of Yuanjiang decoction, self-administered, 200 ml orally, twice per day and supportive therapy was provided at the discretion of the clinicians.
This decoction consists of 6 herbs: including Alpinia officinarum Hance (Family: Zingiberaceae, Plant part: Rhizome), 12 g; Zingiber officinale Roscoe (Family: Zingiberaceae, Plant part: Rhizome), 6 g; Cinnamomum verum J.Presl (Family: Lauraceae, Plant part: Cortex), 6 g; Piper longum L. (Family: Piperaceae, Plant part: Fructus), 12 g; Corydalis yanhusuo (Family: Papaveraceae, Plant part: Rhizome), 15 g; Curcuma aromatica Salisb. (Family: Zingiberaceae, Plant part: Radix), 12 g (Figure 1).
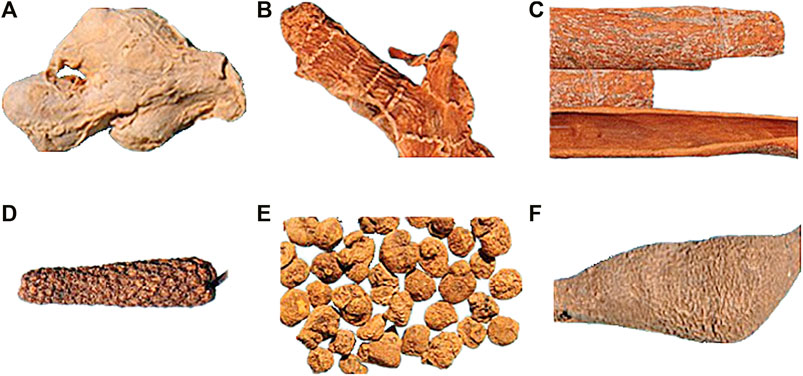
FIGURE 1. Example of 6 herbs of Yuanjiang decoction. (A), Zingiberis rhizoma; (B), Alpiniae officinarum rhizoma; (C), Cinnamomi cortex; (D), Piperis longi fructus; (E), Corydalis rhizoma; (F), Curcumae radix.
The procedure for preparing decoction is shown in Figure 2. In brief, a specialist pharmacist was responsible for decoction management and quality control. Before decoction preparation, all herbs were tested for heavy metals, microbial contamination, and residual pesticides. All the herbs were weighed precisely and placed in non-woven decocting bag (40*40 cm), then they were transferred into an automatic decocting machine (Beijing Donghuayuan Medical Equipment Co. Ltd., YJD20-GL). Before decocting, the herbs were immersed in water (drug-solvent ratio 1:15) for 30 min. Then they were decocted under 110° (Celsius) and 150 kPa for 30 min and concentrate to 400 ml. Finally, the decoctions were automatically packed with a specification of 200 ml. Our study comply with the best practice guidelines of the leading journals for pharmacological studies on natural products (Heinrich et al., 2020).

FIGURE 2. The procedure for preparing a decoction (A), herbs preparation; (B), machine decocting; (C), decoction packing; (D), decoction packages distributed to participants.
Participants were instructed to drink the Yuanjiang decoctions 30 min after breakfast and dinner, respectively, and not to take any other drugs, tea or coffee within half an hour before and after taking the decoction to avoid possible reactions with the Chinese medicine ingredients.
For the present study, we examined the effects of Yuanjiang decoction at 4, 8, 12, and 16 weeks into treatment.
Outcomes
The primary outcome was the proportion of participants who achieved a favorable treatment outcome at 16 weeks. The favorable treatment outcome was the improvement of bradyarrhythmia-related symptoms. This was defined as either or both, a minimum increase of 5 bpm in heart rate, or a minimum heart rate of more than 40 bpm (Zhang et al., 2019). The bradyarrhythmia-related symptoms were assessed using self-completed visual analogue scales (VAS). It assessed a specific symptom identified by the patient as being the most troublesome during prior therapy (symptom-specific VAS score). The patient-specific symptoms included manifestations of syncope or near syncope, transient dizziness or lightheadedness, or confessional states resulting from cerebral hypoperfusion attributable to slow heart rate. Fatigue, exercise intolerance may also result from bradyarrhythmia. The stem question for the symptom-specific VAS was, “How severe was your [X] today?” in which “X” was replaced with the patient’s specific symptom. For VAS questions, the patient responded by making a mark between 0 mm (no symptoms) and 100 mm (maximum intensity for the symptom in question) on a horizontal line. A difference of at least 13 mm in the VAS pain score was considered to be clinically significant (Breivik et al., 2008).
For this study, the definition of Class I indications of permanent pacemaker implantation was based on the ACC/AHA/HRS 2008 Guidelines (Epstein et al., 2008). The definitions of sinus node dysfunction, sinus pause, sinoatrial exit block and atrioventricular block were based on 2018 ACC/AHA/HRS Guideline (Kusumoto et al., 2018). The low SES was defined as monthly income less than 1600 China Yuan (CNY), approximately 230 US dollars. The definition of myocarditis was based on the Current State of Knowledge on Aetiology, Diagnosis, Management, and Therapy of Myocarditis (Caforio et al., 2013). The definition of coronary artery disease was based on the 2016 ACC/AHA Guideline (Levine et al., 2016). The definition of hypertension was based on the 2018 ESC/ESH Guideline (Emrich et al., 2019). The definition of Paroxysmal AF and atrial premature complexes was based on the 2015 ACC/AHA/HRS Guideline (Page et al., 2015). The definition of premature ventricular contractions was based on the 2017 AHA/ACC/HRS Guideline (Al-Khatib et al., 2017). The definition of diabetes mellitus was based on the Update on Prevention of Cardiovascular Disease in Adults with Type 2 Diabetes Mellitus in Light of Recent Evidence (Fox et al., 2015). The definition of current smoking was having smoked 100 cigarettes in one’s lifetime and currently smoking cigarettes (George et al., 2019).
Statistical Analysis
Based on our clinical practice experience (Li et al., 2017), the proportion of participants who achieved a favorable treatment outcome at 16 weeks was estimated to be 60%. A sample size of 180 participants was calculated to provide 80% power, assuming a 20% drop-out.
Intent-to-treat (ITT) approach was applied in this analysis, and the participants who were lost to contact or terminated from the study were considered to be unfavorable treatment outcome. The measurement data were presented as means±SDs. The t-test was used for comparisons which met Gaussian distribution and homogeneity of variance, whereas the nonparametric test was used for comparisons which did not meet homogeneity of variance. The chi-square test was used for numeral data. The logistic regression analysis was used to calculate the relationship between potential influencing factors and efficacy, represented with OR value at the 95% confidence interval. The Kaplan-Meier curve was used for analyses of optimal treatment time. SPSS 19.0 statistical software (SPSS, Inc.) was used for statistical analysis. p < 0.05 was regarded as statistical significance.
The authors had no access to information that could identify individual participants during or after data collection.
Role of the Funding
The funders of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the report. All authors had full access to the data, participated in data analysis and manuscript development, and gave final approval of the manuscript.
Results
Between January 2019 and January 2020, a total of 238 participants were screened for eligibility, of whom 184 were included in the study. After 16 weeks of treatment, 12 participants were lost to contact while 21 participants were terminated from this study and referred for permanent pacemaker implantation, with a total drop-out rate of 17.93% (Figure 3).
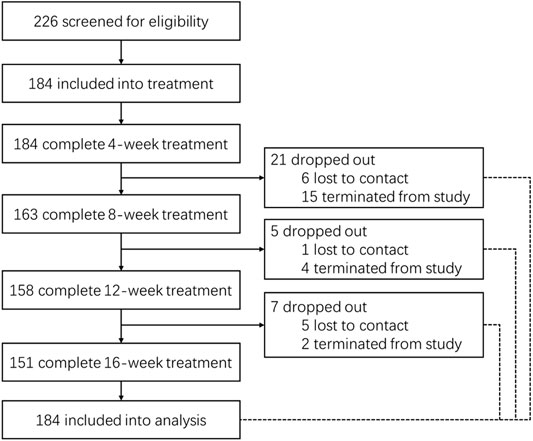
FIGURE 3. The flow chart of participants 12 participants were lost to contact while 21 participants were terminated from this study. This participants who showed syncope during the treatment with heart rate less than 30 bpm were terminated from this study and referred for further treatment, if appropriate.
The baseline characteristics are shown in Table 1. The mean age of participants was 57.83 ± 17.73 years, 39.13% were male, 29.89% were current smokers, and the mean BMI was 19.88 ± 6.88 kg/m2. The average duration of symptomatic bradyarrhythmia was 7.67 ± 6.25 years; 29.89% had atrioventricular block while 37.50% had sinus node dysfunction. At baseline, 21.74% were receiving antihypertensive drugs, 17.39% receiving lipid-lowering drugs and 15.22% receiving aspirin. In addition, 35.33% experienced syncope in the month before treatment.
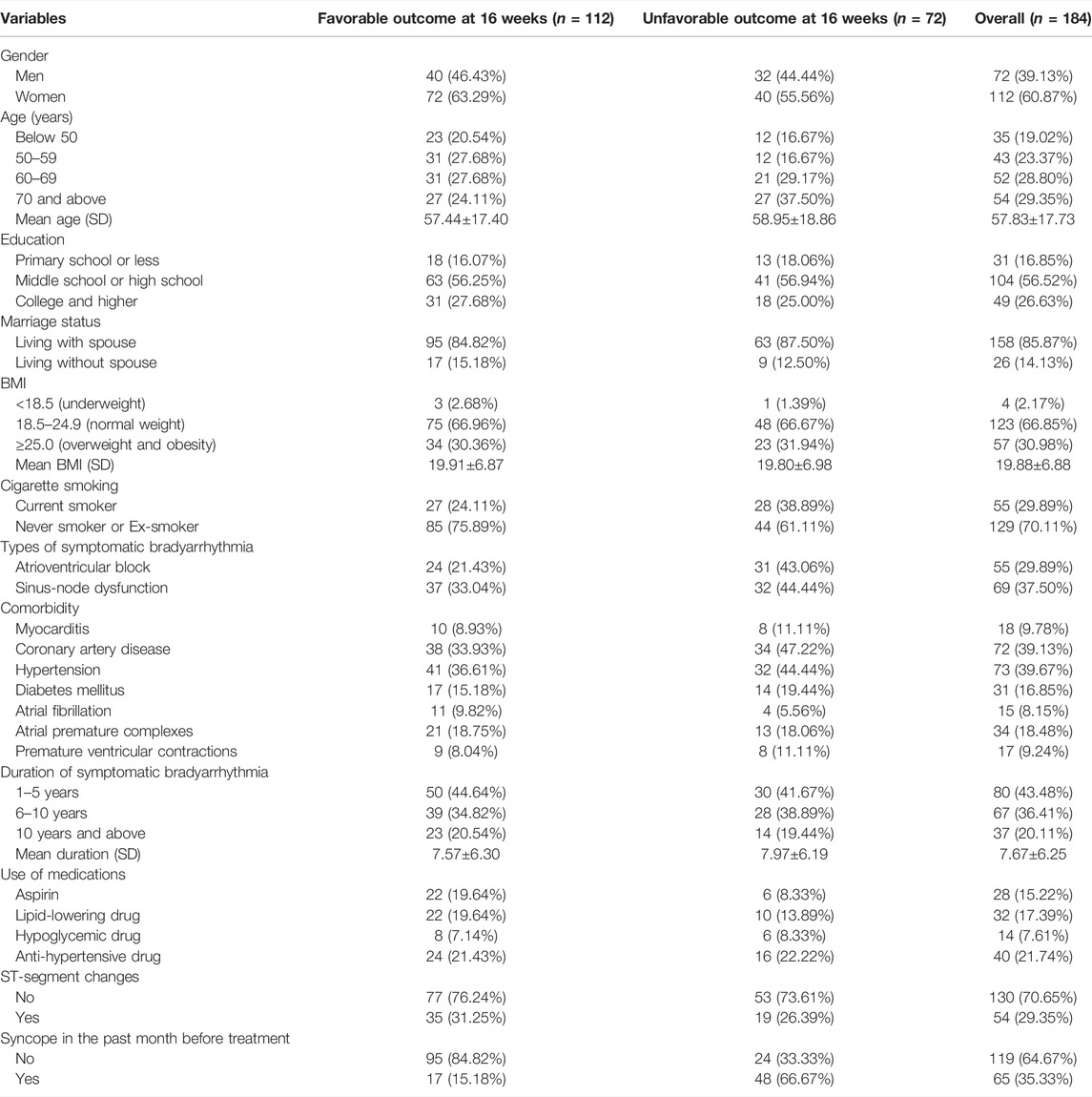
TABLE 1. Demographics of the study population.
Regarding the safety of the Yuanjiang decoction, 12 participants (6.52%) reported xerostomia, 8 participants (4.35%) reported constipation, and 6 participants (3.26%) reported sleepiness. No participants left the study because of these adverse events.
Regarding compliance of the Yuanjiang decoction, a total of 41,216 bags were planned for use; among them, 37,064 bags (89.93%) were distributed to participants, and 30,665 bags (74.40%) were administered by the participants based on self-reports. Also, 142 participants (77.17%) completed at least 8-week Yuanjiang decoction.
For the primary outcome, as shown in Figure 4, based on ITT approach, the proportion of participants with favorable treatment outcome was 65.22% at 4 weeks, 59.78% at 8 weeks (OR: 1.11, 95% CI: 0.71–1.73), 61.41% at 12 weeks (OR: 1.16, 95% CI: 0.92–1.45) and 60.87% at 16 weeks (OR: 1.15, 95% CI: 0.98–1.35).
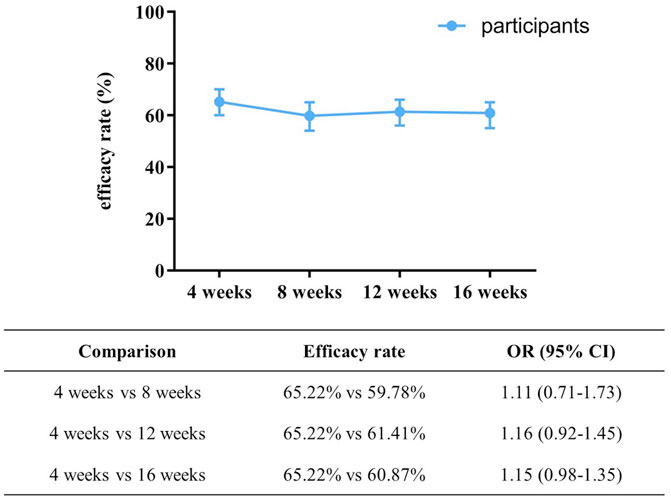
FIGURE 4. The proportion of participants with favorable treatment outcome at different time points. OR was adjusted for gender, age, education, marital status, BMI, cigarette smoking, types of symptomatic bradyarrhythmia, comorbidity, duration of symptomatic bradyarrhythmia, drug combination, ST-segment changes, completed at least 8-week treatment, and syncope in the past month before treatment.
Furthermore, the minimum heart rate was 34.85 ± 4.38 before treatment; this was significantly increased to 39.26 ± 5.32 at 4 weeks (p < 0.05), 39.73 ± 4.96 at 8 weeks (p < 0.05), 40.70 ± 5.01 at 12 weeks (p < 0.05) and 42.04 ± 4.87 at 16 weeks into treatment (p < 0.05). The results of the Kaplan-Meier analysis showed the median time to achieve a favorable treatment outcome was 8 weeks (Figure 5A). Clinical improvement was greater among ex-smokers or never smokers than smokers (Figure 5B), and among those without atrioventricular block than those with an atrioventricular block (Figure 5C), and among those who did not experience syncope in the past month before treatment than those who had syncope (Figure 5D).
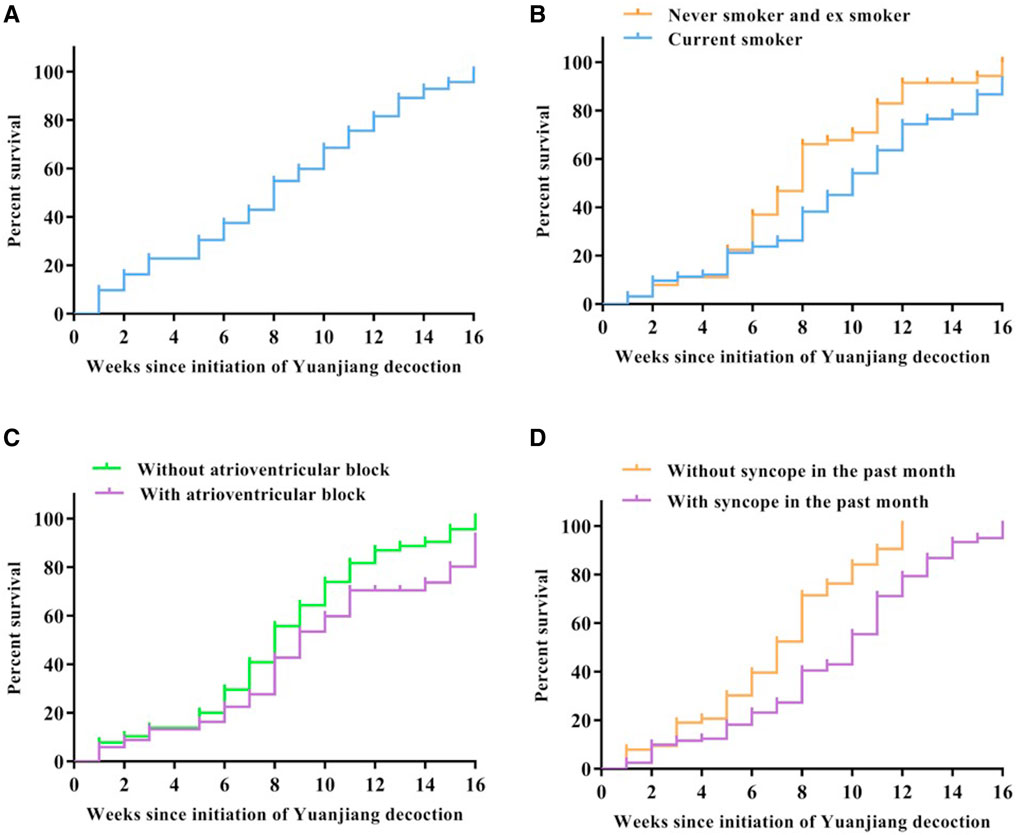
FIGURE 5. Cumulative incidence of clinical improvement. Clinical improvement is shown in the full cohort (A), in the cohort stratified by smoking status [(B), p = 0.013], in the cohort stratified by atrioventricular block [(C), p = 0.017] and in the cohort stratified by syncope in the past month before treatment [(D), p = 0.032].
After multifactor regression analysis (Table 2), the favorable treatment outcome at 16 weeks was significantly associated with the completion of at least 8 weeks treatment (OR: 2.053, 95% CI: 1.064–3.560), while unfavorable treatment outcome was significantly associated with an atrioventricular block (OR: 0.255, 95% CI: 0.083–0.784), current smoking (OR: 0.343, 95% CI: 0.027–0.487), and syncope in the month before treatment (OR: 0.321, 95%CI: 0.114–0.904).
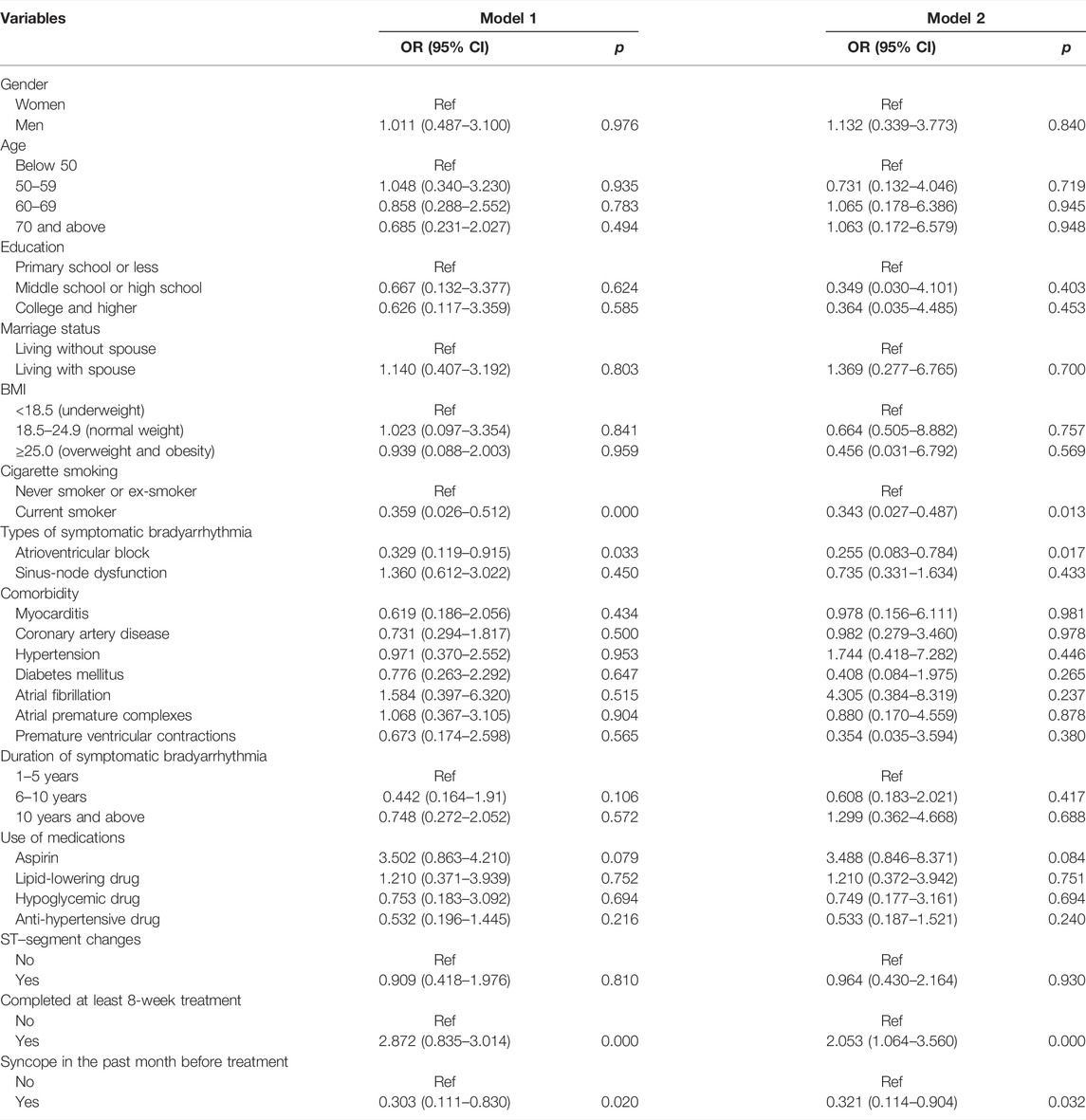
TABLE 2. The Adjusted ORs for favorable treatment outcome at 16 weeks.
Discussion
To date, no therapy other than permanent pacemaker implantation has demonstrated sufficient efficacy for patients with symptomatic bradyarrhythmia. Our findings address several knowledge gaps about alternative treatment options for this condition. In our study, the favorable treatment outcome was observed in 60.87% of participants after 16 weeks of treatment, with completion of at least 8 weeks of treatment as an important contributing factor. Moreover, current smoking was significantly associated with unfavorable treatment outcome, suggesting that smoking cessation intervention should be implemented. However, the patients with atrioventricular block and those who experienced syncope before treatment showed unfavorable outcome, thus concomitant intensive supportive therapy should be provided for these patients.
The safety of Chinese herbal medicines is often queried. Aristolochia fangchi (Tankeu et al., 2016) and Ephedra (Odaguchi et al., 2019) are reported with a number of serious adverse effects on the cardiovascular and nervous system. The herbs of Yuanjiang decoction used in this study have been standard for decades. More importantly, although the participants in our study were elderly, had low SES and predominantly presented with severe symptoms, only 26 (14.13%) participants experienced mild adverse events, and no serious adverse effects were observed. However, it is important to also note that 21 of 184 participants were terminated from this trial due to worsening symptoms of bradyarrhythmia. Given the relatively short intervention period of our study, more evidence on the safety of Yuanjiang decoction is needed before its use becomes widespread.
The mechanism of Traditional Chinese medicine for symptomatic bradyarrhythmia is complex and remains unclear. Our previous study in rat models showed that Yuanjiang decoction could upregulate the expression of a hyper-polarization-activated cyclic nucleotide-gated cation channel (HCN4) and sodium channel protein type 5 subunit alpha (SCN5a) (Zhang et al., 2018). In addition, Dong and colleagues found that gingerol, the main component of Zingiberis Rhizoma, may promote the release of catecholamine from the adrenal medulla to antagonize the decrease of heart rate caused by the vagus nerve (Dong et al., 2018). Investigators also found that the tetrahydropalmatine in Corydalis Rhizoma could increase the activities of Na+-K+-ATPase and Ca2+-ATPase, promote Na+-Ca2+ exchange and increase intracellular Ca2+ concentration (Li et al., 2014). More studies are needed to clarify the mechanisms of Yuanjiang decoction.
Symptomatic bradyarrhythmia is difficult to treat and may have poor long-term outcomes without permanent pacemaker implantation. Since the first permanent pacemaker implantation in the late 1950s, clinical use of these devices has increased exponentially, and ongoing innovation in their design has resulted in a reduction in device-associated risks as well as a significant improvement in device performance and subsequent patient outcomes (Boriani et al., 2014). However, implantation of a permanent pacemaker is likely influenced by factors other than the patient’s age or associated medical conditions. Of note, the pacemakers are costly in China, resulting in a sizeable economic burden. Previous investigators have raised the concern that patients with low SES may have reduced access to more advanced technology (Muñoz et al., 2019). To address this unmet medical and social need, we developed the Yuanjiang decoction, with focus on clinical and cost-effectiveness at the same time. Within the analysis reported here, when clinical effects and economic costs are combined into a single metric, the use of Yuanjiang decoction is expected to yield substantial health benefits.
This study has important clinical implications. Traditional Chinese medicine and Western medicine have contrasting approaches to the prevention and treatment of diseases. Western medicine is superior in the rapid amelioration of symptoms, while Traditional Chinese medicine may provide a holistic approach for disease prevention and long-term care (Wong et al., 2001). With the findings of this study, we suggest that therapeutic strategies merging the merits of both TCM and Western medicine approaches could contribute to the improved management of patients with symptomatic bradyarrhythmia.
Despite the encouraging findings from this study, some aspects of the design may have limited the value of the data. Firstly, as explained above, there cannot be a control group for apparent ethical reasons in this compassionate-use study. To be able to assess the Yuanjiang decoction more meticulously, we are now in the process of collecting one-year follow-up data, which will be reported in the future. Secondly, because this was not a randomized controlled trial, the treatment benefits cannot be weighted properly, since it must be compared against historical controls. Also, although compatible with previous studies, especially in the Chinese population, the selection of primary outcome requires more supportive evidence. Fourthly, expectation bias caused by their belief in traditional Chinese medicine cannot be eliminated. Finally, owing to the nature of the program, several variables, such as cardiac electrophysiology, were not assessed (Schmidt et al., 2017).
Conclusion
This compassionate-use study demonstrates that 3 out of 5 5 participants had encouraging outcomes after 16 weeks of treatment with Yuanjiang decoction, without serious adverse events. In addition, this study identified several key factors that affect the treatment outcome. These findings helped inform the design and assess the feasibility of a large-scale randomized clinical trial.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Xiyuan Hospital of China Academy of Chinese Medical Sciences before the start of the study. The patients/participants provided their written informed consent to participate in this study. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
LQ-Y and WW-L conceived and designed the study. LQ-Y supervised the study. LZ did the statistical analysis. All authors contributed to data collection, analysis, and interpretation. ZW-T, LZ, and ZB-C drafted the report. All authors revised the report and approved the final version before submission.
Funding
This study was supported by National Natural Science Foundation of China (82004352), Academic Inheritance studio of WW-L and Fundamental Research Funds for the Central public welfare research institutes (ZZ14-YQ-006).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank all the participants and their families for their participation in this study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.764930/full#supplementary-material
References
Al-Khatib, S. M., Stevenson, W. G., Ackerman, M. J., Bryant, W. J., Callans, D. J., Curtis, A. B., et al. (2017). 2017 AHA/ACC/HRS Guideline for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm 15 (10), e190–e252. doi:10.1016/j.hrthm.2017.10.035
Boriani, G., Tukkie, R., Manolis, A. S., Mont, L., Pürerfellner, H., Santini, M., et al. (2014). Atrial Antitachycardia Pacing and Managed Ventricular Pacing in Bradycardia Patients with Paroxysmal or Persistent Atrial Tachyarrhythmias: the MINERVA Randomized Multicentre International Trial. Eur. Heart J. 35 (35), 2352–2362. doi:10.1093/eurheartj/ehu165
Breivik, H., Borchgrevink, P. C., Allen, S. M., Rosseland, L. A., Romundstad, L., Hals, E. K., et al. (2008). Assessment of Pain. Br. J. Anaesth. 101 (1), 17–24. doi:10.1093/bja/aen103
Caforio, A. L., Pankuweit, S., Arbustini, E., Basso, C., Gimeno-Blanes, J., Felix, S. B., et al. (2013). Current State of Knowledge on Aetiology, Diagnosis, Management, and Therapy of Myocarditis: a Position Statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 34 (33), 2636–2648d. doi:10.1093/eurheartj/eht210
Cao, J. L., Li, X. L., Meng, F., and Gong, Y. (2020). Expert Consensus on Clinical Application of Chinese Herbal Medicine Decoction Pieces (In Chinese). Zhongguo Zhong Yao Za Zhi 45 (13), 3238–3244.
Chan, K. (2005). Chinese Medicinal Materials and Their Interface with Western Medical Concepts. J. Ethnopharmacol 96 (1-2), 1–18. doi:10.1016/j.jep.2004.09.019
Clémenty, N., Carion, P. L., Léotoing, L., Lamarsalle, L., Wilquin-Bequet, F., Brown, B., et al. (2018). Infections and Associated Costs Following Cardiovascular Implantable Electronic Device Implantations: a Nationwide Cohort Study. Europace 20 (12), 1974–1980. doi:10.1093/europace/eux387
Clémenty, N., Fernandes, J., Carion, P. L., de Léotoing, L., Lamarsalle, L., Wilquin-Bequet, F., et al. (2019). Pacemaker Complications and Costs: a Nationwide Economic Study. J. Med. Econ. 22 (11), 1171–1178. doi:10.1080/13696998.2019.1652186
Dong, Y., Yao, K. W., and Wang, J. (2018). Pharmacological Effects and Clinical Applications of Zingiber Officinale and its Processed Products. Zhongguo Zhong Yao Za Zhi 43 (10), 2020–2024. doi:10.19540/j.cnki.cjcmm.20180226.002
Emrich, I. E., Böhm, M., and Mahfoud, F. (2019). The 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension: A German point of View. Eur. Heart J. 40 (23), 1830–1831. doi:10.1093/eurheartj/ehz381
Epstein, A. E., DiMarco, J. P., Ellenbogen, K. A., Estes, N. A., Freedman, R. A., Gettes, L. S., et al. (2013). 2012 ACCF/AHA/HRS Focused Update Incorporated into the ACCF/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation 127 (3), e283–352. doi:10.1161/CIR.0b013e318276ce9b
Epstein, A. E., DiMarco, J. P., Ellenbogen, K. A., Estes, N. A., Freedman, R. A., Gettes, L. S., et al. (2008). ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) Developed in Collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 51 (21), e1–62. doi:10.1016/j.jacc.2008.02.032
Fox, C. S., Golden, S. H., Anderson, C., Bray, G. A., Burke, L. E., de Boer, I. H., et al. (2015). Update on Prevention of Cardiovascular Disease in Adults with Type 2 Diabetes Mellitus in Light of Recent Evidence: A Scientific Statement from the American Heart Association and the American Diabetes Association. Diabetes Care 38 (8), 1777–1803. doi:10.2337/dci15-0012
Gao, J., Wang, T., Yao, X., Xie, W., Shi, X., He, S., et al. (2019). Clinical Evidence-Guided Network Pharmacology Analysis Reveals a Critical Contribution of β1-adrenoreceptor Upregulation to Bradycardia Alleviation by Shenxian-Shengmai. BMC Complement. Altern. Med. 19 (1), 357. doi:10.1186/s12906-019-2769-0
George, J., Hussain, M., Vadiveloo, T., Ireland, S., Hopkinson, P., Struthers, A. D., et al. (2019). Cardiovascular Effects of Switching from Tobacco Cigarettes to Electronic Cigarettes. J. Am. Coll. Cardiol. 74 (25), 3112–3120. doi:10.1016/j.jacc.2019.09.067
Gillam, M. H., Pratt, N. L., Inacio, M. C. S., Shakib, S., Sanders, P., Lau, D. H., et al. (2018). Rehospitalizations for Complications and Mortality Following Pacemaker Implantation: A Retrospective Cohort Study in an Older Population. Clin. Cardiol. 41 (11), 1480–1486. doi:10.1002/clc.23091
Heinrich, M., Appendino, G., Efferth, T., Fürst, R., Izzo, A. A., Kayser, O., et al. (2020). Best Practice in Research - Overcoming Common Challenges in Phytopharmacological Research. J. Ethnopharmacol 246, 112230. doi:10.1016/j.jep.2019.112230
Honarbakhsh, S., Hunter, L., Chow, A., and Hunter, R. J. (2018). Bradyarrhythmias and Pacemakers. BMJ 360, k642. doi:10.1136/bmj.k642
Hu, H. Y., Ji, Z. C., Yu, D. D., Yang, F. W., Wang, H., Zheng, W. K., et al. (2020). Network Meta-Analysis of Randomized Controlled Trials of Chinese Patent Medicine for Bradyarrhythmia. Zhongguo Zhong Yao Za Zhi 45 (05), 1149–1158. doi:10.19540/j.cnki.cjcmm.20190802.501
Hua, W., and Zhang, S. (2018). Forge Ahead and Learn from the Brilliant-Ten Years Review of Chinese Cardiac Pacing Career (In Chinese). Chin. J. Card. Arrhythmias 22 (01), 8–10.
Johansen, J. B., Jørgensen, O. D., Møller, M., Arnsbo, P., Mortensen, P. T., and Nielsen, J. C. (2011). Infection after Pacemaker Implantation: Infection Rates and Risk Factors Associated with Infection in a Population-Based Cohort Study of 46299 Consecutive Patients. Eur. Heart J. 32 (8), 991–998. doi:10.1093/eurheartj/ehq497
Kusumoto, F. M., Schoenfeld, M. H., Barrett, C., Edgerton, J. R., Ellenbogen, K. A., Gold, M. R., et al. (2018). 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 74 (7), e51–e156. doi:10.1016/j.jacc.2018.10.044
Levine, G. N., Bates, E. R., Bittl, J. A., Brindis, R. G., Fihn, S. D., Fleisher, L. A., et al. (2016). 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 68 (10), 1082–1115. doi:10.1016/j.jacc.2016.03.513
Li, Q. Y., Ma, X. Z., and Weng, W. L. (2017). WENG Weiliang's Experience in Treating Bradycardia Arrhythmia (In Chinese). J. Traditional Chin. Med. 58 (04), 287–290.
Li, R., Cai, Q. Q., Niu, Y. B., Yang, S. C., and Dou, Z. Y. (2014). Comparative Study between Crude Corydalis Rhizoma and Vinegar Corydalis Rhizoma in Pharmacological Action (In Chinese). Chin. J. Exp. Traditional Med. Formulae 19, 133–137.
Liu, M. Y., and Weng, W. L. (2020). WENG Weiliang's Experience in Treating Bradycardia Arrhythmia (In Chinese). Lishizhen Med. Materia Med. Res. 02, 456–458.
Liu, S., Tian, G., Chen, J., Zhang, X., Wu, A., Li, M., et al. (2018). Traditional Chinese Medicine for Bradyarrhythmia: Evidence and Potential Mechanisms. Front. Pharmacol. 9, 324. doi:10.3389/fphar.2018.00324
Liu, Y., Li, N., Jia, Z., Lu, F., and Pu, J. (2014). Chinese Medicine Shensongyangxin Is Effective for Patients with Bradycardia: Results of a Randomized, Double-Blind, Placebo-Controlled Multicenter Trial. Evid. Based Complement. Alternat Med. 2014, 605714. doi:10.1155/2014/605714
Ma, L. Y., Chen, W. W., Gao, R. L., Liu, L. S., Zhu, M. L., Wang, Y. J., et al. (2020). China Cardiovascular Diseases Report 2018: an Updated Summary. J. Geriatr. Cardiol. 17 (1), 1–8. doi:10.11909/j.issn.1671-5411.2020.01.001
Mond, H. G., and Proclemer, A. (2011). The 11th World Survey of Cardiac Pacing and Implantable Cardioverter-Defibrillators: Calendar Year 2009--a World Society of Arrhythmia's Project. Pacing Clin. Electrophysiol. 34 (8), 1013–1027. doi:10.1111/j.1540-8159.2011.03150.x
Muñoz, D., Uzoije, P., Reynolds, C., Miller, R., Walkley, D., Pappalardo, S., et al. (2019). Polypill for Cardiovascular Disease Prevention in an Underserved Population. N. Engl. J. Med. 381 (12), 1114–1123. doi:10.1056/NEJMoa1815359
Neumar, R. W., Otto, C. W., Link, M. S., Kronick, S. L., Shuster, M., Callaway, C. W., et al. (2010). Part 8: Adult Advanced Cardiovascular Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 122 (18 Suppl. 3), S729–S767. doi:10.1161/CIRCULATIONAHA.110.970988
Odaguchi, H., Hyuga, S., Sekine, M., Nakamori, S., Takemoto, H., Huang, X., et al. (2019). The Adverse Effects of Ephedra Herb and the Safety of Ephedrine Alkaloids-free Ephedra Herb Extract (EFE). Yakugaku Zasshi 139 (11), 1417–1425. doi:10.1248/yakushi.19-00122
Page, R. L., Joglar, J. A., Caldwell, M. A., Calkins, H., Conti, J. B., Deal, B. J., et al. (2015). 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients with Supraventricular Tachycardia: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 133 (14), e471–505. doi:10.1161/CIR.0000000000000310
Schmidt, G., Huster, K. M., and Malik, M. (2017). Cardiac Electrophysiology: Signals to Decrypt and to Decipher. Eur. Heart J. 38 (27), 2119–2121. doi:10.1093/eurheartj/ehx212
Tankeu, S., Vermaak, I., Chen, W., Sandasi, M., and Viljoen, A. (2016). Differentiation between Two "fang Ji" Herbal Medicines, Stephania Tetrandra and the Nephrotoxic Aristolochia Fangchi, Using Hyperspectral Imaging. Phytochemistry 122, 213–222. doi:10.1016/j.phytochem.2015.11.008
Wen, C., Wu, L., Ling, H., and Li, L. (2007). Salutary Effects of Corydalis Yanhusuo Extract on Cardiac Hypertrophy Due to Pressure Overload in Rats. J. Pharm. Pharmacol. 59 (8), 1159–1165. doi:10.1211/jpp.59.8.0015
Wong, R., Sagar, C. M., and Sagar, S. M. (2001). Integration of Chinese Medicine into Supportive Cancer Care: a Modern Role for an Ancient Tradition. Cancer Treat. Rev. 27 (4), 235–246. doi:10.1053/ctrv.2001.0227
Yang, H. Z., Liang, Y. H., and Ren, H. (1992). Effect of Compound and Minor Prescription of Heat-Nature Products Radix Aconiti Lateralis Preparata, Rhizoma Zingiberis and Cortex Cinnamomi on the Sympathetic Nervous System, Adrenal Gland, TSH and LH. Zhongguo Zhong Yao Za Zhi 17 (11), 688–704.
Zhang, F., Zou, J., Yu, H., Li, X., Kojodjojo, P., Cai, X., et al. (2019). Acute Efficacy of a Traditional Chinese Medicine for Treatment of Frequent Premature Ventricular Contractions in Patients with Concomitant Sinus Bradycardia: Results from a Double-Blind, Placebo-Controlled, Multicentre, Randomized Clinical Trial. Evid. Based Complement. Alternat. Med. 2019, 3917282. doi:10.1155/2019/3917282
Keywords: bradyarrhythmia, compassionate use, Yuanjiang decoction, traditional Chinese medicinal prescription, prospective pilot trial
Citation: Wan-Tong Z, Bao-Chen Z, Zhao L, Xu-Jie W, Rui G, Ning X, Wei T, Yu-Fei W, Miles P, Wei-Liang W, Hao-Xiang L and Qiu-Yan L (2022) Compassionate Use of Yuanjiang Decoction, a Traditional Chinese Medicinal Prescription, for Symptomatic Bradyarrhythmia. Front. Pharmacol. 13:764930. doi: 10.3389/fphar.2022.764930
Received: 26 August 2021; Accepted: 11 February 2022;
Published: 11 April 2022.
Edited by:
Pulok Kumar Mukherjee, Institute of Bio-Resources and Sustainable Development (IBSD), IndiaReviewed by:
Claudio Ferrante, University of Studies G. d’Annunzio Chieti and Pescara, ItalyMasoud Amiri, Erasmus Medical Center, Netherlands
Copyright © 2022 Wan-Tong, Bao-Chen, Zhao, Xu-Jie, Rui, Ning, Wei, Yu-Fei, Miles, Wei-Liang, Hao-Xiang and Qiu-Yan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weng Wei-Liang, ww6488@126.com; Li Qiu-Yan, liqiuyan1968@sohu.com
†These authors have contributed equally to this work