
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 24 September 2020
Sec. Pediatric Neurology
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.526986
 Aditya Subramaniam1Ronald Ming Ren Tan1,2Derrick Chan1,3Zhi Min Ng1,3Chao Yan Dong4Jasmine Xun Yi Feng5Shu-Ling Chong1,2*
Aditya Subramaniam1Ronald Ming Ren Tan1,2Derrick Chan1,3Zhi Min Ng1,3Chao Yan Dong4Jasmine Xun Yi Feng5Shu-Ling Chong1,2*Background: Pediatric sports-induced concussions have become a topic of interest and concern in the scientific community. Already, the literature is rich with studies that have identified numerous short-term and long-term consequences of childhood sports-induced concussions. However, there are very few studies that have identified how well the students who participate in concussion-prone sports and their coaches understand these consequences and how they can be avoided. This study aimed to explore student athletes' and their coaches' understanding of the concept of concussion and how it is managed both immediately after the injury occurs and during long-term recovery.
Methods: This study utilized a qualitative design. The study was conducted in local and international schools in Singapore. Participants were recruited through purposive sampling. 42 student athletes aged 13–18 who participated in rugby, softball, football, cricket, volleyball, and/or water polo were recruited. Fourteen coaches who coached these same sports were also recruited. Four focus groups and three semi-structured interviews were conducted. Data collected were then analyzed with thematic analysis. Risk factors were assessed through four domains of focus: understanding of what concussion is; attitudes toward concussion; existing protocols for treating concussion; and return-to-school and return-to-play protocols. As this is a qualitative study, outcome measures were not identified.
Results: Analysis of the data revealed four themes for each group. For student-athletes these included: limited understanding of concussion; non-reporting of injuries; variable supervision of athletes; and a lack of established return-to-school and return-to-play guidelines. For coaches these included: variable understanding of concussion; insufficient formal training in concussion management; limited medical support in managing injuries; and lack of understanding and adherence to return-to-school and return-to-play protocols.
Conclusions: Of the themes identified, the most pressing was a lack of clearly defined return-to-play guidelines. This is an urgent issue that needs to be jointly addressed by healthcare professionals and schools with evidence-based guidelines.
Sports- and recreation-related concussions (SRRC) constitute significant injuries among children and adolescents (1). An estimated 582,000–635,000 patients under the age of 19 are diagnosed with SRRC in the United States annually, and a large proportion of children and adolescents leave their SRRCs untreated (2). Serious medical complications have been found to occur after SRRCs, including post-traumatic seizures and epilepsy (3, 4). Traumatic brain injury-related neuropathological changes are potentially serious consequences of concussion in adults who play contact sports (5). Although there is a paucity of prospective studies that clearly describe the relationship between SRRCs during childhood and adolescence, and long-term neurological sequelae, there are reports that exposure to American Football before the age of 12 may be associated with an increased chance of developing impairment in executive function later in life (6).
Student athletes are known to under-report injuries for a variety of reasons, including the tendency to underestimate the severity of their symptoms (7). There is also evidence to suggest that when student athletes are treated for concussion, they are unlikely to follow medical advice and return to play prematurely, the primary reason being pressure from their teammates (8, 9). In a study by McLeod et al. (10), it was found that while most sports coaches are aware of the overt symptoms of concussion, many are unable to identify more subtle symptoms such as vision problems, sleep disturbances, and nausea. Additionally, they found that 42% of coaches felt that loss of consciousness was required for the diagnosis of concussion, despite the Consensus Statement on Concussion in Sport (11) stating the contrary. These studies show that many coaches are unaware of critical aspects of concussion and how to manage it.
Currently, there is a paucity of literature investigating the understanding of SRRCs amongst student athletes and their coaches in Singapore. There is no clear legislation and a lack of documented concussion management protocols for student athletes in Singapore. Children and athletes who are brought to primary care or tertiary institutions for concussion injuries are managed in a very heterogenous way, depending on individual physician practices. There is a lack in communication on concussion management between physicians and the community, the latter including sports coaches and students.
Through interviewing student athletes and their coaches, this qualitative study aims to explore student athletes' and their coaches' understanding of four domains of SRRC: understanding of what a concussion is, attitudes toward concussion, existing school safety protocols for treating concussion, and return-to-school and return-to-play protocols. By establishing this, we hope to be able to address the knowledge gaps on SRRCs among student athletes and their coaches and to tailor injury control education.
We conducted focus group discussions (FGDs) for students and coaches from August 2018 to April 2019. We also conducted semi-structured interviews (SSIs) for coaches who could not attend scheduled FGDs. Both methods offered distinct advantages: FGDs promote dynamic discussion and group thinking while SSIs promote a more personalized rapport which can lead to more candid, genuine responses (12, 13).
This study was given ethical approval by the SingHealth Centralized Institutional Review Board [CIRB Ref: 2018/2746], with documentation of informed consent. All student participants gave written assent and their parents/guardians gave written informed consent. All coaches gave written informed consent in accordance with the Declaration of Helsinki.
We contacted both local and international schools in Singapore that are known for their participation in contact sports. Of six schools contacted, three schools agreed to help us recruit students and coaches. Two of these schools were part of the local system, and one was an international school. As most school children in Singapore are educated in the local system, we felt that this selection was representative of the overall student athlete population. We recruited student athletes aged 13–18 who participated in rugby, softball, football, cricket, volleyball, and/or water polo. Those with a history of prior neurological diagnoses or surgeries were not included in the study. Likewise, we recruited coaches who coached these same sports. All SSI participants were contacted individually.
This study used purposive sampling to ensure that participants who played in or coached more injury prone sports were better represented. Emphasis was placed on recruiting rugby and football players as studies have shown these sports are more prone to head injury than others (14). This would ensure that our interviews on concussion understanding and safety protocols (including return-to-school and return-to-play) were correctly targeted at the most relevant students and coaches. As this was a qualitative study, a sample size was not pre-calculated. Instead, data was gathered until a saturation point was reached where no new information emerged from the participants.
After a comprehensive literature review and input by experts (pediatricians who worked in this field and qualitative researchers), two interview guides were developed, one for students and another for coaches (Appendix in Supplementary Material). These guides were used throughout the study to ensure consistency in data collection. The interviews began with open-ended questions such as “How would you define ‘concussion'?” and were followed up with probing and clarifying questions.
All FGDs and SSIs were facilitated by three of the authors (AS, RT, and CSL), who were trained in qualitative methods. Facilitators ensured that documented informed consent was taken from all participants before the discussions began. Demographic data were collected from both students and coaches. Data on age, type of sports, and duration of participation were collected for student athletes. Data on the type of sports coached and duration of coaching were collected for coaches.
All discussions and interviews were audio recorded with a portable digital recording device and transcribed verbatim. Using the methodology outlined by Braun and Clarke (15), the data were analyzed with thematic analysis. AS, RT, and CSL familiarized themselves with the transcripts by rereading them several times and then coded each transcript using the code-recode strategy. All discrepancies in coding were resolved through discussion. This served to retain the trustworthiness of the data. Through this process, coded utterances were grouped into themes and frequency of utterances was recorded.
Four student FGDs that involved 42 student athletes were conducted, at which point data saturation was achieved. Each FGD comprised 10 to 11 participants and lasted from 55 to 65 min. Ninety-three (93%) were males and the median age of the participants was 16 years old with an Interquartile Range (IQR) of 15–16 years old. The median duration of sports participation was 5.0 years (IQR 1.0–7.0 years). Twenty (47.6%) were rugby players, 9 (21.4%) were football players, 6 (14.3%) were cricket players, 5 (11.9%) were softball players, 3 (7.1%) were water polo players, and 3 (7.1%) played other sports.
Fourteen coaches were recruited in total, at which point data saturation was achieved. 11 coaches were interviewed over two FGDs that lasted ~45–75 min, and the remaining three coaches were interviewed over three SSIs that lasted between 30 and 45 min. The median years of coaching were 14.5 years with an IQR of 8.5–21.5 years. Nine (64.2%) were rugby coaches, five (35.7%) were football coaches, and four (28.6%) were basketball coaches. One (7.1%) coached cricket, ice hockey, field hockey, volleyball, badminton, or wrestling.
Four major themes emerged from the student and coach sample data. We report the themes, along with top 2–3 most frequently discussed subthemes and supporting quotes, in Tables 1, 2, respectively (found on page 14 and 17, respectively).
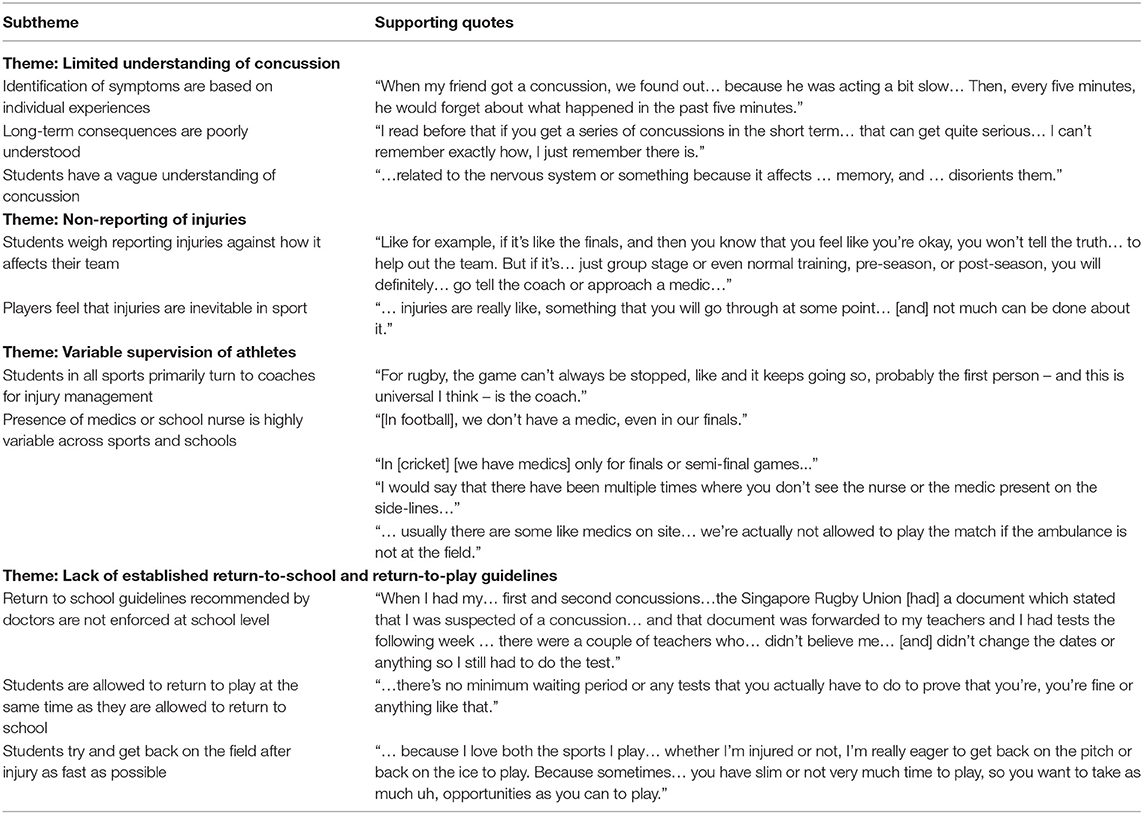
Table 1. Students' perceptions and understanding of concussion and its management.
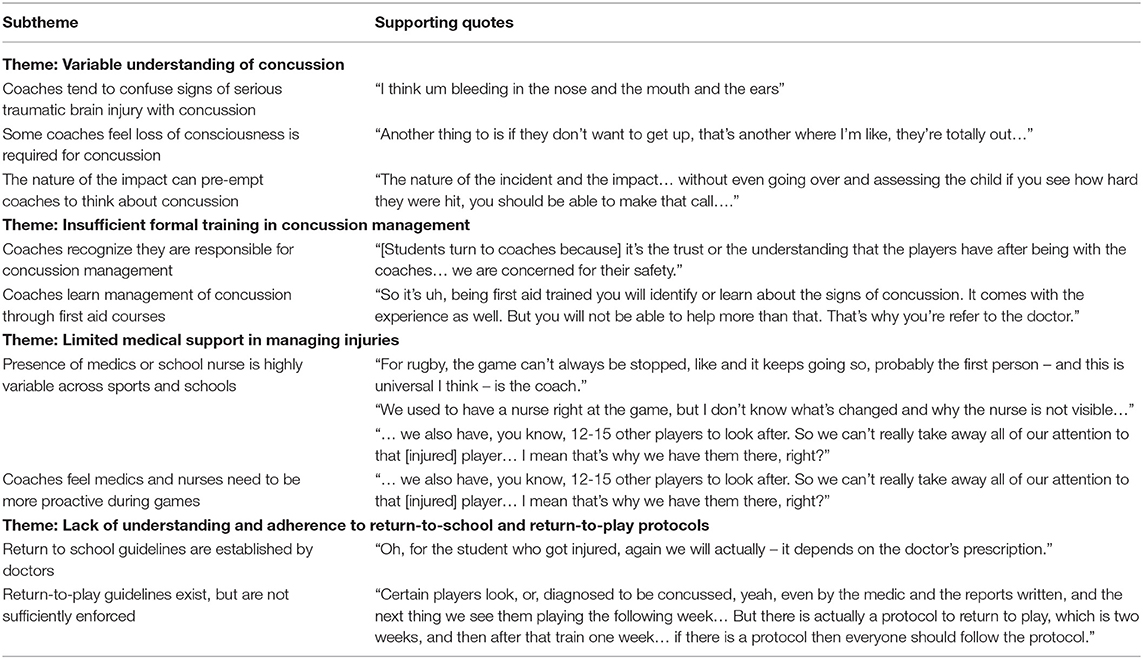
Table 2. Coaches' perceptions and understanding of concussion and its management.
Many students correctly identified that concussion was a form of brain injury, but struggled to identify specific symptoms. Most students could only identify specific symptoms of concussion through experiences they or their friends had gone through. Those who had experienced concussion stated that they did not properly understand what a concussion felt like until they experienced one. Understanding of concussion was greatest amongst rugby players. Long-term consequences of concussion were not well understood, however. Some student athletes felt there were no long-term consequences, while others felt the consequences were serious, but had difficulty listing any.
Almost all students felt that they should only report injuries if their injuries would hinder the team's performance. Reports of peer pressure from their own and the opposing team were shared. Students also felt that injury is inevitable in sports, and reporting every injury was impractical.
Almost all students identified their coach as the primary decision-maker in injury management, with otherwise variable medical supervision. In almost all schools, rugby players reported that medics were present for all tournament matches. Cricket and softball players shared that medics were only present at semi-final and final matches, while students playing other sports reported that medics were never on-site.
Students from all schools reported that their doctor decided when they were allowed to return to school. However, some shared instances of still having symptoms after returning to school. Most students stated they were allowed to return to play after returning to school, equating return-to-school as return-to-play. Students were extremely eager to return to play, often citing the fact that they felt pressured to participate and succeed in their sport as much as possible.
Many coaches demonstrated sufficient knowledge to diagnose a concussion. However, they would often confuse signs of concussion with more serious signs of traumatic brain injury (bleeding from the ears, pupil non-reactive to light, etc.). A few coaches felt that a child is not considered concussed until they lose consciousness. Many coaches agreed that the severity of impact was a reliable indicator of how likely concussion had occurred. Rugby coaches were the most familiar with concussion symptoms and signs, followed by football coaches.
All coaches agreed that they were primarily responsible for taking care of a student when they are injured. Many coaches shared that they received information about concussion management through first aid courses. No coaches had received training on management of concussion outside of these courses.
In two out of three schools, rugby coaches reported that medics were present for all matches. Football coaches shared that medics were present at quarter-, semi-, and final matches. However, in one school, coaches supervised all sports without medical assistance. Where medics were present, coaches felt that they are physically positioned too far from the pitch to witness how the injury occurred and often had to have the incident described to them, which wasted treatment time. Coaches without the support of medical supervision felt that the lack of supervision was dangerous and felt overburdened.
All coaches stated that there was no school policy on return-to-school after a concussion, and that the doctor seeing the student after their injury made this decision. As for return-to-play, most coaches allowed students to return to play once they returned to school. One school's coaches stated however that a return-to-play guideline was in place, but that not all students were following it. This guideline involved a gradual return to play that should take 3 weeks; however, it was poorly enforced.
We present—to our knowledge—the first study in Singapore seeking to identify the understanding of and attitudes toward concussion amongst local and international student athletes and their coaches. Students had basic knowledge of what concussion is; however, their terminology was vague and the majority lacked an understanding of the long-term consequences. Most coaches had an understanding of both the definition and symptoms of concussion, but could not differentiate signs of severe traumatic brain injury from concussion. A minority of coaches incorrectly stated that loss of consciousness was required for the diagnosis of concussion. Students and coaches agree that the coaches are primarily responsible for managing injuries; however, both groups identified a lack of medical assistance given to the coaches. Finally, the lack of adherence to return-to-play protocols was a troubling finding, and we propose that it should be addressed with urgency. An evidence-based policy that outlines how students should return to full participation after suffering from a concussion needs to be established and implemented as soon as possible.
A summary of other qualitative and cross-sectional studies that have examined concussion in other countries can be found in Table 3. Triangulating our findings with that of existing literature suggests agreement of broad themes but has also highlighted some inconsistencies.
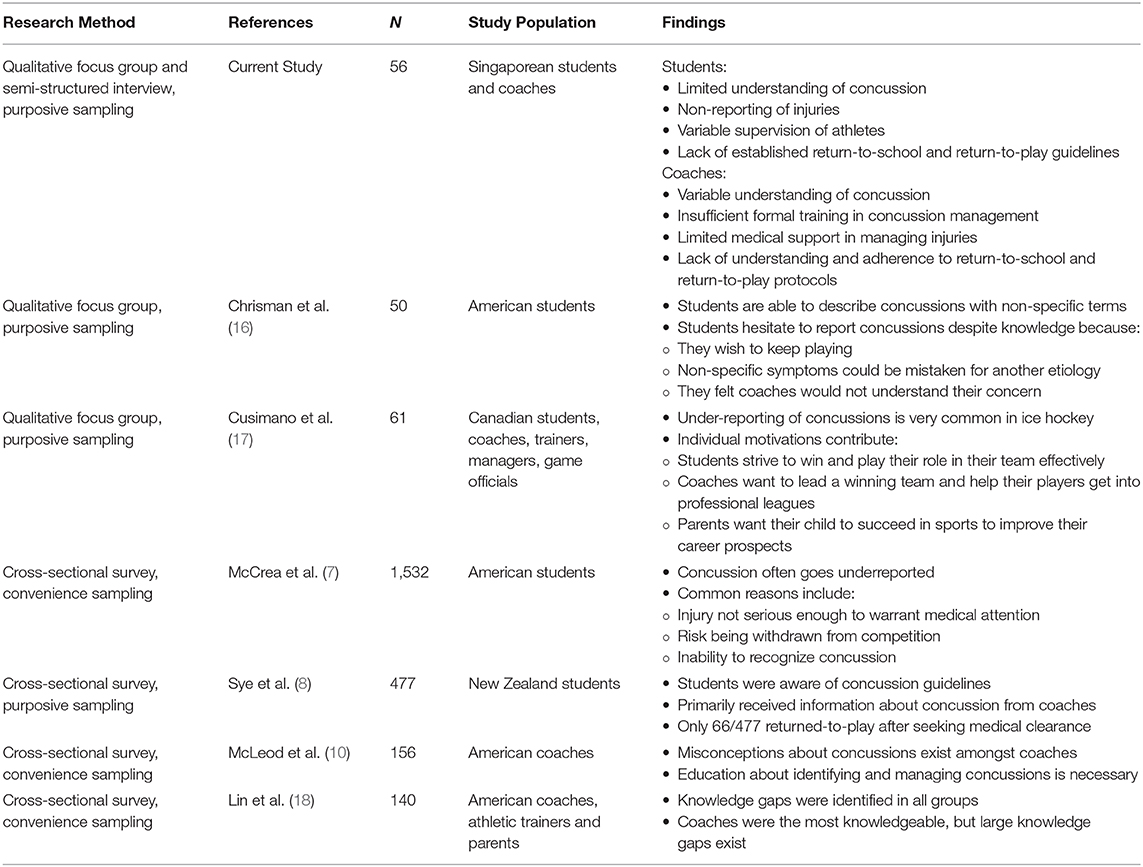
Table 3. Comparison of studies exploring understanding and management of concussion.
Regarding understanding of concussion in students, findings varied from study to study. McCrea et al. (7) found that students did not have sufficient understanding of either the seriousness or the symptoms of concussion. Cusimano et al. (17) found that 25–50% of all students surveyed could identify 0–1 symptoms of concussion. Chrisman et al. (16) found that, although student athletes used vague terms to describe concussion, their understanding was greater than what was reported in prior studies. Our study found that many students in Singapore have a limited understanding of how to identify a concussion injury. Educating student athletes in Singapore about signs and symptoms of concussion and giving them the vocabulary to describe their injuries may prove to be an effective way to discern between a truly minor head injury and a concussion.
Student athletes are dangerously underreporting potential concussions, but for differing reasons. The findings from McCrea et al. (7), an earlier study, suggest that this is likely due to the lack of knowledge. Covassin et al. (19) more recently demonstrated that the HEADS UP campaign by the Centers for Disease Control has increased concussion awareness amongst both students and coaches. Chrisman et al. (16), on the other hand, reported that student athletes do not report concussions despite their knowledge of symptoms and signs, instead citing three major barriers: their motivation to play their sport as much as possible, the fact that the symptoms of concussion can be attributed to a minor etiology, and fearing disapproval from coaches. Our study also showed that despite some understanding of concussion, students hesitate to report their injuries and are eager to return to play after sustaining their injury. We identified fear of disappointing their teammates as a barrier to reporting injuries. However, we did not identify fear of disapproval from coaches as a barrier for reporting injury. Instead, our data suggest that students feel comfortable reporting injuries to their coaches. Given that Chrisman et al. (16) surveyed students in America, this discrepancy may be due to cultural differences. As such, a multi-prong approach may be required. Besides increasing concussion awareness and potential consequences, encouraging open communication between student athletes, and between coaches and athletes, may help increase the chance of early diagnosis and treatment.
As for coaches, McLeod et al. (10) and Lin et al. (18) both reported that while coaches were knowledgeable, further education was necessary. McLeod et al. (10) found that, while coaches could identify overt symptoms of concussion, they could not identify more subtle signs and symptoms such as sleep disturbances and vision problems. Lin et al. (18) also found similar knowledge gaps about concussions. Both studies advocate for more specific education on concussion. Our results also showed that, while coaches could recognize overt signs and symptoms of concussions, knowledge gaps still exist that need to be addressed. Similar to these studies, we feel coaches in Singapore could benefit from more in-depth education on concussion over and above first aid courses.
Finally, our data showed that a clearly defined return-to-play protocol is urgently required. The Consensus Statement on Concussion in Sport heavily advocates for this, as does the Centers for Disease Control HEADS UP program (11, 20). Therefore, separate return-to-school and return-to-play guidelines should be clearly established. The United States Centers for Disease Control recommends a gradual, 5-step increase in activity during this period until full symptom recovery. A randomized controlled trial recently published by Leddy et al. (21) showed that this model of recovery, known as progressive subsymptom threshold exercise, could significantly reduce the duration of concussion symptoms. Distinct enforcement of return-to-play guidelines that is separate from return-to-school guidelines is a crucial step that Singapore must implement. The current standard of allowing students to return-to-play once they are back in school can be associated with adverse outcomes. A distinct enforcement of return-to-play guidelines is paramount for their safety (20).
We recognize the limitations of our study. Our purposive sampling technique limits the generalizability of the views expressed by the students and coaches to the population at large. However, we feel that purposive sampling helped to gather data from athletes who are at higher risk for SRRC and their coaches. In addition, we preferentially sampled from schools that have a higher participation in rugby in Singapore, which forced us to sample schools from higher socioeconomic backgrounds. This caused us to underrepresent the understanding of concussion among students of lower socioeconomic status. We also did not adequately sample female students who may have different experiences and viewpoints with regards to concussion. Finally, our limited age range did not account for younger athletes. The strength of this study lies in the interviews of both students and coaches, which greatly increased the breadth of our understanding of how concussion is perceived and managed. Our findings may help to generate hypotheses for future concussion research.
Overall, our study showed that while students had more knowledge of concussions than previous studies reported, they struggled to identify long-term consequences. They also hesitated to report head injuries because they may be removed from the game. Coaches had a good general understanding of concussion, but may benefit from specialized training focused on concussions, and, while on-site, would prefer more skilled assistance from medics. Finally, the issue of an established return-to-play policy is an important one. The authors of this study would like to recommend that the schools in Singapore adopt a policy similar to the one recommended by the Centers of Disease Control (20). We acknowledge that this policy may be difficult to implement, but we feel this issue needs to be jointly addressed by healthcare professionals, schools, and coaches to promote the safety and well-being of student athletes with concussion.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by SingHealth Centralized Institutional Review Board [CIRB Ref: 2018/2746]. Written informed consent to participate in this study was provided by the participants and their legal guardian/next of kin.
AS helped conduct the FGDs and SSIs, transcribed all FGDs and SSIs, helped analyze the transcripts, and was a major contributor in writing the manuscript. RT helped conduct the FGDs, helped analyze the transcripts, and was a major contributor in writing the manuscript. DC helped design the methodology, helped with participant recruitment, and contributed to writing the manuscript. ZN helped design the methodology and contributed to writing the manuscript. CD helped design the methodology and helped train the other authors in conducting FGDs. JF helped coordinate consent taking, data collection, and storage. S-LC helped design the methodology, conduct the FGDs, helped analyze the transcripts, and was a major contributor in writing the manuscript. All authors contributed to the article and approved the submitted version.
AS is currently receiving a grant (AM-ETHOS01/FY2018/03-A03) from Duke NUS Medical School in support of this study. Duke NUS Medical School did not contribute to designing the study, data collection, data analysis and interpretation, or writing the manuscript in any way.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank our research coordinators who helped us in this project, Mrs. Michelle Ren Mee Hiong and Ms. Rupini Piragasam for their technical assistance. We would also like to thank Prof. Eva Fenwick from Singapore Eye Research Institute for her assistance with the qualitative analysis.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.526986/full#supplementary-material
SRRC, sports and recreation-related concussion.
1. Gordon KE, Dooley JM, Wood EP. Descriptive epidemiology of concussion. Pediatr Neurol. (2006) 34:376–8. doi: 10.1016/j.pediatrneurol.2005.09.007
2. Bryan MA, Rowhani-Rahbar A, Comstock RD, Rivara F. Sports-and recreation-related concussions in US youth. Pediatrics. (2016) 138:e20154635. doi: 10.1542/peds.2015-4635
3. Christensen J, Pedersen MG, Pedersen CB, Sidenius P, Olsen J, Vestergaard M. Long-term risk of epilepsy after traumatic brain injury in children and young adults: a population-based cohort study. Lancet. (2009) 373:1105–10. doi: 10.1016/S0140-6736(09)60214-2
4. Gardner A, Iverson GL, McCrory P. Chronic traumatic encephalopathy in sport: a systematic review. Br J Sports Med. (2014) 48:84–90. doi: 10.1136/bjsports-2013-092646
5. Harmon KG, Drezner J, Gammons M, Guskiewicz K, Halstead M, Herring S, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Clin J Sport Med. (2013) 23:1–18. doi: 10.1097/JSM.0b013e31827f5f93
6. Stamm JM, Bourlas AP, Baugh CM, Fritts NG, Daneshvar DH, Martin BM, et al. Age of first exposure to football and later-life cognitive impairment in former NFL players. Neurology. (2015) 84:1114–20. doi: 10.1212/WNL.0000000000001358
7. McCrea M, Hammeke T, Olsen G, Leo P, Guskiewicz K. Unreported concussion in high school football players: implications for prevention. Clin J Sport Med. (2004) 14:13–7. doi: 10.1097/00042752-200401000-00003
8. Sye G, Sullivan SJ, McCrory P. High school rugby players' understanding of concussion and return to play guidelines. Br J Sports Med. (2006) 40:1003–5. doi: 10.1136/bjsm.2005.020511
9. Yard EE, Comstock RD. Compliance with return to play guidelines following concussion in US high school athletes, 2005–2008. Brain Inj. (2009) 23:888–98. doi: 10.1080/02699050903283171
10. McLeod TCV, Schwartz C, Bay RC. Sport-related concussion misunderstandings among youth coaches. Clin J Sport Med. (2007) 17:140–2. doi: 10.1097/JSM.0b013e31803212ae
11. McCrory P, Meeuwisse WH, Aubry M, Cantu RC, Dvorak J, Echemendia RJ, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. (2013) 47:250–8. doi: 10.1136/bjsports-2013-092313
12. Vaughn S, Schumm JS, Sinagub JM. Focus Group Interviews in Education and Psychology. Thousand Oaks, CA: SAGE Publications, Inc. (1996).
13. Barriball KL, While A. Collecting data using a semi-structured interview: a discussion paper. J Adv Nurs. (1994) 19:328–35. doi: 10.1111/j.1365-2648.1994.tb01088.x
14. Harmon KG, Drezner JA, Gammons M, Guskiewicz K, Halstead M, Herring S, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br J Sports Med. (2013) 47:15–26. doi: 10.1136/bjsports-2012-091941
15. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
16. Chrisman SP, Quitiquit C, Rivara FP. Qualitative study of barriers to concussive symptom reporting in high school athletics. J Adolesc Health. (2013) 52:330–5. doi: 10.1016/j.jadohealth.2012.10.271
17. Cusimano MD, Chipman ML, Volpe R, Donnelly P. Canadian minor hockey participants' knowledge about concussion. Can J Neurol Sci. (2009) 36:315–20. doi: 10.1017/S0317167100007046
18. Lin E, Ward I, Lequerica A, Jasey N, Chiaravalloti N. Understanding the level of concussion knowledge in High School Sports in New Jersey. PM R. (2019) 11:1107–14. doi: 10.1002/pmrj.12120
19. Covassin T, Elbin RJ, Sarmiento K. Educating coaches about concussion in sports: evaluation of the CDC's “Heads Up: Concussion in Youth Sports” initiative. J Sch Health. (2012) 82:233–8. doi: 10.1111/j.1746-1561.2012.00692.x
20. Managing Return to Activities | HEADS UP | CDC Injury Center. (n.d.). Available online at: https://www.cdc.gov/headsup/providers/return_to_activities.html (accessed April 16, 2019).
Keywords: pediatrics, head injury, rugby, football, coaches, Asia
Citation: Subramaniam A, Tan RMR, Chan D, Ng ZM, Dong CY, Feng JXY and Chong S-L (2020) Assessment of the Understanding of Concussion and Care Protocols Amongst Student Athletes and Coaches: A Qualitative Study. Front. Pediatr. 8:526986. doi: 10.3389/fped.2020.526986
Received: 26 May 2020; Accepted: 21 August 2020;
Published: 24 September 2020.
Edited by:
Hong Ni, Children's Hospital of Soochow University, ChinaReviewed by:
Caroline J. Ketcham, Elon University, United StatesCopyright © 2020 Subramaniam, Tan, Chan, Ng, Dong, Feng and Chong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shu-Ling Chong, chong.shu-ling@kkh.com.sg
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.