 Bassam Eid1,2†
Bassam Eid1,2† Mary Bou Saleh3†
Mary Bou Saleh3† Imad Melki1,2Paul-Henry Torbey1,2Joelle Najem3Maroun Saber3
Imad Melki1,2Paul-Henry Torbey1,2Joelle Najem3Maroun Saber3 Nada El Osta4,5
Nada El Osta4,5 Lydia Rabbaa Khabbaz3*
Lydia Rabbaa Khabbaz3*- 1Faculty of Medicine, Saint-Joseph University of Beirut, Beirut, Lebanon
- 2Department of Pediatrics, Hôtel-Dieu de France Hospital, Saint-Joseph University of Beirut, Beirut, Lebanon
- 3Laboratoire de Pharmacologie, Pharmacie clinique et Contrôle de qualite des medicaments, Faculty of Pharmacy, Saint-Joseph University of Beirut, Beirut, Lebanon
- 4Craniofacial Research Laboratory, Oral Health Unit, Faculty of Dental Medicine, Saint-Joseph University, Beirut, Lebanon
- 5Department of Prosthodontics, Faculty of Dental Medicine, Saint-Joseph University, Beirut, Lebanon
Objectives: To evaluate possible associations between chronotype, weight, sleep problems, anxiety, and depression among children from 6 to 12 years of age.
Method: One-hundred children aged between 6 and 12 years were randomly recruited in five pediatrician clinics in the capital city of Beirut, Lebanon. The protocol was approved by the ethics committee of Saint-Joseph University and Hotel-Dieu Hospital and an informed written formal consent was obtained from one of the parents. The Sleep Disturbance Scale for Children (CCTQ), the Revised Child Anxiety and Depression Scale (RCADS)-Parent version, and the Children's Chronotype Questionnaire (CCTQ) were used.
Results: The majority of the sample (47%) presented an intermediate chronotype. There was a shift toward evening chronotype with increased age and a significant association between electronic devices use and an evening chronotype. Higher sleep disturbances were also observed among children with an evening chronotype. In particular, disorders of initiating and maintaining sleep, non-restorative sleep, excessive somnolence, and total SDSC were significantly higher among evening type children in our study. Finally, major depression domain scores were significantly higher among children with an evening chronotype.
Conclusions: Several findings of this study are important and explain factors associated to chronotype in children. Two important future perspectives can be highlighted: limiting electronic devices use among children in an effort to reduce circadian rhythm disturbances and identifying and treating sleep problems associated with eveningness, taking into account the possible presence of major depression among this population.
Introduction
Humans show cyclic rhythmicity in a wide range of psychological, cognitive, and physiological behaviors as well as in hormonal variations. This natural rhythmicity is called the circadian rhythm and it affects several processes such as sleep-wake cycles, mood, hormone levels, cognition, and temperature. The trait determining individual circadian preference in rhythm is known as chronotype, which is relative to cycles of external light and dark (1–5). Chronotypes are divided into three main categories: morning, intermediate, and evening.
Young children (2–6 years of age) seem to show a relatively strong preference for morningness (6–8) but transition toward eveningness begins in early childhood (9) and this shift is significantly more marked in adolescence (10) when a delay in the timing of sleep tends to be seen (11). At the end of the adolescence, a change toward morningness occurs (12). Studies among adolescents and adults have shown that eveningness was significantly associated with obesity when it is compared to morningness (13, 14) and evening chronotype was associated with changes in eating behavior (14–16) such as poor dietary control, high total calories and cholesterol intakes, consumption of a larger portion, late-night food intake, and a tendency to omit breakfast among adults (17, 18). Studies of the links between chronotype and weight among children are very scarce. Only one study was conducted among children with ADHD and revealed that evening preference plays a role in a mechanism linking ADHD to obesity (19). In addition to its possible association with weight, circadian preference was strongly linked with sleep quality in adults (20, 21) and eveningness was related to more sleeping difficulties and in particular to insomnia (22). In pre-school children (aged 4.5 years old), those with an evening chronotype seem to present more sleep difficulties than morning types as reported by parents, and consequently, more negative social consequences (23). Sleep problems were also found to be concurrent with anxiety, depression, conduct problems, and hyperactivity in both children (24, 25) and adolescents (26, 27).
Existing evidence suggests that sleep dysfunction during childhood could be an early manifestation of future adjustment problems (28, 29). Thus, sleep may be used as an early marker of psychopathology developing later and it may enable specialists to identify individuals at risk before the development of more serious symptoms (30). Indeed, among preschool children, sleep problems predicted depression and anxiety at 9–13 years (29). Furthermore, eveningness and sleep difficulties during childhood have been linked to worse academic performance later on, both at school and in university (31) and to adjustment difficulties, defined as internalizing and externalizing problems (32).
Even though several studies examined sleep among children, few of them focused on chronotype, and those were mainly conducted among adolescents. Eveningness has been previously linked to anxiety, depression, and general affective problems among adolescents (33–35) but no such data are available for children.
The period just before adolescence can be critical in determining future sleep pattern and psychological problems and very little is known on the associations between sleep, circadian preference, anxiety, and depression in children during this period. Thus, the primary objective of this study was to investigate the links between the chronotype, weight, sleep problems, anxiety, and depression among children aged between 6 and 12 years.
Materials and Methods
Study Design and Population
The study was conducted between March and December 2018. First, five pediatrician clinics were randomly selected from a list of clinics based in Beirut. and randomly recruited in five pediatrician clinics in the capital city of Beirut, Lebanon. Inclusion was done during vaccination visit (before the administration of the vaccine) to make sure that the child is not sick at the time of the inclusion. Briefly, a list of appointments was provided on Monday morning (and for the coming week) by the staff, highlighting vaccination visits. From this list, selection was randomly performed. The exclusion criteria were: children taking any medication, children with any chronic diseases. A trained research assistant interviewed the parents in the waiting room. One-hundred and fifty parent's children were approached, of whom 28 refused to participate in the study, and 22 children presented at least one exclusion criteria. The final study sample consisted of 100 children aged between 6 and 12 years. In addition to filling the questionnaires listed below, socio-demographic information was recorded. Physical activity and electronic devices use were also collected. For physical activity, since the number of participants with no activity (n = 3) was small, the two categories of physical activity (no activity and 1 h/week) were combined. The categories were 0–1 h/week, 2 h/week, and ≥3 h/week. For electronic devices use, four categories were used: 0, 1, 2, and ≥3 h/week.
Sleep Disturbances
The Sleep Disturbance Scale for Children (SDSC) consists of 26 questions evaluating sleep problems during the 6 previous months. SDSC uses a five-point scale and a total sleep time of 1 (9–11 h) to 5 (<5 h) and for sleep latency of 1 (<15 min) to 5 (>60 min). The frequency of the symptoms of sleep disorder is measured on a likers scale of five-point: never (1); occasionally, meaning once or twice per month (2); sometimes, meaning once, or twice per week (3); often, meaning 3–5 times per week (4) and always, meaning six or seven times per week (5). Furthermore, in children, SDSC identifies six types of symptoms of sleep disorders: early and late sleep disorders (sleep latency, sleep duration, nocturnal awakenings, and sleep anxiety), sleep breathing disorders (snoring, breathing) disturbances of arousal (such as sleepwalking, nightmares, and night terrors), disorders of sleep-wake transition (rhythmic movements, hypnotic saccades, and bruxism), disorders of excessive sleepiness (difficulty to wake up, tiredness in the morning, and inappropriate nap) and sleep hyperhidrosis (or night sweating). Calculation of a total score and a score for each symptom is performed for each child. A higher score indicates higher risk of developing sleep disorders (36, 37). The Chronbach alpha of the questionnaire was 0.661.
Chronotype
The Children's Chronotype Questionnaire (CCTQ) (38) was developed based upon the previous work of Roenneberg et al. (39–41) and Carskadon et al. (42, 43).
The CCTQ is a 27-item, mixed format. Parents can respond to several open-ended questions concerning sleep/wake parameters for scheduled days (non-holidays) and holidays (free days). It has 27 items and a five-point chronotype (CT) score (44). It contains: 16 questions about sleep and wake parameters (e.g., lights-off time, bedtime, sleep latency, rising time, wake-up time, fully alert time, and regular naps) for scheduled and free days; In addition, there is a 10-item morningness/eveningness scale (range of 10–48); and one item number 27 named “chronotype (CT)” (range of 1–5). This is a single-item measure. Parents read a short description of different chronotypes and selected one of five categories that best represents their child's circadian phase preference (i.e., definitely a morning type, rather a morning type than an evening type, neither/nor type, rather an evening type than a morning type, or definitely an evening type).
The total score from the MES [morningness/eveningness (M/E) scale] is a sum of scores of items 17–26 only, and ranges from 10 to 48 (38). This score is used to classify individuals as: morning type, intermediate type, and evening type (scores of ≤ 23, 24–32, and ≥33, respectively) (2). The questionnaire yielded a Cronbach alpha of 0.619.
RCADS-P
The Revised Child Anxiety and Depression Scale (RCADS)-Parent version is a self-assessment scale developed to identify and screen for the clinical symptoms of anxiety and depression in children or adolescents and is filled by the parents. This questionnaire includes 47 questions grouped into six subscales: Separation Anxiety Disorder, Anxiety Disorder (General Anxiety Disorder), Social Phobia, Panic Disorder, Major Depressive Disorder, and Obsessive Compulsive Disorder. RCADS provides a score for each subscale as well as a total score for anxiety, which is the sum of all anxiety subscales except MDD, a total score for all the scales (sum of six subscales). The higher the score, the more the child presents the clinical symptomatology of anxiety and depression (45, 46). The questionnaire had a Cronbach alpha of 0.759.
Ethical Considerations
The study protocol obtained the approval of Saint-Joseph University ethics committee of and Hotel-Dieu Hospital ethic committee (USJ, HDF, number CEHDF 1102). Prior to participating, an informed written formal consent was given by one of the parents. The study was conducted between March and December 2018. The self-administered anonymous questionnaires were filled by the children's parent(s).
Statistical Analysis
The statistical analyses were performed with SPSS software for Windows (version 24.0, Chicago, IL, USA). The level of significance was set at 0.05. The mean and standard deviation were calculated for continuous variables and percentage was calculated for categorical variables. The normality of the distribution of continuous variables was assessed by Kolmogorov-Smirnov tests. In the first step, univariate analyses using the Student's t-test or non-parametric Mann-Whitney test and ANOVA (analysis of variance) or its equivalent non-parametric Kruskal-Wallis test were performed. ANOVA (analysis of variance) followed by Tukey post-hoc tests or its equivalent non-parametric Kruskal-Wallis test were performed to evaluate the association between continuous variables.
To evaluate the association between continuous variables, Pearson and Spearman correlation coefficients were calculated, and to assess the relationship between categorical variables, Fisher Exact tests, and Chi-square independence tests were performed. In the second step, multiple regression analyses were performed according to the Enter Method; all independent variables with a -p- <0.200 were entered into the equation simultaneously. Collinearity among independent variables was also examined. Finally, two regression models were executed; the first model included age, electronic device, social phobia, major depression, separation anxiety, and SDSC. Since, the variables disorders of initiating and maintaining sleep, non-restorative sleep, and sleep breathing disorders are domains that belong to SDSC, they were not included in the same multivariate model. Hence, the second model includes: age, electronic device, social phobia, major depression, separation anxiety, and disorders of maintaining sleep, non-restorative sleep and sleep breathing disorders.
The sample size was calculated according to the formula of Tabachnick and Fidell (47) taking into consideration the number of independent variables to include in the model: the formula used was N = 50 + 8m (m being the number of independent variables for the primary outcome); Given that m = 6, we had to include at least 98 subjects in the study.
Results
Sociodemographic Characteristics of the Participants
The total number of children included in this study was 100 children. The mean age of the population is 9.10 (±2.25) years old. Twenty percent of the children were overweight and 19% were obese (Table 1).
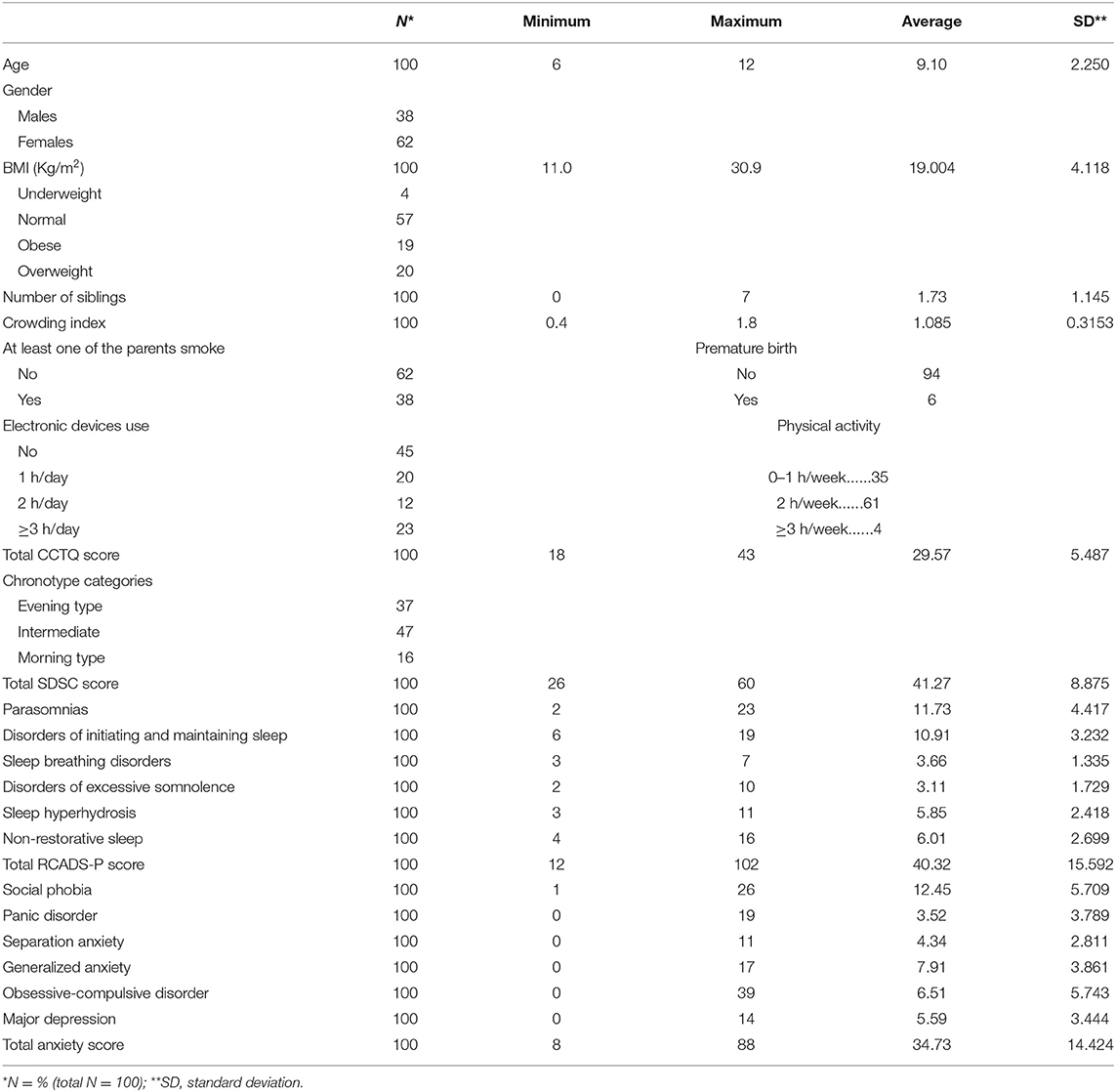
Table 1. Socio-demographic characteristics, eating patterns, physical activity, and electronic devices use of the participants and results obtained for the questionnaires of SDSC, CCTQ, and RCADS-P.
Physical activity and electronic devices use are also reported.
Scores of the CCTQ, SDSC, and RCADS-P Questionnaires
Approximately, half of the sample (47%) were classified as having an intermediate chronotype. The total SDSC and CCTQ scores were respectively 41.27 ± 8.875 and 29.57 ± 5.487. Detailed results are presented in Table 1.
Association Between Chronotype, BMI, Sleep, and RCADS-P Domains: Results of the Univariate Analysis
Evening type children were significantly older, but no associations were observed between chronotype and BMI (Table 2). Furthermore, there was a significant association between chronotype and electronic devices use: among evening type children, 52% used electronic devices ≥ 3 h/week vs. 4.3% only among morning type children (Table 2). Table 3 shows significant associations between chronotype categories and SDSC or RCADS-P domains and Table 4 presents correlations between chronotype scores and SDSC or RCADS-P domains.
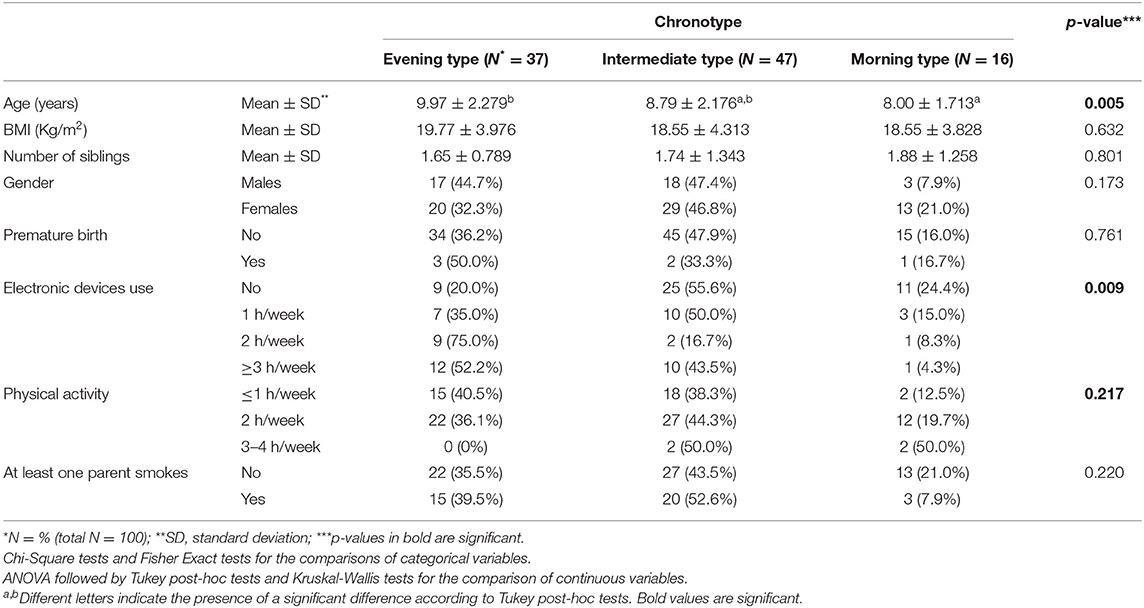
Table 2. Association between chronotype categories and participants' characteristics.
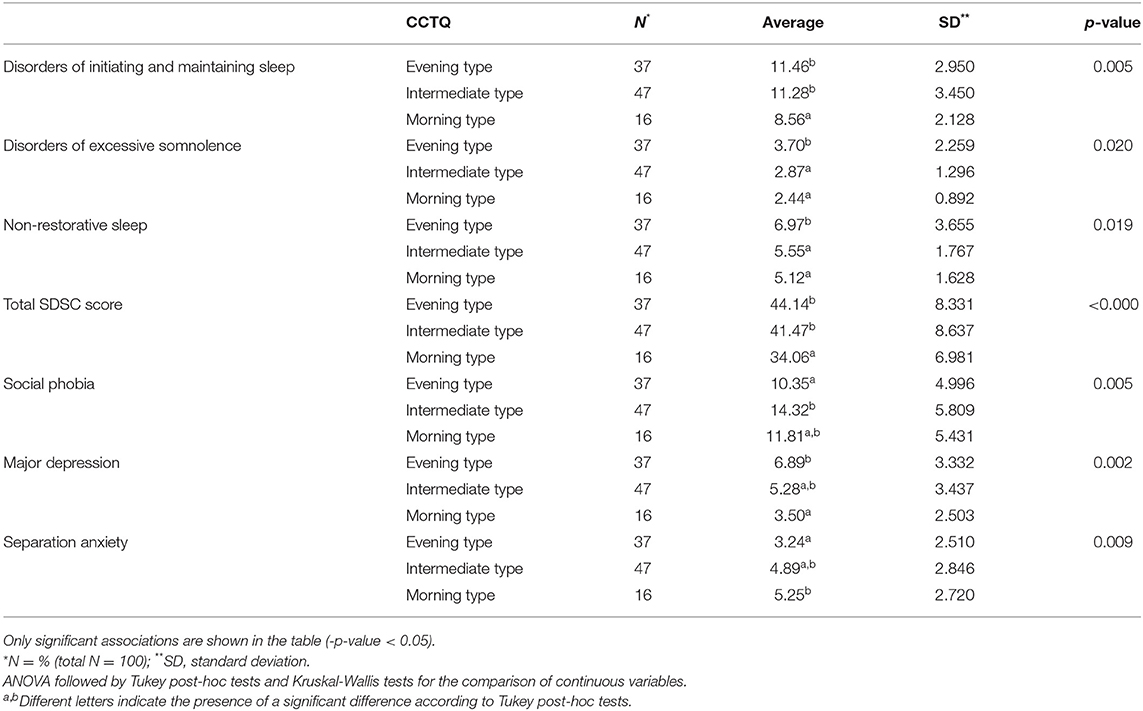
Table 3. Associations between chronotype categories, SDSC, and RCADS-P domains (N = 100).
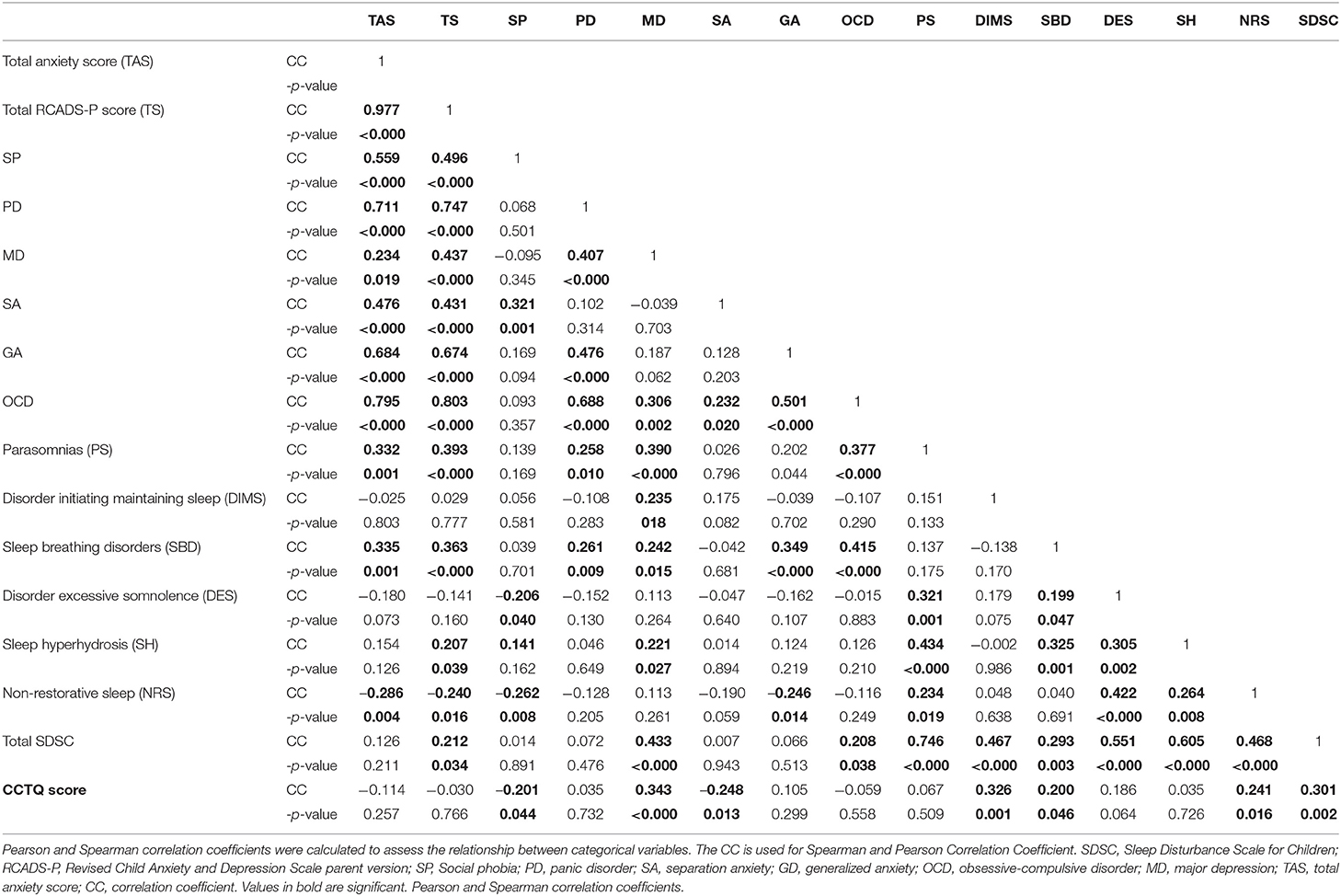
Table 4. Correlations between SDSC, CCTQ, and RCADS-P scores (N = 100).
Association Between Chronotype, BMI, Sleep, and RCADS-P Domains: Results of the Multivariate Analysis
Later chronotype (higher CCTQ score) was associated with higher SDSC score, indicating greater sleep disturbance; It was also associated with older age, electronic devices use and with higher score on the major depression domain of the RCADS-P (Table 5).
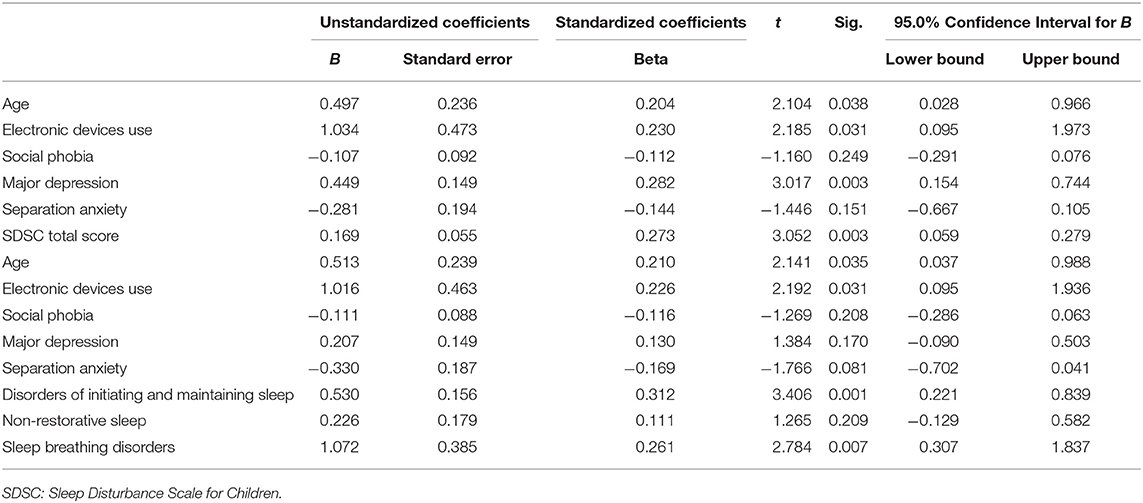
Table 5. Multivariate analysis according to Enter Method: chronotype score taken as the dependent variable.
Discussion
Our results showed that the majority of the sample (47%) presented an intermediate chronotype which is consistent with several previously conducted studies (42, 48); However, 37% of the sample presented an evening chronotype, which was higher than other studies (48). This could be explained by the fact that different instruments are used, such as the youth self-report with the Morningness/Eveningness Scale in Children (MESC) in the study of Carskadon et al. (42). Furthermore, differences in age and gender distribution exist between the different study's samples. Among our sample, the average age was around 9 years old, which is closer to puberty onset, especially in females (consisting 62% of our sample). Indeed, it was previously reported that the onset of puberty triggers an evening preference among approximately 40% of youth, which is compounded by social changes (e.g., less parental control, technology) (49, 50). In addition, the chronotype depends on genetic and environmental factors (51) and these factors are specific to each population and each culture.
There was a shift toward evening chronotype with increased age: evening type children were significantly older than morning type (9.97 ± 2.279 vs. 8.00 ± 1.713 years of age). It was previously reported that a shift toward later sleep rhythm occurs from early to late adolescence (48, 52) and eveningness was associated with older participants in another recent study conducted among participants aged from 11 to 19 years (48).
Excessive use of electronic media (such as computers, tablets, smartphones, gaming consoles, etc.) among adolescents was known to be associated with a disruption in the circadian clock, irregular, shortened, and later sleep onset (53). Little is known about this topic among children, but one could predict that the same consequences would be seen. Indeed, our results showed a significant association between electronic devices use and an evening chronotype.
Higher sleep disturbances were also observed among children with an evening chronotype, similarily to previous report about eveningness among youth resulting in sleep deprivation (49, 50). Several authors previously noted that an evening preference was associated with an irregular sleep-wake schedule (54). In particular, disorders of initiating and maintaining sleep, non-restorative sleep, excessive somnolence, and total SDSC were significantly higher among evening type children in our study. In fact, the most common symptom of sleep disorders is non-restorative sleep, which results in daytime sleepiness (55). Several studies demonstrated that non-restorative sleep is associated with other various health problems such as heart disease, respiratory diseases, obesity, depressive symptoms, and suicide among adults (56). Non-restorative sleep and a short sleep duration were significantly linked to suicidal ideation in adolescents (57). Very few data exist about the consequences of non-restorative sleep among children but they are probably problematic. Thus, interventions aiming at screening sleep problems, especially non-restorative sleep associated with eveningness among children seem important because they might prevent further sleep complications later on in life.
Finally, anxiety domains of the RCADS-P were not associated to chronotype after performing the multivariate analysis but major depression scores were significantly higher among children with an evening chronotype (38–44). Exhibiting preference for eveningness has already been associated with several negative outcomes, in particular, depression (58–64), poor academic performance (34, 61), physical inactivity, higher rates of alcohol use, of smoking, and obesity (65, 66) among adolescents and adults. A recent report among children and adolescents between 11 and 19 years old (42) also showed that eveningness was associated with higher levels of depression.
The reciprocal effects between chronotype and depression are poorly understood during the critical developmental period extending from childhood to adolescence and the nature of our study (cross-sectional) does not allow to draw hypothesis on the cause-effect relationship between chronotype and depression. In addition, the nature of the questionnaire used (RCADS-P), which is a screening and not a diagnostic tool, does not allow to assume a diagnosis of major depression, only a high suspicion of it.
Our findings should take into account several limitations. The results were obtained through questionnaires filled out by the parent of the child. Although, parents are aware of when they put their children to bed and when they wake up, the ability of parents to report on their child's preference for evening vs. morning is more limited. No information about Tanner Stage was available even though it could affect chronotype. The cross-sectional design of this study limits the authors' ability to determine whether later chronotype preceded or followed the existence of high depression scores on the RCADS-P; thus, the methodology is not adapted to establish a causal relationship between chronotype and depression suspicion. Finally, we excluded any chronic disease and of chronic medication intake, which prevented us from studying the impact of comorbidities on chronotype.
Despite these limitations, several findings observed in this study explain factors associated to circadian rhythm disturbances in children; the aspects explored are important and warrant further investigations.
Conclusion
Significant associations were observed in this study between chronotype and sleep as well as between chronotype and major depression domain of the RCADS-P among children. Based on our results, two important future perspectives can be highlighted: (i) limiting electronic devices use among children in an effort to reduce circadian rhythm disturbances and (ii) identifying and treating sleep problems associated with eveningness, taking into account the possible presence of major depression among this population.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by ethics committee of Saint-Joseph University and Hotel-Dieu Hospital. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
BE and MB: data collection and analysis. P-HT and IM: data collection and protocol design. NE: statistical analysis and protocol design. JN and MS: data collection and writing manuscript draft. LR: protocol design, interpretation of data, writing the draft, and final manuscript.
Funding
This work was supported by Saint-Joseph university research council (FPH76).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank the research council of Saint-Joseph university.
References
1. Adan A, Archer SN, Hidalgo MP, Di Milia L, Natale V, Randler C. Circadian typology: a comprehensive review. Chronobiol Int. (2012) 29:1153–75. doi: 10.3109/07420528.2012.719971
2. Dursun OB, Ogutlu H, Esin IS. Turkish Validation and Adaptation of Children's Chronotype Questionnaire (CCTQ). Eurasian J Med. (2015) 47:56–61. doi: 10.5152/eajm.2014.0061
3. Nielsen T. Nightmares associated with the eveningness chronotype. J Biol Rhythms. (2010) 25:53–62. doi: 10.1177/0748730409351677
4. Selvi Y, Gulec M, Agargun MY, Besiroglu L. Mood changes after sleep deprivation in morningness-eveningness chronotypes in healthy individuals. J Sleep Res. (2007) 16:241–4. doi: 10.1111/j.1365-2869.2007.00596.x
6. Nakade M, Akimitsu O, Wada K, Krejci M, Noji T, Taniwaki N, et al. Can breakfast tryptophan and vitamin B6 intake and morning exposure to sunlight promote morning-typology in young children aged 2 to 6 years? J Physiol Anthropol. (2012) 31:11. doi: 10.1186/1880-6805-31-11
8. Simpkin CT, Jenni OG, Carskadon MA, Wright KP, Akacem LD, Garlo KG, et al. Chronotype is associated with the timing of the circadian clock and sleep in toddlers. J Sleep Res. (2014) 23:397–405. doi: 10.1111/jsr.12142
9. Randler C, Faßl C, Kalb N. From Lark to Owl: developmental changes in morningness-eveningness from new-borns to early adulthood. Sci Rep. (2017) 7:45874. doi: 10.1038/srep45874
10. Gau S-F, Soong W-T. The transition of sleep-wake patterns in early adolescence. Sleep. (2003) 26:449–54. doi: 10.1093/sleep/26.4.449
12. Roenneberg T, Kuehnle T, Pramstaller PP, Ricken J, Havel M, Guth A, et al. A marker for the end of adolescence. Curr Biol. (2004) 14:R1038–R39. doi: 10.1016/j.cub.2004.11.039
13. Culnan E, Kloss JD, Grandner M. A prospective study of weight gain associated with chronotype among college freshmen. Chronobiol Int. (2013) 30:682–90. doi: 10.3109/07420528.2013.782311
14. Lucassen EA, Zhao X, Rother KI, Mattingly MS, Courville AB, de Jonge L, et al. Evening chronotype is associated with changes in eating behavior, more sleep apnea, and increased stress hormones in short sleeping obese individuals. PLoS One. (2013) 8:e56519. doi: 10.1371/journal.pone.0056519
15. Yu JH, Yun C-H, Ahn JH, Suh S, Cho HJ, Lee SK, et al. Evening chronotype is associated with metabolic disorders and body composition in middle-aged adults. J Clin Endocrinol Metab. (2015) 100:1494–502. doi: 10.1210/jc.2014-3754
16. Arora T, Taheri S. Associations among late chronotype, body mass index and dietary behaviors in young adolescents. Int J Obes. (2015) 39:39–44. doi: 10.1038/ijo.2014.157
17. Mota MC, Waterhouse J, De-Souza DA, Rossato LT, Silva CM, Araújo MBJ, et al. Association between chronotype, food intake and physical activity in medical residents. Chronobiol Int. (2016) 33:730–9. doi: 10.3109/07420528.2016.1167711
18. Nakade M, Takeuchi H, Kurotani M, Harada T. Effects of meal habits and alcohol/cigarette consumption on morningness-eveningness preference and sleep habits by Japanese female students aged 18-29. J Physiol Anthropol. (2009) 28:83–90. doi: 10.2114/jpa2.28.83
19. Türkoglu S, Çetin FH. The relationship between chronotype and obesity in children and adolescent with attention deficit hyperactivity disorder. Chronobiol Int. (2019) 36:1138–47. doi: 10.1080/07420528.2019.1622131
20. Merikanto I, Kronholm E, Peltonen M, Laatikainen T, Lahti T, Partonen T. Relation of chronotype to sleep complaints in the general Finnish population. Chronobiol Int. (2012) 29:311–7. doi: 10.3109/07420528.2012.655870
21. Merikanto I, Paavonen EJ, Saarenpää-Heikkilä O, Paunio T, Partonen T. Eveningness associates with smoking and sleep problems among pregnant women. Chronobiol Int. (2017) 34:650–8. doi: 10.1080/07420528.2017.1293085
22. Soehner AM, Kennedy KS, Monk TH. Circadian preference and sleep-wake regularity: associations with self-report sleep parameters in daytime-working adults. Chronobiol Int. (2011) 28:802–9. doi: 10.3109/07420528.2011.613137
23. Jafar NK, Tham EKH, Eng DZH, Goh DYT, Teoh O-H, Lee YS, et al. The association between chronotype and sleep problems in preschool children. Sleep Med. (2017) 30:240–4. doi: 10.1016/j.sleep.2016.11.015
24. Carvalho Bos S, Gomes A, Clemente V, Marques M, Pereira AT, Maia B, et al. Sleep and behavioral/emotional problems in children: a population-based study. Sleep Med. (2009) 10:66–74. doi: 10.1016/j.sleep.2007.10.020
25. Rubens SL, Evans SC, Becker SP, Fite PJ, Tountas AM. Self-reported time in bed and sleep quality in association with internalizing and externalizing symptoms in school-age youth. Child Psychiatry Hum Dev. (2017) 48:455–67. doi: 10.1007/s10578-016-0672-1
26. Sivertsen B, Harvey AG, Lundervold AJ, Hysing M. Sleep problems and depression in adolescence: results from a large population-based study of Norwegian adolescents aged 16-18 years. Eur Child Adolesc Psychiatry. (2014) 23:681–9. doi: 10.1007/s00787-013-0502-y
27. Coulombe JA, Reid GJ, Boyle MH, Racine Y. Sleep problems, tiredness, and psychological symptoms among healthy adolescents. J Pediatr Psychol. (2011) 36:25–35. doi: 10.1093/jpepsy/jsq028
28. Wang B, Isensee C, Becker A, Wong J, Eastwood PR, Huang R-C, et al. Developmental trajectories of sleep problems from childhood to adolescence both predict and are predicted by emotional and behavioral problems. Front Psychol. (2016) 7:1874. doi: 10.3389/fpsyg.2016.01874
29. Whalen DJ, Gilbert KE, Barch DM, Luby JL, Belden AC. Variation in common preschool sleep problems as an early predictor for depression and anxiety symptom severity across time. J Child Psychol Psychiatry. (2017) 58:151–9. doi: 10.1111/jcpp.12639
30. Sadeh A, Tikotzky L, Kahn M. Sleep in infancy and childhood: implications for emotional and behavioral difficulties in adolescence and beyond. Curr Opin Psychiatry. (2014) 27:453–9. doi: 10.1097/YCO.0000000000000109
31. Tonetti L, Natale V, Randler C. Association between circadian preference and academic achievement: a systematic review and meta-analysis. Chronobiol Int. (2015) 32:792–801. doi: 10.3109/07420528.2015.1049271
32. Astill RG, Van der Heijden KB, Van Ijzendoorn MH, Van Someren EJW. Sleep, cognition, and behavioral problems in school-age children: a century of research meta-analyzed. Psychol Bull. (2012) 138:1109–38. doi: 10.1037/a0028204
33. Tzischinsky O, Shochat T. Eveningness, sleep patterns, daytime functioning, and quality of life in Israeli adolescents. Chronobiol Int. (2011) 28:338–43. doi: 10.3109/07420528.2011.560698
34. Giannotti F, Cortesi F, Sebastiani T, Ottaviano S. Circadian preference, sleep and daytime behaviour in adolescence. J Sleep Res. (2002) 11:191–9. doi: 10.1046/j.1365-2869.2002.00302.x
35. Pabst SR, Negriff S, Dorn LD, Susman EJ, Huang B. Depression and anxiety in adolescent females: the impact of sleep preference and body mass index. J Adolesc Health Off Publ Soc Adolesc Med. (2009) 44:554–60. doi: 10.1016/j.jadohealth.2008.11.012
36. Putois B, Leslie W, Gustin MP, Challamel M-J, Raoux A, Guignard-Perret A, et al. The French sleep disturbance scale for children. Sleep Med. (2017) 32:56–65. doi: 10.1016/j.sleep.2016.12.008
37. Huang MM, Qian Z, Wang J, Vaughn MG, Lee YL, Dong GH. Validation of the sleep disturbance scale for children and prevalence of parent-reported sleep disorder symptoms in Chinese children. Sleep Med. (2014) 15:923–8. doi: 10.1016/j.sleep.2014.03.023
38. Werner H, LeBourgeois MK, Geiger A, Jenni OG. Assessment of chronotype in four- to eleven-year-old children: reliability and validity of the children's chronotype questionnaire (CCTQ). Chronobiol Int. (2009) 26:992–1014. doi: 10.1080/07420520903044505
39. Munich Chronotype Questionnaire (MCTQ). Available online at: https://www.thoracic.org/members/assemblies/assemblies/srn/questionaires/mctq.php (cited Mar 31, 2020).
40. Zavada A, Gordijn MCM, Beersma DGM, Daan S, Roenneberg T. Comparison of the munich chronotype questionnaire with the Horne-Ostberg's morningness-eveningness score. Chronobiol Int. (2005) 22:267–78. doi: 10.1081/CBI-200053536
41. Roenneberg T, Wirz-Justice A, Merrow M. Life between clocks: daily temporal patterns of human chronotypes. J Biol Rhythms. (2003) 18:80–90. doi: 10.1177/0748730402239679
42. Carskadon MA, Vieira C, Acebo C. Association between puberty and delayed phase preference. Sleep. (1993) 16:258–62. doi: 10.1093/sleep/16.3.258
43. Carskadon MA, Wolfson AR, Acebo C, Tzischinsky O, Seifer R. Adolescent sleep patterns, circadian timing, and sleepiness at a transition to early school days. Sleep. (1998) 21:871–81. doi: 10.1093/sleep/21.8.871
44. Desor JA, Beauchamp GK. Longitudinal changes in sweet preferences in humans. Physiol Behav. (1987) 39:639–41. doi: 10.1016/0031-9384(87)90166-1
45. Spence SH. Structure of anxiety symptoms among children: a confirmatory factor-analytic study. J Abnorm Psychol. (1997) 106:280–97. doi: 10.1037/0021-843X.106.2.280
46. Chorpita BF, Yim L, Moffitt C, Umemoto LA, Francis SE. Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behav Res Ther. (2000) 38:835–55. doi: 10.1016/S0005-7967(99)00130-8
47. Tabachnick BG, Fidell LS. Using Multivariate Statistics. 4th ed. Needham Heights, Mass: Allyn and Bacon (2001). Available online at: https://trove.nla.gov.au/version/8267663 (cited May 28, 2019).
48. Haraden DA, Mullin BC, Hankin BL. The relationship between depression and chronotype: a longitudinal assessment during childhood and adolescence. Depress Anxiety. (2017) 34:967–76. doi: 10.1002/da.22682
49. Gradisar M, Gardner G, Dohnt H. Recent worldwide sleep patterns and problems during adolescence: a review and meta-analysis of age, region, and sleep. Sleep Med. (2011) 12:110–8. doi: 10.1016/j.sleep.2010.11.008
50. Carskadon M, Mindell J, Drake C. Contemporary sleep patterns of adolescents in the USA: results of the 2006 National Sleep Foundation Sleep in America poll. J Sleep Res. (2006) 15:165–74.
51. Archer SN, Robilliard DL, Skene DJ, Smits M, Williams A, Arendt J, et al. A length polymorphism in the circadian clock gene per3 is linked to delayed sleep phase syndrome and extreme diurnal preference. Sleep. (2003) 26:413–5. doi: 10.1093/sleep/26.4.413
52. Merikanto I, Lahti J, Kuula L, Heinonen K, Räikkönen K, Andersson S, et al. Circadian preference and sleep timing from childhood to adolescence in relation to genetic variants from a genome-wide association study. Sleep Med. (2018) 50:36–41. doi: 10.1016/j.sleep.2018.04.015
53. Touitou Y, Touitou D, Reinberg A. Disruption of adolescents' circadian clock: the vicious circle of media use, exposure to light at night, sleep loss and risk behaviors. J Physiol Paris. (2016) 110(4 Pt B):467–79. doi: 10.1016/j.jphysparis.2017.05.001
54. Gau SSF, Kessler RC, Tseng W-L, Wu Y-Y, Chiu Y-N, Yeh C-B, et al. Association between sleep problems and symptoms of attention-deficit/hyperactivity disorder in young adults. Sleep. (2007) 30:195–201. doi: 10.1093/sleep/30.2.195
55. Nunes ML, Bruni O. Insomnia in childhood and adolescence: clinical aspects, diagnosis, and therapeutic approach. J Pediatr (Rio J). (2015) 91(6 Suppl 1):S26–35. doi: 10.1016/j.jped.2015.08.006
56. Hidaka T, Endo S, Kasuga H, Masuishi Y, Kakamu T, Kumagai T, et al. Associations of presence or absence of exercise and/or physical activity with non-restorative sleep by gender and age: a cross-sectional study. BMJ Open. (2019) 9:e025730. doi: 10.1136/bmjopen-2018-025730
57. Park JH, Yoo J-H, Kim SH. Associations between non-restorative sleep, short sleep duration and suicidality: findings from a representative sample of Korean adolescents. Psychiatry Clin Neurosci. (2013) 67:28–34. doi: 10.1111/j.1440-1819.2012.02394.x
58. Drennan MD, Klauber MR, Kripke DF, Goyette LM. The effects of depression and age on the Horne-Ostberg morningness-eveningness score. J Affect Disord. (1991) 23:93–8. doi: 10.1016/0165-0327(91)90096-B
59. Kitamura T, Sun C, Martin J, Kitch LJ, Schnitzer MJ, Tonegawa S. Entorhinal cortical ocean cells encode specific contexts and drive context-specific fear memory. Neuron. (2015) 87:1317–31. doi: 10.1016/j.neuron.2015.08.036
60. Hidalgo CA, Blumm N, Barabási A-L, Christakis NA. A dynamic network approach for the study of human phenotypes. PLOS Comput Biol. (2009) 5:e1000353. doi: 10.1371/journal.pcbi.1000353
61. Merikanto I, Lahti T, Kronholm E, Peltonen M, Laatikainen T, Vartiainen E, et al. Evening types are prone to depression. Chronobiol Int. (2013) 30:719–25. doi: 10.3109/07420528.2013.784770
62. Chelminski I, Ferraro FR, Petros TV, Plaud JJ. An analysis of the “eveningness-morningness” dimension in “depressive” college students. J Affect Disord. (1999) 52:19–29. doi: 10.1016/S0165-0327(98)00051-2
63. Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep. (2013) 36:1059–68. doi: 10.5665/sleep.2810
64. Dorn LD, Negriff S, Huang B, Pabst S, Hillman J, Braverman P, et al. Menstrual symptoms in adolescent girls: association with smoking, depressive symptoms, and anxiety. J Adolesc Health. (2009) 44:237–43. doi: 10.1016/j.jadohealth.2008.07.018
65. Roenneberg T, Allebrandt KV, Merrow M, Vetter C. Social jetlag and obesity. Curr Biol. (2012) 22:939–43. doi: 10.1016/j.cub.2012.03.038
Keywords: chronotype, weight, sleep, anxiety, depression, children
Citation: Eid B, Bou Saleh M, Melki I, Torbey P-H, Najem J, Saber M, El Osta N and Rabbaa Khabbaz L (2020) Evaluation of Chronotype Among Children and Associations With BMI, Sleep, Anxiety, and Depression. Front. Neurol. 11:416. doi: 10.3389/fneur.2020.00416
Received: 14 February 2020; Accepted: 20 April 2020;
Published: 05 June 2020.
Edited by:
Maurice M. Ohayon, Stanford University, United StatesReviewed by:
Lourdes DelRosso, University of Washington, United StatesKristen Knutson, Northwestern Medicine, United States
Copyright © 2020 Eid, Bou Saleh, Melki, Torbey, Najem, Saber, El Osta and Rabbaa Khabbaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lydia Rabbaa Khabbaz, bHlkaWEua2hhYmJhekB1c2ouZWR1Lmxi
†These authors have contributed equally to this work