 Louis Garnier1*
Louis Garnier1* François Ducray2
François Ducray2 Clotilde Verlut3Marcella-Ionela Mihai4
Clotilde Verlut3Marcella-Ionela Mihai4 Françoise Cattin5
Françoise Cattin5 Antoine Petit6Elsa Curtit1
Antoine Petit6Elsa Curtit1- 1Department of Medical Oncology, University Hospital of Besançon, Besançon, France
- 2Department of Neuro-Oncology, Hospices Civils de Lyon, Lyon, France
- 3Department of Neurology, University Hospital of Besançon, Besançon, France
- 4Department of Pathology, University Hospital of Besançon, Besançon, France
- 5Department of Radiology, University Hospital of Besançon, Besançon, France
- 6Department of Neurosurgery, University Hospital of Besançon, Besançon, France
Spinal ganglioglioma is a rare low-grade, slow-growing tumor of the central nervous system affecting mostly children and young adults. After surgery, some patients show tumor recurrence and/or malignant transformation. Gangliogliomas harbor molecular deficiencies such as mutations in the B-rapidly accelerated fibrosarcoma (BRAF) gene, resulting in activation of a downstream signaling pathway and cancer development. Vemurafenib is a BRAF inhibitor used to treat patients with BRAF V600E-mutated cancer. Although a few studies have reported the clinical responses in gangliogliomas, the sequence and duration of treatment have not been established. We describe a case of an adult with a progressive BRAF V600E mutant spinal cord ganglioglioma 9 years after surgery who was treated with vemurafenib. This treatment resulted in a partial response within 2 months, which was sustained for more than a year. The patient then decided to stop treatment because of side effects. Despite this decision, the tumor showed no sign of progression 21 months after treatment discontinuation. This is the first reported case of a response to vemurafenib in an adult with progressive spinal cord BRAF V600E-mutated ganglioglioma which was sustained after treatment discontinuation.
Introduction
Ganglioglioma is a neuronal tumor representing 1% of all primary brain tumors and nearly 5% of pediatric and young adult central nervous system tumors. Histologically, ganglioglioma is composed of both neoplastic neuronal cells and neoplastic glial cells. The glial cells contingent includes astrocyte cells with atypia (1). Most (>90%) gangliogliomas are classified as grade I according to the 2016 World Health Organization (WHO) classification and are genetically defined by multiple alterations (2). Ganglioglioma are typically located in the brain, most often in the temporal lobe and rarely in the spinal cord (3). The cornerstone of curative treatment for ganglioglioma is total surgical resection. The prognosis depends on the quality of surgery (4–9). Complete resection is not always possible, frequently because of the proximity of eloquent structures or vessels. Moreover, even after imaging-confirmed complete resection, recurrence can occur (10).
Treatment strategies are limited for recurrent disease. Radiotherapy has been indicated for high-grade or incompletely resected low-grade ganglioglioma, but these recommendations are not based on high scientific levels of evidence (4, 5, 11–15). Some cases of malignant transformation after radiotherapy have been reported (16, 17). Chemotherapy and systemic therapy are not recommended in the clinical routine and can be discussed on a case-by-case basis after the failure of local therapies (5, 15).
BRAF is located on chromosome 7 (7q34) and encodes B-raf, a serine/threonine protein kinase that mediates the cellular response to growth signals (18). B-raf is a member of the Ras/Raf/MEK/ERK/MAP kinase pathway, which is frequently activated in human cancers. More than 30 mutations have been detected in BRAF. One of the mutational hot spots of BRAF is at nucleotide 1799; mutations at this site lead to the exchange of valine with glutamate at amino acid position 600. The BRAF V600E mutant constitutively activates downstream signaling pathways. The BRAF V600E mutation occurs in 10–60% of gangliogliomas depending on the study and anatomic site, with lower frequency in the spinal cord (2, 19–21). This mutation appears to be associated with lower recurrence-free survival (22). Therefore, MAPK pathway inhibition is an attractive treatment option for recurrent or high-grade ganglioglioma (23).
Vemurafenib is a competitive small-molecule serine–threonine kinase inhibitor that functions by binding to the ATP-binding domain of mutant BRAF. Vemurafenib was first licensed for the treatment of advanced melanoma (24). Its administration is now known to be safe and effective for melanoma brain metastases and can result in tumor regression (25). Some case reports have shown an objective tumor response to BRAF inhibitor treatment alone or in combination with chemotherapy or targeted therapy in pediatric and young adult BRAF V600E gangliogliomas (26–37). However, there are no reports of a prolonged response to monotherapy with vemurafenib in an adult with progressive grade I ganglioglioma. There is a lack of data regarding the use of vemurafenib in gangliogliomas. Particularly, it is unknown how long this treatment should be administered in responding patients. Herein, we describe a case of successful treatment with vemurafenib in a patient with a BRAF V600E-mutated progressive cervical spinal cord ganglioglioma, with a stable disease 21 months after treatment discontinuation.
Case Report Presentation
Clinical History and Histological Findings
A 22-year-old male referred to the emergency department in July 2006 for fluctuating paresthesia with motor dysfunction of the left arm and leg associated with cervical pain, which had been evolving for 1 year. Otherwise, his medical clinical history was unremarkable. Magnetic resonance imaging (MRI) of the spine revealed a suspicious lesion within the left spinal cord at the levels of C3–C5. The patient underwent subtotal resection in August 2006. An MRI of the spine 1 month following surgery showed a residual tumor of 27 × 8 mm with strong patchy enhancement following gadolinium administration within the left spinal cord at the level of the bottom of C3 to the top of C5, isointense T1 signal, and heterogeneously hyperintense T2 signal. There was an associated syringomyelia at the rostral and caudal aspects of the enhancing tumor, mostly from C2 to C7. Moreover, T2 hyperintensity was observed in the spinal cord above and below the syringomyelia without associated enhancement (Figure 1).
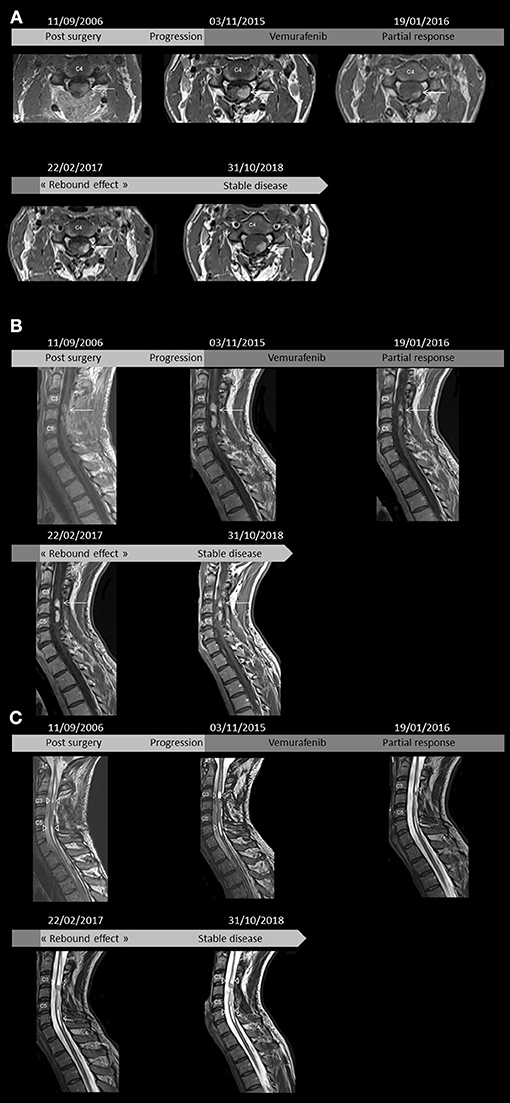
Figure 1. Axial T1-weighted images between C3 and C4 of T1-weighted cervical spine magnetic resonance imaging (MRI) after gadolinium injection administration show dominant, patchy intense enhancing left-sided lesion within the spinal cord (arrows) 1 month after surgery, in pre-treatment with vemurafenib, 8 weeks after the beginning of vemurafenib, 2 months after vemurafenib discontinuation, and last follow-up (A). Sagittal post contrast T1-weighted images revealed lesions between C3 and C4 as well as C4 and C5 (arrows) 1 month after surgery, in pre-treatment, 8 weeks after beginning treatment, 2 months after discontinuation, and last follow-up (B). Sagittal T2-weighted images showing syringomyelia (arrowheads) rostral and caudal to the intramedullary tumor 1 month after surgery, at pre-treatment, 8 weeks after beginning treatment, 2 months after discontinuation, and last follow-up. Note the T2 hyperintensity in the spinal cord above and below the syringomyelia without associated enhancement (C).
The histological examination of the lesion showed a tissue with mixed glial and neuronal components (Figures 2A,B), the presence of fusiform cells with anisonucleosis, sustained by blood vessels with thickened wall surrounded by lymphocytic cuffs, with eosinophilic granular bodies, and Rosenthal fibers. Binucleated neurons were visualized by calretinine, neurofilament, and synaptophysin staining. Many glial cells showed S100 and CD34 immunoreactivity and diffuse glial fibrillary acidic protein. The Ki-67 labeling index was very low (<1%) and some parts of the tissue were positive for P53 in immunohistochemistry analysis. Molecular analysis revealed immunoreactivity to isocitrate deshydrogenase gene 1 (IDH1 R132H) and a loss of chromosome 9p. Despite the presence of an IDH mutation, central pathological review led to the diagnosis of WHO grade I ganglioglioma (1).
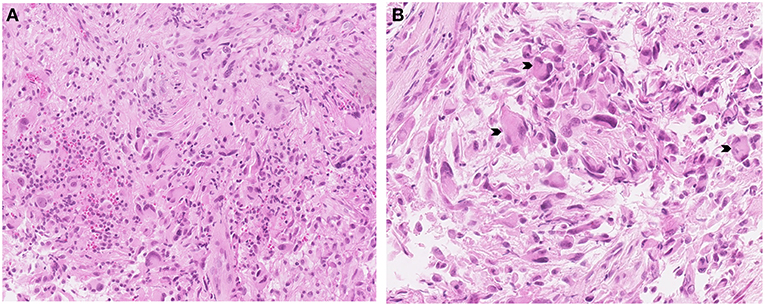
Figure 2. Astrocytic glial cell population with grouped ganglion cells, marked in hematoxylin-Eosin-Saffron staining (original magnification X18) (A), neuronal components characterized by larger numbers of binucleated or multinucleated cells (arrowheads) with a cellular glial background evaluated by hematoxylin-Eosin-Saffron staining (original magnification X28) (B).
Postoperatively, the patient maintained his neurological symptoms and had Brown-Sequard syndrome and micturition dysfunctions.
The patient was followed up with for 9 years until MRI demonstrated tumor progression. Tumor measurements were then 36 × 12 mm, corresponding to a 50% increase in size (Figure 1). At this time, a second resection was considered too risky and gross tumor resection was not possible. No other treatment was administered because of the lack of proof of chemotherapy and radiotherapy interest. This was consistent with increased arm and leg dysfunction.
Gene Testing
Molecular testing for evaluation of target therapy was implemented using tissue collected during surgery after obtaining written informed and signed consent. In July 2015, genomic DNA was extracted from the tumor tissue with a QIAamp® DNA mini Kit (QIAGEN, Hilden, Germany) for standard direct sequencing of exon 15 of BRAF, which was analyzed by using a SNaPshot® kit (Thermo Fisher Scientific, Waltham, MA, USA). The results revealed a V600E BRAF mutation and no mutation in RAS.
Patient Management and Outcomes
Based on these results, in November 2015, the patient was started on vemurafenib 960 mg orally twice daily [100% of the recommended dose in adults for melanoma (24)]. This treatment was determined as part of “AcSé,” a French program known as “Secure access to innovative targeted therapies” (38). After 8 weeks of treatment, the patient was neurologically stable and brain MRI showed a >50% decrease in tumor size (Figure 1). A steady partial response was observed for more than 13 months. Toxicities were measured by the Common Terminology Criteria for Adverse Events v4.0 and included grade I myalgia, arthralgia, and asthenia as well as grade I maculopapular rash (folliculitis with microcysts on legs and arms treated with topical retinoids). After 13 months of treatment, the patient decided to stop the treatment because of grade II photosensibility and other dermatological side effects (Figures 3A–C). To manage his rashes, folliculitis, and microcysts, the patient applied glycerol as a topical emollient, 30% pure urea cream, and Trétinoine (topical retinoid). His palmar-plantar erythrodysesthesia syndrome (hyperkeratosis) was treated with topical fluorouracil/salicylic acid and even curettage for some areas. Photoprotection was achieved by applying sun cream during treatment. No topical steroid was used. His Eastern Cooperative Oncology Group Performance Status decreased to 2 because of grade II asthenia. Two months after stopping treatment, MRI revealed that the disease was stable and had not significantly progressed according to RANO criteria (39) (Figure 1). Six months after stopping vemurafenib, grade I dermatological side effects persisted but the patient had recovered to a normal Performance Status and MRI showed no signs of progression.
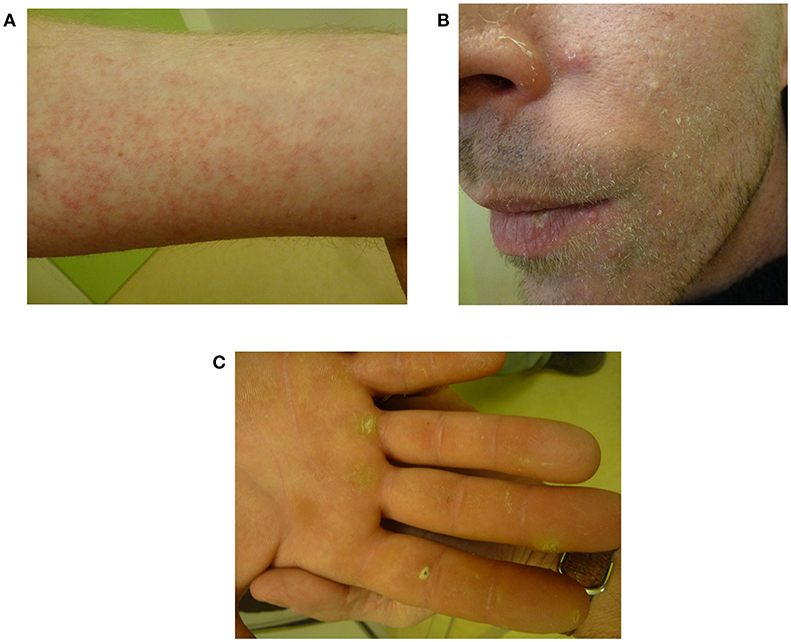
Figure 3. Dermatological toxicities after 13 months of vemurafenib, representing a grade II maculopapular rash (A), microcysts (B), and hyperkeratosis as part of palmar-plantar erythrodysesthesia syndrome (C).
Twenty-one months after vemurafenib discontinuation in October 2018, MRI and neurological examination showed stable disease (Figure 1) and the patient had no side effects. Although the disease is incurable nature, his neurologic and cognitive functions and quality of life were preserved.
Discussion
To our knowledge, this is the first case of an adult with progressive BRAF V600E-mutated spinal ganglioglioma successfully treated with vemurafenib as a single agent and with ongoing and prolonged stable residual disease 21 months after vemurafenib discontinuation.
Epidemiology
The first description of ganglioglioma was detected in 1870 by Loretz and further studied in 1926 by Perkins. Ganglioglioma is a rare tumor of the central nervous system accounting for 1–1.5% of all spinal tumors (4, 40, 41). Gross total resection is the most reliable treatment (10, 42). While the larger part of this disease occurs in the temporal lobe, causing epilepsy (5) and showing a male preference, its spinal location makes treatment difficult, increasing the risk of recurrence (10, 42). Dudley et al. used the large Surveillance Epidemiology and End Results database, which represents nearly one-third of North America's population, and identified 348 children with low-grade gangliogliomas to study their characteristics (8). This was the largest study to evaluate the spinal location of this rare tumor. Spinal cord gangliogliomas represented 3.5% of cases, with nearly 100% of survival at 5 years and the highest percentage of gross total resection of more than 83%.
Imaging Findings
MRI findings for supratentorial ganglioglioma can be divided into three groups: cystic, cystic-solid and solid (43). For intramedullary ganglioglioma, imaging manifestation varied considerably (44). In a recent study of 142 cases, all gangliogliomas in the cervicomedullary junction and all BRAF mutation-positive ganglioglioma were contrast-positive (21). Our case had a solid lesion with patchy enhancement and a cystic component, which was consistent with previous reports (45). Furthermore, the rapid but not significant regrowth of the tumor after treatment discontinuation in our case may be associated with a “rebound effect,” as described previously (30, 37). This is analogous to pseudo-progression. Indeed, pseudo-progression is commonly observed in asymptomatic patients and occurs at weeks and up to 3 months after treatment. However, previous studies showed that pseudo-progression occurs because of radiotherapy and is characterized by transient T1 gadolinium enhancement resulting from breakdown of the blood brain barrier, which typically resolves spontaneously without treatment (46). Pseudo-progression has also been described in patients treated with immunotherapy, but its incidence is unknown because of the lack of available data. In the two previous reports (30, 37), the therapeutic benefit was again achieved after vemurafenib re-introduction. Re-activation of the Ras/Raf/MEK/ERK/MAP kinase pathway may occur, but the biological mechanism remains unclear.
Outcomes and Treatments
In a retrospective review of 58 patients (median age at diagnosis of 8.5 years) who underwent surgical resection, the 5- and 10-year overall survival rates were 89 and 83%, respectively. The spinal cord location was associated with a 3.5-fold increased risk of recurrence compared to cerebral gangliogliomas (47).
The efficacy of chemotherapy for adjuvant or recurrent ganglioglioma is uncertain and remains controversial (48), with a high risk of serious adverse events. Recommendations for the use of radiotherapy at progression are based on case reports and small cohorts, particularly in the spinal cord (49). Radiotherapy may result in a better local control for subtotal resection in the supratentorial location, but does not improve overall survival (4, 5, 11–15). Some case reports even suggested that radiotherapy can result in malignant transformation (16, 17). Based on these reports, we did not treat our patient with radiotherapy or chemotherapy.
Histopathological and Molecular Features
The presence of the BRAF V600E mutation suggests that use of BRAF inhibitors are efficient for treating recurrent gangliogliomas. BRAF mutation appears in 8% of human cancers (50). The BRAF V600E mutation was found more often in pediatric low-grade than in high-grade gliomas (2, 18, 51), likely because low-grade gliomas are the most frequent brain tumors in children (52). Patients with BRAF V600E mutation exhibit shorter progression-free survival (22, 53). However, the prognostic value of this mutation in recent studies is controversial (54). Thereby, Jones et al. suggested that caution should be used when interpreting the BRAF mutations status as an independent prognostic marker (55).
BRAF V600E mutations were detected in nearly 20% of gangliogliomas in a screen of 1,320 nervous system tumors (19). This was the second most frequently BRAF-mutated cerebral tumor entity after pleomorphic xanthoastrocytoma. In another cohort, 50% gangliogliomas were mutated (20). In a recent series, BRAF V600E mutations were detected in 38% of cases but all spinal cord gangliogliomas were wild-type (56). Another group identified only two tumors among 19 (10%) intramedullary gangliogliomas harboring a BRAF V600E mutation (3).
Young adult age, synaptophysin positive tumor, lymphocytic cuffs, and a high Ki67 level (mean 2.5%) have been shown to be associated with the BRAF V600E mutated status (57). However, the results of Ki67 analysis did not reach statistical significance. Moreover, the mutation appears to be present in the neuronal component or both the neuronal and glial components, but never in the glial component alone (5, 57–59). IDH mutations were reported in 8% of cases in a series of 100 gangliogliomas (60). The presence of this mutation was correlated with a greater risk of recurrence and malignant transformation. In the 2016 WHO classification, detection of IDH1 mutation in a tumor resembling a ganglioglioma strongly supported the diagnosis of an infiltrating glioma with ensnared neurons (1, 61). However, as observed in our patient, it has been increasingly recognized that some circumscribed gliomas can harbor mutations typically encountered in diffuse gliomas (such as IDH and histone mutations) (62–65). Occasionally, H3K27M mutations have been reported in midline gangliogliomas (66). In contrast to diffuse gliomas, H3K27M mutations do not appear to be associated with a poor prognosis in circumscribed gliomas. The H3K27M mutation status was not determined in our case.
Ganglioglioma Treated With BRAF Inhibitors: Review of Case Reports
There are some previous descriptions of the efficacy of vemurafenib and dabrafenib (another BRAF inhibitor) in low- and high-grade gliomas other than ganglioglioma (35, 67–71). In a basket study with vemurafenib in BRAF V600E mutation-positive non-melanoma cancers (35), the objective response rate in BRAF-mutant gliomas was 25%. Previously reported cases of gangliogliomas treated with a BRAF inhibitor are listed in Table 1 (26–37). The response to vemurafenib in our patient was consistent with the response to BRAF inhibitors observed in previously reported cases, including one case of spinal ganglioglioma in a 2-year-old child (29). However, all cases except for one were located in the cerebrum or were brainstem gangliogliomas, with half of the cases being anaplastic gangliogliomas (9/19) (28, 32–36). In eight cases (8/19) (26, 27, 32–34, 36, 37), the BRAF inhibitor was associated with another treatment or surgery, making the analysis of the response to the BRAF inhibitor difficult. Based on the analysis of the present case and previously reported cases, a complete response was obtained in 15% (3/20) and partial response in 50% (10/20) of cases at a median of 3.2 months after starting treatment and the estimated progression-free survival was 14 months. In 12 patients in whom a BRAF inhibitor was administered as a single agent, the response rate was 50% (6/12) (one complete response and partial response in all other patients). Additionally, 33% (4/12) showed stable disease and 17% (2/12) showed progressive disease. The estimated progression-free survival was 11 months. The median follow-up time after starting treatment was 14.5 months, while this time period was 36 months in our case, including 21 months of stable disease after discontinuation. The present case is remarkable because our patient had spinal ganglioglioma treated with vemurafenib alone and a long follow-up. Interestingly, 2 months after vemurafenib disruption for patient convenience, a moderate (<25%) increase in the size of the contrast enhancement was observed, after which the tumor remained stable in subsequent MRIs. This rapid but not significant regrowth was consistent with the previous report of a “rebound effect” following vemurafenib disruption after protracted exposure to this treatment (30). In this situation, vemurafenib re-challenge may be effective (30), but the present case suggests that close follow-up is another option, as further tumor progression may not systematically occur. In recent years, BRAF/MEK double blockade with vemurafenib and cobimetinib or dabrafenib and trametinib was shown to be a more effective strategy than targeting BRAF alone in patients with BRAF-mutant advanced melanoma (72). Dual BRAF/MEK inhibition has also been suggested as a promising activity in BRAF-mutant gliomas that may overcome (36, 73) vemurafenib resistance. A prospective study is needed to assess the efficacy of this combination in gangliogliomas.
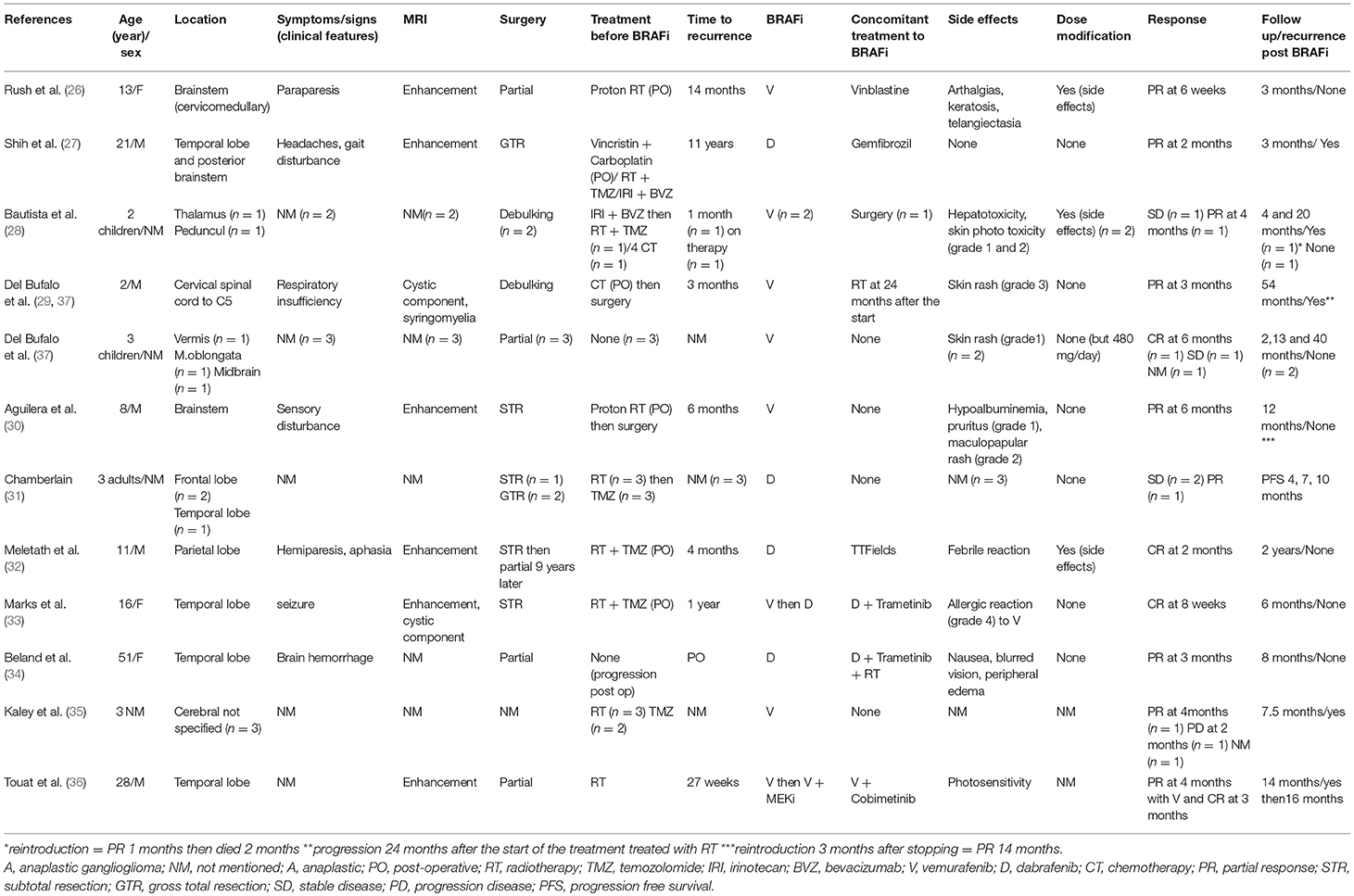
Table 1. Comprehensive list of reported cases of ganglioglioma treated with BRAF inhibitor with reported outcomes.
In our case, the patient asked for treatment discontinuation because of dermatological toxicity. To avoid treatment discontinuation, intermittent dosing could have been used, which has been shown to result in persistent efficacy and improve tolerability as a means of managing BRAF inhibitor toxicity (74). Another possibility may have been switching the patient to another, better-tolerated BRAF inhibitor such as dabrafenib or combining the treatment with an MEK inhibitor which is paradoxically associated with fewer secondary effects than BRAF inhibitors alone (33).
Conclusion
Treatments after surgery for recurrent or progressive spinal cord BRAF V600E-mutated ganglioglioma are scarce and the optimal treatment sequence is unknown. We present a case of a sustained and ongoing response to vemurafenib nearly 2 years after the patient interrupted treatment. In the absence of gold standard management in such cases, the present case suggests that vemurafenib should be considered in BRAF-mutant spinal gangliogliomas requiring treatment other than surgery. The BRAF mutation should be routinely detected in all gangliogliomas even in cases in which IDH mutation suggests diffuse astrocytoma. A safety and pilot efficacy clinical trial of vemurafenib as a single agent against BRAF V600E mutant recurrent or refractory low-grade ganglioglioma in children is ongoing (ClinicalTrials.gov Identifier: NCT01748149). Moreover, the association between the BRAF and MEK inhibitor should be studied in a large cohort, as this treatment may have survival benefits in melanoma (72), and enrollment is currently ongoing for a study of de novo low-grade and relapsed or refractory high-grade gliomas (ClinicalTrials.gov Identifier: NCT02684058 and NCT02124772). Second-generation BRAF and MEK inhibitors are also being evaluated (ClinicalTrials.gov Identifier: NCT02285439 and NCT03429803).
Ethics Statement
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author Contributions
LG participated in the treatment of the patient, did the literature search, and drafted the manuscript. EC and CV instructed and participated in the treatment of the patient. EC and FD provided critical revisions of the manuscript for important intellectual content. M-IM carefully reviewed the pathological findings. FC carefully reviewed the radiology findings. AP carefully reviewed the surgical findings. All authors read and approved the final manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank Prof. François Aubin, Department of dermatology, University Hospital, Besançon, France, for the photos.
References
1. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization classification of tumors of the central nervous System: a summary. Acta Neuropathol. (2016) 131:803–20. doi: 10.1007/s00401-016-1545-1
2. Pekmezci M, Villanueva-Meyer JE, Goode B, Van Ziffle J, Onodera C, Grenert JP, et al. The genetic landscape of ganglioglioma. Acta Neuropathol Commun. (2018) 6:47. doi: 10.1186/s40478-018-0551-z
3. Gessi M, Dörner E, Dreschmann V, Antonelli M, Waha A, Giangaspero F, et al. Intramedullary gangliogliomas: histopathologic and molecular features of 25 cases. Hum Pathol. (2016) 49:107–13. doi: 10.1016/j.humpath.2015.09.041
4. Jallo GI, Freed D, Epstein FJ. Spinal Cord Gangliogliomas: A Review of 56 patients. J Neurooncol. (2004) 68:71–7. doi: 10.1023/B:NEON.0000024747.66993.26
5. Soffietti R, Rudà R, Reardon D. Rare glial tumors. In: Berger MS, Weller M, editors. Handbook of Clinical Neurology (Amsterdam; Oxford, UK; Cambridge, MA: Elsevier), 399–415. doi: 10.1016/B978-0-12-802997-8.00024-4
6. Luyken C, Blümcke I, Fimmers R, Urbach H, Wiestler OD, Schramm J. Supratentorial gangliogliomas: histopathologic grading and tumor recurrence in 184 patients with a median follow-up of 8 years: outcome and prognosis in gangliogliomas. Cancer. (2004) 101:146–55. doi: 10.1002/cncr.20332
7. Compton JJ, Issa Laack NN, Eckel LJ, Schomas DA, Giannini C, Meyer FB. Long-term outcomes for low-grade intracranial ganglioglioma: 30-year experience from the Mayo Clinic: clinical article. J Neurosurg. (2012) 117:825–30. doi: 10.3171/2012.7.JNS111260
8. Dudley RWR, Torok MR, Gallegos DR, Mulcahy-Levy JM, Hoffman LM, Liu AK, et al. Pediatric Low-Grade Ganglioglioma: epidemiology, treatments, and outcome analysis on 348 children from the surveillance, epidemiology, and end results database. Neurosurgery. (2015) 76:313–20. doi: 10.1227/NEU.0000000000000619
9. Haydon DH, Dahiya S, Smyth MD, Limbrick DD, Leonard JR. Greater extent of resection improves ganglioglioma recurrence-free survival in children: a volumetric analysis. Neurosurgery. (2014) 75:37–42. doi: 10.1227/NEU.0000000000000349
10. Khashab ME, Gargan L, Margraf L, Koral K, Nejat F, Swift D, et al. Predictors of tumor progression among children with gangliogliomas: clinical article. J Neurosurg Pediatr. (2009) 3:461–6. doi: 10.3171/2009.2.PEDS0861
11. Liauw SL, Byer JE, Yachnis AT, Amdur RJ, Mendenhall WM. Radiotherapy after subtotally resected or recurrent ganglioglioma. Int J Radiat Oncol. (2007) 67:244–7. doi: 10.1016/j.ijrobp.2006.08.029
12. Rades D, Zwick L, Leppert J, Bonsanto MM, Tronnier V, Dunst J, et al. The role of postoperative radiotherapy for the treatment of gangliogliomas. Cancer. (2010) 116:432–42. doi: 10.1002/cncr.24716
13. Yust-Katz S, Anderson MD, Liu D, Wu J, Yuan Y, Olar A, et al. Clinical and prognostic features of adult patients with gangliogliomas. Neuro Oncol. (2014) 16:409–13. doi: 10.1093/neuonc/not169
14. Celli P, Scarpinati M, Nardacci B, Cervoni L, Cantore GP. Gangliogliomas of the cerebral hemispheres. Report of 14 cases with long-term follow-up and review of the literature. Acta Neurochir. (1993) 125:52–7. doi: 10.1007/BF01401828
15. Majores M, von Lehe M, Fassunke J, Schramm J, Becker AJ, Simon M. Tumor recurrence and malignant progression of gangliogliomas. Cancer. (2008) 113:3355–63. doi: 10.1002/cncr.23965
16. Mittelbronn M, Schittenhelm J, Lemke D, Ritz R, Nägele T, Weller M, et al. Low grade ganglioglioma rapidly progressing to a WHO grade IV tumor showing malignant transformation in both astroglial and neuronal cell components: malignant progression in ganglioglioma. Neuropathology. (2007) 27:463–7. doi: 10.1111/j.1440-1789.2007.00800.x
17. Tarnaris A, O'Brien C, Redfern RM. Ganglioglioma with anaplastic recurrence of the neuronal element following radiotherapy. Clin Neurol Neurosurg. (2006) 108:761–7. doi: 10.1016/j.clineuro.2005.09.005
18. Basto D, Trovisco V, Lopes JM, Martins A, Pardal F, Soares P, et al. Mutation analysis of B-RAF gene in human gliomas. Acta Neuropathol. (2005) 109:207–10. doi: 10.1007/s00401-004-0936-x
19. Schindler G, Capper D, Meyer J, Janzarik W, Omran H, Herold-Mende C, et al. Analysis of BRAF V600E mutation in 1,320 nervous system tumors reveals high mutation frequencies in pleomorphic xanthoastrocytoma, ganglioglioma and extra-cerebellar pilocytic astrocytoma. Acta Neuropathol. (2011) 121:397–405. doi: 10.1007/s00401-011-0802-6
20. Dougherty MJ, Santi M, Brose MS, Ma C, Resnick AC, Sievert AJ, et al. Activating mutations in BRAF characterize a spectrum of pediatric low-grade gliomas. Neuro Oncol. (2010) 12:621–30. doi: 10.1093/neuonc/noq007
21. Janjua MB, Ivasyk I, Pisapia DJ, Souweidane MM. Ganglioglioma of brain stem and cervicomedullary junction: a 50 years review of literature. J Clin Neurosci. (2017) 44:34–46. doi: 10.1016/j.jocn.2017.06.021
22. Dahiya S, Haydon DH, Alvarado D, Gurnett CA, Gutmann DH, Leonard JR. BRAFV600E mutation is a negative prognosticator in pediatric ganglioglioma. Acta Neuropathol. (2013) 125:901–10. doi: 10.1007/s00401-013-1120-y
23. Pfister S, Janzarik WG, Remke M, Ernst A, Werft W, Becker N, et al. BRAF gene duplication constitutes a mechanism of MAPK pathway activation in low-grade astrocytomas. J Clin Invest. (2008) 118:1739–49. doi: 10.1172/JCI33656
24. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, et al. Improved survival with vemurafenib in melanoma with BRAF V600E Mutation. N Engl J Med. (2011) 364:2507–16. doi: 10.1056/NEJMoa1103782
25. Dummer R, Goldinger SM, Turtschi CP, Eggmann NB, Michielin O, Mitchell L, et al. Vemurafenib in patients with BRAFV600 mutation-positive melanoma with symptomatic brain metastases: Final results of an open-label pilot study. Eur J Cancer. (2014) 50:611–21. doi: 10.1016/j.ejca.2013.11.002
26. Rush S, Foreman N, Liu A. Brainstem ganglioglioma successfully treated with vemurafenib. J Clin Oncol. (2013) 31:e159–e160. doi: 10.1200/JCO.2012.44.1568
27. Shih KC, Shastry M, Williams JT, Jelsma PF, Abram SR, Ayyanar K, et al. Successful Treatment With Dabrafenib (GSK2118436) in a Patient With Ganglioglioma. J Clin Oncol. (2014) 32:e98–100. doi: 10.1200/JCO.2013.48.6852
28. Bautista F, Paci A, Minard-Colin V, Dufour C, Grill J, Lacroix L, et al. Vemurafenib in pediatric patients with BRAFV 600E mutated high-grade gliomas: vemurafenib in pediatric high-grade gliomas. Pediatr Blood Cancer. (2014) 61:1101–3. doi: 10.1002/pbc.24891
29. del Bufalo F, Carai A, Figà-Talamanca L, Pettorini B, Mallucci C, Giangaspero F, et al. Response of recurrent BRAFV600E mutated ganglioglioma to Vemurafenib as single agent. J Transl Med. (2014) 12:356. doi: 10.1186/s12967-014-0356-1
30. Aguilera D, Janss A, Mazewski C, Castellino RC, Schniederjan M, Hayes L, et al. Successful retreatment of a child with a refractory brainstem ganglioglioma with vemurafenib: vemurafenib response in recurrent ganglioglioma. Pediatr Blood Cancer. (2016) 63:541–3. doi: 10.1002/pbc.25787
31. Chamberlain MC. Recurrent ganglioglioma in adults treated with BRAF inhibitors. CNS Oncol. (2016) 5:27–9. doi: 10.2217/cns.15.40
32. Meletath SK, Pavlick D, Brennan T, Hamilton R, Chmielecki J, Elvin JA, et al. Personalized treatment for a patient with a BRAF V600E mutation using dabrafenib and a tumor treatment fields device in a high-grade glioma arising from ganglioglioma. J Natl Compr Canc Netw. (2016) 14:1345–50. doi: 10.6004/jnccn.2016.0145
33. Marks AM, Bindra RS, DiLuna ML, Huttner A, Jairam V, Kahle KT, et al. Response to the BRAF/MEK inhibitors dabrafenib/trametinib in an adolescent with a BRAF V600E mutated anaplastic ganglioglioma intolerant to vemurafenib. Pediatr Blood Cancer. (2018) 65:e26969. doi: 10.1002/pbc.26969
34. Beland B, Tsang RY, Sutherland G. Unprecedented response to combination BRAF and MEK inhibitors in adult anaplastic ganglioglioma. J Neurooncol. (2018) 137:667–9. doi: 10.1007/s11060-018-2760-5
35. Kaley T, Touat M, Subbiah V, Hollebecque A, Rodon J, Lockhart AC, et al. BRAF Inhibition in BRAFV600-mutant gliomas: results from the VE-BASKET study. J Clin Oncol. (2018) 10:3477–484. doi: 10.1200/JCO.2018.78.9990
36. Touat M, Gratieux J, Condette Auliac S, Sejean K, Aldea S, Savatovsky J, et al. Vemurafenib and cobimetinib overcome resistance to vemurafenib in BRAF -mutant ganglioglioma. Neurology. (2018) 91:523–5. doi: 10.1212/WNL.0000000000006171
37. Del Bufalo F, Ceglie G, Cacchione A, Alessi I, Colafati GS, Carai A, et al. BRAF V600E inhibitor (Vemurafenib) for BRAF V600E mutated low grade gliomas. Front Oncol. (2018) 8:526. doi: 10.3389/fonc.2018.00526
38. AcSé Vemurafenib - Carte des Centres. Available online at: https://www.google.com/maps/d/viewer?mid=1_GaxU0IDJ5WrUacH4z2dxZ7r2CU (Accessed June 5, 2017).
39. Van den Bent MJ, Wefel JS, Schiff D, Taphoorn MJB, Jaeckle K, Junck L, et al. Response assessment in neuro-oncology (a report of the RANO group): assessment of outcome in trials of diffuse low-grade gliomas. Lancet Oncol. (2011) 12:583–593. doi: 10.1016/S1470-2045(11)70057-2
40. Satyarthee G, Mehta V, Vaishya S. Ganglioglioma of the spinal cord: Report of two cases and review of literature. J Clin Neurosci. (2004) 11:199–202. doi: 10.1016/S0967-5868(03)00124-3
41. Oppenheimer D, Johnson M, Judkins A. Ganglioglioma of the Spinal Cord. J Clin Imaging Sci. (2015) 5:53. doi: 10.4103/2156-7514.166355
42. Zaky W, Patil SS, Park M, Liu D, Wang W-L, Wani KM, et al. Ganglioglioma in children and young adults: single institution experience and review of the literature. J Neurooncol. (2018) 139:739–47. doi: 10.1007/s11060-018-2921-6
43. Zhang D, Henning TD, Zou L-G, Hu L-B, Wen L, Feng X-Y, et al. Intracranial ganglioglioma: clinicopathological and MRI findings in 16 patients. Clin Radiol. (2008) 63:80–91. doi: 10.1016/j.crad.2007.06.010
44. Patel U, Pinto RS, Miller DC, Handler MS, Rorke LB, Epstein FJ, et al. MR of Spinal Cord Ganglioglioma. AJNR Am J Neuroradiol. (1998) 19:879–87.
45. Yang C, Li G, Fang J, Wu L, Yang T, Deng X, et al. Intramedullary gangliogliomas: clinical features, surgical outcomes, and neuropathic scoliosis. J Neurooncol. (2014) 116:135–43. doi: 10.1007/s11060-013-1267-3
46. Thust SC, van den Bent MJ, Smits M. Pseudoprogression of brain tumors: pseudoprogression of Brain Tumors. J Magn Reson Imaging. (2018) 48:571–89. doi: 10.1002/jmri.26171
47. Lang FF, Epstein FJ, Ransohoff J, Allen JC, Wisoff J, Abbott IR, et al. Central nervous system gangliogliomas: Part 2: clinical outcome. J Neurosurg. (1993) 79:867–73.
48. Varshneya K, Sarmiento JM, Nuño M, Lagman C, Mukherjee D, Nuño K, et al. A national perspective of adult gangliogliomas. J Clin Neurosci. (2016) 30:65–70. doi: 10.1016/j.jocn.2015.12.028
49. Lotfinia I, Vahedi P. Intramedullary cervical spinal cord ganglioglioma, review of the literature and therapeutic controversies. Spinal Cord. (2009) 47:87–90. doi: 10.1038/sc.2008.69
50. Millington GWM. Mutations of the BRAF gene in human cancer, by Davies et al. (Nature 2002; 417: 949-54). Clin Exp Dermatol. (2013) 38:222–3. doi: 10.1111/ced.12015
51. Nicolaides TP, Li H, Solomon DA, Hariono S, Hashizume R, Barkovich K, et al. Targeted Therapy for BRAFV600E Malignant Astrocytoma. Clin Cancer Res. (2011) 17:7595–04. doi: 10.1158/1078-0432.CCR-11-1456
52. Lassaletta A, Zapotocky M, Mistry M, Ramaswamy V, Honnorat M, Krishnatry R, et al. Therapeutic and prognostic implications of BRAF V600E in pediatric low-grade gliomas. J Clin Oncol. (2017) 35:2934–41. doi: 10.1200/JCO.2016.71.8726
53. Chen X, Pan C, Zhang P, Xu C, Sun Y, Yu H, et al. BRAF V600E mutation is a significant prognosticator of the tumour regrowth rate in brainstem gangliogliomas. J Clin Neurosci. (2017) 46:50–7. doi: 10.1016/j.jocn.2017.09.014
54. Vuong HG, Altibi AMA, Duong UNP, Ngo HTT, Pham TQ, Fung K-M, et al. BRAF mutation is associated with an improved survival in glioma—a systematic review and meta-analysis. Mol Neurobiol. (2017) 55:3718–24 doi: 10.1007/s12035-017-0599-y
55. Jones DTW, Witt O, Pfister SM. BRAF V600E status alone is not sufficient as a prognostic biomarker in pediatric low-grade glioma. J Clin Oncol. (2018) 36:96. doi: 10.1200/JCO.2017.75.8987
56. Breton Q, Plouhinec H, Prunier-Mirebeau D, Boisselier B, Michalak S, Menei P, et al. BRAF-V600E immunohistochemistry in a large series of glial and glial-neuronal tumors. Brain Behav. (2017) 7:e00641. doi: 10.1002/brb3.641
57. Koelsche C, Wöhrer A, Jeibmann A, Schittenhelm J, Schindler G, Preusser M, et al. Mutant BRAF V600E protein in ganglioglioma is predominantly expressed by neuronal tumor cells. Acta Neuropathol. (2013) 125:891–900. doi: 10.1007/s00401-013-1100-2
58. Chappé C, Padovani L, Scavarda D, Forest F, Nanni-Metellus I, Loundou A, et al. Dysembryoplastic neuroepithelial tumors share with pleomorphic xanthoastrocytomas and gangliogliomas BRAF V600E mutation and expression: BRAF V600E in glioneuronal tumors. Brain Pathol. (2013) 23:574–83. doi: 10.1111/bpa.12048
59. Momota H, Shimoyama Y. Recurrent papillary glioneuronal tumor presenting as a ganglioglioma with the BRAF V600E mutation: Letter to the Editor. Neuropathology. (2015) 35:603–5. doi: 10.1111/neup.12215
60. Horbinski C, Kofler J, Yeaney G, Camelo-Piragua S, Venneti S, Louis DN, et al. Isocitrate dehydrogenase 1 analysis differentiates gangliogliomas from infiltrative gliomas: IDH1 in gangliogliomas. Brain Pathol. (2011) 564–74. doi: 10.1111/j.1750-3639.2011.00480.x
61. Tan C, McLendon R. Histological approach to neuronal and mixed neuronal-glial tumors of the central nervous system. Glioma. (2018) 1:89. doi: 10.4103/glioma.glioma_24_18
62. Louis DN, Giannini C, Capper D, Paulus W, Figarella-Branger D, Lopes M, et al. cIMPACT-NOW update 2 diagnostic clarifcations for difuse midline louis2018.pdf. Acta Neuropathol. (2018) 135:639–42. doi: 10.1007/s00401-018-1826-y
63. Morita S, Nitta M, Muragaki Y, Komori T, Masui K, Maruyama T. Brainstem pilocytic astrocytoma with H3 K27M mutation: case report. J Neurosurg. (2018) 129:593–597. doi: 10.3171/2017.4.JNS162443
64. Yamada S, Kipp B, Voss J, Giannini C, Raghunathan A. Combined “Infiltrating Astrocytoma/Pleomorphic Xanthoastrocytoma” Harboring IDH1 R132H and BRAF V600E Mutations. Am J Surg Pathol. (2016) 40:279–84. doi: 10.1097/PAS.0000000000000515
65. López G, Oberheim Bush NA, Berger MS, Perry A, Solomon DA. Diffuse non-midline glioma with H3F3A K27M mutation: a prognostic and treatment dilemma. Acta Neuropathol Commun. (2017) 5:38. doi: 10.1186/s40478-017-0440-x
66. Kleinschmidt-DeMasters BK, Levy JMM. H3 K27M-mutant gliomas in adults vs. children share similar histological features and adverse prognosis. Clin Neuropathol. (2018) 37:53–63. doi: 10.5414/NP301085
67. Burger MC, Ronellenfitsch MW, Lorenz NI, Wagner M, Voss M, Capper D, et al. Dabrafenib in patients with recurrent, BRAF V600E mutated malignant glioma and leptomeningeal disease. Oncol Rep. (2017) 38:3291–96. doi: 10.3892/or.2017.6013
68. West ES, Williams VL, Morelli JG. Vemurafenib-Induced Neutrophilic Panniculitis in a Child with a Brainstem Glioma. Pediatr Dermatol. (2015) 32:153–4. doi: 10.1111/pde.12316
69. Chamberlain MC. Salvage therapy with BRAF inhibitors for recurrent pleomorphic xanthoastrocytoma: a retrospective case series. J Neurooncol. (2013) 114:237–40. doi: 10.1007/s11060-013-1176-5
70. Skrypek M, Foreman N, Guillaume D, Moertel C. Pilomyxoid astrocytoma treated successfully with vemurafenib: pilomyxoid astrocytoma and vemurafenib. Pediatr Blood Cancer. (2014) 61:2099–100. doi: 10.1002/pbc.25084
71. Robinson GW, Orr BA, Gajjar A. Complete clinical regression of a BRAF V600E-mutant pediatric glioblastoma multiforme after BRAF inhibitor therapy. BMC Cancer. (2014) 14:258. doi: 10.1186/1471-2407-14-258
72. Hauschild A, Larkin J, Ribas A, Dréno B, Flaherty KT, Ascierto PA, et al. Modeled prognostic subgroups for survival and treatment outcomes in BRAF V600–mutated metastatic melanoma: pooled analysis of 4 randomized clinical Trials. JAMA Oncol. (2018) 4:1382–8. doi: 10.1001/jamaoncol.2018.2668
73. Migliorini D, Aguiar D, Vargas M-I, Lobrinus A, Dietrich P-Y. BRAF/MEK double blockade in refractory anaplastic pleomorphic xanthoastrocytoma. Neurology. (2017) 88:1291–3. doi: 10.1212/WNL.0000000000003767
Keywords: central nervous system tumor, spinal cord, ganglioglioma, BRAF, vemurafenib, safety, tumor regression
Citation: Garnier L, Ducray F, Verlut C, Mihai M-I, Cattin F, Petit A and Curtit E (2019) Prolonged Response Induced by Single Agent Vemurafenib in a BRAF V600E Spinal Ganglioglioma: A Case Report and Review of the Literature. Front. Oncol. 9:177. doi: 10.3389/fonc.2019.00177
Received: 07 December 2018; Accepted: 04 March 2019;
Published: 26 March 2019.
Edited by:
Gordon Li, Stanford University, United StatesReviewed by:
Ofelia Cruz, Hospital Sant Joan de Déu Barcelona, SpainCarsten Friedrich, University of Rostock, Germany
Kwong-Hon Kevin Chow, Stamford Hospital, United States
Copyright © 2019 Garnier, Ducray, Verlut, Mihai, Cattin, Petit and Curtit. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Louis Garnier, Z2Fybmllci1sb3Vpc0Bob3RtYWlsLmZy