
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol. , 14 July 2020
Sec. Hematologic Malignancies
Volume 10 - 2020 | https://doi.org/10.3389/fonc.2020.01133
This article is part of the Research Topic Cutaneous B-cell Lymphomas View all 6 articles
 Alessandro Di Stefani1,2
Alessandro Di Stefani1,2 Luca Tagliaferri3
Luca Tagliaferri3 Valentina Lancellotta3*†
Valentina Lancellotta3*† Bruno Fionda3Barbara Fossati1,2Mario Balducci3Francesco Federico4,5Stefan Hohaus6,7
Bruno Fionda3Barbara Fossati1,2Mario Balducci3Francesco Federico4,5Stefan Hohaus6,7 Clara De Simone1,2Maria Antonietta Gambacorta2,8Ketty Peris1,2
Clara De Simone1,2Maria Antonietta Gambacorta2,8Ketty Peris1,2Primary cutaneous B-cell lymphomas (PCBCL) are rare types of extranodal non-Hodgkin's lymphoma. The choice of treatment usually depends on the variant of PCBCL, number, size, and location of the lesions, involved body surface area as well as patient's age and health condition. The efficacy of radiotherapy (RT) in the treatment of PCBCL has been widely reported conversely, data about the acute and late skin toxicity, patient's treatment satisfaction and quality of life are scarce. A systematic search using PubMed, Scopus, and Cochrane library was performed to identify full original articles analyzing the safety of RT in patients with PCBCL with the primary outcome to assess the acute and late skin toxicity. Secondary outcomes were complete remission, disease free survival, and overall survival. The literature search resulted in 276 articles including eight studies assessing the safety of RT for the treatment of PCBCL. Most patients (median 73%, range 11.9–99.9%) were recorded as having acute skin toxicity of grade 1–2, while acute grade 3–4 toxicity occurred in a median of 8% (range 4–23%) of patients. A median of 20% (range 4–54%) of patients had late skin toxicity of grade 1–2. No late grade 3–4 toxicity was reported. Only one study evaluated patient's satisfaction showing that the 97% of patients were satisfied with radiation therapy. This systematic review confirms the safety of RT in the treatment of PCBCL. Patients with a PCBCL should be managed in highly specialized centers in the context of a multidisciplinary team including dermatologist, hematologist, pathologist, and radiation oncologist.
Primary cutaneous B-cell lymphomas (PCBCL) are rare clinical and histopathological subtypes of extranodal non-Hodgkin's lymphoma (1). The fourth edition of the World Health Organization (WHO) classification system of hematopoietic and lymphoid tumors defined three major PCBCL categories, including: (i) primary cutaneous marginal zone lymphoma (PCMZL), (ii) primary cutaneous follicle center lymphoma (PCFCL), and (iii) primary cutaneous diffuse large B cell lymphoma, leg type (PCDLBCL, LT) (2). The term “PCLBCL, other” or “non otherwise specified” (NOS) encompasses all rare cases of PCBCL not adaptable in the histopathological criteria of the above-mentioned PCLBCL (3). PCBCL have an indolent clinical course in the majority of cases, with 5-year survival rates between 90 and 100% for PCMZL and PCFCL, which are also the most frequent (4–6). Instead, PCDLBCL, LT has a worse prognosis, with 5-year survival rates lower than 50% (4–6). Exclusion of systemic disease is of outermost importance, as PCBCL have a completely different clinical behavior, prognosis, and treatment approach compared with lymphomas characterized by nodal and visceral involvement (4–7). Treatment approaches for PCBCL include surgical excision, radiotherapy (RT), rituximab, and systemic chemotherapy (4–11). As no randomized controlled trials have been performed, treatment recommendations for PCBCL were based on small retrospective studies and single center experiences. To overcome this problem, the European Organization for Research and Treatment of Cancer (EORTC) and International Society for Cutaneous Lymphomas (ISCL), the European Society for Medical Oncology and the International Lymphoma Radiation Oncology Group (ESMO-ILROG) have published consensus treatment recommendations (5, 6, 11). In most cases, optimal patient management requires a multidisciplinary approach, including dermatologists, hematologists, pathologists, and radiation oncologists. RT is considered the most effective treatment for unilesional or localized lesions, with high local control rates and favorable outcome (7–10). Recurrence rates after RT range from 25 to 63% though these data do not differentiate unilesional from multilesional PCBCL (8, 10) and clinical predictive factors for relapse are not yet available.
While the efficacy of RT in the treatment of PCBCL has been widely reported in literature, the acute and late toxicity as well as patient's satisfaction of treatment remained poorly analyzed. Because PCZML and PCFCL are two indolent lymphoproliferative diseases characterized by a good prognosis, it is essential to ensure patient's quality of life and good cosmetic results along with clinical outcome. The present systematic review was performed to primarily assess the safety of RT as treatment of PCBCL.
A systematic search using PubMed, Scopus, and Cochrane library was performed to identify full original articles analyzing the safety of RT in patients with PCBCL. ClinicalTrials.gov was searched for ongoing or recently completed trials, and PROSPERO was searched for ongoing or recently completed systematic reviews. The studies were identified through the following medical subject headings (MeSH) and keywords including “primary cutaneous B cell lymphoma” and “radiotherapy.” The search was restricted to the English language. The Medline search strategy was: “radiotherapy” [Mesh] OR “radiotherapy” [All Fields] AND “primary cutaneous B cell lymphoma” [All Fields]. To avoid missing relevant studies we chose this strategy with high sensitivity but low specificity. We analyzed only clinical full-text studies of PCBCL patients treated with RT. Conference papers, surveys, letters, editorials, book chapters, and reviews were excluded. The time of publication was restricted to the period between 1990 and 2018. Two independent radiation oncologists expert in RT (VL, BRF) screened citations in the titles and abstracts to identify appropriate papers. Eligible citations were retrieved for full-text review. Uncertainties about article inclusion in the review were controlled by an expert multidisciplinary team composed by a radiation oncologist expert in hematological malignancies (MB), a hematologist expert in lymphoproliferative diseases (SH), a pathologist expert in dermatopathology (FF), a dermatologist expert in dermato-surgery (BAF), and a dermatologist expert in skin lymphomas (CDS). Finally, an expert multidisciplinary committee (ADS, LT, MAG, and KP) performed an independent check and the definitive approval of the review.
The primary outcome of our systematic review was the acute and late toxicity. Secondary outcomes included complete remission, disease-free survival, and overall survival. A summary table was created including mono/multicentric studies, sample size, median age, acute and late toxicity, complete remission (CR), disease-free survival (DFS), and overall survival (OS) (Table 1).
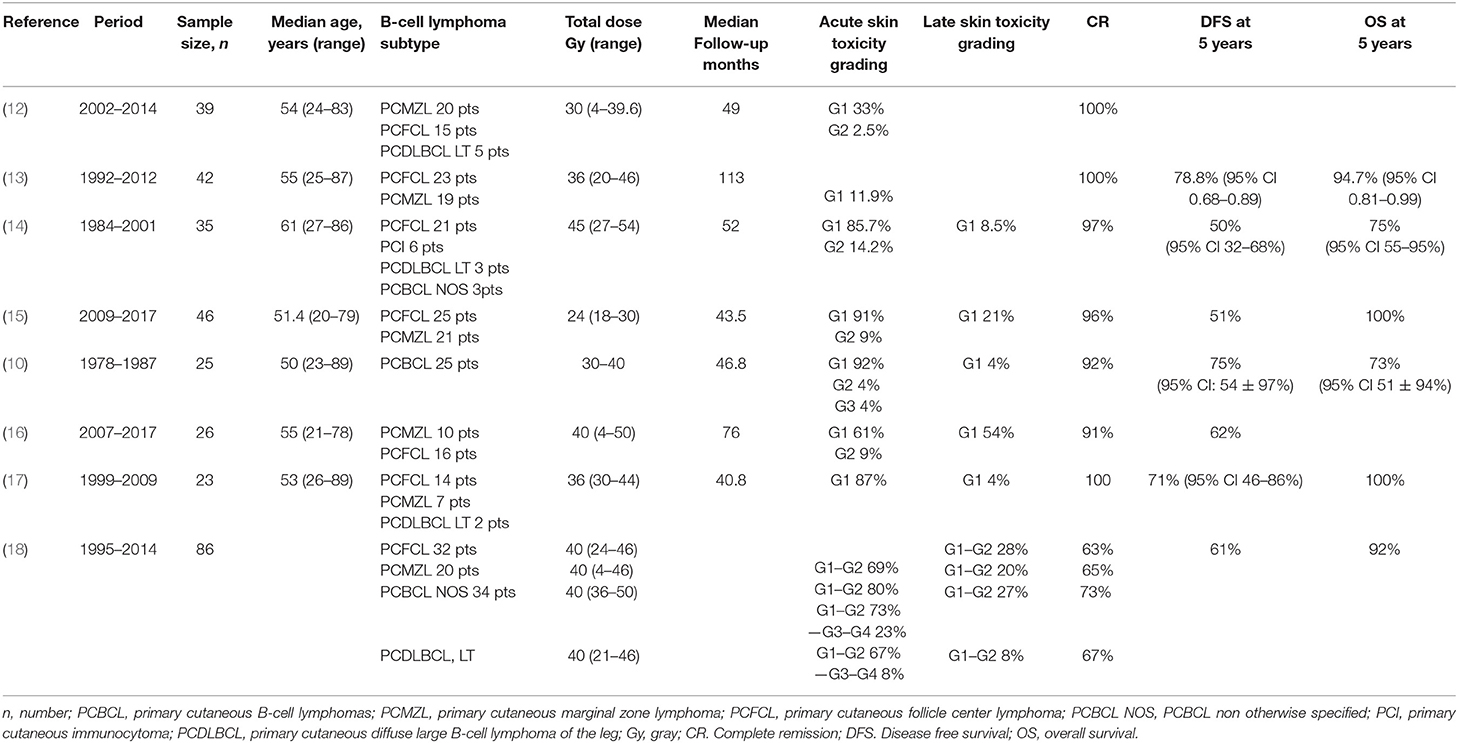
Table 1. Characteristics of the studies included in the systematic review.
The literature search resulted in 276 articles. After exclusion on the basis of the title and abstract, and exclusion of conference papers, surveys, letters, editorials, book chapters, reviews, and language other than English, 19 papers were assessed via full text for eligibility. Of these, 11 articles were excluded because of insufficient data, while eight studies were considered adequate to evaluate the safety of RT for the treatment of PCBCL (Figure 1). All studies were retrospective (10, 12–18). In accordance with the selection criteria, only data from the RT toxicity arms were extracted and considered for the analysis. Table 1 lists the characteristics of the studies included in our review. We identified 322 patients (median age: 54 years), 97 of whom were affected by PCZML, 146 by PCFCL, 44 by PCDLBCL, LT, and 35 were PCBCL non otherwise specified (NOS). All patients underwent external beam RT. Multiagent systemic treatment was reported in five of the eight studies. The median proportion of patients treated with chemotherapy before RT was 21% (range 12–52%). Surgery was performed in 15 patients (4.6%). External beam RT was delivered with a median total dose of 36 Gy (range 4–54 Gy). The median follow-up was 49 months (range 40.8–113 months).
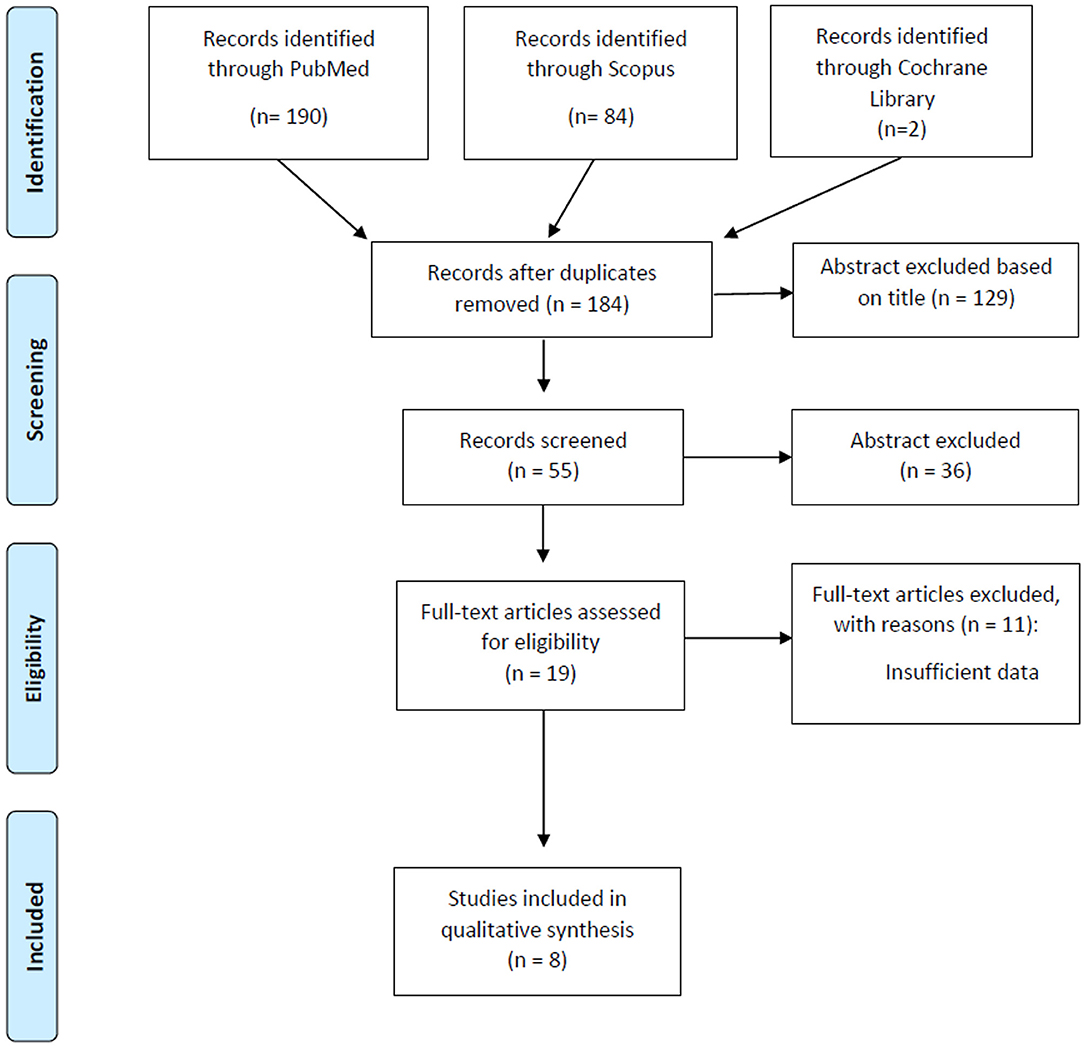
Figure 1. PRISMA flow-chart for outcome and late adverse effects.
Most patients (median 73%, range 11.9–99.9%) were recorded as having acute skin toxicity of grade 1–2 (consisting in erythema, xerosis, and itching), while acute skin toxicity of grade 3–4 occurred in a median of 8% (range 4–23%) of patients (consisting in exudative dermatitis, erosions, and skin necrosis). A median of 20% (range 4–54%) of patients experienced late grade 1–2 skin toxicity (consisting in mild pigmentation changes, atrophy, telangiectasis, and hair loss in the irradiation field). No late grade 3–4 toxicity was observed. A single study compared conventional-dose RT to low-dose RT in terms of acute toxicities showing a lower incidence of grade 1 and grade 2 in de-escalated RT approach (70 vs. 14% grade 1; 8 vs. 0% grade 2; p = 0.004) (16).
Just one study reported patient's satisfaction of cosmetic results by an oral standardized questionnaire showing that 35/36 patients answered to be satisfied by radiation therapy; the only patient resulted unsatisfied due to acute toxicity and late sequelae (15).
The median CR rate following RT was 92% (range 63–100%). Relapse occurred in 34.7% of patients (29.5% outside the radiation field and 5.2% in field). DFS at 5 years was 62% (range 50–78.8%) and the OS at 5 years was 93.5% (range 73–100%).
The efficacy of RT in the treatment of PCBCL has been widely reported in literature, however, the safety as well as patient's satisfaction remained poorly analyzed. The main aim of our systematic review was to evaluate the acute and late toxicity of RT in the treatment of PCBCL. The present systematic review shows the safety of RT with the most common toxicity being grade 1–2 acute skin toxicity.
Several therapeutic modalities are available for PCBCL and consensus treatment recommendations usually depends basically on the type of PCBCL, the size, and location of the lesions In patients with solitary or localized lesions of PCDLBCL, LT, or PCLBCL NOS, the first line treatment is the R-CHOP (rituximab, cyclophosphamide, adriamycin, vincristine, and prednisone) regimen, followed by local RT. If the patient does not tolerate chemotherapy, RT alone or RT combined with rituximab may be used (11, 15–18). In PCMCL and PCFCL patients with solitary skin lesions, low-dose radiation therapy is safe and effective, with a complete remission rate approaching 100% (19–22). Radiation therapy does not appear to be inferior to multiagent chemotherapy also in patients with multiple lesions and no differences in relapse rate and long-term DFS were reported between patients treated with surgery or RT (21–23).
The indolent clinical behavior of PCMZL and PCFCL along with the rarity of extracutaneous relapses make local radiation a valid treatment option, nevertheless in clinical practice the management continues to include local surgical resection or systemic chemotherapy (4). Many studies showed that cancer specific survival for PCMZL and PCFCL is close to 100%, and DFS for solitary lesions is 77% indicating that too aggressive treatments are not necessary (24). Sometime, treatment choice is based not only on patient- and disease-related factors but is also influenced in the single center by issues related to equipment availability and institutional-based experiences (25). RT of PCBCL is a highly individualized treatment and has been demonstrated to be extremely effective in all subtypes. Since the decision of the dose and field size is highly dependent on the histologic subtype and extent of the skin involvement as well as on previous treatments, the type of RT technique plays a crucial role in achieving optimal outcome. Most frequently applied local RT method is the use of multiple energies of electron beams (26). However, there are also technical issues influencing the choice of the preferred RT technique. External beam radiation represents the most common application but in selected cases interventional RT, also called brachytherapy, in form of an individual surface mold, could be a better solution. The major differences between these two RT technologies are based on technical and physical details of the optimal application of the right dose to the right target. From a physical point of view, the homogenous irradiation of highly irregular clinical targets on the surface of the body, like hand, fingers, foot, or full face is not always possible with electron/photons beams, but well applicable with individual surface molds. From a technical point of view, optimal target coverage and highly conformal dose distribution are applicable without numerous field matchings or complex bolus applications. The use of the potential of individual dose intensity modulation by the stepping source technology combined with individual CT-based dose-volume optimization results in excellent dosimetric coverage of complex superficial targets, also in large and individually shaped volumes (27, 28).
Surface mold brachytherapy is rarely reported in the treatment of cutaneous lymphomas, however, the successful use of this technology is common and frequently reported in the treatment of other cutaneous tumors such as non-melanoma skin cancers (29–41). Interventional RT may be proposed as the treatment of choice for elderly patients with poor performance status and/or severe co-morbidities, due to its relatively short total treatment time. Interventional RT avoids the difficulties associated with age-related loss of mobility, patient positioning, and set-up procedures (42, 43). Although most of the recently published review papers advise to apply local RT for PCBCL, none of them discusses the application of surface molds (5, 6, 11).
Patients with PCBCL have an excellent OS, therefore the preservation of quality of life and the reduction of toxicity should be the main treatment goals, and should be also considered as outcome measures in clinical trials comparing treatment modalities. Few studies analyzed the acute and late skin toxicity after RT. Our systematic review showed that RT is safe in the treatment of PCBCL: although acute skin toxicity occurred in the great majority of the patients, it was mild, rarely exceeding grade 1–2, and consisted mostly in erythema, dry skin, and pruritus. As well, grade 1–2 late skin toxicity was observed in about 20% of patients essentially in the form of dyschromia, more rarely atrophy, telangiectasis, and alopecia in the irradiation field. The type of skin toxicities resulted consistent in all included studies. Moreover, no cases of secondary skin cancers in the radiation field were reported. Literature data reported a wide variation in toxicity rates and a correct interpretation is further complicated by the various clinical scoring criteria used in different studies like radiation therapy oncology group (RTOG) or common terminology criteria for adverse events (CTCAE). Moreover, no studies explored the correlation between RT toxicity rate and previous treatments, probably due to the low proportion of patients treated by chemotherapy and/or surgery before RT. Finally, only one study out of eight analyzed the association of RT total dose with the incidence and severity of skin toxicity highlighting a reduced rate in the low-dose RT (16). Remarkably, effective local control has been achieved even with doses as low as 4 Gy, especially in indolent PCBCL (12).
Patient's satisfaction with treatment results is still a rarely analyzed endpoint in PCBCL. A single study evaluated patient's opinion about cosmetic result of RT showing that in almost the totality of patients skin tolerance of RT was considered satisfactory for the excellent long-term cosmetic outcome. The only patient who was unsatisfied, indeed complained of acute toxicity and late sequelae (15).
The paucity of studies on this topic highlights the importance of a multidisciplinary team including dermatologist, hematologist, pathologist, surgeon as well as radiation oncologist, and interventional radiotherapist for a more individualized management of PCBCL patients (44). The pivotal role of a multidisciplinary setting was recently evidenced in a study on patients with esophageal cancer demonstrating the independent influence of the hospital of diagnosis on the probability to receive curative treatment (45). It is important to increase awareness regarding PCBCL treatment, particularly emphasizing the favorable clinical course and excellent cosmetic outcomes after interventional RT, in order to reduce the risk of overtreatment with high doses of RT or systemic chemotherapy. The possibility to identify one subgroup of PCBCL (i.e., PCMZL and PCFCL) with indolent behavior should be used for the selection of patients eligible to interventional RT ensuring safe treatment and better quality of life. A combined analysis of treatment results from different centers is highly needed in order to create predictive models (43, 46–56).
In conclusion, this systematic review confirms the safety of RT in the treatment of PCBCL with an excellent long-term cosmetic result for almost all patients associated with high patient's satisfaction and good quality of life. Patients with a PCBCL should be managed in centers where a close collaboration between dermatologists, hematologists, pathologists, and radiation oncologists exists.
All datasets analyzed for this study are included in the article/supplementary material.
Conception and design: AD, LT, MG, and KP. Data collection: VL, BFo, CD, BFi, FF, SH, and MB. Manuscript writing: AS, VL, and LT. Analysis and interpretation of data: AS, LT, MG, and KP. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Tadiotto Cicogna G, Ferranti M, Lazzarotto A, Alaibac M. Biological approaches to aggressive cutaneous B-cell lymphomas. Front Oncol. (2019) 9:1238. doi: 10.3389/fonc.2019.01238
2. Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. (2016) 127:2375–90. doi: 10.1182/blood-2016-01-643569
3. Selva R, Violetti SA, Delfino C, Grandi V, Cicchelli S, Tomasini C, et al. A literature revision in primary cutaneous B-cell lymphoma. Indian J Dermatol. (2017) 62:146–57. doi: 10.4103/ijd.IJD_74_17
4. Wilcox RA. Cutaneous B-cell lymphomas: 2019 update on diagnosis, risk stratification, and management. Am J Hematol. (2018) 93:1427–30. doi: 10.1002/ajh.25224
5. Willemze R, Hodak E, Zinzani PL, Specht L, Ladetto M. ESMO guidelines committee. primary cutaneous lymphomas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2018) 29:30–40. doi: 10.1093/annonc/mdy133
6. Specht L, Dabaja B, Illidge T, Wilson LD, Hoppe RT, International Lymphoma Radiation Oncology Group. Modern radiation therapy for primary cutaneous lymphomas: field and dose guidelines from the International Lymphoma Radiation Oncology Group. Int J Radiat Oncol Biol Phys. (2015) 92:32–9. doi: 10.1016/j.ijrobp.2015.01.008
7. Lima M. Cutaneous primary B-cell lymphomas: from diagnosis to treatment. An Bras Dermatol. (2015) 90:687–706. doi: 10.1590/abd1806-4841.20153638
8. Senff NJ, Hoefnagel JJ, Neelis KJ, Vermeer MH, Noordijk EM, Willemze R, Dutch Cutaneous Lymphoma Group. Results of radiotherapy in 153 primary cutaneous B-cell lymphomas classified according to the WHO-EORTC classification. Arch Dermatol. (2007) 143:1520–6. doi: 10.1001/archderm.143.12.1520
9. Willemze R. Primary cutaneous B-cell lymphoma: classification and treatment. Curr Opin Oncol. (2006) 18:425–31. doi: 10.1097/01.cco.0000239879.31463.42
10. Kirova Y, Piedbois Y, Le Bourgeois JP. Radiotherapy in the management of cutaneous B-cell lymphoma. Our experience in 25 cases. Radiother Oncol. (1999) 52:15–8. doi: 10.1016/S0167-8140(99)00089-4
11. Senff NJ, Noordijk EM, Kim YH, Bagot M, Berti E, Cerroni L, et al. European Organization for Research and Treatment of Cancer and International Society for Cutaneous Lymphoma consensus recommendations for the management of cutaneous B-cell lymphomas. Blood. (2008) 112:1600–9. doi: 10.1182/blood-2008-04-152850
12. Akhtari M, Reddy JP, Pinnix CC, Allen PK, Osborne EM, Gunther JR, et al. Primary cutaneous B-cell lymphoma (non-leg type) has excellent outcomes even after very low dose radiation as single-modality therapy. Leuk Lymphoma. (2016) 57:34–8. doi: 10.3109/10428194.2015.1040012
13. De Felice F, Grapulin L, Pieroni A, Salerno F, D'Elia GM, Pulsoni A, et al. Radiation therapy in indolent primary cutaneous B cell lymphoma: a single institute experience. Ann Hematol. (2018) 97:2411–6. doi: 10.1007/s00277-018-3471-x
14. Eich HT, Eich D, Micke O, Süttzer H, Casper C, Krieg T, et al. Long-term efficacy, curative potential, and prognostic factors of radiotherapy in primary cutaneous B-cell lymphoma. Int J Radiat Oncol Biol Phys. (2003) 55:899–906. doi: 10.1016/S0360-3016(02)04199-8
15. Gauci ML, Quero L, Ram-Wolff C, Guillerm S, M'Barek B, Lebbé C, et al. Outcomes of radiation therapy of indolent cutaneous B-cell lymphomas and literature review. J Eur Acad Dermatol Venereol. (2018) 32:1668–73. doi: 10.1111/jdv.14972
16. Oertel M, Elsayad K, Weishaupt C, Steinbrink K, Eich HT. De-escalated radiotherapy for indolent primary cutaneous B-cell lymphoma. Strahlenther Onkol. (2020) 196:126–31. doi: 10.1007/s00066-019-01541-7
17. Pashtan I, Mauch PM, Chen YH, Dorfman DM, Silver B, Ng AK. Radiotherapy in the management of localized primary cutaneous B-cell lymphoma. Leuk Lymphoma. (2013) 54:726–30. doi: 10.3109/10428194.2012.723707
18. Pedretti S, Urpis M, Leali C, Borghetti P, Baushi L, Sala R, et al. Primary cutaneous non-Hodgkin lymphoma: results of a retrospective analysis in the light of the recent ILROG guidelines. Tumori. (2018) 104:394–400. doi: 10.5301/tj.5000606
19. Malachowski SJ, Sun J, Chen PL, Seminario-Vidal L. Diagnosis and management of cutaneous B-cell lymphomas. Dermatol Clin. (2019) 37:443–54. doi: 10.1016/j.det.2019.05.004
20. Bekkenk MW, Vermeer MH, Geerts ML, Noordijk EM, Heule F, van Voorst Vader PC, et al. Treatment of multifocal primary cutaneous B-cell lymphoma: a clinical follow-up study of 29 patients. J Clin Oncol. (1999) 17:2471–8. doi: 10.1200/JCO.1999.17.8.2471
21. Dummer R, Kempf W, Hess Schmid M, Häffner A, Burg G. Therapy of cutaneous lymphoma–current practice and future developments. Onkologie. (2003) 26:366–72. doi: 10.1159/000072098
22. Dreno B. Standard and new treatments in cutaneous B-cell lymphomas. J Cutan Pathol. (2006) 33:47–51. doi: 10.1111/j.0303-6987.2006.00544.x
23. Kiyohara T, Kumakiri M, Kobayashi H, Nakamura H, Ohkawara A. Cutaneous marginal zone B-cell lymphoma: a case accompanied by massive plasmacytoid cells. J Am Acad Dermatol. (2003) 48:82–5. doi: 10.1067/mjd.2003.154
24. Sah A, Barrans SL, Parapia LA, Jack AS, Owen RG. Cutaneous B-cell lymphoma: pathological spectrum and clinical outcome in 51 consecutive patients. Am J Hematol. (2004) 75:195–9. doi: 10.1002/ajh.20019
25. Smith BD, Glusac EJ, McNiff JM, Smith GL, Heald PW, Cooper DL, et al. Primary cutaneous B-cell lymphoma treated with radiotherapy: a comparison of the European Organization for Research and Treatment of Cancer and the WHO classification systems. J Clin Oncol. (2004) 22:634–9. doi: 10.1200/JCO.2004.08.044
26. Servitje O1, Muniesa C, Benavente Y, Monsálvez V, Garcia-Muret MP, Gallardo F, et al. Primary cutaneous marginal zone B-cell lymphoma: response to treatment and disease-free survival in a series of 137 patients. J Am Acad Dermatol. (2013) 69:357–65. doi: 10.1016/j.jaad.2013.04.047
27. Rijlaarsdam JU, van der Putte SC, Berti E, Kerl H, Rieger E, Toonstra J, et al. Cutaneous immunocytomas: a clinicopathologic study of 26 cases. Histopathology. (1993) 23:117–25. doi: 10.1111/j.1365-2559.1993.tb00469.x
28. Opstelten JL, de Wijkerslooth LR, Leenders M, Bac DJ, Brink MA, Loffeld BC, et al. Variation in palliative care of esophageal cancer in clinical practice: factors associated with treatment decisions. Dis Esophagus. (2017) 30:1–7. doi: 10.1111/dote.12478
29. Dai Y, Li C, Xie Y, Liu X, Zhang J, Zhou J, et al. Interventions for dysphagia in oesophageal cancer. Cochrane Database Syst Rev. (2014) 10:CD005048. doi: 10.1002/14651858.CD005048.pub4
30. Million L, Yi EJ, Wu F, Von Eyben R, Campbell BA, Dabaja B, et al. Radiation therapy for primary cutaneous anaplastic large cell lymphoma: an international Lymphoma Radiation Oncology Group multi institutional experience. Int J Radiat Oncol Biol Phys. (2016) 95:1454–59. doi: 10.1016/j.ijrobp.2016.03.023
31. Devlin PM, St. James SL, Goddard AL, O'Farrell DA, Buzurovic I, Friesen SA, et al. Dose fidelity and conformality for high- dose-rate surface applicator brachytherapy for cutaneous lymphoma lesions of the hand and feet. Brachytherapy. (2014) 13(Suppl 1):S110. doi: 10.1016/j.brachy.2014.02.405
32. O'Farrell DA, Friesen S, Busorovic I, Bhagwat MS, Damato AL, Hansen JL, et al. A HDR method for the treatment of full face cutaneous T-cell lymphoma. Brachytherapy. (2014) 13(Suppl 1):S44–S5. doi: 10.1016/j.brachy.2014.02.272
33. Svoboda VHJ, Kovarik J, Morris F. High dose rate microselectron molds in the treatment of skin tumors. Int J Radiat Oncol Biol Phys. (1995) 31:967–72. doi: 10.1016/0360-3016(94)00485-4
34. Leung JT. Extensive basal cell carcinoma treated with the mould radiotherapy technique. Australas Radiol. (1997) 41:20–1. doi: 10.1111/j.1440-1673.1997.tb00462.x
35. Rudoltz MS, Perkins RS, Luthmann RW, Fracke TD, Green TM, Eaglstein NF, et al. High-dose-rate brachytherapy with a custom surface mold to treat recurrent squamous cell carcinomas of the forearm. J Am Acad Dermatol. (1998) 38:1003–5. doi: 10.1016/S0190-9622(98)70593-6
36. Fabrini MG, Perrone F, De Liguoro M, Cionini L. High-dose-rate brachytherapy in a large squamous cell carcinoma of the hand. Brachytherapy. (2008) 7:270–5. doi: 10.1016/j.brachy.2008.04.004
37. Budrukkar A, Dasgupta A, Pandit P, Laskar SG, Murthy V, Upreti RR, et al. Clinical outcomes with high-dose-rate surface mould brachytherapy for intra-oral and skin malignancies involving head and neck region. J Contemp Brachytherapy. (2017) 9:242–50. doi: 10.5114/jcb.2017.66773
38. Guix B, Finestres F, Tello J, Palma C, Martinez A, Guix J, et al. Treatment of skin carcinomas of the face by high-dose-rate brachytherapy and custom-made surface molds. In J Radiat Oncol Biol Phys. (2000) 47:95–102. doi: 10.1016/S0360-3016(99)00547-7
39. Maroñas M, Guinot JL, Arribas L, Carrascosa M, Tortajada MI, Carmona R, et al. Treatment of facial cutaneous carcinoma with high-dose-rate contact brachytherapy with customized molds. Brachytherapy. (2011) 10:221–7. doi: 10.1016/j.brachy.2010.08.005
40. Rose JN, McLaughlin PY, Hanna TP, D'Souza D, Sur R, Falkson CB. Surface mold brachytherapy for nonmelanoma skin cancer: Canadian patterns of practice. Pract Radiat Oncol. (2014) 4:398–403. doi: 10.1016/j.prro.2013.12.003
41. Montero A, Hernanz R, Capuz AB, Fernández E, Hervás A, Colmenares R, et al. High-dose-rate (HDR) plesiotherapy with custom-made moulds for the treatment of non-melanoma skin cancer. Clin Trans Oncol. (2009) 11:760–4. doi: 10.1007/s12094-009-0439-2
42. Ray A, Basu A, Deb A, Aich RK, Biswas LN, Pal JK. Plesiotherapy for non-melanoma skin cancer: innovating to overcome! Indian J Dermatol. (2010) 55:363–6. doi: 10.4103/0019-5154.74547
43. Ferrandina G, Lucidi A, Paglia A, Corrado G, Macchia G, Tagliaferri L, et al. Role of comorbidities in locally advanced cervical cancer patients administered preoperative chemoradiation: impact on outcome and treatment-related complications. Eur J Surg Oncol. (2012) 38:238–44. doi: 10.1016/j.ejso.2011.12.001
44. Peris K, Fargnoli MC, Garbe C, Kaufmann R, Bastholt L, Seguin NB, et al. Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines. Eur J Cancer. (2019) 118:10–34. doi: 10.1016/j.ejca.2019.06.003
45. Koëter M, van Steenbergen LN, Lemmens VE, Rutten HJ, Roukema JA, Wijnhoven BP, et al. Hospital of diagnosis and probability to receive a curative treatment for oesophageal cancer. Eur J Surg Oncol. (2014) 40:1338–45. doi: 10.1016/j.ejso.2013.12.024
46. Guinot JL, Rembielak A, Perez-Calatayud J, Rodríguez-Villalba S, Skowronek J, Tagliaferri L, et al. GEC-ESTRO ACROP recommendations in skin brachytherapy. Radiother Oncol. (2018) 126:377–85. doi: 10.1016/j.radonc.2018.01.013
47. Lancellotta V, Kovács G, Tagliaferri L, Perrucci E, Rembielak A, Stingeni L, et al. The role of personalized Interventional Radiotherapy (brachytherapy) in the management of older patients with non-melanoma skin cancer. J Geriatr Oncol. (2019) 10:514–7. doi: 10.1016/j.jgo.2018.09.009
48. Lancellotta V, Kovács G, Tagliaferri L, Perrucci E, Colloca G, Valentini V, et al. Age is not a limiting factor in interventional radiotherapy (brachytherapy) for patients with localized cancer. Biomed Res Int. (2018) 2018:2178469. doi: 10.1155/2018/2178469
49. Kovács G, Tagliaferri L, Valentini V. Is an Interventional Oncology Center an advantage in the service of cancer patients or in the education? The Gemelli Hospital and INTERACTS experience. J Contemp Brachytherapy. (2017) 9:497–8. doi: 10.5114/jcb.2017.72603
50. Tagliaferri L, Budrukkar A, Lenkowicz J, Cambeiro M, Bussu F, Guinot JL, et al. ENT COBRA ONTOLOGY: the covariates classification system proposed by the Head & Neck and Skin GEC-ESTRO Working Group for interdisciplinary standardized data collection in head and neck patient cohorts treated with interventional radiotherapy (brachytherapy). J Contemp Brachytherapy. (2018) 10:260–6. doi: 10.5114/jcb.2018.76982
51. Tagliaferri L, Gobitti C, Colloca GF, Boldrini L, Farina E, Furlan C, et al. A new standardized data collection system for interdisciplinary thyroid cancer management: thyroid COBRA. Eur J Intern Med. (2018) 53:73–8. doi: 10.1016/j.ejim.2018.02.012
52. Tagliaferri L, Pagliara MM, Masciocchi C, Scupola A, Azario L, Grimaldi G, et al. Nomogram for predicting radiation maculopathy in patients treated with Ruthenium-106 plaque brachytherapy for uveal melanoma. J Contemp Brachytherapy. (2017) 9:540–7. doi: 10.5114/jcb.2017.71795
53. Tagliaferri L, Kovács G, Autorino R, Budrukkar A, Guinot JL, Hildebrand G, et al. ENT COBRA (Consortium for Brachytherapy Data Analysis): interdisciplinary standardized data collection system for head and neck patients treated with interventional radiotherapy (brachytherapy). J Contemp Brachytherapy. (2016) 8:336–43. doi: 10.5114/jcb.2016.61958
54. Frakulli R, Galuppi A, Cammelli S, Macchia G, Cima S, Gambacorta MA, et al. Brachytherapy in non melanoma skin cancer of eyelid: a systematic review. J Contemp Brachytherapy. (2015) 7:497–502. doi: 10.5114/jcb.2015.56465
55. Ota K, Adar T, Dover L, Khachemoune A. Review: the reemergence of brachytherapy as treatment for non-melanoma skin cancer. J Dermatolog Treat. (2018) 29:170–5. doi: 10.1080/09546634.2017.1341617
Keywords: primary cutaneous B-cell lymphoma, toxicity, radiotherapy, brachytherapy, multidisciplinary
Citation: Di Stefani A, Tagliaferri L, Lancellotta V, Fionda B, Fossati B, Balducci M, Federico F, Hohaus S, De Simone C, Gambacorta MA and Peris K (2020) The Safety of Radiotherapy in the Treatment of Primary Cutaneous B-Cell Lymphoma: A Multidisciplinary Systematic Review. Front. Oncol. 10:1133. doi: 10.3389/fonc.2020.01133
Received: 25 February 2020; Accepted: 05 June 2020;
Published: 14 July 2020.
Edited by:
Onder Alpdogan, Thomas Jefferson University, United StatesReviewed by:
Alberto Fabbri, Siena University Hospital, ItalyCopyright © 2020 Di Stefani, Tagliaferri, Lancellotta, Fionda, Fossati, Balducci, Federico, Hohaus, De Simone, Gambacorta and Peris. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Valentina Lancellotta, dmFsZW50aW5hLmxhbmNlbGxvdHRhQHBvbGljbGluaWNvZ2VtZWxsaS5pdA==
†ORCID: Valentina Lancellotta orcid.org/0000-0003-3507-7051
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.