
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 22 July 2020
Sec. Cancer Epidemiology and Prevention
Volume 10 - 2020 | https://doi.org/10.3389/fonc.2020.01279
This article is part of the Research Topic COVID-19 Infection in Cancer Patients: How Can We Help Patients and Oncologists? View all 38 articles
 Beth Russell1†
Beth Russell1† Charlotte Moss1†
Charlotte Moss1† Sophie Papa2,3
Sophie Papa2,3 Sheeba Irshad2,3Paul Ross2James Spicer2,3
Sheeba Irshad2,3Paul Ross2James Spicer2,3 Shahram Kordasti2,4
Shahram Kordasti2,4 Danielle Crawley1,2
Danielle Crawley1,2 Harriet Wylie1Fidelma Cahill1
Harriet Wylie1Fidelma Cahill1 Anna Haire1Kamarul Zaki2Fareen Rahman2Ailsa Sita-Lumsden2Debra Josephs1,2
Anna Haire1Kamarul Zaki2Fareen Rahman2Ailsa Sita-Lumsden2Debra Josephs1,2 Deborah Enting1,2Mary Lei2Sharmistha Ghosh2Claire Harrison2,4Angela Swampillai2Elinor Sawyer2,3Andrea D'Souza2Simon Gomberg2Paul Fields4David Wrench4
Deborah Enting1,2Mary Lei2Sharmistha Ghosh2Claire Harrison2,4Angela Swampillai2Elinor Sawyer2,3Andrea D'Souza2Simon Gomberg2Paul Fields4David Wrench4 Kavita Raj4Mary Gleeson4Kate Bailey4Richard Dillon4,5Matthew Streetly4Anne Rigg2Richard Sullivan3
Kavita Raj4Mary Gleeson4Kate Bailey4Richard Dillon4,5Matthew Streetly4Anne Rigg2Richard Sullivan3 Saoirse Dolly2‡
Saoirse Dolly2‡ Mieke Van Hemelrijck1,2*‡
Mieke Van Hemelrijck1,2*‡Background: There is insufficient evidence to support clinical decision-making for cancer patients diagnosed with COVID-19 due to the lack of large studies.
Methods: We used data from a single large UK Cancer Center to assess the demographic/clinical characteristics of 156 cancer patients with a confirmed COVID-19 diagnosis between 29 February and 12 May 2020. Logistic/Cox proportional hazards models were used to identify which demographic and/or clinical characteristics were associated with COVID-19 severity/death.
Results: 128 (82%) presented with mild/moderate COVID-19 and 28 (18%) with a severe case of the disease. An initial cancer diagnosis >24 months before COVID-19 [OR: 1.74 (95% CI: 0.71–4.26)], presenting with fever [6.21 (1.76–21.99)], dyspnea [2.60 (1.00–6.76)], gastro-intestinal symptoms [7.38 (2.71–20.16)], or higher levels of C-reactive protein [9.43 (0.73–121.12)] were linked with greater COVID-19 severity. During a median follow-up of 37 days, 34 patients had died of COVID-19 (22%). Being of Asian ethnicity [3.73 (1.28–10.91)], receiving palliative treatment [5.74 (1.15–28.79)], having an initial cancer diagnosis >24 months before [2.14 (1.04–4.44)], dyspnea [4.94 (1.99–12.25)], and increased CRP levels [10.35 (1.05–52.21)] were positively associated with COVID-19 death. An inverse association was observed with increased levels of albumin [0.04 (0.01–0.04)].
Conclusions: A longer-established diagnosis of cancer was associated with increased severity of infection as well as COVID-19 death, possibly reflecting the effects a more advanced malignant disease has on this infection. Asian ethnicity and palliative treatment were also associated with COVID-19 death in cancer patients.
In the context of cancer, the COVID-19 pandemic has led to a series of challenging decisions that must be made (1, 2). Patient visits to the cancer clinic increase the potential risk of infection when the alternative is self-isolation at home, and some cancer treatments may predispose patients to moderate or severe harmful effects of COVID-19 (3, 4). Current precautionary management decisions being made for cancer patients are based on assumptions supported by limited evidence, based on small case series from China and Italy (5–13) and larger series from New York (14, 15) and a recent consortium of 900 patients from over 85 hospitals in the USA, Canada, and Spain (16). As a result of their limited sample sizes, most studies were not able to distinguish between the effects of age, cancer, and other comorbidities on COVID-19 outcomes in this population (17, 18). Moreover, the case series from New York analyzed which patient characteristics are associated with COVID-19 death, but only made a comparison with non-cancer patients (14, 15). The first results of the COVID-19 and Cancer Consortium provide insights from a large cohort in terms of COVID-19 mortality, though a wide variety of institutions with different COVID-19 testing procedures were included (16). In addition, recently published prognostic studies in COVID-19 positive patients have been judged to be at high risk of bias, mainly due to non-representative selection of control patients, exclusion of patients who had not experienced the event of interest by the end of the study, high risk of model overfitting, and limited information on model building strategies used (19).
It can be difficult to confidently diagnose COVID-19 symptoms in cancer patients, as presenting features of the infection are often similar to cancer symptoms and treatment-related adverse events (17, 20). This may result in a delayed or missed COVID-19 diagnosis, which could lead to the confounding of cases and infection mortality rates, as well as late interventions for more life-threatening diseases (21). In addition, COVID-19 may be a barrier to dignified and humane end-of-life cancer care (17). Finally, the pandemic is causing huge service reconfiguration for both curative and palliative oncology care, resulting in fewer clinic visits due to social distancing (22), cessation of screening, and delays or changes in treatments that will inevitably have serious impacts on cancer-related mortality and morbidity (17, 21). Our recent systematic review reported there is currently no definitive evidence that specific cytotoxic drugs are contraindicated in cancer patients infected with COVID-19 (23).
Larger studies with multivariate models are urgently warranted to further explore this intersection of COVID-19 and cancer in terms of clinical outcomes, so as to inform oncological care during this outbreak and potential future pandemics (24). Guy's Cancer Center in South-East London, which treats ~8,800 patients annually, including 4,500 new diagnoses, is one of the largest Comprehensive Cancer Centers in the UK and is currently at the epicenter of the UK COVID-19 epidemic.
Guy's Cancer Cohort, a research ethics committee approved research database (Reference number: 18/NW/0297) of all routinely collected clinical data of cancer patients at Guy's and St Thomas' NHS Foundation Trust (GSTT), forms the basis of this observational study (25). The database contains routinely collected prospective and retrospective demographic/clinical data on all cancer patients treated at Guy's Cancer Center. We have an established clinical database for all cancer patients tested for COVID-19 either in outpatient clinics or ward settings since 29 February 2020. Using the unique hospital number, these databases were merged prior to anonymization for research purposes. We assessed outcomes included in the core outcome sets currently being developed for COVID-19 to ensure all relevant information is collected in our COVID specific database (26).
We have included cancer patients who received a diagnosis of COVID-19 from a positive PCR test from 29th February to 12th May 2020. Until 30 April 2020, a COVID-19 test was ordered for cancer patients if they presented with symptoms necessitating hospitalization or if they were scheduled to undergo a cancer-related treatment. From 1 May 2020, COVID-19 testing was introduced as a part of standard care, with about 25% of patients being swabbed daily depending on staff and testing kit availability. A total of 1,507 patients were tested between 29 February and 12 May 2020, of whom 156 had COVID-19 (10%).
In this analysis of our data, we had three aims:
1) To describe demographic and clinical characteristics of COVID-19 positive cancer patients, in terms of their COVID-19 and cancer diagnoses.
2) To identify which demographic and/or clinical factors were associated with COVID-19 severity in cancer patients.
3) To identify which demographic and/or clinical factors were associated with COVID-19 death in cancer patients.
Descriptive statistics were used to address the first aim. Most variables had several categories for the purpose of these descriptive analyses but were collapsed for the purpose of regression analyses due to the sample size of our cohort. Socio-economic status (low, middle, high) was determined based on the English Indices of Multiple Deprivation for postcodes (27). Lymphocyte count (×109) was categorized as ≤0.5, 0.6–0.8, 0.9–1.2, and >1.2 based on the Common Terminology Criteria for Adverse Events v.5 (CTCAE). For the other laboratory variables, we created tertiles instead of clinical cut-offs due to cancer patients already having abnormal values for most of these blood markers (Ferritin, C-reactive protein, and albumin). Radical treatment was defined as those patients with a chance of long-term survival or cure.
For the second aim, we conducted logistic regression analyses. Mild/moderate COVID-19 was defined as pneumonia with or without sepsis (i.e., those patients managed on the ward), whereas severe COVID-19 was defined as acute respiratory distress syndrome (ARDS) or septic shock (i.e., those patients where severity reached the criteria for Intensive Care Unit admission, if deemed clinically appropriate). These definitions were based on the WHO COVID-19 classification (28). The models used to quantify the association between each factor and COVID-19 severity were defined through a directed acyclic graph (DAG) (Figure A1). Each factor was individually set as the main exposure variable in the model in order to determine the minimal adjustments required for each factor (Table A1).
The third research aim was addressed with Cox proportional hazards regression analyses, whereby the models were defined as above (Table A1). Follow-up was defined from the date of COVID testing until death or 12 May 2020.
All statistical analyses were conducted with STATA version 15.1.
One hundred and twenty-eight patients (82%) presented with mild/moderate COVID-19 and 28 patients (18%) with severe COVID-19 (Table 1). More patients were male (58%) and aged 60+ (68%; median age: 67). However, 14% of the cancer population was aged <50 years (n = 21; median age: 41). When stratified by COVID grade, more male cancer patients presented with severe disease (68%). Most patients were from a lower socio-economic background (81%). With respect to ethnicity, about half were White, 22% were Black (n = 32), and 4% were of Asian (n = 6) origin. When stratified by COVID grade, a slightly larger proportion of patients from a white ethnic background had severe COVID (57%). Hypertension was the most reported comorbidity (47%), followed by diabetes mellitus (22%), renal impairment (19%), and cardiovascular disease (19%). However, benign lung conditions were more commonly reported for those who presented with severe COVID-19 (29 vs. 13% in those with mild COVID-19).
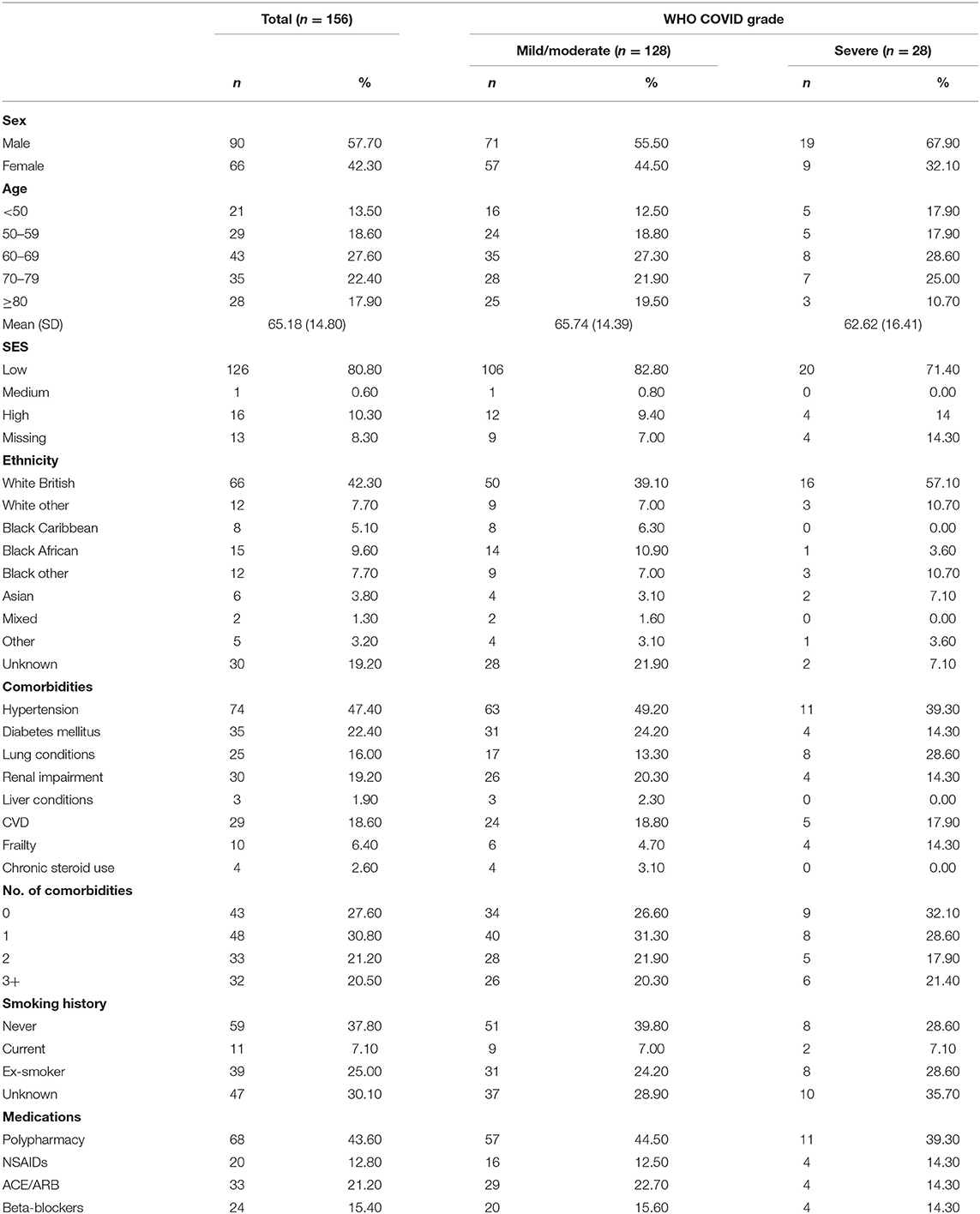
Table 1. Demographic characteristics of COVID-19 positive cancer patients.
The most frequently reported tumor types were urological/gynecological (29%), followed by hematological (18%) and breast (15%) (Table 2). The first group (n = 45) comprised of 21 prostate, 8 renal, 5 bladder, and 11 gynecological cancers. Of the 28 hematological malignancies, four (14.3%) were myeloid and 24 (85.7%) were lymphoid. Of all cancer patients tested for COVID-19, 80 were positive after their cancer-related hospital admission (51%), of which 61 were solid tumors (76%) and 19 were hematological cancers (24%). When stratified by COVID-19 severity, the largest proportion of cancers presenting with severe COVID were hematological (36%). A large proportion of patients had advanced cancer (40% stage IV) and were diagnosed with their malignancy in the last 12 months (46%).
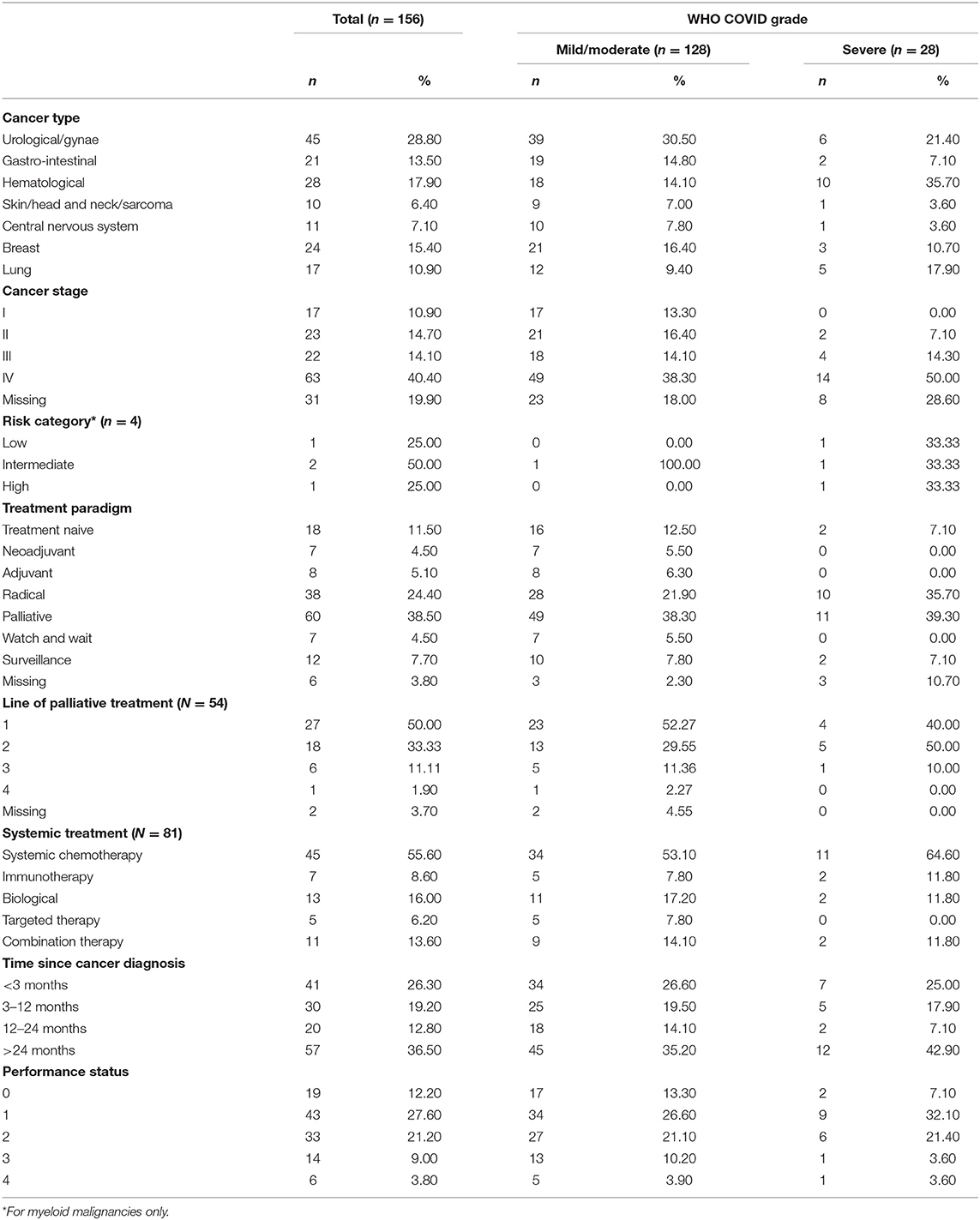
Table 2. Tumor characteristics of COVID-19 positive cancer patients.
Overall, 39% of patients were receiving palliative treatment, 25% were receiving radical treatment, and 12% were treatment naive. Treatment distributions were reasonably comparable between COVID-19 severity groups. Of the 81 patients on systemic treatment within the last 2 years, 54 were in a palliative setting; of these, 50% were 1st line, 33% 2nd line, and 13% on ≥3rd treatment line. However, the majority of severe COVID-19 patients were on third line metastatic treatment. Table 2 provides further details on the cancer characteristics.
Forty six percentage of the cancer patients diagnosed with COVID-19 in this cohort presented with a cough and 52% had a fever. Most patients were molecularly diagnosed within seven days of their initial symptoms (58%) (Table 3). More patients in the severe COVID-19 group presented with C-reactive protein (CRP) values in the highest tertile (46 vs. 22% for mild/moderate disease). Similarly, they had a lower lymphocyte count [43 vs. 21% in the lowest category (≤0.5)] and lower albumin levels (39 vs. 22% in the lowest tertile).
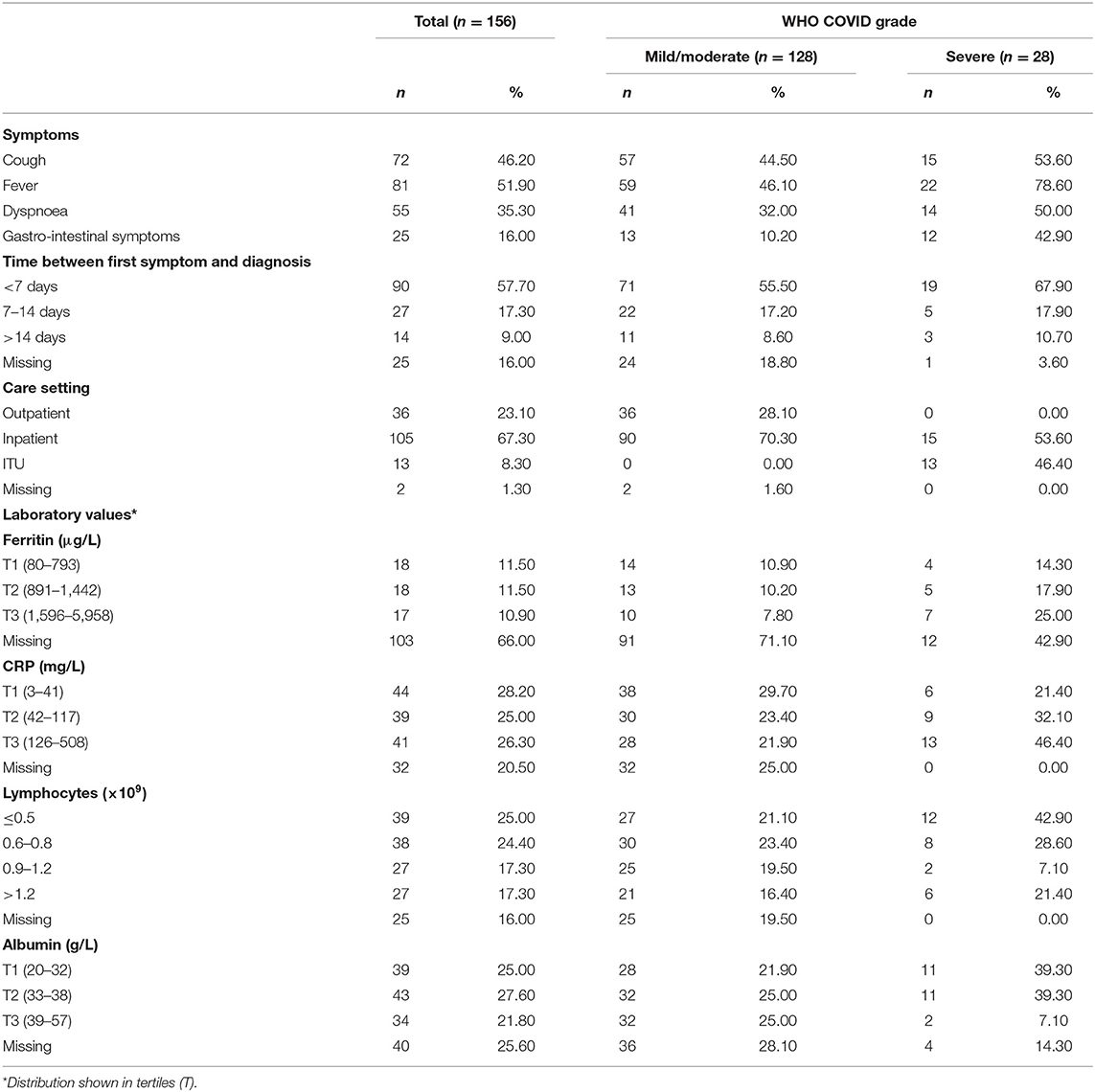
Table 3. COVID-19 presentation of COVID-19 positive cancer patients.
The odds ratios (ORs) for the associations between the various demographic and clinical factors and COVID-19 severity status are shown in Table 4. There was a non-statistically significant indication that those patients who were diagnosed with cancer more than 24 months ago were at a higher risk of presenting with severe COVID-19 as compared to those diagnosed during the last 24 months [OR: 1.74 (95% CI: 0.71–4.26)]. With respect to symptom presentation, those presenting with a fever, dyspnea, or gastro-intestinal symptoms were at a higher risk of having severe COVID-19 as compared to those without these symptoms [OR: 6.21 (1.76–21.99), 2.60 (1.00–6.76), and 7.38 (2.71–20.16), respectively].
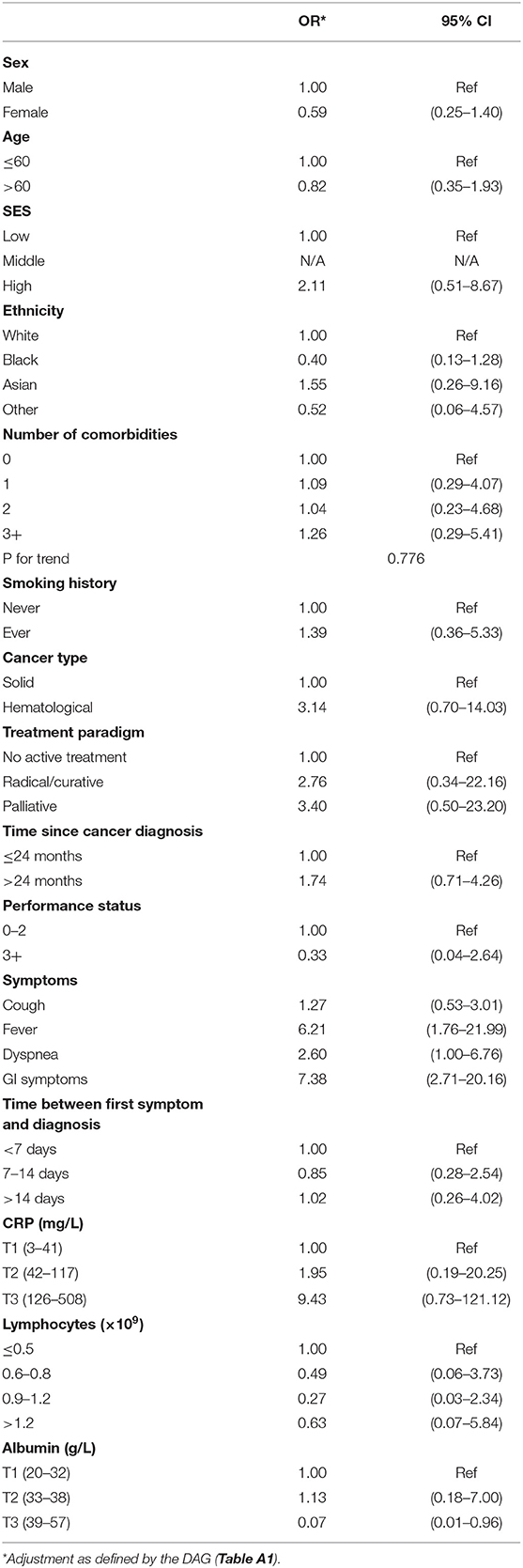
Table 4. Odds Ratios and 95% confidence intervals for COVID-19 severity in cancer patients.
During a median follow-up of 37 days (IQR: 18–49), 34 cancer patients had died of COVID-19 (22%) (Table 5). Several cancer patient characteristics were found to be positively associated with risk of COVID-19 death: being of Asian ethnicity [as compared to white—HR: 3.73 (95% CI: 1.28–10.91)], receiving palliative treatment [as compared to no active treatment—HR: 5.74 (95% CI: 1.15–28.79)], time since cancer diagnosis >24 months [as compared to ≤24 months—HR: 2.14 (95% CI: 1.04–4.44)], presenting with dyspnea [as compared to no dyspnea—HR: 4.94 (95% CI: 1.99–12.25)], and having high CRP levels [3rd tertile vs. 1st tertile—HR: 10.35 (95% CI: 1.05–52.21)]. In addition, an inverse association with death from COVID-19 was observed with normal albumin levels [3rd tertile vs. 1st tertile—HR: 0.04 (95% CI: 0.01–0.04)].
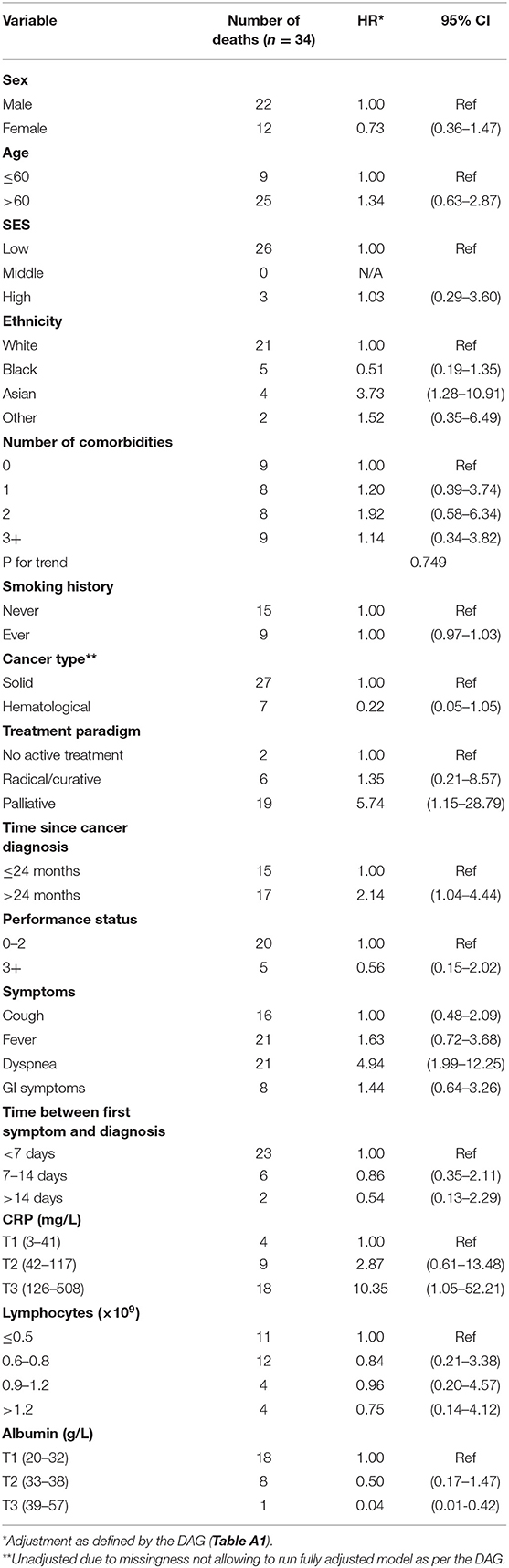
Table 5. Hazard Ratios and 95 %Confidence intervals for COVID-19 death in cancer patients.
Using multivariate modeling based on a directed acyclic graph, this study reports on a large cohort of COVID-19 positive cancer patients from a single institution. Low SES, hypertension, and diabetes were common in cancer patients with COVID-19. Age, sex, ethnicity, SES, and current cancer treatment were found to not be associated with severity of COVID-19 infection in cancer patients. However, receipt of a cancer diagnosis more than 24 months previously (as compared to within 24 months) and presenting with fever, dyspnea, or gastro-intestinal symptoms were linked with higher odds of developing severe illness as compared to mild/moderate COVID-19. Higher levels of CRP and ferritin were also associated with more severe COVID-19 disease in infected cancer patients. During a median follow-up of 37 days, the following cancer patient characteristics were found to be positively associated with COVID-19 death: Asian ethnicity, palliative treatment, initial cancer diagnosis >24 months, dyspnea at presentation, and high CRP levels. Normal serum albumin levels were inversely associated with death from COVID-19 in cancer patients.
Several retrospective cohort studies published using data from hospitals situated in Wuhan, China, Northern Italy, Canada, and the USA have reported on the clinical characteristics of COVID-19 positive cancer patients with sample sizes varying from 9 to 85, two slightly larger series of >200 patients, and a big data Consortium including over 85 institutions and 900 patients (5–12, 16). The median age reported in these studies was similar to our study, with a range from 63 to 72 years. A larger proportion of male patients has been observed. Lung cancer was the most commonly reported cancer in the Zhang et al. (5), Yu et al. (8), Yang et al. (10), and Stroppa et al. (11) studies, but only accounted for 11% in our patient population. Zhang et al. (5) estimated that in their cohort, 29% of patients tested positive for COVID-19 following hospital admission, whereas this was estimated at 51% in our cohort. Interpretation of this statistic is difficult given the latency between exposure and manifestations of infection, meaning patients diagnosed after admission may have been infected outside of the hospital. Several studies (6, 10) noted that hypertension, diabetes, and coronary heart disease were the most commonly reported comorbidities.
Our cancer cohort is similar in distribution of age, sex, and comorbidities to the case series reported to date. The ethnicity and SES of our COVID-19 positive cancer patients are most likely a reflection of the catchment area of our Cancer Center in South-East London (29), covering more deprived boroughs (Lambeth and Southwark). Based on the number of cancer patients treated at our Cancer Center in 2019, about 49% of patients are of a White ethnic background. Variations observed with the published data in terms of cancer type, stage, and treatment may be a reflection of clinical practice (e.g., intensity of treatment and frequency of hospital visits), of relative cancer incidence, or of extent of treatment changes introduced as mitigation in the face of the emerging pandemic. For example, the most recently reported age-standardized lung cancer incidence rates for males and females in Wuhan are 54.1 and 19.1 per 100,000, whereas these are estimated to be 37.5 and 24.3 per 100,000 in London (30). Early modification and prioritization of treatment was introduced at our center, in accordance with now-published guidance (31).
Comparably to our study, both the Zhang and the Du studies also reported fever, cough, shortness of breath, and dyspnea as common clinical features (5, 6). As in the Chinese cohort of 85 fatal cases, our severe COVID-19 patients had comparable laboratory findings: decreased lymphocytes, increased CRP, and decreased albumin (6).
Severe events were reported for 54% of the study population and mortality for 29% in the Zhang study, as compared to 18 and 22% in our cohort. Zhang et al. also reported that recent treatment within 14 days was associated with an increased risk of developing severe events (28 days) (5). This difference with our observations may be attributed to different definitions of severe events, as it was not entirely clear how these were defined by Zhang et al. As highlighted by Wynants et al. in their assessment of current statistical models published for COVID-19 (19), there is a need for consistent use of outcome definitions. However, our observations of a positive association with CRP levels is in line with most COVID-19 studies published to date (32). Apart from the CCC-19 Consortium (16), no study to date has specifically looked at COVID-19 severity at presentation in COVID-19 positive cancer patients and hence our observation of an association with time since cancer diagnosis and presenting symptoms needs further validation in other large cohorts with homogenous definitions of inclusion criteria, testing strategies, and outcome measures. However, it is possible that time since cancer diagnosis is also a reflection of the extent of the disease and progression along the palliative patient pathway from diagnosis to death.
The study by Yu et al. reported three deaths (25%) (8). In the larger series from New York, Mehta et al. reported an overall case fatality rate of 28%, with 37% for hematological malignancies and 25% for solid tumors (14). The CCC-19 Consortium reported a 30-day mortality rate due to COVID-19 of 13% (16). In our cohort, the overall case fatality rate was 22%, with 25% for hematological cancers and 21% for solid tumors. As more than 85 institutions were included in the CCC-19 Consortium (16), it is possible that differences in COVID-19 practice as well as cancer treatments between the numerous centers may explain the slightly lower death rate as compared to reports from single center studies. Moreover, our median follow-up is 37 days as compared to 21 days for the Consortium. The heterogeneity between centers may also explain why performance status was found to be associated with COVID-19 outcomes, an observation not identified in our single center cohort.
Our observations of Asian ethnicity being associated with increased mortality from COVID-19 in cancer patients is of interest, given the recent speculations about the disproportionate effects of COVID-19 on Black, Asian, and minority ethnic communities (33) as well as the confounding factor of vitamin D deficiency (34). However, longer follow-up studies are required to disentangle the association between ethnicity and COVID-19 death in cancer patients.
Whilst this is one of the largest single center COVID-19 positive cancer cohorts to date, our sample size is still relatively modest and hence confidence intervals for some statistically significant observations are still wide. No firm conclusions in terms of prognostic modeling can be drawn as of yet (19). Current analyses aimed to generate further hypotheses on patient or tumor characteristics indicative of severity or of death from COVID-19 in the context of cancer. Our data for some of the patient characteristics is limited; for example, smoking status was missing for 29% of patients and hence likely underestimates the proportion of smokers. COVID testing in the UK has only been implemented gradually during the period of our data collection, and there is selection bias in favor of patients being tested as inpatients. Our analysis is likely to have missed cancer outpatients under our care diagnosed with COVID-19 at other hospitals—however this is most likely to be an even more important issue for global Consortia with many hospitals only adding a few cases to the overall dataset.
In light of these differences in COVID-19 management and cancer treatments between centers, it is important to note that our hospital has a specialized highly infectious disease unit with extracorporeal membrane oxygenation (ECMO) facilities, which ensured very experienced critical care management of COVID patients. A standard clinical approach was used, with concurrent antibiotics to cover bacterial infection and early escalation of treatment decisions, including appropriateness of ITU admission. No standard use of other agents (steroids or antivirals) was applied unless within the context of a clinical trial. Moreover, our general oncological approach was to maintain standard anti-cancer treatment (including surgery, radiotherapy, and systemic treatments) where it was safe and reasonable to do so. Our Cancer Center managed to continue oncology services throughout the COVID pandemic, whereas other Centers may have redeployed staff that precluded this.
It is also a strength of our study that we used clearly defined definitions of COVID-19 severity, as well as a DAG to develop the different models, as to date very limited knowledge is available regarding the intersection between COVID-19 and cancer (19). Detailed information on our modeling will help comparison with future studies with larger sample sizes and longer follow-ups.
Our analysis of one of the largest single center series of COVID-19 positive cancer patients to date confirms a similar distribution of age, sex, and comorbidities as reported for other populations. Reflecting the general population, presenting with fever, dyspnea, gastro-intestinal symptoms, higher levels of CRP, or ferritin were also indicators of COVID-19 severity in the cancer population. Similarly, we noted that dyspnea at presentation, high CRP levels, and low levels of albumin were associated with death from COVID-19. With respect to cancer specific observations, patients who have lived longer with their cancer were found to be more susceptible to a greater infection severity, possibly reflecting the effect of a more advanced malignant disease-as almost half of the severe cohort were on third line metastatic treatment-or the impact of this infection. The latter was also found to be associated with COVID-19 death in cancer patients, as were being of Asian ethnicity and receiving palliative treatment. Further validation will be provided from other large case series, as well as from those including longer follow-ups, to provide more definite guidance for oncological care.
Data can be obtained by researchers via an application to the Access Committee of Guy's Cancer Cohort. An application form can be obtained via Charlotte Moss, Y2hhcmxvdHRlLm1vc3NAa2NsLmFjLnVr.
Guy's Cancer Cohort, a research ethics committee approved research database (Reference Number: 18/NW/0297) of all routinely collected clinical data of cancer patients at Guy's and St Thomas' NHS Foundation Trust (GSTT), forms the basis of this observational study.
BR, CM, PR, DC, HW, FC, AH, KZ, FR, AS-L, DJ, SD, ML, SGh, ES, AD'S, SGo, DE, PF, DW, KR, MG, KB, RD, MS, and AS: data collection. BR, CM, SP, SI, PR, JS, SD, and MVH: study design. BR, CM, MVH, and SD: data analysis. MVH, BR, CM, SD, SP, RS, PR, JS, SK, and CH: manuscript drafting. All authors: final approval of manuscript.
This research was supported by the National Institute for Health Research (NIHR) Biomedical Research Centre (BRC) based at Guy's and St Thomas' NHS Foundation Trust and King's College London (IS-BRC-1215-20006). The authors are solely responsible for study design, data collection, analysis, decision to publish, and preparation of the manuscript. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. We also acknowledge support from Cancer Research UK King's Health Partners Centre at King's College London and Guy's and St Thomas' NHS Foundation Trust Charity Cancer Fund.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We are grateful to Graham Roberts for providing us with the descriptive statistics of the cancer patients treated at our Cancer Centre. This article has been released as a preprint at medRxiv (35).
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2020.01279/full#supplementary-material
1. Ueda M, Martins R, Hendrie PC, McDonnell T, Crews JR, Wong TL, et al. Managing cancer care during the COVID-19 pandemic: agility and collaboration toward a common goal. J Natl Compr Canc Netw. (2020) 18:1–4. doi: 10.6004/jnccn.2020.7560
2. Robinson AG, Gyawali B, Evans G. COVID-19 and cancer: do we really know what we think we know? Nat Rev Clin Oncol. (2020) 17:386–8. doi: 10.1038/s41571-020-0394-y
3. Hanna TP, Evans GA, Booth CM. Cancer, COVID-19 and the precautionary principle: prioritizing treatment during a global pandemic. Nat Rev Clin Oncol. (2020) 17:268–70. doi: 10.1038/s41571-020-0362-6
4. Sidaway P. COVID-19 and cancer: what we know so far. Nat Rev Clin Oncol. (2020) 17:336. doi: 10.1038/s41571-020-0366-2
5. Zhang L, Zhu F, Xie L, Wang C, Wang J, Chen R, et al. Clinical characteristics of COVID-19-infected cancer patients: a retrospective case study in three hospitals within Wuhan, China. Ann Oncol. (2020) 31:894–901. doi: 10.1016/j.annonc.2020.03.296
6. Du Y, Tu L, Zhu P, Mu M, Wang R, Yang P, et al. Clinical features of 85 fatal cases of COVID-19 from Wuhan: a retrospective observational study. Am J Respir Crit Care Med. (2020) 201:1372–9. doi: 10.2139/ssrn.3546088
7. Desai A, Sachdeva S, Parekh T, Desai R. COVID-19 and cancer: lessons from a pooled meta-analysis. JCO Glob Oncol. (2020) 6:557–9. doi: 10.1200/GO.20.00097
8. Yu J, Ouyang W, Chua MLK, Xie C. SARS-CoV-2 transmission in patients with cancer at a tertiary care hospital in Wuhan, China. JAMA Oncol. (2020) e200980. doi: 10.1001/jamaoncol.2020.0980. [Epub ahead of print].
9. Liang W, Guan W, Chen R, Wang W, Li J, Xu K, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. (2020) 21:335–7. doi: 10.1016/S1470-2045(20)30096-6
10. Yang F, Shi S, Zhu J, Shi J, Dai K, Chen X. Clinical characteristics and outcomes of cancer patients with COVID-19. J Med Virol. (2020). doi: 10.1002/jmv.25972. [Epub ahead of print].
11. Stroppa EM, Toscani I, Citterio C, Anselmi E, Zaffignani E, Codeluppi M, et al. Coronavirus disease-2019 in cancer patients. a report of the first 25 cancer patients in a western country (Italy). Future Oncol. (2020). doi: 10.2217/fon-2020-0369. [Epub ahead of print].
12. Trapani D, Marra A, Curigliano G. The experience on coronavirus disease 2019 and cancer from an oncology hub institution in Milan, Lombardy Region. Eur J Cancer. (2020) 132:199–206. doi: 10.1016/j.ejca.2020.04.017
13. Ma J, Yin J, Qian Y, Wu Y. Clinical characteristics and prognosis in cancer patients with COVID-19: a single center's retrospective study. J Infect. (2020). doi: 10.1016/j.jinf.2020.04.006. [Epub ahead of print].
14. Mehta V, Goel S, Kabarriti R, Cole D, Goldfinger M, Acuna-Villaorduna A, et al. Case fatality rate of cancer patients with COVID-19 in a New York hospital system. Cancer Discov. (2020). doi: 10.1158/2159-8290.CD-20-0516. [Epub ahead of print].
15. Miyashita H, Mikami T, Chopra N, Yamada T, Chernyavsky S, Rizk D, et al. Do patients with cancer have a poorer prognosis of COVID-19? an experience in New York City. Ann Oncol. (2020). doi: 10.1016/j.annonc.2020.04.006. [Epub ahead of print].
16. Kuderer N, Choueiri TK, Shah DP, Shyr Y, Rubinstein SM, Rivera DR, et al. Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study. Lancet. (2020) 395:1907–18. doi: 10.1016/S0140-6736(20)31187-9
17. Spicer J, Chamberlain C, Papa S. Provision of cancer care during the COVID-19 pandemice. Nat Rev Clin Oncol. (2020) 17:329–31. doi: 10.1038/s41571-020-0370-6
18. Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. (2020). doi: 10.1001/jama.2020.4683. [Epub ahead of print].
19. Wynants L, Van Calster B, Bonten MMJ, Collins GS, Debray TPA, De Vos M, et al. Prediction models for diagnosis and prognosis of covid-19 infection: systematic review and critical appraisal. BMJ. (2020) 369:m1328. doi: 10.1101/2020.03.24.20041020
20. Russell B, Moss C, Rigg A, Hopkins C, Papa S, van Hemelrijck M. Anosmia and ageusia are emerging as symptoms in patients with COVID-19: what does the current evidence say? Ecancermedicalscience. (2020) 14:ed98. doi: 10.3332/ecancer.2020.ed98
21. Schrag D, Hershman DL, Basch E. Oncology practice during the covid-19 pandemic. JAMA. (2020). doi: 10.1001/jama.2020.6236. [Epub ahead of print].
22. Cancer care goes virtual in response to COVID-19. Cancer Discov. (2020) 10:755. doi: 10.1158/2159-8290.CD-NB2020-027
23. Russell B, Moss C, George G, Santaolalla A, Cope A, Papa S, et al. Associations between immune-suppressive and stimulating drugs and novel Covid-19 – a systematic review of current evidence. Ecancer. (2020) 14:1022. doi: 10.3332/ecancer.2020.1022
24. Al-Shamsi HO, Alhazzani W, Alhuraiji A, Coomes EA, Chemaly RF, Almuhanna M, et al. A practical approach to the management of cancer patients during the novel coronavirus disease 2019. (COVID-19) pandemic: an international collaborative group. Oncologist. (2020) 25:e936–45. doi: 10.1634/theoncologist.2020-0213
25. Moss C, Haire A, Cahill F, Enting D, Hughes S, Smith D, et al. Guy's cancer cohort - real world evidence for cancer pathways. BMC Cancer. (2020) 20:187. doi: 10.1186/s12885-020-6667-0
26. COMET Initiative. Core Outcome Set Development for COVID-19. (2020). Available online at: http://www.comet-initiative.org/Studies/Details/1538
27. Office of National Statistics. English Indices of Deprivation. (2020). Available online at: https://www.gov.uk/government/statistics/english-indices-of-deprivatio-2010 (accessed November 25, 2016).
28. World Health Organisation. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is Suspected. Geneva. (2020).
30. International Agencey for Research on Cancer. CI5 X: Cancer Incidence in Five Continents Volume XI. (2020). Available online at: https://ci5.iarc.fr/Default.aspx
31. National Institute of Health and Care Excellence. COVID-19 Rapid Guideline: Delivery of Systemic Anticancer Treatments. (2020). Available online at: www.nice.org.uk/guidance/ng161
32. Kermali M, Khalsa RK, Pillai K, Ismail Z, Harky A. The role of biomarkers in diagnosis of COVID-19 - A systematic review. Life Sci. (2020) 254:117788. doi: 10.1016/j.lfs.2020.117788
33. Kirby T. Evidence mounts on the disproportionate effect of COVID-19 on ethnic minorities. Lancet Respir Med. (2020). doi: 10.1016/S2213-2600(20)30228-9. [Epub ahead of print].
34. Mitchell F. Vitamin-D and COVID-19: do deficient risk a poorer outcome? Lancet Diabetes Endocrinol. (2020). doi: 10.1016/S2213-8587(20)30183-2. [Epub ahead of print].
Keywords: COVID-19, cancer, SARS-CoV-2, outcomes, directed acyclic graph
Citation: Russell B, Moss C, Papa S, Irshad S, Ross P, Spicer J, Kordasti S, Crawley D, Wylie H, Cahill F, Haire A, Zaki K, Rahman F, Sita-Lumsden A, Josephs D, Enting D, Lei M, Ghosh S, Harrison C, Swampillai A, Sawyer E, D'Souza A, Gomberg S, Fields P, Wrench D, Raj K, Gleeson M, Bailey K, Dillon R, Streetly M, Rigg A, Sullivan R, Dolly S and Van Hemelrijck M (2020) Factors Affecting COVID-19 Outcomes in Cancer Patients: A First Report From Guy's Cancer Center in London. Front. Oncol. 10:1279. doi: 10.3389/fonc.2020.01279
Received: 01 June 2020; Accepted: 19 June 2020;
Published: 22 July 2020.
Edited by:
Thierry Olivier Philip, Institut Curie, FranceReviewed by:
Abdelbaset Mohamed Elasbali, Al Jouf University, Saudi ArabiaCopyright © 2020 Russell, Moss, Papa, Irshad, Ross, Spicer, Kordasti, Crawley, Wylie, Cahill, Haire, Zaki, Rahman, Sita-Lumsden, Josephs, Enting, Lei, Ghosh, Harrison, Swampillai, Sawyer, D'Souza, Gomberg, Fields, Wrench, Raj, Gleeson, Bailey, Dillon, Streetly, Rigg, Sullivan, Dolly and Van Hemelrijck. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mieke Van Hemelrijck, bWlla2UudmFuaGVtZWxyaWpja0BrY2wuYWMudWs=
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.