
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 13 August 2019
Sec. Genitourinary Oncology
Volume 9 - 2019 | https://doi.org/10.3389/fonc.2019.00751
This article is part of the Research Topic Optimizing Local Therapy for High-Risk Prostate Cancer: Evidence and Emerging Options View all 13 articles
 Stefan Alexander Koerber1,2,3*
Stefan Alexander Koerber1,2,3* Erik Winter1
Erik Winter1 Sonja Katayama1,2,3
Sonja Katayama1,2,3 Alla Slynko4Matthias Felix Haefner1,2,3
Alla Slynko4Matthias Felix Haefner1,2,3 Matthias Uhl1,2,3Florian Sterzing1,5Gregor Habl1,6Kai Schubert1Juergen Debus1,2,3,7,8,9Klaus Herfarth1,2,3,7
Matthias Uhl1,2,3Florian Sterzing1,5Gregor Habl1,6Kai Schubert1Juergen Debus1,2,3,7,8,9Klaus Herfarth1,2,3,7Introduction: This prospective, non-randomized phase II trial aimed to investigate the role of additional irradiation of the pelvic nodes for patients with prostate cancer and a high risk for nodal metastases using helical intensity-modulated radiotherapy with daily image guidance (IMRT/IGRT).
Methods and materials: Between 2009 and 2012, 40 men with treatment-naïve prostate cancer and a risk of lymph node involvement of more than 20% were enrolled in the PLATIN-1 trial. All patients received definitive, helical IMRT of the pelvic nodes (total dose of 51.0 Gy) with a simultaneous integrated boost (SIB) to the prostate (total dose of 76.5 Gy) in 34 fractions. Antihormonal therapy (AHT) was administered for a minimum of 2 months before radiotherapy continuing for at least 24 months.
Results: After a median follow-up of 71 months (range: 5–95 months), pelvic irradiation was associated with a 5-year overall survival (OS) and biochemical progression-free survival (bPFS) of 94.3% and 83.6%, respectively. For our cohort, no grade 4 gastrointestinal (GI) and genitourinary (GU) toxicity was observed. Quality of life (QoL) assessed by EORTC QLQ-C30 questionnaire was comparable to EORTC reference values without significant changes.
Conclusion: The current trial demonstrates that elective IMRT/IGRT of the pelvic nodes with SIB to the prostate for patients with a high-risk of lymphatic spread is safe and shows an excellent clinical outcome without compromising the quality of life. The PLATIN-1 trial delivers eminent baseline data for future studies using modern irradiation techniques.
With an estimated incidence of 164,690 new prostate cancer cases in the United States in 2018, carcinoma of the prostate remains the most common malignancy in men (1). For intermediate and high-risk disease according to d'Amico criteria (2), surgery or radiotherapy are available curative, definitive treatment options. Although survival rates are much better compared to other malignant tumors, biochemical relapse occurred in a substantial proportion of patients. For dose-escalated irradiation, prostate-specific antigen (PSA) progression was reported in up to 35% of patients with intermediate or high-risk prostate cancer after 5 years (3). Many patients were diagnosed with lymph node metastases which are usually not included in the initial radiation field. Results from prostate-specific membrane antigen (PSMA) imaging showed positive, pelvic lymph nodes in up to 43.7% (4). Therefore, many studies focused on the role of whole pelvic radiotherapy (WPRT) including pelvic nodes. In 2003, Roach et al. observed a statistically significant improved progression-free survival for patients undergoing WPRT plus neoadjuvant and concurrent hormonal therapy (NCHT) in comparison with prostate-only irradiation (POI) (5). However, the benefit lost the level of significance with longer follow-up (6). This trial and several studies using more conventional radiation techniques reported on acute and/ or late gastrointestinal (GI) and genitourinary (GU) toxicities which occurred more frequently compared to POI (7–9). Moreover, there are some other trials questioning the clinical benefit of WPRT (10, 11).
By integration of modern radiation techniques like intensity-modulated radiotherapy (IMRT), a reduction of acute and late toxicities seems to be possible (12–14). The PLATIN-1 (Prostate and Lymph Node Irradiation with Integrated-Boost-IMRT after neoadjuvant hormonal therapy [NHT]) trial evaluates the role of modern IMRT/ image-guided radiotherapy (IGRT) technique for treatment-naïve prostate cancer patients undergoing optimized WPRT. By using a moderately hypofractionated, simultaneous integrated boost (SIB) to the prostate, the current study also analyzes the influence of moderate hypofractionation on biological effectiveness in a definitive treatment setting after NHT (15). The present article reports on late toxicity and clinical outcome of this cohort.
The present study was approved by the local ethics review board (S-034/2009). In total, 40 men with treatment-naïve and histologically proven prostate cancer were prospectively enrolled in the PLATIN-1 trial between May 2009 and December 2012. All patients had no suspicious lymph node in pelvic computed tomography (CT) or magnetic resonance imaging (MRI) and an estimated risk of pelvic lymph node involvement exceeding 20% according to the Roach formula {2/3 PSA + [(GS−6) × 10]}(16). Antihormonal therapy (AHT) was authorized for all patients and consisted of a minimum of 2 months neoadjuvant treatment and the advice of continuation for at least 24 months after irradiation if tolerated. AHT included luteinizing hormone-releasing hormone (LHRH) agonists or antiandrogen medication.
Treatment planning and radiation were performed as described previously (15). In summary, patients were irradiated once daily and five fractions a week. The prescribed dose of 95% of the planning target volume of the pelvic lymph nodes (PTV-L) was 51.0 Gray (Gy) with a single dose of 1.5 Gy. A simultaneously integrated boost (SIB) of 76.5 Gy was prescribed to 95% of the PTV prostate (PTV-P) with a single dose of 2.25 Gy. Irradiation was performed with helical IMRT/ IGRT using a Tomotherapy® system (Accuray, USA).
Before irradiation, during treatment (weekly) and at the end of the treatment prostate-specific symptoms and treatment toxicity were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Effects (NCI CTCAE) version 3.0. Assessment of QoL using the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire-Core 30 (QLQ-C30) was first performed before treatment. The PSA level was assessed every 3 months. The follow-up schedule included visits at 2.5, 6, 12, 18, and 24 months including toxicity records and QoL records (performed only at 6, 12, and 24 months). Patients were regularly followed thereafter based on local standard operating procedures. This included measurement of PSA levels and toxicity assessment. The median follow-up was 71 months.
The primary objective was the examination of biochemical progression-free survival (bPFS), clinical relapse-free survival (cRFS) and overall survival (OS) for patients suffering from non-metastatic prostate cancer undergoing both IGRT/IMRT and AHT. Furthermore, the secondary objectives were to examine late toxicity and prostate specific symptoms. Biochemical failure was defined according to the Phoenix criteria (17), clinical failure was defined as the existence of local recurrence or metastases detected by CT including PET-CT, MRI or bone scan, which were performed after clinical evidence based on symptoms. The Kaplan-Meier method was used for calculating bPFS, cRFS, and OS.
All statistical analyses were performed by using SPSS v.25.0 and a P-Value of < 0.05 was defined as significant.
Due to an increase of PSA levels during NHT, two patients were excluded from the study before radiotherapy. The patient's characteristics of the remaining 38 were previously described by Habl et al. (15). Median age was 70.5 years with a range of 51–75 years. According to the Roach formula, a risk of LNI of more than 40% was calculated for 6 patients (15.8%) of the cohort while 32 patients (84.2%) had a risk of 20–40%. Twenty-seven patients (71.1%) received LHRH agonists, seven patients (18.4%) antiandrogen therapy (bicalutamide) and four patients (10.5%) both (complete androgen deprivation). Only 8 patients (21.1%) received AHT for the required period of 24 to 36 months. Twelve patients (31.6%) stopped AHT within 6 to 24 months of follow-up, 13 patients (34.2%) after a maximum period of 5 months (including NHT) due to intolerance or side effects. AHT was continued for five patients (13.2%) until the current evaluation (Table 1). For all patients, irradiation was performed as specified in the protocol.
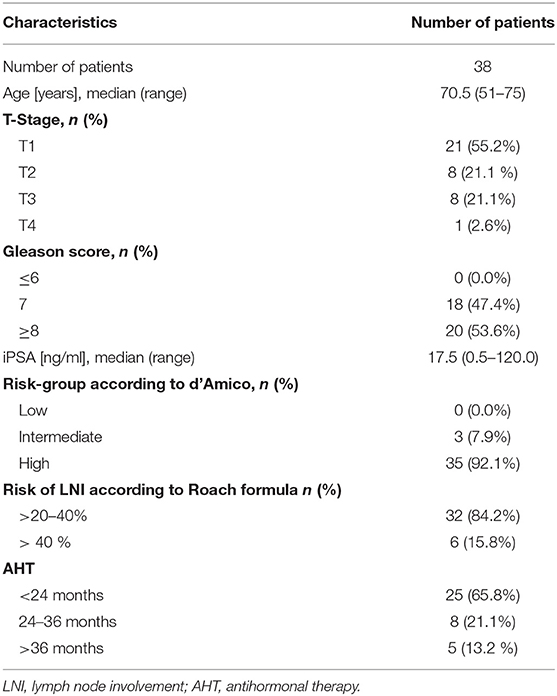
Table 1. Patient's characteristics.
After a median follow-up of 71 months (range: 5–95 months), 34 out of 38 patients (89.5%) were still alive. One patient died almost 7 months after irradiation due to a newly diagnosed, metastasized esophageal cancer. One patient died after 61 months due to cardiac disease, another after 44 months due to acute myeloic leukemia. For one patient, the reason for death is unknown. The 2-year and 5-year overall survival (OS) rates were 97.3% (95% confidence interval [CI] 96.4–98.2%) and 94.3% (95% CI 93.1-95.6%), respectively (Figure 1). In 21.5% (8 patients) of the cohort, a biochemical relapse occurred. For four patients with PSA relapse, further imaging with MRI, CT and/ or bone scan was performed. One patient was diagnosed with local recurrence, two patients with bone metastases. No nodal relapse within the pelvis occurred. A biochemical progression-free survival (bPFS) of 89.2% (95% CI 87.6–90.8%) and 83.6% (95% CI 81.6–85.6%) was observed at 2 and 5 years, respectively (Figure 2).
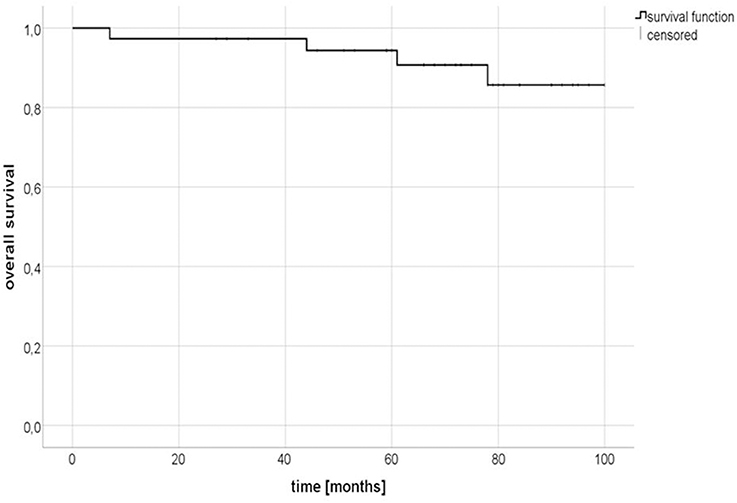
Figure 1. Kaplan-Meier estimates of overall survival (OS).
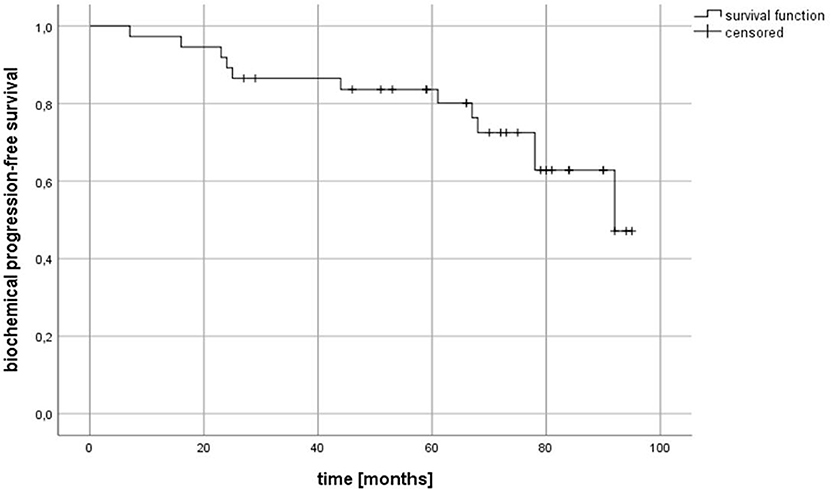
Figure 2. Kaplan-Meier estimates of biochemical progression-free survival (bPFS).
At the time of last follow-up, toxicity data were available for 29 patients. We observed no grade 3 and 4 late toxicity with regard to gastrointestinal (GI) side effects. Two men (5.3%) reported on grade 1 enteritis, one patient (2.6%) on grade 2 enteritis with pain and moderate bleedings. No proctitis or diarrhea occurred in our cohort at the time of follow-up.
For patients undergoing helical IMRT, there was no grade 4 genitourinary (GU) toxicity. The cumulative incidence of grade 3 urinary side effects was 2.6% including one patient with stress incontinence. Urge incontinence occurred for 9 patients (23.7%; grade 1) and 3 patients (7.9%; grade 2), respectively. Only one patient (2.6%) reported on a light cystitis (grade 1). Without current AHT, five patients (13.1%) reported on grade 2/3 erectile dysfunction, while grade 2/3 loss of libido was found for 16 patients (42.1%). Two patients (5.3%) were identified with grade 1 edema and three patients (7.9%) with grade 2 edema at the time of follow-up. No grade 3 or 4 edema was observed for the entire cohort (Table 2).
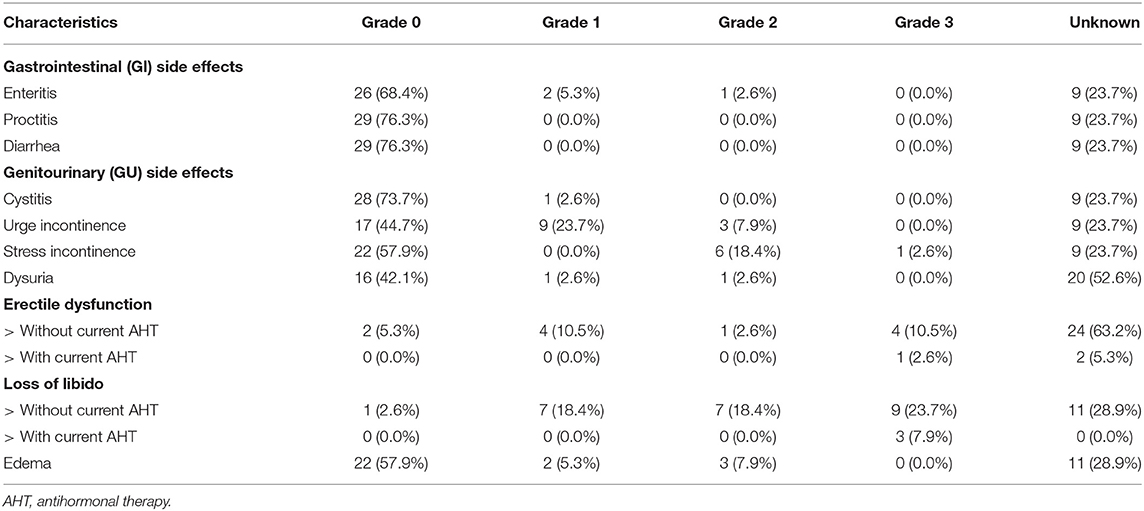
Table 2. Late toxicity (median follow up: 71 months; n = 38).
After a median follow-up of 71 months, IMRT/ IGRT of the prostate and pelvic nodes continued to be well-tolerated without excessive side effects. For our cohort of 38 men treated in the present study, no severe (grade 3/4) GI toxicity occurred. The Genitourinary Study Group (GETUG)-1 trial – one of the largest prospective studies investigating the role of pelvic node irradiation–reported on a grade 3/4 toxicity rate for the digestive tract of 10.7% after a median follow-up of 42.1 months. In this trial, irradiation was performed with a four-field box to a total dose of 46 Gy to the pelvis and a maximum of 70 Gy to the prostate (10). Although total dose to the prostate was lower compared to our PLATIN-1 trial according to former guidelines, the reduced number of side effects in the present study can be explained by the use of modern treatment techniques like IMRT in combination with daily imaging (IGRT). This is in accordance with other studies using IMRT: Pervez et al. observed no grade 3/4 late GI toxicity in a group of 60 patients undergoing irradiation of the pelvic nodes and prostate (total dose: 45/68 Gy) in 25 fractions at 5 years follow-up timepoint (18). Similar results were described for GU side effects, however, a direct comparison is difficult due to a lack of detailed data in the majority of other reports and a limited number of feedbacks in our cohort. In the present study, 68.9% of the patients were unwilling or unable to provide any information about their erectile function. Nevertheless, in addition to the reported grade 2/3 erectile dysfunction rate of 14.3% for the current study, a high number of genital constraints might automatically result from AHT and the increasing age of the patients. In the Prostate Testing for Cancer and Treatment (ProtecT) trial, a group of 1,643 men with a median age of 62 years was included. At 72-months follow up, erection not firm enough for intercourse was found for 73% in the radiotherapy compared to 70% in the active surveillance (AS) group (19). Even watchful waiting caused similar limitations in 80% of men in the Scandinavian Prostate Cancer Group-4 at 144-months follow-up, although the median age of this cohort was also younger (64 years) than that of the present PLATIN-1 trial (70.5 years) (20). Age might the relatively high rate of incontinence in our cohort. In total, 21% reported on grade 2/3 stress incontinence while urge incontinence was observed for 7.9% at the time of follow-up. In a phase 1/2 dose-escalation study from UK, the 2-year cumulative rates of grade 2+/grade 3+ bladder toxicity were 4.2%/ 4.2% (cohort 1), respectively. This study investigated the role of IMRT to the prostate (total dose of 70 to 74 Gy) and pelvic lymph nodes (total dose for cohort 1: 50 Gy) including 25 patients with prostate cancer (21). However, our cohort also showed high rates of incontinence before irradiation. Almost 16 % of men included in the PLATIN-1 trial complained about grade 1/2 incontinence at baseline. Overall quality of life assessed by the EORTC QLQ-C30 questionnaire remained largely stable at 71-months follow-up. Global health score was 68.1, which is in accordance with EORTC reference values of prostate cancer patients. Compared to month 24, there was a significant improvement of global health status (15). One explanation might be that also protracted, radiotherapy-related symptoms disappeared and AHT was finished for almost all patients. Our observations are at least comparable to a recent report published by Lips et al. comparing QoL in patients with locally advanced prostate cancer after 76 Gy IMRT vs. 70 Gy conformal radiotherapy. The authors concluded that dose-escalated IMRT/ IGRT can be performed without deterioration in QoL (22). The expansion of the target volume by adding pelvic lymph nodes also seems to cause no substantial change, if modern radiation technique is used. At least in our cohort of 38 men undergoing helical IMRT, no significant variations for QoL scores were observed compared to reference values.
However, one crucial question remains: Is there an oncological benefit for pelvic node irradiation in non-metastatic patients with prostate cancer? While several retrospective and small prospective studies report on promising results (9, 18, 21, 23–25), two randomized phase III trials failed to show an improved survival for patients undergoing pelvic irradiation (Table 3): The last update of the GETUG-01 randomized study evaluating 446 men with prostate carcinoma summarized, that pelvic nodes irradiation was not able to improve event-free survival (EFS) or OS after a median follow-up of 11.4 years (11). For the RTOG 9413 cohort including 1,322 patients, an improved PFS was observed for NHT plus WPRT compared with NHT plus prostate-only radiotherapy (PORT) and WPRT and adjuvant hormonal therapy after a median follow-up of 8.8 years. Nevertheless, WPRT did not show an improvement in OS compared to PORT while leading to an increased risk of grade 3 or worse GI toxicity with the use of conventional four-field technique (6). In the present trial, IMRT/ IGRT of the pelvic lymph nodes with a simultaneous integrated boost to the prostate achieved no nodal relapse and excellent 5-year bPFS and OS of 83.6% and 94.3% considering the high rate of high-risk patients and short-term (<24 months) AHT. Although the PLATIN-1 trial was a prospective trial using modern radiation technique, the current study was not powered to provide sufficient data regarding oncological outcome. Due to the small number of patients, the non-randomized setting and a certain number of men with only short-term AHT–major limitations of our study—there is still a lack of evidence regarding prophylactic irradiation of pelvic nodes for patients with prostate cancer. Both, the GETUG-01 and the RTOG 9413 were not able to show a general benefit for WPRT, however, from today's view several parameters could limit the results of them: Besides broad inclusion criteria (GETUG-01) and a low total dose according to former guidelines, the four-field technique without image guidance could have resulted in insufficient doses within some areas like the presacral or external iliac nodes. Therefore, the present PLATIN-1 trial formed a solid basis for ongoing trials using modern photon or proton irradiation and was an important contribution to evaluate prophylactic pelvic node irradiation using IMRT/ IGRT, but more evidence is needed about whether or not an expanded target volume is beneficial to men with non-metastatic, high-risk prostate cancer. With the end of recruitment for one upcoming study, the RTOG 0924 trial, expected by late summer 2019 (6), further information should be available.
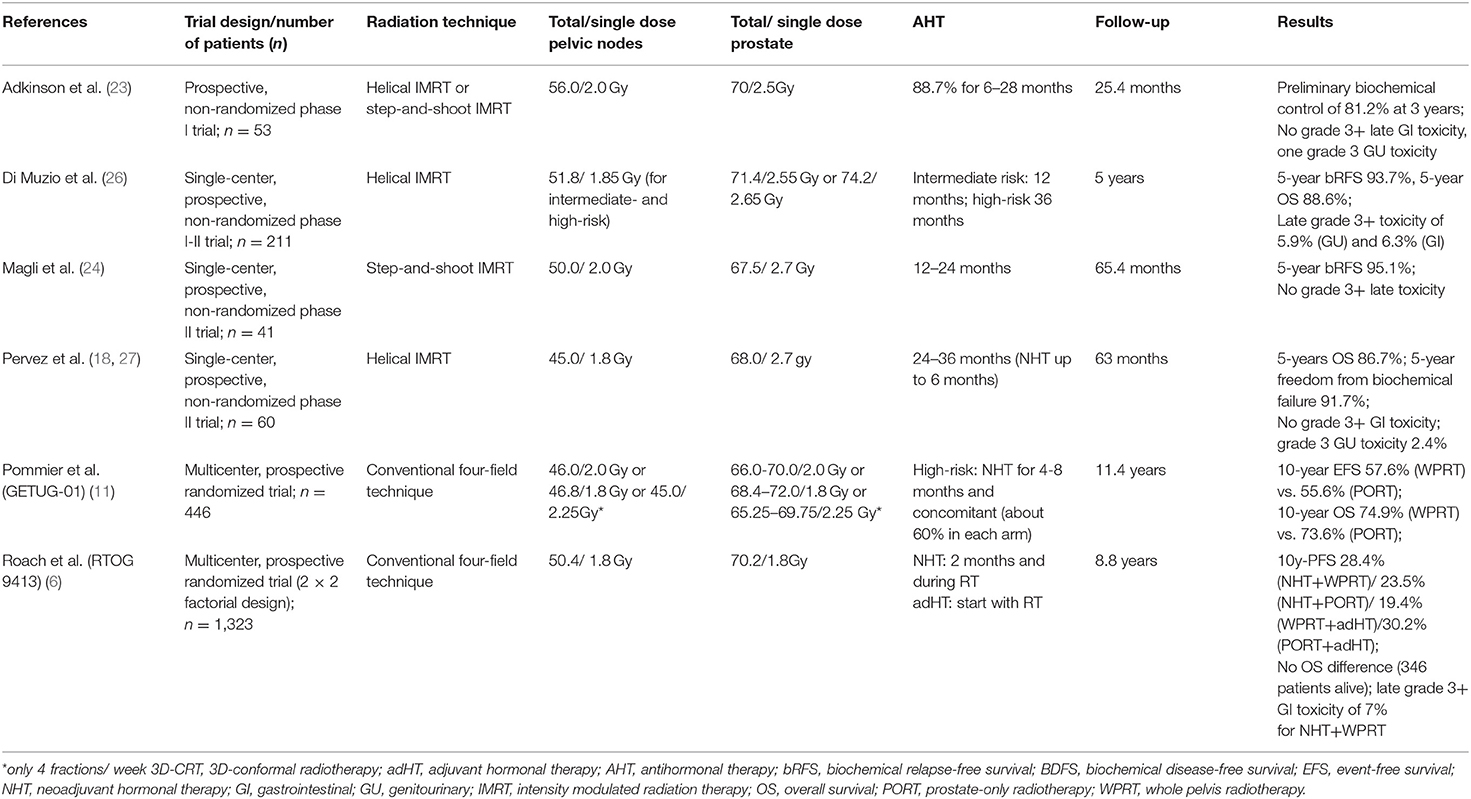
Table 3. Overview of prospective trials evaluating the role of WPRT.
In summary, the present PLATIN-1 trial confirms that helical IMRT of the pelvic nodes with a simultaneous integrated boost to the prostate can be performed without severe toxicity and significant deterioration in QoL. Even when our trial achieved excellent oncological outcome, there is still a need for further randomized studies evaluating the role of prophylactic, pelvic irradiation for patients with prostate carcinoma and a high risk for LNI.
All datasets generated for this study are included in the manuscript/supplementary files.
SAK and EW were the main investigators who collected and evaluated the clinical information. AS conducted the statistical analysis and critically evaluated the paper. SK, MH, MU, FS, and GH assisted the main author in patient enrollment, data collection and revising the final draft. The paper was wrote by SAK and critically evaluated by KS, KH, and JD. KH and JD designed and supervised the prospective trial. All authors read and approved the final version of the paper.
The PLATIN trial was supported by the Tschira Foundation (project number 00.153.2009).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors gratefully acknowledge the radiation oncology study office, especially Renate Haselmann and Alexandros Gioules, for their great support. Furthermore, we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding programme Open Access Publishing, by the Baden-Württemberg Ministry of Science, Research and the Arts and by Ruprechts-Karls-Universität Heidelberg.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. (2018) 68:7–30. doi: 10.3322/caac.21442
2. D'Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. (1998) 280:969–74. doi: 10.1001/jama.280.11.969
3. Peeters ST, Heemsbergen WD, Koper PC, van Putten WL, Slot A, Dielwart MF, et al. Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J Clin Oncol. (2006) 24:1990–6. doi: 10.1200/JCO.2005.05.2530
4. Koerber SA, Will L, Kratochwil C, Haefner MF, Rathke H, Kremer C, et al. 68Ga-PSMA-11 PET/CT in primary and recurrent prostate carcinoma: implications for radiotherapeutic management in 121 patients. J Nucl Med. (2018) pii: jnumed.118.211086. doi: 10.2967/jnumed.118.211086
5. Roach M, DeSilvio M, Lawton C, Uhl V, Machtay M, Seider MJ, et al. Phase III trial comparing whole-pelvic versus prostate-only radiotherapy and neoadjuvant versus adjuvant combined androgen suppression: radiation therapy oncology group 9413. J Clin Oncol. (2003) 21:1904–11. doi: 10.1200/JCO.2003.05.004
6. Roach M, Moughan J, Lawton CAF, Dicker AP, Zeitzer KL, Gore EM, et al. Sequence of hormonal therapy and radiotherapy field size in unfavourable, localized prostate cancer (NRG/RTOG 9413): long-term results of a randomized, phase 3 trial. Lancet Oncol. (2018) 19:1504–15. doi: 10.1016/S1470-2045(18)30528-X
7. Perez CA, Lee HK, Georgiou A, Lockett MA. Technical factors affecting morbidity in definitive irradiation for localized carcinoma of the prostate. Int J Radiat Oncol Biol Phys. (1994) 28:811–9. doi: 10.1016/0360-3016(94)90100-7
8. Zelefsky MJ, Leibel SA, Gaudin PB, Kutcher GJ, Fleshner NE, Venkatramen ES, et al. Dose escalation with three-dimensional conformal radiation therapy affects the outcome in prostate cancer. Int J Radiat Oncol Biol Phys. (1998) 41:491–500. doi: 10.1016/S0360-3016(98)00091-1
9. Aizer AA, Yu JB, McKeon AM, Decker RH, Colberg JW, Peschel RE. Whole pelvic radiotherapy versus prostate only radiotherapy in the management of locally advanced or aggressive prostate adenocarcinoma. Int J Radiat Oncol Biol Phys. (2009) 75:1344–9. doi: 10.1016/j.ijrobp.2008.12.082
10. Pommier P, Chabaud S, Lagrange JL, Richaud P, Lesaunier F, Le Prise E, et al. Is there a role for pelvic irradiation in localized prostate adenocarcinoma? Preliminary results of GETUG-01. J Clin Oncol. (2007) 25:5366–73. doi: 10.1200/JCO.2006.10.5171
11. Pommier P, Chabaud S, Lagrange JL, Richaud P, Le Prise E, Wagner JP, et al. Is there a role for pelvic irradiation in localized prostate adenocarcinoma? update of the long-term survival results of the GETUG-01 randomized study. Int J Radiat Oncol Biol Phys. (2016) 96:759–69. doi: 10.1016/j.ijrobp.2016.06.2455
12. Ashman JB, Zelefsky MJ, Hunt MS, Leibel SA, Fuks Z. Whole pelvic radiotherapy for prostate cancer using 3D conformal and intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys. (2005) 63:765–71. doi: 10.1016/j.ijrobp.2005.02.050
13. Zelefsky MJ, Levin EJ, Hunt M, Yamada Y, Shippy AM, Jackson A, et al. Incidence of late rectal and urinary toxicities after three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys. (2008) 70:1124–9. doi: 10.1016/j.ijrobp.2007.11.044
14. Katayama S, Habl G, Kessel K, Edler L, Debus J, Herfarth K, et al. Helical intensity-modulated radiotherapy oft he pelvic lymph nodes with integrated boost to the prostate bed – initial results oft he PLATIN 3 Trial. BMC Cancer. (2014) 14:20. doi: 10.1186/1471-2407-14-20
15. Habl G, Katayama S, Uhl M, Kessel KA, Edler L, Debus J, et al. Helical intensity-modulated radiotherapy of the pelvic lymph nodes with a simultaneous integrated boost to the prostate–first results of the PLATIN 1 trial. BMC Cancer. (2015) 15:868. doi: 10.1186/s12885-015-1886-5
16. Roach M, Marquez C, Yuo HS, Narayan P, Coleman L, Nseyo UO, et al. Predicting the risk of lymph node involvement using the pre-treatment prostate specific antigen and Gleason score in men with clinically localized prostate cancer. Int J Radiat Oncol Biol Phys. (1994) 28:33–7. doi: 10.1016/0360-3016(94)90138-4
17. Horwitz EM, Thames HD, Kuban DA, Levy LB, Kupelian PA, Martinez AA, et al. Definitions of biochemical failure that best predict clinical failure in patients with prostate cancer treated with external beam radiation alone a multi-institutional pooled analysis. J Urol. (2005) 173:797–802. doi: 10.1097/01.ju.0000152556.53602.64
18. Pervez N, Boychak A, Drodge CS, Yee D, Le D, Murtha A, et al. Late toxicity and outcomes in high-risk prostate cancer patients treated with hypofractionated IMRT and long-term androgen suppression treatment. Am J Clin Oncol. (2017) 40:200–6. doi: 10.1097/COC.0000000000000133
19. Donovan JL, Hamdy FC, Lane JA, Mason M, Metcalfe C, Walsh E, et al. Patient-reported outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med. (2016) 375:1425–37. doi: 10.1056/NEJMoa1606221.
20. Johansson E, Steineck G, Holmberg L, Johansson JE, Nyberg T, Ruutu M, et al. Long-term quality-of-life outcomes after radical prostatectomy or watchful waiting the Scandinavian Prostate Cancer Group-4 randomised trial. Lancet Oncol. (2011) 12:891–9. doi: 10.1016/S1470-2045(11)70162-0
21. Reis Ferreira M, Khan A, Thomas K, Truelove L, McNair H, Gao A, et al. Phase 1/2 dose-escalation study of the use of intensity modulated radiation therapy to treat the prostate and pelvic nodes in patients with prostate cancer. Int J Radiat Oncol Biol Phys. (2017) 99:1234–42. doi: 10.1016/j.ijrobp.2017.07.041
22. Lips I, Dehnad H, Kruger AB, van Moorselaar J, van der Heide U, Battermann J, et al. Health-related quality of life in patients with locally advanced prostate cancer after 76 Gy intensity-modulated radiotherapy vs. 70 Gy conformal radiotherapy in a prospective and longitudinal study. Int J Radiat Oncol Biol Phys. (2007) 69:656–61. doi: 10.1016/j.ijrobp.2007.04.013
23. Adkison JB, McHaffie DR, Bentzen SM, Patel RR, Khuntia D, Petereit DG, et al. Phase I trial of pelvic nodal dose escalation with hypofractionated IMRT for high-risk prostate cancer. Int J Radiat Oncol Biol Phys. (2012) 82:184–90. doi: 10.1016/j.ijrobp.2010.09.018
24. Magli A, Moretti E, Tullio A, Giannarini G, Tonetto F, Urpis M, et al. Hypofractionated simultaneous integrated boost (IMRT-SIB) with pelvic nodal irradiation and concurrent androgen deprivation therapy for high-risk prostate cancer results of a prospective phase II trial. Prostate Cancer Prostatic Dis. (2018) 21:269–76. doi: 10.1038/s41391-018-0034-0
25. Mantini G, Tagliaferri L, Mattiucci GC, Balducci M, Frascino V, Dinapoli N, et al. Effect of whole pelvic radiotherapy for patients with locally advanced prostate cancer treated with radiotherapy and long-term androgen deprivation therapy. Int J Radiat Oncol Biol Phys. (2011) 81:e721–6. doi: 10.1016/j.ijrobp.2010.12.003
26. Di Muzio NG, Fodor A, Noris Chiorda B, Broggi S, Mangili P, Valdagni R, et al. Moderate hypofractionation with simultaneous integrated boost in prostate cancer: long-term results of a phase I-II study. Clin Oncol. (2016) 28:490–500. doi: 10.1016/j.clon.2016.02.005
Keywords: prostate cancer, radiotherapy, pelvic nodes, IMRT, tomotherapy®, simultaneous integrated boost, elective node irradiation
Citation: Koerber SA, Winter E, Katayama S, Slynko A, Haefner MF, Uhl M, Sterzing F, Habl G, Schubert K, Debus J and Herfarth K (2019) Elective Node Irradiation With Integrated Boost to the Prostate Using Helical IMRT–Clinical Outcome of the Prospective PLATIN-1 Trial. Front. Oncol. 9:751. doi: 10.3389/fonc.2019.00751
Received: 22 May 2019; Accepted: 26 July 2019;
Published: 13 August 2019.
Edited by:
Timothy Showalter, School of Medicine, University of Virginia, United StatesReviewed by:
Vadim S. Koshkin, University of California San Francisco, United StatesCopyright © 2019 Koerber, Winter, Katayama, Slynko, Haefner, Uhl, Sterzing, Habl, Schubert, Debus and Herfarth. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefan Alexander Koerber, c3RlZmFuLmtvZXJiZXJAbWVkLnVuaS1oZWlkZWxiZXJnLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.