 Michael H. Schönfeld1*
Michael H. Schönfeld1* Reza Kabiri1
Reza Kabiri1 Helge C. Kniep1
Helge C. Kniep1 Lukas Meyer1
Lukas Meyer1 Rosalie McDonough1Jan Sedlacik1,2Marielle Ernst1
Rosalie McDonough1Jan Sedlacik1,2Marielle Ernst1 Gabriel Broocks1
Gabriel Broocks1 Tobias Faizy1
Tobias Faizy1 Gerhard Schön3
Gerhard Schön3 Bastian Cheng4
Bastian Cheng4 Götz Thomalla4
Götz Thomalla4 Jens Fiehler1
Jens Fiehler1 Uta Hanning1
Uta Hanning1- 1Department of Diagnostic and Interventional Neuroradiology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 2Biomedical Engineering Department, Centre for the Developing Brain, School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom
- 3Institute of Medical Biometry and Epidemiology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 4Department of Neurology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Background: Thrombus fragmentation causing distal emboli is a feared complication during mechanical thrombectomy (MT). We aimed to investigate the impact of procedural parameters and thrombus properties on the incidence of peripheral emboli after MT for large vessel occlusions (LVO).
Methods: We performed a prospective analysis of patients with LVO stroke successfully treated with MT, defined as a score of 2b, 2c, or 3 on the thrombolysis in cerebral infarction (TICI) scale. A follow-up MRI including high-resolution diffusion-weighted imaging (DWI) was performed within 24 h following MT. The primary endpoint was the number and volume of peripheral emboli, classified as punctuate DWI lesions distant to the diffusion-restricted core lesion. Further analysis included the influence of baseline characteristics, procedural and outcome parameters, and thrombus properties on peripheral emboli.
Results: Thirty-seven patients with successful MT met the inclusion criteria. Use of a balloon guide catheter (BGC) and TICI were the only independent predictors for a reduced number of peripheral emboli. The use of a BGC led to a significant reduction in the number and volume of peripheral emboli, with a median number/volume of peripheral emboli of 4.5/287 μl (IQR 1.25–8.25/76–569 μl) vs. 12/938 μl (IQR 4–19/242–1,836 μl). In cases where BGC was not employed, the number of peripheral emboli increased with decreasing TICI scores.
Conclusions: BGC-aided MT reduces the number of peripheral emboli in successful but incomplete reperfusion (TICI 2b and 2c). The effectiveness of this strategy therefore goes above and beyond that which can be demonstrated by the TICI score alone.
Introduction
Mechanical thrombectomy (MT) has become a standard treatment for acute ischemic stroke due to large vessel occlusion (LVO) following publication of multiple randomized trials demonstrating its efficacy (1). Thrombus fragmentation, a complication of MT, can result in peripheral emboli which, in turn, can worsen clinical outcomes (2). The occurrence of peripheral emboli is not only influenced by various technical aspects of MT, but also likely by the occlusion site and individual thrombus properties (3–5). Persistent thrombi after MT can only be detected on post-interventional digital subtraction angiography (DSA) if the occluded vessel is large enough and can affect the thrombolysis in cerebral infarction (TICI) score. Additionally, higher TICI reperfusion scores are known to be associated with improved rates of favorable functional outcome (6, 7). Notably, the majority of peripheral emboli released during MT are smaller in size (8). These small fragments might cause vessel obstructions not detectable by DSA but only by magnetic resonance imaging (MRI) (9). Hence, these emboli are generally not considered in the final TICI rating after recanalization.
Recently, we found that peripheral ischemic lesions resulting from these emboli can frequently be detected on high-resolution diffusion-weighted imaging (DWI) despite supposed complete reperfusion in DSA (10). The assessment of potentially superior treatment techniques or predictors of outcome following MT by standard outcome or imaging measures requires a large patient cohort. The use of peripheral emboli as a surrogate parameter may help to tease apart the more subtle differences between the currently available treatment options.
We aimed to analyze the influence of procedural details, the location of the occlusion, as well as the thrombus properties on the occurrence of peripheral emboli, as detected by high-resolution DWI (HR-DWI). We hypothesized that the number of peripheral emboli during MT of LVO can be reduced with the utilization of balloon guide catheters (BGC).
Materials and Methods
Inclusion Criteria and Study Endpoints
We conducted a prospective study of patients treated with MT for LVO at a tertiary stroke center between August 2017 and March 2019. Inclusion criteria were defined as follows: (1) anterior circulation LVO; (2) thrombectomy as endovascular therapy; (3) successful reperfusion (defined as TICI ≥2b); (4) post-interventional MRI follow-up imaging including a HR-DWI sequence.
The primary study endpoint was defined as the absolute number and volume of peripheral emboli detected on HR-DWI MRI imaging following MT. A further analysis of possible factors influencing the incidence of peripheral emboli after MT was performed, including BGC utilization.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The local ethics committee approved the study (Ethics Committee of the Board of Physicians Hamburg; approval number WF 019/19) and waived the requirement to obtain informed consent.
Endovascular Treatment
If eligible, all patients received intravenous thrombolysis (IVT) with alteplase prior to MT (11). Procedures were performed via a femoral artery approach under conscious sedation or general anesthesia. The choice of thrombectomy devices, including the selection of a BGC, was at the discretion of the treating neurointerventionalist. No formal decision process was applied for the choice of treatment technique.
Magnetic Resonance Imaging (MRI)
MRI was performed on a 1.5 T MRI scanner (Siemens Magnetom Avanto, Erlangen, Germany) within 24 h following intervention.
Axial whole-brain HR-DWI was performed using single-shot, multi-slice, spin-echo, echo-planar imaging sequences with diffusion gradients in three orthogonal directions and the following parameters: TR/TE 13000/90 ms, b-values of 0, 500 and 1,000 sec/mm2, matrix 192 × 192, no gap, field of view 240, slice thickness 2 mm, no gap, and an acquisition time of 457 s.
Imaging Analysis
Density of the thrombus and the contralateral vessel was determined in 1 mm thick axial reconstructions of non-enhanced computed tomography scans (CT) by placement of 1–2 mm2 regions of interest. Thrombus density was represented in both Hounsfield units and as a density ratio (density of the thrombus/density of the contralateral vessel). Thrombus length was measured on multiplanar reconstructions of pre-interventional CT-angiography.
Post-interventional DSA imaging was rated according to the revised TICI definition proposed by Noser et al. and endorsed by Goyal et al. (12). Here, TICI grade 2b is defined as reperfusion of more than 50% of the expected territory, grade 2c as near-complete perfusion without a clearly visible thrombus, yet delay in contrast run-off and grade 3 as complete perfusion with physiological filling of all distal branches of the expected territory in a normal hemodynamic fashion (13).
The first pass effect (FPE) was defined as achieving near-complete reperfusion (TICI ≥2c) after single-device and adjunctive technique approach (14).
Peripheral emboli were defined as diffusion restrictions on DWI distant to a continuous core DWI lesion. They were classified as lesions either within the vascular territory of the primary LVO or emboli into new territories.
All DWI lesions were semi-automatically segmented using seed growing algorithms provided by the Analyze 11.0 software package (AnalyzeDirect, Inc., Overland Park, KS, USA). Imaging analysis was performed independently by two readers that did not participate in the endovascular procedure. Discrepancies between readers were resolved by consensus.
Statistical Analysis
The impact of thrombus and interventional parameters on the number of peripheral emboli was first assessed in univariable regression models. Then Poisson regression was used to model the effect of independent predictors on the number of peripheral emboli. As independent parameters, we analyzed i.v. alteplase, occlusion location, thrombus density and length, devices used, number of revascularization attempts, reperfusion score, and FPE.
Data is reported using standard descriptive statistics. Wilcoxon signed rank test was performed to compare continuous variables, as appropriate. Chi Square test and Fisher's exact test were used to compare categorial variables. All statistics were calculated using SPSS 24.0 (IBM SPSS Statistics for Windows, Armonk, NY: IBM Corp.) and R 3.61 (R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. Vienna, Austria, 2019). P < 0.05 were considered statistically significant.
Results
Study Population
Thirty-seven patients met the inclusion criteria and were prospectively enrolled in the study (Figure 1). The median age was 71 years (IQR 65.5–80) and 51.4% (19/37) were female. The median time from onset to recanalization was 275 min (IQR 227–385). On admission, the median ASPECTS was 7 (6–9) and the median NIHSS was 14 (9.5–16.5). On initial CT scans, the median thrombus length was 15 mm (IQR 10.5–20) and the median thrombus density was 60 HU (IQR 53.5–64.5). 45.9% (17/37) of all patients received i.v. alteplase prior to MT. All LVOs were located within in the anterior circulation, including 29.7% (11/37) in the terminal internal carotid artery (tICA) and 70.3% (26/37) in the M1 segment of the media cerebral artery (MCA). 18.9% (7/37) of all occlusions were tandem occlusions with concomitant extracranial ICA stenosis. Table 1 gives a detailed overview of the patient baseline characteristics and outcome data.
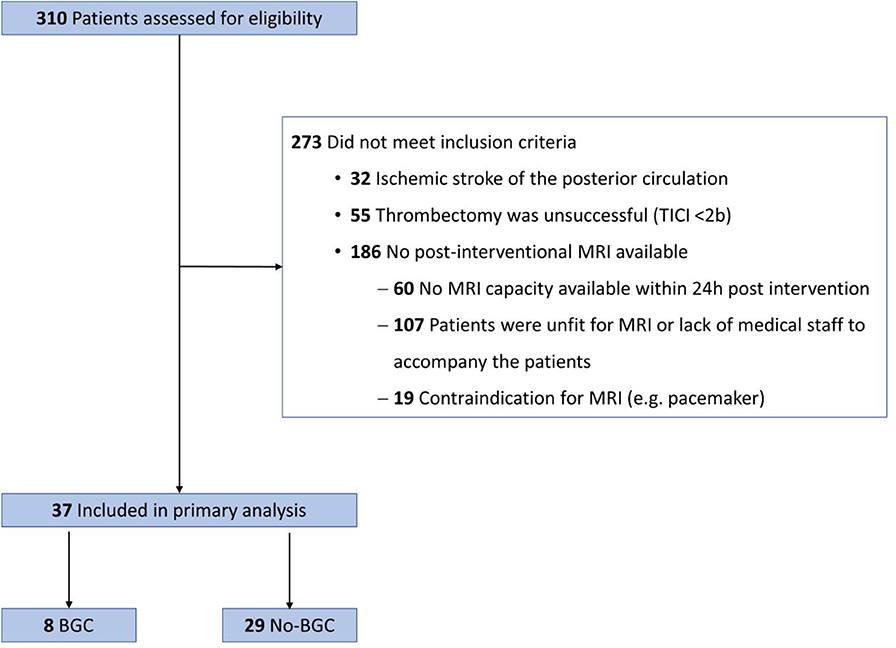
Figure 1. Flowchart of patients included in the study from August 2017 to March 2019. BGC, balloon guide catheter; TICI, thrombolysis in cerebral infarction; MRI, Magnetic Resonance Imaging.
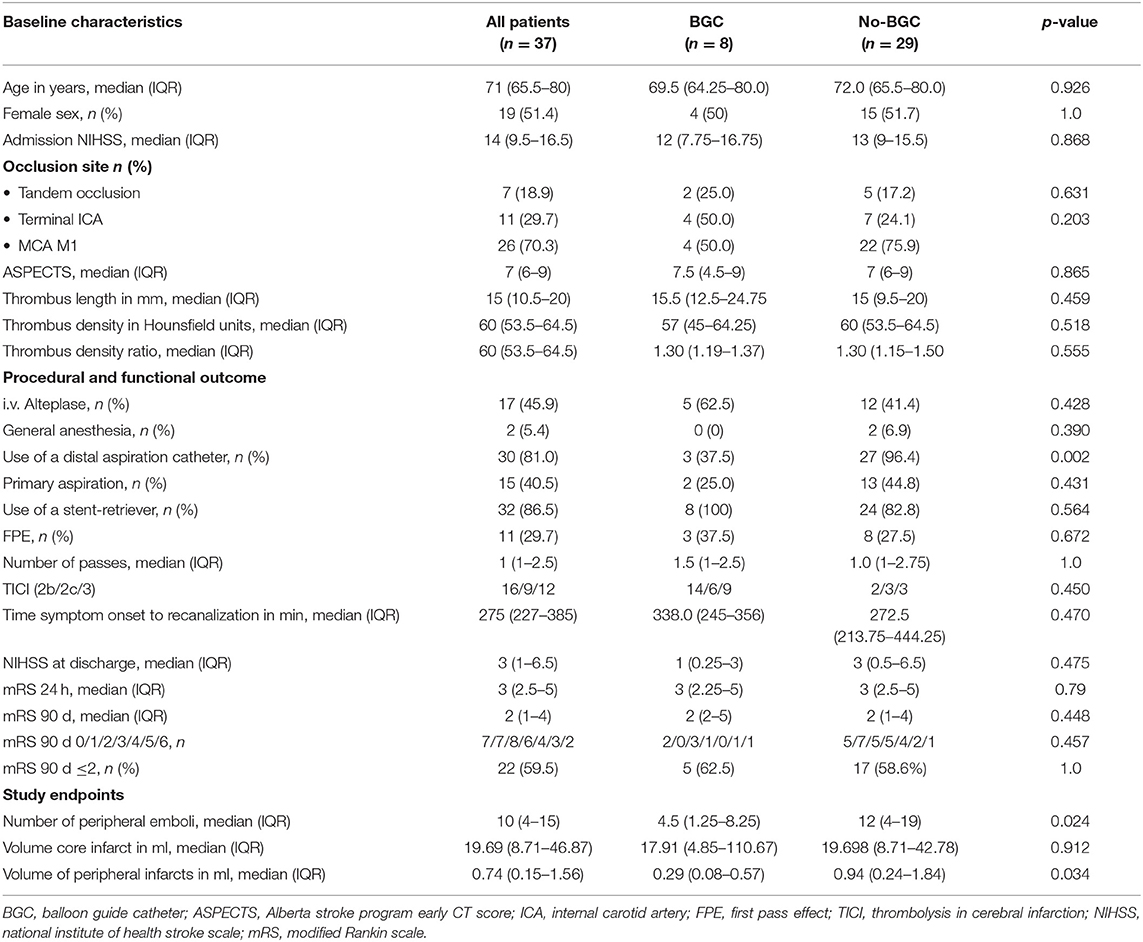
Table 1. Comparison of patient baseline characteristics, procedural and functional outcome, and study endpoints between patients treated with and without balloon guide catheters.
Study Endpoints
In univariate linear regression analysis FPE, reperfusion success assessed with the TICI scale, and the use of BGC were found to be predictors for the number of peripheral emboli (Table 2).
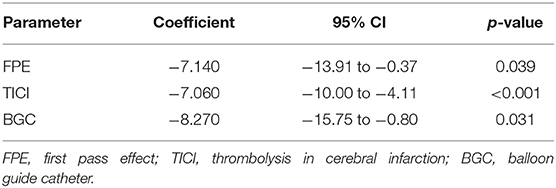
Table 2. Univariate linear regression analysis of predictors for peripheral emboli.
FPE was excluded from the Poisson regression model due to its direct relationship with the TICI rating; all cases with FPE are rated as either TICI 2c or 3. Based on an ordinal scale, TICI entered the model in the subcategories 2b, 2c, and 3. The predictive value of BGC use and TICI for the number of peripheral emboli was confirmed in the Poisson regression model after adjusting for the interaction between TICI and BGC. In cases where BGC was not employed, the number of peripheral emboli decreased with increasing TICI scores. With BGC, however, the reduction of the number of peripheral emboli with increasing TICI scores was less pronounced and the number of peripheral emboli after successful but incomplete reperfusion (TICI 2b and 2c) was lower compared to patients treated without BGC (Figure 2, Table 3).
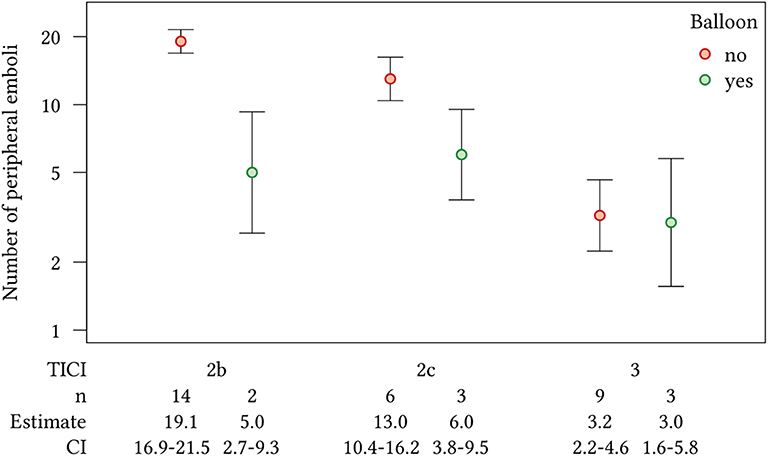
Figure 2. Effect plot showing the number of peripheral emboli with 95% CI in the Poisson regression model, with the interaction of TICI score and the use of a BGC.
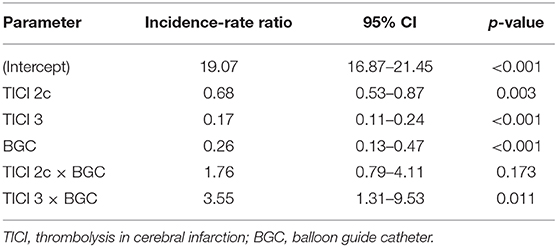
Table 3. Poisson regression model with interaction of TICI and the use of a BGC for the prediction of peripheral emboli.
For all patients receiving BGC-aided MT, the incidence of peripheral emboli was significantly lower (median 4.5 vs. 12; p = 0.024), and the total volume of peripheral ischemias was significantly lower (median 938 vs. 287 μl; p = 0.034) compared to those who were treated without BGC use (Figure 3). The “BGC cohort” and the “non-BGC” cohort did not differ significantly regarding demographics, pre-interventional ASPECTS, occlusion location, previous administration of i.v. alteplase, thrombus properties, MT success, and total number of revascularization attempts. Distal aspiration catheters were used more often in cases where BGC was not employed (Table 1).
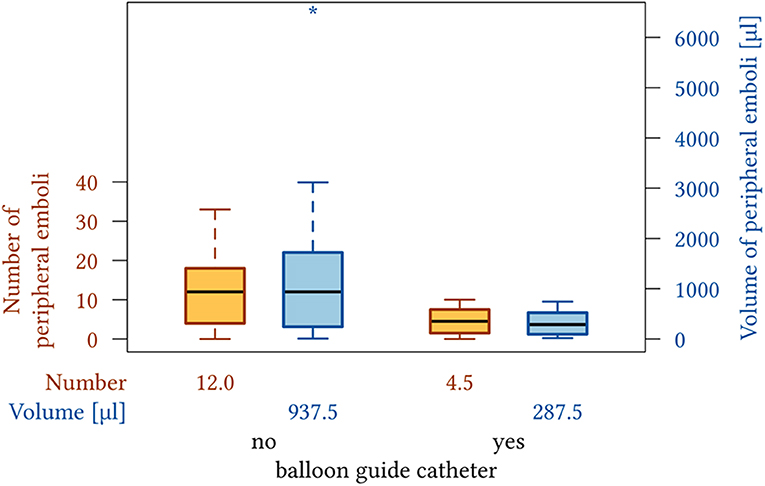
Figure 3. Box plot showing the number and volume of peripheral emboli seen after MT without and with the use of a BCG.
Discussion
Our analysis further supports the hypothesis that the utilization of BGCs reduces the number of peripheral emboli detected as peripheral ischemia after MT of LVO. While there was no significant difference in the number of peripheral emboli when complete reperfusion was achieved (TICI 3), the use of BGC reduced the number of peripheral emboli after successful but incomplete reperfusion (TICI 2b and 2c).
This is the first study investigating the impact of baseline characteristics, procedural and outcome parameters, as well as thrombus properties on the incidence of peripheral emboli after MT with high-resolution DWI.
In-vitro and animal models have demonstrated the reduction in the number of peripheral emboli with BGC via two mechanisms; both antegrade flow arrest and concurrent aspiration at the balloon guide reduce migration of the entrapped thrombus or fragmented clots extracted by the stent retriever (4, 15). An in-vitro vascular phantom occlusion model showed that BGC offered a two-fold improvement in soft elastic clot fragmentation compared with a standard guide catheter (16). In a porcine model, Nikoubashman et al. demonstrated that BGC utilization provided reliable flow arrest and flow reversal with manual syringe aspiration, whereas aspiration with a conventional 8 F guide catheter resulted in either collapse of the vessel or oscillatory flow, potentially permitting antegrade flow (4).
The first clinical evidence for the use of BGC came from an analysis of the NASA registry data that found improved clinical outcomes and reperfusion scores (17). A meta-analysis of non-randomized trials suggested that use of BGC is associated with superior clinical and angiographic outcomes (18). Recently, analysis of the data gathered in the STRATIS Stroke Thrombectomy Registry and TRACK registry came to the same conclusion that the use of BGC is an independent predictor of clinical and angiographic outcome (19, 20). Our study further reaffirms the reperfusion benefit of BGC, beyond angiographic findings.
In MT without BGC, reperfusion success was a predictor for the number of peripheral emboli in our study. This is in line with previous studies in which reperfusion success was found to be the most important modifiable predictor for outcome (21). Accordingly, the largest proportion of patients with excellent functional outcome (mRS ≤ 1) is seen in cases in which complete reperfusion (TICI 3) was achieved (21, 22). Consequently, the neurointerventionalist performing MT should aim to achieve the best reperfusion success possible.
FPE was also a predictor for the number of peripheral emboli in the univariate analysis. Recently, Nikoubashman et al. reported that FPE was an independent factor for favorable outcome, however their analysis did not test for the influence of BGC (23). It has been shown that the use of BGC facilitates FPE and, by definition, the FPE influences the TICI score (20). It is therefore not an independent variable and was removed from the multivariate model in our study.
None of the other baseline characteristics, thrombus properties, or procedural details had a significant effect on the number of peripheral emboli in our study.
Utilizing the technique that achieves the highest possible grade of reperfusion success at first pass is important to minimize the risk of clot fragmentation and downstream emboli. Our study reinforces the benefit of BGC in achieving better reperfusion results, which in turn leads to improved clinical outcomes in patients with LVO stroke.
The clinical impact of peripheral emboli is uncertain. They may, along with other modifiable factors that are associated with poor outcomes following stroke (procedural emboli into the anterior cerebral artery territory, hypertension, hyperglycemia, and fever), help elucidate why some patients despite successful reperfusion and small core infarcts do not regain functional independency (24, 25). In our study, the total volume of peripheral emboli made up only a small fraction of the ischemic core volume. However, not only the size of the infarct core, but also infarct location, can have a significant impact on clinical outcome (26). If located within eloquent brain regions (e.g., the motor cortex or corticospinal tract) even small lesions could have a substantial impact on a patient's level of functional independence. Furthermore, primarily subclinical DWI lesions could manifest as early neurocognitive changes (27).
Our findings demonstrate the use of imaging markers for the design of future stroke studies. Results from in-vitro testing and porcine in vivo models have provided some evidence for recommendations for procedural details that were otherwise based on hypothetical considerations, (4, 16). But designing a clinical trial to provide evidence for these recommendations will be difficult. A clinical trial seeking to test a true improvement in functional outcomes to this already very effective therapeutic strategy would require many patients, as well as an extended study period. The use of a surrogate outcome measure may therefore be justified to investigate new interventions in proof-of-concept studies. Although the TICI scale is an established predictive tool, it is not able to capture fine subtleties between the current treatment options, potentially explaining the varied outcomes observed for the same reperfusion scores. Techniques that reduce the number of peripheral emboli may therefore be preferable, as they could increase the frequency of favorable outcome, thereby partially resolving such discrepancies. The authors of a recent systematic review and meta-analysis concluded that DWI could be used as surrogate outcome measure for procedural stroke after carotid revascularization (28). For acute stroke treatment, DWI infarct growth has already been proposed as a surrogate endpoint for future stroke therapy trials in order to reduce sample sizes (29). Acquiring HR-DWI to detect peripheral emboli may add to this metric.
A major limitation of this study is that we did not acquire pre-interventional HR-DWI to detect the peri-interventional occurrence of ischemic lesions. Although desirable, unnecessarily delaying treatment by nearly 8 min (the acquisition time of HR-DWI) is not justifiable. Furthermore, small ischemic lesions likely would not yet be detectable due to the acute time window (30). Some ischemias might have resulted from pre-interventional fragmentation of the thrombus. Comparing pre- and post-treatment MRI of a large cohort of patients with LVO, Gratz et al. found that patients more commonly present with a single thrombus rather than with multiple thrombi (2). Therefore, persisting vessel occlusion after recanalization of the initial LVO is likely the result of thrombus fragmentation during the MT procedure rather than the presence of a second, pre-existing thrombus. Furthermore, the reduction of emboli with the use of a BGC is in itself another convincing argument for the peri-interventional incidence of most of the peripheral emboli.
Another limitation is the low rate of BGC cases. This is due to the fact that the favored technique in our department includes the use of a large bore distal aspiration catheter, incompatible with our current BGC. Nevertheless, despite our small cohort size, the association between BGC use and reduced number of emboli is evident.
Conclusion
Incidence of peripheral emboli after MT for LVO stroke is lower with the utilization of a BGC for successful but incomplete reperfusion (TICI scale 2b and 2c). When observed in HR-DWI this effect goes above and beyond the TICI scale. Therefore, MT with proximal flow-arrest could have a greater influence on procedural and functional outcomes than initially expected. Further studies investigating the role of BGC in MT are urgently needed to confirm these findings.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Board of Physicians Hamburg. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
MS, JS, JF, and UH conceptualized the study. MS, RK, HK, JS, ME, GB, TF, BC, and GT collected the data. MS, HK, and GS performed the statistical analysis. MS, RM, LM, and UH drafted the manuscript. MS, RK, HK, LM, RM, JS, ME, GB, TF, BC, JF, and GT revised the manuscript.
Conflict of Interest
JF: Consultant for Acandis, Boehringer Ingelheim, Codman, Microvention, Sequent, Stryker. Speaker for Bayer Healthcare, Bracco, Covidien/ev3, Penumbra, Philips, Siemens. Grants from Bundesministeriums für Wirtschaft und Energie (BMWi), Bundesministerium für Bildung und Forschung (BMBF), Deutsche Forschungsgemeinschaft (DFG), European Union (EU), Covidien, Stryker (THRILL study), Microvention (ERASER study), Philips. GT: Received personal fees as consultant/lecturer from Acandis, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb/Pfizer, Daichi Sankyo, Stryker, and research grants from Bayer, Federal Ministry for Economic Affairs and Energy (BMWi), Corona-Foundation, German Research Foundation (DFG), Else Kröner-Fresenius Foundation, European Union (Horizon 2020), German Innovation Fund.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. (2016) 387:1723–31. doi: 10.1016/S0140-6736(16)00163-X
2. Gratz PP, Schroth G, Gralla J, Mattle HP, Fischer U, Jung S, et al. Whole-brain susceptibility-weighted thrombus imaging in stroke: fragmented thrombi predict worse outcome. AJNR Am J Neuroradiol. (2015) 36:1277–82. doi: 10.3174/ajnr.A4275
3. Sporns PB, Hanning U, Schwindt W, Velasco A, Buerke B, Cnyrim C, et al. Ischemic stroke: histological thrombus composition and pre-interventional CT attenuation are associated with intervention time and rate of secondary embolism. Cerebrovasc Dis. (2017) 44:344–50. doi: 10.1159/000481578
4. Nikoubashman O, Wischer D, Hennemann HM, Sandmann J, Sichtermann T, Muschenich FS, et al. Balloon-guide catheters are needed for effective flow reversal during mechanical thrombectomy. AJNR Am J Neuroradiol. (2018) 39:2077–81. doi: 10.3174/ajnr.A5829
5. Yeo LLL, Holmberg A, Mpotsaris A, Soderman M, Holmin S, Kuntze Soderqvist A, et al. Posterior circulation occlusions may be associated with distal emboli during thrombectomy : factors for distal embolization and a review of the literature. Clin Neuroradiol. (2019) 29:425–33. doi: 10.1007/s00062-018-0679-z
6. Behme D, Tsogkas I, Colla R, Gera RG, Schregel K, Hesse AC, et al. Validation of the extended thrombolysis in cerebral infarction score in a real world cohort. PLoS ONE. (2019) 14:e0210334. doi: 10.1371/journal.pone.0210334
7. Liebeskind DS, Bracard S, Guillemin F, Jahan R, Jovin TG, Majoie CB, et al. eTICI reperfusion: defining success in endovascular stroke therapy. J Neurointerv Surg. (2019) 11:433–8. doi: 10.1136/neurintsurg-2018-014127
8. Chueh JY, Puri AS, Wakhloo AK, Gounis MJ. Risk of distal embolization with stent retriever thrombectomy and ADAPT. J Neurointerv Surg. (2016) 8:197–202. doi: 10.1136/neurintsurg-2014-011491
9. Klinger-Gratz PP, Schroth G, Gralla J, Jung S, Weisstanner C, Verma RK, et al. Protected stent retriever thrombectomy prevents iatrogenic emboli in new vascular territories. Neuroradiology. (2015) 57:1045–54. doi: 10.1007/s00234-015-1583-8
10. Schonfeld MH, Kabiri R, Kniep HC, Meyer L, Sedlacik J, Ernst M, et al. Sub-angiographic peripheral emboli in high resolution DWI after endovascular recanalization. J. Neurol. (2020) 267:1401–6. doi: 10.1007/s00415-020-09719-1
11. DGN. Akuttherapie des Ischämischen Schlaganfalls – Rekanalisierende Therapie (Ergänzung 2015) (2015)
12. Goyal M, Fargen KM, Turk AS, Mocco J, Liebeskind DS, Frei D, et al. 2C or not 2C: defining an improved revascularization grading scale and the need for standardization of angiography outcomes in stroke trials. J Neurointerv Surg. (2014) 6:83–6. doi: 10.1136/neurintsurg-2013-010665
13. Noser EA, Shaltoni HM, Hall CE, Alexandrov AV, Garami Z, Cacayorin ED, et al. Aggressive mechanical clot disruption: a safe adjunct to thrombolytic therapy in acute stroke? Stroke. (2005) 36:292–6. doi: 10.1161/01.STR.0000152331.93770.18
14. Zaidat OO, Castonguay AC, Linfante I, Gupta R, Martin CO, Holloway WE, et al. First pass effect: a new measure for stroke thrombectomy devices. Stroke. (2018) 49:660–6. doi: 10.1161/STROKEAHA.117.020315
15. Gralla J, Schroth G, Remonda L, Nedeltchev K, Slotboom J, Brekenfeld C. Mechanical thrombectomy for acute ischemic stroke: thrombus-device interaction, efficiency, and complications in vivo. Stroke. (2006) 37:3019–24. doi: 10.1161/01.STR.0000248457.55493.85
16. Chueh JY, Kuhn AL, Puri AS, Wilson SD, Wakhloo AK, Gounis MJ. Reduction in distal emboli with proximal flow control during mechanical thrombectomy: a quantitative in vitro study. Stroke. (2013) 44:1396–401. doi: 10.1161/STROKEAHA.111.670463
17. Nguyen TN, Malisch T, Castonguay AC, Gupta R, Sun CH, Martin CO, et al. Balloon guide catheter improves revascularization and clinical outcomes with the Solitaire device: analysis of the North American solitaire acute stroke registry. Stroke. (2014) 45:141–5. doi: 10.1161/STROKEAHA.113.002407
18. Brinjikji W, Starke RM, Murad MH, Fiorella D, Pereira VM, Goyal M, et al. Impact of balloon guide catheter on technical and clinical outcomes: a systematic review and meta-analysis. J Neurointerv Surg. (2018) 10:335–9. doi: 10.1136/neurintsurg-2017-013179
19. Nguyen TN, Castonguay AC, Nogueira RG, Haussen DC, English JD, Satti SR, et al. Effect of balloon guide catheter on clinical outcomes and reperfusion in Trevo thrombectomy. J Neurointerv Surg. (2019) 11:861–5. doi: 10.1136/neurintsurg-2018-014452
20. Zaidat OO, Mueller-Kronast NH, Hassan AE, Haussen DC, Jadhav AP, Froehler MT, et al. Impact of balloon guide catheter use on clinical and angiographic outcomes in the stratis stroke thrombectomy registry. Stroke. (2019) 50:697–704. doi: 10.1161/STROKEAHA.118.021126
21. Kaesmacher J, Dobrocky T, Heldner MR, Bellwald S, Mosimann PJ, Mordasini P, et al. Systematic review and meta-analysis on outcome differences among patients with TICI2b versus TICI3 reperfusions: success revisited. J Neurol Neurosurg Psychiatr. (2018) 89:910–7. doi: 10.1136/jnnp-2017-317602
22. Rizvi A, Seyedsaadat SM, Murad MH, Brinjikji W, Fitzgerald ST, Kadirvel R, et al. Redefining 'success': a systematic review and meta-analysis comparing outcomes between incomplete and complete revascularization. J Neurointerv Surg. (2019) 11:9–13. doi: 10.1136/neurintsurg-2018-013950
23. Nikoubashman O, Dekeyzer S, Riabikin A, Keulers A, Reich A, Mpotsaris A, et al. True first-pass effect. Stroke. (2019) 50:2140–6. doi: 10.1161/STROKEAHA.119.025148
24. Chalumeau V, Blanc R, Redjem H, Ciccio G, Smajda S, Desilles JP, et al. Anterior cerebral artery embolism during thrombectomy increases disability and mortality. J Neurointerv Surg. (2018) 10:1057–62. doi: 10.1136/neurintsurg-2018-013793
25. Rabinstein AA, Albers GW, Brinjikji W, Koch S. Factors that may contribute to poor outcome despite good reperfusion after acute endovascular stroke therapy. Int J Stroke. (2019) 14:23–31. doi: 10.1177/1747493018799979
26. Ernst M, Boers AMM, Aigner A, Berkhemer OA, Yoo AJ, Roos YB, et al. Association of computed tomography ischemic lesion location with functional outcome in acute large vessel occlusion ischemic stroke. Stroke. (2017) 48:2426–33. doi: 10.1161/STROKEAHA.117.017513
27. Fanning JP, Wesley AJ, Walters DL, Eeles EM, Barnett AG, Platts DG, et al. Neurological injury in intermediate-risk transcatheter aortic valve implantation. J Am Heart Assoc. (2016) 5:e004203. doi: 10.1161/JAHA.116.004203
28. Traenka C, Engelter ST, Brown MM, Dobson J, Frost C, Bonati LH. Silent brain infarcts on diffusion-weighted imaging after carotid revascularisation: a surrogate outcome measure for procedural stroke? A systematic review and meta-analysis. Eur Stroke J. (2019) 4:127–43. doi: 10.1177/2396987318824491
29. Sah RG, d'Esterre CD, Hill MD, Hafeez M, Tariq S, Forkert ND, et al. Diffusion-weighted imaging lesion growth occurs despite recanalization in acute ischemic stroke: implications for future treatment trials. Int J Stroke. (2019) 14:257–64. doi: 10.1177/1747493018798550
Keywords: ischemic stroke, cerebrovascular disease/stroke, revascularization, embolism, magnetic resonance imaging (MRI)
Citation: Schönfeld MH, Kabiri R, Kniep HC, Meyer L, McDonough R, Sedlacik J, Ernst M, Broocks G, Faizy T, Schön G, Cheng B, Thomalla G, Fiehler J and Hanning U (2020) Effect of Balloon Guide Catheter Utilization on the Incidence of Sub-angiographic Peripheral Emboli on High-Resolution DWI After Thrombectomy: A Prospective Observational Study. Front. Neurol. 11:386. doi: 10.3389/fneur.2020.00386
Received: 31 January 2020; Accepted: 17 April 2020;
Published: 07 May 2020.
Edited by:
Thanh Nguyen, Boston University, United StatesReviewed by:
Alicia C. Castonguay, University of Toledo, United StatesNirav Bhatt, Emory University, United States
Copyright © 2020 Schönfeld, Kabiri, Kniep, Meyer, McDonough, Sedlacik, Ernst, Broocks, Faizy, Schön, Cheng, Thomalla, Fiehler and Hanning. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael H. Schönfeld, bS5zY2hvZW5mZWxkQHVrZS5kZQ==