Corrigendum: Sex-differences in oral anticoagulant-related intracerebral hemorrhage
 Josefine Grundtvig1,2*
Josefine Grundtvig1,2* Christian Ovesen1
Christian Ovesen1 Thorsten Steiner2,3,4
Thorsten Steiner2,3,4 Cheryl Carcel5David Gaist6
Cheryl Carcel5David Gaist6 Louisa Christensen1,2Jacob Marstrand1,2Per Meden1,2Sverre Rosenbaum1
Louisa Christensen1,2Jacob Marstrand1,2Per Meden1,2Sverre Rosenbaum1 Helle K. Iversen2,7Christina Kruuse2,8Thomas Christensen7Karen Ægidius6
Helle K. Iversen2,7Christina Kruuse2,8Thomas Christensen7Karen Ægidius6 Inger Havsteen9
Inger Havsteen9 Hanne Christensen1,2*
Hanne Christensen1,2*- 1Department of Neurology, Bispebjerg Hospital, Copenhagen, Denmark
- 2Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
- 3Department of Neurology, Klinikum Frankfurt Höchst, Frankfurt, Germany
- 4Department of Neurology, Heidelberg University Hospital, Heidelberg, Germany
- 5The George Institute for Global Health, University of New South Wales, Sydney, NSW, Australia
- 6Research Unit for Neurology, Odense University Hospital, University of Southern Denmark, Odense, Denmark
- 7Department of Neurology, Rigshospitalet, Copenhagen, Denmark
- 8Department of Neurology, Herlev Hospital, Copenhagen, Denmark
- 9Department of Radiology, Bispebjerg Hospital, Copenhagen, Denmark
Introduction and Aim: Data remain limited on sex-differences in patients with oral anticoagulant (OAC)-related intracerebral hemorrhage (ICH). We aim to explore similarities and differences in risk factors, acute presentation, treatments, and outcome in men and women admitted with OAC-related ICH.
Method: This study was a retrospective observational study based on 401 consecutive patients with OAC-related ICH admitted within 24 h of symptom onset. The study was registered on osf.io. We performed logarithmic regression and cox-regression adjusting for age, hematoma volume, Charlson Comorbidity Index (CCI), and pre-stroke modified Ranking Scale (mRS). Gender and age were excluded from CHA2DS2-VASc and CCI was not adjusted for age.
Results: A total of 226 men and 175 women were identified. More men were pre-treated with vitamin K-antagonists (73.5% men vs. 60.6% women) and more women with non-vitamin K-antagonist oral anticoagulants (26.5% men vs. 39.4% women), p = 0.009. Women were older (mean age 81.9 vs. 76.9 years, p < 0.001). CHA2DS2-VASc and CCI were similar in men and women.
Hematoma volumes (22.1 ml in men and 19.1 ml in women) and National Institute of Health Stroke Scale (NIHSS) scores (13 vs. 13) were not statistically different, while median Glasgow Coma Scale (GCS) was lower in women, (14 [8;15] vs. 14 [10;15] p = 0.003).
Women's probability of receiving reversal agents was significantly lower (adjusted odds ratio [aOR] = 0.52, p = 0.007) but not for surgical clot removal (aOR = 0.56, p = 0.25). Women had higher odds of receiving do-not-resuscitate (DNR) orders within a week (aOR = 1.67, p = 0.04). There were no sex-differences in neurological deterioration (aOR = 1.48, p = 0.10), ability to walk at 3 months (aOR = 0.69, p = 0.21) or 1-year mortality (adjusted hazard ratio = 1.18, p = 0.27).
Conclusion: Significant sex-differences were observed in age, risk factors, access to treatment, and DNRs while no significant differences were observed in comorbidity burden, stroke severity, or hematoma volume. Outcomes, such as adjusted mortality, ability to walk, and neurological deterioration, were comparable. This study supports the presence of sex-differences in risk factors and care but not in presentation and outcomes.
Introduction
There is a growing literature documenting sex differences in risk factors, presentation, treatment interventions, and outcome in stroke. Women are in general older at the time of stroke and have a higher frequency of hypertension (1). Atrial fibrillation (AF) increases the risk of stroke more in women than it does in men (2). Women are also more likely to present with non-traditional stroke symptoms as compared to men and women possibly have a greater benefit from physical activity in the prevention of cardiovascular disease (1). It is consistently reported that women have worse outcomes after stroke, which partly results from older age, worse pre-stroke functional status, and higher comorbidity; however, after adjusting for these factors, women still have worse outcomes (1).
A recent publication demonstrated (3) that women with acute stroke were more likely to be admitted to an acute stroke unit, but less likely to be intubated, to be given treatment for fever, or be admitted to an Intensive Care Unit (ICU). On admission, women had higher odds of having received pre-stroke antihypertensive medication and lower odds of taking antiplatelets, being treated with antidiabetics or lipid-lowering drugs, while no differences in the use of oral anticoagulants were observed. In the total stroke population, case-fatality rates were higher in women than men. However, in multivariable analyses, the risk of death was lower in women than men indicating that the unadjusted estimates were due to confounding. This finding was not significant in the intracerebral hemorrhage (ICH) population alone (3). Based on the 5-dimensional EuroQol, female patients have significantly worse scores on all parameters except for mobility (3). A sub-analysis of the Intensive Blood Pressure Reduction in Acute Cerebral Hamorrhage trials (INTERACT 1 and 2) found a higher adjusted mortality in men as compared to women (4).
Oral anticoagulant (OAC)-related ICH is a devastating presentation of stroke with very high fatality rates (5–7). Following the increased use of OAC, the number of patients with OAC-related ICH is increasing (8). So far, there are no reports available that have explored if sex-differences are present in the OAC-related ICH.
The aim of this study was to investigate that sex differences were present in risk factors, acute presentation, treatment interventions, and outcome in OAC-related ICH.
Materials and Methods
COOL-ICH
The analysis was performed using data from the Capital Region Anticoagulation-related ICH study (the COOL-ICH study) cohort. The cohort was based on all patients presenting with an imaging-confirmed OAC-related ICH within 24 h of symptom onset to one of five neurological or neurosurgical departments in the Capital Region of Denmark (approximate population of 1.9 million) from January 2010 to June 2018. In Denmark, the procedure for all patients with stroke is to admit them to a stroke unit and these admissions are then audited by the Danish Stroke Registry (9, 10). For this study, patients were identified for the COOL-ICH cohort using two different approaches: (1) the Danish Stroke Registry in which all departments treating stroke patients are legally obliged to report to and (2) by discharge lists from the individual neurology and neurosurgery departments. Patients with an underlying cause (e.g., vascular malformation or trauma) or a pre-stroke modified Rankin Scale (mRS) above 4 were excluded (Figure 1).
FIGURE 1
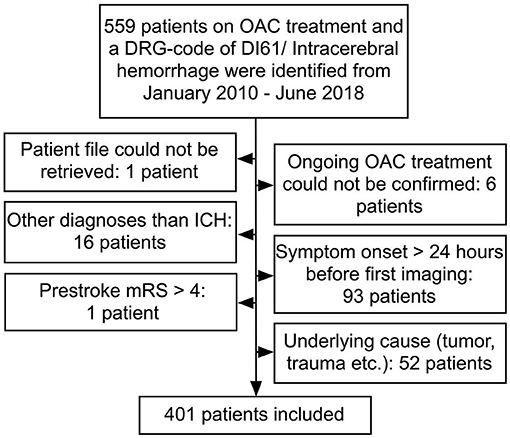
Figure 1. Patient flow. Patients may be counted more than once, if they fulfilled more than one exclusion criteria. OAC, oral anticoagulant; ICH, intracerebral hemorrhage; mRS, modified Rankin Scale.
National Institute of Health Stroke Scale (NIHSS) was if not available in patients' files estimated (11). Female sex and age were excluded from CHA2DS2-VASc (12) as a predictor to be able to compare men and women. To be able to assess multimorbidity separate from age, we did not age-adjust Charlson Comorbidity Index (CCI) (13). The ability to walk at 3 months was assessed based on the note closest to 3 months after stroke in the patient's file.
All clinical imaging was systematically assessed by one senior neuroradiologist (IH). The neuroradiologist was blinded to all other information than the imaging prescription note. This would always include sex and age and may or may not have included information on OAC and concomitant diseases. Hematoma volume was assessed using the ABC/2 method (14). For each participant outcome, data (neurological deterioration and ability to walk) were adjudicated by two independent senior neurologists (LC, JM, PM, SR, HI, CK, TC, and KÆ) based on medical charts, which were blinded for admission to hospital, treating physicians and type of oral anticoagulant; in cases of disagreement, HC had the final say. Neurological deterioration was defined as a fall in Glasgow Coma Scale (GCS) of 2 points or more, and an increase in NIHSS of 4 points or more or 4 strokes. In progression (SIP) score points, using the first recorded neurological status as reference. A more comprehensive protocol is available online, which was completed before the initiation of data acquisition (15).
MEDSTAT
MEDSTAT is a publicly available online database based on all prescription drugs dispensed at Danish pharmacies, from which aggregate yearly numbers can be retrieved (16). Based on numbers from the Capital Region of Denmark, accessed in MEDSTAT, we retrieved the number of patients for each year (2010–2018) who had presented a prescription for a Vitamin-K antagonist [VKA, ATC B01AA (17)], Dabigatran [ATC B01AE07 (18)], or a direct factor Xa inhibitor [ATC B01AF (18)].
Statistical Analysis
For each group (men or women), we calculated means and medians as appropriate on numerical variables and percentages for categorical variables. Differences were tested using the t-test or Mann–Whitney U test and the chi-square or Fisher's exact test. Based on the MEDSTAT data, we made a figure, including the number of patients per year of both men and women treated with either VKAs or non-vitamin K-antagonist oral anticoagulants (NOACs) during 2010–2018, as well as a figure with number of ICHs per year, per 1,000 patients who had presented at least one prescription for either NOAC or VKA during that year. We calculated unadjusted odds ratios (ORs) between men and women for pharmacological reversal, surgical clot removal, external ventricular drains (EVD), ICU (neuro-intensive or general), intubation, and do-not-resuscitate (DNR) orders within 24 h as well as within the first week, neurological deterioration within 24 h and 7 days and finally for the ability to walk at 3 months. We also calculated adjusted ORs for men and women with the above-mentioned variables; adjusting for age, CCI, hematoma volume, pre-stroke mRS, and admission GCS. The Cox regression was performed using days from ICH admission until both 1-year death and 7-day death with sex as the independent variable. Both an unadjusted hazard ratio (HR) was calculated as well as one where we adjusted for the same variables as in the logistic regression. For pre-stroke mRS, we detected non-proportional hazards, and stratified this variable, with only a small change in the coefficient for sex.
Ethics
The COOL-ICH study was approved by the Danish Patient Safety Authority (3-3013-2102/1) and the Danish Protection Agency (2012-58-0004). No ethical approval was needed for this study according to the Danish law. Data reporting was followed the STROBE statement.
Results
Occurrence of OAC-ICH in Men and Women
In the COOL-ICH cohort, 226 (56.4%) patients were men and 175 (43.6%) patients were women. Looking at sales of OAC, more men than women were treated with both NOAC and VKA during the study period, but number of ICH per 1,000 patients treated with OAC were comparable, though most years, this was a little lower for NOAC-treated men than for NOAC-treated women (Figure 2).
FIGURE 2
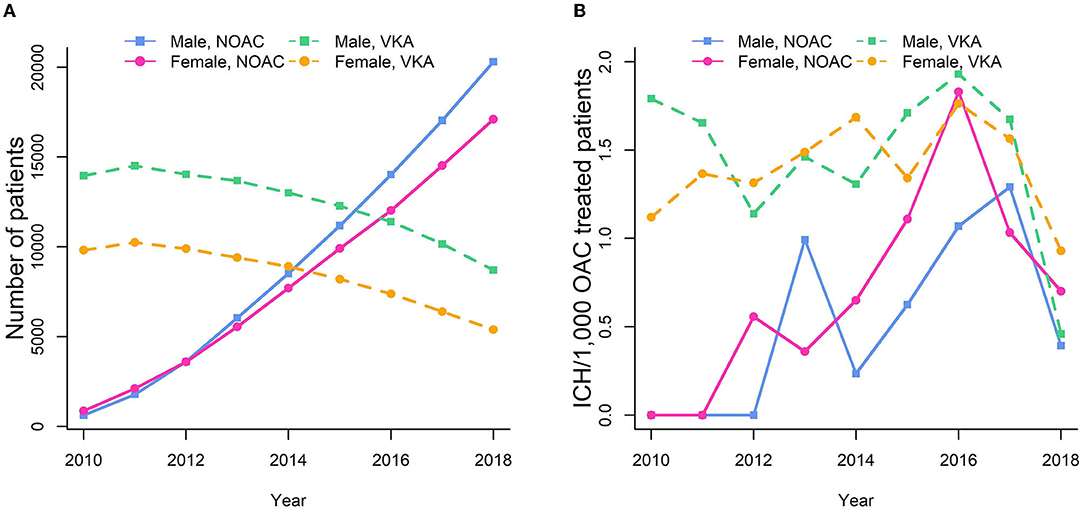
Figure 2. (A) Sale of OAC by sex. (B) ICHs/1,000 patients who have presented at least one prescription within that year.
Patient Characteristics
Female patients were significantly older and had a significantly higher pre-stroke mRS (Table 1). No differences were observed in risk factors (AF, hypertension, hyperlipidemia, previous ischemic stroke or transient ischemic attack, previous venous thromboembolism, diabetes, kidney disease, chronic pulmonary disease, congestive heart failure, previous myocardial infarction, and dementia) except for tobacco and alcohol use, where a significant male preponderance was observed (Table 1; Figure 3). There were no differences between men and women in CCI and CHA2DS2-VASc (Table 1; Figure 4).
TABLE 1
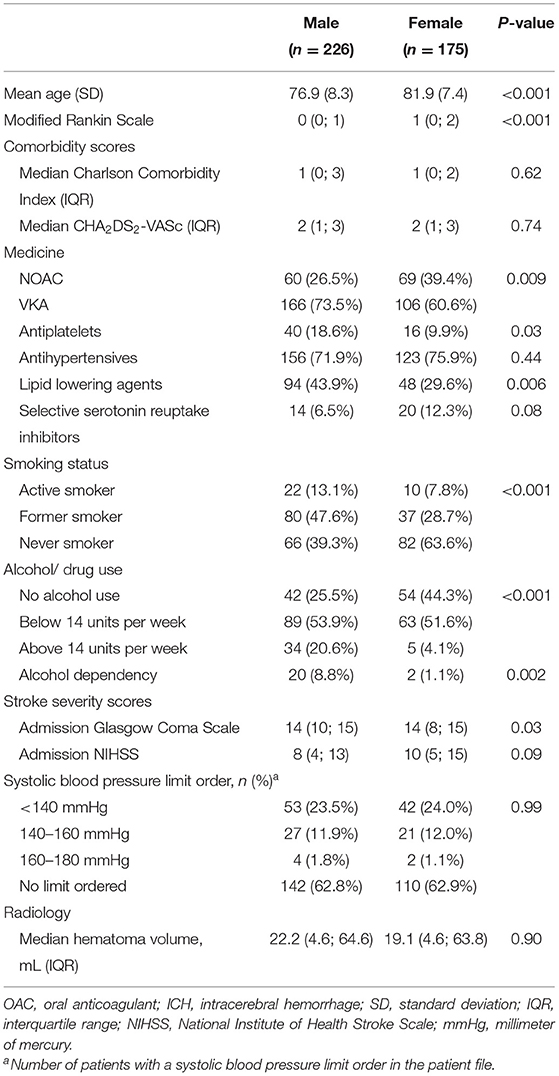
Table 1. Baseline data in 401 men and women with oral anticoagulant (OAC)-related intracerebral hemorrhage (ICH).
FIGURE 3
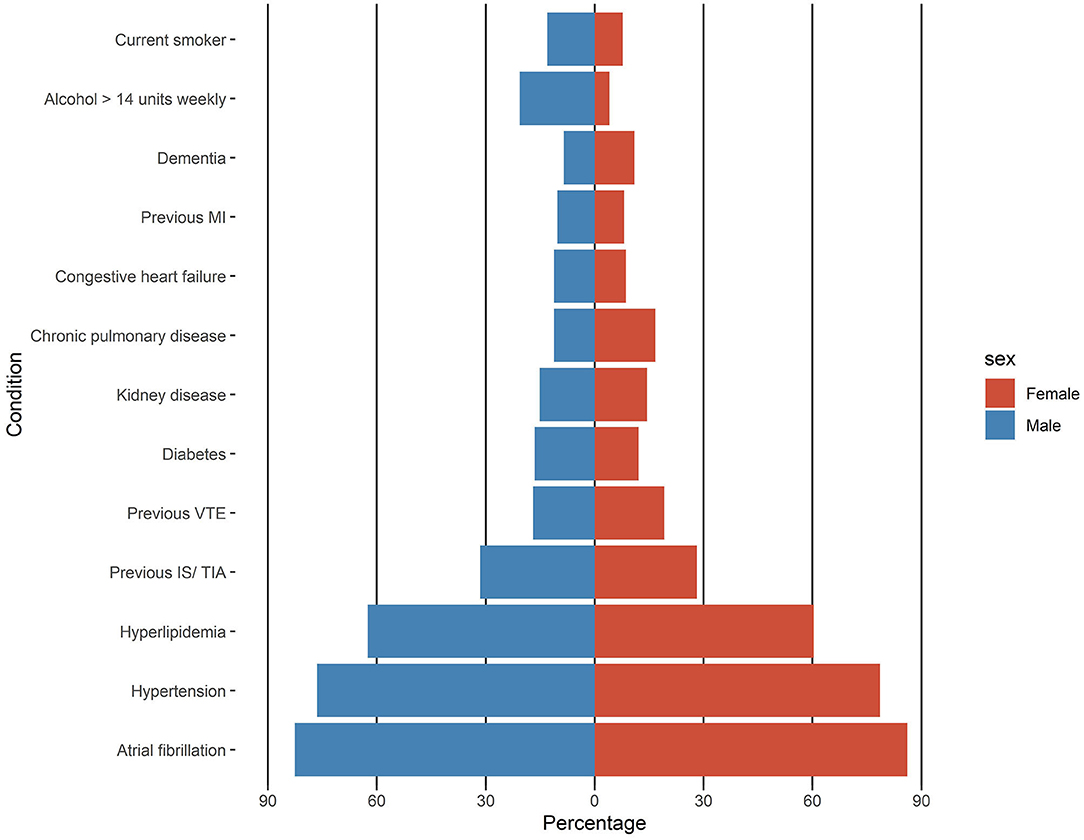
Figure 3. Baseline risk factors in men and women with oral anticoagulant-related intracerebral hemorrhage. MI, myocardial infarction; VTE, venous thromboembolism; IS, ischemic stroke; TIA, transient ischemic attack.
FIGURE 4
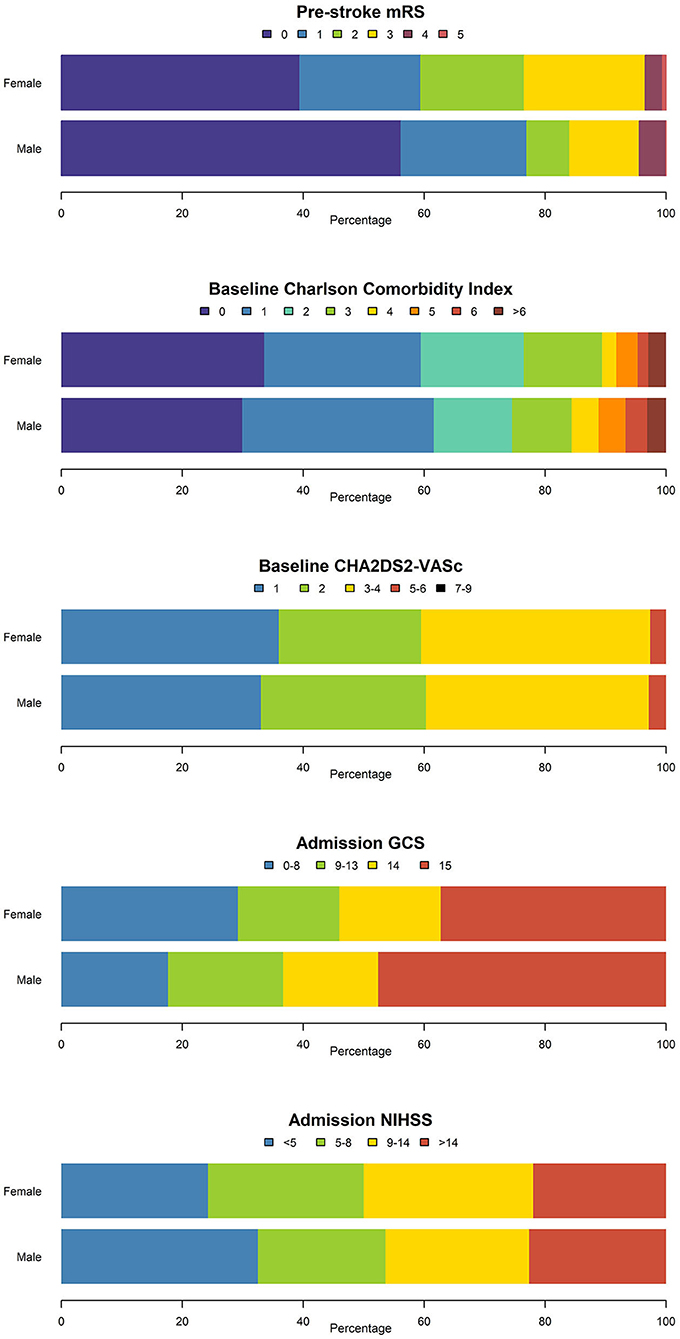
Figure 4. Disability-, comorbidity-, and stroke-severity scores in men and women with OAC-ICH. mRS, modified Rankin Scale; GCS, Glasgow Coma Scale; NIHSS, National Institutes of Health Stroke Scale.
Baseline Medications
In the COOL-ICH cohort, fewer men than women were on NOACs and more men were on VKAs (Table 1). Men were more frequently co-treated with antiplatelets as well as lipid-lowering drugs. There were no significant differences between men and women in the use of antihypertensive drugs or selective serotonin reuptake inhibitors (SSRI) (Table 1). Only three patients were concomitantly on dual antiplatelet treatment, one man and two women.
Acute ICH Event: Presentation and Interventions
Time from ICH symptom onset to admission was similar (p = 0.56) for male patients (median: 3.2 h, IQR: 1.4; 9.2) and female ones (median: 3.7 h, IQR: 1.6; 8.1). No significant difference in time to imaging was observed. Women had marginally more clinically severe presentations on admission, but this only reached significance in GCS and no differences were observed in hematoma volume (Table 1).
Men were significantly more likely to be treated with pharmacological reversal agents (e.g., prothrombin protein complex [any dose], platelet suspension, fresh frozen plasma, tranexamic acid, specific antidotes, etc.) than women (Table 2).
TABLE 2
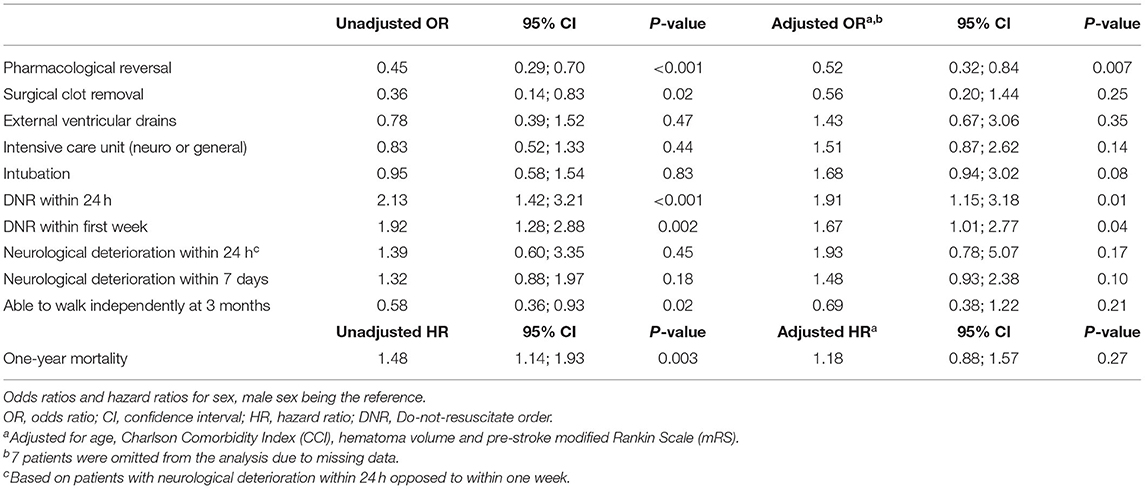
Table 2. Interventions and outcomes in 226 men and 175 women with OAC-related ICH.
No sex differences were present in prescribing systolic blood pressure limits for the administration of acute antihypertensive treatment; however, blood pressure orders were only applied in less than half of the patients (Table 1).
More men than women had surgical clot removal, but this was not significant in the adjusted analysis. No differences were observed in use of EVD (Table 2).
Do-Not-Resuscitate Orders
Do-not-resuscitate orders (DNRs) were given more often to women both within 7 days and 24 h based on both unadjusted OR and adjusted OR. The time from admission to the DNR decision was significantly longer for men than women, p = 0.01 (Figure 5). Of the patients that were given a DNR within 24 h, female patients were significantly older, had a significantly lower CCI as well as significantly lower hematoma volumes (57.6 ml vs. 50.2 ml, p < 0.001), with no differences between men and women with DNR orders in mRS, GCS, NIHSS, or 1-year mortality (Table 3).
FIGURE 5
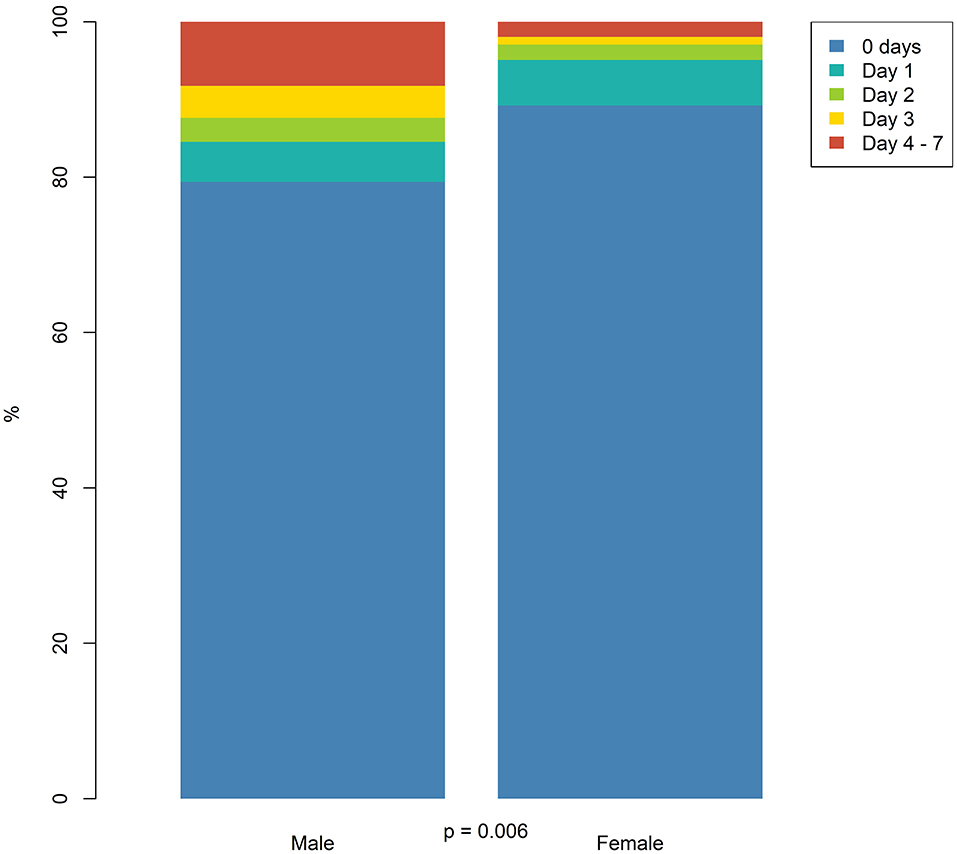
Figure 5. Time from admission to do-not-resuscitate (DNR) within the first week.
TABLE 3
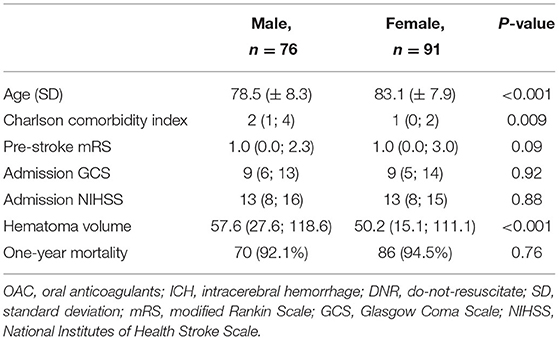
Table 3. Patients with OAC-related ICH given DNR orders within 24 h.
Outcome
No differences were observed in rates of neurological deterioration. Male patients were significantly more likely to be able to walk at 3 months than female patients, but this was not the case in the adjusted analysis (Table 2). The median time from the admission to the evaluation of the ability to walk was 82 days for men (IQR: 42; 92) and 71 days for women (IQR: 41; 93), p = 0.57. Fifty percent of male patients had died within 1 year of the ICH, in comparison to 65% of women (Figure 6); however, in the Cox-regression analysis, female sex did not increase the risk of 1-year death significantly (p = 0.33) when adjusting for age, hematoma volume, CCI, and pre-stroke mRS (Table 2).
FIGURE 6
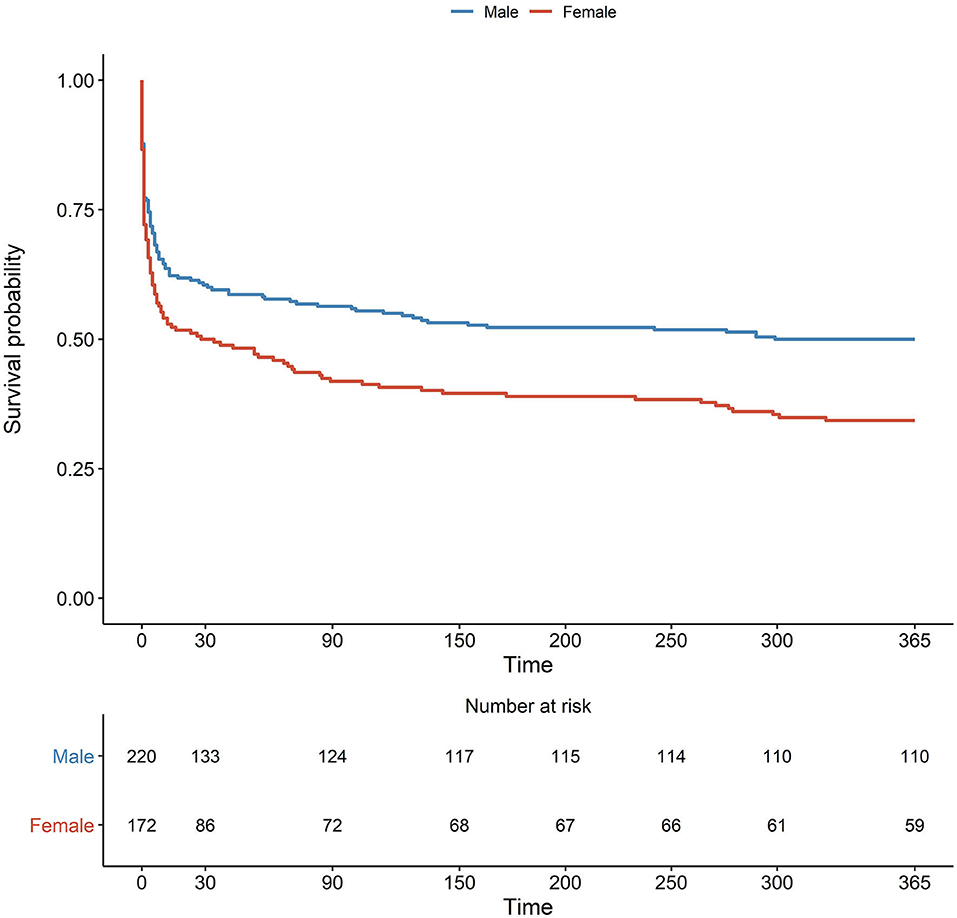
Figure 6. Kaplan–Meier plot with numbers at risk and number of events.
Discussion
More men than women were exposed to OAC in the Capital Region of Denmark during the observation period, with a comparable number of OAC-related ICH per 1,000 OAC-treated patients between men and women each year. Female patients were older and had a higher pre-stroke mRS. CCI and CHA2DS2-VASc were comparable in men and women. Fewer men than women were pre-treated with a NOAC. More men than women were pre-treated with VKA as well as concomitantly with antiplatelets and lipid-lowering agents. Male patients also had a higher tendency toward smoking and alcohol.
Upon the admission, female patients had a marginally, but significantly, lower GCS, with no differences in NIHSS or hematoma volume. Female patients were less likely to be given pharmacological reversal and more likely to be given a DNR order. When adjusting for age, hematoma volume, pre-stroke mRS, and CCI, there were no differences between men and women in neurological deterioration, ability to walk at 3 months or death.
Data from the American PINNACLE registry showed increased use of VKA in male as compared to female AF patients (19). Another study found that significantly more newly diagnosed male AF patients were treated with almost all types of OAC except for rivaroxaban. They also found a higher rate of ICH in the female patients, though this was no longer significant when adjusting for age, CCI, congestive heart failure, diabetes mellitus, region, insurance plan, and receipt of concomitant medications (20).
The observed differences in risk factors between the sexes, such as age, corroborate previous findings (1, 21). These findings are most likely determined both by biological and cultural factors.
The higher rates of the use of lipid-lowering agents and antiplatelets are in accordance to previous reports (3, 22–26). A potential explanation may be the higher frequency of atherosclerotic disease in men (22–26).
No differences were observed in NIHSS or hematoma volume, albeit GCS was somewhat lower in women. Nonetheless, women less often received reversal agents or clot removal surgery and DNR orders were more frequent. The lower frequency of women treated with clot removal surgery may be explained by the age, CCI, hematoma volume, and pre-stroke mRS of the women (Table 2). These factors, however, did not explain the difference in reversal agents or DNR orders. The sex difference in the use of DNR orders corresponds to previous findings in ICH patients (27) as well as patients successfully resuscitated from in-hospital cardiac arrest (28). The finding of female sex being an independent predictor of receiving a DNR order in the adjusted analyses underlines the need for further investigation into the unconscious bias in the doctors prescribing the DNR orders.
Female sex was no longer an independent predictor of neurological deterioration or inability to walk when adjusting for age, hematoma volume, CCI, and pre-stroke mRS. The observed unadjusted higher mortality in women was probably due to the sex differences in baseline characteristics, as adjusted analysis indicated no sex difference in case fatality.
Despite equal hematoma volume and NIHSS on admission, reversal therapy and surgical hematoma removal were less often applied to women in comparison to men, though in adjusted analysis, this only remained significant for reversal therapy, potentially due to less numbers in surgical treatment. This finding is in line with DNR orders being issued more frequently and earlier in female patients.
Sex differences in stroke care have previously been reported, however, adjusted survival rates are higher in women in comparison to men after stroke in most reports (1, 3, 21, 22, 24). We found no differences between sexes in adjusted 1-year mortality after ICH. However, DNR orders may worsen outcomes independently in ICH patients (29–32) and it is possible that the increased use of DNR orders in women in our study may have contributed to a decreased survival.
Our observation of few interventions in women with ICH is in accordance with previous reports (3). Guidelines in stroke care have changed during the observation period, and recommendations to proactively reverse anticoagulation were only implemented in Denmark at the end of the observation period (33). Nonetheless, this does not explain the difference in reversal attempts between the sexes. Although there is no strong evidence supporting neither reversal therapy so far, this is the case both in men and women, i.e., irrespective of gender (33, 34).
Implicit gender bias has been identified as an explanatory factor in testing in acute myocardial infarction (35), where female sex is associated with frailty and increased caution in relation to interventions. There are so far no data available if this phenomenon is also relevant to stroke.
With the well-known predictive value of DNRs (28–31), our findings underline the need for further investigation into the interaction of age, age bias, sex, and gender bias in treatment decisions. Our findings further support a difference in the pathophysiology of stroke in male and female patients—possibly at least partly based on lifestyle, underlining the need for including women in stroke trials but also the need for research in the pathophysiology of stroke in men and women.
Limitations
There are some limitations to this study: the study is retrospective and observational and restricted to hospitalized patients. This methodology may have reduced the validity of variables that are mostly narratively described in patients' files, including neurological deterioration and ability to walk at 3-months. Despite mandatory admission to the stroke unit, some patients may have been missed, e.g., due to death before hospital admission or if admitted to another specialty in case of other higher prioritized condition, or if diagnostic brain imaging was only performed at 24 h or later. Based on our data, it was not possible to assess adherence to prescribed OAC. No quality-of-life data were available; these could have provided further insights into qualitative outcomes. As to blood pressure control in the acute phase, we only have data on the prescriptions, not on the actual blood pressure levels.
Strengths
The study is based on a well-defined catchment area (Capital Region of Denmark) with a public healthcare system providing all acute healthcare for the population free of charge and independent of personal income. The risk of selection bias is, therefore, low. All institutions have easy access to the explored interventions, such as reversal therapies. Data acquisition followed a detailed protocol, which was published before the data collection. All imaging were reassessed confirming a diagnosis, and endpoints adjudicated by senior neurologists.
Conclusions
This study demonstrated that women receive less treatment interventions and more DNR orders than men after OAC-related ICH. This cannot be fully explained by differences in the presentations of patients though age is no doubt a contributing factor. There is a need for research that can support reducing sex-based inequity in treatment and care. There were no significant differences in ICH rates between men and women.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
CO and HC conceived the study. JG, CO, HC, and TS developed the protocol. HC, JG, CO, TS, and DG planned data analysis. JG, CO, and HC acquired data and performed data analysis. JG performed the statistical analysis. IH planned and performed radiological analysis. LC, JM, PM, SR, HI, CK, TC, and KÆ adjudicated outcomes and HC re-adjudicated outcomes with conflicts between first two observers. All authors reviewed the manuscript critically and approved the final version of the manuscript.
Funding
This work was supported by the Lundbeck Foundation and Grosserer A.V. Lykfeldt of Hustrus Legat. The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of Interest
CO has received a travel grant from Merck, Sharp, and Dohme. HC has received personal honoraria for speaking/educational activities from Boehringer-Ingelheim, Bristol-Myers-Squibb, Bayer, Daichi-Sanko and has received honoraria paid to her institution for services as National Lead in trials sponsored by Bayer and Alexion.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cordonnier C, Sprigg N, Sandset EC, Pavlovic A, Sunnerhagen KS, Caso V, et al. Stroke in women—from evidence to inequalities. Nat Rev Neurol. (2017) 13:521–32. doi: 10.1038/nrneurol.2017.95
2. Nezu T, Hosomi N, Kondo K, Aoki S, Matsumoto M, Kobayashi S. Greater Severity of Neurological Defects in Women Admitted With Atrial Fibrillation-Related Stroke. Circ J. (2016) 80:250–5. doi: 10.1253/circj.CJ-15-0873
3. Carcel C, Wang X, Sandset EC, Delcourt C, Arima H, Lindley R, et al. Sex differences in treatment and outcome after stroke. Neurology. (2019) 93:e2170–80. doi: 10.1212/WNL.0000000000008615
4. Sandset EC, Wang X, Carcel C, Sato S, Delcourt C, Arima H, et al. Sex differences in treatment, radiological features and outcome after intracerebral haemorrhage: pooled analysis of Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage trials 1 and 2. Eur Stroke J. (2020) 5:345–50. doi: 10.1177/2396987320957513
5. Hart RG, Boop BS, Anderson DC. Oral anticoagulants and intracranial hemorrhage: facts and hypotheses. Stroke. (1995) 26:1471–7. doi: 10.1161/01.STR.26.8.1471
6. Hart RG, Diener HC, Yang S, Connolly SJ, Wallentin L, Reilly PA, et al. Intracranial hemorrhage in atrial fibrillation patients during anticoagulation with warfarin or dabigatran: The RE-LY trial. Stroke. (2012) 43:1511–7. doi: 10.1161/STROKEAHA.112.650614
7. Cervera Á, Amaro S, Chamorro Á. Oral anticoagulant-associated intracerebral hemorrhage. J Neurol. (2012) 259:212–24. doi: 10.1007/s00415-011-6153-3
8. Grundtvig J, Ovesen C, Havsteen I, Christensen T, Gaist D, Iversen HK, et al. Trends in incidence of oral anticoagulant-related intracerebral hemorrhage and sales of oral anticoagulants in Capital Region of Denmark 2010–2017. Eur Stroke J. (2021)239:698732110087. doi: 10.1177/23969873211008770
9. Johnsen S, Ingeman A, Holmager Hunborg H, Zielke Schaarup S, Gyllenborg J. The danish stroke registry. Clin Epidemiol. Volume. (2016) 8:697–702. doi: 10.2147/CLEP.S103662
10. Hald S, Kring Sloth C, Hey S, Madsen C, Nguyen N, Rodríguez L, et al. Intracerebral hemorrhage: positive predictive value of diagnosis codes in two nationwide Danish registries. Clin Epidemiol. Volume. (2018) 10:941–8. doi: 10.2147/CLEP.S167576
11. Williams LS, Yilmaz EY, Lopez-Yunez AM. Retrospective assessment of initial stroke severity with the NIH stroke scale. Stroke. (2000) 31:858–62. doi: 10.1161/01.STR.31.4.858
12. Lip GYH, Nieuwlaat R, Pisters R, Lane DA, Crijns HJGM. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach. Chest. (2010) 137:263–72. doi: 10.1378/chest.09-1584
13. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. (1987) 40:373–83. doi: 10.1016/0021-9681(87)90171-8
14. Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M, et al. The ABCs of measuring intracerebral hemorrhage volumes. Stroke. (1996) 27:1304–5. doi: 10.1161/01.STR.27.8.1304
15. Ovesen C, Christensen H. COOL-ICH protocol. (2018). Available online at: https://osf.io/85c94/ (accessed November 9, 2021).
16. Danish Health Data Authority. Own calculations based on MEDSTAT. Available online at: http://www.medstat.dk (accessed November 11, 2021).
17. WHO Collaborating Centre for Drug Statistics Methodology. ATC: Structure and Principles. 15-02-2018 Available online at: https://www.whocc.no/atc/structure_and_principles/ (accessed November 4, 2021).
18. WHO Collaborating Centre for Drug Statistics Methodology. ATC: Structure and Principles. 15-02-2018
19. Thompson LE, Maddox TM, Lei L, Grunwald GK, Bradley SM, Peterson PN, et al. Sex Differences in the Use of Oral Anticoagulants for Atrial Fibrillation: A Report From the National Cardiovascular Data Registry (NCDR ®) PINNACLE Registry. J Am Heart Assoc. (2017) 6:6801. doi: 10.1161/JAHA.117.005801
20. Yong CM, Tremmel JA, Lansberg MG, Fan J, Askari M, Turakhia MP. Sex differences in oral anticoagulation and outcomes of stroke and intracranial bleeding in newly diagnosed atrial fibrillation. J Am Heart Assoc. (2020) 9:15689. doi: 10.1161/JAHA.120.015689
21. Christensen H, Bushnell C. Stroke in Women. Contin Lifelong Learn Neurol. (2020) 26:363–85. doi: 10.1212/CON.0000000000000836
22. Reeves MJ, Bushnell CD, Howard G, Gargano JW, Duncan PW, Lynch G, et al. Sex differences in stroke: epidemiology, clinical presentation, medical care, and outcomes. Lancet Neurol. (2008) 7:915–26. doi: 10.1016/S1474-4422(08)70193-5
23. Nanna MG, Wang TY, Xiang Q, Goldberg AC, Robinson JG, Roger VL, et al. Sex differences in the use of statins in community practice. Circ Cardiovasc Qual Outcomes. (2019) 12:62. doi: 10.1161/CIRCOUTCOMES.118.005562
24. Marzona I, Proietti M, Vannini T, Tettamanti M, Nobili A, Medaglia M, et al. Sex-related differences in prevalence, treatment and outcomes in patients with atrial fibrillation. Intern Emerg Med. (2020) 15:231–40. doi: 10.1007/s11739-019-02134-z
25. Dans AL, Connolly SJ, Wallentin L, Yang S, Nakamya J, Brueckmann M, et al. Concomitant use of antiplatelet therapy with dabigatran or warfarin in the randomized evaluation of long-term anticoagulation therapy (RE-LY) trial. Circulation. (2013) 127:634–40. doi: 10.1161/CIRCULATIONAHA.112.115386
26. Xu H, Ruff CT, Giugliano RP, Murphy SA, Nordio F, Patel I, et al. Concomitant use of single antiplatelet therapy with edoxaban or warfarin in patients with atrial fibrillation: analysis from the ENGAGE AF-TIMI48 Trial. J Am Heart Assoc. (2016) 5:87. doi: 10.1161/JAHA.115.002587
27. Nakagawa K, Vento MA, Seto TB, Koenig MA, Asai SM, Chang CWJ, et al. Sex differences in the use of early do-not-resuscitate orders after intracerebral hemorrhage. Stroke. (2013) 44:3229–31. doi: 10.1161/STROKEAHA.113.002814
28. Perman SM, Beaty BL, Daugherty SL, Havranek EP, Haukoos JS, Juarez-Colunga E, et al. Do Sex differences exist in the establishment of “do not attempt resuscitation” orders and survival in patients successfully resuscitated from in-hospital cardiac arrest? J Am Heart Assoc. (2020) 9:14200. doi: 10.1161/JAHA.119.014200
29. Zahuranec DB, Lisabeth LD, Gonzales NR, Longwell PJ, Smith MA, Garcia NM. Early care limitations independently predict mortality after intracerebral hemorrhage. Neurology. (2007) 68:1651–7. doi: 10.1212/01.wnl.0000261906.93238.72
30. Becker KJ, Baxter AB, Cohen WA, Bybee HM, Tirschwell DL, Newell DW, et al. Withdrawal of support in intracerebral hemorrhage may lead to self-fulfilling prophecies. Neurology. (2001) 56:766–72. doi: 10.1212/WNL.56.6.766
31. Fan J-S, Huang H-H, Chen Y-C, How C-K, Yen DH-T. Emergency department DNR order in patients with spontaneous intracerebral hemorrhage. Am J Emerg Med. (2017) 35:1850–4. doi: 10.1016/j.ajem.2017.06.016
32. Hiraoka E, Arai J, Kojima S, Norisue Y, Suzuki T, Homma Y, et al. Early DNR Order and Long-term prognosis among patients hospitalized for acute heart failure: single-center cohort study in Japan. Int J Gen Med. Volume. (2020) 13:721–8. doi: 10.2147/IJGM.S252651
33. Christensen H, Cordonnier C, Kõrv J, Lal A, Ovesen C, Purrucker JC, et al. European stroke organisation guideline on reversal of oral anticoagulants in acute intracerebral haemorrhage. Eur Stroke J. (2019) 4:294–306. doi: 10.1177/2396987319849763
34. Steiner T, Salman RA-S, Beer R, Christensen H, Cordonnier C, Csiba L, et al. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke. (2014) 9:840–55. doi: 10.1111/ijs.12309
Keywords: stroke, sex-differences, ICH, oral anticoagulation, vitamin K-antagonist, stroke in women, intracerebral hemorrhage (ICH), NOAC
Citation: Grundtvig J, Ovesen C, Steiner T, Carcel C, Gaist D, Christensen L, Marstrand J, Meden P, Rosenbaum S, Iversen HK, Kruuse C, Christensen T, Ægidius K, Havsteen I and Christensen H (2022) Sex-Differences in Oral Anticoagulant-Related Intracerebral Hemorrhage. Front. Neurol. 13:832903. doi: 10.3389/fneur.2022.832903
Received: 10 December 2021; Accepted: 31 January 2022;
Published: 03 March 2022.
Edited by:
Svetlana Lorenzano, Sapienza University of Rome, ItalyReviewed by:
Corina Epple, Klinikum Hanau GmbH, GermanyMarialuisa Zedde, IRCCS Local Health Authority of Reggio Emilia, Italy
Copyright © 2022 Grundtvig, Ovesen, Steiner, Carcel, Gaist, Christensen, Marstrand, Meden, Rosenbaum, Iversen, Kruuse, Christensen, Ægidius, Havsteen and Christensen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josefine Grundtvig, josefine.liv.gilling.grundtvig@regionh.dk; Hanne Christensen, Hanne.Krarup.Christensen@regionh.dk