
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Neurol. , 29 September 2020
Sec. Neuro-Otology
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.563373
 Vasilios M. Polymeropoulos*
Vasilios M. Polymeropoulos* Mark É. Czeisler
Mark É. Czeisler Mary M. Gibson†
Mary M. Gibson† Austin A. Anderson†
Austin A. Anderson† Jane Miglo
Jane Miglo Jingyuan Wang
Jingyuan Wang Changfu Xiao
Changfu Xiao Christos M. Polymeropoulos
Christos M. Polymeropoulos Gunther Birznieks
Gunther Birznieks Mihael H. Polymeropoulos
Mihael H. PolymeropoulosIntroduction: Novel therapies are needed for the treatment of motion sickness given the inadequate relief and bothersome and dangerous adverse effects of currently approved therapies. Neurokinin-1 (NK1) receptor antagonists have the potential to be effective in improving the symptoms of motion sickness, given the involvement of Substance P in nauseogenic and emetic pathways and the expression of NK1 receptors in the gastrointestinal system. Here we evaluated the efficacy of tradipitant, a novel NK1 receptor antagonist, in preventing motion sickness in variable sea conditions.
Methods: A total of 126 adults participated in the Motion Sifnos study. Groups of participants were assigned to one of seven boat trips lasting ~4 h on the Pacific Ocean. Participants were randomized 1:1 to tradipitant 170 mg or placebo and completed the Motion Sickness Severity Scale (MSSS) every 30 min, in addition to other assessments. Severity of motion sickness was assessed with the incidence of vomiting and the MSSS.
Results: Participants on tradipitant had a significantly lower incidence of vomiting as compared to those on placebo across all boat trips (tradipitant = 17.5%, placebo = 39.7%, p = 0.0039). For trips exposed to rough sea conditions, the difference in the incidence of vomiting between the groups was more dramatic (tradipitant = 15.79%, placebo = 72.22%, p = 0.0009). Across these trips, motion sickness symptoms were significantly lower in the tradipitant group compared to the placebo group (tradipitant = 3.19, placebo = 4.57, p = 0.0235).
Discussion: Tradipitant has the potential to be an effective therapy for the prevention of vomiting and treatment of nausea in people with motion sickness.
Motion sickness is a disorder that has been plaguing travelers in various vehicles since antiquity (1). Nausea and vomiting are the core symptoms of motion sickness (2). Other symptoms may include sweating, dizziness, headache, irritability, loss of appetite, and a cluster of symptoms described as sopite syndrome (yawning, drowsiness, and apathy) (3). The etiology and pathogenesis of disease are most commonly theorized as an aggregation of conflicting sensory information that leads to an unpleasant physiological reaction resulting in the symptoms described above (4, 5). The sensory mismatch resulting in motion sickness has been postulated to be due to discordance between actual and expected movement as perceived by the visual, vestibular, and kinesthetic systems (3). The mismatch can occur between two different systems or can be due to mismatch in intra-vestibular sensory inputs (a difference between semicircular canal and otoliths) (6). Travelers with motion sickness have impaired cognitive performance, which can be of increased burden and danger in professional environments (7). Although there is a significant demand for efficacious therapies, the only currently approved treatments in the United States are dimenhydrinate (Dramamine), hyoscine (Scopolamine), and meclizine (Dramamine non-drowsy). These therapies carry incomplete efficacy and can have bothersome and dangerous adverse effects, such as drowsiness and dizziness (8). Specifically, the adverse effects of hyoscine include dry mouth, dizziness, somnolence, visual impairment, agitation, confusion, and mydriasis (9). Dimenhydrinate was found to significantly inhibit psychomotor performance when used as a therapy for motion sickness in naval crews, impairing decision reaction time and auditory digit span (10). Meclizine can induce drowsiness and has been found to negatively impact short-term memory (11). An ideal therapy would be efficacious in the treatment of the cardinal symptoms of nausea and vomiting without inducing the array of adverse effects as seen with current medications.
NK1 receptor antagonists have the potential to be effective in the treatment of motion sickness in humans. Centrally, NK1 receptors are expressed in the network of brainstem nuclei including the area postrema and nucleus tractus solitarius (NTS) that are involved in the regulation of vomiting (12). Transmission of emetogenic sensory and emotional signals from higher cortical centers to the NTS can result in reflexive vomiting. The vestibular centers in the brainstem send signals to the NTS to trigger emesis in response to vertigo, dizziness, or visuospatial disorientation (13). When the NTS receives the direct input from those sources, Substance P (SP), the most abundant neurokinin, is released (14). Substance P preferentially binds to the NK1 receptors densely located in the NTS, which triggers this cascade of physiological responses, including emesis (13). Peripherally, NK1 receptors are expressed in the neurons projecting to the antrum of the stomach, in enteric neurons, in the smooth muscle of the small intestine, and within the wall of the submucosal blood vessels (15, 16). Given this distribution within the central, peripheral, and enteric nervous systems, as well as within peripheral tissues, NK1 receptor-induced nausea and emesis may be mediated by a combination of all of these physiologic systems.
NK1 receptor antagonists are effective and approved for the treatment of nausea and vomiting in other indications. Maropitant is an approved NK1 receptor antagonist shown to be effective for the prevention of vomiting in dogs and cats due to motion sickness (17). The NK1 receptor antagonist aprepitant is approved for the prevention of post-operative nausea and vomiting (18).
Tradipitant (VLY-686) is a novel NK1 receptor antagonist in development for the treatment of gastroparesis and atopic dermatitis. Tradipitant was shown to be effective in the treatment of nausea and vomiting in gastroparesis in a 4-week randomized study (19). Given this evidence to support the use of tradipitant as an NK1 receptor antagonist to treat nausea and vomiting and specifically in motion sickness, we designed and conducted the Motion Sifnos study.
Regarding the election of modality to induce motion sickness, we conducted the study in natural sea conditions in the Pacific Ocean for several reasons: (1) seasickness is the classical archetype to induce motion sickness; (2) exposure to natural sea motion supports the study conditions as ecologically valid; and (3) simulation in real-world conditions offers the unique opportunity to evaluate the medication as it would be used once available to the public. Further, sea travel consists of vertical sinusoidal motions induced by waves. The amplitude of these motions is related to the wave height and corresponds to heave (linear vertical motion), which is the strongest stimulus to induce motion sickness in sea travel, contributing more to provocation than the angular accelerations of pitch, roll, and yaw (20). The frequency and acceleration of vertical sinusoidal motions can also be assessed. In an evaluation of motion sickness incidence as a function of the frequency and acceleration of vertical sinusoidal motion, wave frequencies around 0.2 Hz were most provocative, and motion sickness incidence increased with acceleration (proportional to the amplitude of the waves) across all wave frequencies (21). The goal of the Motion Sifnos study was to examine the effects of tradipitant in treating the symptoms of motion sickness, with a focus on the core symptoms.
The Motion Sifnos study (NCT03772340) was a randomized, double-blind placebo-controlled study on the Pacific Ocean near Los Angeles, California, to evaluate the efficacy and safety of tradipitant in the treatment of motion sickness.
Eligible participants were adults aged between 18 and 75 years with a history of motion sickness, otherwise in good health (determined by medical and psychiatric history, physical examination, electrocardiography, serum chemistry, hematology, urinalysis, and urine toxicology), and lacking any major nausea-inducing disorders. All participants provided written informed consent. Ethical oversight of the study procedures was conducted by the Institutional Review Board at Advarra. The majority of participants had described sea travel to most severely exacerbate their symptoms of motion sickness. Recruitment of participants was accomplished through advertisements, participant databases, and pre-screening interviews conducted online or by phone script.
Using a Motion Sickness Eligibility Questionnaire (MSEQ), 1,270 people opted in online or by phone declaring interest for participation in the study. Participants eligible based on the MSEQ criteria were contacted to provide more information for the study and interviewed about their symptoms of motion sickness to determine eligibility. A total of 150 people were screened for eligibility, and 126 eligible people who met screening criteria were randomized and took part in the travel assessment (Figure 1). Groups ranging from 10 to 26 participants took part in a single boat trip travel assessment, among the seven that occurred in total from January to May 2019. Groups were organized based on time and scheduling availability of participants, site staff, nautical professionals, and weather conditions.
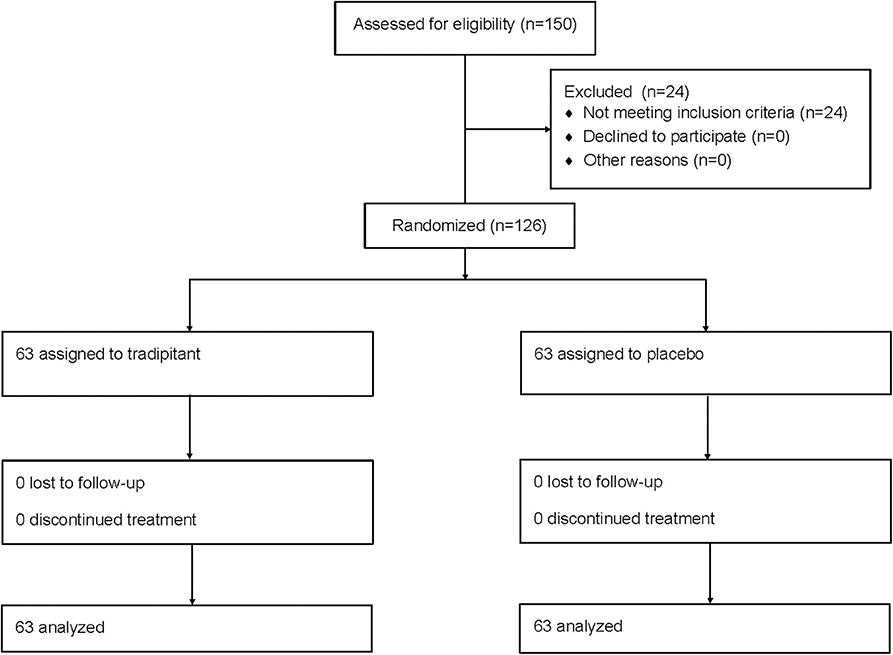
Figure 1. Participant flow diagram. The flow diagram illustrates how participants entered and completed the Motion Sifnos study.
At Visit 1 (V1), participants were screened with medical history, physical exam, electrocardiogram, and laboratory tests. Critical screening criteria included a reported history of motion sickness and lacking a history of another chronic nausea inducing disorder such as irritable bowel syndrome, gastroparesis, or cyclic vomiting syndrome. Collection of adverse event information began at the time the informed consent form was signed and continued through the end of the study. Upon arrival on the day of the boat trip (Visit 2–V2), participants were randomly assigned (1:1 ratio) through an Interactive Web Response System and administered either two oral capsules totaling tradipitant 170 mg or two oral capsules of placebo identical in appearance ~60 min prior to initiation of the travel assessment on the boat.
Participants engaged in a travel assessment during which they spent 237–250 min on the boat in the Pacific Ocean, except where severe weather conditions limited one boat trip (Boat 5) to 148 min. The monohull boats were about 100 feet in length with indoor seating cabins and visibility to the outside. Each boat was temperature-controlled and chartered by a full staff of nautical professionals. Trips occurred on a different day under variable sea conditions. Duration of travel, route, average wave height, wave period, wind speed, and wind direction were recorded. The study was designed to have participants on the boat in the sea to expose them to realistic conditions to elicit symptoms of motion sickness. The stimulus was variable based on different movements induced by natural sea conditions.
On the boat, participants were instructed to remain in assigned seats and were seated with no one sitting directly adjacent to them. Participants had access to snacks including water, juice, and crackers, and could access restrooms. Every 30 min from the initiation of the trip participants were instructed to fill out the Motion Sickness Severity Scale (MSSS) to assess their symptoms of motion sickness. The MSSS is a 7-point scale scored 0–6 based on participant selection of symptom severity from the following choices: no symptoms, stomach awareness or discomfort, mild nausea, moderate nausea, severe nausea, retching, vomiting (Figure 2) (22). The MSSS reflects the severity of the core symptoms of motion sickness as experienced and reported by the participant.
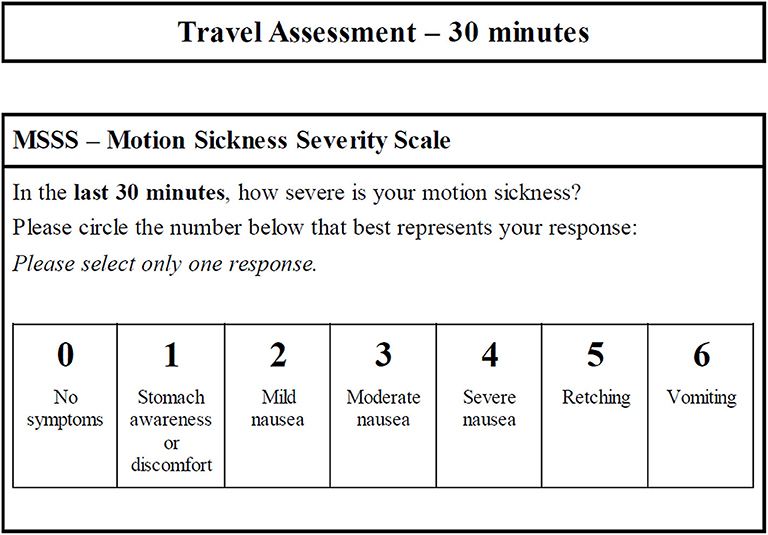
Figure 2. Motion Sickness Severity Scale (MSSS). The questionnaire is utilized for clarity and rapid completion (especially for participants experiencing nausea or vomiting) to facilitate repeated use over the duration of boat travel. In the event a participant vomited and felt too ill to proceed, there was an option to complete the end of study questionnaires early and move to a different area on the boat to relax and alleviate their symptoms. A synopsis of the procedure is outlined in this figure.
At the conclusion of travel, participants completed several questionnaires including the Motion Sickness Assessment Questionnaire (MSAQ) and the Patient Global Impression Scale—Subjective (PGI-S) for motion sickness (Figure 3) (23, 24). The MSAQ is a 16-item questionnaire ranging from 0 to 9 that was developed to create a validated questionnaire for motion sickness that encompasses all symptoms of motion sickness subdivided by body system, though not all of these symptoms are shared by all people (2, 23). The PGI-S for motion sickness is a 5-item scale rated 0–4 where subjects indicate their severity of motion sickness ranging from none to very severe.
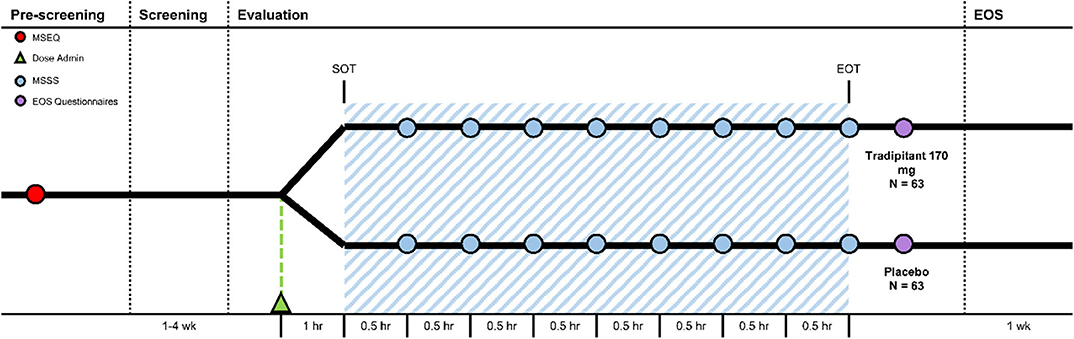
Figure 3. Motion Sifnos Study design. The Motion Sickness Eligibility Questionnaire (MSEQ, red circle) was used to pre-screen prospective participants for self-reported histories of motion sickness. Approximately 60 min prior to the start of travel (SOT), participants were randomized (Dose Administration, green triangle). The blue shaded area represents boat travel. The MSSS was administered every 30 min (MSSS, blue circle). Approximately 30–60 min after the end of travel (EOT), participants were instructed to complete the end of study questionnaires (EOS Questionnaires, purple circle).
There were two primary assessments for the study: the incidence (percentage of participants) of vomiting (indicated by a score of 6 on the MSSS or by election to complete the end of study questionnaires early due to sickness severity) and the severity of motion sickness (as measured by the highest score indicated on the MSSS) during the trip. The incidence of vomiting was analyzed by a Cochran-Mantel-Haenszel (CMH) test adjusting for the trip. The most severe motion sickness severity was analyzed using an analysis of variance (ANOVA) with the main effect of treatment and boat trip. The MSAQ and PGI-S were analyzed using an ANOVA in the same manner as MSSS worst score. A sample size of up to 75 participants per arm (150 total) provided around 86% power to detect a 0.8-point difference in MSSS scores between tradipitant and placebo, with the standard deviation of motion sickness severity assumed to be around 1.6 points on the MSSS. The original sample size estimation was determined based on the endpoint of MSSS. However, to the advice of the regulatory agency, the primary endpoint was changed to rate of vomiting. As such, we re-estimated the sample size and determined that the study was properly powered with a smaller sample. As compared to the original sample size, the sample size was 126, to compare a difference of 30%, and providing a power of around 93%.
Additional analyses were conducted to evaluate the treatment effect under different sea conditions given the established interaction between sea conditions and motion sickness incidence (20). For the analyses, boat trips exposed to wave heights >1.2 m, corresponding to a Beaufort scale of 4, were considered the “Rough Sea Conditions” subgroup, and trips exposed to wave heights ≤1.2 m were considered the “Calm Sea Conditions” subgroup.
Statistical significance was evaluated using an a priori significance level set to α = 0.05. To quantify the efficacy of tradipitant in reducing vomiting incidence in rough sea conditions, the relative risk reduction (RRR) was calculated. In this context the RRR is the relative decrease in the risk of vomiting in the tradipitant group compared to the placebo group.
All randomized participants completed the study. Baseline demographic characteristics for the study population are reported in Table 1. Participants were of a diverse age, ethnicity, and physical characteristics representative of the US population. Females made up 77% of the study population, as anticipated given epidemiological data (25). There was an average of 18 participants per boat trip. Summary statistics for the boat trip are reported in Table 2. Across trips, the frequency of vertical sinusoidal oscillation as derived from wave period was between 0.09 and 0.20 Hz. The average wave height across trips was 0.99 m (standard deviation [sd] = 0.38) and the average wind speed was 11.48 knots (sd = 6.91).
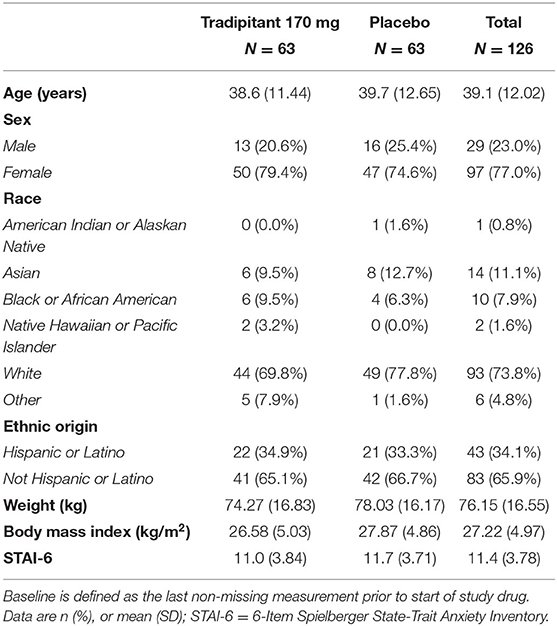
Table 1. Baseline characteristics for the Motion Sifnos Study population.
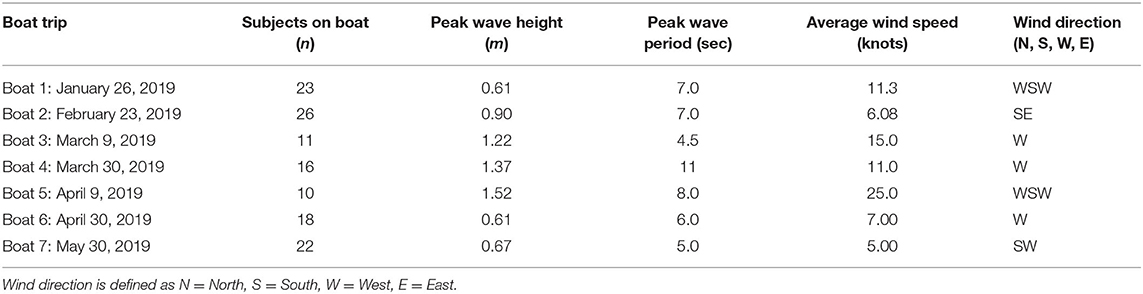
Table 2. Summary of boat trip conditions.
A summary of assessments for the intent-to-treat (ITT) population is reported in Table 3. The incidence of vomiting in the tradipitant group was significantly higher than the placebo group across boat trips (Figure 4). In boats exposed to rough sea conditions the magnitude of difference in the incidence of vomiting was greater between groups (tradipitant = 15.8%, placebo = 72.2%, p = 0.0009, n = 37). In these boat trips with higher waves and worse sea conditions, participants taking tradipitant reduced their risk of vomiting by 78% compared to participants taking placebo (RRR = 78%, n = 37).
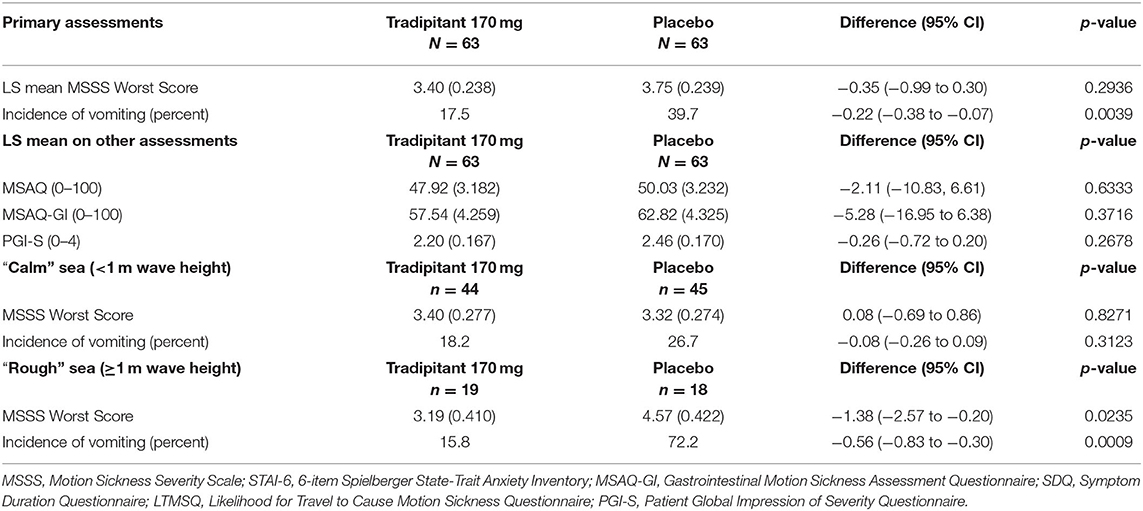
Table 3. Summary of endpoints: motion sickness symptom assessments for the ITT population.
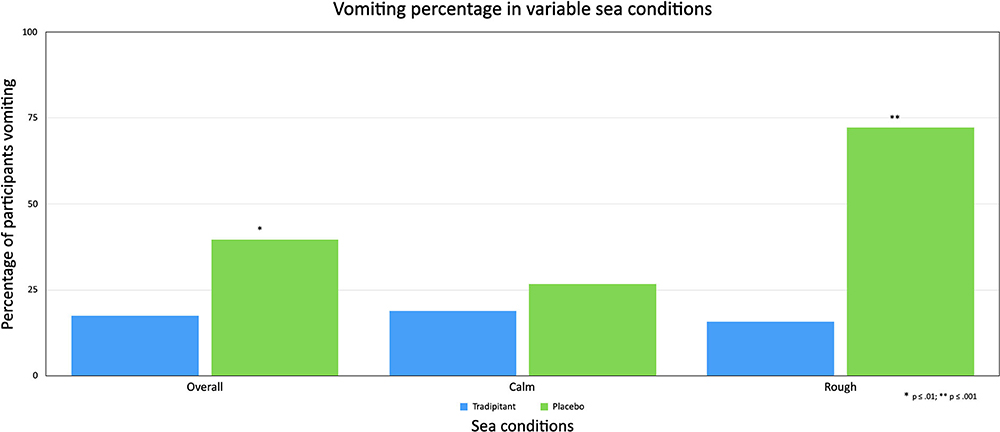
Figure 4. Vomiting percentage in variable sea conditions. The figure reflects the percentage of participants vomiting (incidence of vomiting) across different sea conditions. A participant was considered as having vomited if they ever marked a score of 6 (vomiting) on the MSSS or vomited and elected to complete end of travel questionnaires before the end of travel.
In a comparison of the placebo subgroups in rough vs. calm sea conditions, the incidence of vomiting in participants taking placebo increased significantly in rough sea conditions (difference = 45.55%, p = 0.0014 [Fisher's exact test]), as did motion sickness severity as measured by the MSSS worst score (difference = 1.17, p = 0.0465). In contrast, the incidence of vomiting in participants taking tradipitant remained similar in boat trips in rough and calm sea conditions (rough = 15.79%, calm = 18.18%, difference = 2.39%, p = 1.0 [Fisher's exact test]) and the magnitude of symptoms (difference = 0.32, p = 0.4519) did not differ significantly.
Across all boat trips, participants on tradipitant rated their most severe motion sickness as lower compared to those on placebo, though this difference was not statistically significant (LS mean MSSS: tradipitant = 3.40, placebo = 3.75, p = 0.2936, n = 126). In rough sea conditions, tradipitant participants' most severe motion sickness symptoms were significantly improved as compared to the placebo group (LS mean MSSS: tradipitant = 3.19, placebo = 4.57, p = 0.0235, n = 37). In calm sea conditions, participants in both groups rated their symptoms as similar (LS mean MSSS: tradipitant = 3.40, placebo = 3.32, p = 0.8271, n = 89).
In an analysis of all boat trips, assessments of MSAQ and PGI-S between treatment groups were not significantly different. When examining these assessments in boat trips in rough sea conditions, the difference between groups for the following assessments all favored the tradipitant group though were not statistically significant: MSAQ (tradipitant = 49.9, placebo = 59.0, p = 0.2915), MSAQ-GI (tradipitant = 60.3, placebo = 76.4, p = 0.1468), PGI-S (tradipitant = 2.29, placebo = 3.00, p = 0.1372). There was no significant difference in the rate of vomiting when examined by gender for participants taking tradipitant (females = 18.00%, males = 15.38%, p = 1.00) or placebo (females = 40.43%, males = 37.50%, p = 1.00). There was no significant difference in the rate of vomiting when examined by age for participants taking tradipitant (age<40 = 18.40%, age≥40 = 16.00%, p = 1.00) or placebo (age<40 = 34.29%, age≥40 = 46.43%, p = 0.4438).
Tradipitant 170 mg was well-tolerated during the study. Tradipitant participants reported somnolence and headache more frequently than participants in the placebo group (somnolence: tradipitant = 27%, placebo = 12.7%; headache: tradipitant = 12.7%, placebo = 7.9%). No serious adverse events were reported during study participation.
The Motion Sifnos Study demonstrated the effects of tradipitant in the improvement of the core symptoms of motion sickness, particularly robust in rough seas. In our analyses, the consideration of the effect of variable sea conditions was important. Heave and oscillatory frequency have been established as primary stimuli of motion sickness during sea travel, with the angular acceleration of pitch, roll, and yaw contributing to a lesser degree (20). The wave frequency of all trips was in the range of the most provocative vertical sinusoidal oscillatatory frequencies, which is typically around 0.2 Hz (21). Although heave motion and acceleration of vertical sinusoidal oscillation were not directly recorded, increased wave height (which likely correlates with increased vertical displacement) was associated with increased motion sickness severity. Participants in the placebo group experienced a significantly higher incidence of vomiting and worsening of symptoms under these highly provocative conditions with increasing wave heights, consistent with the literature (26). Without an adequate stimulus (higher waves) and subsequent development of motion sickness symptoms in travelers, it would be difficult to demonstrate an improvement with tradipitant as compared to placebo without significant production of symptoms to alleviate. Notably, the incidence of vomiting and magnitude of symptoms remained similarly low in tradipitant participants across sea conditions.
The election of motion sickness questionnaires for the assessment of nausea and vomiting needed to meet three critical criteria: (1) can be conducted quickly during travel and while feeling ill; (2) captures the cardinal elements and commonly shared symptoms of motion sickness; and (3) is validated through the use in other studies. The MSSS is a validated questionnaire previously used in the pivotal study of scopolamine in the treatment of motion sickness in sea travel (22). A similar scale titled the Motion Sickness Rating Scale (MSRS) has been used in the study of motion sickness which is a numerical rating scale focusing on the symptoms of stomach awareness, nausea, and vomiting (27). Future studies for tradipitant could examine the symptoms of nausea and vomiting separately, provided they are easy to complete for the participant. The MSAQ was employed following travel to assess the constellation of symptoms a person may experience with motion sickness. A limitation of the MSAQ in this study is that although nausea and vomiting are widely shared symptoms among people experiencing motion sickness, the host of other symptoms that may be experienced are variable between people. Ideally if motion sickness stimulus and conditions could be identically replicated, a study could be conducted that establishes a baseline level of illness with questionnaires such as the MSSS and MSAQ, to understand the magnitude of an individual's improvement of their unique experience with motion sickness with tradipitant.
In this study, by studying various sea conditions, we also demonstrate and validate a model for studying motion sickness effectively using wave height as a core component of the model. The findings suggest that rough sea conditions as indicated by wave height have a direct effect on the utility of sea travel as a model for studying motion sickness.
Overall, limited adverse effects were reported. Participants on tradipitant reported a low rate of adverse effects, generally reported as mild in nature. This stands in contrast to other approved therapeutics including dimenhydrinate and hyoscine that carry significant and hazardous adverse effects, that may include cognitive impairment, confusion, and visual impairment.
The presumed mechanism of tradipitant would be to treat the core symptoms of motion sickness by acting at the level of the NK1 receptors in the brainstem to prevent vomiting and at the NK1 receptors in the gut influencing nauseogenic pathways and gastric motility. Mitigation of these symptoms as assessed by the MSSS supports the efficacy of tradipitant in improving these symptoms.
Tradipitant if available could be of immediate utility to civilian travelers and for both professional and military use. This study demonstrated the potent anti-emetic effect of tradipitant that may be of significant benefit to the general public and in at-risk occupational settings including astronauts who suffer from severe motion sickness in the first few days of travel, especially given that vomiting in the space suit can pose a significant hazard (28). In other professional environments including on sea and in the air, tradipitant may be a useful primary or adjunct therapy given its demonstrated efficacy and mild adverse effect profile compared to currently available pharmacological therapies.
All datasets generated for this study are included in the article/supplementary material.
The studies involving human participants were reviewed and approved by Advarra IRB. The patients/participants provided their written informed consent to participate in this study.
VP, GB, CP, CX, and MP contributed to the study concept and design. JW, CP, CX, VP, and MP developed the statistical analysis plan. VP wrote the report in collaboration with MC, MG, AA, JM, and CP revised the report with participation from all authors. All authors reviewed and approved the report before submission.
All research was funded by Vanda Pharmaceuticals.
All authors were employed by Vanda Pharmaceuticals.
We thank the participants of the study for their commitment to help us in find a new treatment for motion sickness. We thank Dr. Daniel Norman MD and the site study staff. We thank the nautical staff involved in the boat travel assessment. We thank Dr. Behrang Keshavarz PhD for his guidance. We thank our colleagues at Vanda Pharmaceuticals for their support in conducting the study including Suzanne Quebbeman, Xian Cui, Patrick Collins, Pan Wang, Grace Li, Zibo Wang, and Katerina Polymeropoulos. This article was released as a pre-print at medrxiv.org (Polymeropoulos et al.). This work was sponsored by Vanda Pharmaceuticals.
1. Huppert D, Benson J, Brandt T. A historical view of motion sickness-a plague at sea and on land, also with military impact. Front Neurol. (2017) 8:114. doi: 10.3389/fneur.2017.00114
2. Golding JF. Motion sickness. In: Furman JM, Lempert T, editors. Handbook of Clinical Neurology. Amsterdam, Boston, Heidelberg, London, New York, Oxford, Paris, San Diego, San Francisco, Singapore, Sydney. Tokyo: Elsevier. (2016). p. 371–90.
3. Graybiel A, Knepton J. Sopite syndrome: a sometimes sole manifestation of motion sickness. Aviat Space Envrion Med. (1976) 47:873–82.
4. Reason JT. Motion sickness adaptation: a neural mismatch model. J R Soc Med. (1978) 71:819–29. doi: 10.1177/014107687807101109
5. Stott JRR. Mechanisms and treatment of motion illness. In: Davis CJ, Lake-Bakaar GV, Grahame-Smith DG, editors. Nausea and Vomiting: Mechanisms and Treatment. Advances in Applied Neurological Sciences. Berlin, Heidelberg: Springer. (1986). p. 110–29.
6. Reason J. Motion sickness: Some theoretical and practical considerations. Appl Ergon. (1978) 9:163–7. doi: 10.1016/0003-6870(78)90008-X
7. Matsangas P, McCauley ME, Becker W. The effect of mild motion sickness and sopite syndrome on multitasking cognitive performance. Hum Factors. (2014) 56:1124–35. doi: 10.1177/0018720814522484
8. Brainard A, Gresham C. Prevention and treatment of motion sickness. Am Fam Phys. (2014) 90:41–46.
10. Gordon CR, Gonen A, Nachum Z, Doweck I, Spitzer O, Shupak A. The effects of dimenhydrinate, cinnarizine and transdermal scopolamine on performance. J Psychopharmacol. (2001) 15:167–72. doi: 10.1177/026988110101500311
11. Weerts AP, Pattyn N, Van de Heyning PH, Wuyts FL. Evaluation of the effects of anti-motion sickness drugs on subjective sleepiness and cognitive performance of healthy males. J Psychopharmacol. (2014) 28:655–64. doi: 10.1177/0269881113516201
12. Saito R, Takano Y, Kamiya HO. Roles of substance P and NK(1) receptor in the brainstem in the development of emesis. J Pharmacol Sci. (2003) 91:87–94. doi: 10.1254/jphs.91.87
13. Stahl SM. The ups and downs of novel antiemetic drugs, part 1: substance P, 5-HT, and the neuropharmacology of vomiting. J Clin Psychiatry. (2003) 64:498–99. doi: 10.4088/JCP.v64n0501
14. Otsuka M, Yoshioka K. Neurotransmitter functions of mammalian tachykinins. Physiol Rev. (1993) 73:229–308. doi: 10.1152/physrev.1993.73.2.229
15. Smith VC, Sagot MA, Wong H, Buchan AM. Cellular expression of the neurokinin 1 receptor in the human antrum. J Auton Nerv Syst. (2000) 79:165–72. doi: 10.1016/S0165-1838(99)00092-2
16. Renzi D, Pellegrini B, Tonelli F, Surrenti C, Calabrò A. Substance P (neurokinin-1) and neurokinin A (neurokinin-2) receptor gene and protein expression in the healthy and inflamed human intestine. Am J Pathol. (2000) 157:1511–22. doi: 10.1016/S0002-9440(10)64789-X
17. Conder GA, Sedlacek HS, Boucher JF, Clemence RG. Efficacy and safety of maropitant, a selective neurokinin 1 receptor antagonist, in two randomized clinical trials for prevention of vomiting due to motion sickness in dogs. J Vet Pharmacy Ther. (2008) 31:528–32. doi: 10.1111/j.1365-2885.2008.00990.x
18. Diemunsch P, Joshi GP, Brichant JF. Neurokinin-1 receptor antagonists in the prevention of postoperative nausea and vomiting. Br J Anaesth. (2009) 103:7–13. doi: 10.1093/bja/aep125
19. Carlin JL, Lieberman VR, Dahal A, Keefe MS, Xiao C, Birznieks G, et al. Efficacy and safety of tradipitant in patients with diabetic and idiopathic gastroparesis in a randomized, placebo-controlled trial. Gastroenterology. (2020). doi: 10.1053/j.gastro.2020.07.029. [Epub ahead of print].
20. Lawther A, Griffin MJ. Prediction of the incidence of motion sickness from the magnitude, frequency, and duration of vertical oscillation. J Acoust Soc Am. (1987) 82:957–66. doi: 10.1121/1.395295
21. O'Hanlon JF, McCauley ME. Motion sickness incidence as a function of the frequency and acceleration of vertical sinusoidal motion. Aerosp Med. (1974) 45:366–9. doi: 10.21236/AD0768215
22. Price NM, Schmitt LG, McGuire J, Shaw JE, Trobough G. Transdermal scopolamine in the prevention of motion sickness at sea. Clin Pharmacol Ther. (1981) 29:414–19. doi: 10.1038/clpt.1981.57
23. Gianaros PJ, Muth ER, Mordkoff JT, Levine ME, Stern RM. A questionnaire for the assessment of the multiple dimensions of motion sickness. Aviat Space Environ Med. (2001) 72:115–19.
24. Yalcin I, Bump RC. Validation of two global impression questionnaires for incontinence. Am J Obstet Gynecol. (2003) 189:98–101. doi: 10.1067/mob.2003.379
25. Klosterhalfen S, Kellermann S, Pan F, Stockhorst U, Hall G, Enck P. Effects of ethnicity and gender on motion sickness susceptibility. Aviat Space Environ Med. (2005) 76:1051–7.
26. Alexander SJ, Cotzin M. Studies of motion sickness; the effects upon sickness rates of waves of various frequencies but identical acceleration. J Exp Psychol. (1947) 37:440–48. doi: 10.1037/h0063240
27. Golding JF, Paillard AC, Normand H, Besnard S, Denise P. Prevalence, predictors, and prevention of motion sickness in zero-G parabolic flights. Aerosp Med Hum Perform. (2017) 88:3–9. doi: 10.3357/AMHP.4705.2017
Keywords: motion sickness, tradipitant, neurokinin-1, seasickness, seasickness prevention
Citation: Polymeropoulos VM, Czeisler MÉ, Gibson MM, Anderson AA, Miglo J, Wang J, Xiao C, Polymeropoulos CM, Birznieks G and Polymeropoulos MH (2020) Tradipitant in the Treatment of Motion Sickness: A Randomized, Double-Blind, Placebo-Controlled Study. Front. Neurol. 11:563373. doi: 10.3389/fneur.2020.563373
Received: 27 May 2020; Accepted: 20 August 2020;
Published: 29 September 2020.
Edited by:
Carey David Balaban, University of Pittsburgh, United StatesReviewed by:
Michael C. Schubert, Johns Hopkins University, United StatesCopyright © 2020 Polymeropoulos, Czeisler, Gibson, Anderson, Miglo, Wang, Xiao, Polymeropoulos, Birznieks and Polymeropoulos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vasilios M. Polymeropoulos, dmFzaWxpb3MucG9seW1lcm9wb3Vsb3NAdmFuZGFwaGFybWEuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.