
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurosci. , 07 August 2019
Sec. Neural Technology
Volume 13 - 2019 | https://doi.org/10.3389/fnins.2019.00783
This article is part of the Research Topic Neural Electroceuticals: Interfacing with the Nervous System with Electrical Stimulation View all 42 articles
 Linus Haberbosch1,2*
Linus Haberbosch1,2* Abhishek Datta3
Abhishek Datta3 Chris Thomas3
Chris Thomas3 Andreas Jooß1
Andreas Jooß1 Arvid Köhn1
Arvid Köhn1 Maria Rönnefarth1,4
Maria Rönnefarth1,4 Michael Scholz5
Michael Scholz5 Stephan A. Brandt1
Stephan A. Brandt1 Sein Schmidt1,4
Sein Schmidt1,4Background: While alternating current stimulation (ACS) is gaining relevance as a tool in research and approaching clinical applications, its mechanisms of action remain unclear. A review by Schutter and colleagues argues for a retinal origin of transcranial ACS’ neuromodulatory effects. Interestingly, there is an alternative application form of ACS specifically targeting α-oscillations in the visual cortex via periorbital electrodes (retinofugal alternating current stimulation, rACS). To further compare these two methods and investigate retinal effects of ACS, we first aim to establish the safety and tolerability of rACS.
Objective: The goal of our research was to evaluate the safety of rACS via finite-element modeling, theoretical safety limits and subjective report.
Methods: 20 healthy subjects were stimulated with rACS as well as photic stimulation and reported adverse events following stimulation. We analyzed stimulation parameters at electrode level as well as distributed metric estimates from an ultra-high spatial resolution magnetic resonance imaging (MRI)-derived finite element human head model and compared them to existing safety limits.
Results: Topographical modeling revealed the highest current densities in the anterior visual pathway, particularly retina and optic nerve. Stimulation parameters and finite element modeling estimates of rACS were found to be well below existing safety limits. No serious adverse events occurred.
Conclusion: Our findings are in line with existing safety guidelines for retinal and neural damage and establish the tolerability and feasibility of rACS. In comparison to tACS, retinofugal stimulation of the visual cortex provides an anatomically circumscribed model to systematically study the mechanisms of action of ACS.
Non-invasive brain stimulation (NiBS) is an effective method for research, as well as a promising tool for therapy in cognitive and clinical neuroscience (Paulus, 2003; Hallett, 2007; Liew et al., 2014). Its effects range from direct brief modification of neural activity to long lasting recovery maximization following neural injury (Hallett, 2005; Talelli and Rothwell, 2006; Hummel et al., 2008; Sandrini and Cohen, 2013). Recently, transcranial alternating current stimulation (tACS), characterized by oscillatory low-voltage stimulation, showed promising effects on the motor system (Feurra et al., 2011, 2013), motor performance (Pogosyan et al., 2009; Joundi et al., 2012), memory (Marshall et al., 2006; Polania et al., 2012), higher order cognition (Santarnecchi et al., 2013, 2016) and tremor (Brittain et al., 2013). Despite these encouraging results, tACS’ mechanisms of action remain unclear (Zaghi et al., 2010) and a retinal contribution to its effects on neural synchrony is still being discussed (Schutter, 2016).
Retinofugal alternating current stimulation (rACS) is a comparably novel form of alternating current stimulation (ACS). In contrast to tACS, rACS is characterized by transmission along retinofugal tracts terminating predominantly in cortical visual areas and neuromodulation of central rhythms (Gall et al., 2011; Schmidt et al., 2013a). While differing from other forms of NiBS in regard to stimulation site, rACS shares its use of alternating current and effects on the intrinsic frequencies of the visual system with tACS (Schmidt et al., 2013a; Haberbosch et al., 2019). Moreover, in comparison to other forms of NiBS (namely, most types of tES) with diffusely induced electric fields (EF) throughout large parts of the brain (Peterchev et al., 2012), rACS affects the well-defined retinofugal pathway (Rager and Singer, 1998) for stimulation confined to the visual system. Thus, rACS renders a unique means to study mechanisms underlying NiBS as it physiologically affects the circumscribed primary visual cortex with separate input from each eye.
Before any novel method can be employed to its full potential or compared with other methodologies, establishing its safety and tolerability is critically important (Bath et al., 2014). The lack of knowledge of safety parameters could culminate in ineffective or even hazardous use (Antal et al., 2008; Bath et al., 2014). While ineffective stimulation could lead to incoherent findings regarding stimulation effects, effective but hazardous use could possibly result in severe adverse events and lasting damages in stimulation subjects. As rACS is used for research purposes, its safety as well as tolerability has to be determined rigorously.
Refraining from potentially dangerous invasive measures, the safety of a novel NiBS montage should be assessed in several different ways.
Firstly, stimulation parameters can be compared to theoretical safety limits as established for NiBS and neural tissue damage in animal studies (Agnew and McCreery, 1987; Liebetanz et al., 2009; Jackson et al., 2017), which have since been used to assess NiBS safety in human studies (Poreisz et al., 2007; Bikson et al., 2009, 2016). The primarily employed metrics include current density (A/m2) and charge density (C/m2), although other parameters such as charge per phase (C/ph) have been proposed to account for the shifting polarity of AC stimulation (Nitsche et al., 2003; Merrill et al., 2005).
Secondly, these safety metrics can be modeled onto CNS structures (Datta et al., 2011; Bikson et al., 2016), to determine the possibility of damage at critical locations (Bikson et al., 2016) while accounting for anatomy and electrode position (Bikson et al., 2009; Bikson and Datta, 2012; Peterchev et al., 2012; Saturnino et al., 2015).
Finally, experimental validation of theoretical results by subjective reports of adverse events with validated questionnaires can be acquired (Brunoni et al., 2011). These reports are also instrumental in assessing the tolerability of the novel method.
In this study we hypothesized that rACS is to be considered safe if: (1) Stimulation parameters (current and charge densities at the electrode) are within theoretical safety limits, (2) finite element modeling data shows the same for EF estimates and current densities at eye, retina and cortex, and (3) adverse events do not exceed that of other established stimulation methods in rate as well as severity.
To address the primary hypothesis, the stimulation parameters of rACS were recorded during stimulation and employed for the calculation of safety limits. Ultra-high resolution topographical finite element modeling was performed to identify regions of critical interest and to calculate theoretical safety parameters. Adverse events were identified with an extended adverse events questionnaire developed for tDCS (Brunoni et al., 2011). For direct experimental comparison, we employed simple and safe photic stimulation (PS) (Walker et al., 1944) as the gold-standard method for stimulation of the retinofugal pathway regarding safety and clinical experience (Cobb, 1947; Trenite et al., 1999).
To address the safety profile of rACS, we observed and questioned 20 test subjects during rACS and PS sessions. We assessed cutaneous, retinal and central adverse events and drew a comparison between PS and rACS.
We stimulated 20 healthy volunteers (10 men), mean age 25.9 ± 4.95, as part of a study investigating a common framework of action for NiBS. The subjects were interviewed prior to experimentation regarding their state of health. We applied established exclusion criteria for NiBS (Brunoni et al., 2012) and added evidence for photophobia and photosensitive epilepsy. Written informed consent was obtained from all individual participants included in the study. The subjects received financial compensation for their participation. All procedures were performed in accordance with the ethical standards of the Ethics Committee of the Charité – Universitätsmedizin Berlin (“Ethikkommission der Charité – Universitätsmedizin Berlin”) and with the 1964 Declaration of Helsinki and its later amendments. This study adheres to the principles of good scientific practice of the Charité – Universitätsmedizin Berlin (“Grundsätze der Charité zur Sicherung guter wissenschaftlicher Praxis”).
Retinofugal alternating current stimulation was applied via a multi-channel low-voltage stimulation device certified for clinical use, which delivered weak oscillatory current sinus-pulses over four individual periorbital electrodes, respectively (NextWave, Eyetronic, Germany). The four superficial active stimulating electrodes (Grass SAFELEADTM gold electrodes, Astro-Med, Inc., RI, United States) were contained in foam-padded stimulation goggles and bilaterally made skin contact via small felt buffers (0.35 cm2) superior and inferior to the eye. The return electrode (rectangular electrode, 30 × 30 mm polished stainless steel) was fastened on the back of the neck at the midline.
Alternating current was applied at 10 Hz, as ACS has shown robust effects at this frequency (Kanai et al., 2008; Helfrich et al., 2014; Vossen et al., 2015) and gold standard PS typically also employs 10 Hz stimulation (Photic driving) (Walker et al., 1944). Stimulation amplitude was set to 120% phosphene threshold (resulting in 351.69 μA (SD 63.95) peak-to-peak amplitude). The phosphene threshold was determined employing an ascending method of limits (Herrick, 1967) provided by the NextWave software. rACS was delivered in 30 s blocks followed by 30 s pauses over 10 min. The subjects were told to keep their eyes open and focus a fixed point on a white surface in 1 m distance for the duration of the experiment.
To assess the safety parameters of stimulation we additionally calculated the effective amplitude. The effective amplitude of the applied current is defined as the time normed integral of the signal, which simplifies to its mean value for discrete signals as is the case here, since the used stimulator receives an equidistant sampled discrete function as input. In the simplest case of a pure sine wave this simplifies to the following formula:
In the case of more complex stimuli such as noise + sine wave or signals with an additional amplitude modulation, the use of peak-to-peak “a(max)” values to describe the resulting electrical power of an electric current stimulation would be misleading.
Regarding charge, we decided to refrain from more complex line integral calculations, and instead used the following simple formula:
This was done to ensure straightforward comparability of resulting values. It also adds to the rigidity of our safety considerations by rather over-than underestimating the injected charge.
Photic Stimulation was applied via two 3 × 5 cm multi-color white LEDs contained in the stimulation goggles, which work via red, green and blue LEDs mixing their emissions to form white light. To be able to compare stimulation intensities with rACS, sinusoidal pulses of white light were applied at an intensity of 120% light threshold and with a frequency of 10 Hz. This threshold was also determined by an ascending method of limits and resulted in an average luminous intensity of 1.24 cd (±0.44) for stimulation.
The stimulation was also delivered in 30 s blocks followed by 30 s pauses over 10 min, and the subjects received the same instructions as for rACS.
The ultra-high resolution head and neck model (MIDA: Multimodal Imaging-Based Detailed Anatomical Model) available through the IT’IS Foundation was used in this study (Iacono et al., 2015). The nifti (.nii) color masks from the MIDA model were first processed in MATLAB to re-create segmentation masks based on intensity values. These masks were then imported into Simpleware (Synopsys Ltd., CA, United States) and any errors in continuity and anatomical details were manually corrected for Datta et al. (2012). Masks with similar electrical conductivities were then merged to a single compartment barring the regions of interest (eye structures) in order to perform individual current flow analysis through them. For instance, mandible, teeth, vertebra, skull dipole, skull inner table, skull outer table, hyoid bone were combined with the skull mask but eye retina, choroid, and sclera were treated as individual masks.
The stimulation electrodes were created as CAD files mimicking the exact physical geometry and dimensions of the electrodes used in the experiments. The electrodes were positioned interactively within the image data simulating the electrode montage used for rACS (see Figure 1C). The adaptive meshes derived from the segmentation masks were then imported into COMSOL Multiphysics (Burlington, MA, United States) for finite element computation. The final model comprised >10 million elements with >15 million degrees of freedom.
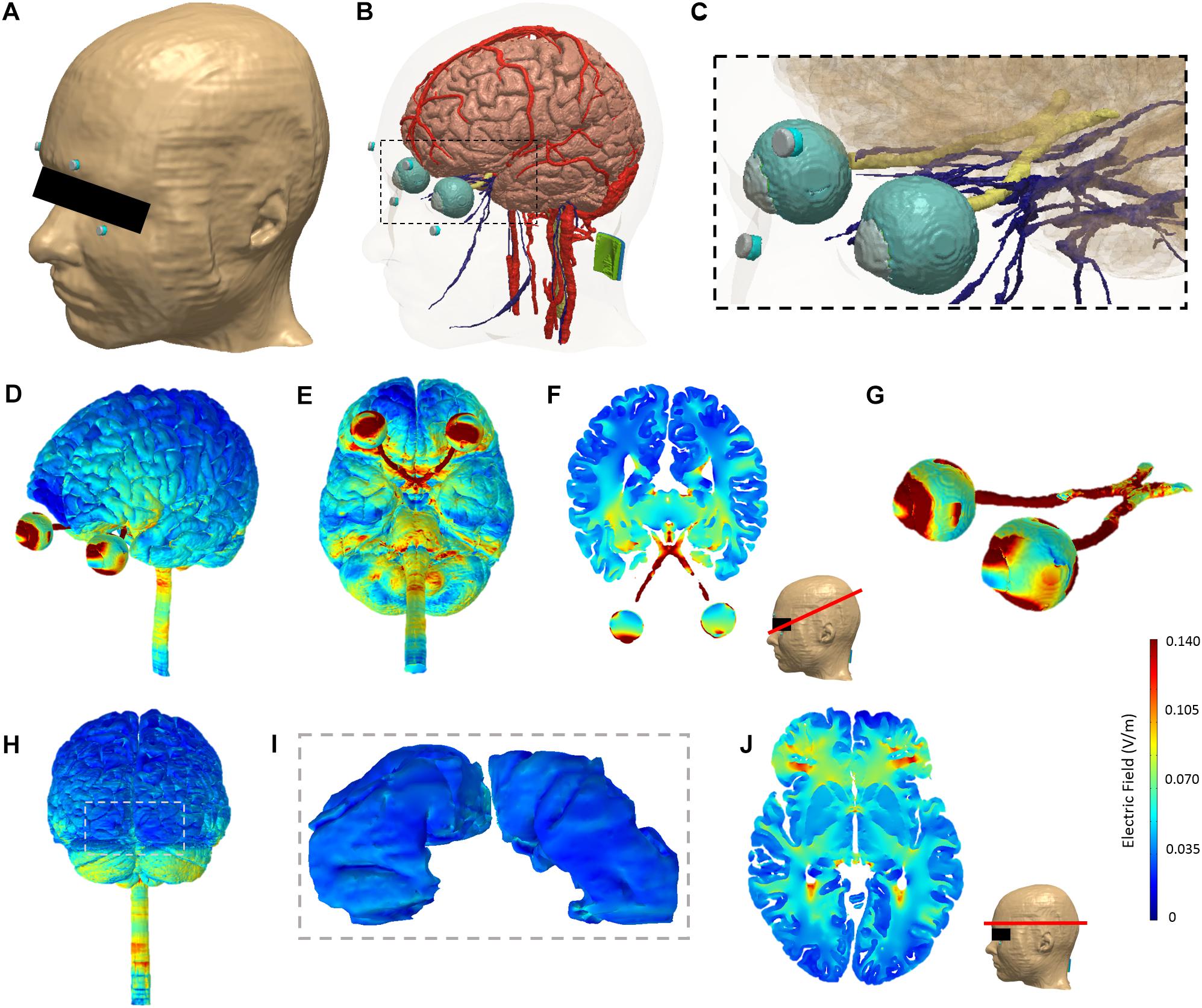
Figure 1. Model segmentation and finite element analysis. The ultra-high resolution MIDA model was adapted for analysis in this study. (A) Skin tissue mask with periorbital electrodes (gray: electrode; blue: sponge). (B) The modeled brain, cranial nerves, blood vessels, eye structure, optic nerves, and electrodes (both active periorbital and the return inion electrode shown). (C) Zoomed view corresponding to the dashed section in panel (B) highlighting segmentation detail in the region of interest. Finite element analysis of current flow produced by rACS: Induced electric field magnitude plots on the cortical and eye level perspective (D) and bottom view (E). A representative axial 2D cross-section view of electric field magnitude following the retinofugal tract was chosen and plotted (F). Panel (G) shows the induced electric field on the eyes and optic nerve. Panel (H) shows the rear view. Panel (I) shows the primary visual cortex (V1) corresponding to the dashed section in panel (H). A representative 2D axial cross-section view of electric field magnitude taken at the level of half of the visual cortex along the superior–inferior plane is shown in panel (J).
The representative isotropic average electrical conductivities assigned to the different tissue compartments and the electrode materials (in S/m) are listed in Table 1.
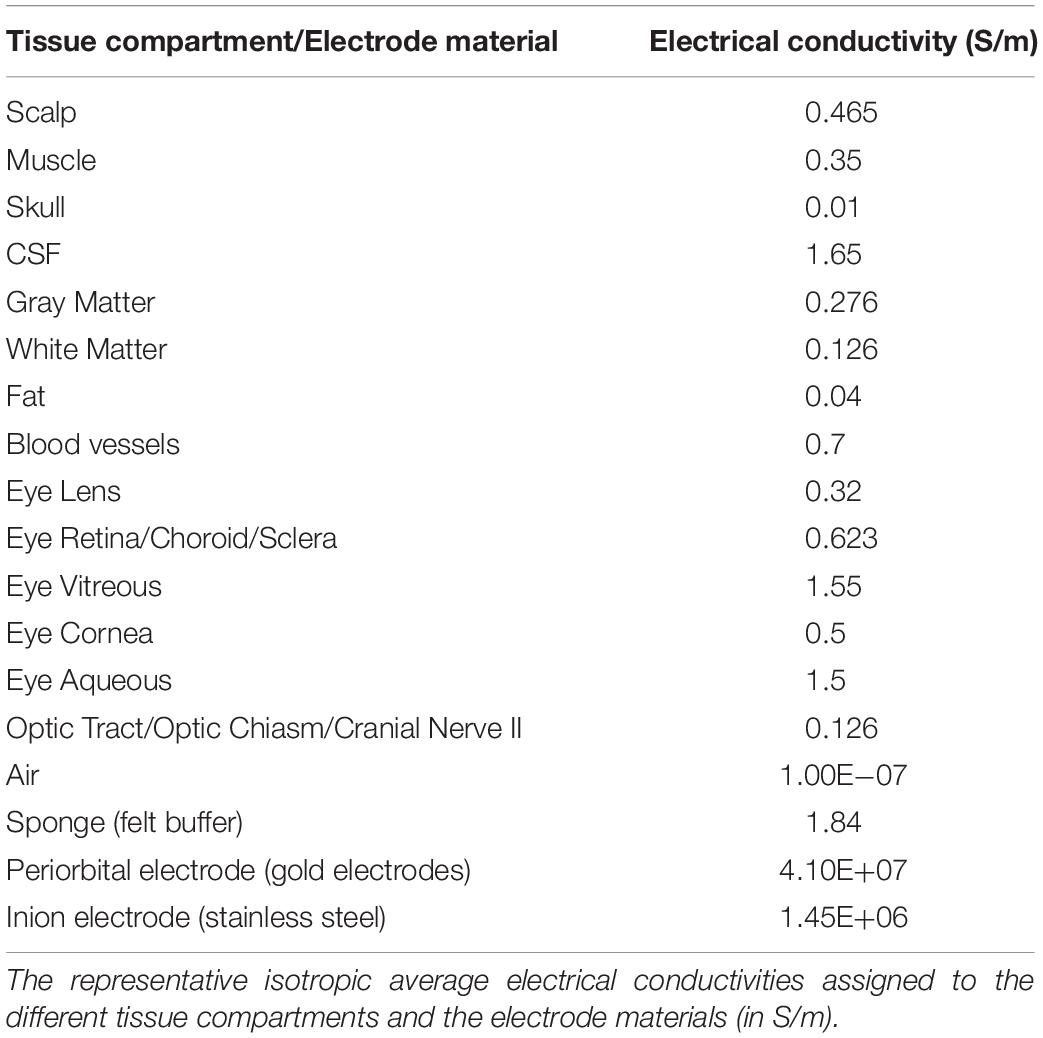
Table 1. Assigned electrical conductivities.
The Laplace equation was solved and current densities corresponding to 350 μA total current were applied at the anode or active electrode (s). Ground was applied at the return electrode and all other external surfaces were treated as insulated. The linear iterative solver of conjugate gradients with a relative tolerance of 1E-6 was used.
Surface as well as cross-sectional EF magnitude maps on the gray matter, retina, and the optic nerve were obtained. For the scalp, the surface current density magnitude plot was obtained.
The questionnaire we employed is based on the one proposed by Brunoni et al. (2011) and investigated the presence of headaches, difficulties in concentrating, acute mood changes, visual perceptual changes, fatigue and discomforting sensations tingling, itching and/or burning under the electrodes during and after rACS, as well as PS. The item “Difficulties in concentrating” was defined in accordance with Montgomery and Asberg (1979), while the item “Fatigue” was defined in accordance with Chaudhuri and Behan (2004).
We modified the questionnaire by adding a description of phosphenes. Furthermore, to assess the overall tolerability, we defined the broad category of “Pain” as a summary of all discomforting sensations mentioned above and added a Numeric Rating Scale (NRS-11, 11 stages from 0 to 10, 10 being the strongest imaginable pain and 0 the absence of pain) (Farrar et al., 2001) as a more in-depth and reliable measurement (Downie et al., 1978). We discarded the four-point intensity rating for the other categories to avoid a “halo effect” bias (Streiner and Norman, 2008). We assumed that the foreign body feeling reported for physiologically similar transcorneal electrical stimulation (TCES) came from the electrode lying directly on the cornea (Gekeler et al., 2006) and therefore decided not to include it.
Three months after stimulation, the subjects received a second questionnaire to identify late and longer lasting after-effects.
As the data is not normally distributed and equal variance of residuals cannot be assumed, the severity of pain was analyzed in Wilcoxon Signed Ranks Tests for paired samples. The nominally scaled side effects were analyzed in Fishers Exact Tests, as expected values in several of the cells of a contingency table are below the recommended threshold for a classical Chi-Squared Test (Larntz, 1978). P-values of <0.05 were considered significant. All analyses were performed using IBM SPSS Statistics, Version 19.0.0.1 (IBM, United States).
An average 10 Hz phosphene threshold at 290.50 μV (SD 45.36), impedances at 12.05 kΩ (SD 2.89), and an average amplitude of 351.69 μA (SD 63.95) were noted. Calculated from peak-to-peak amplitude, the current density at electrode level amounted to a mean 1.00 mA/cm2 (SD 0.28), and the charge density to 0.60 C/cm2 (SD 0.11). As sine waves pulses were employed, we additionally calculated the effective amplitude, resulting in a mean 248.68 μA (SD 47.0). Using effective amplitude, current density amounted to a mean 0.71 mA/cm2 (SD 0.13), and the charge density to 0.42 C/cm2 (SD 0.08). RACS was found to be well within safety limits and the findings comparable to other similar stimulation methods (see Table 2). Regarding stimulation amplitude, rACS (0.35 mA) was comparable to most TCES and tES montages (ranging from 0.08 to 1.2 mA). Electrosleep and the maximum intensity stimulation employed by Gekeler et al. (2006) were found to employ higher amplitudes (3–25 mA). The stimulated area (0.35 cm2) is smaller than most tES montages (16–35 cm2), comparable only to Electrosleep and TCES (0.35–1.25 cm2). Regarding stimulation frequencies, rACS was compared to studies using similar frequencies (10–20 Hz), with the exceptions of Electrosleep, which is set at higher frequencies (100 Hz) as well as the non-oscillating tDCS and Gekeler’s TCES. The calculations following these observations place the charge density of rACS just above the TCES of Ma et al. (2014) and far below the safety limit published by Liebetanz et al. (2009). This is consistent for charge per phase and charge density per phase. Regarding current density, rACS (1 mA/cm2) ranks below Ma (1.2 mA/cm2), well below the maximum intensity employed by Gekeler (8.57 mA/cm2) and far below the safety limit proposed by McCreery (25 mA/cm2). These findings are even more pronounced when using effective amplitude.
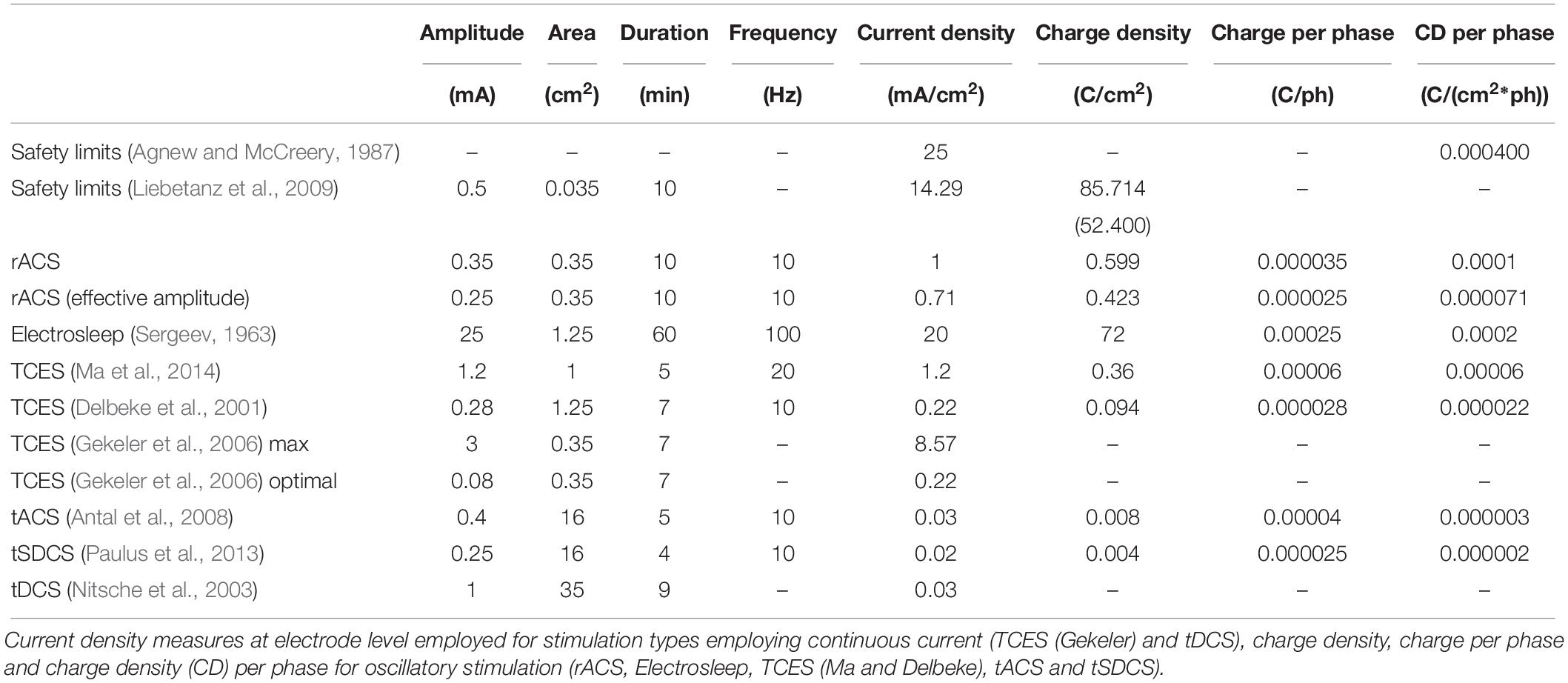
Table 2. Comparison of stimulation parameters.
The EF distributed by rACS is strongest at the eye level, with the highest current density estimates at the retina. Further areas of elevated current densities are optic nerve and cortex (Figures 1A,B).
The calculated maximum current density at the retina amounted to a maximum of 1.24 A/m2, while optic nerve (0.33 A/m2) and cortex (0.13 A/m2) were both subjected to less current flow. Regarding the EF, we estimated a maximum of 2.6 V/m in the optic nerve, followed by 1.99 V/m for the retina and 0.47 V/m for the cortex. Finally, current density at skin level underneath the active electrode amounted to a maximum induced value of 14.79 A/m2 (Figure 1C), with the EF estimated at 31.80 V/m. It should be noted that due to edge effects, the observed values are higher than the current density toward the middle of the electrode which is simply the current injected over the contact area. For a detailed view, see Table 3.
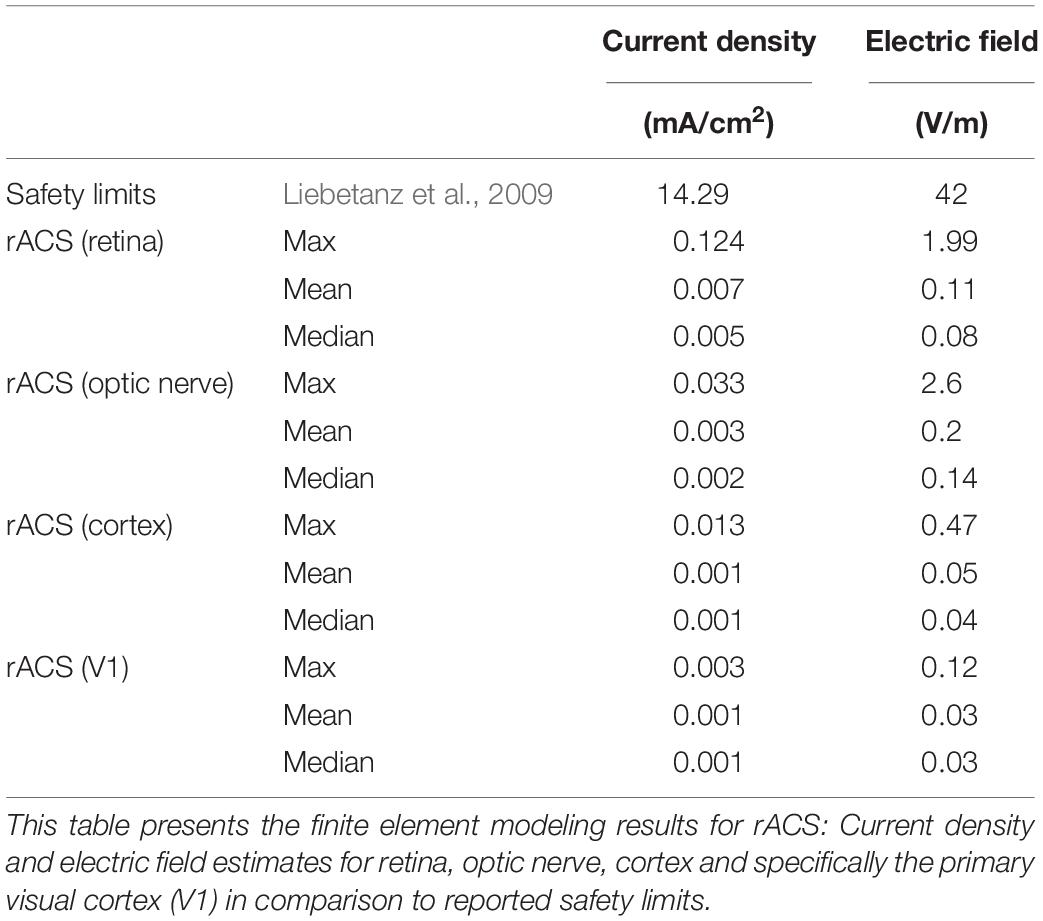
Table 3. Modeling data and comparison to safety limits.
Table 4 summarizes the adverse events in the 20 rACS and PS sessions in healthy participants. None of the subjects requested the stimulation to be terminated or required medical attention. In their subjective reports, rACS associated adverse events were predominant during stimulation, and PS associated adverse events were predominant following stimulation. More explicitly, a tingling sensation occurred in 70% of the subjects during but not after rACS. An itching sensation under the electrodes was reported by 30% of the subjects during rACS and 25% after rACS. A burning sensation was felt by 30% of the participants during but not after rACS. Fatigue occurred during, as well as after, stimulation in 35 and 20% of the rACS and PS group, respectively. Headaches were reported only by PS participants during stimulation (15%). After stimulation, it was reported by 5% for both PS, as well as rACS participants. Difficulties in concentrating were reported by 10% of the participants after PS, but not after rACS. There were no cases of acute mood changes, nausea and visual perceptual changes or lasting adverse events 3 months after stimulation.
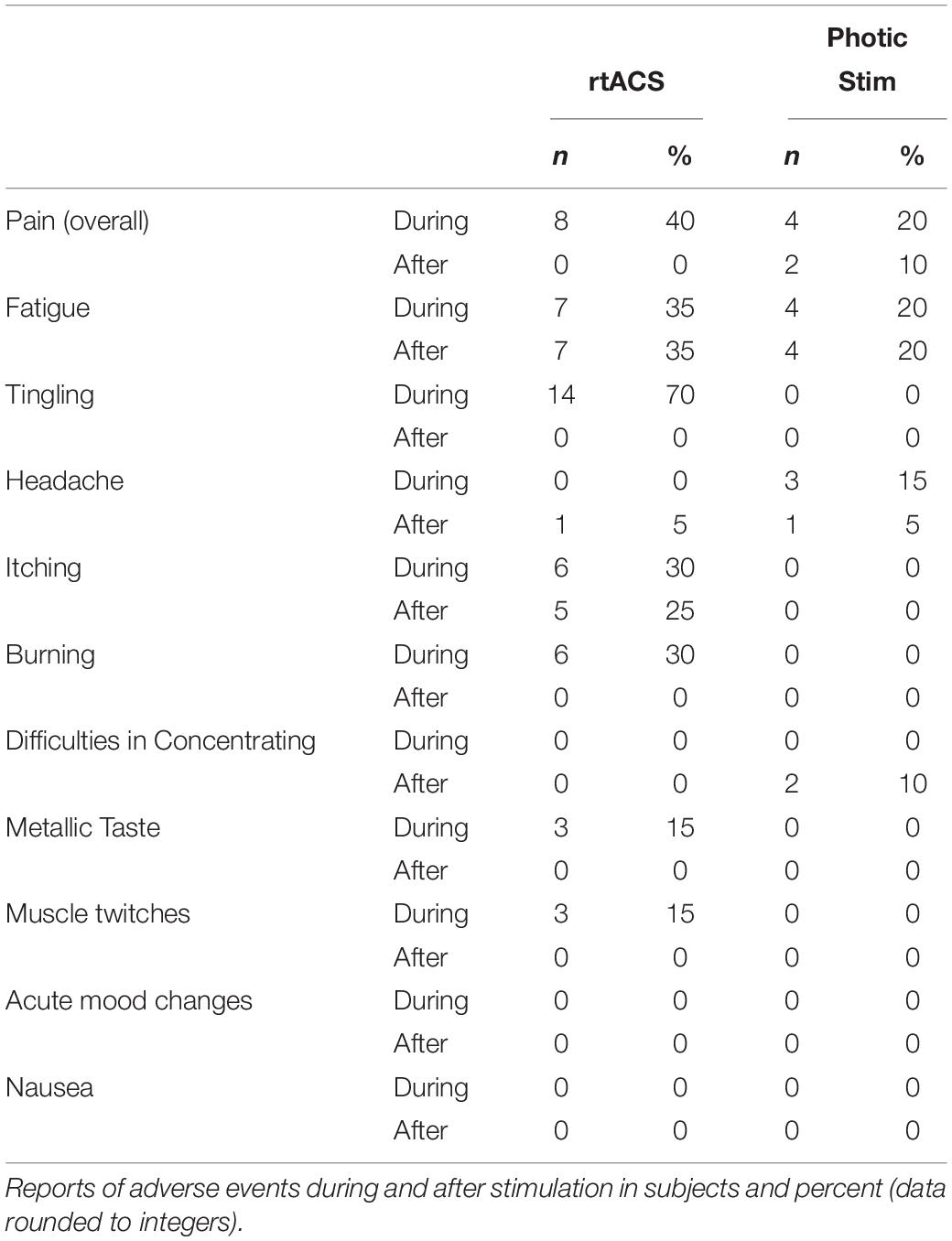
Table 4. Adverse events for rACS and PS.
Forty-percent of the subjects reported pain (Figure 2A) during rACS (mean intensity 2.5, SD 1.73) and 20% during PS (2.75, SD 0.83). While none of the participants reported pain after rACS, this was the case for 10% after PS (1.5, SD 0.5).
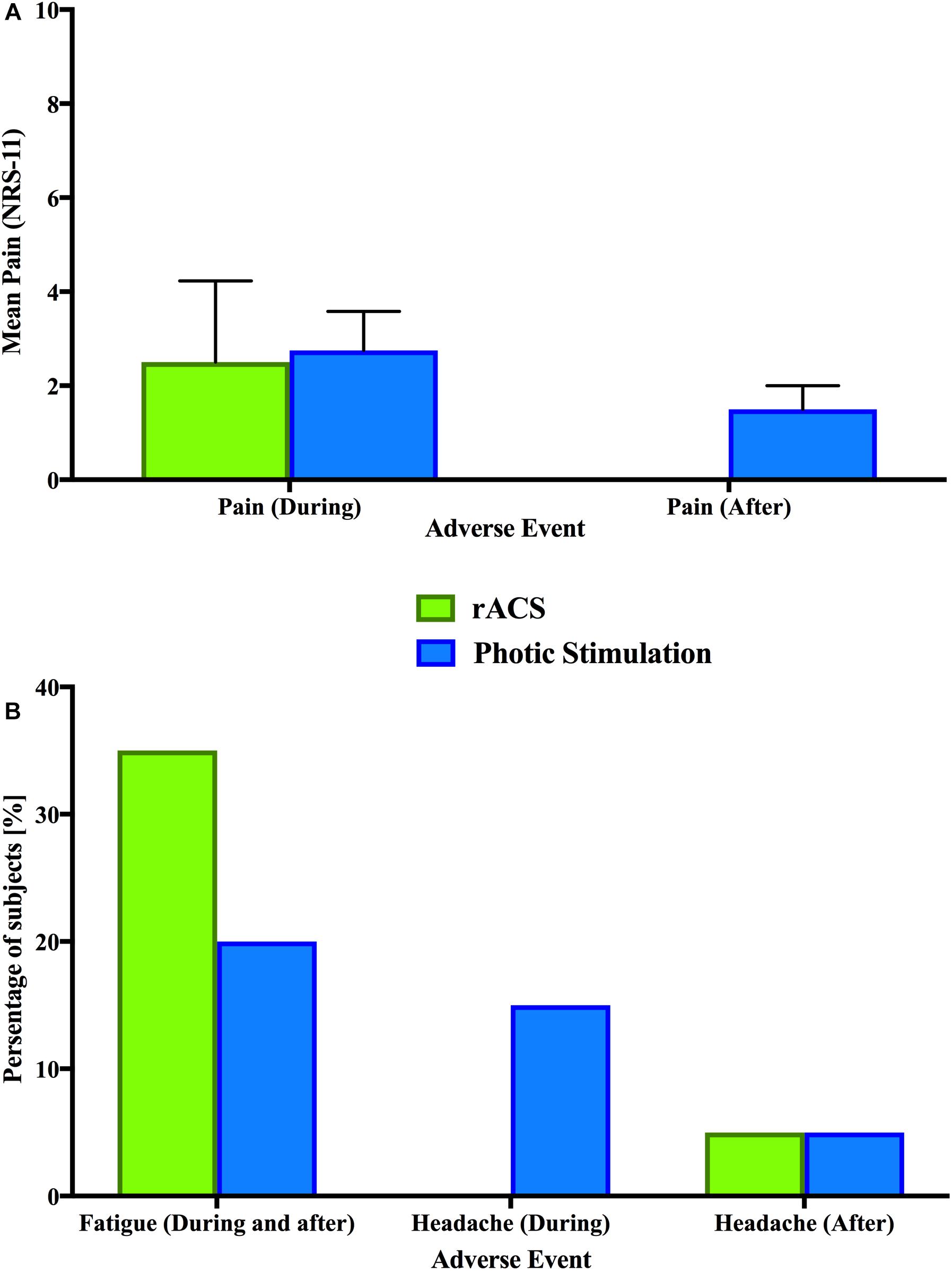
Figure 2. Adverse events. A comparison of adverse events between rACS (green) and PS (blue). None of the depicted differences were significant in Bonferroni-corrected multiple comparisons. (A) Depicted is the mean rating (NRS-11) of overall pain and discomfort in affected subjects during and after stimulation. Error bars represent the standard deviation. (B) Comparison of shared adverse events (fatigue and headache) in percentage of subjects.
In the statistical analyses, rACS and PS showed no significant effect of stimulation type (rACS versus PS) on pain intensity as assessed by Wilcoxon Signed Ranks Tests (Figure 2A), fatigue, headache and difficulties in concentrating as assessed by Fisher’s Exact Tests (Figure 2B) during as well as after stimulation. PS and rACS significantly differed regarding skin sensations of tingling, itching and burning (P < 0.05, Fisher’s Exact Tests), which all occurred exclusively in rACS. For a more detailed view, see Tables 5, 6. The full dataset behind this comparison is available as Supplementary Material.
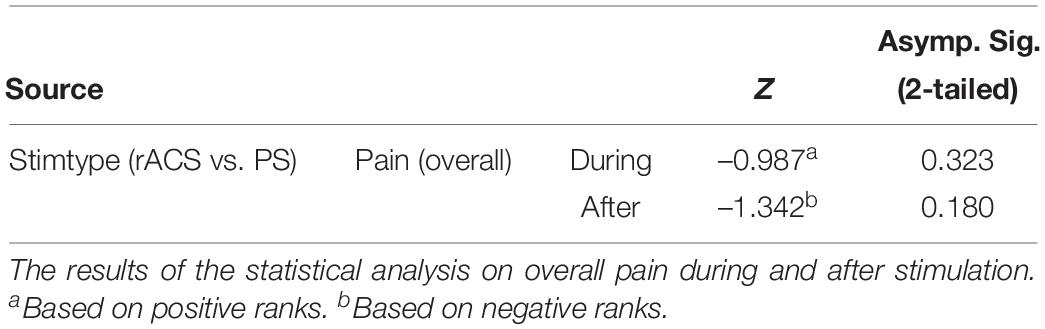
Table 5. Results of the Wilcoxon-signed ranks tests.
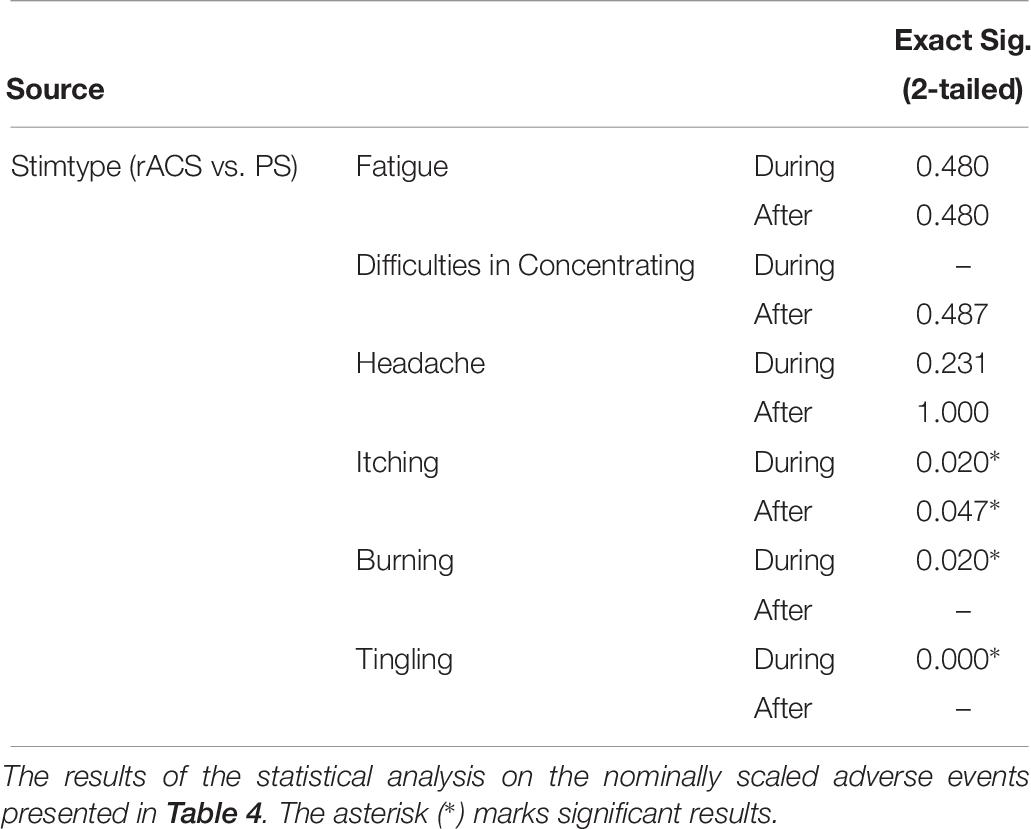
Table 6. Results of the Fisher’s exact tests.
To address the safety profile of rACS, we assessed theoretical safety limits as well as finite-element modeling data and compared the reported adverse events for rACS and simple PS.
The primary findings are that rACS is safe based on the following observations: (1) stimulation parameters (current and charge densities at the electrode) are within theoretical safety limits, (2) finite element modeling data shows the same for EF estimates and current densities at eye, retina and cortex, and (3) adverse events are comparable to PS in direct experimental comparison (see Tables 3, 4) and rate as well as severity of adverse events did not exceed that of other established brain stimulation methods (see Table 2).
To be efficacious and safe, a stimulation system must stimulate neural tissue without damaging tissue or electrode. Tissue damage is caused when excitable tissue is overstimulated and electrode damage ensues as metal oxidation occurs (Peterchev et al., 2012). Current density and charge density have been proposed as predictors for such damage (Bikson et al., 2016).
Current density is the proposed optimal safety parameter for a constant current stimulation (Nitsche et al., 2003) and can be derived from the effective amplitude and compared to safety limits (Agnew and McCreery, 1987) as well as other similar stimulation paradigms (Gekeler et al., 2006; Ma et al., 2014).
We find that rACS current densities are within reported safety limits for tissue damage (Yuen et al., 1981; Lindenblatt and Silny, 2002; Liebetanz et al., 2009; Gellner et al., 2016).
While current density is a well-established safety parameter, it is best suited for assessing the safety of constant current stimulation. ACS injects less charge than constant current stimulation of the same amplitude (Liebetanz et al., 2009; Schmidt et al., 2013a), dependent on stimulation frequency and duty cycle (Chaieb et al., 2014). The safety limits of charge balanced ACS, such as rACS, are therefore more precisely determined by charge density and charge per phase (Nitsche et al., 2003; Merrill et al., 2005).
We find that rACS charge densities are also within reported safety limits for tissue damage (Yuen et al., 1981; Lindenblatt and Silny, 2002; Liebetanz et al., 2009; Gellner et al., 2016; Jackson et al., 2017).
While stimulating at higher current and charge densities than most forms of tES, rACS stimulation parameters proved comparable to dose parameters reported for TCES using up to 10 mA per pulse to establish safety guidelines (Gekeler et al., 2011), well below early montage parameters for both stronger and longer stimulation used in early studies addressing Electrosleep therapy (Robinovitch, 1914; Knutson, 1967; Peterchev et al., 2012), and well below current densities reported for stimulation via implanted self-sizing spiral cuff electrodes in blind patients over the course of several years (Delbeke, 2011) (see Table 2).
Despite arguable differences between different stimulation techniques, there are remarkable similarities, e.g., comparably distant periorbital montage of electrodes, as well as modeling results for the serial resistance of the skin and eyelid (Delbeke et al., 2000; Merrill et al., 2005; Gekeler et al., 2006) to motivate this comparison.
This leads to the conclusion that the employed charge injection was safe with regards to possible tissue as well as electrode damage. In the future, studies addressing the calculation of rheobase and chronaxie and stimulation with variable pulse parameters might help to further reduce charge injection to the minimum necessary to efficaciously achieve a neuronal response (Irnich, 1980, 2010; Delbeke et al., 2001).
Expectedly, the EF distribution shows a clear focus on retina and optic nerve, while the cortical electric current flow is much weaker. Due to the electrode montage being superior–inferior, we see stronger EFs in the temporal regions and at the return electrode. While there is increased flow through the subcortical structures, brain stem and cerebellum, there appears to be no strong current flow to occipital areas, with a maximum current density of 0.033 A/m2 and a maximum EF of 0.1208 V/m (Table 3 and Figure 1).
This confirms the retinofugal pathway as the primary target of rACS. Still, stimulation intensity should be closely monitored, as strong over-threshold stimulation might lead to unwanted effects on subcortical structures.
Evidence from relevant animal models indicates that brain injury by tDCS occurs at predicted brain current densities (14.9 A/m2) (Liebetanz et al., 2009; Gellner et al., 2016; Jackson et al., 2017). Considering the well-established threshold proposed by Liebetanz et al. (2009), rACS maximum current densities rank two orders of magnitude (OOM) below lesion threshold for retina and optic nerve and three OOM below for the cortex.
Additionally, all of the EF estimates are at least one OOM below the safety threshold of 42 V/m (Liebetanz et al., 2009; Gellner et al., 2016; Jackson et al., 2017). It should be noted that, as mentioned above, ACS injects less charge than constant current stimulation of the same amplitude (Liebetanz et al., 2009; Schmidt et al., 2013a), and we calculated the current densities from peak-to-peak amplitude instead of effective amplitude. The risk of damage will consequently rather be over-than underestimated. We therefore conclude the rACS employed in this study should be safe from a modeling standpoint as well.
No fatal or serious adverse events (Wester et al., 2008) were observed for rACS. The most notable adverse events in the present study were tingling, burning, itching and fatigue. The hazard rate for these adverse events is to be considered “very common” (>1/10 cases). This is comparable to results from other forms of tES (Brunoni et al., 2011), suggesting for tDCS that the type of adverse event is mild and their frequency of occurrence is “common.” Direct experimental evidence shows significantly more cutaneous adverse events, but significantly less concentration deficits after stimulation for rACS as compared to PS (Table 5).
As the modeling results showed high maximum current densities and EF estimates at skin level, the presence of cutaneous adverse events during and after rACS comes as no surprise. Comparing rACS and PS regarding the summary category of pain, we have to note the complete lack of cutaneous sensations in PS and that multiple aversive sensations may be clustered and perceived in sum total as painful (Tuckett, 1982).
None of the subjects reported skin rashes or damage. Whereas the applied charge density is clearly strong enough to stimulate C-nociceptors, it is too low and the duration is too short to induce skin damage (Dzhokic et al., 2008). For direct current stimulation, it has been shown that 1 mA via two 7 × 5 cm rubber electrodes in over 2000 stimulation sessions (Loo et al., 2011) can be applied for 20 min with no skin damage. Again, ACS is less likely than direct current stimulation to induce tissue or electrode damage. Although rACS is unlikely to induce skin damage, this study adhered to previous suggestions for avoiding cutaneous adverse events (Loo et al., 2011).
Electrical stimulation of skin nociceptors is known to produce itching, burning and tingling sensations in the animal model, as well as in human subjects (Jarvis and Voita, 1971; Tuckett, 1982; Kellogg et al., 1989; Ledger, 1992). While even persisting shortly after stimulation due to central processes, these sensations are not necessarily indicative of local damage induced by stimulation (Tuckett, 1982).
One third of the subjects reported pain with a median strength of 2.5 NRS. The sensation of pain during and after electric stimulation is understood to be a combination of several factors, with the terminal branches of C-nociceptors of the stimulated skin acting as the primary central conductor (Magerl et al., 1987; Garnsworthy et al., 1988; Hakkinen et al., 1995). This matches subject descriptions of deep and spread pain associated with itch and burning sensations in this study (six cases) as well as anecdotal reports of painful perceptions that could not be attenuated by topical anesthetic and the lack of radiating pain sensations reported elsewhere (Hakkinen et al., 1995). Due to the common occurrence of cutaneous sensations, topical anesthesia might be preferential especially for placebo control or rACS versus PS studies. This study did not use topical anesthesia, as it might mask development of skin damage.
While the feeling of pain and discomfort should be monitored closely in future studies, it should be noted that we found no significant difference between rACS and well-established and tolerable PS regarding overall discomfort/pain (Table 5).
This pain during and after PS is most likely a form of “discomfort glare” associated with visual discomfort, annoyance, irritability or distraction without affecting the ability to see, but leading to symptoms of visual fatigue (Ticleanu and Littlefair, 2015).
As we stimulated our subjects at 120% phosphene threshold, all subjects experienced phosphenes. These phosphenes induced by rACS were typically described as flickering at the edges of the field of view and not experienced as painful.
Historically, phosphenes induced by alternating current have been seen as a purely retinal phenomenon (Rohracher, 1935) resulting from the high susceptibility of the retina to electricity (Ziemssen, 1864). For rACS and other forms of tES the amount of confounding retinal or cortical stimulation following low-voltage stimulation is unknown or a matter of controversy (Paulus, 2010).
Yet, due to the respective montages there should be a magnitude of difference between methods (Peterchev et al., 2012) with TCES inducing the most, rACS with periorbital-occipital montages intermediate, and tES the least retinal stimulation (Delbeke et al., 2001; Thil et al., 2007; Paulus, 2010).
A previous tACS modeling effort indicated why transcranial stimulation may induce retinal phosphenes (Laakso and Hirata, 2013) by virtue of current density induced in the eyes exceeding phosphene thresholds. As different electrode montages result in different current flow patterns, whether a particular montage would result in retinal phosphenes would naturally depend on the montage being studied. Specifically they show that the threshold for retinal phosphenes for commonly used tACS montages is exceeded with stimulation current of 500–1000 μA (depending on the montage considered). Another prior tACS/tDCS modeling effort demonstrated that bilateral montages result in not only more focused current flow but higher current intensities than midline montages (Neuling et al., 2012). While no detailed analysis is performed on the eye regions, the authors state that the closer one of the stimulation electrodes is to the eye regions, the easier it is to perceive phosphenes.
Where exactly rACS phosphenes are generated remains subject to further investigation. While we find the highest EF estimates in the optic nerve, other authors (Brindley, 1955; Ma et al., 2014) suggested bipolar cells, or the parts of rod and cone cells lying inside the external limiting membrane as the main site of stimulation. In line with the flickering at the edges of the field of view as reported by our subjects for rACS at 120% phosphene threshold, it can be argued that inner retinal neurons are the most probable site at which an electrical stimulus exerts its primary effect, with predominant activation of the peripheral retina (Ma et al., 2014). This adds further support to previous findings suggesting that the primary location of the majority of retinal damage (the retinal pigment epithelium, RPE) induced by photochemical noxae is bypassed by electrical stimulation (Grützner et al., 1958). Besides fatigue and cutaneous effects, the participants described more phosphene or light related adverse events in association with well-known and safe PS applied at 120% light threshold than with rACS applied at 120% phosphene threshold.
Fatigue, reported by one third of the subjects after rACS, has been suggested in previous research to be an unspecific effect of tES. Similar to rACS, the early approaches to tES involved two “active” electrodes placed directly over the eyes, presumably to facilitate active current delivery through the optic foramina. These montages were first used in Electrosleep research initiated in Robinovitch (1914), with extensive research following (Obrosow, 1959; Sergeev, 1963; Brown, 1975). The consensus after about 60 years was that Electrosleep induces unspecific sleepiness and fatigue related to stimulation (Guleyupoglu et al., 2013).
The findings in this study, that rACS produces more fatigue than PS, support the notion of an indirect and unspecific central (adverse) effect specific to electrical stimulation. This notion is in line with previous findings showing that action potentials induced by electrical stimulation of the retina can propagate directly to the visual cortex (Grützner et al., 1958), produce different evoked potentials (Potts et al., 1968) and modulate central rhythms (Schmidt et al., 2013a) as well as large scale networks of the brain (Bola et al., 2014).
Beyond fatigue, the possibility of direct structural damage to central nervous structures by rACS seems low considering the distance between charge injection and brain tissue as well as stimulation strength. Yet, for rhythmic PS the danger of inducing an epileptic seizure is well established. Although not found in this study, for electrical stimulation the danger must also be assumed to be high due to neurophysiological similarities with intermittent photic stimulation (IPS) (Brindley, 1955) and proven effects on central processes and neural synchrony (Parra et al., 2003). Additionally, although no reports of seizures after comparable electrical stimulation sessions exist (Brunoni et al., 2012), we will continue to employ photosensitivity and epilepsy as exclusion criteria for future rACS studies.
Having theoretically and experimentally characterized the relative safety profile of rACS, we believe future studies can further investigate retinal mechanisms of action for ACS effects, especially in comparison with tACS. Additionally, rACS allows for studies addressing the interaction of different signal types entering the visual system through two separate input channels (left and right eye) and converging at the level of the primary visual cortex. This provides an promising tool for studies aiming to address a common framework of action for NiBS with more than one input-signal, e.g., noise and oscillation (Schmidt et al., 2013b).
The datasets generated for this study are available on request to the corresponding author.
All protocols conformed to the Declaration of Helsinki, and were approved by the Ethics Committee of the Charité – Universitätsmedizin Berlin (“Ethikkommission der Charité – Universitätsmedizin Berlin”). Informed consent was obtained from all individual participants included in the study. This study adheres to the principles of good scientific practice of the Charité – Universitätsmedizin Berlin (“Grundsätze der Charité zur Sicherung guter wissenschaftlicher Praxis”).
LH, AD, SS, MS, and SB conceived and designed the study. LH, AD, CT, AJ, and SS carried out data acquisition and analysis. LH, AD, and SS drafted the manuscript. CT, AJ, AK, MR, MS, and SB critically revised the manuscript. All authors participated in the interpretation of the data.
This work was supported by the German Research Foundation, DFG grant BR 1691/8-1 and OB 102/22-1.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2019.00783/full#supplementary-material
EF, electrical field; NiBS:, non-invasive brain stimulation; NRS, numeric rating scale; PS, photic stimulation; rACS:, retinofugal alternating current stimulation; RPE, retinal pigment epithelium; tACS, transcranial alternating current stimulation.
Agnew, W. F., and McCreery, D. B. (1987). Considerations for safety in the use of extracranial stimulation for motor evoked potentials. Neurosurgery 20, 143–147.
Antal, A., Boros, K., Poreisz, C., Chaieb, L., Terney, D., and Paulus, W. (2008). Comparatively weak after-effects of transcranial alternating current stimulation (tACS) on cortical excitability in humans. Brain Stimul. 1, 97–105. doi: 10.1016/j.brs.2007.10.001
Bath, P. M., Brainin, M., Brown, C., Campbell, B., Davis, S. M., Donnan, G. A., et al. (2014). Testing devices for the prevention and treatment of stroke and its complications. Int. J. Stroke 9, 683–695. doi: 10.1111/ijs.12302
Bikson, M., and Datta, A. (2012). Guidelines for precise and accurate computational models of tDCS. Brain Stimul. 5, 430–431. doi: 10.1016/j.brs.2011.06.001
Bikson, M., Datta, A., and Elwassif, M. (2009). Establishing safety limits for transcranial direct current stimulation. Clin. Neurophysiol. 120, 1033–1034. doi: 10.1016/j.clinph.2009.03.018
Bikson, M., Grossman, P., Thomas, C., Zannou, A. L., Jiang, J., Adnan, T., et al. (2016). Safety of transcranial direct current stimulation: evidence based update 2016. Brain Stimul. 9, 641–661. doi: 10.1016/j.brs.2016.06.004
Bola, M., Gall, C., Moewes, C., Fedorov, A., Hinrichs, H., and Sabel, B. A. (2014). Brain functional connectivity network breakdown and restoration in blindness. Neurology 83, 542–551. doi: 10.1212/WNL.0000000000000672
Brindley, G. S. (1955). The site of electrical excitation of the human eye. J. Physiol. 127, 189–200. doi: 10.1113/jphysiol.1955.sp005248
Brittain, J. S., Probert-Smith, P., Aziz, T. Z., and Brown, P. (2013). Tremor suppression by rhythmic transcranial current stimulation. Curr. Biol. 23, 436–440. doi: 10.1016/j.cub.2013.01.068
Brown, C. C. (1975). Electroanesthesia and electrosleep. Am. Psychol. 30, 402–410. doi: 10.1037/0003-066x.30.3.402
Brunoni, A. R., Amadera, J., Berbel, B., Volz, M. S., Rizzerio, B. G., and Fregni, F. (2011). A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int. J. Neuropsychopharmacol. 14, 1133–1145. doi: 10.1017/S1461145710001690.
Brunoni, A. R., Nitsche, M. A., Bolognini, N., Bikson, M., Wagner, T., Merabet, L., et al. (2012). Clinical research with transcranial direct current stimulation (tDCS): challenges and future directions. Brain Stimul. 5, 175–195. doi: 10.1016/j.brs.2011.03.002
Chaieb, L., Antal, A., Pisoni, A., Saiote, C., Opitz, A., Ambrus, G. G., et al. (2014). Safety of 5 kHz tACS. Brain Stimul. 7, 92–96. doi: 10.1016/j.brs.2013.08.004
Chaudhuri, A., and Behan, P. O. (2004). Fatigue in neurological disorders. Lancet 363, 978–988. doi: 10.1016/S0140-6736(04)15794-2
Cobb, S. (1947). Photic driving as a cause of clinical seizures in epileptic patients. Arch. Neurol. Psychiatry 58:70. doi: 10.1001/archneurpsyc.1947.02300300080008
Datta, A., Baker, J. M., Bikson, M., and Fridriksson, J. (2011). Individualized model predicts brain current flow during transcranial direct-current stimulation treatment in responsive stroke patient. Brain Stimul. 4, 169–174. doi: 10.1016/j.brs.2010.11.001
Datta, A., Truong, D., Minhas, P., Parra, L., and Bikson, M. (2012). Inter-individual variation during transcranial direct current stimulation and normalization of dose using MRI-derived computational models. Front. Psychiatry 3:91. doi: 10.3389/fpsyt.2012.00091
Delbeke, J. (2011). Electrodes and chronic optic nerve stimulation. Biocybern. Biomed. Eng. 31, 81–94. doi: 10.1016/s0208-5216(11)70021-3
Delbeke, J., Parrini, S., Andrien, A., Oozer, M., Legat, V., and Veraart, C. (2000). Modelling activation of visual structures through eyelid surface electrodes: preliminary result. Pflügers Archiv. Eur. J. Physiol. 440:R4.
Delbeke, J., Pins, D., Michaux, G., Wanet-Defalque, M. -C., Parrini, S., and Veraart, C. (2001). Electrical stimulation of anterior visual pathways in retinitis pigmentosa. Invest. Ophthalmol. Vis. Sci. 42, 291–297.
Downie, W., Leatham, P., Rhind, V., Wright, V., Branco, J., and Anderson, J. (1978). Studies with pain rating scales. Ann. Rheum. Dis. 37, 378–381.
Dzhokic, G., Jovchevska, J., and Dika, A. (2008). Electrical injuries: etiology, pathophysiology and mechanism of injury. Macedonian J. Med. Sci. 1, 54–58. doi: 10.3889/mjms.1857-5773.2008.0019
Farrar, J. T., Young, J. P. Jr., LaMoreaux, L., Werth, J. L., and Poole, R. M. (2001). Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 94, 149–158. doi: 10.1016/s0304-3959(01)00349-9
Feurra, M., Bianco, G., Santarnecchi, E., Del Testa, M., Rossi, A., and Rossi, S. (2011). Frequency-dependent tuning of the human motor system induced by transcranial oscillatory potentials. J. Neurosci. 31, 12165–12170. doi: 10.1523/JNEUROSCI.0978-11.2011
Feurra, M., Pasqualetti, P., Bianco, G., Santarnecchi, E., Rossi, A., and Rossi, S. (2013). State-dependent effects of transcranial oscillatory currents on the motor system: what you think matters. J. Neurosci. 33, 17483–17489. doi: 10.1523/JNEUROSCI.1414-13.2013
Gall, C., Sgorzaly, S., Schmidt, S., Brandt, S., Fedorov, A., and Sabel, B. A. (2011). Noninvasive transorbital alternating current stimulation improves subjective visual functioning and vision-related quality of life in optic neuropathy. Brain Stimul. 4, 175–188. doi: 10.1016/j.brs.2011.07.003
Garnsworthy, R. K., Gully, R. L., Kenins, P., and Westerman, R. A. (1988). Transcutaneous electrical stimulation and the sensation of prickle. J. Neurophysiol. 59, 1116–1127. doi: 10.1152/jn.1988.59.4.1116
Gekeler, F., Messias, A., Ottinger, M., Bartz-Schmidt, K. U., and Zrenner, E. (2006). Phosphenes electrically evoked with DTL electrodes: a study in patients with retinitis pigmentosa, glaucoma, and homonymous visual field loss and normal subjects. Invest. Ophthalmol. Vis. Sci. 47, 4966–4974.
Gekeler, F., Wrobel, W.G., and Messias, A. (2011). Method for treating an eye. United States patent application US 13/199,904. Washington, DC: U.S. Patent and Trademark Office.
Gellner, A. K., Reis, J., and Fritsch, B. (2016). Glia: a neglected player in non-invasive direct current brain stimulation. Front. Cell. Neurosci. 10:188. doi: 10.3389/fncel.2016.00188
Grützner, A., Grüsser, O. -J., and Baumgartner, G. (1958). Reaktionen einzelner Neurone im optischen Cortex der Katze nach elektrischer Reizung des Nervus opticus. Arch. Psychiatrie Nervenkrankheiten 197, 377–404. doi: 10.1007/bf00345845
Guleyupoglu, B., Schestatsky, P., Edwards, D., Fregni, F., and Bikson, M. (2013). Classification of methods in transcranial electrical stimulation (tES) and evolving strategy from historical approaches to contemporary innovations. J. Neurosci. Methods 219, 297–311. doi: 10.1016/j.jneumeth.2013.07.016
Haberbosch, L., Schmidt, S., Jooß, A., Köhn, A., Kozarzewski, L., Rönnefarth, M., et al. (2019). Rebound or entrainment? The influence of alternating current stimulation on individual alpha. Front. Hum. Neurosci. 13:43. doi: 10.3389/fnhum.2019.00043
Hakkinen, V., Eskola, H., Yli-Hankala, A., Nurmikko, T., and Kolehmainen, S. (1995). Which structures are sensitive to painful transcranial electric stimulation? Electromyogr. Clin. Neurophysiol. 35, 377–383.
Hallett, M. (2007). Transcranial magnetic stimulation: a primer. Neuron 55, 187–199. doi: 10.1016/j.neuron.2007.06.026
Helfrich, R. F., Schneider, T. R., Rach, S., Trautmann-Lengsfeld, S. A., Engel, A. K., and Herrmann, C. S. (2014). Entrainment of brain oscillations by transcranial alternating current stimulation. Curr. Biol. 24, 333–339. doi: 10.1016/j.cub.2013.12.041
Herrick, R. M. (1967). Psychophysical methodology: comparison of thresholds of the method of limits and of the method of constant stimuli. Percept. Mot. Skills 24, 915–922. doi: 10.2466/pms.1967.24.3.915
Hummel, F. C., Celnik, P., Pascual-Leone, A., Fregni, F., Byblow, W. D., Buetefisch, C. M., et al. (2008). Controversy: noninvasive and invasive cortical stimulation show efficacy in treating stroke patients. Brain Stimul. 1, 370–382. doi: 10.1016/j.brs.2008.09.003
Iacono, M. I., Neufeld, E., Akinnagbe, E., Bower, K., Wolf, J., Vogiatzis Oikonomidis, I., et al. (2015). MIDA: a multimodal imaging-based detailed anatomical model of the human head and neck. PloS One 10:e0124126. doi: 10.1371/journal.pone.0124126
Irnich, W. (1980). The chronaxie time and its practical importance. Pacing Clin. Electrophysiol. 3, 292–301. doi: 10.1111/j.1540-8159.1980.tb05236.x
Irnich, W. (2010). The terms “chronaxie” and “rheobase” are 100 years old. Pacing Clin. Electrophysiol. 33, 491–496. doi: 10.1111/j.1540-8159.2009.02666.x
Jackson, M. P., Truong, D., Brownlow, M. L., Wagner, J. A., McKinley, R. A., Bikson, M., et al. (2017). Safety parameter considerations of anodal transcranial Direct Current Stimulation in rats. Brain Behav. Immun. 64, 152–161. doi: 10.1016/j.bbi.2017.04.008
Joundi, R. A., Jenkinson, N., Brittain, J. S., Aziz, T. Z., and Brown, P. (2012). Driving oscillatory activity in the human cortex enhances motor performance. Curr. Biol. 22, 403–407. doi: 10.1016/j.cub.2012.01.024
Kanai, R., Chaieb, L., Antal, A., Walsh, V., and Paulus, W. (2008). Frequency-dependent electrical stimulation of the visual cortex. Curr. Biol. 18, 1839–1843. doi: 10.1016/j.cub.2008.10.027
Kellogg, D. L. Jr., Johnson, J. M., and Kosiba, W. A. (1989). Selective abolition of adrenergic vasoconstrictor responses in skin by local iontophoresis of bretylium. Am. J. Physiol. 257(5 Pt 2), H1599-H1606.
Knutson, R.C. (1967). First international symposium on electrosleep therapy and electroanesthesia: a report. Anesth. Analg. 46, 333–339.
Laakso, I., and Hirata, A. (2013). Computational analysis shows why transcranial alternating current stimulation induces retinal phosphenes. J. Neural. Eng. 10:046009. doi: 10.1088/1741-2560/10/4/046009
Larntz, K. (1978). Small-sample comparisons of exact levels for chi-squared goodness-of-fit statistics. J. Am. Stat. Assoc. 73, 253–263. doi: 10.2307/2286650
Ledger, P. W. (1992). Skin biological issues in electrically enhanced transdermal delivery. Adv. Drug Delivery Rev. 9, 289–307. doi: 10.1016/0169-409X(92)90027-N
Liebetanz, D., Koch, R., Mayenfels, S., Konig, F., Paulus, W., and Nitsche, M. A. (2009). Safety limits of cathodal transcranial direct current stimulation in rats. Clin. Neurophysiol. 120, 1161–1167. doi: 10.1016/j.clinph.2009.01.022
Liew, S. L., Santarnecchi, E., Buch, E. R., and Cohen, L. G. (2014). Non-invasive brain stimulation in neurorehabilitation: local and distant effects for motor recovery. Front. Hum. Neurosci. 8:378. doi: 10.3389/fnhum.2014.00378
Lindenblatt, G., and Silny, J. (2002). Electrical phosphenes: on the influence of conductivity inhomogeneities and small-scale structures of the orbita on the current density threshold of excitation. Med. Biol. Eng. Comput. 40, 354–359. doi: 10.1007/bf02344219
Loo, C., Martin, D., Alonzo, A., Gandevia, S., Mitchell, P., and Sachdev, P. (2011). Avoiding skin burns with transcranial direct current stimulation: preliminary considerations. Int. J. Neuropsychopharmacol. 14, 425–426. doi: 10.1017/s1461145710001197
Ma, Z., Cao, P., Sun, P., Li, L., Lu, Y., Yan, Y., et al. (2014). Optical imaging of visual cortical responses evoked by transcorneal electrical stimulation with different parameters. Invest. Ophthalmol. Vis. Sci. 55, 5320–5331. doi: 10.1167/iovs.14-14600
Magerl, W., Szolcsanyi, J., Westerman, R. A., and Handwerker, H. O. (1987). Laser Doppler measurements of skin vasodilation elicited by percutaneous electrical stimulation of nociceptors in humans. Neurosci. Lett. 82, 349–354. doi: 10.1016/0304-3940(87)90281-3
Marshall, L., Helgadottir, H., Molle, M., and Born, J. (2006). Boosting slow oscillations during sleep potentiates memory. Nature 444, 610–613. doi: 10.1038/nature05278
Merrill, D. R., Bikson, M., and Jefferys, J. G. (2005). Electrical stimulation of excitable tissue: design of efficacious and safe protocols. J. Neurosci. Methods 141, 171–198. doi: 10.1016/j.jneumeth.2004.10.020
Montgomery, S. A., and Asberg, M. (1979). A new depression scale designed to be sensitive to change. Br. J. Psychiatry 134, 382–389. doi: 10.1192/bjp.134.4.382
Neuling, T., Wagner, S., Wolters, C. H., Zaehle, T., and Herrmann, C. S. (2012). Finite-element model predicts current density distribution for clinical applications of tDCS and tACS. Front. Psychiatry 3:83. doi: 10.3389/fpsyt.2012.00083
Nitsche, M. A., Liebetanz, D., Lang, N., Antal, A., Tergau, F., and Paulus, W. (2003). Safety criteria for transcranial direct current stimulation (tDCS) in humans. Clin. Neurophysiol. 114, 2220–2222. doi: 10.1016/s1388-2457(03)00235-9
Obrosow, A. E. (1959). “Electrosleep therapy,” in Therapeutic Electricity and Ultraviolet Radiation, ed. S. Licht (New Haven, CT: Imprint unknown), 169.
Parra, J., Kalitzin, S., Iriarte, J., Blanes, W., Velis, D., and Da Silva, F. L. (2003). Gamma-band phase clustering and photosensitivity: is there an underlying mechanism common to photosensitive epilepsy and visual perception? Brain 126, 1164–1172. doi: 10.1093/brain/awg109
Paulus, W. (2003). Transcranial direct current stimulation (tDCS). Suppl. Clin. Neurophysiol. 56, 249–254. doi: 10.1016/s1567-424x(09)70229-6
Paulus, W. (2010). On the difficulties of separating retinal from cortical origins of phosphenes when using transcranial alternating current stimulation (tACS). Clin. Neurophysiol. 121, 987–991. doi: 10.1016/j.clinph.2010.01.029
Paulus, W., Peterchev, A. V., and Ridding, M. (2013). Transcranial electric and magnetic stimulation: technique and paradigms. Handbook Clin. Neurol. 116, 329–342. doi: 10.1016/B978-0-444-53497-2.00027-9
Peterchev, A. V., Wagner, T. A., Miranda, P. C., Nitsche, M. A., Paulus, W., Lisanby, S. H., et al. (2012). Fundamentals of transcranial electric and magnetic stimulation dose: definition, selection, and reporting practices. Brain Stimul. 5, 435–453. doi: 10.1016/j.brs.2011.10.001
Pogosyan, A., Gaynor, L. D., Eusebio, A., and Brown, P. (2009). Boosting cortical activity at Beta-band frequencies slows movement in humans. Curr. Biol. 19, 1637–1641. doi: 10.1016/j.cub.2009.07.074
Polania, R., Paulus, W., and Nitsche, M. A. (2012). Noninvasively decoding the contents of visual working memory in the human prefrontal cortex within high-gamma oscillatory patterns. J. Cogn. Neurosci. 24, 304–314. doi: 10.1162/jocn_a_00151
Poreisz, C., Boros, K., Antal, A., and Paulus, W. (2007). Safety aspects of transcranial direct current stimulation concerning healthy subjects and patients. Brain Res. Bull. 72, 208–214. doi: 10.1016/j.brainresbull.2007.01.004
Potts, A. M., Inoue, J., and Buffum, D. (1968). The electrically evoked response of the visual system (EER). Invest. Ophthalmol. Vis. Sci. 7, 269–278.
Rager, G., and Singer, W. (1998). The response of cat visual cortex to flicker stimuli of variable frequency. Eur. J. Neurosci. 10, 1856–1877. doi: 10.1046/j.1460-9568.1998.00197.x
Robinovitch, L. (1914). “Electrical analgesia, sleep and resuscitation,” in Anesthesia, ed. J.T. Gwathmey (New York, NY: D. Appleton and Company), 628–643.
Rohracher, H. (1935). Die gehirnelektrischen Erscheinungen bei geistiger Arbeit. Zeitschrift für Psychologie und Charakterkunde 136 308–324.
Sandrini, M., and Cohen, L.G. (2013). “Noninvasive brain stimulation in neurorehabilitation,” in Handbook of Clinical Neurology, eds A.M. Lozano & M. Hallett (Amsterdam: Elsevier), 499–524. doi: 10.1016/b978-0-444-53497-2.00040-1
Santarnecchi, E., Muller, T., Rossi, S., Sarkar, A., Polizzotto, N. R., Rossi, A., et al. (2016). Individual differences and specificity of prefrontal gamma frequency-tACS on fluid intelligence capabilities. Cortex 75, 33–43. doi: 10.1016/j.cortex.2015.11.003
Santarnecchi, E., Polizzotto, N. R., Godone, M., Giovannelli, F., Feurra, M., Matzen, L., et al. (2013). Frequency-dependent enhancement of fluid intelligence induced by transcranial oscillatory potentials. Curr. Biol. 23, 1449–1453. doi: 10.1016/j.cub.2013.06.022
Saturnino, G. B., Antunes, A., and Thielscher, A. (2015). On the importance of electrode parameters for shaping electric field patterns generated by tDCS. Neuroimage 120, 25–35. doi: 10.1016/j.neuroimage.2015.06.067
Schmidt, S., Mante, A., Ronnefarth, M., Fleischmann, R., Gall, C., and Brandt, S. A. (2013a). Progressive enhancement of alpha activity and visual function in patients with optic neuropathy: a two-week repeated session alternating current stimulation study. Brain Stimul. 6, 87–93. doi: 10.1016/j.brs.2012.03.008
Schmidt, S., Scholz, M., Obermayer, K., and Brandt, S. A. (2013b). Patterned brain stimulation, what a framework with rhythmic and noisy components might tell us about recovery maximization. Front. Hum. Neurosci. 7:325. doi: 10.3389/fnhum.2013.00325
Schutter, D. J. (2016). Cutaneous retinal activation and neural entrainment in transcranial alternating current stimulation: a systematic review. Neuroimage 140, 83–88. doi: 10.1016/j.neuroimage.2015.09.067
Sergeev, G. V. (1963). Electrosleep as a method of neurotropic therapy of patients with hypertensive disease. Am. Heart J. 66, 138–139. doi: 10.1016/0002-8703(63)90081-4
Streiner, D. L., and Norman, G. R. (2008). Health Measurement Scales: A Practical Guide to their Development and Use. Oxford: Oxford university press.
Talelli, P., and Rothwell, J. (2006). Does brain stimulation after stroke have a future? Curr. Opin. Neurobiol. 19, 543–550. doi: 10.1097/WCO.0b013e32801080d1
Thil, M.-A., Duy, D. T., Colin, I. M., and Delbeke, J. (2007). Time course of tissue remodelling and electrophysiology in the rat sciatic nerve after spiral cuff electrode implantation. J. Neuroimmunol. 185, 103–114. doi: 10.1016/j.jneuroim.2007.01.021
Ticleanu, C., and Littlefair, P. (2015). A summary of LED lighting impacts on health. Int. J. Sustain. Light. 17, 5–11. doi: 10.26607/ijsl.v17i0.11
Trenite, D. G., Binnie, C. D., Harding, G. F., Wilkins, A., Covanis, T., Eeg-Olofsson, O., et al. (1999). Medical technology assessment photic stimulation–standardization of screening methods. Neurophysiol. Clin. 29, 318–324. doi: 10.1016/s0987-7053(99)90045-x
Tuckett, R. P. (1982). Itch evoked by electrical stimulation of the skin. J. Invest. Dermatol. 79, 368–373. doi: 10.1111/1523-1747.ep12529734
Vossen, A., Gross, J., and Thut, G. (2015). Alpha power increase after transcranial alternating current stimulation at alpha frequency (alpha-tACS) reflects plastic changes rather than entrainment. Brain Stimul. 8, 499–508. doi: 10.1016/j.brs.2014.12.004
Walker, A. E., Woolf, J. I., Halstead, W. C., and Case, T. J. (1944). Photic driving. Arch. Neurol. Psychiatry 52, 117–125.
Wester, K., Jönsson, A. K., Spigset, O., Druid, H., and Hägg, S. (2008). Incidence of fatal adverse drug reactions: a population based study. Br. J. Clin. Pharmacol. 65, 573–579. doi: 10.1111/j.1365-2125.2007.03064.x
Yuen, T. G., Agnew, W. F., Bullara, L. A., Jacques, S., and McCreery, D. B. (1981). Histological evaluation of neural damage from electrical stimulation: considerations for the selection of parameters for clinical application. Neurosurgery 9, 292–299. doi: 10.1227/00006123-198109000-00013
Zaghi, S., Acar, M., Hultgren, B., Boggio, P. S., and Fregni, F. (2010). Noninvasive brain stimulation with low-intensity electrical currents: putative mechanisms of action for direct and alternating current stimulation. Neuroscientist 16, 285–307. doi: 10.1177/1073858409336227
Keywords: retinofugal alternating current stimulation, electrical stimulation, feasibility, tolerability, safety, adverse events, finite element modeling
Citation: Haberbosch L, Datta A, Thomas C, Jooß A, Köhn A, Rönnefarth M, Scholz M, Brandt SA and Schmidt S (2019) Safety Aspects, Tolerability and Modeling of Retinofugal Alternating Current Stimulation. Front. Neurosci. 13:783. doi: 10.3389/fnins.2019.00783
Received: 24 March 2019; Accepted: 12 July 2019;
Published: 07 August 2019.
Edited by:
Mikhail Lebedev, Duke University, United StatesReviewed by:
Till R. Schneider, Universität Hamburg, GermanyCopyright © 2019 Haberbosch, Datta, Thomas, Jooß, Köhn, Rönnefarth, Scholz, Brandt and Schmidt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Linus Haberbosch, bGludXMuaGFiZXJib3NjaEBjaGFyaXRlLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.