 Jitendra Meena
Jitendra Meena Georgie Mathew
Georgie Mathew Pankaj Hari
Pankaj Hari Aditi Sinha
Aditi Sinha Arvind Bagga
Arvind Bagga
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr. , 31 March 2020
Sec. Pediatric Nephrology
Volume 8 - 2020 | https://doi.org/10.3389/fped.2020.00084
This article is part of the Research Topic Highlights in Pediatric Nephrology: 2021 View all 15 articles
Introduction: Urinary tract infection (UTI) in children leads to renal scarring in 10–15% of patients. Urinary tract anomalies and bladder and bowel dysfunction (BBD) are documented risk factors for recurrent UTIs. Estimates of baseline prevalence of BBD in children with UTI will help the clinician in the management strategy. Hence, a systematic review and meta-analysis was conducted to estimate the pooled prevalence of BBD.
Methods: MEDLINE, EMBASE, and CENTRAL (Cochrane Central Register of Controlled Trials) databases were searched for articles related to UTI, primary vesicoureteral reflux (VUR), and BBD. We included studies that provided prevalence of BBD in toilet-trained patients aged 1–18 years with UTI and/or VUR. BBD was defined based on clinical history or questionnaire or urodynamic studies. Two authors independently reviewed, assessed, and abstracted data from studies. Pooled prevalence was calculated based on a random effects model.
Results: Forty-three studies fulfilling the eligibility criteria were selected from a total of 1,731 studies. Among patients presenting with UTI without primary VUR, pooled prevalence of BBD was 41% (95% CI: 26–55; nine studies, 920 patients, I2 = 96.0%), whereas its prevalence in patients with primary VUR was 49% (43–56; 30 studies, 5,060 patients, I2 = 96.0%). Weighting by the study design and quality did not affect the prevalence. In patients with primary VUR, prevalence of BBD was higher in females (53%; 42–65) than in males (44%; 15–73). In studies where urodynamic study was used for the diagnosis of BBD, prevalence was 63%. The presence of BBD in patients with primary VUR increased risk of recurrent UTIs [relative risk (RR): 2.1; 1.7–2.5]. In five studies that reported separate data on constipation, pooled prevalence of constipation was 27% (16–37).
Conclusion: Almost half of the patients with primary VUR have BBD, and its presence increases the risk of recurrent UTIs. Trends of high BBD prevalence were also observed in patients presenting with UTI without VUR. These prevalence estimates suggest that all toilet-trained children presenting with UTI with or without VUR should be assessed for BBD, which will help in their further management.
Urinary tract infections (UTIs) are one of the most commonly encountered infections in childhood and may lead to long-term sequelae in a proportion of patients (1, 2). Whereas, presence of urinary tract anomalies is a known risk factor for recurrent UTIs in children, risk of recurrence is also influenced by age, gender, and bladder and bowel dysfunction (BBD) (3, 4). The term BBD is used to describe the spectrum of lower urinary tract symptoms accompanying bowel disturbance in the form of constipation and/or encopresis (4). BBD has also been reported as one of the important risk factors for recurrent UTIs in children. The risk of UTI is higher in patients with BBD and primary vesicoureteral reflux (VUR) than in patients with only VUR (5). Presence of BBD delays resolution of VUR and increases risk of UTI following reimplantation (6, 7). BBD has also been reported to impact the rate of breakthrough UTIs in patients with VUR who are on continuous antibiotic prophylaxis (5). As the presence of BBD in patients with UTI affects long-term outcomes, early recognition, and treatment are essential (6). In patients with UTI, variable prevalence (18–54%) of BBD has been reported in previous studies. Knowledge about the baseline prevalence of BBD in toilet-trained children presenting with UTI with or without primary VUR will help clinician in planning the management strategy for these patients (8). We performed a systematic review and meta-analysis to provide pooled estimates of prevalence of BBD in patients presenting with UTI and/or primary VUR.
The aim of this study was to determine the prevalence of BBD in toilet-trained children with UTI with or without primary VUR.
What is the prevalence of BBD in toilet-trained children with UTI with or without primary VUR?
A systematic review and meta-analysis was performed by review of observational and interventional trials published between January 1980 and December 2018.
All published data during 1980–2018 were searched for prevalence of BBD in toilet-trained children with UTIs with or without primary VUR. No interventions or comparators were assessed.
Protocol for the study was published (PROSPERO: CRD42019127086) and conducted in accordance with the Meta-analysis Of Observational Studies in Epidemiology guidelines (9). Two authors (JM and GM) independently performed literature search in MEDLINE, EMBASE, and CENTRAL (Cochrane Central Register of Controlled Trials) for original articles published, between January 1980 and December 2018. Search strategy design included patients aged 1–18 years with UTI and/or primary VUR. Search strategy was based on four basic groups of terminology: study population (pediatric/children/adolescent) and terms related to or describing the BBD, UTI, and VUR. Terminologies used for literature search were as follows: Bladder bowel dysfunction, dysfunctional elimination syndrome, dysfunctional voiding, lower urinary tract dysfunction, enuresis, urinary incontinence, urgency, overactive bladder, constipation, encopresis, fecal incontinence, vesicoureteral reflux, urinary tract infection, pyelonephritis, cystitis, pediatric, children, adolescent, prevalence, and incidence. Specific search strategies were created for each search engine by using MeSH term and terms described above (Supplementary Table 1). Electronic search was also supplemented by hand search of bibliographies of the included studies and relevant review articles.
Predefined criteria were used for final selection of studies included in the review. All observational studies and controlled trials were included in this review if they (i) reported data on BBD prevalence in patients aged 1–18 years with UTI and/or primary VUR and (ii) defined BBD based on clinical history or questionnaire or urodynamic studies (UDSs). Conference abstracts were also included if they provided sufficient information on sample size, methods of data collection, case definition, and prevalence of BBD. Studies were excluded if they reported (i) BBD prevalence in 10 or less patients; (ii) patients with neurological abnormalities that affect normal functioning of bladder and bowel, or secondary VUR; (iii) non-toilet-trained children; and (iv) in languages other than English. A well-structured, standardized proforma was used for data extraction. Data included information for risk of bias assessment of the study, prevalence of BBD, author name, year of publication, journal, study setting and design, study population, baseline demographic characteristics, details of intervention, and control group (in case of randomized controlled trials), case definition of BBD, and recurrence of UTI. Any disagreement between two reviewers was resolved through discussion with the third author (PH).
The authors independently assessed the quality of articles using the Cochrane risk bias tool for randomized controlled trials. Quality of observation studies was assessed by using a risk of bias assessment tool developed by Hoy et al. for prevalence studies (10). We reviewed full-text articles to determine the following: (i) whether study participants are a close representation of true population; (ii) whether the method used for selection of the study participants was appropriate; (iii) whether data were directly collected from patients and their response rate; (iv) whether acceptable case definition and tool were used for defining BBD and UTI; and (v) whether appropriate numerator and denominator were used for calculating prevalence of BBD. Disagreement between two authors in assessment of risk of bias was resolved by the third author (PH).
Meta-analysis was performed using Stata version 14. We pooled data from individual studies using random effects model with assumption that BBD prevalence would be variable across the studies. Forest plots represent studies in order of year of publication. Heterogeneity in studies was explored by inspection of forest plot as well as using chi-square test on Cochran's Q statistics. Study heterogeneity was assessed by using the Higgins and Thompson I2 method (11). The I2 heterogeneity was categorized as follows: 0–50% low, 50–75% moderate, and >75% considerable heterogeneity. Sensitivity analyses were undertaken to investigate the individual study influence and the studies using only low risk of bias. A subgroup analysis was performed to explain heterogeneity and calculate prevalence of BBD by sex, study design (controlled trials and prospective and retrospective observation studies), and method of assessment.
A total of 1,731 articles were identified through the search strategy in all databases (PubMed 667, EMBASE 525, and CENTRAL 539). There were 1,319 articles after removing 412 duplicates, and 105 of these articles were assessed as potentially relevant, for the systematic review, by screening through the title and abstract. Among these, 80 were full-text original articles, whereas the rest 25 were conference abstracts (Figure 1). We also screened the reference list of the full-text articles, but no additional article was identified through this process. Finally, 43 studies comprising 6,627 patients were selected for this review (Table 1).
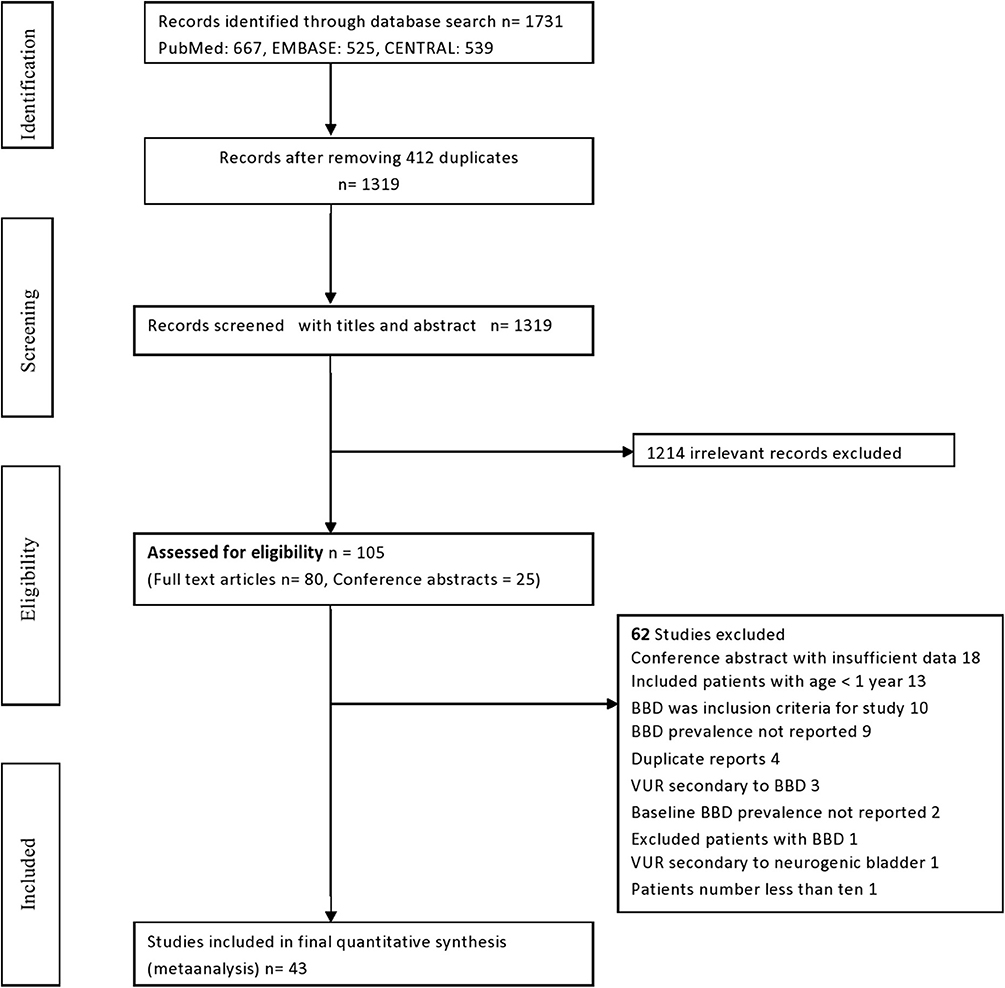
Figure 1. Systematic review flow diagram for selection of studies.
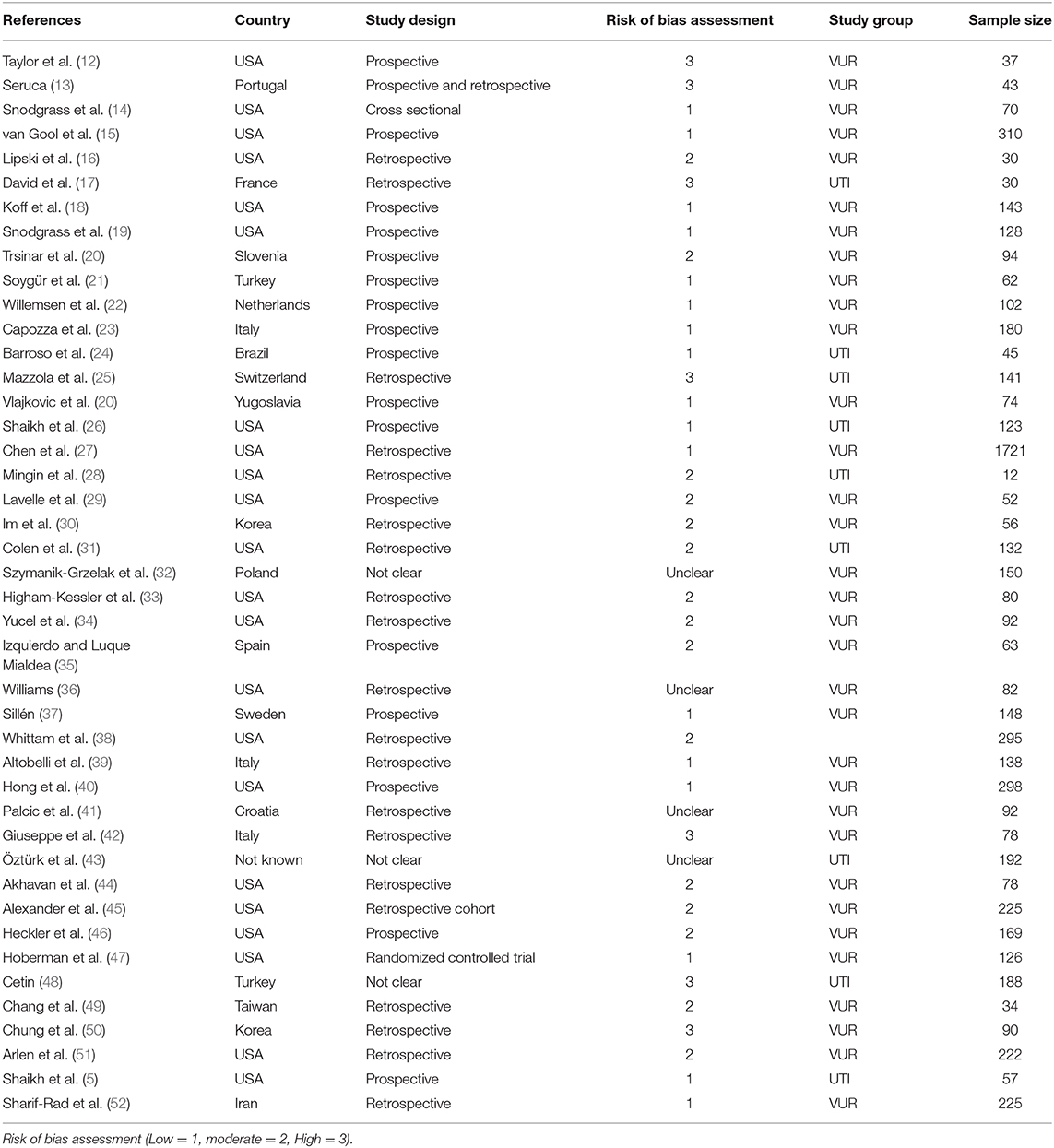
Table 1. Basic characteristics of studies included in the systematic review.
On the basis of patients enrolled, we categorized studies into two groups: (i) nine studies of patients with UTI and without primary VUR (5, 17, 24–26, 28, 31, 43, 53) and (ii) 30 studies of patients with primary VUR (12–16, 18–23, 27, 29, 30, 32–35, 37–42, 44–47, 49–52, 54). Three studies were included in the final systematic review as they reported data on rates of recurrence of UTI (15, 22, 45), and one study by Chung et al. provided data on constipation (50).
A total of nine studies comprising of 920 patients reported prevalence of BBD in toilet-trained children presenting with UTI without VUR (5, 17, 24–26, 28, 31, 43, 53). The pooled prevalence of BBD in patients with UTI was 41% (95% CI: 26–55%) (Figure 2). Owing to high heterogeneity (I2 = 95.99%), random effects estimates were used. Three studies reported separate data on prevalence of BBD in girls, at 41% (95% CI: 25–58%). None of the studies provided separate information on prevalence of BBD in boys. On a subgroup analysis, the prevalence of BBD was higher (51%, 10–93%) in prospective studies as compared with retrospective studies (35%, 21–49%).

Figure 2. Prevalence of bladder dysfunction in children with urinary tract infection (UTI) without primary vesicoureteral reflux (VUR).
Thirty studies comprising 5,060 patients reported prevalence of BBD in patients with primary VUR (14–16, 18–23, 27, 29, 30, 32–35, 37–42, 44–47, 49–52, 54–58). The pooled prevalence of BBD was 49% (95% CI: 43–56%) (Figure 3). In this group of studies, the heterogeneity was also high (I2 = 96%). Separate data for prevalence of BBD for boys were reported in five studies, with pooled prevalence of 44% (95% CI: 15–73%). Seven studies reported data for girls with BBD prevalence of 53% (95% CI: 42–65%). In studies with high risk of bias, the prevalence of BBD was high (71%), as compared with that in studies with low-to-moderate risk of bias (45% and 48%). No difference in BBD prevalence was observed when comparing prospective with retrospective studies. In eight studies that used UDS, the pooled prevalence of BBD was 63% (95% CI: 56–70%; I2 = 52.8%).
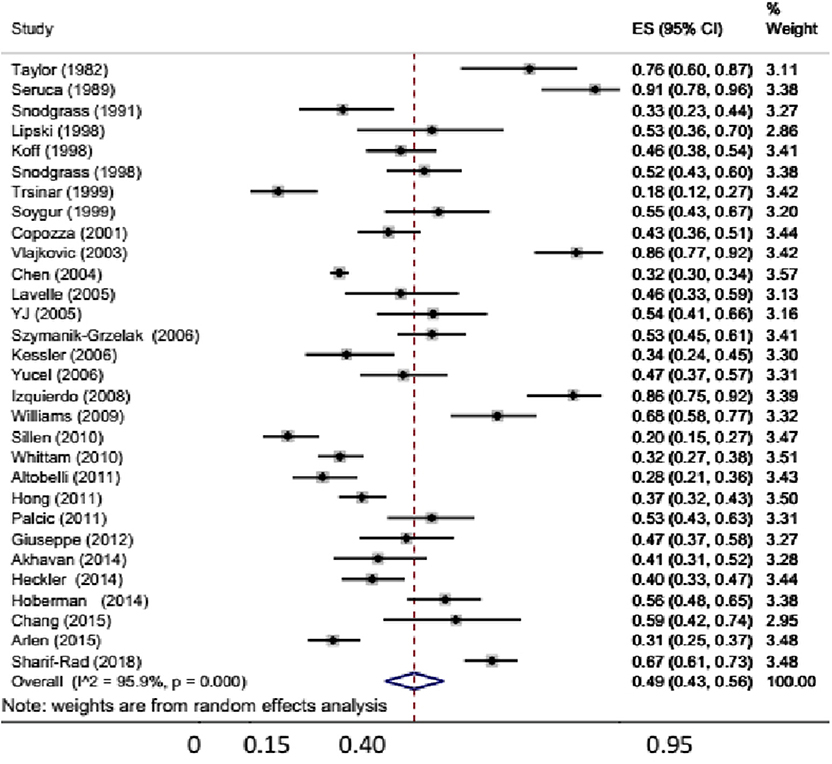
Figure 3. Prevalence of bladder dysfunction in children with primary vesicoureteral reflux (VUR).
Seven studies of patients with primary VUR explored the relationship between recurrence of UTI and BBD (15, 18, 19, 22, 37, 45, 47). A meta-analysis of these studies using random effects estimate showed that in the presence of BBD, the risk of recurrent UTIs was increased two-fold, as compared with that in patients without BBD (RR: 2.01; 95% CI: 1.47–2.74, I2 = 57.3%) (Figure 4). One study in patients with UTI without primary VUR reported that the presence of BBD did not significantly increase the risk of UTI (RR: 1.07, 95% CI: 0.51–2.23).

Figure 4. Risk of recurrence of urinary tract infection (UTI) in patients with vesicoureteral reflux (VUR) and bladder and bowel dysfunction (BBD) compared with patients without BBD.
Two studies on patients with UTI showed that the pooled prevalence of constipation was 30% (95% CI: 25–36%) (24). Data for constipation were reported in 972 patients with primary VUR across seven studies (18, 21, 40, 47, 49, 50, 52). Pooled prevalence of constipation from these seven studies was 27% (95% CI: 16–37%).
Quality of studies was assessed based on Cochrane risk bias tool for randomized trials, and a modified tool by Hoy et al. was used for observational studies (10). Based on these tools, seven studies were at high risk of bias, 17 at moderate risk of bias, and 15 at low risk of bias, whereas in four studies, risk of bias could not be assessed owing to insufficient information (Table 1).
Patients with bladder dysfunction are at increased risk of bowel dysfunction and vice versa. Anatomical and function interaction that leads to this increase risk has been well-established. BBD is an important risk factor for UTI in children, more so in the ones who are toilet trained. In a meta-analysis, the American Urological Association (AUA) guideline for the management of primary VUR showed that the presence of BBD significantly delayed resolution of VUR (7). In children presenting with UTI, who already possess a risk factor like primary VUR, the presence of BBD further increases risk of breakthrough UTI even while on antibiotic prophylaxis (5). Two recent studies support the notion that BBD predisposes patients for recurrence of UTI and increases risk of renal scarring as well (3, 5). Recently, a reanalysis of data from the RIVUR trial by Wang et al. showed that antibiotic prophylaxis is more beneficial in the group of patients with BBD compared with those without it (8). Hence, it is of paramount importance to assess children presenting with UTI for BBD even in the presence of other anatomical risk factors before deciding management strategy. In this review, we found that prevalence of BBD is slightly higher in patients with primary VUR than in patients with UTI without VUR. Within primary VUR, cohort girls had higher prevalence of BBD than boys. When BBD is assessed by more invasive tools like UDS, almost two-thirds of patients with primary VUR were detected to have BBD. In the present meta-analysis, we also found that the presence of BBD increases risk of recurrence of UTI by almost two times in patients with primary VUR. Functional constipation was documented in almost one-third of the patients with either VUR or UTI. Prevalence of BBD in patients with UTI without VUR is clearly higher, in the present meta-analysis, than in the general population of school-going children (20%) (55). This higher prevalence of BBD in children with UTI than the general population might point toward a strong association between BBD and UTI.
We found higher prevalence of BBD in patients with primary VUR than did a meta-analysis in the 2010 guideline for management of VUR by the AUA. In the meta-analysis by AUA, pooled prevalence of BBD in 15 studies was 31%. We used a predefined strategy for selection of the studies, which resulted in inclusion of different studies compared with those included in the meta-analysis by AUA. We also found that BBD is more common in girls with VUR, which could explain higher risk of breakthrough UTI in girls. Gaither et al. also reported higher risk of BBD in girls (56). Prevalence of BBD in patients with primary VUR, in the present meta-analysis, has varied from 18 to 91% (14–16, 18–23, 27, 29, 30, 32–35, 37–42, 44–47, 49–52, 54–58). This large variation in prevalence is likely due to multiple factors, which include characteristics of study population, study design, intervention, and assessment tool used for BBD. The largest randomized trial (RIVUR) in patients with primary VUR reported almost similar prevalence of BBD (56%) as in the present meta-analysis.
The relationship between VUR, BBD, and recurrent UTIs is complex and not so well-understood. A previous report from Shaikh et al. showed that patients with both VUR and BBD have the highest rate of recurrent UTIs than have patients with only VUR or BBD (5). This meta-analysis underscores the same fact and showed almost two-fold higher risk of recurrent UTIs in patients with coexisting VUR and BBD than in patients with VUR alone. Reanalysis of RIVUR trial showed that a subgroup of patients with both VUR and BBD had the most benefit from antibiotic prophylaxis. Significant reduction in recurrent UTIs following successful management of BBD with urotherapy has been reported, which again suggests a strong role of BBD in recurrence of UTI (57, 58). Hence, evaluation for BBD is essential while planning management for patients with primary VUR.
Prevalence of functional constipation was reported to be 9.5% in healthy children in a recent systematic review (59). In our review, prevalence of constipation was almost three times higher in children with or without VUR, suggesting that BBD is an important risk factor for UTI in toilet-trained children. A systematic review reported that 37–64% patients with functional constipation have lower urinary tract symptoms, hinting toward the association of BBD.
There are few limitations of our systematic review. Large heterogeneity for final pooled prevalence could be considered a limitation; however, because there is no existing standardized diagnostic criterion to define BBD in children, we had to use all previous studies that provided data for BBD prevalence using various definitions. Second, the large heterogeneity could be because studies with all kinds of study design have been used in the present review, although in the sensitivity analysis, we could not find any major difference in various subgroups. Third, we had to exclude many studies that included infants, as these children aged <1 year are likely to be non-toilet trained and because diagnosing BBD in them is difficult. This exclusion criterion was defined a priori. Finally, we had limited our search to English-language databases only; hence, it might have resulted in exclusion of few studies published in non-English languages.
This systematic review has several strengths. First, we followed a rigorous methodology that included a comprehensive search of three major databases of medical literature, predefined protocol for study selection process, data extraction, and a statistical analysis that was registered in PROSPERO. We provided estimated pooled prevalence of BBD separately, in children with UTI only without VUR and other cohort of patients with primary VUR. We also showed that in patients with VUR, prevalence of BBD is higher in girls, which could explain higher number of recurrent UTIs in girls. Finally, we also assessed relative risk of recurrence of UTI in patients with both VUR and BBD and with VUR alone.
In summary, this systematic review of currently available literature shows that BBD is common in toilet-trained children presenting with UTI with or without primary VUR. A subgroup meta-analysis also shows that functional constipation is common in these children, with almost every third child affected with it. We also found that the presence of both BBD and VUR doubles the risk of recurrence of UTI; hence, all children presenting with UTI should be carefully evaluated for presence of BBD and managed accordingly. As BBD is an important risk factor for UTI recurrence, in future, intervention trials for patients with primary VUR should be stratified as per presence of BBD.
All datasets generated for this study are included in the article/Supplementary Materials.
JM conceived of the presented idea, formulated the protocol, and wrote the manuscript. JM and GM did independent data collection and analysis. PH decided on conflicting data interpretation. AS, AB, and PH provided critical feedback. All authors discussed the result and helped shape the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.00084/full#supplementary-material
1. Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. (2008) 27:302–8. doi: 10.1097/INF.0b013e31815e4122
2. Shaikh N, Craig JC, Rovers MM, Da Dalt L, Gardikis S, Hoberman A, et al. Identification of children and adolescents at risk for renal scarring after a first urinary tract infection: a meta- analysis with individual patient data. JAMA Pediatr. (2014) 168:893–900. doi: 10.1001/jamapediatrics.2014.637
3. Keren R, Shaikh N, Pohl H, Gravens-Mueller L, Ivanova A, Zaoutis L, et al. Risk factors for recurrent urinary tract infection and renal scarring. Pediatrics. (2015) 136:e13–21. doi: 10.1542/peds.2015-0409
4. Conway PH, Cnaan A, Zaoutis T, Henry BV, Grundmeier RW, Keren R. Recurrent urinary tract infections in children: risk factors and association with prophylactic antimicrobials. JAMA. (2007) 298:179–86. doi: 10.1001/jama.298.2.179
5. Shaikh N, Hoberman A, Keren R, Gotman N, Docimo S, Mathews R, et al. Recurrent urinary tract infections in children with bladder and bowel dysfunction. Pediatrics. (2016) 137:e20152982. doi: 10.1542/peds.2015-2982
6. Yang S, Chua ME, Bauer S, Wright A, Brandström P, Hoebeke P, et al. Diagnosis and management of bladder bowel dysfunction in children with urinary tract infections: a position statement from the International Children's Continence Society. Pediatr Nephrol. (2018) 33:2207–19. doi: 10.1007/s00467-017-3799-9
7. Peters CA, Skoog SJ, Arant BS, Copp HL, Elder JS, Hudson RG, et al. Summary of the AUA guideline on management of primary vesicoureteral reflux in children. J Urol. (2010) 184:1134–44. doi: 10.1016/j.juro.2010.05.065
8. Wang ZT, Wehbi E, Alam Y, Khoury A. A reanalysis of the RIVUR trial using a risk classification system. J Urol. (2018) 199:1608–14. doi: 10.1016/j.juro.2017.11.080
9. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
10. Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. (2012) 65:934–9. doi: 10.1016/j.jclinepi.2011.11.014
11. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
12. Taylor CM, Corkery JJ, White RH. Micturition symptoms and unstable bladder activity in girls with primary vesicoureteric reflux. Br J Urol. (1982) 54:494–8. doi: 10.1111/j.1464-410X.1982.tb13573.x
13. Seruca H. Vesicoureteral reflux and voiding dysfunction: a prospective study. J Urol. (1989) 142 (2 Pt 2):494–8; discussion 501. doi: 10.1016/S0022-5347(17)38794-3
14. Snodgrass W. Relationship of voiding dysfunction to urinary tract infection and vesicoureteral reflux in children. Urology. (1991) 38:341–4. doi: 10.1016/0090-4295(91)80148-Z
15. van Gool JD, Hjälmås K, Tamminen-Möbius T, Olbing H. Historical clues to the complex of dysfunctional voiding, urinary tract infection and vesicoureteral reflux. The International Reflux Study in Children. J Urol. (1992) 148(5 Pt 2):1699–702. doi: 10.1016/S0022-5347(17)37006-4
16. Lipski BA, Mitchell ME, Burns MW. Voiding dysfunction after bilateral extravesical ureteral reimplantation. J Urol. (1998) 159:1019–21. doi: 10.1016/S0022-5347(01)63826-6
17. David C, Dacher JN, Monroc M, Eurin D, Le Dosseur P. [Retrograde cystography after a first episode of acute pyelonephritis in the child and adolescent]. J Radiol. (1998) 79:133–7.
18. Koff SA, Wagner TT, Jayanthi VR. The relationship among dysfunctional elimination syndromes, primary vesicoureteral reflux and urinary tract infections in children. J Urol. (1998) 160(3 Pt 2):1019–22. doi: 10.1016/S0022-5347(01)62686-7
19. Snodgrass W. The impact of treated dysfunctional voiding on the nonsurgical management of vesicoureteral reflux. J Urol. (1998) 160:1823–5. doi: 10.1016/S0022-5347(01)62425-X
20. Trsinar B, Cotic D, Oblak C. Possible causes of unsuccessful endoscopic collagen treatment of vesicoureteric reflux in children. Eur Urol. (1999) 36:635–9. doi: 10.1159/000020059
21. Soygür T, Arikan N, Yeşilli C, Gögüş O. Relationship among pediatric voiding dysfunction and vesicoureteral reflux and renal scars. Urology. (1999) 54:905–8. doi: 10.1016/S0090-4295(99)00291-5
22. Willemsen J, Nijman RJ. Vesicoureteral reflux and videourodynamic studies: results of a prospective study. Urology. (2000) 55:939–43. doi: 10.1016/S0090-4295(00)00549-5
23. Capozza N, Patricolo M, Lais A, Matarazzo E, Caione P. Endoscopic treatment of vesico-ureteral reflux: twelve years' experience. Urol Int. (2001) 67:228–31. doi: 10.1159/000050993
24. Barroso U Jr, Barroso DV, Jacobino M, Vinhaes AJ, Macedo A Jr, Srougi M. Etiology of urinary tract infection in scholar children. Int Braz J Urol. (2003) 29:450–4. doi: 10.1590/S1677-55382003000500012
25. Mazzola BL, von Vigier RO, Marchand S, Tönz M, Bianchetti MG. Behavioral and functional abnormalities linked with recurrent urinary tract infections in girls. J Nephrol. (2003) 16:133–8.
26. Shaikh N, Hoberman A, Wise B, Kurs-Lasky M, Kearney D, Naylor S, et al. Dysfunctional elimination syndrome: is it related to urinary tract infection or vesicoureteral reflux diagnosed early in life? Pediatrics. (2003) 112:1134–7. doi: 10.1542/peds.112.5.1134
27. Chen JJ, Mao W, Homayoon K, Steinhardt GF. A multivariate analysis of dysfunctional elimination syndrome, and its relationships with gender, urinary tract infection and vesicoureteral reflux in children. J Urol. (2004) 171:1907–10. doi: 10.1097/01.ju.0000120288.82950.a2
28. Mingin GC, Hinds A, Nguyen HT, Baskin LS. Children with a febrile urinary tract infection and a negative radiologic workup: factors predictive of recurrence. Urology. (2004) 63:562–?5; discussion 565. doi: 10.1016/j.urology.2003.10.055
29. Lavelle MT, Conlin MJ, Skoog SJ. Subureteral injection of Deflux for correction of reflux: analysis of factors predicting success. Urology. (2005) 65:564–7. doi: 10.1016/j.urology.2004.09.068
30. Im YJ, Jeon HJ, Han SW. The impact of voiding dysfunction on vesicoureteral reflux and renal scars. Korean J Urol. (2005) 46:897. doi: 10.3978/j.issn.2223-4683.2012.06.09
31. Colen J, Docimo SG, Stanitski K, Sweeney DD, Wise B, Brandt P, et al. Dysfunctional elimination syndrome is a negative predictor for vesicoureteral reflux. J Pediatr Urol. (2006) 2:312–5. doi: 10.1016/j.jpurol.2006.01.013
32. Szymanik-Grzelak H, Sladowska J, Panczyk-Tomaszewska M, Sekowska R, Roszkowska-Blaim M. [Voiding dysfunction in children with vesicoureteral reflux]. Przegl Lek. (2006) 63 (Suppl. 3):142–5.
33. Higham-Kessler J, Reinert SE, Snodgrass WT, Hensle TW, Koyle MA, Hurwitz RS, et al. A review of failures of endoscopic treatment of vesicoureteral reflux with dextranomer microspheres. J Urol. (2007) 177:710–4; discussion 714–715. doi: 10.1016/j.juro.2006.09.082
34. Yucel S, Ates M, Erdogru T, Baykara M. Dysfunctional elimination syndrome in three generations of one family: might it be hereditary? Urology. (2004) 64:1231.e15–17. doi: 10.1016/j.urology.2004.06.034
35. Izquierdo RM-C, Luque Mialdea R. [Evaluation of the lower urinary tract function in pediatric patients with primary vesicoureteral reflux]. Arch Esp Urol. (2008) 61:191–207.
36. Williams H, Roelof BA, Venkatesan K, Steinhardt G. The impact of subureteral injection of Deflux for vesicoureteral reflux on children with voiding dysfunction. J Urol. (2009) 181:4. doi: 10.1016/S0022-5347(09)60633-9
37. Sillén U. Bladder dysfunction and vesicoureteral reflux. Adv Urol. (2008) 2008:815472. doi: 10.1155/2008/815472
38. Whittam BM, Thomasch JR, Makari JH, Tanaka ST, Thomas JC, Pope JC, et al. Febrile urinary tract infection after ureteroneocystostomy: a contemporary assessment at a single institution. J Urol. (2010) 183:688–92. doi: 10.1016/j.juro.2009.10.039
39. Altobelli E, Buscarini M, Nappo SG, Nguyen HT, Caione P. Urodynamics investigation on children with vesicoureteral reflux identifies overactive bladder and poor compliance in those with voiding dysfunction. Pediatr Surg Int. (2011) 27:517–22. doi: 10.1007/s00383-010-2822-z
40. Hong YK, Onal B, Diamond DA, Retik AB, Cendron M, Nguyen HT. Robot-assisted laparoscopic excision of symptomatic retrovesical cysts in boys and young adults. J Urol. (2011) 186:2372–8. doi: 10.1016/j.juro.2011.07.113
41. Palcic I, Strizic H, Cvitkovic RA. Urodynamic findings in children with vesicoureteral reflux after three years of age. Pediatr Nephrol. (2011) 26:1697. doi: 10.1007/s00467-011-1958-y
42. Giuseppe M, Chia L, Valeria M, Alessandro P. The outcome of children with VUR and voiding dysfunction managed with urotherapy. Neurourol Urodyn. (2012) 31(Suppl. 1):S22. doi: 10.1002/nau.22259
43. Öztürk BB, Özcakar B, Kavaz A, Ekim M, Yalcinkaya F. Voiding dysfunction in patients with urinary tract infection. Pediatr Nephrol. (2012) 27:9 doi: 10.1007/s00467-012-2232-7
44. Akhavan A, Avery D, Lendvay TS. Robot-assisted extravesical ureteral reimplantation: outcomes and conclusions from 78 ureters. J Pediatr Urol. (2014) 10:864–8. doi: 10.1016/j.jpurol.2014.01.028
45. Alexander SE, Arlen AM, Storm DW, Kieran K, Cooper CS. Bladder volume at onset of vesicoureteral reflux is an independent risk factor for breakthrough febrile urinary tract infection. J Urol. (2015) 193:1342–6. doi: 10.1016/j.juro.2014.10.002
46. Heckler AM, Sung J, Watters S, Martinez Acevedo A, Conlin M, Skoog S. The long-term incidence of urinary tract infection after endoscopic management of vesicoureteral reflux. Urology. (2014) 83:1383–7. doi: 10.1016/j.urology.2013.12.045
47. Hoberman A, Greenfield S, Mattoo T, Keren R, Mathews R, Pohl H, et al. Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med. (2014) 370:2367–76. doi: 10.1056/NEJMoa1401811
48. Cetin N, Sav NM, Yildiz B. The prevalence of constipation, enuresis and voiding dysfunction symptoms in children with uncomplicated recurrent urinary tract infection. Pediatric Nephrol. (2015). 30:1596.
49. Chang S-J, Tsai L-P, Hsu C-K, Yang SS. Elevated postvoid residual urine volume predicting recurrence of urinary tract infections in toilet-trained children. Pediatr Nephrol. (2015) 30:131–7. doi: 10.1007/s00467-014-3009-y
50. Chung JM, Park CS, Lee SD. Postoperative ureteral obstruction after endoscopic treatment for vesicoureteral reflux. Korean J Urol. (2015) 56:533–9. doi: 10.4111/kju.2015.56.7.533
51. Arlen AM, Cooper CS, Leong T. Role of body mass index in school-aged children with lower urinary tract dysfunction: does weight classification predict treatment outcome? J Pediatr Urol. (2017) 13:454.e1–454.e5. doi: 10.1016/j.jpurol.2017.03.033
52. Sharifi-Rad L, Ladi-Seyedian S-S, Amirzargar H, Kajbafzadeh A-M. Pelvic floor electromyography and urine flow patterns in children with vesicoureteral reflux and lower urinary tract symptoms. Int Braz J Urol. (2018) 44:1207–14. doi: 10.1590/s1677-5538.ibju.2018.0401
53. Tuygun C, Sertcelik N, Bakirtas H, Cakici H, Cetin K, Imamoglu AM. Usefulness of a new dysfunctional voiding and incontinence scoring system in predicting treatment effect in children with voiding dysfunction. Urol Int. (2007) 79:76–82. doi: 10.1159/000102919
54. Vlajković M, Ilić S, Bogićević M, Rajić M, Ristić L, Petronijević V, et al. Radionuclide voiding patterns in children with vesicoureteral reflux. Eur J Nucl Med Mol Imaging. (2003) 30:532–7. doi: 10.1007/s00259-002-1077-x
55. Vaz GT, Vasconcelos MM, Oliveira EA, Ferreira AL, Magalhães PG, Silva FM, et al. Prevalence of lower urinary tract symptoms in school-age children. Pediatr Nephrol. (2012) 27:597–603. doi: 10.1007/s00467-011-2028-1
56. Gaither TW, Cooper CS, Kornberg Z, Baskin LS, Copp HL. Risk factors for the development of bladder and bowel dysfunction. Pediatrics. (2018) 141:e20172797. doi: 10.1542/peds.2017-2797
57. Kajbafzadeh A-M, Sharifi-Rad L, Ghahestani SM, Ahmadi H, Kajbafzadeh M, Mahboubi AH. Animated biofeedback: an ideal treatment for children with dysfunctional elimination syndrome. J Urol. (2011) 186:2379–84. doi: 10.1016/j.juro.2011.07.118
58. Azevedo RVM de, Oliveira EA, Vasconcelos MM de A, Castro BAC de Pereira FR, Duarte NFV, et al. Impact of an interdisciplinary approach in children and adolescents with lower urinary tract dysfunction (LUTD). Braz J Nephrol. (2014) 36:451–9. doi: 10.5935/0101-2800.20140065
Keywords: dysfunctional elimination syndrome, vesicoureteral reflux, voiding dysfunction, constipation, urinary tract infection
Citation: Meena J, Mathew G, Hari P, Sinha A and Bagga A (2020) Prevalence of Bladder and Bowel Dysfunction in Toilet-Trained Children With Urinary Tract Infection and/or Primary Vesicoureteral Reflux: A Systematic Review and Meta-Analysis. Front. Pediatr. 8:84. doi: 10.3389/fped.2020.00084
Received: 13 October 2019; Accepted: 19 February 2020;
Published: 31 March 2020.
Edited by:
Sidharth Kumar Sethi, Medanta the Medicity, IndiaReviewed by:
Kjell Tullus, Great Ormond Street Hospital UCL Biomedical Research Centre, United KingdomCopyright © 2020 Meena, Mathew, Hari, Sinha and Bagga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pankaj Hari, cGFua2FqaGFyaUBob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.