 Ahmad M. Eid
Ahmad M. Eid Nidal Jaradat
Nidal Jaradat
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 14 February 2020
Sec. Ethnopharmacology
Volume 11 - 2020 | https://doi.org/10.3389/fphar.2020.00046
The use of herbal products by pregnant and lactating mothers without awareness of their harmful effects may expose both mother and fetus or infant to great dangers, such as abortion, premature delivery, uterine bleeding, and physical and mental retardation of the fetus. Thus, the aim of this study was to investigate the extent to which herbal product treatment is used and the reason for which such products are used and to ensure that these reasons are correct. An ethnopharmacological survey (cross-sectional observational design study) using a pre-piloted questionnaire was undertaken on herbal products used by pregnant and lactating women in the West Bank area of Palestine. A questionnaire was distributed to 350 pregnant and lactating women. The informed consent forms, ethics, and aims of the present study were reviewed and approved by the Institutional Review Board (IRB) at An-Najah National University. To identify the most important species used, the use value (UV) index was employed, while the SPSS program was used to analyze the data. Collected data revealed that 13 medicinal plants are utilized, while 12 plants are not used during pregnancy. Moreover, 15 plants are utilized and 9 plants are not used during lactation for treating and dealing with various problems. The most commonly used plants belonged to 14 families, including Lamiaceae, Apiaceae, Leguminosae, and Rubiaceae. The plants most used during pregnancy were sage (Salvia fruticosa), anise (Pimpinella anisum), and peppermint (Mentha × piperita). Castor (Ricinus communis) oil, ginger (Zingiber officinale), saffron (Crocus sativus), and senna (Senna alexandrina) mostly were not used by pregnant women. Moreover, cinnamon (Cinnamomum verum), anise (P. anisum), peppermint (M. piperita), and sage (S. fruticosa) were mostly used during lactation. Castor (R. communis) oil, ginger (Z. officinale), garlic (Allium sativum), and aloe (Aloe vera) mostly were not used during lactation. This study is of great importance in order to decrease the possibility of endangering the lives of fetuses and infants. A combined effort among researchers, scientists, lactating women, and pregnant women may help in changing wrong uses and thoughts about medicinal plants and help to improve the overall health of both mother and fetus.
Palestine is a holy land for Christians, Jews, and Muslims, and many civilizations have passed through this land over time (Canaanite, British, Jewish, Roman, etc.). This has led to the exposure todiverse cultures, especially in the use of medicinal plants, folkloric foods, and cosmetics. Due to the geographical location of Palestine in the Mediterranean region, it has many distinctive characteristics, including fertile soil and a moderate climate (Mendelssohn and Yom-Tov, 1999; Lev, 2006). In addition, Palestine was and still is a very important crossroad of trade between the East and the West, adding a special characteristic to the use of medicinal plants (Azaizeh et al., 2006; Azaizeh et al., 2010; Ben-Arye and Samuels, 2015), especially among pregnant and lactating women. Evidence of the ancient use of medicinal plants in the Mediterranean region was found in a cave from about 60,000 years ago (Saad et al., 2005).
In recent years, people in developing and advanced countries have used medicines that originate from natural sources to improve the quality of their life (Schoen et al., 2007). The use of plants during pregnancy and lactation differs from woman to woman due to the environment in which they live, their income, knowledge in phototherapeutic products, and side effects (Gluckman et al., 2015). Based on a literature review, there are few studies or clinical trials on the safety and efficacy of using herbs during pregnancy and lactation in the West Bank area of Palestine (Jaafari et al., 2016; Ahmed et al., 2017; Ung et al., 2017).
The use of plants by pregnant and lactating mothers without awareness of their harmful effects exposes both mother and fetus or baby to great dangers, like abortion, premature term, uterine bleeding, and physical and mental retardation of the fetus (Holst et al., 2009; John and Shantakumari, 2015). The most sensitive period in pregnancy is the embryogenesis stage, in which tissues differentiate and organogenesis occurs, so teratogenicity is higher (Dennery, 2007). Many physiological changes happen during pregnancy, which may cause nausea, vomiting, heartburn, constipation, hypertension, peripheral edema, hemorrhoids, and varicose veins (Moreira et al., 2014; Paupério et al., 2014).
In addition, there are changes during lactation, such as transient hair loss, postpartum depression, and changes in the skin (Beicovrtch, 1987). Because of these changes, pregnant and lactating women consider treating these issues with safe methods that avoid medications, which may include plants. The safest approach to provide substantial relief for common symptoms is using plants, which do not have strict regulations like modern medicine and are increasingly used (Lewis and Elvin-Lewis, 2003; Teschke and Eickhoff, 2015). Thus, it is important to understand the extent to which plant treatments are used, as well as the specific products used, the reason for which they are used, and factors that may predict which women are least likely to use them.
An ethnopharmacological survey (cross-sectional observational design study) using a pre-piloted questionnaire (Supplementary Material) was undertaken on herbal remedies used by pregnant and lactating women in the West Bank area of Palestine (Tulkarm, Nablus, Tubas, Jenin, Qalqilya, Salfeit, Jericho, Ramallah, Bethlehem, Jerusalem, and Hebron). Table 1 presents the socio-demographic characteristics of the participants, who were interviewed in the period from November 2017 to February 2018. A convenience sample method was used as an approach to the survey. The anonymous survey was piloted and reviewed in order to help in understanding, validating, clarifying, and producing a reliable study. The interviews were conducted by five trained researchers, who interviewed and collected the questionnaires from the study participants face to face in Arabic, the local language of the informants. The duration of the interviews ranged from 30 to 45 min, with one visit per interviewee in each case.
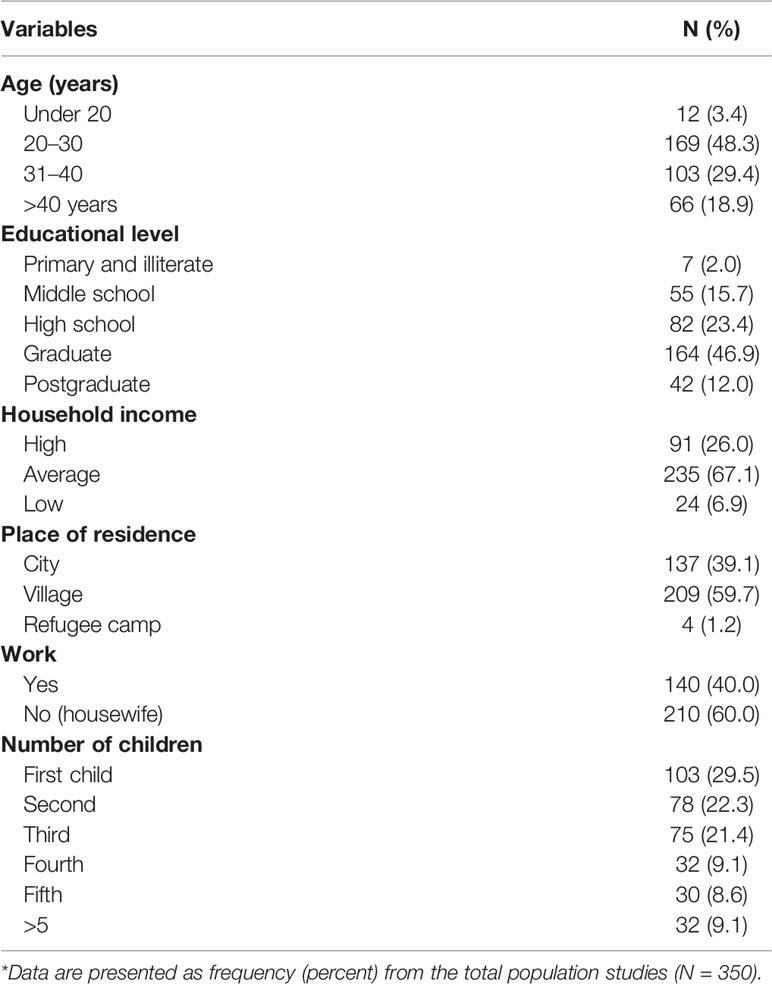
Table 1 Socio-demographic characteristics of the study population (N = 350).
The informed consent forms, ethics, and aims of the present study were reviewed and approved by the Institutional Review Board (IRB) at An-Najah National University (IRB archived number [20] October 2017).
The pre-piloted and validated questionnaires were administered through personal contact. This method is an effective and easy option for data collection. The objective of this survey was to obtain information on several issues, including (i) the names of plants commonly used during pregnancy and lactation, (ii) the period of pregnancy when the herbs are used, (iii) the methods of preparing the herbs, (iv) the reasons for using the herbs, and (v) problems that occurred during the use of these herbs. In most cases, the interviews often started in the form of informal discussions to achieve the confidence of the interviewees. The study was conducted in accordance with the current Good Clinical Practice (GCP) Guidelines (EME, 1997) and the requirements of the declarations of Helsinki (World Medical Association, 2008) and the International Conference on Harmonization (ICH, 1996) Guidelines. Written informed consent was obtained from the participants. In addition, the interviewed women signed a free, prior, and informed consent form, and to protect their interest, they were informed by the researchers in detail about the current study and its purposes. The women were not offered any incentives, and they were able to withdraw from the study at any time.
All of the plants were identified by the pharmacognosist Dr Nidal Jaradat after they were collected from the interviewees and kept in special glass frames. To verify and confirm the identity of each plant species stated by the interviewees, photographs and live specimens were used. Medicinal use was accepted as valid only if it was mentioned by at least three women. A herbarium specimen number was given for each sample of the collected herbs, as shown in Table 2, and voucher samples were kept at the Pharmacognosy Laboratory of the Department of Pharmacy, Faculty of Medicine and Health Sciences, An-Najah National University.
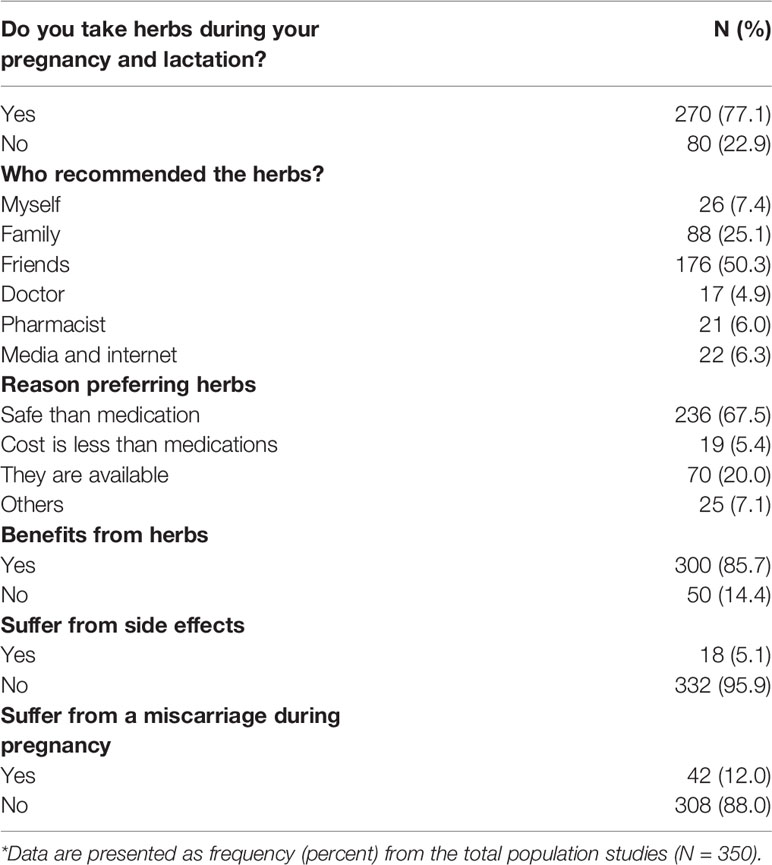
Table 2 Do you take herbs during your pregnancy and lactation.
The use value (UV) is a quantitative value that can be used in order to show the relative importance of plant species known locally. It is calculated based on the following equation:
where UV is the use value of plant species, n is the number of informants, and U is the number of citations per plant species (Friedman et al., 1986).
The significance of medicinal plant families was assessed using the family use values (FUV), which were calculated according to the following equation:
where UVs = use values of the taxa, and ns = total number of species within each family, which were used for the specific condition in the West Bank area of Palestine (Pieroni et al., 2004).
The Statistical Package for Social Sciences (SPSS version 17.0) and Microsoft Excel 2010 were used for the analysis of the data presented in this study. The significant association and the relation between different variables were evaluated using Pearson's correlation chi-square, with a significance level of p ≤ 0.05.
Three hundred and fifty women were interviewed in the current survey, and questionnaires were completed. The socio-demographic characteristics are summarized in Table 1. The majority of respondents (48.3%) are 20–30 years of age and have various educational backgrounds, but most of them (46.9%) had a university education, while a minority (2.0%) of respondents was between the primary and illiterate levels of education. This ratio of illiterate versus university graduate women who participated in this study fits well with the most recent status of education in Palestine. Moreover, household income was sampled, and the majority of the participants have an average income (67.1%). In addition, most live in villages (59.7%), and 60.0% of the women who participated in the study are housewives. Knowledge about natural products was also investigated; indeed, the majority of the informants (77.1%) used herbs. Most of them (67.5%) used herbal plants because they believe they are safer than medications. Table 2 shows that most mothers (67.5%) used the plants because they believe they are safer than medications during pregnancy and lactation, and most of them obtained information from relatives and friends (50.3%) and family members (25.1%).
In a survey regarding the use of herbal plants by pregnant and lactating women in Palestine, a total of 30 plant species distributed across 19 families were reported as locally traditionally used, which are presented in different tables according to their use. All families reported in this study are explained in Tables 3–6. Overall, the most commonly used FUV families were Apiaceae, Lamiaceae, and Leguminosae, respectively, with only one plant species reported for the remaining families.
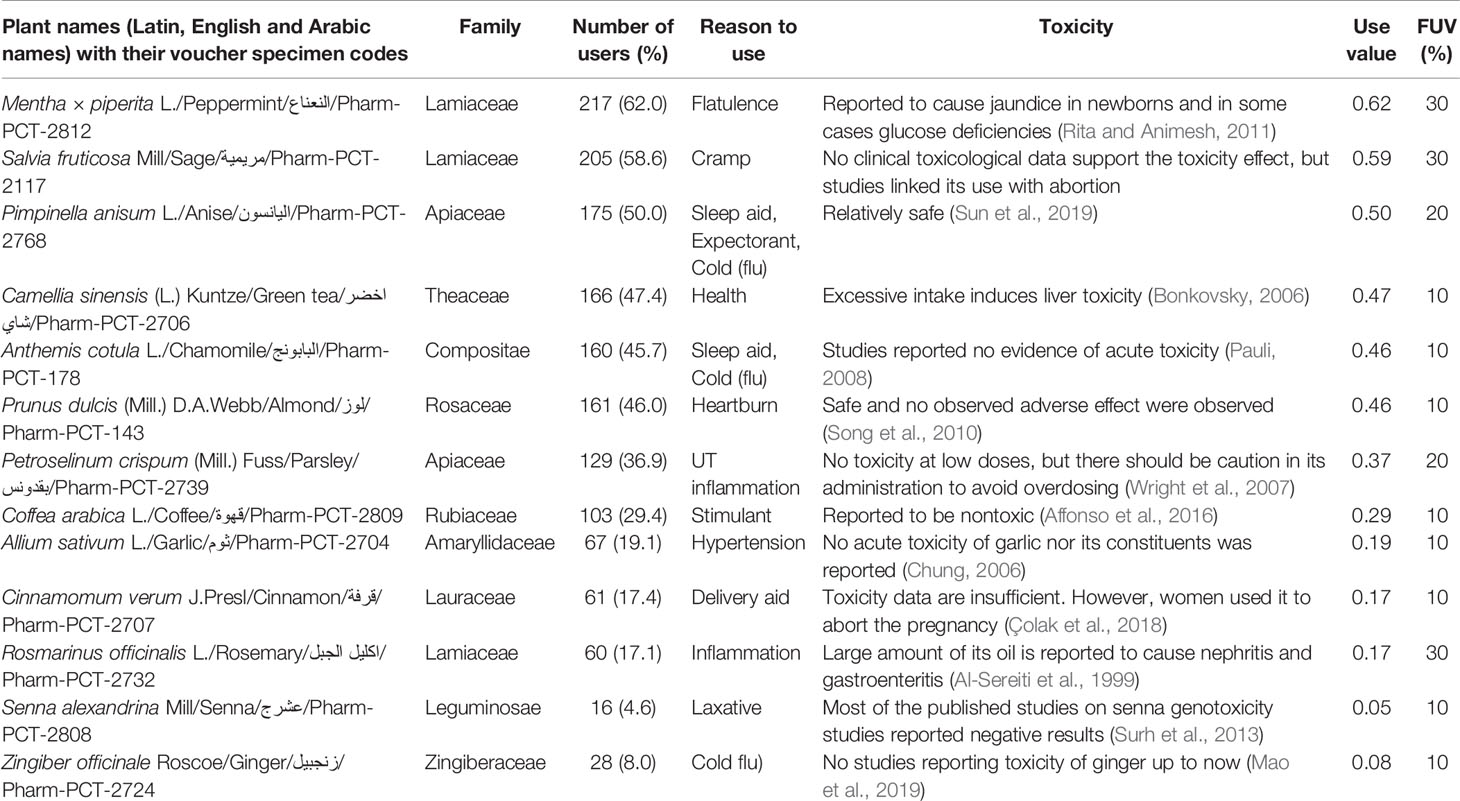
Table 3 Medicinal plants used during pregnancy.
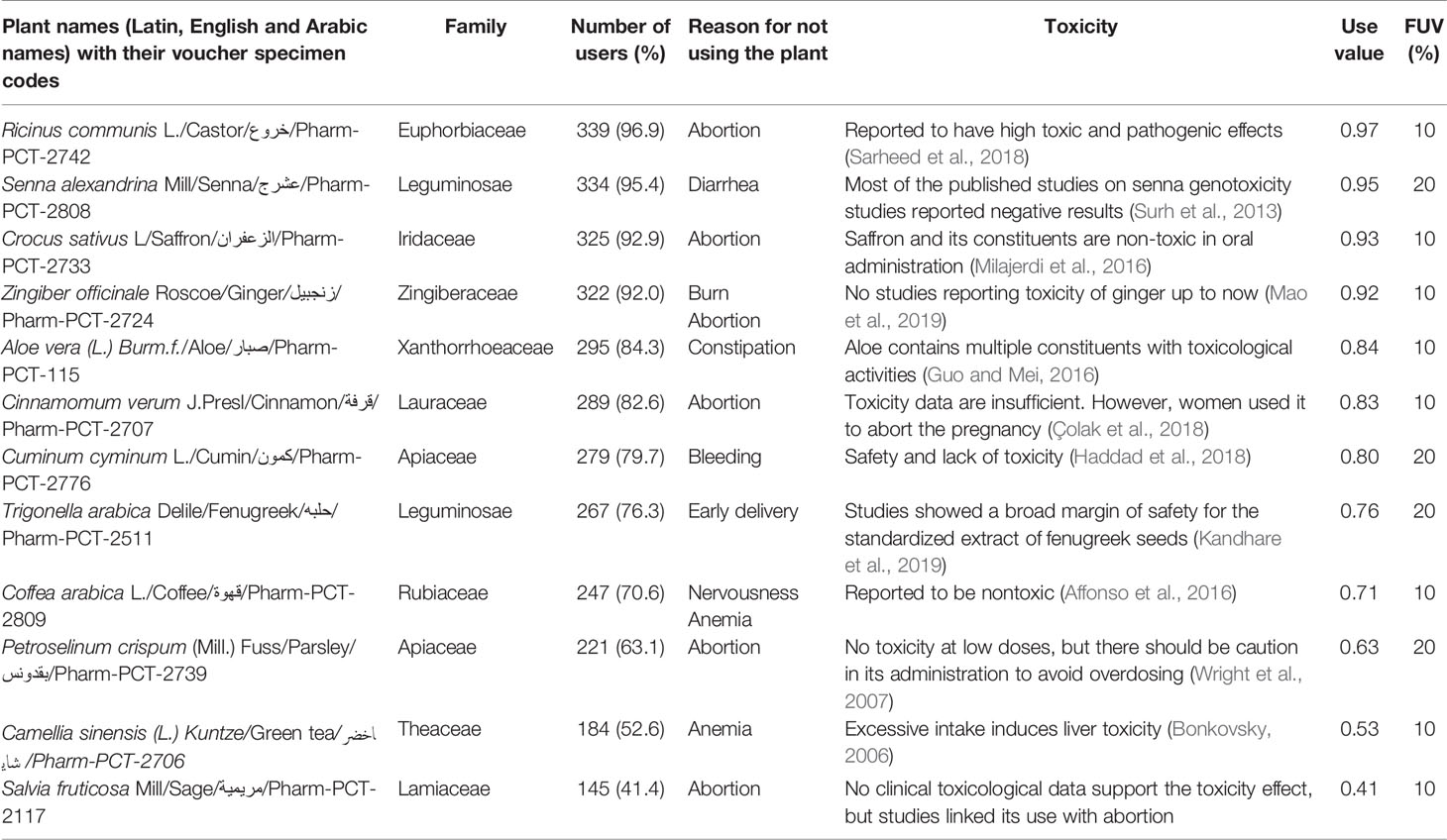
Table 4 Medicinal plants not used during pregnancy.
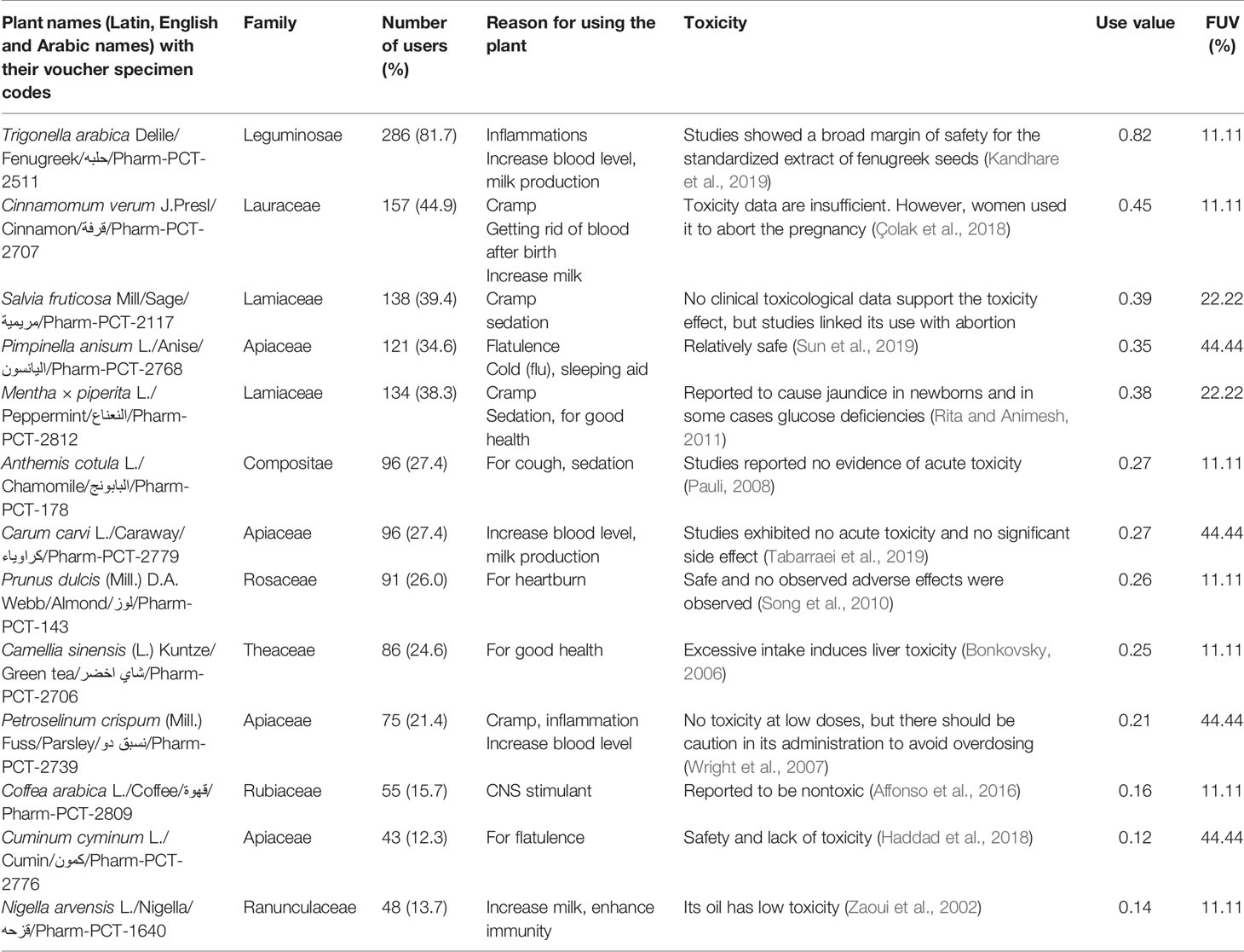
Table 5 Medicinal plants used during lactation.
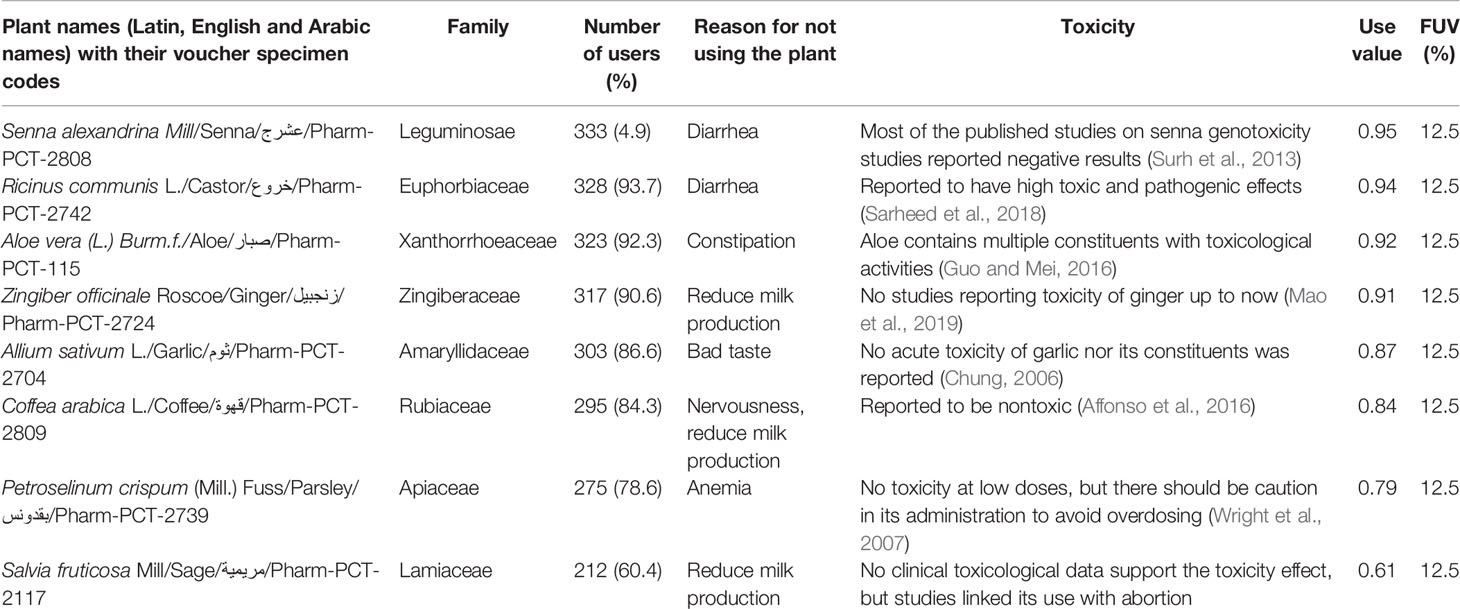
Table 6 Medicinal plants which cannot be used during lactation.
However, the current survey results revealed that peppermint (Mentha × piperita), sage (Salvia fruticosa), and anise (Pimpinella anisum) are the most used plants during pregnancy, with UV values of 0.62, 0.59, and 0.50, respectively, as presented in Table 3. Table 4 shows that castor (Ricinus communis), senna (Senna alexandrina), and saffron (Crocus sativus) are the least used plants during pregnancy, with UV values of 0.97, 0.95, and 0.93, respectively. Moreover, Table 5 shows that fenugreek (Trigonella arabica), cinnamon (Cinnamomum verum), and sage (S. fruticosa) are the most utilized plants during lactation, with UV values of 0.82, 0.45, and 0.39, respectively. Finally, Table 6 reveals that senna (S. alexandrina), castor (R. communis), and aloe (Aloe vera) are the least utilized plants during lactation, with UV values of 0.95, 0.94, and 0.92, respectively.
Table 3 presents the plants that were cited by the pregnant participants with the number of users, the UV, and the reason for using the plant. Peppermint (M. piperita) was reported to be used to control flatulence and for calming, with the highest UV of 0.62, followed by sage (S. fruticosa) used for digestive problems, including cramps and loss of appetite, with a UV of 0.59. Other plants were reported for different uses, such as cinnamon (C. verum) reported to be used for delivery aid, and other herbs that may act as stimulants, such as coffee (Coffea arabica). Senna (S. alexandrina) was reported to be used as a laxative, with the lowest UV among other plants reported. In addition, ginger (Zingiber officinale), chamomile (Anthemis cotula), and anise (P. anisum) were reported to be used for the treatment of flu and its symptoms. Heath green tea (Camellia sinensis) was one of the best plants used. Garlic (Allium sativum) was reported to be used by participants for hypotension. Parsley (Petroselinum crispum) and rosemary (Rosmarinus officinalis) act as pain relievers with anti-inflammatory properties. Almond (Prunus dulcis) was reported to be used to prevent or reduce heartburn. Cinnamon (C. verum), senna (S. alexandrina), and ginger (Z. officinale) were infrequently reported by the participants and had the lowest UV, which was explained when they were presented with high UV in Table 4, which shows the least used plants by the participants.
Those with a negative attitude toward the use of medicinal plants suggested that herbal drugs are not pure or clean; they cause more adverse effects and have no clearly defined dosages, such that a few of the plants are included and presented in Table 4. Some plants should be avoided by pregnant women due to possible abortion-inducing effects, such as sage (S. fruticosa), cinnamon (C. verum), castor (R. communis), ginger (Z. officinale), parsley (P. crispum), and saffron (C. sativus). Castor (R. communis), senna (S. alexandrina), saffron (C. sativus), ginger (Z. officinale), and cinnamon (C. verum) were reported with the highest UV (0.97, 0.95, 0.93, 0.92, and 0.85, respectively), due to their direct influence on the pregnancy. Too much caffeine can lead to nervousness and iron deficiency, which can cause anemia. Moreover, caffeine isolated from coffee (C. arabica) and green tea (C. sinensis) can inhibit the absorption of calcium and iron. In addition, the use of too much senna (S. alexandrina) for the treatment of constipation may lead to diarrhea and spasm. Fenugreek (Trigonella arabica) is a plant that may cause early delivery. Other plants were reported for different reasons, while those reported as directly responsible for abortion were sage (S. fruticosa), cinnamon (C. verum), castor (R. communis), ginger (Z. officinale), fenugreek (T. arabica), parsley (P. crispum), and saffron (C. sativus).
Tables 5 and 6 present plants that were used or not used by lactating women. From Table 5, it is observed that most of the plants were used for similar reasons, such as increasing milk production, improving health by increasing the blood level, and helping to get rid of symptoms after birth. Cinnamon (C. verum), sage (S. fruticosa), peppermint (M. piperita), and anise (P. anisum) were the highest reported, with UV of 0.45, 0.39, 0.38, and 0.35, respectively. Cumin (Cuminum cyminum) had the lowest UV of 0.12. Sage (S. fruticosa), peppermint (M. piperita), cinnamon (C. verum), and parsley (P. crispum) were reported to be used for the treatment of cramps. For sleep induction, sage (S. fruticosa), peppermint (M. piperita), anise (P. anisum), and chamomile (A. cotula) were used. In addition, to increase milk production, women took caraway (Carum carvi), nigella (Nigella arvensis), cinnamon (C. verum), and fenugreek (T. arabica). To increase blood level, they used caraway (C. carvi), parsley (P. crispum), and fenugreek (T. arabica). For cold and flu, they took anise (P. anisum) and rosemary (R. officinalis). Chamomile (A. cotula) was also used as an antitussive, and nigella (N. arvensis) was used to boost immunity and to aid in getting rid of blood after birth.
Table 6 shows the plants that cannot be used, mostly for the same reason, which directly or indirectly influence the production of milk. For example, they do not use coffee (C. arabica) because it causes nervousness and decreases milk. Castor (R. communis) and senna (S. alexandrina) cause diarrhea. Parsley (P. crispum) causes anemia. Fenugreek (T. arabica) makes the milk taste bad. Sage (S. fruticosa) and ginger (Z. officinale) were highlighted by the participants as reducing milk. Senna (S. alexandrina) and castor (R. communis) were reported with the highest UV of 0.95 and 0.94, respectively, for causing diarrhea, indirectly influencing the production of milk by the impact on overall health.
Table 7 summarizes the parts used and the method of preparation of plants used during pregnancy and lactation. Seeds and leaves were the most used parts of all the plants. Boiling with water was the most common preparation method, while a few plants were eaten without boiling or other preparation methods.
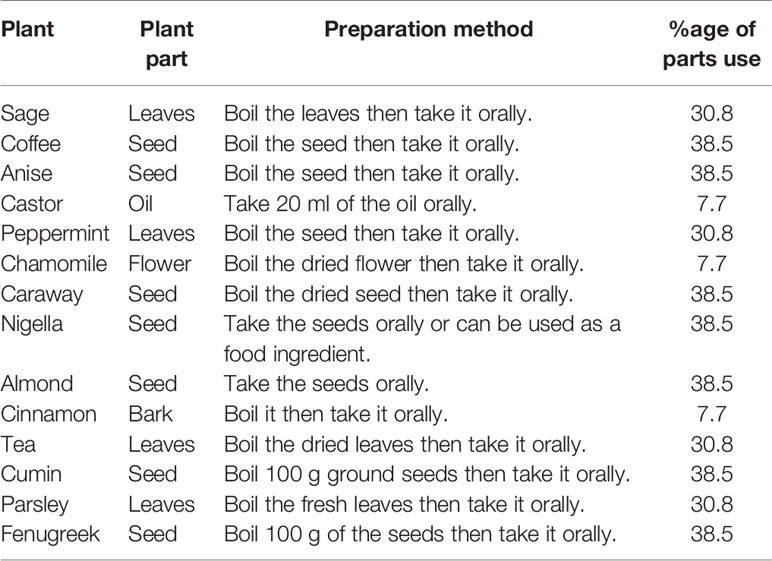
Table 7 Plant products, parts used and preparation methods.
Usually, most of the communities used herbal remedies based on their experience or on the advice of relatives or friends. Therefore, it is necessary to find out the correct scientific evidence for the use, which may help form a correct understanding toward plants. From Table 3, it is concluded that anise (P. anisum), sage (S. fruticosa), and peppermint (M. piperita) were mostly used by pregnant women for the reasons that were mentioned earlier in the results and according to different studies, which found that peppermint (M. piperita) tea can be used to treat cramps (Rodriguez-Fragoso et al., 2008; Herro and Jacob, 2010; Taheri et al., 2011).
Anise (P. anisum) can be used for stomach upset (Liu et al., 2008) and intestinal gases (Myers et al., 2009) and as an expectorant (Gradinaru et al., 2014). According to Table 4, castor oil (R. communis), ginger (Z. officinale), saffron (C. sativus), and senna (S. alexandrina) mostly were not used during pregnancy. However, the most common reason for using castor oil (R. communis) during pregnancy is for labor induction (Kelly et al., 2013). Abortion occurs mostly during the first 24 h after taking castor oil (R. communis); common side effects are vomiting, diarrhea, and nausea. Nausea commonly occurs among pregnant women, and ginger (Z. officinale) can be used to solve this problem, but not for vomiting (Bryer, 2005).
Studies show that saffron (C. sativus) can adversely affect the growth of fetuses and induce several fetal malformations, noticeably skeletal malformations (Osgerby et al., 2002). Great caution should be taken when saffron (C. sativus) is used during pregnancy. Senna (S. alexandrina) has a strong effect, as it stimulates the uterus and affects fetal cell development. Long-term use, frequent use, or use of high doses has been linked to serious side effects, including laxative dependence and liver damage (Vanderperren et al., 2005).
As shown in Table 5, cinnamon (C. verum), anise (P. anisum), peppermint (M. piperita), and sage (S. fruticosa) were mostly used during lactation. Studies have affirmed that cinnamon (C. verum) has many benefits, including management of blood glucose levels (Hlebowicz et al., 2007), weight loss (Whitfield et al., 2016), detoxification (Xing et al., 2014), and increasing the amount of milk (Guler and Seker, 2009; Dog, 2009), but it should not be combined with fenugreek (T. arabica) because it can lower blood pressure (Talpur et al., 2005). Anise (P. anisum) can be used to increase the amount of milk (Kent et al., 2012), for constipation and irritable bowel syndrome (Mercadante et al., 2011; Mosaffa-Jahromi et al., 2016), and to induce sleep (Marinov and Valcheva-Kuzmanova, 2015). Peppermint (M. piperita) is mainly used to induce calming and relaxing effects (Cook and Lynch, 2008). Sage (S. fruticosa) is not used for increasing the amount of milk, but it can be used for abdominal pain, occasional nausea, and vomiting (Boone and Shields, 2005; Wilhelm et al., 2007).
There are contradictory opinions regarding the medicinal effect of parsley (P. crispum) and its effect as an abortifacient product. For example, in a study conducted on pigs, Chaudhary et al. (1986) found that photodermatitis occurred due to the presence of furocoumarins. Moreover, Awe and Banjoko (2013) reported that P. crispum ethanol leaf extract exhibited hepatotoxic and nephrotoxic activities. A study on P. crispum oil (0.6 ml/kg body weight) showed protective activity against zearalenone-induced reproductive toxicity and improved testosterone levels in mature male mice (Salah-Abbès et al., 2009). In addition, P. crispum ethanol seed extract (5 mg/kg) reduced the dysfunction in rat kidney caused by prostadin-induced abortion via immunohistochemical and immunofluorescent staining and biochemical analysis (Rezazad and Farokhi, 2014). Moreover, parsley (P. crispum) herb and root have approval status by the German Commission E for the urinary tract and kidney stones (Nathan and Scholten, 1999).
Apiol is the major component of parsley (P. crispum) essential oil, and its preparations have no legitimate use in therapeutics. The dangers associated with their use, especially in the haphazard and unrestricted dosages in attempts at abortion, have provoked legislation making such preparations available for sale by prescription only. It is common knowledge that this regulation is being flouted (Quinn et al., 1958). However, the apiol essential oil abortifacient effect has been documented in hospitals. For example, an unmarried primiparous 23-year-old woman was admitted to a hospital with an inevitable abortion. She menstruated regularly every 28 days, the last period being on June 15, 1973. She purchased a box of abortifacient capsules, which, according to the box, contained “Ferri carbonas saccharatus 2.55 gr; aloe 0.2 gr; tansy OS l gr; oleum pulegii 0.13 gr; apiol 0.13 gr; ferri oxydum praecipitatum rubrum 0.25 gr” (David and Randall, 1974). In fact, in medicine, apiole has been used for the treatment of menstrual disorders and as an abortifacient. It is an irritant, and, in high doses, it can cause liver and kidney damage. Cases of death due to attempted abortion using apiole have been reported (Amerio et al., 1968). The question of how apiole may cause abortion is unclarified; however, Rodolfo Marri, after conducting an experiment on isolated rabbit and guinea pig uteri, found an increase in strength and tone of contraction after the consumption of a small dose, while a large dose had a depressing effect on the uterus (Shorter, 2017).
Finally, Table 6 shows most of the medicinal plants that are not used by lactating women. These plants were castor oil (R. communis), ginger (Z. officinale), garlic (A. sativum), and aloe (A. vera). Traditionally, lactating women do not use castor oil (R. communis), as it causes diarrhea, which they thought will influence milk production due to the loss of fluids and nutrition during diarrhea. This traditional knowledge is in line with the scientific fact that castor oil (R. communis) is usually used as a laxative (Umukoro and Ashorobi, 2005; Ezenwali et al., 2010), but scientifically, castor oil (R. communis) should not be used during lactation for a more serious reason, as castor seeds (R. communis) contain a toxic glycoprotein called ricin, which has the ability to agglutinate blood cells. It is taken into cells by endocytosis and causes acute cell death by inactivation of ribosomal RNA, inhibiting protein synthesis. Ricin is approximately 1,000-fold more toxic following parenteral administration or inhalation than by the oral route because of its destruction in the intestine (Alexander et al., 2008). The women do not use ginger (Z. officinale), as they think it reduces milk production, while a prior investigation shows that if ginger (Z. officinale) is used immediately postpartum, it can improve milk production (Paritakul et al., 2016). More studies are needed to determine the effect of ginger (Z. officinale) on milk production at greater than 3 days postpartum.
Human milk is not just a complex mixture of substances that best meets the nutritional requirements of the infant; the flavor of human milk is altered when lactating women eat sulfur-containing foods such as garlic (A. sativum). When human milk is flavored with garlic (A. sativum), infants breastfeed longer and suck more overall than they do when this flavor is absent, at least under conditions in which the mothers have been ingesting bland diets for several days. However, garlic (A. sativum) appears to be safe in amounts usually used in food preparation. Garlic (A. sativum) may change the smell of breast milk and affect a baby's feeding. There is no information on the safety of garlic (A. sativum) supplements in breastfeeding (Mennella and Beauchamp, 1993).
Aloe (A. vera) gel is used to help heal cracked nipples (Eghdampour et al., 2013; Saeidi et al., 2015); however, it is better to remove aloe (A. vera) gel from the nipple areas before feeding the baby, because the bitter taste of the aloe (A. vera) gel may influence the baby's feeding. Aloe (A. vera) latex is a yellow-colored liquid that comes from the inner skin of the aloe (A. vera) leaf. It can be taken orally in both dried and liquid forms. Aloe (A. vera) latex should be avoided, as it has a strong laxative effect (Sim et al., 2013).
In conclusion, it is found that sometimes there were differences between traditional and scientific uses of herbal remedies during pregnancy and lactation. For example, traditional use of anise (P. anisum) differed greatly from its scientific uses for stomach upset and intestinal gases, as an expectorant, and to increase the amount of milk. In addition, ginger (Z. officinale) can be used for nausea, but a burning sensation prevents pregnant women from using it. Moreover, some herbal remedies should be avoided, like senna (S. alexandrina), which can stimulate the uterus and affect fetal cell development, and castor oil (R. communis), which leads to abortion. Traditionally, it is thought that saffron (C. sativus) can cause abortion, but it adversely affects the growth of the fetus and induces several malformations. Cinnamon (C. verum) is traditionally used for cramping, but scientifically it is used for weight loss, detoxification, and an increased amount of milk. Peppermint (M. piperita) is medicinally used for calming and relaxation, but there is no reason for using it traditionally. Sage (S. fruticosa) is used traditionally for cramping, and medicinally it can be taken for occasional nausea and vomiting. Ginger (Z. officinale) is traditionally prohibited, as it is thought to decrease milk production, but studies have showed that the immediate postpartum use of ginger (Z. officinale) can improve milk volume. Finally, garlic (A. sativum) was not used for its bad taste and smell, as it changes the smell of breast milk and affects the baby's feeding. Therefore, the community, especially pregnant and lactating women, should be educated regarding the correct usage of medicinal plants during pregnancy and lactation in order to decrease the possibility of endangering the lives of fetuses and infants.
All datasets generated for this study are included in the article/Supplementary Material.
The studies involving human participants were reviewed and approved by the Institutional Review Board (IRB) - An-Najah National University. The patients/participants provided their written informed consent to participate in this study.
Study conception and design: AE. Acquisition, analysis and/or interpretation of data: AE, NJ. Final approval and overall responsibility for this published work: AE, NJ.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2020.00046/full#supplementary-material
Çolak, Ç., Elibol, E., Demir, T., Kıvçak, B. (2018). Overdose of Cinnamon Barks Is the Cause of Poisoning in the Gediatric Patient: Case Report. J. US-Chin. Med. Sci. 15, 26–28. doi: 10.17265/1548-6648/2018.01.004
Affonso, R. C. L., Voytena, A. P. L., Fanan, S., Pitz, H., Coelho, D. S., Horstmann, A. L., et al. (2016). Phytochemical composition, antioxidant activity, and the effect of the aqueous extract of coffee (Coffea arabica L.) bean residual press cake on the skin wound healing. Oxid. Med. Cell. Longev 2016, 10. doi: 10.1155/2016/1923754
Ahmed, M., Hwang, J. H., Choi, S., Han, D. (2017). Safety classification of herbal medicines used among pregnant women in Asian countries: a systematic review. BMC Complement. Altern. Med. 17, 489. doi: 10.1186/s12906-017-1995-6
Alexander, J., Benford, D., Cockburn, A., Cravedi, J.-P., Dogliotti, E., Domenico, A. D., et al. (2008). ). Theobromine as undesirable substances in animal feed-scientific opinion of the panel on contaminants in the food chain. EFSA J. 725, 1–66. doi: 10.2903/j.efsa.2008.725
Al-Sereiti, M., Abu-Amer, K., Sena, P. (1999). Pharmacology of rosemary (Rosmarinus officinalis Linn.) and its therapeutic potentials. Indian J. Exp. Biol. 37, 124–130.
Amerio, A., De Benedictis, G., Leondeff, J., Mastrangelo, F., Coratelli, P. (1968). Nephropathy due to apiol. Minerva Nefrol 15, 49–70.
Awe, E. O., Banjoko, S. O. (2013). Biochemical and haematological assessment of toxic effects of the leaf ethanol extract of Petroselinum crispum (Mill) Nyman ex AW Hill (Parsley) in rats. BMC Complem. Altern. Med. 13, 75. doi: 10.1186/1472-6882-13-75
Azaizeh, H., Saad, B., Khalil, K., Said, O. (2006). The state of the art of traditional Arab herbal medicine in the Eastern region of the Mediterranean: a review. Evid. Based Complement. Alternat. Med. 3, 229–235. doi: 10.1093/ecam/nel034
Azaizeh, H., Saad, B., Cooper, E., Said, O. (2010). Traditional Arabic and Islamic medicine, a re-emerging health aid. Evid. Based Complement. Alternat. Med. 7, 419–424. doi: 10.1093/ecam/nen039
Beicovrtch, F. B. (1987). Female weight and reproductive condition in a population of olive baboons (Papio anubis). Am. J. Primatol. 12, 189–195. doi: 10.1002/ajp.1350120206
Ben-Arye, E., Samuels, N. (2015). Homeopathy on the crossroads of traditional and integrative medicine in the Middle-East. J. Med. Person 13, 65–71. doi: 10.1007/s12682-014-0196-z
Bonkovsky, H. L. (2006). Hepatotoxicity associated with supplements containing Chinese green tea (Camellia sinensis). Ann. Intern. Med. 144, 68. doi: 10.7326/0003-4819-144-1-200601030-00020
Boone, S. A., Shields, K. M. (2005). Treating pregnancy-related nausea and vomiting with ginger. Ann. Pharmacother. 39, 1710–1713. doi: 10.1345/aph.1G086
Bryer, E. (2005). A literature review of the effectiveness of ginger in alleviating mild-to-moderate nausea and vomiting of pregnancy. J. Midwifery Womens Health 50, 1–3. doi: 10.1016/j.jmwh.2004.08.023
Chaudhary, S., Ceska, O., Tétu, C., Warrington, P., Ashwood-Smith, M., Poulton, G. (1986). Oxypeucedanin, a major furocoumarin in parsley, Petroselinum crispum. Planta Med. 52, 462–464. doi: 10.1055/s-2007-969254
Chung, L. Y. (2006). The antioxidant properties of garlic compounds: allyl cysteine, alliin, allicin, and allyl disulfide. J. Med. Food 9, 205–213. doi: 10.1089/jmf.2006.9.205
Cook, N., Lynch, J. (2008). Aromatherapy: reviewing evidence for its mechanisms of action and CNS effects. Br. J. Neurosci. Nurs. 4, 595–601. doi: 10.12968/bjnn.2008.4.12.31963
David, T., Randall, S. (1974). Fetal malformations: A hazard of attempted abortion. Forensic. Sci. 4, 71–73. doi: 10.1016/0300-9432(74)90079-X
Dennery, P. A. (2007). Effects of oxidative stress on embryonic development. Birth Defects Res. C. Embryo Today 81, 155–162. doi: 10.1002/bdrc.20098
Dog, T. L. (2009). The use of botanicals during pregnancy and lactation. Altern. Ther. Health Med. 15, 54–58.
Eghdampour, F., Jahdie, F., Kheyrkhah, M., Taghizadeh, M., Naghizadeh, S., Hagani, H. (2013). The impact of Aloe vera and calendula on perineal healing after episiotomy in primiparous women: a randomized clinical trial. J. Caring Sci. 2, 279–286. doi: 10.5681/jcs.2013.033
Ezenwali, M., Njoku, O., Okoli, C. (2010). Studies on the anti-diarrheal properties of seed extract of Monodora tenuifolia. Int. J. App. Res. Nat. Prod 2, 20–26. doi: 10.1.1.863.2948
Friedman, J., Yaniv, Z., Dafni, A., Palewitch, D. (1986). A preliminary classification of the healing potential of medicinal plants, based on a rational analysis of an ethnopharmacological field survey among Bedouins in the Negev Desert, Israel. J. Ethnopharmacol. 16, 275–287. doi: 10.1016/0378-8741(86)90094-2
Gluckman, P., Hanson, M., Seng, C. Y., Bardsley, A. (2015). Nutrition and lifestyle for pregnancy and breastfeeding (USA: Oxford University Press). doi: 10.1093/med/9780198722700.001.0001
Gradinaru, A. C., Miron, A., Trifan, A., Spac, A., Brebu, M., Aprotosoaie, A. C. (2014). Screening of antibacterial effects of anise essential oil alone and in combination with conventional antibiotics against Streptococcus pneumoniae clinical isolates. Rev. Med. Chir. Soc Med. Nat. Iasi 118, 537–543.
Guler, S., Seker, M. (2009). The effect of cinnamon and guar gum on bacillus cereus population in milk. J. Food Process. Preserv 33, 415–426. doi: 10.1111/j.1745-4549.2009.00417.x
Guo, X., Mei, N. (2016). Aloe vera: A review of toxicity and adverse clinical effects. J. Environ. Sci. Health C 34, 77–96. doi: 10.1080/10590501.2016.1166826
Haddad, B., Bidgolia, S. A., Qomic, M., Asgarpanaha, J. (2018). Organ toxicity and estrogen like effects of cuminum cyminum. l seed essential oil: a hormonal, histopathological and immunohistochemical study in female mice. J. Pharm. Sci. 4, 1–11. doi: 10.20431/2455-1538.0402001
Herro, E., Jacob, S. E. (2010). Mentha piperita (peppermint). Dermatitis 21, 327–329. doi: 10.2310/6620.2011.10080
Hlebowicz, J., Darwiche, G., Björgell, O., Almér, L.-O. (2007). Effect of cinnamon on postprandial blood glucose, gastric emptying, and satiety in healthy subjects. Am. J. Clin. Nutr. 85, 1552–1556. doi: 10.1093/ajcn/85.6.1552
Holst, L., Wright, D., Haavik, S., Nordeng, H. (2009). The use and the user of herbal remedies during pregnancy. J. Altern. Complement. Med. 15, 787–792. doi: 10.1089/acm.2008.0467
Jaafari, M., Fotoohi, A., Razavi, N., Abdian Asl, A. (2016). Herbal medicine in pregnancy. Adv. Herb. Med. 2, 54–66.
John, L. J., Shantakumari, N. (2015). Herbal medicines use during pregnancy: a review from the Middle East. Oman Med. J. 30, 229–236. doi: 10.5001/omj.2015.48
Kandhare, A. D., Thakurdesai, P. A., Wangikar, P., Bodhankar, S. L. (2019). A systematic literature review of fenugreek seed toxicity by using ToxRTool: evidence from preclinical and clinical studies. Heliyon 5, e01536. doi: 10.1080/10590501.2016.1166826
Kelly, A. J., Kavanagh, J., Thomas, J. (2013). Castor oil, bath and/or enema for cervical priming and induction of labour. Cochrane Database Syst. Rev. 24. doi: 10.1002/14651858.CD003099.pub2
Kent, J. C., Prime, D. K., Garbin, C. P. (2012). Principles for maintaining or increasing breast milk production. J. Obstet. Gynecol. Neonatal Nurs. 41, 114–121. doi: 10.1111/j.1552-6909.2011.01313.x
Lev, E. (2006). Ethno-diversity within current ethno-pharmacology as part of Israeli traditional medicine–a review. J. Ethnobiol. Ethnomed. 2, 2–4. doi: 10.1186/1746-4269-2-4
Lewis, W. H., Elvin-Lewis, M. P. (2003). Medical botany: plants affecting human health (USA: John Wiley & Sons).
Liu, H., Qiu, N., Ding, H., Yao, R. (2008). Polyphenols contents and antioxidant capacity of 68 Chinese herbals suitable for medical or food uses. Food Res. Int. 41, 363–370. doi: 10.1016/j.foodres.2007.12.012
Mao, Q.-Q., Xu, X.-Y., Cao, S.-Y., Gan, R.-Y., Corke, H., Li, H.-B. (2019). Bioactive compounds and bioactivities of ginger (Zingiber officinale Roscoe). Foods 8, 185. doi: 10.3390/foods8060185
Marinov, V., Valcheva-Kuzmanova, S. (2015). Review on the pharmacological activities of anethole. Scr. Sci. Pharm. 2, 14–19. doi: 10.14748/ssp.v2i2.1141
Mennella, J. A., Beauchamp, G. K. (1993). The effects of repeated exposure to garlic-flavored milk on the nursling's behavior. Pediatr. Res. 34, 805–808. doi: 10.1203/00006450-199312000-00022
Mercadante, S., Ferrera, P., Casuccio, A. (2011). Effectiveness and tolerability of amidotrizoate for the treatment of constipation resistant to laxatives in advanced cancer patients. J. Pain Symptom Manage 41, 421–425. doi: 10.1016/j.jpainsymman.2010.04.022
Milajerdi, A., Djafarian, K., Hosseini, B. (2016). The toxicity of saffron (Crocus sativus L.) and its constituents against normal and cancer cells. J. Nutr. Intermed. Metabol 3, 23–32. doi: 10.1016/j.jnim.2015.12.332
Moreira, R. R. D., Camargo, F. R., Quílez, A. M., Salgueiro, L., Cavaleiro, C. (2014). Medicinal plants in pregnancy and lactation: perception of the health risk and practical educational group in Araraquara, São Paulo State. Brazil. J. Gen. Pract. 3, 1–6. doi: 10.4172/2329-9126.1000190
Mosaffa-Jahromi, M., Lankarani, K. B., Pasalar, M., Afsharypuor, S., Tamaddon, A.-M. (2016). Efficacy and safety of enteric coated capsules of anise oil to treat irritable bowel syndrome. J. Ethnopharmacol. 194, 937–946. doi: 10.1016/j.jep.2016.10.083
Myers, S. R., Hawrelak, J., Cattley, T. (2009). Essential oils in the treatment of intestinal dysbiosis: a preliminary in vitro study. Altern. Med. Rev. 14, 380–384.
Nathan, M., Scholten, R. (1999). The complete german commission e monographs: Therapeutic guide to herbal medicines. Ann. Intern. Med. 130, 459–459. doi: 10.7326/0003-4819-130-5-199903020-00024
Osgerby, J., Wathes, D., Howard, D., Gadd, T. (2002). The effect of maternal undernutrition on ovine fetal growth. J. Endocrinol. 173, 131–142. doi: 10.1677/joe.0.1730131
Paritakul, P., Ruangrongmorakot, K., Laosooksathit, W., Suksamarnwong, M., Puapornpong, P. (2016). The effect of ginger on breast milk volume in the early postpartum period: a randomized, double-blind controlled trial. Breastfeed. Med. 11, 361–365. doi: 10.1089/bfm.2016.0073
Pauli, A. (2008). Relationship between lipophilicity and toxicity of essential oils. Int. J. Essen. Oil Ther. 2, 60–68.
Paupério, A., Severo, M., Lopes, C., Moreira, P., Cooke, L., Oliveira, A. (2014). Could the Food Neophobia Scale be adapted to pregnant women? A Confirmatory factor Anal. In A Portuguese sample. Appetite 75, 110–116. doi: 10.1016/j.appet.2013.12.023
Pieroni, A., Quave, C. L., Villanelli, M. L., Mangino, P., Sabbatini, G., Santini, L., et al. (2004). Ethnopharmacognostic survey on the natural ingredients used in folk cosmetics, cosmeceuticals and remedies for healing skin diseases in the inland Marches, Central-Eastern Italy. J. Ethnopharmacol. 91, 331–344. doi: 10.1016/j.jep.2004.01.015
Rezazad, M., Farokhi, F. (2014). Protective effect of Petroselinum crispum extract in abortion using prostadin-induced renal dysfunction in female rats. Avicenna J. Phytomed 4, 312–319.
Rita, P., Animesh, D. K. (2011). An updated overview on peppermint (Mentha piperita L.). Int. Res. J. Pharm. 2, 1–10.
Rodriguez-Fragoso, L., Reyes-Esparza, J., Burchiel, S. W., Herrera-Ruiz, D., Torres, E. (2008). Risks and benefits of commonly used herbal medicines in Mexico. Toxicol. Appl. Pharmacol. 227, 125–135. doi: 10.1016/j.taap.2007.10.005
Saad, B., Azaizeh, H., Said, O. (2005). Tradition and perspectives of Arab herbal medicine: a review. Evid. Based Complement. Alternat. Med. 2, 475–479. doi: 10.1093/ecam/neh133
Saeidi, R., Tafazoli, M., Gholami, M., Mazloom, R. (2015). New treatment for nipple soreness in breastfeeding mothers: a clinical trial study. Iran. J. Neonatol. 6, 48–51. doi: 10.22038/IJN.2015.4495
Salah-Abbès, J. B., Abbès, S., Abdel-Wahhab, M. A., Oueslati, R. (2009). Raphanus sativus extract protects against zearalenone induced reproductive toxicity, oxidative stress and mutagenic alterations in male Balb/c mice. Toxicon 53, 525–533. doi: 10.1016/j.toxicon.2009.01.013
Sarheed, N. M., Kokas, O. F., Ridh, D. a. a. M. (2018). The toxicity of Castor beans and its treatment with Doxycycline in local rabbits. Int. J. Pharm. Qual. Assur 9, 1–16. doi: 10.25258/ijpqa.v9i2.13649
Schoen, C., Osborn, R., Doty, M. M., Bishop, M., Peugh, J., Murukutla, N. (2007). Toward higher-performance health systems: adults' health care experiences in seven countries, 2007: actual experiences with health care systems bring to light, and to life, the systemwide problems in these countries. Health Aff 26, 717–734. doi: 10.1377/hlthaff.26.6.w717
Shorter, E. (2017). Women"s bodies: a social history of women"s encounter with health, ill-health and medicine (USA: Routledge).
Sim, T. F., Sherriff, J., Hattingh, H. L., Parsons, R., Tee, L. B. (2013). The use of herbal medicines during breastfeeding: a population-based survey in Western Australia. BMC Complement. Altern. Med. 13, 317. doi: 10.1186/1472-6882-13-317
Song, Y., Wang, W., Cui, W., Zhang, X., Zhang, W., Xiang, Q., et al. (2010). A subchronic oral toxicity study of almond skins in rats. Food Chem. Toxicol. 48, 373–376. doi: 10.1016/j.fct.2009.10.025
Sun, W., Shahrajabian, M. H., Cheng, Q. (2019). Anise (Pimpinella anisum L.), a dominant spice and traditional medicinal herb for both food and medicinal purposes. Cogent Biol. 5, 1673688. doi: 10.1080/23312025.2019.1673688
Surh, I., Brix, A., French, J. E., Collins, B. J., Sanders, J. M., Vallant, M., et al. (2013). Toxicology and carcinogenesis study of senna in C3B6. 129F1-Trp53 tm1Brd N12 haploinsufficient mice. Toxicol. Pathol. 41, 770–778. doi: 10.1177/0192623312464304
Tabarraei, H., Hassan, J., Parvizi, M. R., Golshahi, H. (2019). Evaluation of the acute and sub-acute toxicity of the black caraway seed essential oil in Wistar rats. Toxicol. Rep. 6, 869–874. doi: 10.1016/j.toxrep.2019.08.010
Taheri, J. B., Azimi, S., Rafieian, N., Akhavan Zanjani, H. (2011). Herbs in dentistry. Int. Dent. J. 61, 287–296. doi: 10.1111/j.1875-595X.2011.00064.x
Talpur, N., Echard, B., Ingram, C., Bagchi, D., Preuss, H. (2005). Effects of a novel formulation of essential oils on glucose–insulin metabolism in diabetic and hypertensive rats: a pilot study. Diabetes Obes. Metab. 7, 193–199. doi: 10.1111/j.1463-1326.2004.00386.x
Teschke, R., Eickhoff, A. (2015). Herbal hepatotoxicity in traditional and modern medicine: actual key issues and new encouraging steps. Front. Pharmacol. 6, 72. doi: 10.3389/fphar.2015.00072
Umukoro, S., Ashorobi, R. (2005). Effect of aframomum melegueta. seed extract on castor oil–induced diarrhea. Pharm. Biol. 43, 330–333. doi: 10.1080/13880200590951748
Ung, C. O. L., Harnett, J., Hu, H. (2017). Community pharmacist's responsibilities with regards to traditional medicine/complementary medicine products: a systematic literature review. Res. Soc. Adm. Pharm. 13, 686–716. doi: 10.1016/j.sapharm.2016.08.001
Vanderperren, B., Rizzo, M., Angenot, L., Haufroid, V., Jadoul, M., Hantson, P. (2005). Acute liver failure with renal impairment related to the abuse of senna anthraquinone glycosides. Ann. Pharmacother. 39, 1353–1357. doi: 10.1345/aph.1E670
Whitfield, P., Parry-Strong, A., Walsh, E., Weatherall, M., Krebs, J. D. (2016). The effect of a cinnamon-, chromium-and magnesium-formulated honey on glycaemic control, weight loss and lipid parameters in type 2 diabetes: an open-label cross-over randomised controlled trial. Eur. J. Nutr. 55, 1123–1131. doi: 10.1007/s00394-015-0926-x
Wilhelm, S. M., Dehoorne-Smith, M. L., Kale-Pradhan, P. B. (2007). Prevention of postoperative nausea and vomiting. Ann. Pharmacother. 41, 68–78. doi: 10.1345/aph.1H398
Wright, C., Van-Buren, L., Kroner, C., Koning, M. (2007). Herbal medicines as diuretics: a review of the scientific evidence. J. Ethnopharmacol. 114, 1–31. doi: 10.1016/j.jep.2007.07.023
Xing, F., Hua, H., Selvaraj, J. N., Yuan, Y., Zhao, Y., Zhou, L., et al. (2014). Degradation of fumonisin B1 by cinnamon essential oil. Food Control 38, 37–40. doi: 10.1016/j.foodcont.2013.09.045
Keywords: medicinal plants, pregnancy, lactation, public health, ethnopharmacology
Citation: Eid AM and Jaradat N (2020) Public Knowledge, Attitude, and Practice on Herbal Remedies Used During Pregnancy and Lactation in West Bank Palestine. Front. Pharmacol. 11:46. doi: 10.3389/fphar.2020.00046
Received: 08 August 2019; Accepted: 14 January 2020;
Published: 14 February 2020.
Edited by:
Lyndy Joy McGaw, University of Pretoria, South AfricaReviewed by:
Christian Agyare, Kwame Nkrumah University of Science and Technology, GhanaCopyright © 2020 Eid and Jaradat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ahmad M. Eid, YWhtYWRlaWRAbmFqYWguZWR1; Nidal Jaradat, bmlkYWxqYXJhZGF0QG5hamFoLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.