
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr. , 15 September 2020
Sec. Pediatric Immunology
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.00545
This article is part of the Research Topic Dietary Interventions and Nutritional Factors in the Prevention of Allergic Diseases in Infants View all 16 articles
 Enza D'Auria1*
Enza D'Auria1* Diego G. Peroni2
Diego G. Peroni2 Marco Ugo Andrea Sartorio1
Marco Ugo Andrea Sartorio1 Elvira Verduci1
Elvira Verduci1 Gian Vincenzo Zuccotti1
Gian Vincenzo Zuccotti1 Carina Venter3
Carina Venter3Nutrients in foods are not eaten in isolation and food intake interacts in a complex manner, affecting health and disease outcomes. For this reason, focusing on the whole “pattern” of dietary intake instead of the single nutrients or groups of nutrients when studying diseases outcomes is increasingly appealing and growing. Diet diversity refers to the variety of foods being eaten, and the terms, diversity or variety, are often used interchangeably. When the overall diet is characterized by healthy foods, diet diversity will reflect a diversity/variety of healthy foods eaten over a period of time. The introduction of solid foods in the 1st year of life is considered a measure of increased diet diversity. Consuming a diverse range of foods and food allergens in the first year of life may increase intake of important nutrients and positively affect the gut microbiome structure and function. Intake of omega-3 fatty acids and fibers/prebiotics may be particularly important but more information is required about dose and which individuals are most likely to benefit. Increased diet diversity in the first year of life is also associated with reduced food allergy outcomes. In addition to diet diversity, diet indices are considered measures of overall diet quality and can be used as a simple assessment of dietary intake. The focus of this paper is to review and critically address the current knowledge of the association between diet diversity and diet indices and allergy outcomes. Based on the current evidence, we recommend the introduction of solid foods, including common allergenic solids, during the 1st year of life, according to the infant's neuro-developmental abilities and familial or cultural habits. For infants with severe AD and/or FA, medical assessment may be advisable before introducing common food allergens into the diet. Limited evidence exist about the role of diet indices in pregnancy and allergic disease in the offspring, and the most promising results indicate a reduction in childhood wheeze and/or asthma intake.
Diet diversity is defined as the variety of food being eaten; the term “variety” can be used instead of “diversity” (1). If the diet consists of healthy foods, diet diversity will reflect a diversity/variety of healthy foods eaten over a period of time. Diet diversity may include the number of foods/food groups and the period and the frequency of consumption (2). In this review, we consider the introduction of solid foods in the first year of life as a measure of increased diet diversity. A more diverse diet in the 1st years of life may increase exposure to food allergens, thereby promoting tolerance development (3–7). Diet diversity may also promote an increased intake of nutrients which can be associated with allergic disease prevention. Finally, diet diversity may play a role in allergy prevention by modifying the gut microbiome. During introduction of solid food in the weaning period, higher diet diversity may increase gut microbiome diversity (8). Data regarding the effect of diet diversity in the 1st year of life and atopic dermatitis, rhinitis, and asthma development are conflicting (2).
In this review, we include studies investigating diet diversity, the development of clinical allergy outcomes, and sensitization to aeroallergens and/or foods. In addition to diet diversity, diet indices are considered measures of overall diet quality and offer a simple assessment of dietary intake. In the few last decades, several indices have been developed and employed (9). We focus on diet indices and subsequent development of allergy, with particular emphasis on the Mediterranean diet. We used a combined search strategy using search terms from three EAACI papers (2, 10, 11).
In part 1, we summarize the road map leading to current recommendations on food allergen introduction in the 1st year of life. In part 2, we focus on the effect of diet diversity and diet indices in pregnancy, lactation, and 1st year of life on allergy development.
Recommendations regarding solid food introduction in early life have changed dramatically in the past two decades. In the early 2000s, the American Academy of Pediatrics (AAP) proposed commencing complementary feeding after first six months and to delay introduction of food allergens until after one year of age in infants considered at high risk for allergy development, such as those having a first-degree relative with a history of allergic diseases. The AAP suggested introduction of milk containing foods after the age 1 year, egg after age two years, and peanuts, tree nuts, and fish after age 3 years (12).
This advice was mainly based on the evidence from two studies; the former (13) showed that early introduction of allergenic foods at 3 months increased risk of atopic disease, and the latter demonstrated a correlation existing between diet diversity before 4 months of life and risk of developing eczema later (14).
In 2006, the American College of Allergy, Asthma, and Immunology (ACAAI) suggested delayed introduction of potential allergenic foods also for children without a risk of atopy/allergic diseases (15). Despite these recommendations, the prevalence of food allergy (FA) continued to increase in Western countries (16). Many observational studies highlighted that postponing the introduction into the diet of foods with an allergenic potential may cause an increased risk of IgE-sensitization and FA (3, 17–22), especially to peanut (3) and egg (19). In support of these studies, the dual allergen hypothesis proposed that early oral food allergen introduction opposed to exposure via the skin might be protective against food allergy (23). This hypothesis is sustained by the fact that skin exposure to food allergens in infants with eczematous skin may favor a Th2 response leading to allergic sensitization (24), whereas oral exposure leads to tolerance.
In 2008, the AAP updated their previous recommendations highlighting that there was not sufficient evidence to postpone introduction into the infants' diet of potential allergenic foods (25). No recommendations were made at that stage about the timing of the introduction of foods. The lack of clear information about food allergen intake at the time was addressed by a number of randomized controlled trials.
The Learning Early About Peanut Allergy (LEAP) study by Du Toit et al. (4) demonstrated that introduction of peanut in high-risk atopic infants younger than 1 year old suffering from severe atopic dermatitis and/or egg allergy could reduce the development of peanut allergy. In this study, 640 infants were randomly divided into two groups: some were assigned to consume peanuts, other to avoid peanuts up to 60 months of age. Development of peanut allergy was then tested by an oral food challenge.
The intention to threat analysis showed a significantly lower prevalence of PA in the intervention group than in the control group both in the group with a negative SPT to peanut at the beginning of the study and in children with SPT results of 1–4 mm. Noteworthy, infants (7/640) who had never been fed peanuts previously had positive oral peanut challenge at enrolment both in the case of positive SPTs (6 out of 47, 12.8%) and negative SPTs (1 out of 272, 0.4%).
The authors used the term “early introduction” reflecting introduction between 4 and 11 months, differently from the delayed introduction (after 2 years of age), previously recommended in international guidelines (12), indicating the importance of introducing peanut in the 1st year of life and continuing with regular peanut intake once introduced.
The LEAP-On follow-up study showed that cessation of peanut intake for 1 year, after consumption for 5 years, did not lead to a significant increase of peanut allergy by 6 years of age (26).
The ongoing Preventing Peanut Allergy in Atopic Dermatitis (PEAAD) trial is evaluating if peanut ingestion for one year, in infants and children aged 5–30 months and suffering from AD, may have an effect on the development of peanut allergy (27).
Several randomized controlled trials (RCTs) focused on clarifying whether the earlier introduction (before 6 months of age) of other potential allergenic foods (e.g., egg) into diet may prevent the occurrence of developing allergic sensitization and FA (4, 26, 28–32). These RCTs are summarized in Table 1.
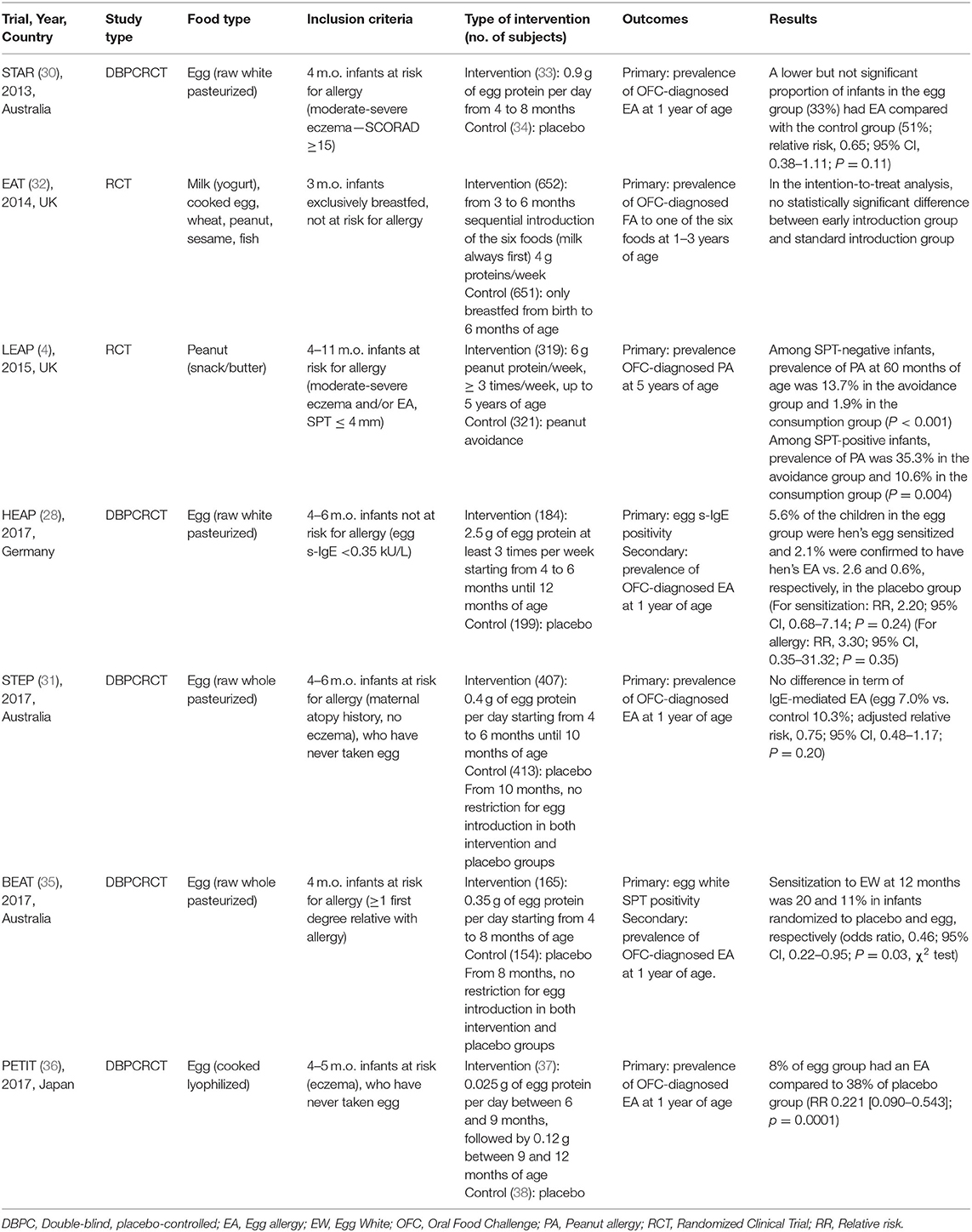
Table 1. Food allergy prevention via early introduction of allergenic food: list of RCTs.
Studies evaluating the effects of early introduction of egg gave contrasting results, probably related to variation in the study design (populations, outcomes) and in the dose and the form of egg used (i.e., cooked vs. raw egg; Table 1).
The Solid Timing for Allergy Research (STAR Study) (30) trial reported that early introduction of egg had no protective effect on the development of EA in high risk infants who had never eaten egg. The study was discontinued because of a high rate of allergic reactions to pasteurized raw egg. Since then, two RCTs showed no difference in the development of egg sensitization or EA in high risk infants consuming or avoiding egg.
The Australian Study Starting Time of Egg Protein (STEP) trial (31) considered 820 at risk infants (e.g., infants with atopic mothers) who had never consumed egg and did not show allergic symptoms. Infants were randomly allocated to consume pasteurized raw egg or placebo from 4 to 6 months of life until 10 months. No differences were found at the intention-to-treat (ITT) analysis between the active and placebo groups in terms of OFC-diagnosed EA development (7% active vs. 10.3% control) and in cutaneous sensitization, defined by positive egg SPT (10.8% active vs. 15.1% control, P = 0.15) at 12 months.
The Beat Egg Allergy Trial (BEAT) (35) randomized children at high risk (having at least a first-degree relative with atopic disease), not sensitized, to receive pasteurized whole raw egg powder or placebo from 4 to 8 months of age. At 12 months, no difference was observed for the percentages of positive challenge between the two groups (10.5% active vs. 6.2% placebo), despite a lower prevalence of sensitization to egg white in the active group.
In the Hen's Egg Allergy Prevention (HEAP) (28) infants aged 4–6 months without risk factors for allergy development were recruited and randomly assigned to be fed pasteurized raw egg white powder or placebo. At 12 months of age, no difference was observed in the prevalence of EA or egg specific-IgE between the two groups.
The most recent Prevention of Egg allergy with Tiny Amount Intake (PETIT) (36) trial assessed the safety and efficacy of a step-wise introduction of heated egg (equivalent to 0.2 g of whole egg boiled for 15 min) in a sample of infants with mild to severe atopic dermatitis, no immediate allergic reaction to egg, and no history of immediate allergic reaction to egg or to any type of food. All infants were treated with topical treatment for AD during the study.
The results of the study showed a statistically significant decrease of OFC-diagnosed EA at 12 months of age in the study group (8% intervention vs. 38% control, p < 0.0001).
However, it should be pointed out that only per protocol analysis was conducted and the primary outcome (OFC-diagnosed EA) was not established in 26 (17%) infants; thus, these findings need to be treated with caution.
A recent meta-analysis of RCTs (39) (Table 1) showed with moderate evidence that egg introduction at the age of 4–6 months reduces EA occurrence. However, the conclusions of this meta-analysis mainly relied on the results of the PETIT study (36), in which the stepwise introduction of cooked egg from six months of age seemed to be effective in reducing EA prevalence.
A recent RCT showed that avoiding cow's milk formula supplementation in newborns for the first 3 days of life reduce sensitization to cow's milk and food allergy (40).
Similarly, a Finnish cohort study (n = 6,200 infants), with a follow-up of 18–34 months, found that exposure to cow's milk (CM) proteins within the first few days of life increased the risk for CM allergy (34). In contrast, a cohort study from Israel reported that the introduction of CM proteins within the first 2 weeks of life was associated to a lower risk of CM allergy development, and introduction between 4 and 6 months of life was associated to a higher risk (40).
Omega-3 fatty acids (present in fatty fish) have anti-inflammatory properties. Observational studies investigated if a relationship exists between the timing of fish introduction and the risk of subsequent asthma and atopic diseases (41–45). Pooling the results of these studies showed that there is limited evidence to support early fish introduction (before 9 months of life) for reducing the risk of allergic sensitization, rhinitis (35), and asthma (46). Nevertheless, fish contains important nutrients and omega-3 fatty acids play an important role in development of the central nervous system (47, 48). We feel reasonable to recommend fish introduction during the second semester of life, timing based on local tradition, weaning approach, and family preferences (49, 50).
In summary, the introduction of peanuts from 4 to 11 months of age in infants at high risk of developing PA may be beneficial to prevent peanut allergy. The same may be true for introduction of heated egg. With regard to early introduction of other allergenic foods (milk, fish, and cereals) most of the available data are from observational studies and do not prove a cause-effect relationship.
The Enquiring About Tolerance (EAT) is the only intervention trial which aimed to investigate the effects on allergy development of early ingestion of different food allergens (i.e., milk, peanut, egg, wheat, fish, and sesame) in exclusively breastfed infants with unknown risk of allergy status (32).
The per protocol analysis revealed a statistically significant decrease of overall FA (2.4 vs. 7.3%, p = 0.01), PA (0 vs. 2.5%, p = 0.003; NNT 40) in the early introduction group compared to the control; the ITT analysis did not show a different occurrence of FA to at least one of the six foods at three years follow-up. In the per protocol analysis, the NNT was very high. The findings of this study suggested a possible effect on FA prevention with introduction of foods and food allergens between 3 and 6 months of age. However, non-adherence rate in the intervention group was substantial (68.1%) and may lead to bias in the per-protocol analysis (51). It also indicated the difficulty for parents to introduce so many allergens at such an early age (33). Of note, the lowest adherence rate was reported for the introduction of egg (43.1%).
In many of these studies, infants were sensitized just before introducing the allergenic food/s (4, 24, 26, 27). This suggests that other factors, including genetics, epigenetics, and gut flora, could take part in FA development before weaning (52–56).
In response to the Learning Early About Peanut (LEAP) study (4) and a number of RCTs on egg and multiple allergen introductions, guidelines around the world were adapted. The first were the ASCIA (57) guidelines suggesting that peanut, cooked egg, wheat, and dairy foods should be introduced into infants' diet in the 1st year of life. The NIAID (USA) guidelines (2017) (58) suggested different peanut introduction schedules depending on the degree of risk: in infants affected by severe atopic dermatitis and/or EA from 4 to 6 months while around 6 months in infants with mild to moderate eczema and that family and cultural feeding practices should be followed in infants with no eczema or any food allergies. The latest COT report (UK) (59) and BSACI guidance (60) suggest to introduce complementary foods, in the general population, from around 6 months of age, including peanut and egg. The BSACI guidance suggests that in high risk infants, parents may wish to start complementary feeding around 4 months of age. Parents may also consider to include egg and peanut, but current guidelines are in disagreement about the feasibility and need for assessment prior to introduction.
The most recent update AAP guidelines (61) state that there is no evidence for postponing food allergen introduction beyond 4–6 months, including allergenic foods.
In summary: Evidence suggests introduction of peanut and egg before 11 months of age in high risk infants, after medical assessment. These foods can be given also as part of the weaning diet in low risk infants, ideally before 1 year. There is no/limited evidence regarding the other food allergens but it does not suggest to delay introduction of these foods unnecessarily (Table 2).
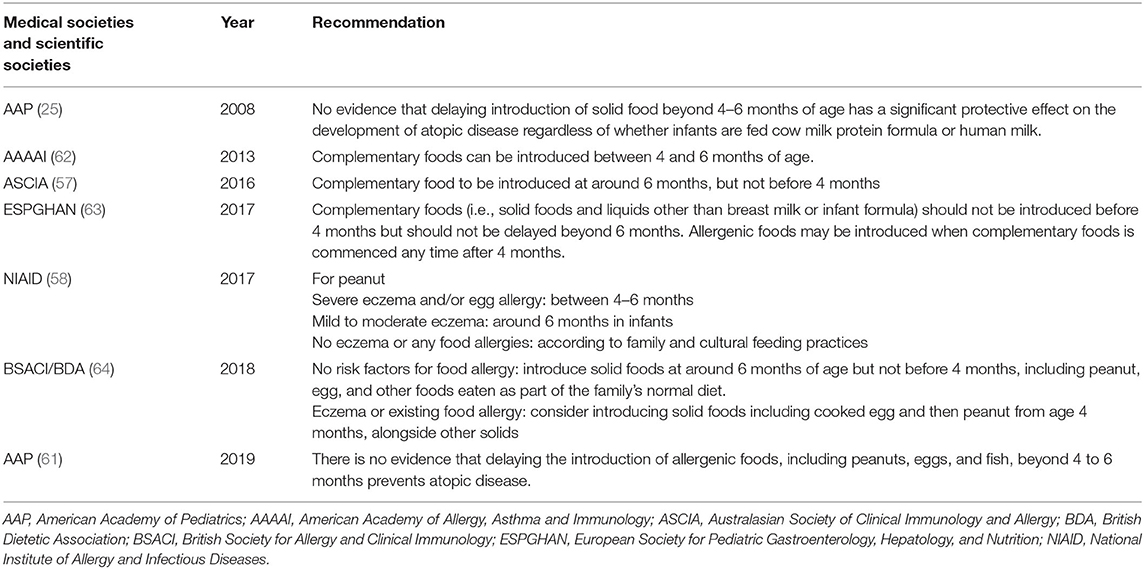
Table 2. Timing of the introduction of potential food allergens.
The role of diet diversity in pregnancy and offspring outcomes has not been studied.
The PASTEUR/EFRAIM Study by Carole Roduit et al. (37) is the first study specifically describing the role of diet variety in early life and its effect on food allergy development. This prospective, multicenter study evaluated the association between complementary food introduction in the 1st year of life and allergy sensitization or clinical outcomes up to 6 years of age. In this study, diet variety was defined by investigators in two ways: Definition 1: group of 15 different foods frequently assumed by 80% of the study population in the first 12 months of age. Definition 2: group of the 6 major foods introduced in the first 6 months or first 12 months of life. The risk of sensitization to food allergens at the age of 4.5 or 6 years was higher in the group of children with lower diet diversity. The same study also showed a reduction in reported doctor-diagnosed food allergy up to 6 years of age associated with increased introduction of vegetables/fruits, cereals, bread, meat, cake, and yogurt within the first 6 months or first 12 months of life.
In addition to this study, Venter et al. (38) recently reported an association between increased diet diversity in the first year of life and reduced odds of food allergy over the first decade of life. In particular, they showed that the introduction of each additional food at 6 months of age reduced by 10.8% the odds of developing food allergy over the first 10 years of life. Moreover, for each additional food allergen introduced by 12 months, it reported a significant reduction of 33.2% in the likelihood of food allergy over the first 10 years of life. These studies may indicate that diet diversity is associated with increased nutrient intake, including those nutrients which could have a protective role on allergy development (omega-3 fatty acids and non-digestible fibers) (65, 66). Other studies investigated the effect of diet diversity in early life and allergy outcomes are summarized in Table 3.
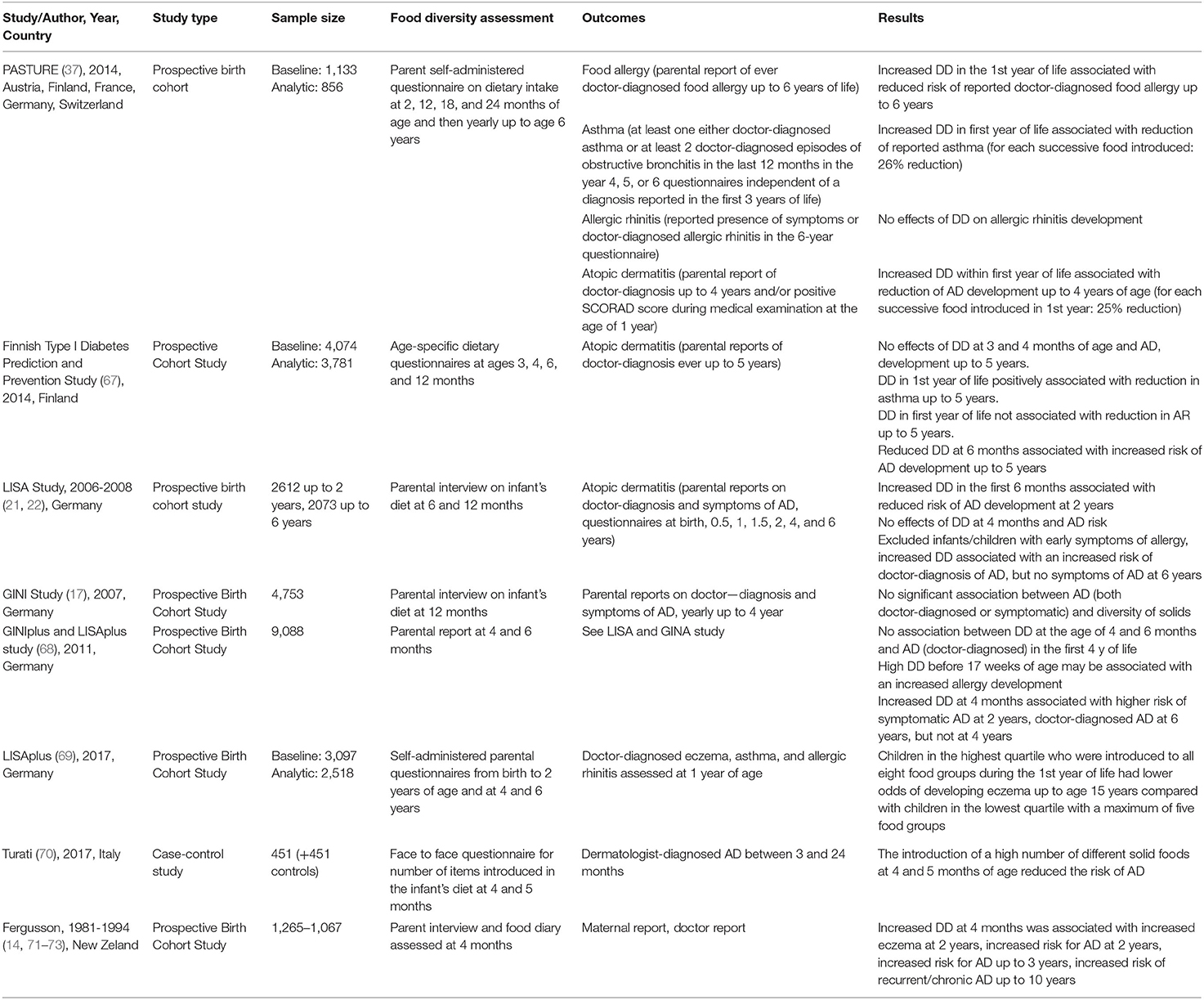
Table 3. Allergy prevention via diet diversity increase: list of studies.
Omega-3 long-chain polyunsaturated fatty acids (LCPUFAs) are essential nutrients found in many foods such as fatty/oily fish, fish oil, and nuts (66, 74, 75). Evidence from in vitro and in vivo studies have shown that omega-3 fatty acids are able to lower pro-inflammatory cytokines and antagonize IgE responses and mast cells degranulation (66, 74). An imbalance in omega-6 fatty acid intake vs. omega-3 fatty acid in people eating a Western Diet (76, 77) has been considered as a possible reason for the increase in allergic diseases. This may be due to the pro-inflammatory activity of omega-6 fatty which favors a Th2 immune response (78).
However, other than some effect on allergen sensitization, evidence from RCTS is not conclusive to support omega-3 fatty acid supplementation for offspring allergy prevention during pregnancy and/or lactation (65, 66). Omega-3 fatty acid supplementation has also been studied in infancy and childhood with conflicting results. Using house dust mite (HDM) avoidance and dietary fatty acid modification during the first 5 years of life, the Childhood Asthma Prevention Study (CAPS) showed modification of the plasma fatty acids status (increasing omega-3/omega-6 ratio) at age 5 years, but no clinical effects (79).
D'Vaz et al. (80) showed that in infants at high risk of atopy, supplementation of omega 3 fatty acids for the first 6 months of life had beneficial effects on preventing sensitization, eczema, and food allergy. Similarly, Birch et al. (81) demonstrated that infant formula supplemented with omega-3 fatty acids in healthy infants is protective against allergic disease (wheezing/asthma, wheezing/asthma/atopic dermatitis, or any allergy) throughout three years of life. The difference in findings of these studies may be explained by differences in the underlying diet, high risk/low risk populations, dose of supplements used, timing and duration of supplementation, or serum levels of omega-3 intake at the start of the trial (75, 79, 80, 82, 83).
Prebiotics are defined as a “substrate that is selectively utilized by host microorganisms conferring a health benefit” (84). They naturally occur in foods or can be artificially produced as galactooligosaccharides (GOS) and fructooligosaccharides (FOS). In the large bowel, prebiotics undergo fermentation by local bacteria modulating the microbiota composition. Microbiota can, in turn, produce beneficial metabolites such as short-chain fatty acids with known anti-inflammatory effects. Human milk contains more than different 400 oligosaccharides which act also as prebiotics (66) and can shape infant gut microbiota composition (85). Following from this, prebiotics have been added to infant formula trying to mimic the beneficial effect of breastmilk (85).
A recent metaanalysis including 22 studies assessed the effect of supplementing prebiotics in infants on the risk of development of allergic symptoms. Studies on infants at high risk and normal risk of allergy were included. Most of these studies evaluated FOS with GOS supplementation added to infant formula. The authors concluded that the evidence for supplementation of prebiotics for the prevention of allergies are not strong enough to make any clear recommendations (86).
Focusing on the whole “pattern” of dietary intake instead of the single nutrients or groups of nutrients when studying diseases outcomes is therefore increasingly appealing and growing. This is because nutrients and foods are not eaten in isolation. All food intake interacts in a complex manner to determine well-being or disease.
If there is a place for diet diversity in allergy prevention, then the mechanisms of action need to be clarified. Diet diversity may affect the gut microbiome by providing a more diverse food intake which may increase intake of fiber and other nutrients affecting the gut microbiome. Very few studies have compared diet diversity to gut microbiome diversity. The first study conducted by Claesson et al. (87) showed that increased diet diversity in the elderly was associated with increased gut microbial diversity. If introduction of solid food is considered an increase in diet diversity, then this would be another example of how diet diversity increases gut microbiome diversity. This was reflected by increased protein intake, carbohydrate, and fiber intake, as well as in increased intake of family foods (88). Increased gut microbial diversity has been related to reduced allergen sensitization (89) and allergy outcomes in both children and adults (90–92).
Three diet indices in pregnancy have been studied in relation to allergy outcomes in infants, the healthy eating index (93–95), the diet inflammatory index (95, 96), and the Mediterranean diet index (93, 97–100) (Table 4).
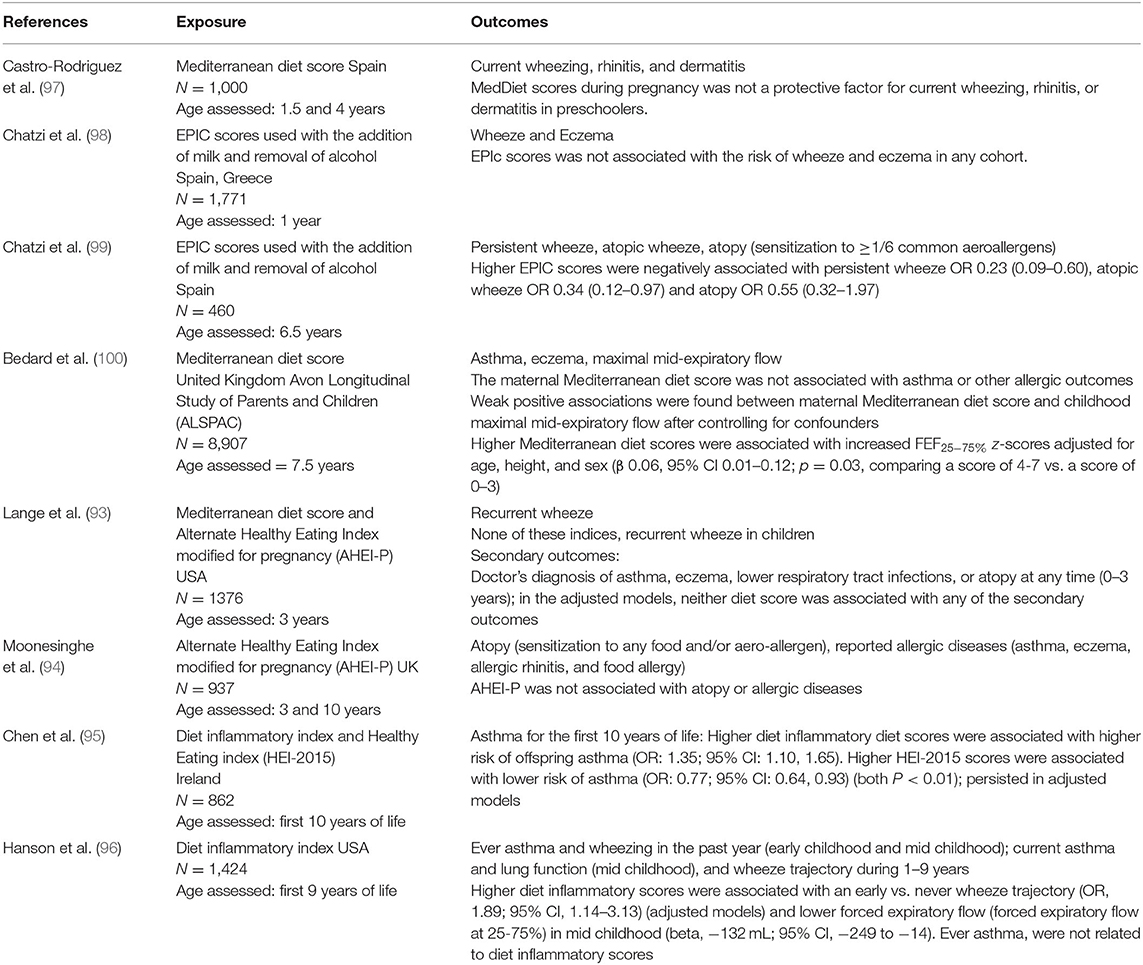
Table 4. Diet indices in pregnancy and allergy outcomes in the offspring.
Three studies have studied the role of healthy eating in pregnancy and childhood allergy outcomes. In one study (Food Allergy and Research Study, UK), the Alternate Healthy Eating Index modified for pregnancy (AHEI-P) was used to examine associations with allergic outcomes in the offspring at 3 and 10 years (94). This study found no association between the AHEI-P and atopy (defined as sensitization to any food and/or aero-allergen) or reported allergic diseases at 3 or 10 years. Lange et al. (93) used data from the Project Viva cohort (US) and found no association between the HEI and recurrent wheeze in infants at the age of 3 years. In contract, Chen et al. (95) using data from an Irish cohort found that higher HEI-2015 scores were associated with lower risk of asthma (OR: 0.77; 95% CI: 0.64, 0.93) (both P < 0.01) and the effect persisted in adjusted models.
Two studies have looked at the association between a pro-inflammatory diet in pregnancy and asthma, wheeze, or lung function outcomes through childhood (95, 96). One recent study from Ireland (95) showed an association between DII scores and asthma outcomes over 10 years. The Project viva (US) study showed an association of DII scores with wheeze trajectories, but not asthma, up to 7.5 years of age (96).
The associations between the Mediterranean diet index and allergy outcomes have been studied in by five cohorts (93, 97–99) (two from Spain, one from Greece, one from the USA, and one from the UK). Four studies investigated wheeze in the infant (93, 97–99), four studies investigated rhinitis, atopic dermatitis, and/or eczema (97–100), two studies included sensitization to food/aero-allergens (93, 99), and two studies investigated asthma in the child (93). Four of the five studies found no association between the Mediterranean diet index and the allergic outcomes studied (93, 97, 98, 100). Childhood persistent wheeze, atopic wheeze, and atopy was associated with the Mediterranean diet index in only one of the studies (99). One study (100) found an association between the Mediterranean diet score and childhood maximal mid-expiratory flow as well as FEF25−75% z-scores.
Based on the current evidence, limited recommendations can be made about the role of diet indices in pregnancy and allergy outcomes in the offspring. The most potential of these indices may be in the prevention of lung function, wheeze, or asthma outcomes in the offspring.
The role of diet indices in infancy vs. subsequent development of allergic outcomes in later childhood have not been conducted. A number of studies have however looked at the Mediterranean diet in childhood vs. allergy outcomes, using either the KIDMED mediterranean score (99, 101–106) or the adult EPIC score (107–115) and the diet inflammatory index (116, 117) (Table 5).
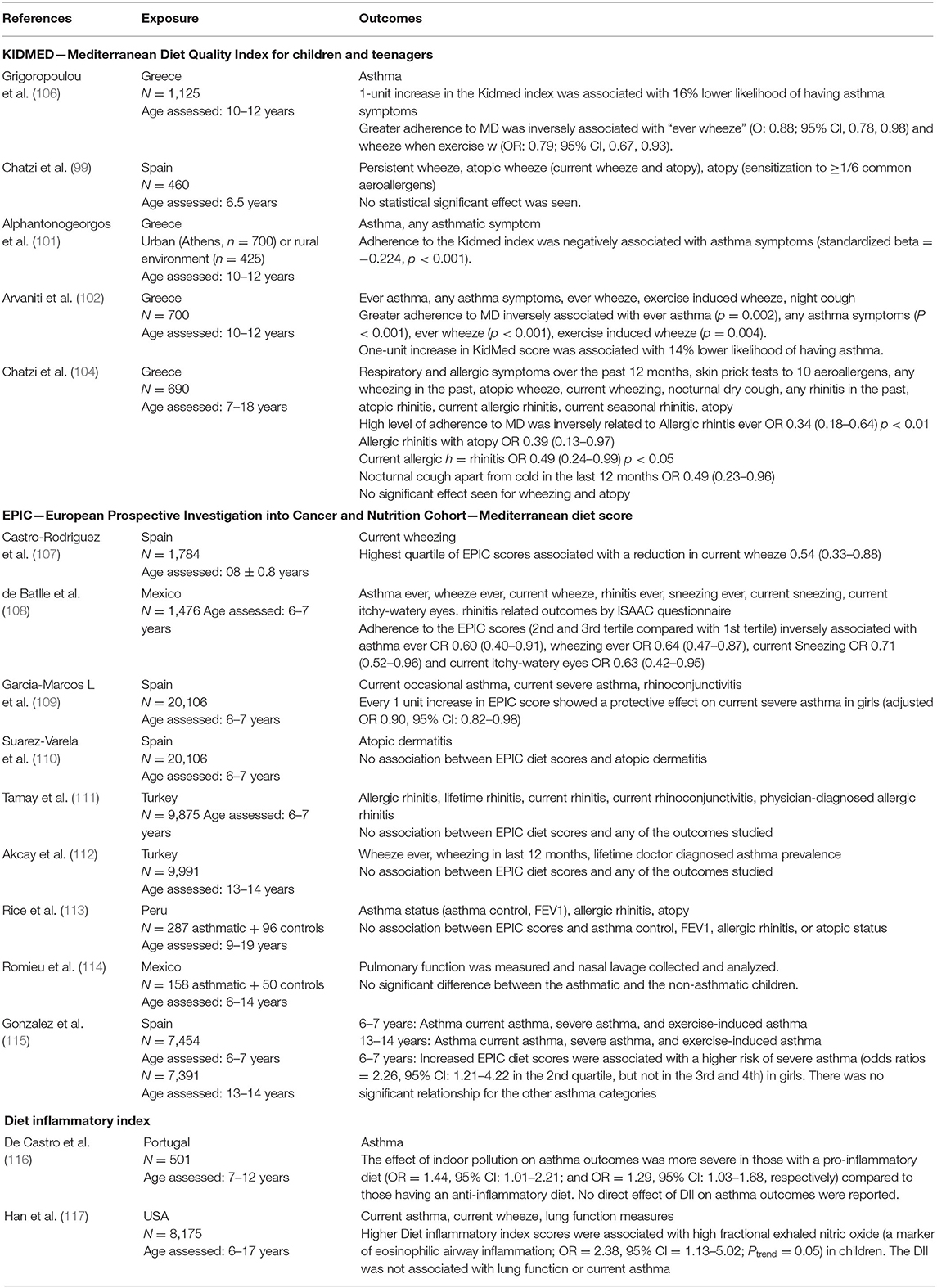
Table 5. Diet indices in childhood and allergy outcomes.
Two studies investigated the role of the diet inflammatory index on allergy development in the children (116, 117) and neither one of these could find an association between diet inflammatory scores and asthma in the child. One study found that indoor pollution on asthma outcomes was more severe in those with a pro-inflammatory diet than those following an anti-inflammatory diet (116).
Three studies found reduced allergy outcomes with an increase in mediterranean diet scores: reduced current wheeze (107), asthma ever, wheezing ever, current sneezing, and current itchy-watery eyes (108), and severe asthma in girls (109). Five studies found no effect on any of the outcomes studied (110–114) and one study found an increased risk of severe asthma, with increased mediterranean diet scores (115).
Based on the current evidence, we recommend the introduction of solid foods, including common allergenic foods, during the 1st year of life, according to the infant's neuro-developmental abilities and familial or cultural habits.
In infants with severe AD and/or FA, medical assessment may be advisable before introducing common food allergens into the diet. Consuming a diverse range of foods in the 1st year of life may increase intake of nutrients and positively affect the gut microbiome composition. Intake of omega-3 fatty acids and fibers/prebiotics may be particularly important, but more information is required about dose and which individuals are most likely to benefit. Increased diet variety in the first year of life is also associated with reduced food allergy outcomes. Limited evidence exist about the role of diet indices in pregnancy and allergic disease in the offspring. The most promising results indicate a reduction in childhood wheeze and/or asthma. Further studies are warranted to investigate the effects of diet diversity during pregnancy and lactation and diet indices in early life on the development of allergic diseases in infants and children.
ED'A conceptualized the paper, wrote the introduction, and the section on diet diversity. DP critically reviewed the draft and proofread the paper. MS wrote the abstract and made tables on diet diversity. EV contributed to write the section on diet diversity. GZ made final revisions of the draft. CV wrote the section on diet indices, made tables on diet indices, and critically reviewed the paper. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Ruel MT. Is dietary diversity an indicator of food security or dietary quality? A review of measurement issues and research needs. Food Nutr Bull. (2003) 24:231–2. doi: 10.1177/156482650302400217
2. Venter C, Meyer RW, Nwaru BI, Roduit C, Untersmayr E, Adel-Patient K, et al. EAACI position paper: influence of dietary fatty acids on asthma, food allergy, and atopic dermatitis. Allergy. (2019) 74:1429–44. doi: 10.1111/all.13764
3. Du Toit G, Katz Y, Sasieni P, Mesher D, Maleki SJ, Fisher HR, et al. Early consumption of peanuts in infancy is associated with a low prevalence of peanut allergy. J Allergy Clin Immunol. (2008) 122:984–91. doi: 10.1016/j.jaci.2008.08.039
4. Du Toit G, Roberts G, Sayre PH, Bahnson HT, Radulovic S, Santos AF, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med. (2015) 372:803–13. doi: 10.1056/NEJMoa1414850
5. Lundell AC, Hesselmar B, Nordström I, Adlerberth I, Wold AE, Rudin A. Higher B-cell activating factor levels at birth are positively associated with maternal dairy farm exposure and negatively related to allergy development. J Allergy Clin Immunol. (2015) 136:1074–82.e3. doi: 10.1016/j.jaci.2015.03.022
6. Matricardi PM. 99th Dahlem conference on infection, inflammation and chronic inflammatory disorders: controversial aspects of the ‘hygiene hypothesis'. Clin Exp Immunol. (2010) 160:98–105. doi: 10.1111/j.1365-2249.2010.04130.x
7. Perkin MR, Logan K, Marrs T, Radulovic S, Craven J, Flohr C, et al. Enquiring about tolerance (EAT) study: feasibility of an early allergenic food introduction regimen. J Allergy Clin Immunol. (2016) 137:1477–86.e8. doi: 10.1016/j.jaci.2015.12.1322
8. Savage JH, Lee-Sarwar KA, Sordillo JE, Lange NE, Zhou Y, O'Connor GT, et al. Diet during pregnancy and infancy and the infant intestinal microbiome. J Pediatr. (2018) 203:47–54.e4. doi: 10.1016/j.jpeds.2018.07.066
9. Fransen HP, Ocké MC. Indices of diet quality. Curr Opin Clin Nutr Metab Care. (2008) 11:559–65. doi: 10.1097/MCO.0b013e32830a49db
10. de Silva D, Geromi M, Halken S, Host A, Panesar SS, Muraro A, et al. Primary prevention of food allergy in children and adults: systematic review. Allergy. (2014) 69:581–9. doi: 10.1111/all.12334
11. Venter C, Greenhawt M, Meyer RW, Agostoni C, Reese I, du Toit G, et al. EAACI position paper on diet diversity in pregnancy, infancy and childhood: novel concepts and implications for studies in allergy and asthma. Allergy. (2020) 75:497–523. doi: 10.1111/all.14051
12. American Academy of Pediatrics. Committee on Nutrition. Hypoallergenic infant formulas. Pediatrics. (2000) 106:346–9. doi: 10.1542/peds.106.2.346
13. Kajosaari M. Atopy prevention in childhood: the role of diet. Prospective 5-year follow-up of high-risk infants with six months exclusive breastfeeding and solid food elimination. Pediatr Allergy Immunol. (1994) 5:26–8. doi: 10.1111/j.1399-3038.1994.tb00344.x
14. Fergusson DM, Horwood LJ, Shannon FT. Early solid feeding and recurrent childhood eczema: a 10-year longitudinal study. Pediatrics. (1990) 86:541–6.
15. Fiocchi A, Assa'ad A, Bahna S. Food allergy and the introduction of solid foods to infants: a consensus document. Adverse Reactions to Foods Committee, American College of Allergy, Asthma and Immunology. Ann Allergy Asthma Immunol. (2006) 97:10–20; quiz 1:77. doi: 10.1016/S1081-1206(10)61364-6
16. Prescott SL, Pawankar R, Allen KJ, Campbell DE, Sinn J, Fiocchi A, et al. A global survey of changing patterns of food allergy burden in children. World Allergy Organ J. (2013) 6:21. doi: 10.1186/1939-4551-6-21
17. Filipiak B, Zutavern A, Koletzko S, von Berg A, Brockow I, Grübl A, et al. Solid food introduction in relation to eczema: results from a four-year prospective birth cohort study. J Pediatr. (2007) 151:352–8. doi: 10.1016/j.jpeds.2007.05.018
18. Koplin JJ, Osborne NJ, Wake M, Martin PE, Gurrin LC, Robinson MN, et al. Can early introduction of egg prevent egg allergy in infants? A population-based study. J Allergy Clin Immunol. (2010) 126:807–13. doi: 10.1016/j.jaci.2010.07.028
19. Nwaru BI, Erkkola M, Lumia M, Kronberg-Kippilä C, Ahonen S, Kaila M, et al. Maternal intake of fatty acids during pregnancy and allergies in the offspring. Br J Nutr. (2012) 108:720–32. doi: 10.1017/S0007114511005940
20. Tromp IIM, Kiefte-de Jong JC, Lebon A, Renders CM, Jaddoe VW, Hofman A, et al. The introduction of allergenic foods and the development of reported wheezing and eczema in childhood: the Generation R study. Arch Pediatr Adolesc Med. (2011) 165:933–8. doi: 10.1001/archpediatrics.2011.93
21. Zutavern A, Brockow I, Schaaf B, Bolte G, von Berg A, Diez U, et al. Timing of solid food introduction in relation to atopic dermatitis and atopic sensitization: results from a prospective birth cohort study. Pediatrics. (2006) 117:401–11. doi: 10.1542/peds.2004-2521
22. Zutavern A, Brockow I, Schaaf B, von Berg A, Diez U, Borte M, et al. Timing of solid food introduction in relation to eczema, asthma, allergic rhinitis, and food and inhalant sensitization at the age of 6 years: results from the prospective birth cohort study LISA. Pediatrics. (2008) 121:e44–52. doi: 10.1542/peds.2006-3553
23. Lack G. Epidemiologic risks for food allergy. J Allergy Clin Immunol. (2008) 121:1331–6. doi: 10.1016/j.jaci.2008.04.032
24. Noti M, Kim BS, Siracusa MC, Rak GD, Kubo M, Moghaddam AE, et al. Exposure to food allergens through inflamed skin promotes intestinal food allergy through the thymic stromal lymphopoietin-basophil axis. J Allergy Clin Immunol. (2014) 133:1390–9:9.e1–6. doi: 10.1016/j.jaci.2014.01.021
25. Greer FR, Sicherer SH, Burks AW. Effects of early nutritional interventions on the development of atopic disease in infants and children: the role of maternal dietary restriction, breastfeeding, timing of introduction of complementary foods, and hydrolyzed formulas. Pediatrics. (2008) 121:183–91. doi: 10.1542/peds.2007-3022
26. Du Toit G, Sayre PH, Roberts G, Sever ML, Lawson K, Bahnson HT, et al. Effect of avoidance on peanut allergy after early peanut consumption. N Engl J Med. (2016) 374:1435–43. doi: 10.1056/NEJMoa1514209
27. Caffarelli C, Di Mauro D, Mastrorilli C. Solid food introduction and the development of food allergies. Nutrients. (2018) 10:1790. doi: 10.3390/nu10111790
28. Bellach J, Schwarz V, Ahrens B, Trendelenburg V, Aksünger Ö, Kalb B, et al. Randomized placebo-controlled trial of hen's egg consumption for primary prevention in infants. J Allergy Clin Immunol. (2017) 139:1591–9.e2. doi: 10.1016/j.jaci.2016.06.045
29. Lødrup Carlsen KC, Rehbinder EM, Skjerven HO, Carlsen MH, Fatnes TA, Fugelli P, et al. Preventing Atopic Dermatitis and ALLergies in Children-the PreventADALL study. Allergy. (2018) 73:2063–70. doi: 10.1111/all.13468
30. Palmer DJ, Metcalfe J, Makrides M, Gold MS, Quinn P, West CE, et al. Early regular egg exposure in infants with eczema: a randomized controlled trial. J Allergy Clin Immunol. (2013) 132:387–92.e1. doi: 10.1016/j.jaci.2013.05.002
31. Palmer DJ, Sullivan TR, Gold MS, Prescott SL, Makrides M. Randomized controlled trial of early regular egg intake to prevent egg allergy. J Allergy Clin Immunol. (2017) 139:1600–7.e2. doi: 10.1016/j.jaci.2016.06.052
32. Perkin MR, Logan K, Tseng A, Raji B, Ayis S, Peacock J, et al. Randomized trial of introduction of allergenic foods in breast-fed infants. N Engl J Med. (2016) 374:1733–43. doi: 10.1056/NEJMoa1514210
33. Voorheis P, Bell S, Cornelsen L, Quaife M, Logan K, Marrs T, et al. Challenges experienced with early introduction and sustained consumption of allergenic foods in the Enquiring About Tolerance (EAT) study: a qualitative analysis. J Allergy Clin Immunol. (2019) 144:1615–23. doi: 10.1016/j.jaci.2019.09.004
34. Saarinen KM, Juntunen-Backman K, Järvenpää AL, Kuitunen P, Lope L, Renlund M, et al. Supplementary feeding in maternity hospitals and the risk of cow's milk allergy: a prospective study of 6209 infants. J Allergy Clin Immunol. (1999) 104:457–61. doi: 10.1016/S0091-6749(99)70393-3
35. Wei-Liang Tan J, Valerio C, Barnes EH, Turner PJ, Van Asperen PA, Kakakios AM, et al. A randomized trial of egg introduction from 4 months of age in infants at risk for egg allergy. J Allergy Clin Immunol. (2017) 139:1621–8.e8. doi: 10.1016/j.jaci.2016.08.035
36. Natsume O, Kabashima S, Nakazato J, Yamamoto-Hanada K, Narita M, Kondo M, et al. Two-step egg introduction for prevention of egg allergy in high-risk infants with eczema (PETIT): a randomised, double-blind, placebo-controlled trial. Lancet. (2017) 389:276–86. doi: 10.1016/S0140-6736(16)31418-0
37. Roduit C, Frei R, Depner M, Schaub B, Loss G, Genuneit J, et al. Increased food diversity in the first year of life is inversely associated with allergic diseases. J Allergy Clin Immunol. (2014) 133:1056–64. doi: 10.1016/j.jaci.2013.12.1044
38. Meyer R, Chebar Lozinsky A, Fleischer DM, Vieira MC, Du Toit G, Vandenplas Y, et al. Diagnosis and management of Non-IgE gastrointestinal allergies in breastfed infants-An EAACI Position Paper. Allergy. (2020) 75:14–32. doi: 10.1111/all.13947
39. Ierodiakonou D, Garcia-Larsen V, Logan A, Groome A, Cunha S, Chivinge J, et al. Timing of allergenic food introduction to the infant diet and risk of allergic or autoimmune disease: a systematic review and meta-analysis. JAMA. (2016) 316:1181–92. doi: 10.1001/jama.2016.12623
40. Urashima M, Mezawa H, Okuyama M, Urashima T, Hirano D, Gocho N, et al. Primary prevention of cow's milk sensitization and food allergy by avoiding supplementation with cow's milk formula at birth: a randomized clinical trial. JAMA Pediatr. (2019) 173:1137–45. doi: 10.1001/jamapediatrics.2019.3544
41. Hesselmar B, Saalman R, Rudin A, Adlerberth I, Wold A. Early fish introduction is associated with less eczema, but not sensitization, in infants. Acta Paediatr. (2010) 99:1861–7. doi: 10.1111/j.1651-2227.2010.01939.x
42. Kull I, Bergström A, Lilja G, Pershagen G, Wickman M. Fish consumption during the first year of life and development of allergic diseases during childhood. Allergy. (2006) 61:1009–15. doi: 10.1111/j.1398-9995.2006.01115.x
43. Nwaru BI, Takkinen HM, Niemelä O, Kaila M, Erkkola M, Ahonen S, et al. Timing of infant feeding in relation to childhood asthma and allergic diseases. J Allergy Clin Immunol. (2013) 131:78–86. doi: 10.1016/j.jaci.2012.10.028
44. Oddy WH, de Klerk NH, Kendall GE, Mihrshahi S, Peat JK. Ratio of omega-6 to omega-3 fatty acids and childhood asthma. J Asthma. (2004) 41:319–26. doi: 10.1081/JAS-120026089
45. Virtanen SM, Kaila M, Pekkanen J, Kenward MG, Uusitalo U, Pietinen P, et al. Early introduction of oats associated with decreased risk of persistent asthma and early introduction of fish with decreased risk of allergic rhinitis. Br J Nutr. (2010) 103:266–73. doi: 10.1017/S0007114509991541
46. Papamichael MM, Shrestha SK, Itsiopoulos C, Erbas B. The role of fish intake on asthma in children: A meta-analysis of observational studies. Pediatr Allergy Immunol. (2018) 29:350–60. doi: 10.1111/pai.12889
47. D'Auria E, Pendezza E, Zuccotti GV. Personalized nutrition in food allergy: tips for clinical practice. Front Pediatr. (2020) 8:113. doi: 10.3389/fped.2020.00113
48. Martinez M. Tissue levels of polyunsaturated fatty acids during early human development. J Pediatr. (1992) 120:S129–38. doi: 10.1016/S0022-3476(05)81247-8
49. D'Auria E, Abrahams M, Zuccotti GV, Venter C. Personalized nutrition approach in food allergy: is it prime time yet? Nutrients. (2019) 11:359. doi: 10.3390/nu11020359
50. D'Auria E, Bergamini M, Staiano A, Banderali G, Pendezza E, Penagini F, et al. Baby-led weaning: what a systematic review of the literature adds on. Ital J Pediatr. (2018) 44:49. doi: 10.1186/s13052-018-0487-8
52. Cahenzli J, Köller Y, Wyss M, Geuking MB, McCoy KD. Intestinal microbial diversity during early-life colonization shapes long-term IgE levels. Cell Host Microbe. (2013) 14:559–70. doi: 10.1016/j.chom.2013.10.004
53. Paparo L, Nocerino R, Cosenza L, Aitoro R, D'Argenio V, Del Monaco V, et al. Epigenetic features of FoxP3 in children with cow's milk allergy. Clin Epigenet. (2016) 8:86. doi: 10.1186/s13148-016-0252-z
54. Sabounchi S, Bollyky J, Nadeau K. Review of environmental impact on the epigenetic regulation of atopic diseases. Curr Allergy Asthma Rep. (2015) 15:33. doi: 10.1007/s11882-015-0533-1
55. Wesemann DR, Nagler CR. The microbiome, timing, and barrier function in the context of allergic disease. Immunity. (2016) 44:728–38. doi: 10.1016/j.immuni.2016.02.002
56. Suaini NHA, Wang Y, Soriano VX, Martino DJ, Allen KJ, Ellis JA, et al. Genetic determinants of paediatric food allergy: a systematic review. Allergy. (2019) 74:1631–48. doi: 10.1111/all.13767
57. ASCIA Guidelines. Infant Feeding and Allergy Prevention. (2016). Available online at: https://www.allergy.org.au/images/pcc/ASCIA_Guidelines_infant_feeding_and_allergy_prevention.pdf (accessed May 04, 2020).
58. Togias A, Cooper SF, Acebal ML, Assa'ad A, Baker JR Jr, Beck LA, et al. Addendum guidelines for the prevention of peanut allergy in the United States: Report of the National Institute of Allergy and Infectious Diseases-sponsored expert panel. J Allergy Clin Immunol. (2017) 139:29–44. doi: 10.1016/j.jaci.2016.10.010
59. Assessing the Health Benefits and Risks of the Introduction of Peanut and Hen's Egg into the Infant Diet Before Six Months of Age in the UK. A Joint Statement from the Scientific Advisory Committee on Nutrition and the Committee on Toxicity of Chemicals in food, Consumer products and the Environment (2018). Available online at: https://cot.food.gov.uk/sites/default/files/jointsacncotallergystatement-april2018.pdf
60. Turner PJ, Feeney M, Meyer R, Perkin MR, Fox AT. Implementing primary prevention of food allergy in infants: new BSACI guidance published. Clin Exp Allergy. (2018) 48:912–5. doi: 10.1111/cea.13218
61. Greer FR, Sicherer SH, Burks AW. The effects of early nutritional interventions on the development of atopic disease in infants and children: the role of maternal dietary restriction, breastfeeding, hydrolyzed formulas, and timing of introduction of allergenic complementary foods. Pediatrics. (2019) 143:e2019081. doi: 10.1542/peds.2019-0281
62. Fleischer DM, Spergel JM, Assa'ad AH, Pongracic JA. Primary prevention of allergic disease through nutritional interventions. J Allergy Clin Immunol Pract. (2013) 1:29–36. doi: 10.1016/j.jaip.2012.09.003
63. Fewtrell M, Bronsky J, Campoy C, Domellöf M, Embleton N, Fidler Mis N, et al. Complementary feeding: a position paper by the european society for paediatric gastroenterology, hepatology, and nutrition (ESPGHAN) committee on nutrition. J Pediatr Gastroenterol Nutr. (2017) 64:119–32. doi: 10.1097/MPG.0000000000001454
64. British Society for Allergy and Clinical Immunology/British Dietetic Association. Preventing Food Allergy in Higher Risk Infants: Guidance for Healthcare Professionals. (2018). Available online at: https://www.bsaci.org/about/early-feeding-guidance (accessed May 04, 2020).
65. Garcia-Larsen V, Ierodiakonou D, Jarrold K, Cunha S, Chivinge J, Robinson Z, et al. Diet during pregnancy and infancy and risk of allergic or autoimmune disease: a systematic review and meta-analysis. PLoS Med. (2018) 15:e1002507. doi: 10.1371/journal.pmed.1002507
66. Venter C, Brown KR, Maslin K, Palmer DJ. Maternal dietary intake in pregnancy and lactation and allergic disease outcomes in offspring. Pediatr Allergy Immunol. (2017) 28:135–43. doi: 10.1111/pai.12682
67. Nwaru BI, Takkinen HM, Kaila M, Erkkola M, Ahonen S, Pekkanen J, et al. Food diversity in infancy and the risk of childhood asthma and allergies. J Allergy Clin Immunol. (2014) 133:1084–91. doi: 10.1016/j.jaci.2013.12.1069
68. Sausenthaler S, Heinrich J, Koletzko S. Early diet and the risk of allergy: what can we learn from the prospective birth cohort studies GINIplus and LISAplus? Am J Clin Nutr. (2011) 94:2012s–7s. doi: 10.3945/ajcn.110.001180
69. Markevych I, Standl M, Lehmann I, von Berg A, Heinrich J. Food diversity during the first year of life and allergic diseases until 15 years. J Allergy Clin Immunol. (2017) 140:1751–4.e4. doi: 10.1016/j.jaci.2017.08.011
70. Turati F, Bertuccio P, Galeone C, Pelucchi C, Naldi L, Bach JF, et al. Early weaning is beneficial to prevent atopic dermatitis occurrence in young children. Allergy. (2016) 71:878–88. doi: 10.1111/all.12864
71. Fergusson DM, Horwood LJ. Early solid food diet and eczema in childhood: a 10-year longitudinal study. Pediatr Allergy Immunol. (1994) 5:44–7. doi: 10.1111/j.1399-3038.1994.tb00347.x
72. Fergusson DM, Horwood LJ, Beautrais AL, Shannon FT, Taylor B. Eczema and infant diet. Clin Allergy. (1981) 11:325–31. doi: 10.1111/j.1365-2222.1981.tb01602.x
73. Fergusson DM, Horwood LJ, Shannon FT. Risk factors in childhood eczema. J Epidemiol Commun Health. (1982) 36:118–22. doi: 10.1136/jech.36.2.118
74. Hoppenbrouwers T, Cvejić Hogervorst JH, Garssen J, Wichers HJ, Willemsen LEM. Long Chain Polyunsaturated Fatty Acids (LCPUFAs) in the prevention of food allergy. Front Immunol. (2019) 10:1118. doi: 10.3389/fimmu.2019.01118
75. Muley P, Shah M, Muley A. Omega-3 fatty acids supplementation in children to prevent asthma: is it worthy?-a systematic review and meta-analysis. J Allergy. (2015) 2015:312052. doi: 10.1155/2015/312052
76. Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med. (2008) 233:674–88. doi: 10.3181/0711-MR-311
77. Simopoulos AP. An increase in the omega-6/omega-3 fatty acid ratio increases the risk for obesity. Nutrients. (2016) 8:128. doi: 10.3390/nu8030128
78. Willemsen LEM. Dietary n-3 long chain polyunsaturated fatty acids in allergy prevention and asthma treatment. Eur J Pharmacol. (2016) 785:174–86. doi: 10.1016/j.ejphar.2016.03.062
79. Marks GB, Mihrshahi S, Kemp AS, Tovey ER, Webb K, Almqvist C, et al. Prevention of asthma during the first 5 years of life: a randomized controlled trial. J Allergy Clin Immunol. (2006) 118:53–61. doi: 10.1016/j.jaci.2006.04.004
80. D'Vaz N, Meldrum SJ, Dunstan JA, Martino D, McCarthy S, Metcalfe J, et al. Postnatal fish oil supplementation in high-risk infants to prevent allergy: randomized controlled trial. Pediatrics. (2012) 130:674–82. doi: 10.1542/peds.2011-3104
81. Birch EE, Khoury JC, Berseth CL, Castañeda YS, Couch JM, Bean J, et al. The impact of early nutrition on incidence of allergic manifestations and common respiratory illnesses in children. J Pediatr. (2010) 156:902–6.e1. doi: 10.1016/j.jpeds.2010.01.002
82. D'Auria E, Miraglia Del Giudice M, Barberi S, Mandelli M, Verduci E, Leonardi S, et al. Omega-3 fatty acids and asthma in children. Allergy Asthma Proc. (2014) 35:233–40. doi: 10.2500/aap.2014.35.3736
83. Yang H, Xun P, He K. Fish and fish oil intake in relation to risk of asthma: a systematic review and meta-analysis. PLoS One. (2013) 8:e80048. doi: 10.1371/journal.pone.0080048
84. Gibson GR, Hutkins R, Sanders ME, Prescott SL, Reimer RA, Salminen SJ, et al. Expert consensus document: the International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat Rev Gastroenterol Hepatol. (2017) 14:491–502. doi: 10.1038/nrgastro.2017.75
85. Forsberg A, West CE, Prescott SL, Jenmalm MC. Pre- and probiotics for allergy prevention: time to revisit recommendations? Clin Exp Allergy. (2016) 46:1506–21. doi: 10.1111/cea.12838
86. Cuello-Garcia C, Fiocchi A, Pawankar R, Yepes-Nuñez JJ. Prebiotics for the prevention of allergies: A systematic review and meta-analysis of randomized controlled trials. Clin Exp Allergy. (2017) 47:1468–77. doi: 10.1111/cea.13042
87. Claesson MJ, Jeffery IB, Conde S, Power SE, O'Connor EM, Cusack S, et al. Gut microbiota composition correlates with diet and health in the elderly. Nature. (2012) 488:178–84. doi: 10.1038/nature11319
88. Laursen MF, Andersen LB, Michaelsen KF, Molgaard C, Trolle E, Bahl MI, et al. Infant gut microbiota development is driven by transition to family foods independent of maternal obesity. mSphere. (2016) 1:e00069–15. doi: 10.1128/mSphere.00069-15
89. Azad MB, Konya T, Guttman DS, Field CJ, Sears MR, HayGlass KT, et al. Infant gut microbiota and food sensitization: associations in the first year of life. Clin Exp Allergy. (2015) 45:632–43. doi: 10.1111/cea.12487
90. Bisgaard H, Li N, Bonnelykke K, Chawes BL, Skov T, Paludan-Muller G, et al. Reduced diversity of the intestinal microbiota during infancy is associated with increased risk of allergic disease at school age. J Allergy Clin Immunol. (2011) 128:646–52.e1–5. doi: 10.1016/j.jaci.2011.04.060
91. Dong P, Feng JJ, Yan DY, Lyu YJ, Xu X. Early-life gut microbiome and cow's milk allergy- a prospective case - control 6-month follow-up study. Saudi J Biol Sci. (2018) 25:875–80. doi: 10.1016/j.sjbs.2017.11.051
92. Hua X, Goedert JJ, Pu A, Yu G, Shi J. Allergy associations with the adult fecal microbiota: analysis of the American gut project. EBioMedicine. (2016) 3:172–9. doi: 10.1016/j.ebiom.2015.11.038
93. Lange NE, Rifas-Shiman SL, Camargo CA Jr, Gold DR, Gillman MW, Litonjua AA, et al. Maternal dietary pattern during pregnancy is not associated with recurrent wheeze in children. J Allergy Clin Immunol. (2010) 126:250–55.e4. doi: 10.1016/j.jaci.2010.05.009
94. Moonesinghe H, Patil VK, Dean T, Arshad SH, Glasbey G, Grundy J, et al. Association between healthy eating in pregnancy and allergic status of the offspring in childhood. Ann Allergy Asthma Immunol. (2016) 116:163–5. doi: 10.1016/j.anai.2015.11.005
95. Chen LW, Lyons B, Navarro P, Shivappa N, Mehegan J, Murrin CM, et al. Maternal dietary inflammatory potential and quality are associated with offspring asthma risk over 10-year follow-up: the lifeways cross-generation cohort study. Am J Clin Nutr. (2020) 111:440–7. doi: 10.1093/ajcn/nqz297
96. Hanson C, Rifas-Shiman SL, Shivappa N, Wirth MD, Hebert JR, Gold D, et al. Associations of prenatal dietary inflammatory potential with childhood respiratory outcomes in project viva. J Allergy Clin Immunol Pract. (2019) 8:945–52.e4. doi: 10.1016/j.jaip.2019.10.010
97. Castro-Rodriguez JA, Ramirez-Hernandez M, Padilla O, Pacheco-Gonzalez RM, Perez-Fernandez V, Garcia-Marcos L. Effect of foods and Mediterranean diet during pregnancy and first years of life on wheezing, rhinitis and dermatitis in preschoolers. Allergol Immunopathol (Madr). (2016) 44:400–9. doi: 10.1016/j.aller.2015.12.002
98. Chatzi L, Garcia R, Roumeliotaki T, Basterrechea M, Begiristain H, Iniguez C, et al. Mediterranean diet adherence during pregnancy and risk of wheeze and eczema in the first year of life: INMA (Spain) and RHEA (Greece) mother-child cohort studies. Br J Nutr. (2013). 110:2058–68. doi: 10.1017/S0007114513001426
99. Chatzi L, Torrent M, Romieu I, Garcia-Esteban R, Ferrer C, Vioque J, et al. Mediterranean diet in pregnancy is protective for wheeze and atopy in childhood. Thorax. (2008) 63:507–13. doi: 10.1136/thx.2007.081745
100. Bedard A, Northstone K, Henderson AJ, Shaheen SO. Mediterranean diet during pregnancy and childhood respiratory and atopic outcomes: birth cohort study. Eur Respir J. (2020) 55. doi: 10.1183/13993003.01215-2019
101. Alphantonogeorgos G, Panagiotakos DB, Grigoropoulou D, Yfanti K, Papoutsakis C, Papadimitriou A, et al. Investigating the associations between Mediterranean diet, physical activity and living environment with childhood asthma using path analysis. Endocr Metab Immune Disord Drug Targets. (2014) 14:226–33. doi: 10.2174/1871530314666140826102514
102. Arvaniti F, Priftis KN, Papadimitriou A, Papadopoulos M, Roma E, Kapsokefalou M, et al. Adherence to the Mediterranean type of diet is associated with lower prevalence of asthma symptoms, among 10-12 years old children: the PANACEA study. Pediatr Allergy Immunol. (2011) 22:283–9. doi: 10.1111/j.1399-3038.2010.01113.x
103. Arvaniti F, Priftis KN, Papadimitriou A, Yiallouros P, Kapsokefalou M, Anthracopoulos MB, et al. Salty-snack eating, television or video-game viewing, and asthma symptoms among 10- to 12-year-old children: the PANACEA study. J Am Diet Assoc. (2011) 111:251–7. doi: 10.1016/j.jada.2010.10.051
104. Chatzi L, Apostolaki G, Bibakis I, Skypala I, Bibaki-Liakou V, Tzanakis N, et al. Protective effect of fruits, vegetables and the Mediterranean diet on asthma and allergies among children in Crete. Thorax. (2007) 62:677–83. doi: 10.1136/thx.2006.069419
105. Chatzi L, Torrent M, Romieu I, Garcia-Esteban R, Ferrer C, Vioque J, et al. Diet, wheeze, and atopy in school children in Menorca, Spain. Pediatr Allergy Immunol. (2007) 18:480–5. doi: 10.1111/j.1399-3038.2007.00596.x
106. Grigoropoulou D, Priftis KN, Yannakoulia M, Papadimitriou A, Anthracopoulos MB, Yfanti K, et al. Urban environment adherence to the Mediterranean diet and prevalence of asthma symptoms among 10- to 12-year-old children: the physical activity, nutrition, and allergies in children examined in Athens study. Allergy Asthma Proc. (2011) 32:351–8. doi: 10.2500/aap.2011.32.3463
107. Castro-Rodriguez JA, Garcia-Marcos L. What are the effects of a mediterranean diet on allergies and asthma in children? Front Pediatr. (2017) 5:72. doi: 10.3389/fped.2017.00072
108. de Batlle J, Garcia-Aymerich J, Barraza-Villarreal A, Anto JM, Romieu I. Mediterranean diet is associated with reduced asthma and rhinitis in Mexican children. Allergy. (2008) 63:1310–6. doi: 10.1111/j.1398-9995.2008.01722.x
109. Garcia-Marcos L, Robertson CF, Ross Anderson H, Ellwood P, Williams HC, Wong GW, et al. Does migration affect asthma, rhinoconjunctivitis and eczema prevalence? Global findings from the international study of asthma and allergies in childhood. Int J Epidemiol. (2014) 43:1846–54. doi: 10.1093/ije/dyu145
110. Suarez-Varela MM, Alvarez LG, Kogan MD, Ferreira JC, Martinez Gimeno A, Aguinaga Ontoso I, et al. Diet and prevalence of atopic eczema in 6 to 7-year-old schoolchildren in Spain: ISAAC phase III. J Investig Allergol Clin Immunol. (2010) 20:469–75.
111. Tamay Z, Akcay A, Ergin A, Guler N. Dietary habits and prevalence of allergic rhinitis in 6 to 7-year-old schoolchildren in Turkey. Allergol Int. (2014) 63:553–62. doi: 10.2332/allergolint.13-OA-0661
112. Akcay A, Tamay Z, Hocaoglu AB, Ergin A, Guler N. Risk factors affecting asthma prevalence in adolescents living in Istanbul, Turkey. Allergol Immunopathol (Madr). (2014) 42:449–58. doi: 10.1016/j.aller.2013.05.005
113. Rice JL, Romero KM, Galvez Davila RM, Meza CT, Bilderback A, Williams DL, et al. Association between adherence to the Mediterranean diet and asthma in Peruvian children. Lung. (2015) 193:893–9. doi: 10.1007/s00408-015-9792-9
114. Romieu I, Barraza-Villarreal A, Escamilla-Nunez C, Texcalac-Sangrador JL, Hernandez-Cadena L, Diaz-Sanchez D, et al. Dietary intake, lung function and airway inflammation in Mexico City school children exposed to air pollutants. Respir Res. (2009) 10:122. doi: 10.1186/1465-9921-10-122
115. Gonzalez Barcala FJ, Pertega S, Bamonde L, Garnelo L, Perez Castro T, Sampedro M, et al. Mediterranean diet and asthma in Spanish schoolchildren. Pediatr Allergy Immunol. (2010) 21:1021–7. doi: 10.1111/j.1399-3038.2010.01080.x
116. de Castro Mendes F, Paciencia I, Cavaleiro Rufo J, Silva D, Cunha P, Farraia M, et al. The inflammatory potential of diet impacts the association between air pollution and childhood asthma. Pediatr Allergy Immunol. (2019) 31:290–6. doi: 10.1111/pai.13185
Keywords: diet diversity, diet indices, pregnancy, allergy outcomes, microbiome
Citation: D'Auria E, Peroni DG, Sartorio MUA, Verduci E, Zuccotti GV and Venter C (2020) The Role of Diet Diversity and Diet Indices on Allergy Outcomes. Front. Pediatr. 8:545. doi: 10.3389/fped.2020.00545
Received: 08 May 2020; Accepted: 29 July 2020;
Published: 15 September 2020.
Edited by:
Claudio Pignata, University of Naples Federico II, ItalyReviewed by:
Riccardo Castagnoli, University of Pavia, ItalyCopyright © 2020 D'Auria, Peroni, Sartorio, Verduci, Zuccotti and Venter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Enza D'Auria, ZW56YS5kYXVyaWFAdW5pbWkuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.