 Jorge Alberto Acevedo-Murillo1Miguel Leonardo García León2Verónica Firo-Reyes3Jorge Luis Santiago-Cordova2†Alejandra Pamela Gonzalez-Rodriguez2
Jorge Alberto Acevedo-Murillo1Miguel Leonardo García León2Verónica Firo-Reyes3Jorge Luis Santiago-Cordova2†Alejandra Pamela Gonzalez-Rodriguez2 Rosa María Wong-Chew2*
Rosa María Wong-Chew2*- 1Hospital Pediátrico de Coyoacán, Mexico City, Mexico
- 2Laboratorio de Investigación en Enfermedades Infecciosas, División de Investigación, Facultad de Medicina, Universidad Nacional Autónoma de México, Mexico City, Mexico
- 3Servicio de Pediatría, Hospital General de México Dr. Eduardo Liceaga, Mexico City, Mexico
Background: Pneumonia caused 704,000 deaths in children younger than 5 years in 2015. Zinc is an important micronutrient due to its role in immune function. Since 2004, WHO recommends zinc supplementation for children with diarrhea to shorten the duration and decrease severity. Zinc supplementation for children with pneumonia is controversial.
Methods: A randomized controlled clinical trial was conducted, and 103 children 1 month to 5 years old with pneumonia were included. Zinc or placebo was given during hospitalization. Clinical symptoms were recorded, and a blood draw was obtained to determine serum zinc levels, lymphoproliferation, and cytokines at hospitalization and at discharge of the patient; a nasal wash was obtained to detect viral or bacterial pathogens by multiplex RT-PCR.
Results: Zinc supplementation improved in fewer hours the clinical status (76 ± 7 vs. 105 ± 8, p = 0.01), the respiratory rate (37 ± 6 vs. 57 ± 7, p = 0.04), and the oxygen saturation (53 ± 7 vs. 87 ± 9, p = 0.007) compared to the placebo group. An increase in IFNγ and IL-2 after treatment in the zinc group was observed.
Conclusions: Zinc supplementation improved some clinical symptoms in children with pneumonia in fewer hours and induced a cellular immune response.
Clinical Trial Registration: The trial was retrospectively registered in ClinicalTrials.gov, identifier NCT03690583, URL https://clinicaltrials.gov/ct2/show/NCT03690583?term=zinc+children&cond=Pneumonia&draw=2&rank=1.
Background
Great progress has been achieved for Millennium Development Goal 4: “to reduce child mortality rate by two-thirds.” The number of deaths in children under 5 decreased almost 40%, from 12.4 million in 1990 to 7.6 million in 2010 and by 51% from 2000 2015 (1, 2). Although infectious diseases are still a major disease burden—pneumonia, diarrhea, and malaria accounted for 30% of deaths in children younger than 5 years old in 2010—it is estimated that lower respiratory tract infections caused 2.74 million deaths in 2015, of which 704,000 were in children younger than 5 years old (3), and 652,572 deaths in 2016 (4). A decrease of 22% was observed in episodes of childhood pneumonia in young children from 178 million in 2000 to 138 million in 2015 and in the number of deaths from pneumonia from 1.7 million in 2000 to 0.9 million in 2015 (2, 5).
Malnutrition is a predisposing factor for recurrent and severe infections and includes zinc deficiency. Approximately 2 billion people in developing countries suffer from zinc deficiency, mainly due to malnutrition. The estimated prevalence of inadequate zinc intake varies from 7.5% in high-income regions to 30% in South Asia, and in the case of Mexico, the estimated prevalence of inadequate zinc intake is 15–25% (6). Zinc is a micronutrient that plays important roles in cell proliferation, differentiation, and immune function, acting as a cofactor for proteins and structural and catalytic functions of enzymes and transcription factors (7). Zinc promotes neutrophil extracellular traps, induces cell-mediated immunity over humoral immunity by regulating factors or differentiation, modulates the proinflammatory response by targeting NFκB, controls oxidative stress, and regulates inflammatory cytokines (8). Zinc deficiency promotes thymic atrophy and lymphopenia and decreases innate and adaptive immunity: it impairs host defense by neutrophils and natural killer cells, phagocytosis, intracellular killing activity, and cytokine production by macrophages and alters proliferation, cytokine production, and antibody secretion of T and B cells (9).
The World Health Organization (WHO) and Unicef recommend, since 2004, zinc supplementation along with oral rehydration to treat acute diarrhea because of the benefit of zinc in shortening and decreasing the severity reported in numerous randomized placebo-controlled trials (10).
In the case of zinc supplementation for children with pneumonia, the results are controversial. Some studies report a marginal improvement in hospital stay (11). Others report no differences in tachypnea, respiratory distress, or days for resolution of pneumonia compared to controls (12–16). And others report improvement in the clinical outcome and duration of hospital stay (17, 18) and prevention of mortality, incidence, and prevalence (19–23), including children with HIV in whom a decrease in days of hospital stay was observed (24). Some report higher basal zinc and better nutritional status as an effect of zinc on time to clinical resolution (25). A study in Uganda reported a decrease in mortality from 12 to 4% in children 6 months to 5 years old with pneumonia, with a decrease in the relative risk of 0.67 in mortality (26).
Cell-mediated immunity plays an important role in the host defense against viruses and bacteria; zinc supplementation in children with some degree of malnutrition and with a severe infection could improve the immune response to an acute infection. There are few reports of the assessment of the immune response in children with pneumonia who receive zinc supplementation along with the standard pneumonia treatment and the detection of the etiological agents by multiplex PCR.
The aim of this study was to evaluate the immunomodulatory effect of zinc supplementation and the correlation of the clinical response and etiological agent in children with pneumonia younger than 5 years old.
Methods
Study Population
Previously healthy children between 1 month and 5 years old with a clinical and/or radiological diagnosis of pneumonia admitted to the Hospital General de Mexico Dr. Eduardo Liceaga and the Hospital Pediátrico de Coyoacán were included. The very-low-income population of Mexico City and the metropolitan area attend these hospitals. The case definition for pneumonia was a child with signs and symptoms including fever, cough, tachycardia, tachypnea, dyspnea, respiratory distress, rales, and/or a radiographic pattern of pneumonia (27–29). Inclusion criteria were previously healthy children with the case definition of pneumonia. Exclusion criteria were zinc intake in the 2 previous weeks, history of cardiac and/or pulmonary disease including asthma, and prematurity.
The study was approved by the Institutional Review Boards of the Faculty of Medicine, Universidad Nacional Autónoma de México (036-2012), Hospital General de México (DI/13/505/05/026), and Hospital Pediátrico de Coyoacán (3020010114); written consent was obtained from parents or guardians. The procedures followed were in accordance with the ethical standards of the Helsinki Declaration.
Randomization and Masking
A triple-blinded randomized controlled clinical trial was conducted. The principal investigator generated the random allocation sequence. The pediatricians who recruited the patients, the patients and their mothers, and the laboratory technicians who performed the immunological and molecular tests did not know who received zinc or placebo.
At the time of admission to the hospital, parents or guardians were invited to have their children with pneumonia participate in the study and signed an informed consent. Children were randomly assigned 1:1 using a list of random numbers generated by Epistats to receive zinc sulfate (10 mg for children younger than 1 year old, 20 mg for children older than 1 year old) or placebo (20 mg of glucose). The list was generated by the principal investigator, and the participants were assigned to each group by the pediatricians recruiting the patients.
Study Procedures
Zinc and placebo contained in identical paper containers marked as A or B were diluted in 1 ml of distilled water and administered every day orally throughout the duration of hospitalization. Both substances looked like white powder inside the envelopes, and when they were diluted in distilled water, they also looked the same. At the inclusion of the child demographic, clinical characteristics, laboratory workup, a chest x-ray, and risk factors for pneumonia were obtained, and during the follow-up, clinical records including heart rate, oxygen saturation, respiratory distress, temperature, cough, rales, wheezing, and feeding capacity were recorded periodically six times a day until the discharge of the patient in a special format designed for this study. The nurses record the vital signs two times per shift in a hospital sheet, and there are three shifts per day. The clinical records were taken from those records and verified by the pediatricians. All the patients received the standard treatment protocol for children with pneumonia, which includes oxygen supplementation and intravenous fluid, and according to the criteria of the consultant physician, penicillin or ampicillin was administered or oseltamivir if influenza was suspected. Two blood draws were obtained, one when the child was admitted to the hospital and another one the day of discharge to perform lymphoproliferation and cytokine assays and to obtain sera, which was frozen at −70°C until processing to determine serum zinc levels.
Nasal washes were also obtained the day of hospitalization by instilling 1 ml of physiological saline solution through a sterile feeding tube connected to a syringe and aspirating the solution from each nostril, placing the content into viral medium, and storing at −70°C until processing to detect viral or bacterial genetic material. The nasal washes and blood samples were processed at the Unidad de Investigación en Medicina Experimental, Facultad de Medicina, UNAM.
Zinc Detection
Zinc in the sera of the patients at hospitalization and discharge was determined using a commercial kit (Zinc Monoliquid Fortress-Diagnostics, USA). Fifty microliters of serum was added to 1,000 μl of the reagent (5-Br-PAPS [2-(5-bromo-2-pyridylazo)-5-(N-propyl-N-sulfopropylamino)-phenol]) incubated for 5 min at 37°C and compared to the standard 200 μg/dl (30.6 mol/L). The sample was read at a wavelength of 560 nm in a Genesys 10S UV-Vis Spectrophotometer (Thermo Scientific); the signal intensity is directly proportional to the amount of zinc. The normal serum zinc is 63.8–110 μg/dl (9.8–16.8 μmol/L).
RT-PCR Technique
The nasal washes were processed using the Anyplex II RV16 kit (Seegene, Seoul, South Korea). The nucleic acid extraction was performed manually using the Ribo_spin GeneAll vRD kit (GeneAll Biotechnology, Seoul, South Korea); before extraction, an internal control of the Anyplex kit was added to each sample. The cDNA was synthesized from extracted RNA with the cDNA Synthesis Kit Premix (Seegene). Subsequently, real-time PCR was carried out in the CFX96 equipment (Bio-Rad) through the Anyplex II RV16 Detection kit, which uses TOCE technology. Amplified respiratory viruses were visualized using the Seegene Viewer software. The Anyplex RV16 kit has the capacity to detect 14 RNA viruses and 2 DNA viruses: respiratory syncytial virus types A and B; influenza virus types A and B; parainfluenza virus types 1–4; adenovirus; metapneumovirus; coronavirus OC43, 229E, and NL63; rhinovirus types A, B, and C; enterovirus; and bocavirus. Bacterial genetic material was detected in nasal washings using the Seeplex RV15 ACE detection kit (Seegene, Seoul Korea) with simultaneous detection with a multiplex PCR using the DPO technology. The kit detects Streptococcus pneumoniae, Haemophilus influenzae, Chlamydophila pneumoniae, Legionella pneumophila, Bordetella pertussis, and Mycoplasma pneumoniae.
Lymphoproliferation Assay
Fresh peripheral blood mononuclear cells (PBMCs) were obtained from whole blood by Ficoll-Hypaque density gradient. PBMCs were placed in a 96-well-plate at 3.0 × 105 cells per well in RMPI 1640 medium (Gibco, Gaithersburg, MD) with 10% normal human sera (Sigma, St. Louis, MO); 5 μg of concanavalin A (Sigma-Aldrich) was added, and cells were incubated at 37°C and 5% CO2 for 5 days. EdU Click-iT Alexa Fluor 488 (Invitrogen) was added for 6 h, and cells were acquired by flow cytometry using the FACSCanto II cytometer (Becton Dickinson); the lymphoproliferation was analyzed using the FacsDiva software (Becton Dickinson) determined by the difference in fluorescence intensity means (MiFID) of the control and ConA wells.
Cytokine Assays
PBMCs were placed in a 96-wells plate at 3.0 x 105 cells per well in RMPI 1640 medium (Gibco, Gaithersburg, MD) with 5% normal human sera (Sigma, St. Louis, MO); 3 μl of Cytostim (Myltenyi Biotec) or medium as negative control was added and incubated at 37°C and 5% CO2 for 6 h, and supernatants of the wells were collected. Cytokines were determined using the Cytometric Bead Array Human Th1/Th2 kit (Becton Dickinson) following the manufacturer's instructions, which includes IL-2, IL-4, IL-6, IL-10, TNF-alpha, and IFN-gamma obtained by flow cytometry (FACSCanto II) and analyzed with the FCAP Array software (Becton Dickinson).
Sample Size Calculation and Statistical Analysis
Sample size calculation was based on the dependent variable time in hours for improvement using G power to calculate the difference between two independent means. The variance and the difference were obtained from a previous publication (30), with an effect size of 0.5, a power of 80%, and alpha of 0.05, obtaining a sample size of 51 per group, 102 total. Frequencies and proportions of clinical and demographic variables were determined by descriptive statistics. Student t and paired t-test were used to contrast quantitative variables; chi square was used to contrast qualitative variables. Malnutrition was calculated by Z score and categorized as presence or absence for analysis. Because the placebo group were younger and smaller, in order to detect a bias, a covariance analysis (ANCOVA) was done adjusting for age, weight, height, body mass index (BMI), vaccination status, and nutrition status the dependent variables (clinical improvement, normalization of respiratory rate, normalization of oxygen saturation). A p < 0.05 was considered statistically significant.
Results
One hundred and seventy patients with pneumonia younger than 5 years old were detected at the participating institutions from January 2014 to February 2016; 62 were not eligible because 39 had asthma, 1 HIV infection, 10 cardiopathy, and 12 pneumopathy, and 5 parents declined to participate. Of those eligible and whose parents accepted to have their children participate, 51 received zinc and 53 placebo. All the participants were included in the analysis because there were no losses, except for one patient in the zinc group who did not have the follow-up information and the blood draw. The patients were followed at the hospitals during their treatment (Figure 1 and Supplementary Table 1).
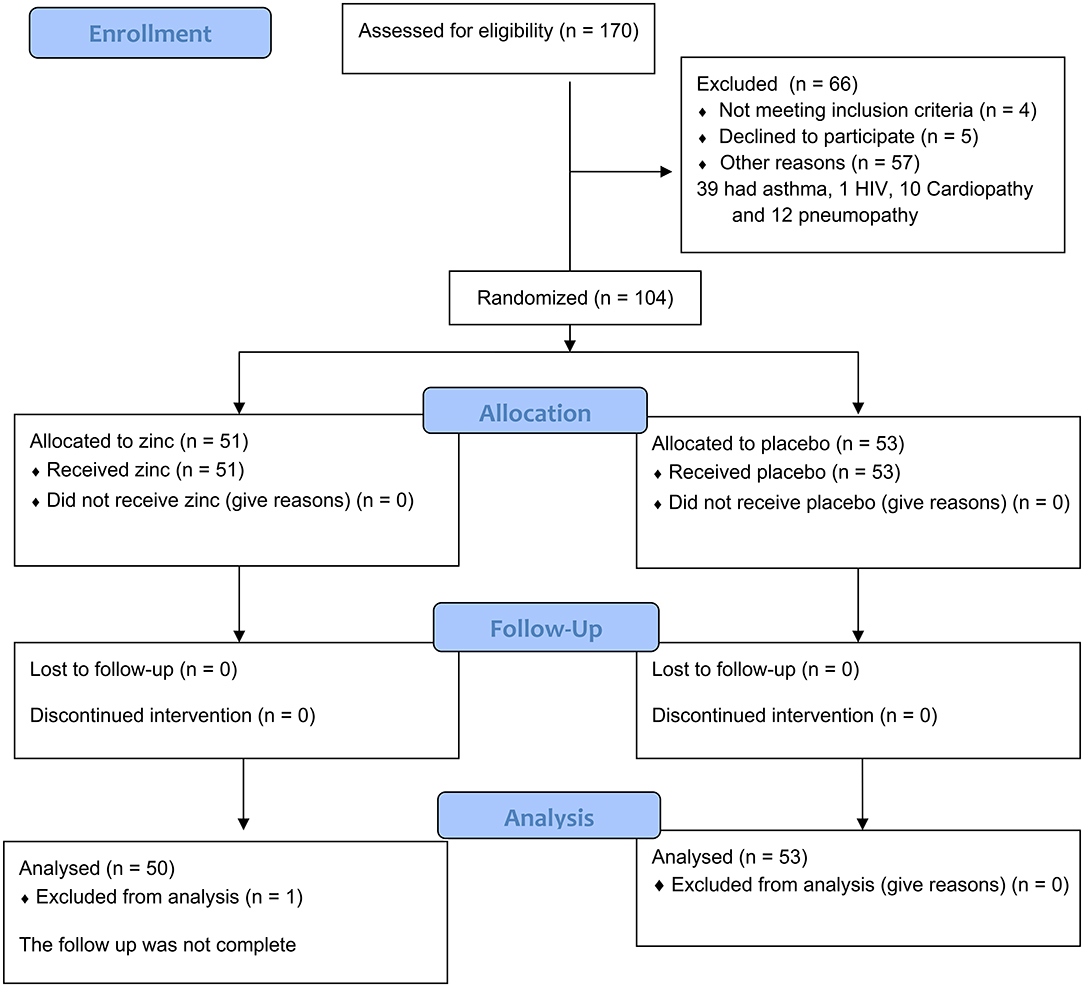
Figure 1. CONSORT flow diagram of the inclusion and analysis of the patients.
Demographic and Clinical Characteristics
The mean ± SE age in the zinc group was 23 ± 2.2 months compared to 18 ± 2.2 in the placebo group (p = 0.09). The children in the placebo group had a lower weight and height compared to the zinc group (9.4 ± 0.5 vs. 11.1 ± 0.5, p = 0.01, and 74.9 ± 2.2 vs. 81.4 ± 2.3, p = 0.05, respectively), and there were more males in the placebo group compared to the zinc group (64 vs. 46%, p = 0.04, respectively). The baseline clinical symptoms were comparable (according to the WHO pneumonia classification)—pneumonia (66 vs. 62%), severe pneumonia (32 vs. 34%, p = 0.83), oxygen saturation (85 ± 0.7 vs. 84 ± 0.7, p = 0.36), and respiratory rate (mean ± SE, 43 ± 1.4 vs. 45 ± 1.5, p = 0.54)—between the zinc and the placebo group, respectively. The predominant radiographic pattern was interstitial (82 vs. 71%), followed by alveolar (9 vs. 13%) and mixed (2 vs. 11%) (p = 0.26), in the zinc and the placebo group. Also comparable was the percentage of children with rales, fever, cough, respiratory distress, rhinorrhea, vomit, nasal flare, and costal retraction by group. No differences in the percentage of symptomatic, antibiotic, or antiviral treatment between groups were observed. Penicillin is used as empiric treatment for CAP in children at the Hospital Pediatrico de Coyoacan and ampicillin at the Hospital General de México, according to local hospital guidelines based on sensitivity patterns (Table 1).
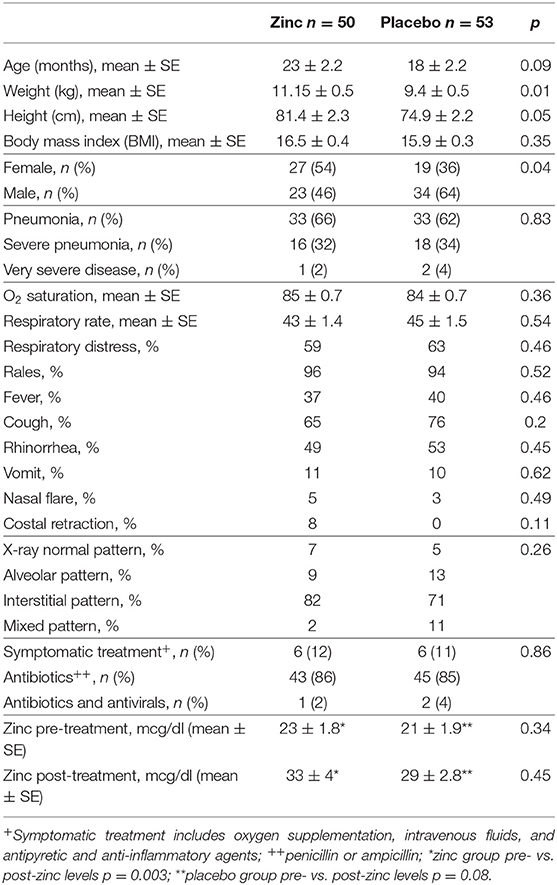
Table 1. Baseline demographic and clinical characteristics of children with pneumonia who received zinc supplementation and placebo.
Zinc levels were below the normal range (63–110 mcg/mL) at baseline (23 ± 1.8 vs. 21 ± 1.9, p = 0.34) and after treatment (33 ± 4 vs. 29 ± 2.8, p = 0.45), and no differences were found between zinc and placebo, respectively. Both groups increased zinc levels after supplementation, but the placebo group was not significant. Although the zinc group showed a statistically significant increase after supplementation (p = 0.003), it did not reach the normal serum level reported (Table 1). No side effects were reported with zinc or placebo supplementation.
Risk Factors
Both groups were comparable for the following risk factors—low income (96 vs. 94%, p = 0.52), malnutrition (23 vs. 28%, p = 0.41), domestic smoking (32 vs. 36%, p = 0.39), absence of breastfeeding (24 vs. 21%, p = 0.88), and overcrowding (62 vs. 58%, p = 0.4), in the zinc and the placebo group, respectively. The proportion of children with an incomplete vaccination schedule was higher in the placebo group (50 vs. 30%, p = 0.04), and there were more children attending daycare centers in the zinc group (32 vs. 11%, p = 0.01) (Table 2).
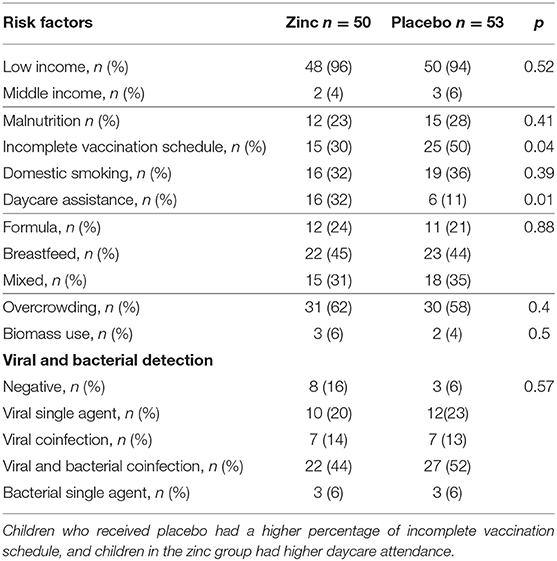
Table 2. Risk factors for pneumonia and viral or bacterial detection.
Viral and Bacterial Detection
The percentage of viral and bacterial detection was comparable among groups−20 vs. 23% one virus, 14 vs. 13% viral coinfection, 44 vs. 52% viral and bacterial coinfection, 6 vs. 6% bacteria (p = 0.57), in the zinc and placebo groups, respectively (Table 2).
Distribution of virus and bacteria in both groups is shown in Figure 2. RSV A and B, rhinovirus, and metapneumovirus were the most frequent detected viruses in both groups as single agents or in combination. H. influenzae and S. pneumoniae were the most frequently detected bacteria in both groups as single agents or in combination. The incidence of pathogens detected was similar in both groups. There were more than three pathogens in the majority of patients in the zinc (58%) and the placebo (65%) group, respectively (Figure 2B). Analysis of only virus (Supplementary Table 2) or only bacteria showed no differences in frequencies among groups.
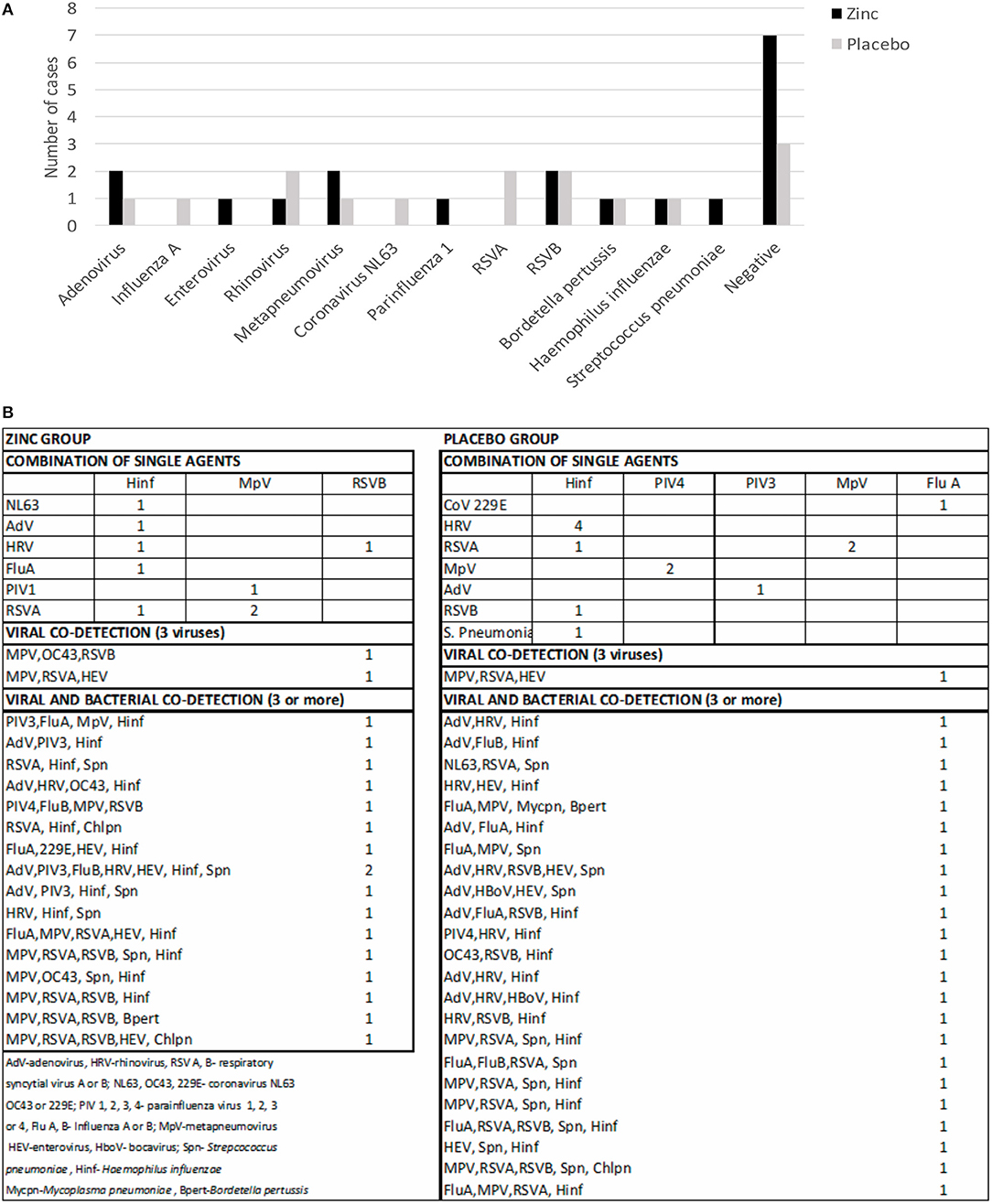
Figure 2. Viral and bacterial detection in children with pneumonia who received zinc or placebo. (A) Detection of single agents by group. (B) Number of combined detection of virus–virus, bacteria–bacteria, or virus–bacteria by group.
Comparison of the Time for Improvement
The clinical improvement (mean in hours of the combination of all the clinical variables) (76 ± 7 vs. 105 ± 8, p = 0.01), the normalization of the respiratory rate (37 ± 6 vs. 57 ± 7, p = 0.04), and the normalization of oxygen saturation (53 ± 7 vs. 87 ± 9, p = 0.007) measured in hours was faster in the zinc group compared to the placebo group and statistically significant. In the analysis of covariance adjusting the effect of zinc for age (because the placebo group were younger), a p of 0.01 was found for time for clinical improvement, 0.07 for respiratory rate, and 0.009 for oxygen saturation, meaning that the younger age in the placebo group was not a bias and had no effect for the better response in the zinc group. Also, weight, height, BMI, gender, vaccination status, and nutrition status had no effect in the covariance analysis on the dependent variables.
There were no statistically significant differences in the normalization of respiratory distress (46 ± 4 vs. 56 ± 6, p = 0.21), normalization of temperature (6 ± 1 vs. 7 ± 2, p = 0.85) in hours, and days of hospitalization (4 ± 0.2 vs. 4.8 ± 0.3, p = 0.91) between the zinc and the placebo group, respectively, although a tendency was observed (Table 3). No deaths were reported in any of the participants of the study.
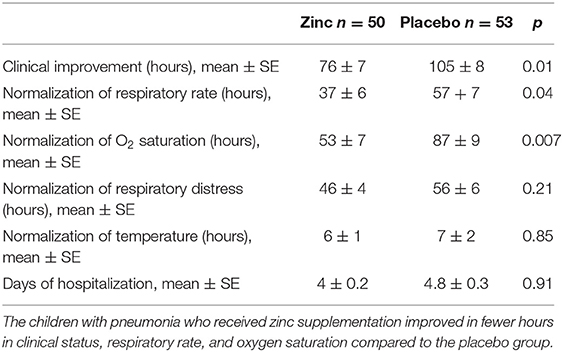
Table 3. Comparison of the time for improvement of clinical symptoms.
No side effects were reported in children who received zinc or placebo.
Immune Response
The lymphoproliferation to concanavalin A of the PBMCs from children with pneumonia measured by EdU Click-iT incorporation were comparable between the zinc (mean ± SE difference of intensity 89 ± 19) and the placebo group (136 ± 25, p = 0.14) before and after treatment (81 ± 20 vs. 93 ± 22, p = 0.7), respectively.
Cytokine responses showed an increase in Th1 pattern for IL-2 (x ± SEM, 22 ± 9 to 46 ± 26) and INF-γ (x ± SEM, 20 ± 6 to 85 ± 59) after supplementation in the zinc group; TNFα (x ± SEM, 665 ± 267 to 1138 ± 359) increased in the placebo group, although in the zinc group, it remained high. From the Th2 cytokines, IL-10 increased in both groups (x ± SEM: zinc 151 ± 46 to 382 ± 128, placebo 253 ± 80 to 425 ± 152), IL-4 decreased (x ± SEM: zinc 3 ± 1 to 0.25 ± 0.2, placebo 3 ± 1 to 0.25 ± 0.25), and IL-6 remained high in both groups (Figure 3).
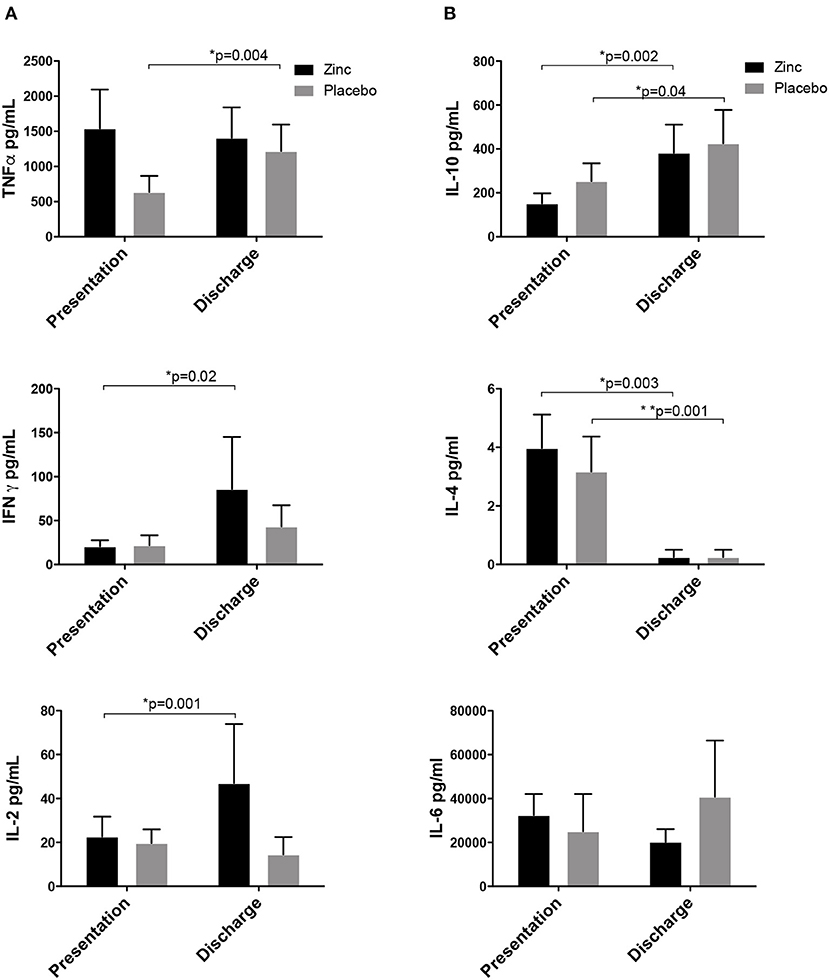
Figure 3. Cytokine responses of children with pneumonia supplemented with zinc or placebo. (A) TH1 cytokines: IL-2 and INF-γ increased in the zinc group, and TNFα increased in the placebo group, although in the zinc group, it remained high. (B) Th2 cytokines: IL-10 increased in both groups, IL-4 decreased, and IL-6 remained high in both groups.
Discussion
Zinc deficiency alters innate and adaptive immunity (8). Zinc supplementation improves immunity, ameliorates chronic dysfunctional inflammatory responses (7), and has been shown to shorten the duration and decrease severity in children with diarrhea, and since 2004, WHO and Unicef recommend zinc supplementation along with oral rehydration (10).
In the case of pneumonia, there are several trials and meta-analyses about zinc supplementation. Some found benefits (17–21, 24, 26, 31), others limited improvement (11), and some found a lack of benefits compared to placebo (12–14, 32). However, the outcomes and methodologies are different in each clinical trial, and there is no immunological and etiological assessment.
We conducted a randomized triple-blinded controlled clinical trial, using the recommended WHO dose of zinc for children with diarrhea in children with pneumonia; measuring the clinical symptoms as previously reported in many RCTs but with a translational approach where we measured cytokines, the lymphoproliferative capacity after zinc supplementation, and serum zinc levels; and detecting the etiological agents by multiplex PCR, trying to find a correlation of the pathogen, the clinical development, and the immune response.
We found that zinc improves oxygen saturation, tachypnea, and clinical status in fewer hours than the placebo group, independently of age, weight, height, BMI, nutritional, or vaccination status according to the covariance analysis, and this correlates with an increase in Th1 cytokines IFNγ and IL-2 in the zinc group at discharge of the patient (after zinc supplementation). Although there was no difference in hospital stay, the respiratory symptoms improved faster. Both hospitals attend to a very-low-income population, and the discharge of a patient depends on many factors; for example, some patients improved but stayed hospitalized to finish the antibiotic treatment due to the lack of resources to buy the antibiotic, or for administrative reasons like payment of the hospitalization and lack of money of the parents. We considered that hospital stay length is not a good clinical marker of improvement in our country, so we looked at other clinical markers, such as respiratory distress, oxygen saturation, or tachypnea, that denote the clinical improvement of the children. Viruses are responsible in up to 81% of the cases of pneumonia in children younger than 5 years old (33). Viruses are intracellular pathogens where a strong cellular immune response is needed, and in the case of both groups, we infer that an increase of proinflammatory cytokines TNFα and IL-6 and Th1 cytokines IFNγ and IL-2 took place between the time of entrance of the pathogen to the organism and the development of pneumonia, which is demonstrated by the lymphoproliferation detected at the moment of pneumonia and slight decrease at resolution when the blood draw was taken. A persistent level of TNFα and IL-6 at both times of detection was observed in both groups; it could be either the important systemic and pulmonary inflammation or the zinc deficiency associated with the production of proinflammatory cytokines such as IL-1β, IL-6, and TNFα (8, 34) because in both groups, serum zinc levels were below normal despite zinc supplementation at the moment of admission with pneumonia and at the discharge. It is noteworthy that TNFα showed a statistically significant increase in the placebo group, but the zinc group had high levels of TNFα at admission with pneumonia that persisted at discharge, comparable to the placebo group in the last measurement (Figure 2A). The increase in IFNγ and IL-2 with zinc supplementation compared to the placebo suggests a promotion of cell-mediated immunity over humoral immunity, also shown by a decrease in IL-4; this cell-mediated immunity could result in faster improvement of the clinical symptoms compared to the placebo group. IL-10, a down-regulatory cytokine, increased at resolution in both groups, which is expected after an inflammatory response takes place and where this cytokine in necessary to return to the basal state. In both groups, inflammation takes place due to the pathogens and the immune response, and it is demonstrated by a high level of proinflammatory cytokines and mononuclear proliferation in the basal blood sample. An explanatory model is shown in Supplementary Figure 1 based on the cytokine and lymphoproliferation responses according to the time of blood draws.
The children in the placebo group had a lower weight and height, which could be a confounding variable, although they were 5 months younger, and that would explain the differences; and it is noteworthy that malnutrition showed no differences between groups. Because of this difference in age, adjusting by age, weight, height, and BMI, the effect of zinc on the respiratory parameters with a covariance analysis did not show an effect, which means the younger age is not a bias in the better response of the zinc group. Another risk factor that was higher in the placebo group was incomplete vaccination schedule (50 vs. 30%, p = 0.04, placebo vs. zinc, respectively), although the results of the multiplex RT-PCR showed a very high proportion of patients with viral infections and co-infections that are not prevented by vaccines included in the Mexican vaccination program. The only virus detected by the PCR included in the National Vaccination program is influenza, and cases of influenza in both groups were comparable; also, S. pneumoniae is in the National Vaccination program, and both groups showed equal frequency. One limitation of the study was that the mothers did not provide the vaccination record; we could not analyze the differences in specific vaccines among groups and could not corroborate the vaccines received by each child.
Zinc levels increased in the treatment group compared to the placebo, but they were below normal levels at admission to the hospital for pneumonia and also at discharge despite the supplementation. It is possible that zinc was depleted by consumption by PBMCs or neutrophils because of the inflammatory response (34), or by the use of bacteria to drive key cellular processes during infection (35), but it is also possible that the children who attended both hospitals are from a very-low-income population, and zinc deficiencies due to malnutrition (in our group, up to 30%) could be the basal state of the children; a control of healthy subjects would have been suitable to answer these questions. Also, it is possible that a higher dose or a longer duration of treatment with zinc would have achieved a better serum zinc level, but we based it on the intervention described by WHO and other studies where the same dose of zinc showed benefits. It is noteworthy that the placebo group also presented a tendency to increase the zinc levels, although not significant; this could be related to the balanced food given at the hospital to very-low-income children.
Although we found many combinations of viruses and bacteria, the capacity to detect multiple bacteria in nasal washes is hard to interpret because only genetic material is detected by the multiplex PCR in the absence of a bronchial culture or blood culture, and the detection could be bacterial colonization, which has been described in up to 64% in the nasopharynx of healthy subjects (36). In the case of viruses, it is unknown if there is colonization or if they are only detected when inflammation and disease exist. No correlations of clinical, immunological, and etiological agents could be made due to the large number of combinations of viruses and/or bacteria. And the proportion of viral, bacterial, or combined detection was comparable between groups.
All the controversies about zinc supplementation for children with pneumonia are based on clinical trials where the zinc is administered and the clinical outcome is measured. We did not attempt to add clinical evidence in the context of a randomized controlled trial that has been extensively published but, rather, to look for immunological evidence of the effect of zinc in children with pneumonia. Some translational studies report immunological evidence of pathologies in humans in little as 5–10 patients; this study with 50 patients in each group adds immune evidence of zinc supplementation in children with pneumonia. This is the first study to provide immunological evidence of a Th1 response in the context of a randomized controlled clinical trial, where translational medicine is applied and where an immunological pattern is detected and correlates with the clinical outcome.
Conclusions
Zinc supplementation showed benefits, shortening the duration of oxygen desaturation, tachypnea, and clinical symptoms in children with pneumonia, showing a Th1 response with the increase of IFNγ and IL-2 cytokines. Zinc supplementation along with the standard protocol for treatment could be further explored as a recommendation for children with pneumonia, which constitutes one of the most frequent causes of morbidity and mortality in children younger than 5 years old.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The study was approved by the Institutional Review Boards of the Faculty of Medicine, Universidad Nacional Autónoma de México (036-2012), Hospital General de México (DI/13/505/05/026), and Hospital Pediátrico de Coyoacán (3020010114); written consent was obtained from parents or guardians. The procedures followed were in accordance with the ethical standards of the Helsinki Declaration.
Author's Note
Previous affiliation of Rosa María Wong-Chew, Miguel Leonardo García-León, Jorge Luis Santiago-Cordova and Alejandra Pamela González-Rodríguez was Unidad de Investigación en Medicina Experimental, Facultad de Medicina, UNAM; Dr. Balmis # 148, Colonia Doctores 06726, México, D.F. The work was presented in part as abstracts at the annual meeting of the Asociación Mexicana de Infectología y Microbiología, San Luis Potosí, México, May 2015, Monterrey, México, May 2016, and the IX National Virology Meeting Puente de Ixtla, Morelos, México, November 2015.
Author Contributions
RW-C: study design, data analysis, data interpretation, writing the manuscript, study coordination, writing a grant, and obtaining financial support for the study. JA-M, VF-R, and JS-C: patient recruitment, sample collection, and review of the manuscript. MG: study design, data interpretation, processing of the blood samples to determine the immune responses (lymphoproliferation and cytokine levels), and review of the manuscript. AG-R: processing of the nasal samples by the multiplex PCR methods to detect viral and bacterial pathogens and review of the manuscript.
Funding
This work was supported by a grant from the Consejo Nacional de Ciencia y Tecnología, Mexico (CONACYT182274), to RW-C, PI.
Conflict of Interest
RW-C reports personal fees from Sanofi Pasteur as a speaker and GSK and Abbvie for advisory boards, outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors are grateful to María Antonieta Espinoza-Torres, Myrna Mar Talavera Torres, Sugely Velasco-Terrones, Ricardo Landa-Gutiérrez, and Cynthia Aixa Rivera-López for their help in the recruitment of patients, and to the Liver, Pancreas and Motility unit of the Universidad Nacional Autonoma de Mexico for the use of the FACSCanto II cytometer.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2019.00431/full#supplementary-material
References
1. Bryce J, Black RE, Victora CG. Millennium development goals 4 and 5: progress and challenges. BMC Med. (2013) 11:225. doi: 10.1186/1741-7015-11-225
2. McAllister DA, Liu L, Shi T, Chu Y, Reed C, Burrows J, et al. Global, regional, and national estimates of pneumonia morbidity and mortality in children younger than 5 years between 2000 and 2015: a systematic analysis. Lancet Glob Health. (2019) 7:e47–57. doi: 10.1016/S2214-109X(18)30408-X
3. Collaborators GL. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect Dis. (2017) 17:1133–61. doi: 10.1016/S1473-3099(17)30396-1
4. GBD 2016 Lower Respiratory Infections Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. (2018) 18:1191–210. doi: 10.1016/S1473-3099(18)30310-4
5. Howie SRC, Murdoch DR. Global childhood pneumonia: the good news, the bad news, and the way ahead. Lancet Glob Health. (2019) 7:e4–5. doi: 10.1016/S2214-109X(18)30446-7
6. Wessells KR, Brown KH. Estimating the global prevalence of zinc deficiency: results based on zinc availability in national food supplies and the prevalence of stunting. PLoS ONE. (2012) 7:e50568. doi: 10.1371/journal.pone.0050568
7. Hojyo S, Fukada T. Zinc transporters and signaling in physiology and pathogenesis. Arch Biochem Biophys. (2016) 611:43–50. doi: 10.1016/j.abb.2016.06.020
8. Gammoh NZ, Rink L. Zinc in infection and inflammation. Nutrients. (2017) 9:624. doi: 10.3390/nu9060624
9. Shankar AH, Prasad AS. Zinc and immune function: the biological basis of altered resistance to infection. Am J Clin Nutr. (1998) 68:447–63S. doi: 10.1093/ajcn/68.2.447S
10. Black CLFWaRE. Zinc Supplementarion for Diarrrhoea Treatment. e-Library of Evidence for Nutrition Actions (eLENA): World Heath Organization (2014).
11. Basnet S, Shrestha PS, Sharma A, Mathisen M, Prasai R, Bhandari N, et al. A randomized controlled trial of zinc as adjuvant therapy for severe pneumonia in young children. Pediatrics. (2012) 129:701–8. doi: 10.1542/peds.2010-3091
12. Ganguly A, Chakraborty S, Datta K, Hazra A, Datta S, Chakraborty J. A randomized controlled trial of oral zinc in acute pneumonia in children aged between 2 months to 5 years. Indian J Pediatr. (2011) 78:1085–90. doi: 10.1007/s12098-011-0495-9
13. Valentiner-Branth P, Shrestha PS, Chandyo RK, Mathisen M, Basnet S, Bhandari N, et al. A randomized controlled trial of the effect of zinc as adjuvant therapy in children 2-35 mo of age with severe or nonsevere pneumonia in Bhaktapur, Nepal. Am J Clin Nutr. (2010) 91:1667–74. doi: 10.3945/ajcn.2009.28907
14. Bose A, Coles CL, Gunavathi, John H, Moses P, Raghupathy P, et al. Efficacy of zinc in the treatment of severe pneumonia in hospitalized children <2 y old. Am J Clin Nutr. (2006) 83:1089–96; quiz 207. doi: 10.1093/ajcn/83.5.1089
15. Tie HT, Tan Q, Luo MZ, Li Q, Yu JL, Wu QC. Zinc as an adjunct to antibiotics for the treatment of severe pneumonia in children <5 years: a meta-analysis of randomised-controlled trials. Br J Nutr. (2016) 115:807–16. doi: 10.1017/S0007114515005449
16. Bagri NK, Bagri N, Jana M, Gupta AK, Wadhwa N, Lodha R, et al. Efficacy of oral zinc supplementation in radiologically confirmed pneumonia: secondary analysis of a randomized controlled trial. J Trop Pediatr. (2018) 64:110–7. doi: 10.1093/tropej/fmx036
17. Valavi E, Hakimzadeh M, Shamsizadeh A, Aminzadeh M, Alghasi A. The efficacy of zinc supplementation on outcome of children with severe pneumonia. A randomized double-blind placebo-controlled clinical trial. Indian J Pediatr. (2011) 78:1079–84. doi: 10.1007/s12098-011-0458-1
18. Wahed MA, Islam MA, Khondakar P, Haque MA. Effect of micronutrients on morbidity and duration of hospital stay in childhood pneumonia. Mymensingh Med J. (2008) 17:S77–83.
19. Yakoob MY, Theodoratou E, Jabeen A, Imdad A, Eisele TP, Ferguson J, et al. Preventive zinc supplementation in developing countries: impact on mortality and morbidity due to diarrhea, pneumonia and malaria. BMC Public Health. (2011) 11(Suppl. 3):S23. doi: 10.1186/1471-2458-11-S3-S23
20. Lassi ZS, Haider BA, Bhutta ZA. Zinc supplementation for the prevention of pneumonia in children aged 2 months to 59 months. Cochrane Database Syst Rev. (2010) 12:CD005978. doi: 10.1002/14651858.CD005978.pub2
21. Fischer Walker C, Black RE. Zinc and the risk for infectious disease. Annu Rev Nutr. (2004) 24:255–75. doi: 10.1146/annurev.nutr.23.011702.073054
22. Wang L, Song Y. Efficacy of zinc given as an adjunct to the treatment of severe pneumonia: a meta-analysis of randomized, double-blind and placebo-controlled trials. Clin Respir J. (2018) 12:857–64. doi: 10.1111/crj.12646
23. Lassi ZS, Moin A, Bhutta ZA. Zinc supplementation for the prevention of pneumonia in children aged 2 months to 59 months. Cochrane Database Syst Rev. (2016) 12:CD005978. doi: 10.1002/14651858.CD005978.pub3
24. Mda S, van Raaij JM, de Villiers FP, MacIntyre UE, Kok FJ. Short-term micronutrient supplementation reduces the duration of pneumonia and diarrheal episodes in HIV-infected children. J Nutr. (2010) 140:969–74. doi: 10.3945/jn.109.110312
25. Sempertegui F, Estrella B, Rodriguez O, Gómez D, Cabezas M, Salgado G, et al. Zinc as an adjunct to the treatment of severe pneumonia in Ecuadorian children: a randomized controlled trial. Am J Clin Nutr. (2014) 99:497–505. doi: 10.3945/ajcn.113.067892
26. Srinivasan MG, Ndeezi G, Mboijana CK, Kiguli S, Bimenya GS, Nankabirwa V, et al. Zinc adjunct therapy reduces case fatality in severe childhood pneumonia: a randomized double blind placebo-controlled trial. BMC Med. (2012) 10:14. doi: 10.1186/1741-7015-10-14
27. Assad FA, Brès P, ten Darn HG, Dowling MAC, Hitze KL, Houang L, et al. Clinical management of acute respiratory infections in children: a WHO memorandum. Bull World Health Organ. (1981) 59:707–16.
28. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. (2011) 53:e25–76. doi: 10.1093/cid/cir531
29. Harris M, Clark J, Coote N, Fletcher P, Harnden A, McKean M, et al. British Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011. Thorax. (2011) 66(Suppl. 2):ii1–23. doi: 10.1136/thoraxjnl-2011-200598
30. Mahalanabis D, Lahiri M, Paul D, Gupta S, Gupta A, Wahed MA, et al. Randomized, double-blind, placebo-controlled clinical trial of the efficacy of treatment with zinc or vitamin A in infants and young children with severe acute lower respiratory infection. Am J Clin Nutr. (2004) 79:430–6. doi: 10.1093/ajcn/79.3.430
31. Shehzad N, Anwar MI, Muqaddas T. Zinc supplementation for the treatment of severe pneumonia in hospitalized children: a randomized controlled trial. Sudan J Paediatr. (2015) 15:37–41.
32. Haider BA, Lassi ZS, Ahmed A, Bhutta ZA. Zinc supplementation as an adjunct to antibiotics in the treatment of pneumonia in children 2 to 59 months of age. Cochrane Database Syst Rev. (2011) CD007368. doi: 10.1002/14651858.CD007368.pub2
33. Wong-Chew RM, Garcia-Leon ML, Noyola DE, Perez Gonzalezc LF, Mezad JG, Vilaseñor-Sierra A, et al. Respiratory viruses detected in Mexican children younger than 5 years old with community-acquired pneumonia: a national multicenter study. Int J Infect Dis. (2017) 62:32–8. doi: 10.1016/j.ijid.2017.06.020
34. Haase H, Rink L. Zinc signals and immune function. Biofactors. (2014) 40:27–40. doi: 10.1002/biof.1114
35. Ma L, Terwilliger A, Maresso AW. Iron and zinc exploitation during bacterial pathogenesis. Metallomics. (2015) 7:1541–54. doi: 10.1039/C5MT00170F
Keywords: zinc supplementation, pneumonia, children, immune response, Th1 cytokines
Citation: Acevedo-Murillo JA, García León ML, Firo-Reyes V, Santiago-Cordova JL, Gonzalez-Rodriguez AP and Wong-Chew RM (2019) Zinc Supplementation Promotes a Th1 Response and Improves Clinical Symptoms in Fewer Hours in Children With Pneumonia Younger Than 5 Years Old. A Randomized Controlled Clinical Trial. Front. Pediatr. 7:431. doi: 10.3389/fped.2019.00431
Received: 14 March 2019; Accepted: 07 October 2019;
Published: 14 November 2019.
Edited by:
Valeriane Leroy, Institut National de la Santé et de la Recherche Médicale (INSERM), FranceReviewed by:
Danilo Buonsenso, Catholic University of the Sacred Heart, ItalyRobindra Basu Roy, London School of Hygiene and Tropical Medicine, United Kingdom
Copyright © 2019 Acevedo-Murillo, García León, Firo-Reyes, Santiago-Cordova, Gonzalez-Rodriguez and Wong-Chew. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosa María Wong-Chew, cm13b25nQHVuYW0ubXg=
†Present address: Jorge Luis Santiago-Cordova, Hospital General de Zona no. 2 del Instituto Mexicano del Seguro Social Hermosillo, Sonora, Mexico