 Sudath Hapuarachchige1*
Sudath Hapuarachchige1* Dmitri Artemov1,2
Dmitri Artemov1,2- 1The Russell H. Morgan Department of Radiology and Radiological Science, The Johns Hopkins University School of Medicine, Baltimore, MD, United States
- 2Department of Oncology, The Sidney Kimmel Comprehensive Cancer Center, The Johns Hopkins University School of Medicine, Baltimore, MD, United States
Theranostics are nano-size or molecular-level agents serving for both diagnosis and therapy. Structurally, they are drug delivery systems integrated with molecular or targeted imaging agents. Theranostics are becoming popular because they are targeted therapeutics and can be used with no or minimal changes for diagnostic imaging to aid in precision medicine. Thus, there is a close relation between theranostics and image-guided therapy (IGT), and theranostics are actually a subclass of IGT in which both therapeutic and imaging functionalities are attributed to a single platform. An important theranostics strategy is biological pretargeting. In pretargeted IGT, first, the target is identified by a target-specific natural or synthetic bioligand followed by a nano-scale or molecular drug delivery component, which form therapeutic clusters by in situ conjugation reactions. If pretargeted drug delivery platforms are labeled with multimodal imaging probes, they can be used as theranostics for both diagnostic imaging and therapy. Optical and nuclear imaging techniques have mostly been used in proof-of-concept studies with pretargeted theranostics. The concept of pretargeting in theranostics is comparatively novel and generally requires a confirmed overexpression of surface receptors on targeted cells/tissue. In addition, the receptors should have natural or synthetic bioligands to be used as pretargeting components. Therefore, applications of pretargeting theranostics are still limited to several cancer types, which overexpress cell-surface markers on the target cancer cells. In this review, recent discoveries of pretargeting theranostics in breast, ovarian, prostate, and colorectal cancers are discussed to highlight main strengths and potential limitations the strategy.
Introduction
Theranostics is a rapidly developing field that combines the unique opportunities offered by nanotechnology with personalized medicine to provide significantly improved treatment efficacy with reduced off-target effects through the specific delivery of therapy to targeted tissues. Theranostic approaches combine imaging that uses one of the non-invasive imaging modalities, with specific delivery of therapeutic components, which can be based on different biophysical and biological principles. Theranostics can be synthesized to have optimal delivery properties, low renal clearance, reduced immunogenicity and antigenicity (for example by PEGylating the surface of theranostic nanoparticles), and high capacity for therapeutic agents, which is required given the limited concentrations of specific molecular markers expressed on cancer cells.
Theranostics
Theranostic probes can be used for both diagnostic imaging and therapy (1). For a truly theranostic application, imaging and therapeutic molecules should be parts of a single platform functionalized with various moieties for specific recognition of molecular targets, imaging markers, and therapeutic compounds. One of the major problems in achieving efficient treatment in this strategy is the uniform delivery and distribution of theranostics with therapeutic cargo in the tumor or sufficiently strong bystander effects of therapy (such as for hyperthermia). As the distribution of nano-scale drug delivery platforms is primarily driven by the passive diffusion facilitated by the enhanced-permeability-retention (EPR) effect, which is present in some solid tumors, optimization of the molecular size, and circulation time of nanoplatforms is of paramount importance for the success of treatment. However, there are additional biological delivery barriers, such as the desmoplastic tumor microenvironment (2) and increased interstitial pressure due to dysfunctional lymphatics in solid tumors (3), which can modulate the delivery. The presence of a functional blood-brain barrier in brain tumors presents an entirely new set of problems with delivery, which is beyond the scope of the current review. Imaging can help to evaluate the uniformity of delivery, but, to achieve high efficacy, the design of a therapeutic system must ensure the effective delivery and distribution of theranostics to all malignant cells within the cancer.
While the initial distribution of theranostics in tumors is driven by passive processes and needs to be optimized based on the intrinsic physicochemical properties of platform, specific retention and cell delivery is typically controlled by active targeting of theranostic to specific molecular targets present on cancer cells using high-affinity molecules, such as antibodies, antibody fragments, affibodies, peptides, etc. It is important to note that, while unique, highly specific molecular targets are preferable for the application of highly cytotoxic theranostics, the initial delivery of theranostics rely on the tumor-specific EPR effect. The “binding site barrier” is a critical factor in targeted drug delivery (4, 5). This issue can be circumvented in theranostic design using biomolecules as platforms and keeping the size of components in subnano level (6).
Pretargeting Theranostic Approach
Important criteria that should be fulfilled for a truly theranostic platform is that the imaging data must provide meaningful information, which can be used to make critical decisions regarding the therapeutic procedure. In pretargeting therapy, the first component is typically used for labeling the target and obtaining the location and size (perhaps tumor stage) of the tumor. Since the pretargeting component is not cytotoxic, its long circulation (and possible weak non-specific binding) does not generate side effects, while providing improved distribution in the tumor. After the target is confirmed, the second therapeutic components can be administered chemoselectively cross-linking the first pretargeting component on cell surface.
Contemporary targeted drug delivery vehicle such as ADCs, with an imaging marker may provide imaging information about the delivery and distribution of the platform in the tumor. Micro-dosing can also be used to track the delivery and image the distribution prior to the administration of the therapeutic dose (Figure 1). However, while these approaches can be considered theranostic, in the first case, imaging would only provide secondary information that cannot be used to change and/or optimize the treatment protocol, and, in the latter case, imaging is limited to a significantly reduced dose and the therapeutic dose of nanomedicine is delivered without image guidance.
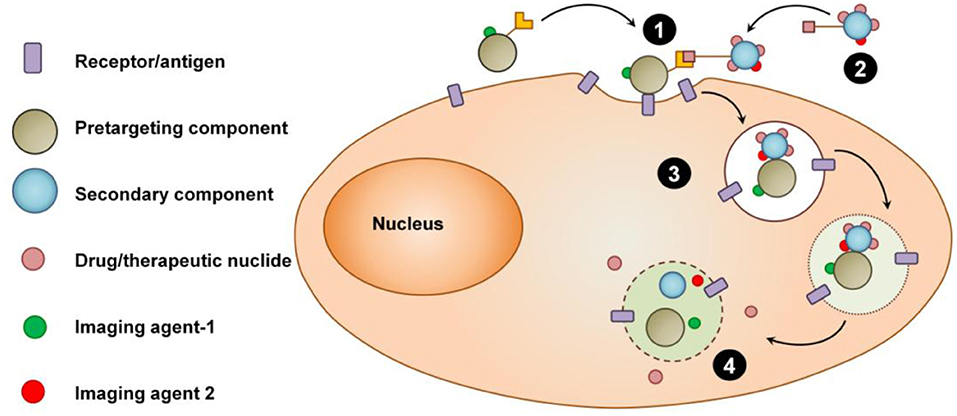
Figure 1. Schematic view of the concept of pretargeting theranostic strategy. (1) Image-guided pretargeting. (2) Therapeutic/radionuclide delivery step. (3) Internalization of the complex of pretargeting-receptor-delivery components. (4) Intracellular release of therapeutics or radionuclides.
In situ Conjugation Methods in Pretargeting Theranostics
The conjugation between pretargeting component and the therapeutic delivery component occurs in the biological system in physiological conditions. This in situ conjugation method should be fast and proceed at 37°C without releasing toxic byproducts. Avidin-biotin interaction is one of the early stage in situ conjugation techniques used for pretargeted imaging and therapy (7). Avidin is a tetrameric protein which binds biotin with high affinity. Since avidin is immunogenic and has a broad non-specific binding, this conjugation method can lead to adverse biological effects and toxicities. Bioorthogonal click chemistry is an alternative conjugation method widely used nowadays for in situ conjugation. Trans-cyclooctene/tetrazine bioorthogonal click reaction is extremely fast and widely used for pretargeting conjugation compared to other reactions in this category such as, copper-free azide-cyclooctyne click chemistry and Staudinger ligation (8, 9). Specific interaction between peptide nucleic acids, which are non-natural DNA/RNA analogs, can also be used for pretargeting approach (10). These compounds are metabolically stable and show low non-specific binding in healthy tissues.
Imaging Strategy in Theranostic Systems
A wide variety of imaging modalities used for theranostics include optical (fluorescence or bioluminescence), nuclear (PET or SPECT), ultrasound, photoacoustic, magnetic particle, and MR imaging techniques (11, 12). The imaging results pretargeting component can be directly used to (i) verify the expression of surface receptors at the target site and (ii) precisely time the administration of the second, drug-delivery component, based on high specific accumulation of the pretargeting component at the target site and clearance from the rest of the body. Expression of receptors can be variable between the primary tumor and distant metastatic sites and not easily accessible by biopsy. Therefore, images from pretargeting component provide a positive confirmation of the receptor expression and a “go” signal for the administration of the cytotoxic drug carrier. Imaging of the drug carrier is equally important, as it can provide positive confirmation of the successful delivery and retention of the cytotoxic component in the tumor. These imaging results can also be used to correlate the delivery and treatment outcomes and to support their use as imaging markers of response. The optical imaging is widely used in preclinical drug developments because it's fast, convenient, non-invasive, safe, and cost-effective (13). High tissue absorbance and scatter are the major disadvantages in optical imaging in deep locations; however, this issue can be partly overcome in preclinical imaging using near infra-red (NIR) dyes (λex in the range of 650–900 nm) (14). In spite of aforementioned problems, NIR optical imaging became a popular imaging technique in pretargeting studies for visualizing the target and the probe and it can provide sufficient information about the target-uptake and biodistribution of the pretargeting component, as well as the tumor dimension and location information in cancer therapy (15).
Nuclear imaging techniques are highly feasible for imaging pretargeting delivery because of excellent sensitivity, quantitative images, and the possibility of using in radiotherapy (16). Nuclear imaging provides sensitivity in the low nM to pM range, but has low spatial resolution and requires an additional anatomical imaging modality, such as CT or MRI, for anatomical reference. PET and SPECT imaging techniques are translational and can be used in both animals and patients. PET provides the highest sensitivity combined with improved spatial resolution; however, it is impossible to differentiate between two tracers with similar half-lives. SPECT provides an intrinsic ability for multi-isotope imaging based on different energy of γ emission (17). However, it is not commonly used for tracking of pretargeting components because of lower sensitivity and spatial resolution. However, it has been used for imaging the second therapeutic component of the system. For instance, in image-guided pretargeting radioimmunotherapy (PRIT), the targeted cells are labeled with antibodies conjugated with TCO groups and treated with SPECT imaging/therapeutic radionuclide conjugated with tetrazine. Pretargeting radiotherapy is one example of combining nuclear imaging to circumvent the use of long-lived radionuclides that is a necessity for sufficient tumor accumulation and target-to-background ratios using conventional approaches (16).
The imaging signals of the second component are mostly used for the biodistribution and pharmacokinetic evaluation and not for detection and evaluation of the tumor, hence the poor contrast and spatial resolution of SPECT imaging can be tolerated. MRI provides high spatial resolution and excellent soft-tissue contrast, but has a moderate sensitivity and requires concentrations of the imaging probe in high micromolar range. Fluorescence optical imaging provides outstanding sensitivity and resolution, but can only be used in superficial locations, such as for image-guided surgical resection, or in optically transparent tissues, such as ocular imaging. Examples of anticancer theranostics applications, which use these multiple imaging modalities are: PET and NIR optical imaging (18); SPECT (19), and MRI (20).
It is important to note that combining a therapeutic platform with short-lived imaging probes presents significant problems because of the short lifetime of the preparation, and consequently, with the logistics of treatment administration and monitoring even if the medication can be formulated in a kit form for rapid radiolabeling (21). Therapeutic modalities used in theranostic nano-platforms include cytotoxic drugs (22–24), radioisotopes (25), optical absorbers for photothermal or photodynamic therapy (26), and phototherapy (27). Specific enzymes can be delivered to activate prodrugs in the context of prodrug therapy (28). Magnetic NPs are therapeutic cargo for magnetic hyperthermia (29), and antibodies, adjuvants, or vaccines can be used for cancer immunotherapy (30). Most often, imaging techniques used in pretargeting theranostics rely on complementary optical and nuclear imaging modalities, such as fluorescence, bioluminescence, PET and SPECT imaging.
Examples of Pretargeted Theranostics
Pretargeted Theranostics in Breast Cancer
Breast cancer is the most prevalent malignancy in women in the United States, and ~20–30% of human BrCa overexpress HER2 receptors, a molecular marker that correlates with cancer aggressiveness, metastasis, and poor prognosis. HER2-overexpressing BrCa are treated with the humanized anti-HER2 monoclonal antibody, Trastuzumab (Tz), which is highly efficacious, but unfortunately, trastuzumab resistance develops over long-term use (31–33). Trastuzumab-based ADC, T-DM1, was developed for treatment of resistant tumors by directly conjugating the chemotherapeutic drug, mertansine, on the antibody to boost cytotoxicity (34). A potential problem with ADCs is their intrinsically highly toxicity, which can cause non-specific off-target effects in normal tissues due to their long circulation times (35). Hapuarachchige et al. (23, 24) has reported a pretargeting strategy driven by bioorthogonal click chemistry to circumvent this issue. In these studies, HER2(+) cancer cells were prelabeled with a trastuzumab mAb, functionalized with a bioorthogonal, click-reactive, TCO group, and the drug-carrier albumin component with the complementary click-reactive Tt group is delivered after free antibodies have cleared the body, to ensure that the toxic drug component accumulates only at the tumor site (Figure 2A). The strategy has been evaluated in human BrCa BT-474 cells and their HER2(+) subcutaneous tumor mouse models. Mice were administered with Tz(TCO)6(CF-680)2 image-guided pretargeting component followed by Alb(Px)2.6(Peg4-Tt)15(CF-750)2 drug delivery component. The result revealed that pretargeting approach driven by bioorthogonal click chemistry has higher therapeutic efficacy than the treatment by drug delivery component alone. This therapeutic regimen, when integrated with molecular imaging modalities, can become an effective theranostic tool that will eventually steer the development of cancer regimens toward precision, individuality, and safety.
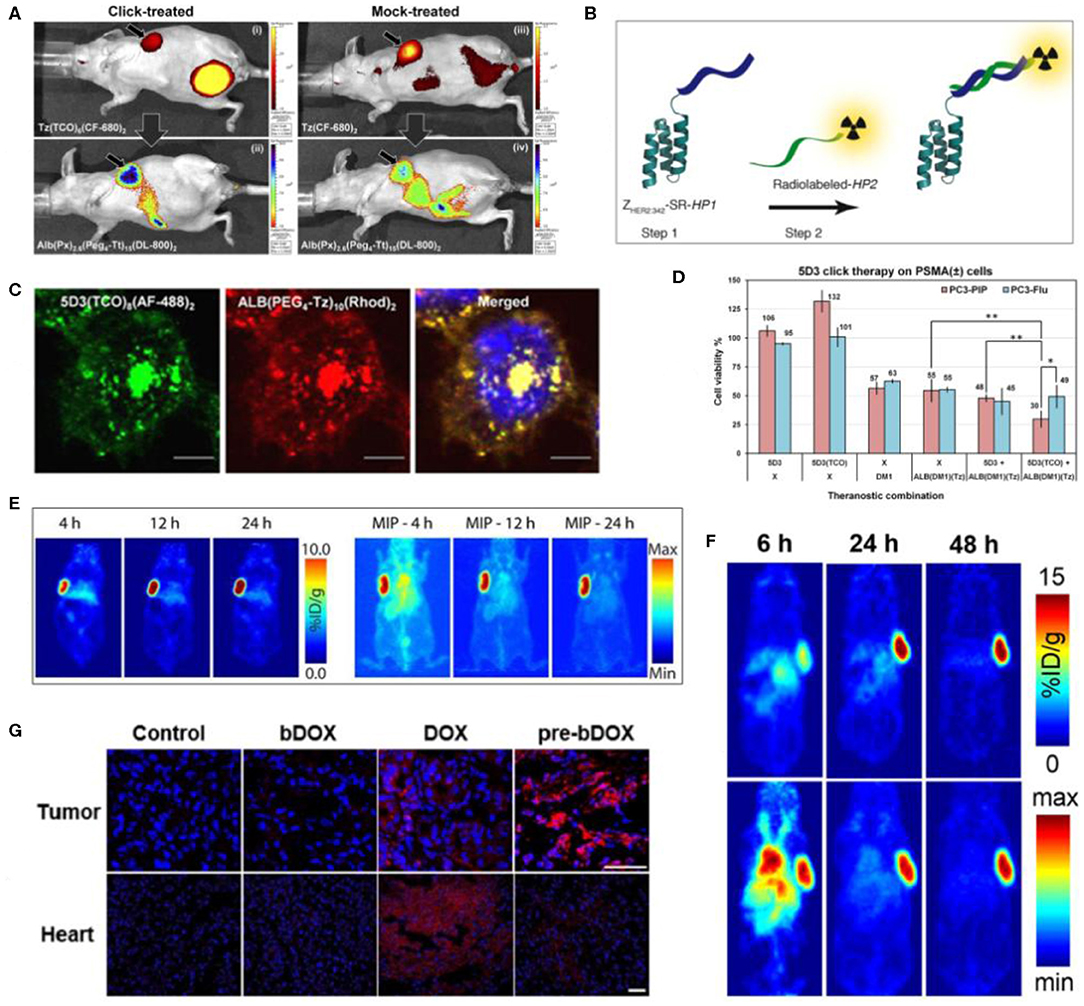
Figure 2. Examples of pretargeted theranostic approaches. (A) In vivo Xenogen fluorescence images after 8 h post-injection of the secondary component (after 20 h post-injection of pretargeting component). (i) Distribution of pretargeting component Tz(TCO)6(CF-680)2 and (ii) tumor uptake of delivery component Alb(Px)2.6(Peg4-Tt)15(DL-800)2. (iii) Distribution of control Tz(CF-680)2 and (iv) Alb(Px)2.6(Peg4-Tt)15(DL-800)2 in a mock-treated mouse (23). (B) Schematic view of the strategy. In step-1 ZHER2:342-SR-HP1 is injected and labeled the HER2(+) tumor cells. Next, the secondary probe HP2 is injected in step 2. The PNA sequence in HP2 is matching with HP1 and hybridized to the pretargeting component bound on cell surface (36). (C) Confocal fluorescence microscope images of pretargeted theranostic approach in PSMA(+) PC3-PIP cells. Distribution of 5D3(TCO)8(AF-488)2 (green), ALB(PEG4-Tz)10(Rhod)2 (red), and Hoechst 33342 nuclear counterstaining (blue) (magnification × 100, bar: 30 μm) (22). (D) In vitro therapeutic study of 5D3(TCO)8. The combination of 5D3(TCO)8 and ALB(DM1)3.3(PEG4-Tz)10 exhibited a selective and enhanced toxicity in PSMA(+) PC3-PIP cells compared to the combination of non-functionalized 5D3 and ALB(DM1)3.3(PEG4-Tz)10 or treatment with a free DM1 or ALB alone. (*p < 0.05, **p < 0.005) (22). (E) Pretargeting PET images of planar and maximum intensity projection (MIP), left and right, respectively in subcutaneous SW1222 tumor bearing nude mice. HuA33-Dye800-TCO was injected (100 μg; 0.66 nmol) and after 48 h, 64Cu-Tz-SarAr was injected. Coronal slices selected from the center of the tumors are shown (37). (F) PET images of the athymic nude mice with subcutaneous SW1222 tumor xenografts. The mice were first injected with huA33(TCO)2.4, followed after 24 h by the injection of [64Cu]Cu-SarAr-Tz and after 24 h by the injection of [177Lu]Lu-DOTA-PEG7-Tz. Images are shown at 6, 24, and 48 h after the injection of [64Cu]Cu-SarAr-Tz. Top row: Coronal planar images through center of the tumor. Bottom row: maximum intensity projections (MIP) (38). (G) Confonal fluorescence images of frozen sections showing doxorubicin drug uptake in tumor and heart tissues after the administration of PBS, un-pretargeting bDOX, free doxorubicin or pretargeting bDOX. Blue color represents DAPI-stained nuclei, and pseudo-red color represents fluorescence from DOX or bDOX. The scale bar: 50 μm. *p < 0.05 (pre-bDOX: pre-targeted bDOX) (39).
Pretargeted Theranostics in Ovarian Cancer
Ovarian cancer is the deadliest gynecological cancer in women; hence, the early detection and treatments are vitally important (40). Efforts have been taken to developed drugs to treat ovarian cancers overexpressing estrogen receptor (ER) and HER2. However, long term use of these novel therapies gains drug resistance. Therefore additional therapeutic approaches, such as radioimmunotherapy are needed to be developed for ovarian cancer to overcome the chemo-resistance issues (41). Affibody is a relatively low molecular weight high-affinity protein, which can be used instead of monoclonal antibodies for diagnostic imaging and therapy. Honarvar et al. (36) has developed a HER2 specific affibody conjugate and complementary secondary imaging component and evaluate in HER2(+) ovarian cancer xenografts. They have synthesized ZHER2:342-SR-HP1 and used it as the pretargeting component with 15-mer HP1 peptide nucleic acid moiety to recognize complementary secondary component, 111In-/125I-HP2 (Figure 2B). The results revealed that the HER2(+) tumor uptake of pretargeting, ZHER2:342-SR-HP1 was significantly higher than HER2 low expressing cells. In the pretargeting approach, accumulation of 111In-HP2 after the administration of ZHER2:342-SR-HP1 was significantly higher compared to the administration of 111In-HP2 alone. In regular radioimmunotherapy, the fast clearance of the secondary component, 111In-HP2, results in low tumor uptake in bones. Pretargeting strategy enhances the accumulation and retention of the radiotherapeutic agent at the target.
Pretargeted Theranostics in Prostate Cancer
Prostate cancer is one of the most devastating cancer types in men. Yearly more than 150,000 patients are diagnosed with prostate cancer and over 30,000 among them die. Despite existing therapies in prostate cancer management, novel therapeutic approaches and drug delivery strategies are still required to save these patients and eradicate the decease completely (42–44). Prostate-specific membrane antigen (PSMA), a type II membrane protein, is highly expressed in aggressive prostate cancer (PCa) (45–48). In our studies, we have used 5D3 mAb, a novel anti-PSMA mAb which exhibits a 10-fold higher binding affinity on PSMA compared to other known anti-PSMA mAb, such as J591 and 7E11 mAbs (49, 50). 5D3 mAb shows fast internalization after complexing with PSMA; however, this strategy has been successfully applied and proven in vitro.
Hapuarachchige et al. (22) has reported a promising pretargeting theranostic approach for treating PSMA-overexpressing prostate cancer using 5D3 mAb. Here, 5D3 conjugated TCO and albumin conjugated with tetrazine have been used as pretargeting and delivery components, respectively. Both components were labeled with fluorophores without spectral profile conflicts to track with optical imaging. PSMA(+) PC3-PIP and PSMA(–) PC3-Flu cells were used to validate the strategy in vitro. The pretargeting component, 5D3(TCO)8(AF-488)2, labeled the PSMA receptors on the targeted cell surface, and was then followed by a second-component, ALB(DM1)2.2(Peg4-Tt)10(Rhod)2 (Figure 2C). The multiple TCO and Tt groups per component, the high density of PSMA receptors per cell surface, and the fast kinetics of the TCO-Tt click reaction are the driving forces for the formation of nanoclusters on the cell surface. An efficient cross-linking of two components on the targeted cell surface leads to enhanced cellular internalization and results in the highest therapeutic effects in PSMA(+) PC3-PIP cells compared to PSMA(–) PC3-Flu cells (Figure 2D). Ideally, the internalization and pharmacokinetics of the pretargeting agent should have similar time scales. After internalization, nanoclusters are hydrolyzed in acidic late endosomes and release cargo drug molecules to the cytoplasm. Eventually, a DM1 anti-tubulin agent blocks the microtubule formation, arresting cell division, and killing targeted cells.
Pretargeted Theranostics in Colorectal Cancer
Colorectal cancer is the most common cancer type in the world after lung and BrCa (51). The surgical approach of managing colorectal cancer is limited for cases with localized tumors but not feasible in early stage tumors and metastatic tumors. Pretargeting radioimmunotherapy is an optimistic solution to overcome these issues (52). As an initiate, Adumeau et al. (37) has reported a pretargeting multimodal PET/NIRF imaging approach for imaging colorectal cancer. They have used humanized A33 monoclonal antibody (huA33) as the pretargeting platform targeting A33-expressing colorectal cancer. HuA33 was conjugated with TCO and labeled with Dye800 NIR fluorophore and used as the pretargeting component with tetrazine–sarcophagine conjugate labeled with 64Cu radionuclide (64Cu-Tz-SarAr). This strategy has been successfully evaluated in SM1222 colorectal cancer xenograft tumor mouse models overexpressing A33 cell surface antigen (Figure 2E). Keinanen et al. (38) from the same group have reported the extension of this study from diagnostic [64Cu]Cu-SarAr-Tz to therapeutic, using [177Lu]Lu-DOTA-PEG7-Tz conjugates, as the secondary component. Both [64Cu]Cu-SarAr-Tz and [177Lu]Lu-DOTA-PEG7-Tz have shown high activity in mice models bearing A33-overexpressing subcutaneous tumors (Figure 2F).
The biotin and avidin chemistry has been successfully used for pretargeting imaging of HER2(+) BrCa in preclinical settings (7). Lectin receptors are overexpressed and many cancer types and avidin can bind with lectin as well. Yao et al. (39) have used this phenomenon for pretargeting theranostic approach for image-guided treatment of human colorectal cancer cells, LS180 and HT-29. In their study, avidin without conjugation has been used as the pretargeting component targeting lectin receptors in colorectal cancer cells and tumors in mouse models. Doxorubicin was conjugated with biotic through an acid sensitive hydrazone linker (bDOX). Because of the hydrazone bonding doxorubicin is in prodrug stage. To evaluate the strategy, colorectal cancer LS180 and HT-29 cells were first treated with avidin followed by the administration of bDOX. Avidin is labeled on the lectin receptors of the targeted cell surface. Then biotinylated dDOX will be complexed with avidin followed by rapid internalization by endocytosis. In late endosomes or lysosomes, at low pH acidic condition, hydrazone bond is cleaved releasing free doxorubicin. Compared to doxorubicin alone, pretargeting approach shows higher cellular uptake of the drug. In vivo study, LS180 colorectal cancer xenograft mouse models were subsequently administered with avidin and bDOX and significant reduction of tumor growth was observed compared to the mice treated with free doxorubicin (Figure 2G). Hence, this strategy is synthetically convenient and exhibits enhanced therapeutic efficacy with minimal systemic toxicities.
Conclusions
Theranostics can be a highly important tool in the development of precision, highly efficient, and safe therapy for the personalized treatment of cancer using molecular information from a patient's tumors. The pretargeting approach can leverage the inherent strengths of the theranostic strategy; however, it will require a strategy of orthogonal conjugation in physiological conditions. The combination of pretargeting imaging and therapy provided several advantages over single-component theranostics. This strategy significantly reduces the circulatory time and off-target toxicity of the drug-carrier component and provides objective criteria for optimization of the treatment protocol based on the results of non-invasive imaging. The prerequisites for successful applications of a pretargeting theranostic approach are (a) high expression of the target receptor and the use of a high binding affinity pretargeting component, (b) optimal internalization of the pretargeting component-receptor molecular complex, which is a complex parameters that depends on the tumor microenvironment conditions and should allow an adequate time window for in situ reactions with a second delivery component, (c) affinity of the binding of two components on the targeted cell surface, and (d) correct combination of imaging agents/imaging modalities and therapeutics on the therapeutic components.
Author Contributions
All authors listed have made equal direct and intellectual contribution to the work and preparation of the manuscript and approved the manuscript for publication.
Funding
This work was supported in part by NIH R01CA209884, DOD PC150837, and Emersion Collective 128821 grants.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor declared a past co-authorship with the authors.
References
1. Langbein T, Weber WA, Eiber M. Future of theranostics: an outlook on precision oncology in nuclear medicine. J Nucl Med. (2019) 60:13S−9S. doi: 10.2967/jnumed.118.220566
2. Mpekris F, Papageorgis P, Polydorou C, Voutouri C, Kalli M, Pirentis AP, et al. Sonic-hedgehog pathway inhibition normalizes desmoplastic tumor microenvironment to improve chemo- and nanotherapy. J Control Release. (2017) 261:105–12. doi: 10.1016/j.jconrel.2017.06.022
3. Jain RK. Delivery of molecular and cellular medicine to solid tumors. Adv Drug Deliv Rev. (2012) 64:353–65. doi: 10.1016/j.addr.2012.09.011
4. Weinstein JN, van Osdol W. Early intervention in cancer using monoclonal antibodies and other biological ligands: micropharmacology and the “Binding Site Barrier”. Cancer Res. (1992) 52:2747s−51s.
5. Ruoslahti E, Bhatia SN, Sailor MJ. Targeting of drugs and nanoparticles to tumors. J Cell Biol. (2010) 188:759–68. doi: 10.1083/jcb.200910104
6. Rosenblum D, Joshi N, Tao W, Karp JM, Peer D. Progress and challenges towards targeted delivery of cancer therapeutics. Nat Commun. (2018) 9:1410. doi: 10.1038/s41467-018-03705-y
7. Zhu W, Okollie B, Bhujwalla ZM, Artemov D. Pamam dendrimer-based contrast agents for Mr imaging of Her-2/Neu Receptors by a three-step pretargeting approach. Magn Reson Med. (2008) 59:679–85. doi: 10.1002/mrm.21508
8. Meyer JP, Houghton JL, Kozlowski P, Abdel-Atti D, Reiner T, Pillarsetty NV, Scholz WW, Zeglis BM, Lewis JS. (18)F-Based Pretargeted pet imaging based on bioorthogonal diels-alder click chemistry. Bioconjug. Chem. (2016) 27:298-301. doi: 10.1021/acs.bioconjchem.5b00504
9. Mushtaq S, Yun SJ, Jeon J. Recent advances in bioorthogonal click chemistry for efficient synthesis of radiotracers and radiopharmaceuticals. Molecules. (2019) 24:3567. doi: 10.3390/molecules24193567
10. Saarbach J, Sabale PM, Winssinger N. Peptide nucleic acid (Pna) and its applications in chemical biology, diagnostics, and therapeutics. Curr Opin Chem Biol. (2019) 52:112–24. doi: 10.1016/j.cbpa.2019.06.006
11. Penet MF, Chen Z, Kakkad S, Pomper MG, Bhujwalla ZM. Theranostic imaging of cancer. Eur J Radiol. (2012) 81(Suppl 1):S124–6. doi: 10.1016/S0720-048X(12)70051-7
12. Yordanova A, Eppard E, Kurpig S, Bundschuh RA, Schonberger S, Gonzalez-Carmona M, et al. Theranostics in nuclear medicine practice. Onco Targets Ther. (2017) 10:4821–8. doi: 10.2147/OTT.S140671
13. Arranz A, Ripoll J. Advances in optical imaging for pharmacological studies. Front Pharmacol. (2015) 6:189. doi: 10.3389/fphar.2015.00189
14. Dang X, Bardhan NM, Qi J, Gu L, Eze NA, Lin CW, et al. Deep-tissue optical imaging of near cellular-sized features. Sci Rep. (2019) 9:3873. doi: 10.1038/s41598-019-39502-w
15. De Grand AM, Lomnes SJ, Lee DS, Pietrzykowski M, Ohnishi S, Morgan TG, et al. Tissue-like phantoms for near-infrared fluorescence imaging system assessment and the training of surgeons. J Biomed Opt. (2006) 11:014007. doi: 10.1117/1.2170579
16. Steen EJL, Edem PE, Norregaard K, Jorgensen JT, Shalgunov V, Kjaer A, et al. Pretargeting in nuclear imaging and radionuclide therapy: improving efficacy of theranostics and nanomedicines. Biomaterials. (2018) 179:209–45. doi: 10.1016/j.biomaterials.2018.06.021
17. Du Y, Links JM, Becker L, DiPaula AF, Frank T, Schuleri KH, et al. Evaluation of simultaneous 201tl/99mtc dual-isotope cardiac spect imaging with model-based crosstalk compensation using canine studies. J Nucl Cardiol. (2014) 21:329–40. doi: 10.1007/s12350-013-9842-8
18. Lee HJ, Ehlerding EB, Jiang D, Barnhart TE, Cao T, Wei W, et al. Dual-labeled pertuzumab for multimodality image-guided ovarian tumor resection. Am J Cancer Res. (2019) 9:1454–68.
19. Spa SJ, Welling MM, van Oosterom MN, Rietbergen DDD, Burgmans MC, Verboom W, et al. A supramolecular approach for liver radioembolization. Theranostics. (2018) 8:2377–86. doi: 10.7150/thno.23567
20. Hu X, Tang Y, Hu Y, Lu F, Lu X, Wang Y, et al. Gadolinium-chelated conjugated polymer-based nanotheranostics for photoacoustic/magnetic resonance/Nir-Ii fluorescence imaging-guided cancer photothermal therapy. Theranostics. (2019) 9:4168–81. doi: 10.7150/thno.34390
21. Ebenhan T, Vorster M, Marjanovic-Painter B, Wagener J, Suthiram J, Modiselle M, et al. Development of a single vial kit solution for radiolabeling of 68ga-Dkfz-Psma-11 and its performance in prostate cancer patients. Molecules. (2015) 20:14860–78. doi: 10.3390/molecules200814860
22. Hapuarachchige S, Huang CT, Donnelly MC, Barinka C, Lupold SE, Pomper MG, et al. Cellular Delivery of bioorthogonal pretargeting therapeutics in Psma-positive prostate cancer. Mol Pharm. (2020) 17:98–108. doi: 10.1021/acs.molpharmaceut.9b00788
23. Hapuarachchige S, Kato Y, Artemov D. Bioorthogonal, Two-component drug delivery in Her2(+) breast cancer mouse models. Sci Rep. (2016) 6:24298. doi: 10.1038/srep24298
24. Hapuarachchige S, Zhu W, Kato Y, Artemov D. Bioorthogonal, Two-component delivery systems based on antibody and drug-loaded nanocarriers for enhanced internalization of nanotherapeutics. Biomaterials. (2014) 35:2346–54. doi: 10.1016/j.biomaterials.2013.11.075
25. Pandit-Taskar N. Targeted radioimmunotherapy and theranostics with alpha emitters. J Med Imaging Radiat Sci. (2019) 50(4 Suppl 1):S41–4. doi: 10.1016/j.jmir.2019.07.006
26. Yang L, Wang J, Yang S, Lu Q, Li P, Li N. Rod-shape Msn@Mos2 nanoplatform for Fl/Msot/Ct imaging-guided photothermal and photodynamic therapy. Theranostics. (2019) 9:3992–4005. doi: 10.7150/thno.32715
27. Chen Y, Chatterjee S, Lisok A, Minn I, Pullambhatla M, Wharram B, et al. A Psma-targeted theranostic agent for photodynamic therapy. J Photochem Photobiol B. (2017) 167:111–6. doi: 10.1016/j.jphotobiol.2016.12.018
28. Chen Z, Penet MF, Krishnamachary B, Banerjee SR, Pomper MG, Bhujwalla ZM. Psma-specific theranostic nanoplex for combination of trail gene and 5-Fc prodrug therapy of prostate cancer. Biomaterials. (2016) 80:57–67. doi: 10.1016/j.biomaterials.2015.11.048
29. Du Y, Liu X, Liang Q, Liang XJ, Tian J. Optimization and design of magnetic ferrite nanoparticles with uniform tumor distribution for highly sensitive Mri/Mpi performance and improved magnetic hyperthermia therapy. Nano Lett. (2019) 19:3618–26. doi: 10.1021/acs.nanolett.9b00630
30. Liu Y, Wang X, Hussain M, Lv M, Dong X, Wang T, et al. Theranostics Applications of nanoparticles in cancer immunotherapy. Med Sci (Basel). (2018) 6:100. doi: 10.3390/medsci6040100
31. Luque-Cabal M, Garcia-Teijido P, Fernandez-Perez Y, Sanchez-Lorenzo L, Palacio-Vazquez I. Mechanisms Behind the resistance to trastuzumab in Her2-amplified breast cancer and strategies to overcome it. Clin Med Insights Oncol. (2016) 10:21–30. doi: 10.4137/CMO.S34537
32. Pohlmann PR, Mayer IA, Mernaugh R. Resistance to trastuzumab in breast cancer. Clin Cancer Res. (2009) 15:7479–91. doi: 10.1158/1078-0432.CCR-09-0636
33. Wang C, Wang L, Yu X, Zhang Y, Meng Y, Wang H, et al. Combating acquired resistance to trastuzumab by an anti-Erbb2 fully human antibody. Oncotarget. (2017) 8:42742–51. doi: 10.18632/oncotarget.17451
34. Girish S, Gupta M, Wang B, Lu D, Krop IE, Vogel CL, et al. Clinical pharmacology of trastuzumab emtansine (T-Dm1): an antibody-drug conjugate in development for the treatment of Her2-positive cancer. Cancer Chemother Pharmacol. (2012) 69:1229–40. doi: 10.1007/s00280-011-1817-3
35. Mahalingaiah PK, Ciurlionis R, Durbin KR, Yeager RL, Philip BK, Bawa B, et al. Potential mechanisms of target-independent uptake and toxicity of antibody-drug conjugates. Pharmacol Ther. (2019) 200:110–25. doi: 10.1016/j.pharmthera.2019.04.008
36. Honarvar H, Westerlund K, Altai M, Sandstrom M, Orlova A, Tolmachev V, et al. Feasibility of affibody molecule-based pna-mediated radionuclide pretargeting of malignant tumors. Theranostics. (2016) 6:93–103. doi: 10.7150/thno.12766
37. Adumeau P, Carnazza KE, Brand C, Carlin SD, Reiner T, Agnew BJ, et al. A Pretargeted approach for the multimodal Pet/Nirf imaging of colorectal cancer. Theranostics. (2016) 6:2267–77. doi: 10.7150/thno.16744
38. Keinanen O, Brennan JM, Membreno R, Fung K, Gangangari K, Dayts EJ, et al. Dual radionuclide theranostic pretargeting. Mol Pharm. (2019) 16:4416–21. doi: 10.1021/acs.molpharmaceut.9b00746
39. Yao M, Ma X, Zhang X, Shi L, Liu T, Liang X, et al. Lectin-mediated pH-sensitive doxorubicin prodrug for pre-targeted chemotherapy of colorectal cancer with enhanced efficacy and reduced side effects. Theranostics. (2019) 9:747–60. doi: 10.7150/thno.29989
40. Maeda K, Sasaki H, Ueda S, Miyamoto S, Terada S, Konishi H, et al. Serum exosomal Microrna-34a as a potential biomarker in epithelial ovarian cancer. J Ovarian Res. (2020) 13:47. doi: 10.1186/s13048-020-00648-1
41. Kasten BB, Arend RC, Katre AA, Kim H, Fan J, Ferrone S, et al. B7-H3-targeted (212)Pb radioimmunotherapy of ovarian cancer in preclinical models. Nucl Med Biol. (2017) 47:23–30. doi: 10.1016/j.nucmedbio.2017.01.003
42. Osanto S, Van Poppel H. Emerging novel therapies for advanced prostate cancer. Ther Adv Urol. (2012) 4:3–12. doi: 10.1177/1756287211432777
43. Clarke JM, Armstrong AJ. Novel therapies for the treatment of advanced prostate cancer. Curr Treat Options Oncol. (2013) 14:109–26. doi: 10.1007/s11864-012-0222-4
44. Poon DM, Ng J, Chan K. Importance of cycles of chemotherapy and postdocetaxel novel therapies in metastatic castration-resistant prostate cancer. Prostate Int. (2015) 3:51–5. doi: 10.1016/j.prnil.2015.03.002
45. Bouchelouche K, Choyke PL, Capala J. Prostate specific membrane antigen - a target for imaging and therapy with radionuclides. Discov Med. (2010) 9:55–61.
46. Bravaccini S, Puccetti M, Bocchini M, Ravaioli S, Celli M, Scarpi E, et al. Psma expression: a potential ally for the pathologist in prostate cancer diagnosis. Sci Rep. (2018) 8:4254. doi: 10.1038/s41598-018-22594-1
47. Mease RC, Foss CA, Pomper MG. Pet Imaging in prostate cancer: focus on prostate-specific membrane antigen. Curr Top Med Chem. (2013) 13:951–62. doi: 10.2174/1568026611313080008
48. Chatalic KL, Veldhoven-Zweistra J, Bolkestein M, Hoeben S, Koning GA, Boerman OC, et al. A novel (1)(1)(1)in-Labeled anti-prostate-specific membrane antigen nanobody for targeted spect/Ct imaging of prostate cancer. J Nucl Med. (2015) 56:1094–9. doi: 10.2967/jnumed.115.156729
49. Novakova Z, Foss CA, Copeland BT, Morath V, Baranova P, Havlinova B, et al. Novel Monoclonal antibodies recognizing human prostate-specific membrane antigen (Psma) as research and theranostic tools. Prostate. (2017) 77:749–64. doi: 10.1002/pros.23311
50. Banerjee SR, Kumar V, Lisok A, Plyku D, Novakova Z, Brummet M, et al. Evaluation of (111)in-Dota-5d3, a surrogate spect imaging agent for radioimmunotherapy of prostate-specific membrane antigen. J Nucl Med. (2019) 60:400–6. doi: 10.2967/jnumed.118.214403
51. McGettigan M, Cardwell CR, Cantwell MM, Tully MA. Physical activity interventions for disease-related physical and mental health during and following treatment in people with non-advanced colorectal cancer. Cochrane Database Syst Rev. (2020) 5:CD012864. doi: 10.1002/14651858.CD012864.pub2
Keywords: theranostics, cancer therapy, pretargeted therapy, drug delivery, nanomedicine, bioorthogonal click chemistry
Citation: Hapuarachchige S and Artemov D (2020) Theranostic Pretargeting Drug Delivery and Imaging Platforms in Cancer Precision Medicine. Front. Oncol. 10:1131. doi: 10.3389/fonc.2020.01131
Received: 09 December 2019; Accepted: 05 June 2020;
Published: 22 July 2020.
Edited by:
Marie-France Penet, Johns Hopkins University, United StatesReviewed by:
M. Carmen Martinez-Bisbal, University of Valencia, SpainGiulio Fracasso, University of Verona, Italy
Copyright © 2020 Hapuarachchige and Artemov. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sudath Hapuarachchige, c2hhcHVhcjFAamguZWR1