
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol., 30 August 2018
Sec. Inflammation Pharmacology
Volume 9 - 2018 | https://doi.org/10.3389/fphar.2018.00914
This article is part of the Research TopicPharmacology of Autoimmune DiseaseView all 16 articles
 Xiao Cai1†
Xiao Cai1† Xiu-Min Chen1†Xuan Xia1Kun Bao1Rong-Rong Wang1Jian-Hong Peng2Hai-Jun Liu3Qiao-Wen Yang1Jing-Yao Yan1Mao-Jie Wang1,4
Xiu-Min Chen1†Xuan Xia1Kun Bao1Rong-Rong Wang1Jian-Hong Peng2Hai-Jun Liu3Qiao-Wen Yang1Jing-Yao Yan1Mao-Jie Wang1,4 Hua Yu5Jin-Jian Lu5
Hua Yu5Jin-Jian Lu5 Yuan-Jia Hu5
Yuan-Jia Hu5 Per-Johan Jakobsson6*Ze-Huai Wen1,7*
Per-Johan Jakobsson6*Ze-Huai Wen1,7* Run-Yue Huang1,8*Qing-Chun Huang1
Run-Yue Huang1,8*Qing-Chun Huang1Background: Rheumatoid Arthritis (RA) is a systemic autoimmune disease leading to joint destruction. The prevention of bone and cartilage destruction has received increased attention in recent years.
Objective: To evaluate the current evidences regarding the bone-protecting efficacy of Chinese medicine or the combination of Chinese medicine and Western medicine for RA.
Methods: We comprehensively searched PubMed, Embase, the Cochrane Library (www.thecochranelibrary.com), the China National Knowledge Infrastructure (CNKI), the Database for Chinese Technical Periodicals (VIP), and SinoMed. We then performed a systematic review and cumulative meta-analysis of all randomized controlled trials (RCTs) assessing the two therapy methods.
Results: Sixteen studies including 1,171 patients were included in the final analysis. The results showed that Chinese medicine could significantly improve the bone mineral density (BMD) (mean difference [MD] = 0.05 /g·cm−2, 95% CI [0.03, 0.08], P < 0.00001), and decrease the serum matrix metalloproteinase 3 (MMP-3) ([SMD] = −2.84, 95% CI [−4.22, −1.47], P < 0.0001).
Conclusions: Chinese medicine may provide an efficiently alternative choice for the treatment of RA in terms of the bone-protecting efficiency. Given the inherent limitations of the included studies, future well-designed RCTs are required to confirm and update the findings of this analysis.
Rheumatoid Arthritis (RA) is a chronic systemic autoimmune disease with symmetric inflammation of aggressive multiple joints (Miossec, 2013). As the most common inflammatory rheumatic disease, the prevalence of RA is about 0.5–1.0% in the world (Tanaka et al., 2014). In China, up to 5 million people suffer from RA with an estimated prevalence of 0.34% (Zhang et al., 2013). The inflammatory cell infiltration of synovium, pannus formation, and the progressive destruction of articular cartilage and bone destruction are the main pathological properties of RA (Mcinnes and Schett, 2011). The data from epidemiological investigations shows that about 90% of RA patients developed bone erosions within 2 years of the disease onset, eventually leading to joint deformities or even disability (Miossec, 2013; Nam et al., 2014). Therefore, RA brings with it a heavy burden and great pain to the families, patients, and even the society as a whole. The question of how to prevent the bone and cartilage from irreversible destruction thus becomes a key issue that doctors and scientists are currently paying more attention to and strive to resolve.
Up to date, there are no systematic reviews and meta-analysis regarding bone-protecting efficiency about Chinese Medicine alone or in combination with Western Medicine in the treatment of RA. We therefore systematically searched and analyzed the available literature to evaluate the efficacy and potential advantages of Chinese Medicine (or a combination of Chinese and Western medicine), when compared with Western Medicine.
All randomized controlled clinical trials.
Adults (usually over 18 years of age) with a diagnosis of RA either using the 1987 American College of Rheumatology (ACR) classification criteria (Arnett et al., 1988) for RA, or using the 2010 ACR/ European League Against Rheumatism (EULAR) classification criteria (Aletaha et al., 2010) for RA.
All experimental groups were treated with oral Chinese medicine or combined Chinese and western medicine. The comparison arm was treated only with oral Western medicine.
The evaluation of radiographic progression of hands. The classification standards refer to AHA standards (Arnett et al., 1988).
The secondary outcomes include the bone mineral density (BMD) and the levels of serum matrix metalloproteinase 3 (MMP-3), a biomarker for bone destruction (Klimiuk et al., 2002).
We developed our search strategies sequentially. The following MeSH terms and their combinations were used to search in [Title/Abstract]: Rheumatoid Arthritis, random, control, and bone. We searched these terms in all databases in order to fit the requirements of the specific database style.
We searched the following electronic databases.
(1) PubMed, inception to 31 December 2017;
(2) EMBASE, inception to 31 December 2017;
(3) The Cochrane Library (www.thecochranelibrary.com), inception to 31 December 2017;
(4) The China National Knowledge Infrastructure (CNKI), inception to 31 December 2017;
(5) The Database for Chinese Technical Periodicals (VIP), inception to 31 December 2017;
(6) SinoMed, inception to 31 December 2017.
In addition, we manually searched the reference lists of the included studies and previous review papers to find additional studies. All references were imported to an EndNote (x6) library and tagged with the name of the database.
Two review authors assessed the titles and abstracts for all the records identified through the search strategies, retrieving full texts for all those that appeared to satisfy the following criteria: the type of study; type of participants; type of intervention; type of measurements. Data from the included studies were extracted and summarized independently by at least two of the authors. Any disagreement was resolved by a discussion among all the authors.
For data extraction, the review team allocated papers to different authors according to their areas of expertise, and two reviewers independently retrieved the details for each publication and tabulated them in a standardized form. The retrieved details include intervention (including characteristics and duration), assignment to groups (including the form of a drug, concealment, and comparability of groups), outcome measures, timing of measurements, adherence to intervention/control, sample size statistical analysis methods as well as adverse events and withdrawals. Two review (XC, RYH) authors independently extracted data from the reviews using a predefined data extraction form created as a Microsoft Excel® spreadsheet.
Studies were rated for evidence level according to the criteria given by the Centre for Evidence-Based Medicines in Oxford, UK (Phillips et al., 2012). Assessment of risk of bias was undertaken for each included study using the Cochrane Collaboration's risk of bias assessment tool (Higgins and Green, 2008). Seven key domains were assessed by two review authors, which include sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other sources of bias. Pairs of review authors judged the key domains as “high risk,” “low risk,” or “unclear” risk of bias. In cases of disagreement between the review authors, the decision was made by consensus.
For each trial, data analysis employed a standard meta-analysis using the methods for continuous data. Mean differences (MD), standardized mean differences (SMD), and 95% confidence intervals (CIs) were calculated for the continuous outcomes (reporting mean and standard deviation of the mean). Where the standard deviations were not explicitly stated, we calculated them from the different means and their respective CIs or P-values.
Where appropriate, we formally assessed heterogeneity of the data using the I2 statistics (Higgins et al., 2003). We judged a value greater than 50% to represent substantial heterogeneity. If results were determined to be heterogeneous (that is I2 > 50%), a random-effects model would be used to further analyze the results. Where we detected this level of heterogeneity and there were sufficient studies available, we conducted subgroup analyses in an attempt to explain the heterogeneity.
We used Egger's test to assess the possibility of publication bias with Stata 11.0.
Where there was no heterogeneity, we used a fixed-effect model, and where there was heterogeneity, we used a random-effects model if there was no clinical heterogeneity. The MD for pooled data in meta-analysis were calculated using a fixed model as outcomes were measured on the same standard scales. Otherwise, the SMD were calculated. Meta-analysis was facilitated by Review Manager 5.3 (Cochrane Collaboration, Oxford, UK) using the statistics as described below.
Where sufficient studies were available and the data was heterogeneous, we carried out separate meta-analyses for studies according to some factors including intervention duration, disease stage, and the form of traditional Chinese medicine (TCM).
In studies where calcium supplements were used, we planned the sensitivity analyses as a priority in order to explore the differences in effect size and to assess whether the conclusions were robust to the decision-making process. The sensitivity analyses included the following:
(1) The effect of risk of bias in included studies—defined as adequate allocation concealment and blinding of outcome assessors; (2) the effect of using calcium supplements.
We undertook a comprehensive literature search, including screening of titles and abstracts. In total, we retrieved 25 fulltext references for further evaluation, including the manual searching of reference lists (9 further full-text studies).
Sixteen studies (Lu et al., 2002; Tang et al., 2005; Ma et al., 2009; Xue et al., 2009; Su, 2010; Li et al., 2012, 2017; Ouyang et al., 2013; He and Xiao, 2014; Ling et al., 2014; Liu, 2014; Liu et al., 2014; Pang et al., 2015; Wu et al., 2015; Xu et al., 2016; Zhang et al., 2016) including 1,171 cases (620 cases for oral Chinese medicine only or combined with western medicine, 551 cases for oral western medicine) fulfilled the predefined inclusion criteria and were included in the final analysis (Figure 1). Examination of the references listed for these studies and for the articles did not yield any further studies for evaluation. Agreement between the two reviewers was 90% for study selection and 92% for quality assessment of trials.
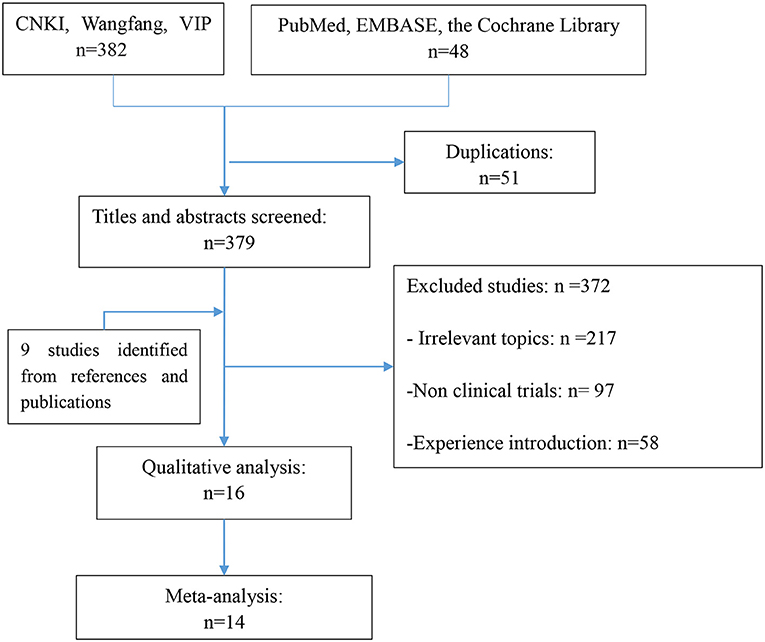
Figure 1. The study flow diagram.
The study flow diagram and search summary are described in Figure 1 and Table 1, respectively.
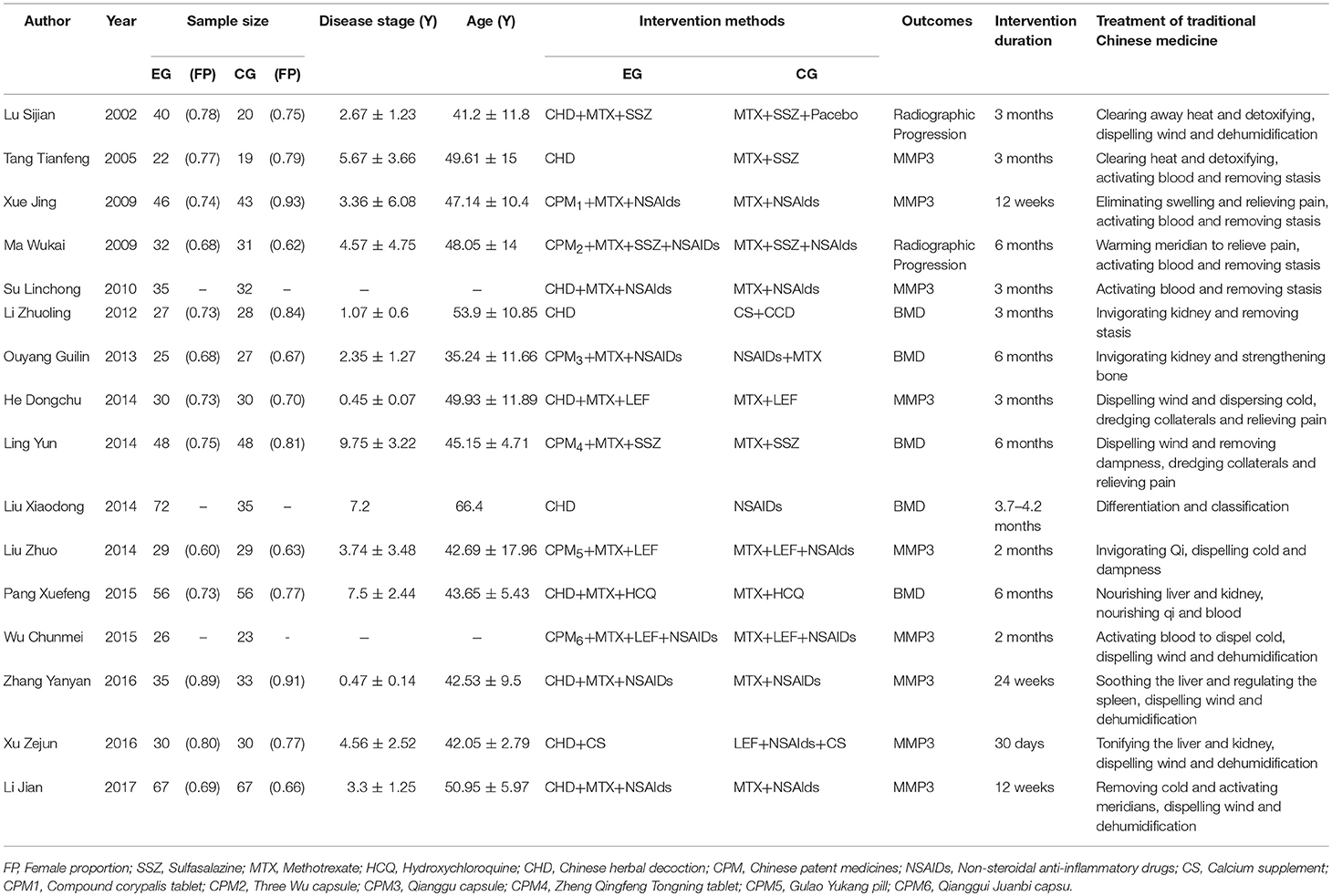
Table 1. Characteristics of the included studies.
A total of 16 articles were included and all of these trials were performed in China. There were 11 articles (Lu et al., 2002; Tang et al., 2005; Ma et al., 2009; Xue et al., 2009; Su, 2010; Li et al., 2012; Ouyang et al., 2013; Ling et al., 2014; Liu et al., 2014; Pang et al., 2015; Xu et al., 2016) that used the ACR 1987 criteria and 4 studies (Liu, 2014; Wu et al., 2015; Zhang et al., 2016; Li et al., 2017) that used the 2010 revised criteria for the ACR/EULAR classification of RA.
The primary outcomes of the included studies were the evaluation of radiographic progression of hands. Only two studies (Lu et al., 2002; Ma et al., 2009) provided changes of X-ray image staging. In two studies (Lu et al., 2002; Ma et al., 2009) the data set was incomplete and, hence we were unable to conduct the analyses of their primary outcomes. Nine studies (Tang et al., 2005; Xue et al., 2009; Su, 2010; He and Xiao, 2014; Liu, 2014; Wu et al., 2015; Xu et al., 2016; Zhang et al., 2016; Li et al., 2017) including 626 patients provided the serum MMP-3 data. Five studies (Li et al., 2012; Ouyang et al., 2013; Ling et al., 2014; Liu et al., 2014; Pang et al., 2015) including 422 patients provided the BMD data. In most of the studies, the BMD was observed by using dual-energy x-ray absorptiometry (DEXA) and biological mechanics methods. Only one study used single-photon absorption to measure the BMD. In these studies, the BMD was assessed by testing the lumbar, vertebra, ulna, or undefined part.
Nine RCTs (two abstracts and seven articles) were excluded: two did not explain the diagnostic criteria, six did not include the outcomes of interest, and one used proprietary Chinese medicine in the control group.
Overall, for most of the included studies the risk of bias was low or unclear. The methodological quality summary for each included study is presented in Figure 2. The review authors' judgments about each methodological quality item are presented as percentages across all the included studies in Figure 3.
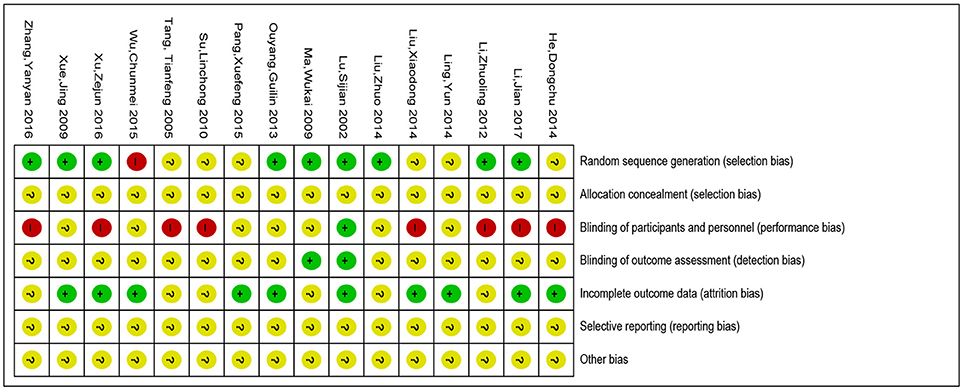
Figure 2. Risk of bias summary of included studies. “?”: unclear risk of bias; “–”: low risk of bias; “+”: high risk of bias.
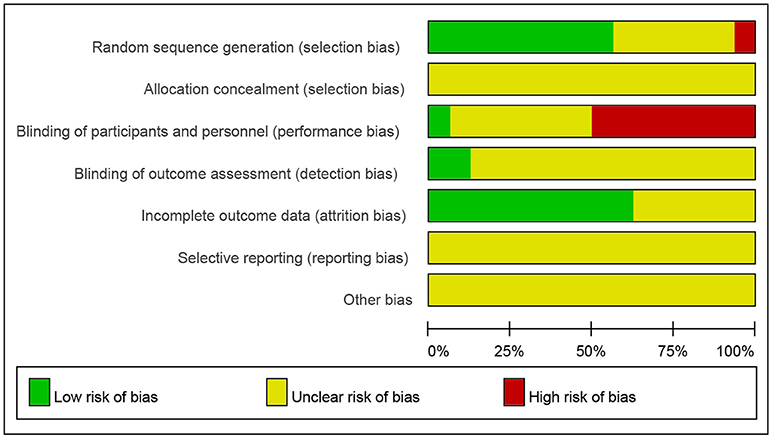
Figure 3. Evaluation for bias risk of included studies.
Investigators described all the studies included as randomized controlled trials. Nine studies (Lu et al., 2002; Ma et al., 2009; Xue et al., 2009; Li et al., 2012, 2017; Ouyang et al., 2013; Liu, 2014; Xu et al., 2016; Zhang et al., 2016) adequately described the random method (low risk of bias). One study (Wu et al., 2015) reported a high risk of bias and the other studies did not clearly describe these methods (unclear risk of bias). Allocation concealment was assessed unclear in all the trials.
Only one trial (Lu et al., 2002) was judged being at low risk of performance bias while eight were at high risk of bias. In 7 trials (Tang et al., 2005; Su, 2010; Li et al., 2012, 2017; He and Xiao, 2014; Liu et al., 2014; Xu et al., 2016; Zhang et al., 2016) the participants were not blinded and these trials were all judged as being at high risk of performance bias. We assessed low risk of detection bias in 2 trials (Lu et al., 2002; Ma et al., 2009) and unclear risk in 14 trials.
Ten studies (Lu et al., 2002; Xue et al., 2009; Ouyang et al., 2013; He and Xiao, 2014; Ling et al., 2014; Liu et al., 2014; Pang et al., 2015; Wu et al., 2015; Xu et al., 2016; Li et al., 2017) were judged being at low risk of attrition bias and others were judged as unclear risk.
All trials were judged as unclear risk since the study protocols were not available and we did not have enough information in the study report to assess selective reporting.
All trials were judged as unclear risk.
Summary of the findings for the main comparison includes that Chinese medicine may provide an efficiently alternative choice for treatment of RA regarding its bone-protecting efficiency.
Only two studies (Lu et al., 2002; Ma et al., 2009) provided changes of X-ray image staging, while two studies (Lu et al., 2002; Ma et al., 2009) did not provide complete data, which made it difficult to merge the analysis. In the Chinese Medicine groups the scores of radiographic progression improved significantly after treatment, whereas no significant difference was found in the Western Medicine groups after treatment.
Pooling the data from 6 studies (Li et al., 2012; Ouyang et al., 2013; Ling et al., 2014; Liu et al., 2014; Pang et al., 2015) that measured the increase in bone mineral density in 422 patients, it was demonstrated that Chinese medicine (or combination of Chinese and western medicine) resulted in more significant effects than the western medicine groups (MD = 0.05/g·cm−2, 95 %CI [0.03, 0.08], P < 0.00001) (Figure 4).
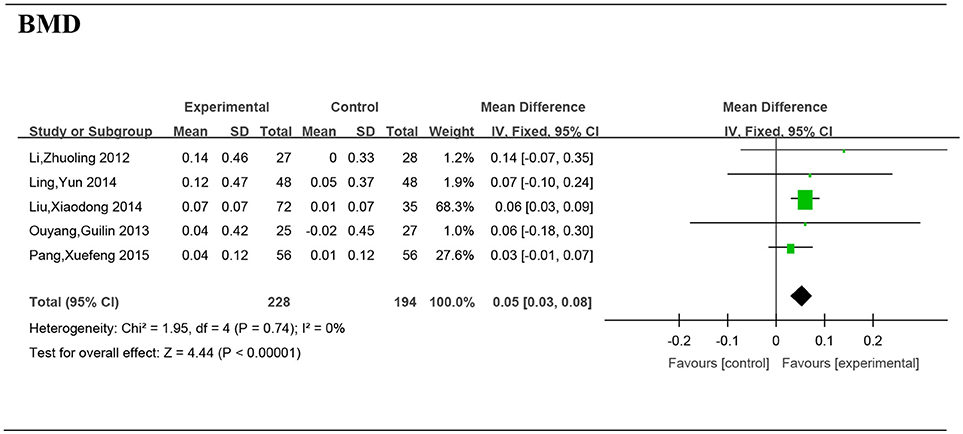
Figure 4. Forest plot and meta-analysis of bone mineral density. Experimental: the group of Chinese Medicine; Control: the group of Western medicine; RA, Rheumatoid Arthritis; SD, standard deviation; IV, inverse variance method; CI, confidence interval.
Nine studies (Tang et al., 2005; Xue et al., 2009; Su, 2010; He and Xiao, 2014; Liu, 2014; Wu et al., 2015; Xu et al., 2016; Zhang et al., 2016; Li et al., 2017) including 626 patients provided the serum MMP-3 data. The I-squared was 98% and the p-value was <0.00001, so a random effects model was adopted for the meta-analysis. Significant differences were found in the reduction of serum MMP-3 levels between the Chinese medicine (or Chinese combined with Western medicine) group and Western medicine group (SMD = −2.84, 95%CI [−4.22, −1.47], P < 0.0001) (Figure 5).
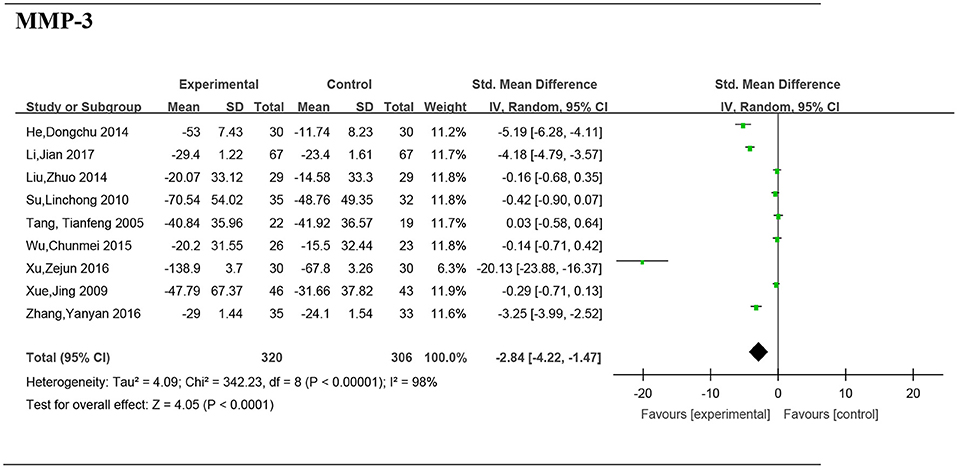
Figure 5. Forest plot and meta-analysis of the serum matrix metalloproteinase 3. Experimental: the group of Chinese Medicine; Control: the group of Western medicine; SD, standard deviation; IV, inverse variance method; CI, confidence interval.
Data from one paper (Xu et al., 2016) reported the significant difference of serum MMP-3 between two groups (SMD: −20.13; 95% CI, −23.88 to −16.37; P < 0.00001) (Figure 6).
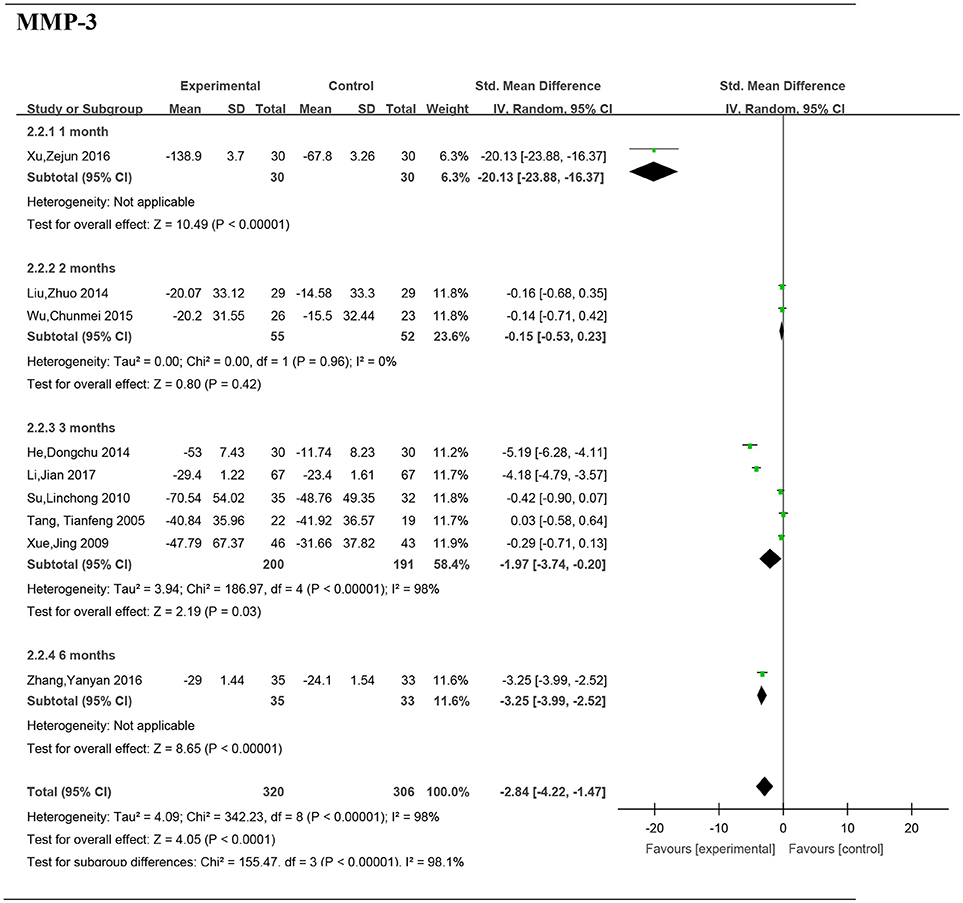
Figure 6. Forest plot and meta-analysis of the serum matrix metalloproteinase 3 of subgroup analysis by intervention duration. Experimental: the group of Chinese Medicine; Control: the group of Western medicine; SD, standard deviation; IV, inverse variance method; CI, confidence interval.
Two studies (Liu, 2014; Wu et al., 2015) including 107 patients reported no significant difference of serum MMP-3 between the groups (SMD: −0.15; 95% CI, −0.5– 0.23; P = 0.42).
Five studies (Tang et al., 2005; Xue et al., 2009; Su, 2010; He and Xiao, 2014; Li et al., 2017) including 391 patients reported a significant difference of MMP-3 between the groups (SMD: −1.97; 95% CI, −3.74 to −0.20; P = 0.03).
Data from one paper (Zhang et al., 2016) reported a significant difference of serum MMP-3 between two groups (SMD: −2.84; 95% CI, −4.22 to −1.47; P < 0.00001).
Two studies (He and Xiao, 2014; Zhang et al., 2016) including 128 patients reported significant difference of MMP-3 between the groups (SMD: −4.18; 95% CI, −6.08 to −2.28; P < 0.0001).
Five studies (Tang et al., 2005; Xue et al., 2009; Liu, 2014; Xu et al., 2016; Li et al., 2017) including 382 patients reported a significant difference of MMP-3 between the groups (SMD: −3.66; 95% CI, −5.84 to −1.49; P = 0.0009) (Figure 7).
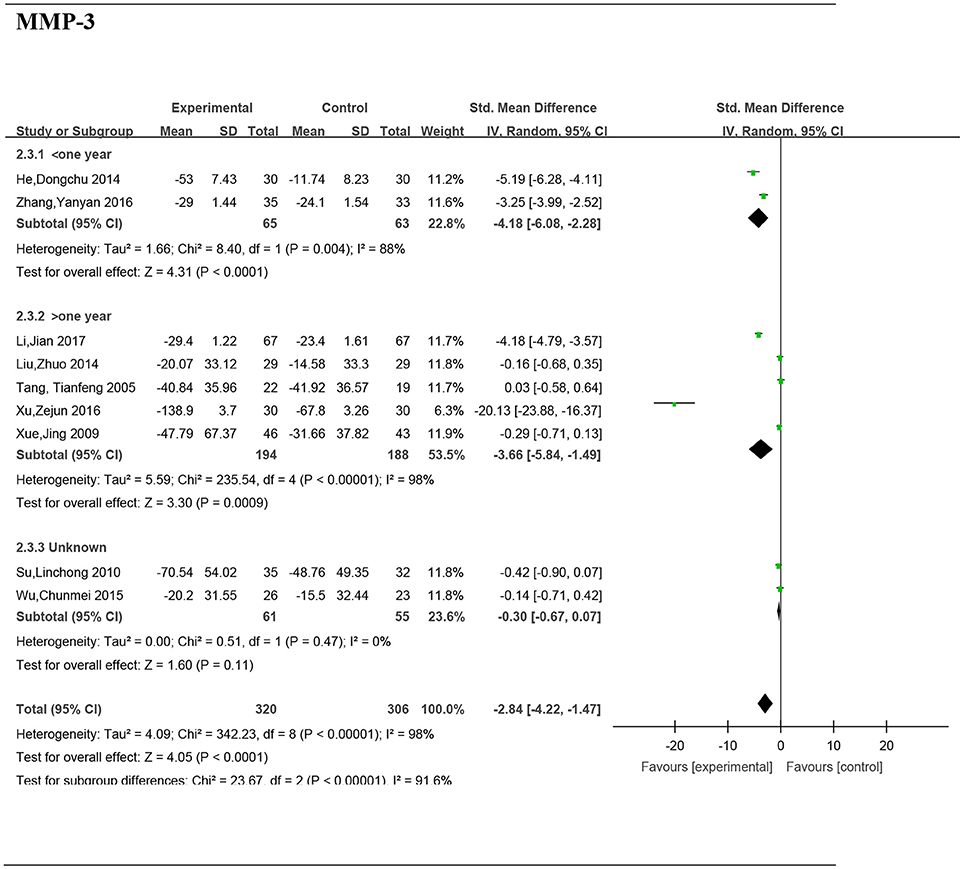
Figure 7. Forest plot and meta-analysis of the serum matrix metalloproteinase 3 of subgroup analysis by disease stage. Experimental: the group of Chinese Medicine; Control: the group of Western medicine; SD, standard deviation; IV, inverse variance method; CI, confidence interval.
Two studies (Su, 2010; Wu et al., 2015) including 116 patients reported no significant difference of MMP-3 between the groups (SMD: −0.3; 95% CI, −0.67 to 0.07; P = 0.11).
Three studies (Xue et al., 2009; Liu, 2014; Wu et al., 2015) including 196 patients reported no significant difference of MMP-3 between the groups (SMD: −0.22; 95% CI, −0.50 to 0.07; P = 0.13) (Figure 8).
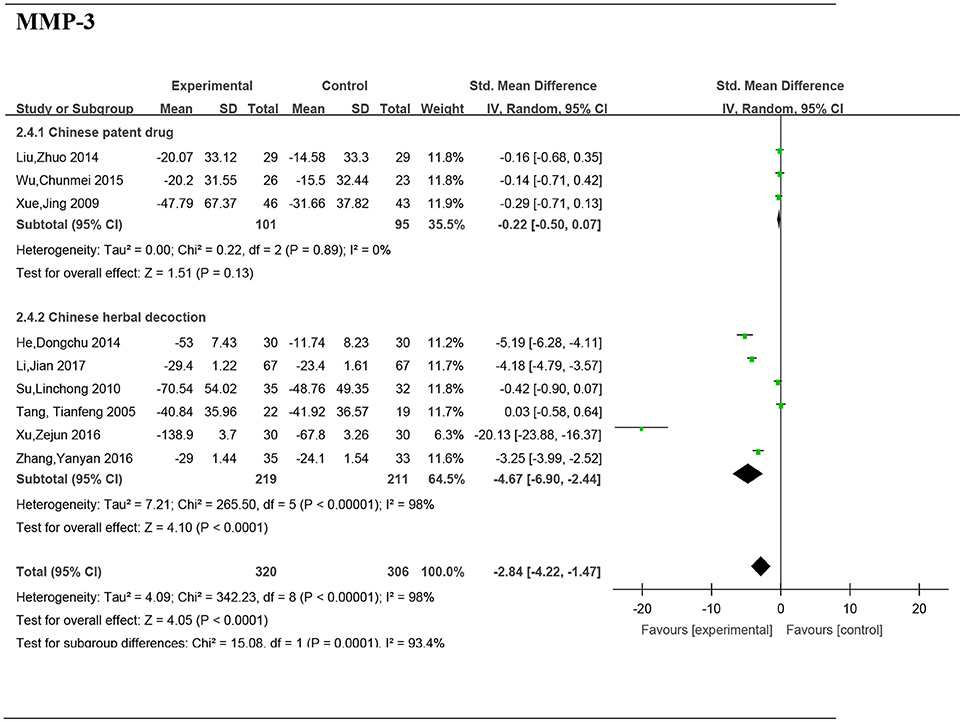
Figure 8. Forest plot and meta-analysis of the serum matrix metalloproteinase 3 of subgroup analysis by the form of a TCM. Experimental: the group of Chinese Medicine; Control: the group of Western medicine; SD, standard deviation; IV, inverse variance method; CI, confidence interval.
Six studies (Tang et al., 2005; Su, 2010; He and Xiao, 2014; Xu et al., 2016; Zhang et al., 2016; Li et al., 2017) including 430 patients reported a significant difference of MMP-3 between the groups (SMD: −4.67; 95% CI, −6.90 to −2.44; P < 0.0001).
We performed sensitivity analyses to explore the differences in effect size and to assess whether the conclusions were robust for the decision-making process. The studies or trials which were judged as high risk or unclear risk of attrition bias were excluded. There was no change in the significance of any of the outcomes (Table 2). In the subgroup of 3 months treatment, two studies (He and Xiao, 2014; Li et al., 2017) were treated by “dispelling wind and dispersing cold,” while other therapies were to “activate blood circulation and remove stasis,” where both are Chinese medical methods to treat diseases. After excluding these two literatures, there was no heterogeneity in the subgroup, and the overall result did not change (Figure 9).

Table 2. Sensitivity analysis.
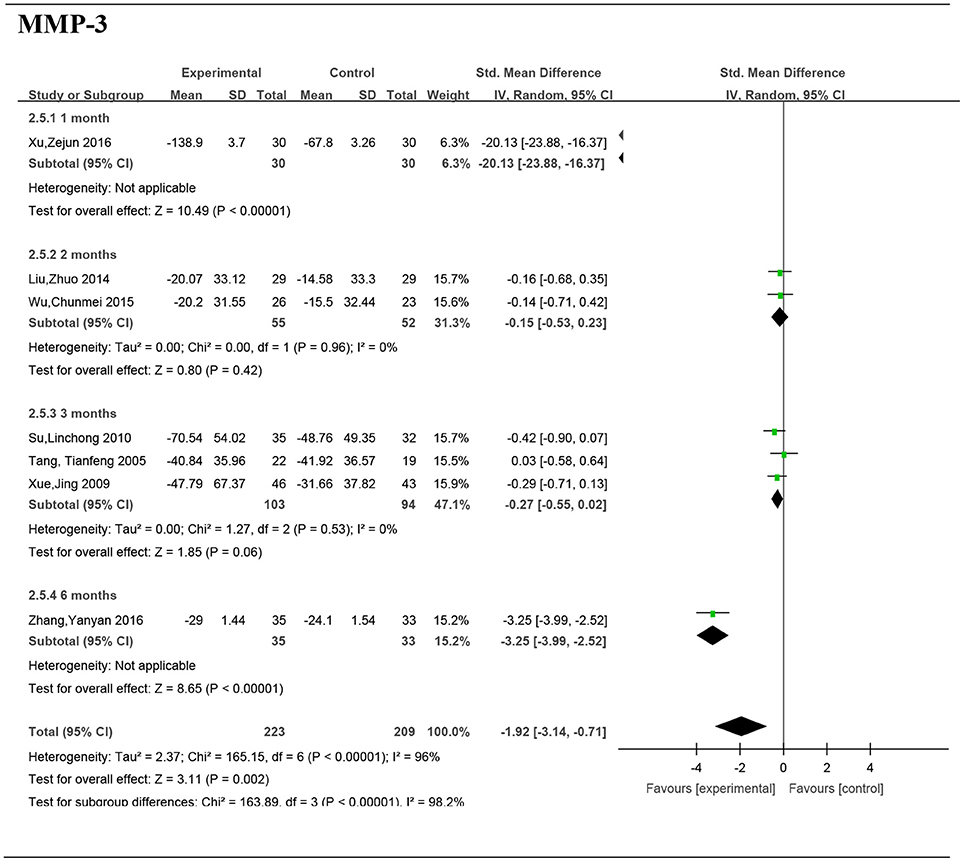
Figure 9. Forest plot and meta-analysis of the serum matrix metalloproteinase 3 of subgroup analysis by intervention duration. Experimental: the group of Chinese Medicine; Control: the group of Western medicine; SD, standard deviation; IV, inverse variance method; CI, confidence interval.
Egger's test of BMD did not suggest significant publication bias (P = 0.661). There is significant publication bias for MMP-3 (P = 0.011) (Table 2).
The aim of this review was to provide an overview of bone-protecting effects of Chinese medicines in the treatment of RA. The review revealed 16 RCTs investigating bone-protecting interventions.
The changes in local metabolism may impair the dynamic balance of bone formation and resorption, finally leading to bone and cartilage destruction of RA (Solomon et al., 2009). As stated, about 90% of the RA patients developed bone erosions within 2 years after onset, eventually processing to joint deformities disability (Miossec, 2013; Nam et al., 2014). Inflammation is the driving force in RA, which gives rise to structural damage during the course of RA (Schett et al., 2008). Conventional DMARDs are extensively used in the treatment of RA, either as monotherapy or in combination with other drugs. Conventional DMARDs have been shown to reduce the expression of the nuclear factor-kappa B ligand in synovial fibroblast cultures, which may indicate a specific effect on the osteoclast (Lee et al., 2004). Among the conventional DMARDs, the most widely used agent is MTX, which is also considered the anchor drug for the treatment of RA. In several evidences, the biologic agents, including the inhibitors of tumor necrosis factor (TNFi), exhibited the effect to somewhat halt the progression of articular erosions (Dohn et al., 2011; Finzel et al., 2011). These agents are usually used in combination with MTX. An RCT comparing denosumab, an antagonist of receptor activator of nuclear factor-kappa B ligand, with placebo in patients of RA showed a statistically significant decrease in erosion score (Cohen et al., 2008). Unfortunately, these biologic agents are too expensive to be widely used in a developing country such as China. Therefore, we urgently need an effective and cheap therapeutic method to block or even treat bone erosion of RA.
We therefore systematically searched and analyzed the available literature to evaluate the efficacy and potential advantages of Chinese Medicine (or combination of Chinese and Western medicine) compared with Western Medicine. In assessing the extent of bone destruction, imaging provides us with a more intuitive evidence. The pooled data of outcomes indicates that Chinese Medicine can improve the imaging findings of RA. Some studies (Ma et al., 2009; Jiang et al., 2012) showed that Chinese medicine has the potential to improve X-ray imaging during RA process. Moreover, the pooled data showed that Chinese medicine (the combination of Chinese and western medicine) are more effective in improving the BMD when compared to the treatment provided using Western medicine only.
Due to the limitation of the number of randomized trials, there is no definite result in the imaging of bone destruction in patients with RA. We try to indirectly reflect the bone protective effect of Chinese and Western Medicine on RA from mineralization of bone tissue, stability of cartilage structure, and degree of bone resorption.
The BMD is an important index reflecting the metabolic status of the skeleton of a human being. The pooled data showed that Chinese medicine (the combination of Chinese and western medicine) is more effective in improving the BMD than only Western medicine treatment.
Pooled data indicated that the MMP-3 level was reduced in the Chinese medicine group. It is known that the MMPs can degrade all the protein components of the cartilage, resulting in destruction of ligaments, cartilage, and bone (Klimiuk et al., 2002). Importantly, MMP-3 has been shown to be mostly related in synovium of advanced RA patients (Klimiuk et al., 2002). Therefore, MMP-3 is defined as a biomarker for bone destruction.
We further carried out a subgroup analysis according to the intervention duration, disease stage, and the form of a TCM, but the heterogeneity in the 3 months test is still very high. Most of the MMP-3 data was tested in the laboratory. In the subgroup of 3 months treatment, two studies were treated by “dispelling wind and dispersing cold,” while other therapies were to “activate blood circulation and remove stasis”; we therefore exclude these two studies. After excluding these studies, there was no significant difference in the subgroup, and the overall result did not change. According to the result, under the intervention of TCM, the serum MMP-3 level could be effectively reduced in a patient with early RA. It is possible that the decoction of Chinese medicine is more effective. The test level difference has a great relationship with the heterogeneity. The precise cause of heterogeneity is unclear, though it may also be due to Traditional Chinese Medicine syndromes and participant characteristics among others.
Pooled data indicated that the Chinese medicine (the combination of Chinese and western medicine) had a better effect in comparison to only Western medicine in reducing the destruction of cartilage.
This meta-analysis of 16 RCTs or CCTs includes 1,171 patients. Our findings suggest that the Chinese traditional medicine leads to a statistically significant increase in the BMD and decrease in MMP-3, which implies that the Chinese medicine may provide an efficient treatment option for RA in terms of the bone-protecting efficiency, especially to patients in China. However, the limitations of this meta-analysis are also to be noted. All the included studies were performed only in China. Many of the studies included a small number of patients. The most important criteria, including the BMD, imaging stage, and MMP-3, were not reported in all the studies. In addition, the limited numbers of RCTs prevented us from reaching any definitive conclusions. Furthermore, bone destruction is a chronic progression, but the study of the literature for 3–6 months does not give long-term results. Therefore, more studies with high quality are urgently needed to judge the full potential of the Chinese traditional medicine for use in bone-protection. Accordingly, the conclusions of this review should be carefully interpreted. Due to the increasing use of Chinese medicine, accurate and complete data on the interactions between Chinese medicine and western medicine are urgently required.
XC, X-MC, R-YH, Z-HW, and P-JJ contributed to the literature database search, data collection, data extraction, data analysis, and writing of the manuscript. XX, KB, R-RW, J-HP, H-JL, Q-WY, J-YY, M-JW, HY, J-JL, Y-JH, and Q-CH performed data analysis and rationalization of the results. The topic was conceptualized by P-JJ, R-YH, and Z-HW.
This study was supported by the grants from Guangzhou University of Chinese Medicine (No. YQ2015044 and No. A1-AFD018161Z1511), the joint grant from Guangdong province science and Technology Department and Guangdong Provincial Academy of Chinese medicine (No. 2014A020221028, 2014A020221031, and 2016A020226041), the grant from Guangzhou Municipal Science and Technology Innovation Committee (No. 201710010076), the National TCM Clinical Research Base Project of the State Administration of Traditional Chinese Medicine (No. JDZX2015197), the Special Project of Guangdong Province Traditional Chinese Medical Hospital (No. YN2015MS05), and the Key Laboratory Open Project Fund from Macau University of Science and Technology (No. MUST-SKL-2016-08). Swedish Research Council (grant no: 2017-02577); Innovative Medicines Initiative (EU/EFPIA) (ULTRA-DD grant no: 115766); The Swedish Rheumatism Association (grant no: R-755861).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
RA, Rheumatoid Arthritis; CNKI, the China National Knowledge Infrastructure; VIP, the VIP Database for Chinese Technical Periodicals; RCTs, randomized controlled trials; EULAR, European League Against Rheumatism; ACR, American College of Rheumatology; SMD, standardized mean difference; MD, mean difference; BMD, bone mineral density; MMP3, Matrix metalloproteinase 3; RR, risk ratio; CIs, confidence intervals; ACR, American Rheumatism Association; OPG, Osteoprotegerin; MMPs, Matrix metallo proteinases; TCM, traditional Chinese medicine.
Aletaha, D., Neogi, T., Silman, A. J., Funovits, J., Felson, D. T., Bingham, C. O. 3rd., et al. (2010). 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 62, 2569–2581. doi: 10.1002/art.27584
Arnett, F. C., Edworthy, S. M., Bloch, D. A., McShane, D. J., Fries, J. F., Cooper, N. S., et al. (1988). The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31, 315–324. doi: 10.1002/art.1780310302
Cohen, S. B., Dore, R. K., Lane, N. E., Ory, P. A., Peterfy, C. G., Sharp, J. T., et al. (2008). Denosumab treatment effects on structural damage, bone mineral density, and bone turnover in rheumatoid arthritis: a twelve-month, multicenter, randomized, double-blind, placebo-controlled, phase II clinical trial. Arthritis Rheum. 58, 1299–1309. doi: 10.1002/art.23417
Dohn, U. M., Ejbjerg, B., Boonen, A., Hetland, M. L., Hansen, M. S., Knudsen, L. S., et al. (2011). No overall progression and occasional repair of erosions despite persistent inflammation in adalimumab-treated rheumatoid arthritis patients: results from a longitudinal comparative MRI, ultrasonography, CT and radiography study. Ann. Rheum. Dis. 70, 252–258. doi: 10.1136/ard.2009.123729
Finzel, S., Rech, J., Schmidt, S., Engelke, K., Englbrecht, M., Stach, C., et al. (2011). Repair of bone erosions in rheumatoid arthritis treated with tumour necrosis factor inhibitors is based on bone apposition at the base of the erosion. Ann. Rheum. Dis. 70, 1587–1593. doi: 10.1136/ard.2010.148395
He, D., and Xiao, J. (2014). Clinical efficacy and safety observation of Bizhengning on rheumatoid arthritis [in Chinese]. Mod. J. Integr. Tradit. Chinese Western Med. 28, 3090–3092+3095. doi: 10.3969/j.issn.1008-8849.2014.28.004
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327, 557–560. doi: 10.1136/bmj.327.7414.557
Higgins, J. P. T., and Green, S. (2008). Cochrane handbook for systematic reviews of interventions. New York, NY: Cochrane Collaboration, John Wiley and Sons.
Jiang, Q., Zhou, X.-Y., Wang, L., Yu, W., Wang, P., Cao, W., et al. (2012). A one-year evaluation of radiographic progression in patients with rheumatoid arthritis treated by Qingre Huoxue Decoction (清热活血方). Chin. J. Integr. Med. 18, 256–261. doi: 10.1007/s11655-011-0793-0
Klimiuk, P. A., Sierakowski, S., Latosiewicz, R., Cylwik, B., Skowronski, J., and Chwiecko, J. (2002). Serum matrix metalloproteinases and tissue inhibitors of metalloproteinases in different histological variants of rheumatoid synovitis. Rheumatology 41, 78–87. doi: 10.1093/rheumatology/41.1.78
Lee, C. K., Lee, E. Y., Chung, S. M., Mun, S. H., Yoo, B., and Moon, H. B. (2004). Effects of disease-modifying antirheumatic drugs and antiinflammatory cytokines on human osteoclastogenesis through interaction with receptor activator of nuclear factor kappaB, osteoprotegerin, and receptor activator of nuclear factor kappaB ligand. Arthritis Rheum 50, 3831–3843. doi: 10.1002/art.20637
Li, J., Rong, B., Jia, J., and Pan, M. (2017). Effect of modified juanbitang on inflammatory factors and serum MMP-3, OPG and RANKL in synovial fluid of patients with wind-cold-wetness type rheumatoid arthritis [in Chinese]. Chin. J. Exp. Tradit. Med. Formulae 22, 165–170. doi: 10.13422/j.cnki.syfjx.2017220165
Li, Z., Wang, R., Sheng, J., Xu, L., Yue, T., Zhu, Q., et al. (2012). Effect of Bushen Huayu Decoction on Bone Metabolism of Patients with Rheumatoid Arthritis in Early Stage [in Chinese]. J. Tradit. Chinese Medi. 53, 215–218. doi: 10.13288/j.11-2166/r.2012.03.014
Ling, Y., Wang, N., Feng, H., Xie, J., and He, D. (2014). Clinical study of sinomenine combined with methotrexate on the repair of bone destruction in rheumatoid arthritis [in Chinese]. World Clinical Drugs 35, 279–282. doi: 10.13683/j.wph.2014.05.008
Liu, X., Zhang, Y., and Wu, J. (2014). An alysis of 107 cases of senile osteoporosis caused by rheumatoid arthritis in TCM [in Chinese]. Clin. J. Chin. Med. 6, 12–14.
Liu, Z. (2014). Gulao Yukang pills Clinical Research on treating Rheumatoid Arthritis with cold-dampness type [in Chinese]. Master, Gansu College of Traditional Chinese Medicine.
Lu, S., Shao, J., Li, X., and Yang, X. (2002). Clinical observation on treatment of rheumatoid arthritis by combined therapy with methotrexate, sulfasalazine and chinese herbal medicine [in Chinese]. Chin. J. Integr. Tradit. Western Med. 22, 571–573. doi: 10.3321/j.issn:1003-5370.2002.08.003
Ma, W., Zhong, Q., Liu, Z., and Yao, X. (2009). A clinical study of Sanwu capsule combined with methotrexate and sulfasalazine in the treatment of rheumatoid arthritis [in Chinese]. J. New Chinese Med. 41, 42–44. doi: 10.13457/j.cnki.jncm.2009.11.061
Mcinnes, I. B., and Schett, G. (2011). The pathogenesis of Rheumatoid Arthritis—NEJM. N. Engl. J. Med. 365, 2205–2219. doi: 10.1056/NEJMra1004965
Miossec, P. (2013). Rheumatoid arthritis: still a chronic disease. Lancet 381, 884–886. doi: 10.1016/S0140-6736(12)62192-8
Nam, J. L., Ramiro, S., Gaujoux-Viala, C., Takase, K., Leon-Garcia, M., Emery, P., et al. (2014). Efficacy of biological disease-modifying antirheumatic drugs: a systematic literature review informing the 2013 update of the EULAR recommendations for the management of rheumatoid arthritis. Ann. Rheum. Dis. 73, 516–528. doi: 10.1136/annrheumdis-2013-204577
Ouyang, G., Feng, X., Xiao, L., Huang, Z., Xia, Q., Han, D., et al. (2013). Evaluation of effect of qianggu capsule combined with methotrexate on bone destruction in rheumatoid arthritis [in Chinese]. Food Drug. 15, 34–37. doi: 10.3969/j.issn.1672-979X.2013.01.012
Pang, X., Liu, H., Wu, Y., Tang, L., Feng, Y., Meng, Y., et al. (2015). Clinical study on treatment of secondary osteoporosis of rheumatoid arthritis by tonifying kidney and rheumatism herbs combined with Western medicine [in Chinese]. World J. Integr. Tradit. Western Med. 10, 47–49. doi: 10.13935/j.cnki.sjzx.150115
Phillips, B., Ball, C., Sackett, D., Badenoch, D., Straus, S., Haynes, B., et al. (2012). Levels of Evidence and Grades of Recommendation. Oxford Centre for Evidence-based Medicine Web site. [Online]. Available online at: http://www.cebm.net/index.aspxo=1025 (Accessed June 1, 2017).
Schett, G., Stach, C., Zwerina, J., Voll, R., and Manger, B. (2008). How antirheumatic drugs protect joints from damage in rheumatoid arthritis. Arthritis Rheum. 58, 2936–2948. doi: 10.1002/art.23951
Solomon, D. H., Finkelstein, J. S., Shadick, N., LeBoff, M. S., Winalski, C. S., Stedman, M., et al. (2009). The relationship between focal erosions and generalized osteoporosis in postmenopausal women with rheumatoid arthritis. Arthritis Rheum. 60, 1624–1631. doi: 10.1002/art.24551
Su, L. (2010). Effects of jinbian qufeng composition on serum MMP-3 and TIMP-1 of patients with rheumatoid arthritis [in Chinese]. J. Hubei Inst. Nat. (Med. Edn.), 27, 8–10. doi: 10.3969/j.issn.1008-8164.2010.04.003
Tanaka, T., Hishitani, Y., and Ogata, A. (2014). Monoclonal antibodies in rheumatoid arthritis: comparative effectiveness of tocilizumab with tumor necrosis factor inhibitors. Biologics 8, 141–153. doi: 10.2147/BTT.S37509
Tang, T., Liang, Q., Luo, X., Chen, J., and Li, X. (2005). Effects of bizhongxiao decoction on serum matrix metalloproteinase 3 and its tissue inhibitors of metalloproteinase 1 in patients with rheumatoid arthritis at active phase [in Chinese]. Chin. J. Clin. Rehabil. 9, 114–116. doi: 10.3321/j.issn:1673-8225.2005.15.059
Wu, C., Shu, F., and He, J. (2015). Analysis of clinical efficacy of qianggui juanbi capsule combined with western medicine treatment of cold dampness blockage type of rheumatoid arthritis. J. Military Surg. Southwest China 17, 664–666. doi: 10.3969/j.issn.1672-7193.2015.06.027
Xu, Z., Xiao, C., Luo, C., Pan, Q., Wu, W., and Li, Z. (2016). Mixed cold and heat rheumatoid arthritis randomized controlled study Yiqi Liwan Tang combined western medicine treatment coercive [in Chinese]. J. Pract. Tradit. Chinese Int. Med. 30, 75–77. doi: 10.13729/j.issn.1671-7813.2016.07.31
Xue, J., Zhang, S., Wang, Q., Yang, X., Zhu, L., Wen, L., et al. (2009). Random open control study of compound recipe Xiantianwu united with Methotrexate on rheumatoid arthritis [in Chinese]. Mod. J. Integr. Tradit. Chinese Western Med. 18, 473–476. doi: 10.3969/j.issn.1008-8849.2009.05.001
Zhang, Y., Wang, J., Jiang, P., and Wu, J. (2016). Efficacy of Hebi formula combined methotrexate on early rheumatoid arthritis patients with disharmony of Gan and Pi syndrome and its effects on serum MMP-3 and RANK/RANKL/OPG expressions. Chin. J. Integr. Tradit. Western Med. 36, 1197–1201. doi: 10.7661/CJIM.2016.10.1197
Keywords: Rheumatoid Arthritis (RA), Chinese medicine, bone-protecting efficiency, systematic review, meta-analysis
Citation: Cai X, Chen X-M, Xia X, Bao K, Wang R-R, Peng J-H, Liu H-J, Yang Q-W, Yan J-Y, Wang M-J, Yu H, Lu J-J, Hu Y-J, Jakobsson P-J, Wen Z-H, Huang R-Y and Huang Q-C (2018) The Bone-Protecting Efficiency of Chinese Medicines Compared With Western Medicines in Rheumatoid Arthritis: A Systematic Review and Meta-Analysis of Comparative Studies. Front. Pharmacol. 9:914. doi: 10.3389/fphar.2018.00914
Received: 11 May 2018; Accepted: 25 July 2018;
Published: 30 August 2018.
Edited by:
Wei Wei, Anhui Medical University, ChinaReviewed by:
Claudio Ferrante, Università degli Studi G. d'Annunzio Chieti e Pescara, ItalyCopyright © 2018 Cai, Chen, Xia, Bao, Wang, Peng, Liu, Yang, Yan, Wang, Yu, Lu, Hu, Jakobsson, Wen, Huang and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Per-Johan Jakobsson, cGVyLWpvaGFuLmpha29ic3NvbkBraS5zZQ==
Ze-Huai Wen, d2VuemhAZ3p1Y20uZWR1LmNu
Run-Yue Huang, cnlodWFuZ0BnenVjbS5lZHUuY24=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.