
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 13 May 2020
Sec. Neonatology
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.00188
 Carlos Zozaya1*
Carlos Zozaya1* Inés García González2Alejandro Avila-Alvarez3Niki Oikonomopoulou1Tomás Sánchez Tamayo4
Inés García González2Alejandro Avila-Alvarez3Niki Oikonomopoulou1Tomás Sánchez Tamayo4 Enrique Salguero4Miguel Saenz de Pipaón5,6
Enrique Salguero4Miguel Saenz de Pipaón5,6 Fermín García-Muñoz Rodrigo7
Fermín García-Muñoz Rodrigo7 María L. Couce2,6
María L. Couce2,6Background: Data regarding the incidence and mortality of necrotizing enterocolitis trends are scarce in the literature. Recently, some preventive strategies have been confirmed (probiotics) or increased (breastfeeding rate). This study aims to describe the trends of necrotizing enterocolitis incidence, treatment, and mortality over the last decade in Spain.
Methods: Multicenter cohort study with data from the Spanish Neonatal Network–SEN1500 database. The study period comprised from January 2005 to December 2017. Preterm infants <32 weeks of gestational age at birth without major congenital malformations were included for analysis. The main study outcomes were necrotizing enterocolitis incidence, co-morbidity (bronchopulmonary dysplasia, late-onset sepsis, cystic periventricular leukomalacia, retinopathy of prematurity, acute kidney injury), mortality, and surgical/non-surgical treatment.
Results: Among the 25,821 included infants, NEC incidence was 8.8% during the whole study period and remained stable when comparing 4-year subperiods. However, more cases were surgically treated (from 48.8% in 2005–2008 to 70.2% in 2015–2017, p < 0.001). Mortality improved from 36.7% in the 2005–2008 to 26.6% in 2015–2017 (p < 0.001). Breastfeeding rates improved over the studied years (24.3% to 40.5%, p < 0.001), while gestational age remained invariable (28.5 weeks, p = 0.20). Prophylactic probiotics were implemented during the study period in some units, reaching 18.6% of the patients in 2015–2017.
Conclusions: The incidence of necrotizing enterocolitis remained stable despite the improvement regarding protective factors frequency. Surgical treatment became more frequent over the study period, whereas mortality decreased.
Necrotizing enterocolitis (NEC), one of the most important causes of morbidity and mortality in preterm infants, is related to dysbiosis, severe inflammation, and ischemic necrosis of the intestinal wall (1). The most consistent risk factor is the prematurity. Indeed, 90% of the cases occur in newborns less than 32 weeks of gestation, and there is an inverse relationship between gestational age and NEC incidence (2). The incidence has remained comparatively stable over the last years, ~6–10% of the very low birthweight infants (1). Nevertheless, it is widely variable according to the literature, ranging from 1.6% in Japan to 22% in Sweden (3, 4).
Over the last decades, some preventive strategies have been implemented (probiotics) or improved (formula rate reduction): whereas no changes regarding the medical treatment have been introduced other than improvements in general neonatal intensive care. Antibiotics, bowel rest and decompression, and supportive intensive care measures remained the standard of care. Surgery in case of perforation, but also in selected cases—clinical deterioration despite medical treatment—might be also part of the treatment. Mortality rate may reach up to 20–45%, which makes NEC one of the leading causes of death in preterm infants (5, 6).
The present study aims to report the incidence, rate of associated co-morbidity, need for surgical treatment, and mortality in very low birthweight neonates included in the SEN1500 database and describe their trends throughout the years 2005–2017 to identify weak points and potential improvement areas.
This is a multicenter cohort study. Data have been extracted from the Spanish Neonatal Network SEN1500 database. In this database, data about all admitted infants born <1500 g at birth are collected (7). For this study, only patients born from 24 to 31+6 weeks gestational age were selected. Patients with major congenital malformations were excluded from the analysis. The study period comprises from January 2005 to December 2017. For data analysis, it has been divided into four sub-periods: 2005–2008, 2009–2011, 2012–2014, and 2015–2017.
NEC was diagnosed in the participant centers based on a pre-specified definition (SEN1500 Manual of Operations) that adopted the Vermont Oxford Network definition (8). Accordingly, NEC was diagnosed based:
a) On the findings during surgery,
b) On a post-mortem study, or
c) On at least one of the following clinical criteria: bilious gastric aspirate or emesis, abdominal distension, or gross or occult blood in the stool, and at least one of the following radiological findings: pneumatosis intestinalis, hepatobiliary gas, or pneumoperitoneum.
NEC was classified in the database as non-surgical/surgical (laparotomy with or without intestinal resection or peritoneal drain insertion), depending on the treatment reported.
Bronchopulmonary dysplasia (BPD) was considered as oxygen at 36 weeks postmenstrual age (moderate-severe BPD) (9). Late-onset sepsis (LONS) was considered if confirmed by blood and/or cerebrospinal fluid (CSF) culture after the third day of life. Cystic periventricular leukomalacia was diagnosed by head ultrasound and defined as multiple small cystic changes affecting the periventricular white mater. Acute kidney injury was defined as oligo-anuria and/or endogenous plasmatic creatinine > 1.5 mg/dl. Small for gestational age was considered as birth weight < 10th percentile based on the 2013 Fenton reference curves (10). Exclusive breast milk feeding at discharge was the only nutritional data available in the original database and was used as a surrogate of exclusive human milk feeding in this study.
Descriptive results are reported as mean ± standard deviation or percentage (n/n denominator), depending on the type of variable. Univariable analysis has been done applying either two-tailed Student t test or exact Fisher test as indicated. Logistic regression models adjusting for confounding factors have been built. ANOVA was used to compare means between more than two groups. Statistical analysis has been performed with Stata 13.1 statistical software (StataCorp, Texas, USA).
A total of 25,821 neonates were included in the present study analysis after 1,324 neonates were excluded because of major congenital malformations. The demographic characteristics of the included infants without NEC and with non-surgical and surgically treated NEC are shown in Table 1. Patients were distributed in the different subperiods as follows: 8,103 patients (731 with NEC) in 2005–2008, 6250 patients (554 with NEC) in 2009–2011, 6312 neonates (532 with NEC) in 2012–2014, and 5156 neonates (440 with NEC) in 2015–2017. The mean gestational age in the cohort remained unchanged over the study period: 28.5 ± 2.1 (2005–2008), 28.5 ± 2.1 (2009–2011), 28.6 ± 2.1 (2012–2014), and 28.5 ± 2.1 (2015–2017) (p = 0.20).
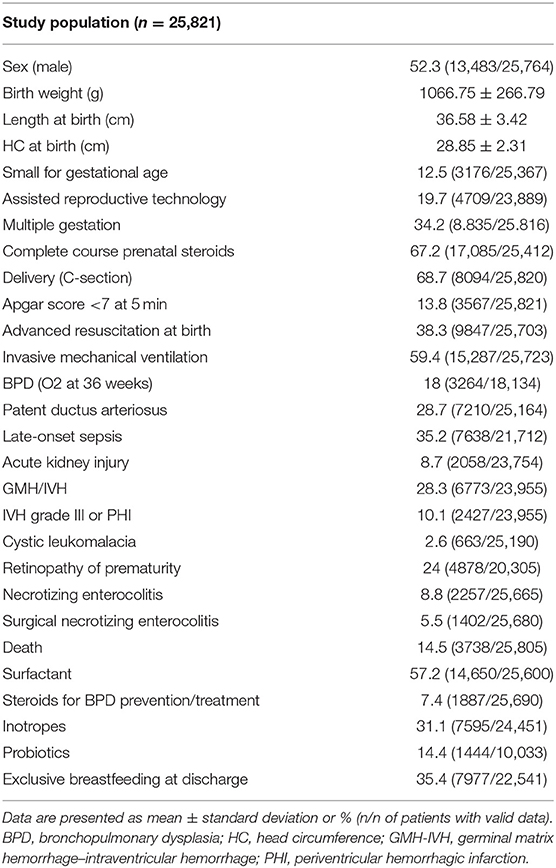
Table 1. Demographic characteristics of the study population.
The average NEC incidence in the cohort over the whole study period was 8.8%. The incidence of surgically treated NEC was 5.5%, which represents 62.3% of all NEC cases. NEC incidence trends over the study period by year are depicted in Figure 1. Overall, NEC incidence remained stable: 9.1% (2005–2008), 9% (2009–2011), 8.5% (2012–2014), and 8.6% (2015–2017) (p = 0.521). Medically treated NEC incidence trended down: 4.9% (2005–2008), 3.4% (2009–2011), 2.49% (2012–2014), and 2.71% (2015–2017) (p < 0.001). On the contrary, there was a significant rise in the proportion of surgically treated cases, increasing from 48.84% (2005–2008) to 64.1% (2009–2011), 72.4% (2012–2014), and 70.2% (2015–2017) (p < 0.001). The evolution of risk and protective factors for NEC trends over the study period are shown in Figure 2.
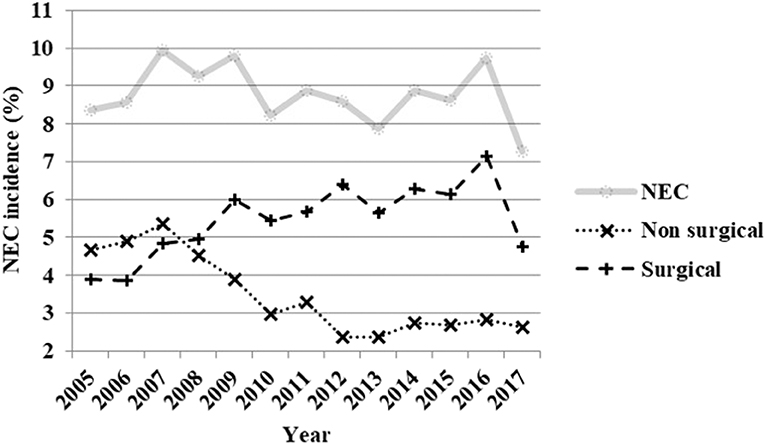
Figure 1. Evolution of necrotizing enterocolitis incidence—NEC (all cases), only medically treated and surgically treated cases—by year from 2005 to 2017.
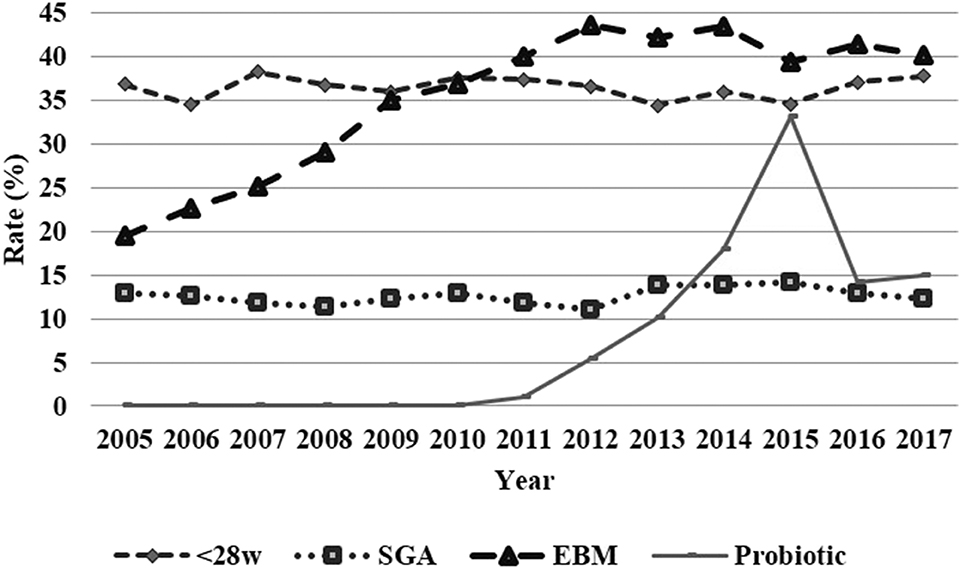
Figure 2. Evolution of risk and protective factors for necrotizing enterocolitis (inferior) by year from 2005 to 2017.
NEC mortality (Figure 3) decreased from 36.7% in the 2005–2008 period to 29.3% (2009–2011) and then to 26% (2012–2014) and 26.6% in the 2015–2017 period (p < 0.001). This significant decrease was seen in both subgroups, surgically, and non-surgically treated NEC patients. In the non-surgical subgroup, it changed from 31.7% (2005–2008) to 24.9% (2009–2011) and then to 19.1% (2012–2014) and 19.1% (2015–2017) (p = 0.004). In the surgically treated patients, mortality trended as follows: 41.9% (2005–2008) to 31.1% (2009–2011), 28.7% (2012–2014), and 29.8% (2015–2017) (p = 0.001). Also, in patients without NEC, mortality rate evolved over the study period, 14.6% (2005–2008), 13.8% (2009–2011), 10.9% (2012–2014), and 10.6% (2015–2017) (p < 0.001), whereas the mean age at death did not vary over these years: 17.5 ± 33.2 (2005–2008), 14.3 ± 23.9 (2009–2011), 17.5 ± 32.6 (2012–2014), and 16.7 ± 37.7 days (p = 0.09).
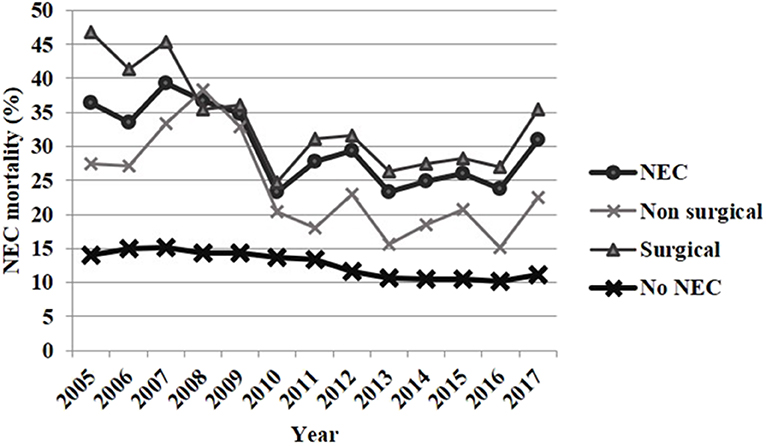
Figure 3. Evolution of necrotizing enterocolitis mortality by year from 2005 to 2017.
There was a statistically significant association between NEC, some common preterm's diseases (BPD, late-onset sepsis, cystic leukomalacia, retinopathy of prematurity, acute kidney injury), and death as shown in Table 2. The risk increased significantly when comparing preterm infants with no NEC with non-surgically treated NEC and finally with surgically treated NEC as seen in Figure 4. Table 3 provides data about the incidence evolution from 2005 to 2017 of these NEC-associated co-morbidities depending on NEC diagnosis and reported treatment. In patients who had surgically treated NEC and died, age at death was 36.1 ± 34.3 (2005–2008), 36.7 ± 36.4 (2009–2011), 37.8 ± 42.3 (2012–2014), and 36.1 ± 33.6 days (2015–2017) (p = 0.98). Mean age at death among non-surviving NEC patients without surgical treatment trended as follows: 23.3 ± 27.7 (2005–2008), 24.1 ± 26.3 (2009–2011), 23.5 ± 26.6 (2012–2014), and 15.6 ± 10.6 days (2015–2017) (p = 0.54).
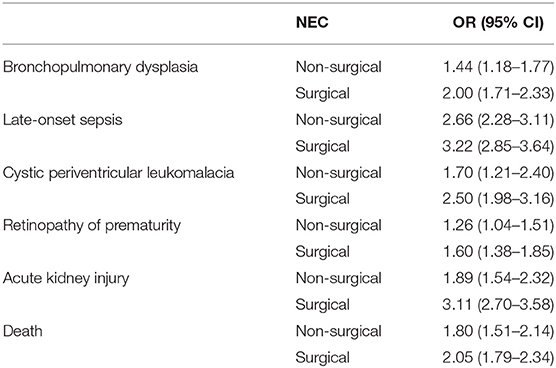
Table 2. Risk of morbi-mortality associated with medically and surgically treated necrotizing enterocolitis compared to preterm infants without necrotizing enterocolitis, adjusted by gestational age.
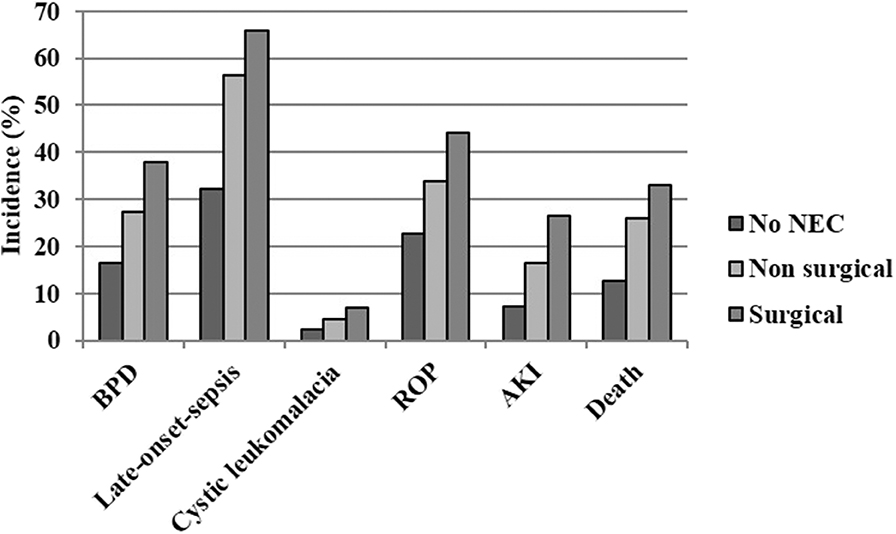
Figure 4. Co-morbidity and mortality associated with necrotizing enterocolitis classified depending on the treatment (only medical or surgical). AKI, acute kidney injury; BPD, bronchopulmonary dysplasia; ROP, retinopathy of prematurity.
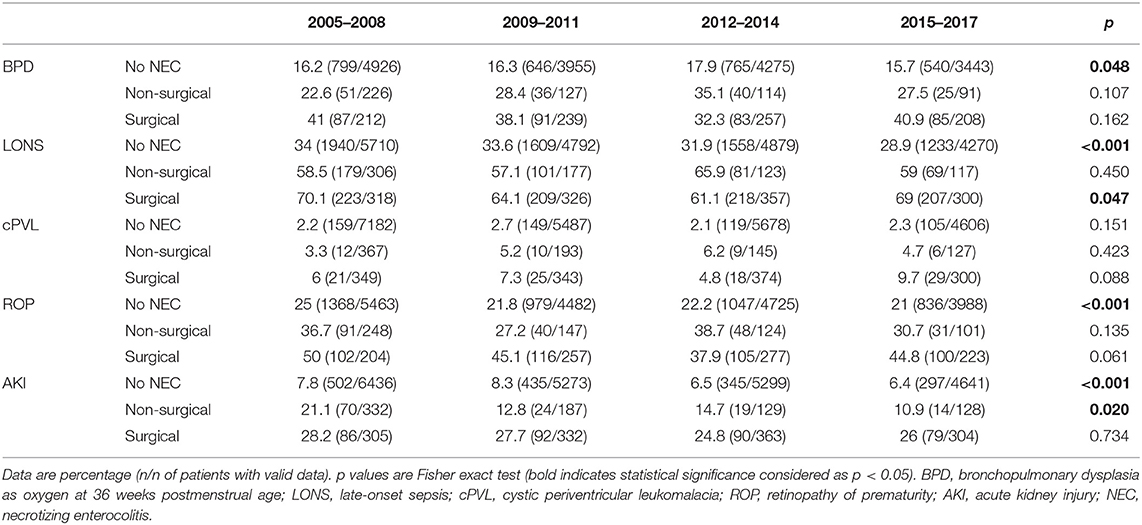
Table 3. Evolution of NEC associated co-morbidities of prematurity according to NEC diagnosis and treatment.
In our cohort, NEC incidence remained stable. According to the literature, an increased incidence has been reported in Sweden (1987–2009) and the Netherlands (2005–2013), whereas the incidence decreased in Australia (1986–1999) and Canada (2013–2017) and remained stable in Switzerland (2000–2012) and in the United States (1993–2012) (4, 11–15). The increased incidence in the Dutch and Swedish studies was attributed to the increased early survival rate and lower gestational age at birth over the study period. In our cohort, the mean gestational age at birth and age at death remained invariable over the study period, which could partly explain why the incidence did not increase. In the Swiss and American cohorts, the mean gestational age also remained unchanged. Of note, the incidence of NEC in our cohort remained mostly unchanged despite the higher rate of exclusive breast milk feeding at discharge and the implementation of probiotics during the study period. Overall, prophylactic probiotics have proved to be protective against NEC (16). However, this seems to be true only for some strains (17) and new studies should clarify which ones are more effective to reduce NEC. During the study period, probiotics were introduced but not universally. A recent survey among Spanish neonatal units showed that only in 23% are prophylactic probiotics used (18). Whether prophylactic probiotics failed in our cohort or the proportion of patients who received probiotics was insufficient remains to be clarified. Breast milk is a protective factor for NEC too. There is a dose response; the more human milk consumed, the less the risk (19). Donor milk is superior to formula but not to breast milk regarding NEC prevention (19). Donor milk, which is increasingly available in our units (87%) (18), has proved to facilitate exclusive breastfeeding at discharge (20). More data about the proportions of breast, donor, and formula milk received from birth to discharge per patient, which we lacked, would be useful to clarify why increasing rates of breastfeeding at discharge—the only nutrition data available in the database—were not associated with a decreased NEC incidence.
In our cohort, the proportion of cases who underwent surgical intervention increased over the studied years. In our opinion, this is more likely to be related to a change in surgical attitudes rather than to an increased rate of perforation among infants with NEC. The indication for surgical treatment varies depending on the surgeon. Only intestinal perforation seems to be accepted as an absolute indication for surgery (21). However, clinical deterioration in the absence of pneumoperitoneum is also a common indication for surgical treatment (22). Surgical cases have high mortality according to the literature (23). This highest mortality probably reflects the fact that the patients who underwent surgery were sicker. In our cohort, surgical cases had higher mortality than non-surgical cases too. However, mortality is also decreasing in the surgically treated NEC patients. Even more, the improvement in mortality is even greater than that seen in no surgical NEC cases and preterm infants without NEC. Decreased NEC mortality (all cases) over the years has also been reported by Ahle et al. in Sweden (4), whereas no changes in mortality over time were found by Heida et al. in the Netherlands (11) or Luig in Australia (12). Interestingly, Heida et al. reported a decreasing rate of surgical interventions (53 to 29%) from 2005 to 2013 in their Dutch cohort (11). They reported a significant decrease in peritoneal drainage insertion (28 to 12%) and a small increment in laparotomy indicated because of pneumoperitoneum (24 to 30%).
Finally, another finding of this study is that morbidity rates decreased over the study period in preterm infants without NEC, whereas this did not occur in infants with NEC diagnosis, which shows a niche for improvement. NEC leads to a systemic inflammatory state (24). Inflammation plays an essential role in the pathophysiology of several complications associated with prematurity like bronchopulmonary dysplasia, retinopathy of prematurity, and cystic periventricular leukomalacia. In fact, NEC is known to be associated with an increased risk of having these complications (25). Current NEC treatments do not focus on reducing this inflammatory state directly. Surgery aims to remove gangrenous bowel segments, with the objective of reducing bacterial translocation, sepsis, and multiorgan dysfunction (23). Some authors have suggested that early laparotomy could improve the outcomes, but the optimal indications and timing for surgery in patients with NEC beyond perforation remain to be clarified (26).
The main limitation of this study is the lack of data regarding the reason for surgical indication, surgical procedures, and timings in the original database. Data about bowel-related NEC complications (i.e., intestinal post-NEC necrosis, short bowel syndrome) are also not collected and therefore could not be studied. Finally, important nutritional data (i.e., proportions of the different feedings) were not available either. A recent survey published by our group describes the current practices regarding NEC in Spain. This survey showed great variation regarding surgical indications and preferred interventions (18). Among the surveyed surgeons, 19% reported that the indications for surgery have remained the same, and 41% said that surgical indications have become more conservative over the last 10 years. On the contrary, 37% considered that early interventions, even in the absence of perforation, were becoming more frequent. However, these surgeons usually worked in high volume centers. The multicenter nature, the prospective data collection, and the big sample size are strengths of the present study. This has allowed us to study the relationship between NEC and other common complications of the preterm infant, for which NEC seems to be a risk factor. This aspect has seldom been described using large cohorts datasets.
Necrotizing enterocolitis incidence remained unchanged over the study period; thus, implementation and search for new preventive strategies are still required. Interestingly, the proportion of NEC patients who underwent surgery trended up from 2005 to 2017. Mortality improved during the studied years in preterm infants with and without NEC diagnosis. However, it has improved more in patients with NEC than in preterm infants without NEC. On the other hand, the incidence of common co-morbidities of preterm birth, in general, improved in patients without NEC while it remained mostly invariable in patients with NEC. New treatments should focus on reducing the common preterm infant co-morbidities in patients with NEC, probably targeting the systemic inflammatory reaction associated with NEC.
The datasets generated for this study are available on request to the corresponding author.
Local Ethics Research Committee of all participant centres approved the data collection protocol when they joined the network. Permission for data analysis was obtained from the executive committee of the Spanish neonatal SEN1500 network. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
All authors contributed in the study design. CZ performed the statistical analysis and drafted the initial manuscript along with IG. AA-A, NO, TS, ES, MS, FG-MR, and MC contributed to interpreting the results and revised the manuscript making important intellectual contributions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We are indebted to all the investigators, coordinators, and members of the Spanish Neonatal Network SEN1500: Complejo Hospitalario Albacete (Andrés Martínez Gutiérrez), Hospital U. de Basurto (Alberto Pérez Legorburu), Hospital Bierzo (María Teresa Prada), Hospital Cabueñes (Rafael García Mozo), Hospital Carlos Haya (Tomás Sánchez Tamayo), Hospital General Castellón (Ramón Aguilera Olmos), Hospital Central Asturias (Belén Fernández Colomer), Hospital Clínic Barcelona (Josep Figueras Aloy), Hospital Clínico San Carlos (Araceli Corredera Sánchez), Hospital Cruces (Amaya Rodríguez Serna), Hospital U. Donostia (M. Ángel Cortajarena Altuna), Hospital Elche (Carolina Vizcaíno), Hospital General de Cataluña (Laura Castells Vilella), Hospital G. de Granollers (Israel Anquela Sanz), Hospital Germans Trias i Pujol (W. Coroleu), Hospital Getafe (Lucía Cabanillas Vilaplana), Hospital Jerez (Mª Victoria Ramos Ramos), Hospital Juan Ramón Jiménez (David Mora Navarro), Hospital Juan XXIII (Mar Albújar), Hospital León (Mª Teresa Palau Benavides), Hospital Miguel Servet (Segundo Rite Gracia), Corporació Parc Taulí (Juan Badia), Hospital San Juan de Deu (Martín Iriondo Sanz), Hospital San Pedro de Logroño (Mª Yolanda Ruiz del Prado), Hospital San Pedro de Alcántara (Mª Jesús López Cuesta), Hospital de la Santa Creu i Sant Pau (Gemma Ginovart Galiana), Hospital Severo Ochoa (María José Santos Muñoz), Hospital Txagorritxu (María Mercedes Martínez Ayucar), Hospital Universitario Arnau de Vilanova (Eduard Solé Mir), Hospital Valme de Sevilla (Josefina Márquez Fernández), Hospital Virgen de la Concha (Víctor Marugán Isabel), Hospital U. Virgen de la Macarena (Mercedes Granero Asensio), Hospital Virgen de la Salud (Ana Belén Escobar Izquierdo), Hospital U. Virgen de las Nieves (Mª Fernanda Moreno Galdó), Hospital Xeral Vigo (María Suárez Albo), Hospital Universitario de Valencia (Javier Estañ Capell), Hospital Universitario de Zaragoza (Purificación Ventura Faci), Hospital Universitario Santiago (Mª José Fernández-Seara), Hospital General de Burgos (Cristina de Frutos Martínez), Hospital General Universitario Alicante (Honorio Sánchez Zaplana), Hospital Universitario de Fuenlabrada (Laura Domingo Comeche), Hospital Universitario Gregorio Marañón (Dorotea Blanco Bravo), Hospital Universitario La Paz (Mª Dolores Elorza), Hospital Materno Infantil de Canarias (Lourdes Urquía Martí), Hospital Universitario Canarias (Pedro A. Fuster Jorge), Hospital Universitario de San Cecilio (Eduardo Narbona), Hospital Universitari i Politecnic La Fe (Isabel Izquierdo Macián), Hospital Universitario Reina Sofía (Mª Pilar Jaraba Caballero), Hospital Universitario Río Hortega (Mª Mar Montejo Vicente), Hospital Universitario Salamanca (Pilar García González), Hospital Universitario Virgen del Rocío (Carmen Macías Díaz), Hospital Universitario Dexeus (Roser Porta), Scias-Hospital Barcelona (Silvia Martínez-Nadal), Hospital Josep Trueta (Alberto Trujillo), Complejo Hospitalario Universitario de Pontevedra (Pilar A. Crespo Suárez), Hospital Universitario de Ciudad Real (Miguel Ángel Cabezas), Hospital Puerta del Mar (Antonio Segado Arenas), Hospital Universitario Marqués de Valdecilla (Isabel de las Cuevas), Hospital Quirón Málaga (Manuel Baca Cots), Hospital de la Zarzuela (M López Gómez), H. Nuestra Señora de la Candelaria (Sabina Romero), H. Madrid Torrelodones (Isabel Llana Martín), H. Puerta de Hierro (C. González Armengod), H. U. Santa Lucía de Cartagena (J.M. Lloreda García), H. Virgen del Camino de Pamplona (Concepción Goñi Orayen), H. U. Quirón Madrid (M López Azorín), Clínica Cocharán (M.D. Muro Sebastián), Complexo H. U. de A Coruña (Alejandro Ávila Álvarez), H. Quirón Sagrado Corazón de Sevilla (Elena García Victori), and H.U. Fundación Jiménez Díaz (T. Carrizosa).
1. Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med. (2011) 364:255–64. doi: 10.1056/NEJMra1005408
2. Samuels N, van de Graaf RA, de Jonge RCJ, Reiss IKM, Vermeulen MJ. Risk factors for necrotizing enterocolitis in neonates: a systematic review of prognostic studies. BMC Pediatr. (2017) 17:1–9. doi: 10.1186/s12887-017-0847-3
3. Isayama T, Lee SK, Mori R, Kusuda S, Fujimura M, Ye XY, et al. Comparison of mortality and morbidity of very low birth weight infants between canada and japan. Pediatrics. (2012) 130:e957–e65. doi: 10.1542/peds.2012-0336
4. Ahle M, Drott P, Andersson RE. Epidemiology and trends of necrotizing enterocolitis in sweden: 1987-2009. Pediatrics. (2013) 132:e443–e51. doi: 10.1542/peds.2012-3847
5. Patel RM, Kandefer S, Walsh MC, Bell EF, Carlo WA, Laptook AR, et al. Causes and timing of death in extremely premature infants from 2000 through 2011. N Engl J Med. (2015) 372:331–40. doi: 10.1056/NEJMoa1403489
6. Shulhan J, Dicken B, Hartling L, Larsen BM. Current knowledge of necrotizing enterocolitis in preterm infants and the impact of different types of enteral nutrition products. Adv Nutr An Int Rev J. (2017) 8:80–91. doi: 10.3945/an.116.013193
7. Moro Serrano M, Fernández Pérez C, Figueras Alloy J, Pérez Rodríguez J, Coll E, Doménech Martínez E, et al. [SEN1500: design and implementation of a registry of infants weighing less than 1,500 g at birth in spain]. An Pediatr (Barc). (2008) 68:181–8. doi: 10.1157/13116235
8. Boghossian NS, Geraci M, Edwards EM, Horbar JD. Morbidity and mortality in small for gestational age infants at 22 to 29 weeks' gestation. Pediatrics. (2018) 141:2533. doi: 10.1542/peds.2017-2533
9. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. (2001) 163:1723–729. doi: 10.1164/ajrccm.163.7.2011060
10. Fenton TR, Kim JH. A systematic review and meta-analysis to revise the fenton growth chart for preterm infants. BMC Pediatr. (2013) 10:59. doi: 10.1186/1471-2431-13-59
11. Heida FH, Stolwijk L, Loos M-LHJ, van den Ende SJ, Onland W, van den Dungen FAM, et al. Increased incidence of necrotizing enterocolitis in the netherlands after implementation of the new dutch guideline for active treatment in extremely preterm infants: results from three academic referral centers. J Pediatr Surg. (2017) 52:273–6. doi: 10.1016/j.jpedsurg.2016.11.024
12. Luig M, Lui K. Epidemiology of necrotizing enterocolitis–Part i: changing regional trends in extremely preterm infants over 14 years. J Paediatr Child Health. (2005) 41:169–73. doi: 10.1111/j.1440-1754.2005.00582.x
13. Shah PS, Dunn M, Aziz K, Shah V, Deshpandey A, Mukerji A, et al. Sustained quality improvement in outcomes of preterm neonates with a gestational age less than 29 weeks: results from the evidence-based practice for improving quality phase 3. Can J Physiol Pharmacol. (2019) 97:213–21. doi: 10.1139/cjpp-2018-0439
14. Chen F, Bajwa NM, Rimensberger PC, Posfay-Barbe KM, Pfister RE, Swiss Neonatal Network. Thirteen-year mortality and morbidity in preterm infants in Switzerland. Arch Dis Child - Fetal Neonatal Ed. (2016) 101:F377–83. doi: 10.1136/archdischild-2015-308579
15. Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993-2012. JAMA. (2015) 314:1039. doi: 10.1001/jama.2015.10244
16. Thomas JP, Raine T, Reddy S, Belteki G. Probiotics for the prevention of necrotising enterocolitis in very low-birth-weight infants: a meta-analysis and systematic review. Acta Paediatr. (2017) 106:1729–741. doi: 10.1111/apa.13902
17. van den Akker CHP, van Goudoever JB, Szajewska H, Embleton ND, Hojsak I, Reid D, et al. Probiotics for preterm infants. J Pediatr Gastroenterol Nutr. (2018) 67:103–22. doi: 10.1097/MPG.0000000000001897
18. Zozaya C, Avila-Alvarez A, Somoza Argibay I, García-Muñoz Rodrigo F, Oikonomopoulou N, Encinas JL, et al. [Prevention, diagnosis and treatment of necrotising enterocolitis in newborns less than 32 weeks at birth in spain]. An Pediatría. (2020) doi: 10.1016/j.anpedi.2019.12.023. [Epub ahead of print].
19. Cacho NT, Parker LA, Neu J. Necrotizing enterocolitis and human milk feeding. Clin Perinatol. (2017) 44:49–67. doi: 10.1016/j.clp.2016.11.009
20. Kantorowska A, Wei JC, Cohen RS, Lawrence RA, Gould JB, Lee HC. Impact of donor milk availability on breast milk use and necrotizing enterocolitis rates. Pediatrics. (2016) 137:e20153123. doi: 10.1542/peds.2015-3123
21. Thakkar HS, Lakhoo K. The surgical management of necrotising enterocolitis (NEC). Early Hum Dev. (2016) 97:25–8. doi: 10.1016/j.earlhumdev.2016.03.002
22. Karam O, Valpacos M, Wilde JCH, Arni D, Pfister RE, Aspirot A, et al. Diagnosis and management of necrotizing enterocolitis: an international survey of neonatologists and pediatric surgeons. Neonatology. (2017) 113:170–6. doi: 10.1159/000484197
23. Carr BD, Gadepalli SK. Does surgical management alter outcome in necrotizing enterocolitis? Clin Perinatol. (2019) 46:89–100. doi: 10.1016/j.clp.2018.09.008
24. Benkoe T, Baumann S, Weninger M, Pones M, Reck C, Rebhandl W, et al. Comprehensive evaluation of 11 cytokines in premature infants with surgical necrotizing enterocolitis. PLoS ONE. (2013) 8:2–7. doi: 10.1371/journal.pone.0058720
25. Shah J, Singhal N, Da Silva O, Rouvinez-Bouali N, Seshia M, Lee SK, et al. Intestinal perforation in very preterm neonates: risk factors and outcomes. J Perinatol. (2015) 35:595–600. doi: 10.1038/jp.2015.41
Keywords: necrotizing enterocolitis, preterm infant, mortality, morbidity, trends
Citation: Zozaya C, García González I, Avila-Alvarez A, Oikonomopoulou N, Sánchez Tamayo T, Salguero E, Saenz de Pipaón M, García-Muñoz Rodrigo F and Couce ML (2020) Incidence, Treatment, and Outcome Trends of Necrotizing Enterocolitis in Preterm Infants: A Multicenter Cohort Study. Front. Pediatr. 8:188. doi: 10.3389/fped.2020.00188
Received: 30 December 2019; Accepted: 30 March 2020;
Published: 13 May 2020.
Edited by:
Bernhard Resch, Medical University of Graz, AustriaReviewed by:
Gangaram Akangire, Children's Mercy Hospital, United StatesCopyright © 2020 Zozaya, García González, Avila-Alvarez, Oikonomopoulou, Sánchez Tamayo, Salguero, Saenz de Pipaón, García-Muñoz Rodrigo and Couce. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Zozaya, Y2FybG9zLnpvemF5YUBzaWNra2lkcy5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.