
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 15 April 2020
Sec. Stroke
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.00214
This article is part of the Research Topic Hemostasis and Stroke View all 19 articles
 Hui Fang1†
Hui Fang1† Xinyi Leng2†
Xinyi Leng2† Yuehua Pu3,4,5,6
Yuehua Pu3,4,5,6 Xinying Zou3,4,5,6
Xinying Zou3,4,5,6 Yuesong Pan3,4,5,6
Yuesong Pan3,4,5,6 Bo Song1Yannie O. Y. Soo2
Bo Song1Yannie O. Y. Soo2 Thomas W. H. Leung2
Thomas W. H. Leung2 Chunxue Wang3,4,5,6
Chunxue Wang3,4,5,6 Xingquan Zhao3,4,5,6Yilong Wang3,4,5,6Yongjun Wang3,4,5,6Ka Sing Wong2
Xingquan Zhao3,4,5,6Yilong Wang3,4,5,6Yongjun Wang3,4,5,6Ka Sing Wong2 Liping Liu3,4,5,6*
Liping Liu3,4,5,6* Yuming Xu1*
Yuming Xu1*  for the CICAS Study Group
for the CICAS Study GroupBackground: Previous studies conflicted in the association between intracranial atherosclerotic stenosis (ICAS) and the severity of white matter changes (WMC).
Aims: We aimed to investigate the relationships between the severity of luminal stenosis and the hemodynamic significance of middle cerebral artery (MCA) stenosis, and the severity of ipsilateral WMC.
Methods: In this cross-sectional study, patients with a recent ischemic stroke or transient ischemic attack and a 50–99% MCA-M1 stenosis in the Chinese Intracranial Atherosclerosis study cohort were analyzed. The post- to pre-stenotic signal intensity ratio (SIR) was obtained in time-of-flight MR angiography (MRA) to represent the hemodynamic significance of MCA-M1 stenosis, with a lower SIR indicating a hemodynamically more severe lesion. The severity of ipsilesional WMC was assessed by an age-related WMC (ARWMC) scale in T2-weighted fluid attenuated inversion recovery MR imaging. The relationships between the degree of MCA-M1 stenosis, SIR, and ipsilesional ARWMC scale were analyzed. The MCA-M1 lesion with a higher percentage of stenosis was chosen for analyses in patients with bilateral MCA-M1 stenoses.
Results: Among 180 subjects (mean age, 64 years), a lower SIR of MCA-M1 stenosis (Spearman correlation coefficient, −0.543; p < 0.001), but not the degree of stenosis (p = 0.93), was significantly linearly correlated with a higher ipsilateral ARWMC. Multivariate ordinal logistic regression identified older age (OR = 1.037; 95% CI, 1.008–1.066; p = 0.011) and lower SIR (OR = 0.010; 95% CI, 0.002–0.058; p < 0.001) as independent predictors for more severe ipsilateral WMC.
Conclusion: Patients with hemodynamically more severe ICAS are more likely to have more severe ipsilateral WMC. Longitudinal studies with sequential imaging exams may further reveal the impact of hemodynamic significance of ICAS on the development and progression of WMC.
White matter changes (WMC) have been linked to cognitive dysfunction, gait impairment and falls, depression, and increased risk of future stroke (1–4), but the pathophysiology underlying development and progression of WMC are not fully elucidated. Previous studies showed conflicting results regarding whether extra- or intra-cranial atherosclerotic disease is associated with WMC, and which is more closely correlated with WMC (5–8).
We had previously proposed an index termed signal intensity ratio (SIR) to quantify the hemodynamic significance of intracranial atherosclerotic stenosis (ICAS), defined as the ratio of distal (post-stenotic) and proximal (pre-stenotic) signal intensities (SIs) obtained in the vessel lumen in time-of-flight magnetic resonance angiography (MRA), which has been recently validated against CT perfusion measures (9–12). In the present study, we aimed to investigate the associations of severity of luminal narrowing and hemodynamic significance of middle cerebral artery (MCA) stenosis by SIR, with the severity of ipsilateral WMC, in ischemic stroke or transient ischemic attack (TIA) patients with MCA stenosis. This may improve our understanding regarding how the presence of ICAS would act on presence or progression of WMC, and may provide therapeutic targets for prevention of the symptoms subsequent to severe WMC.
This was a cross-sectional study based on the Chinese Intracranial Atherosclerosis (CICAS) study (13). CICAS was a prospective, multicenter, hospital-based, cohort study carried out in 22 hospitals covering a wide geographic area throughout China, enrolling non-cardioembolic ischemic stroke or TIA patients (aged 18–80 years) admitted within 7 days of ictus (13). All patients underwent 1.5- or 3.0-T MR exams, including brain and vascular imaging sequences. Details of the inclusion and exclusion criteria, patient demographics, clinical features, and follow-up information have been described previously (13, 14). The study had been approved by Institutional Review Board at the participating hospitals. Each patient gave written informed consent.
Consecutive patients recruited to the CICAS study, who had 50–99% stenosis [Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) criteria (15)] of the M1 segment of unilateral or bilateral MCA (MCA-M1) in time-of-flight MRA, were screened for the current study. Those with time-of-flight MRA and T2-weighted fluid-attenuated inversion recovery (T2-FLAIR) MR images of adequate quality were enrolled and analyzed in the present study. Patients were excluded if (1) there were no T1/T2-weighted images, time-of-flight MRA or T2-FLAIR images, or the image quality was insufficient for assessment of SIR and WMC; or (2) the MCA lesion was located adjacent to an arterial bifurcation or trifurcation, or a perforator, that was not suitable for the measurement of SIR on MRA. A flow chart of patient screening and selection for the current study is provided in Figure 1. Demographics and characteristics of the index ischemic stroke or TIA were collected.
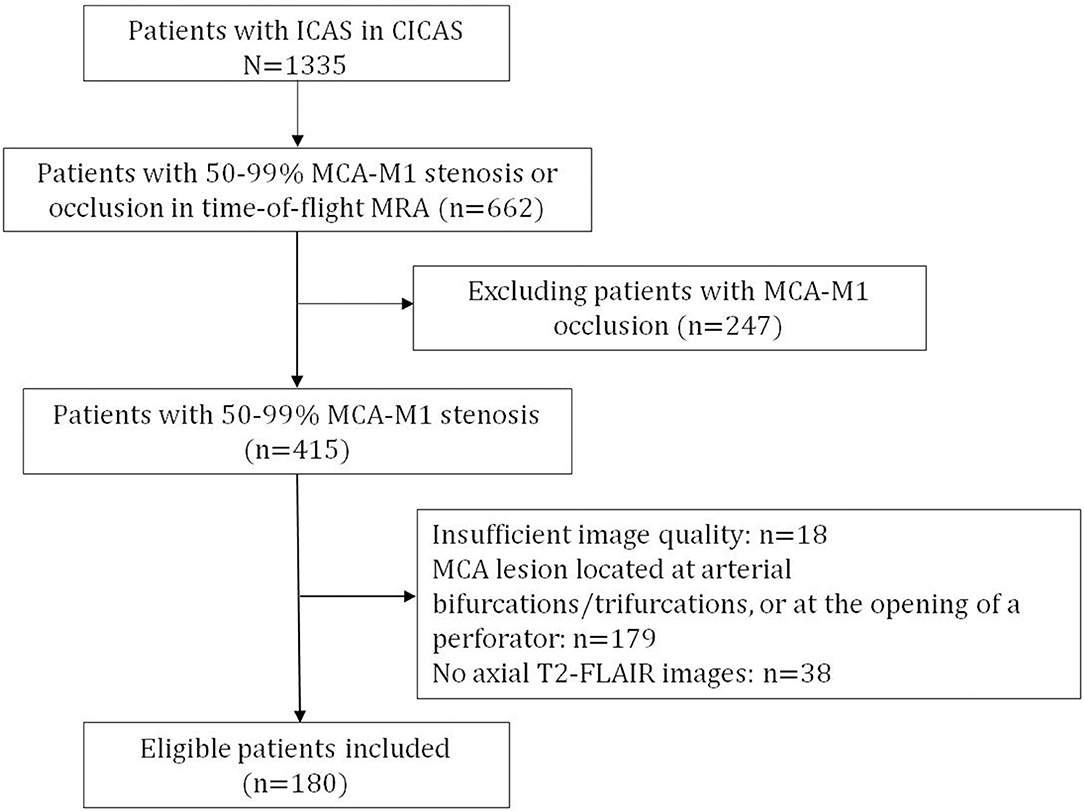
Figure 1. Flow chart of patient screening for the present study.
For each patient, we assessed the percentage of luminal stenosis [the WASID criteria (13, 15)] and the hemodynamic significance (by SIR) of MCA-M1 stenotic lesion in time-of-flight MRA using Phillips DICOM viewer 3.0 (Koninklijke Philips Electronics N.V.), and the severity of ipsilateral WMC by an age-related WMC (ARWMC) scale in axial T1/T2-weighted images and T2-FLAIR images using RadiAnt DICOM Viewer (Medixant). For patients with bilateral MCA-M1 stenoses, the side with a higher degree of stenosis was chosen for image assessment and subsequent analyses.
SIR was obtained in time-of-flight MRA to represent the hemodynamic significance of an MCA-M1 stenosis. The detailed methodology was described previously (10, 16). Briefly, it quantified the relative change in SIs across an ICAS lesion, adjusted by the background SI. Mean SI distal and proximal to MCA-M1 stenosis were measured on the maximum intensity projections (MIPs) showing the highest degree of stenosis of the lesion. In addition, mean background SI was calculated as the mean value of background SIs within the left and right halves of the anterior–posterior direction MIP, in areas adjacent to intracranial internal carotid arteries but free of vessel signals. SIR was then calculated as: SIR = (mean post-stenotic SI – mean background SI)/(mean pre-stenotic SI – mean background SI), with a lower SIR indicating a hemodynamically more severe lesion. The intra-rater (Pearson correlation coefficient, 0.975) and inter-rater reproducibilities (Pearson correlation coefficient, 0.847) of SIR measurement of ICAS lesions have been previously demonstrated (9, 16).
WMC was defined as ill-defined hyperintensities ≥5 mm on both T2-weighted and FLAIR imaging and isointensity on T1-weighted imaging (17, 18). The severity of WMCs was scaled in four regions in the supratentorial hemisphere ipsilateral to the index MCA-M1 stenosis, including the frontal area, the parieto-occipital area, the temporal area (scores 0–3 for each region, respectively, indicating no lesion, focal lesions, beginning confluence of lesions, and diffuse lesions), and the basal ganglia area (scores 0–3, respectively, indicating no lesion, one focal lesion, more than one focal lesion, confluent lesions) (17, 18). The ipsilesional ARWMC scale, ranging from 0 to 12, was calculated as a sum of WMC scores in the four areas, with a larger scale indicating more severe WMC. Two authors (HF and XL) independently evaluated unilateral, supratentorial ARWMC in 20 cases, for the assessment of inter-rater reproducibility of the ARWMC scale. The hemisphere for ARWMC assessment in each patient was determined before the assessment; the two investigators conducting ARWMC assessment were blinded to the data of sites and degrees of stenosis in ICAS lesions in each patient, which were centrally measured by CICAS investigators prior to this sub-study. Kappa test showed that the inter-rater reproducibility of ARWMC assessment was 0.79 for frontal lobe, 0.957 for parietal–occipital lobe, 0.773 for temporal lobe, and 1 for basal ganglia, indicating substantial agreement between the two observers.
Inter-rater reproducibilities of unilateral ARWMC scales of the four regions of interest were assessed by the kappa statistic, with ARWMC as an ordinal variable. Chi-square tests were conducted for the correlations of the degree of MCA-M1 stenosis (50–69% vs. 70–99% stenosis) and SIR (< or ≥ median) as dichotomized variables, with ipsilateral ARWMC scale as an ordinal variable in its quartiles. Spearman correlation coefficients and scatterplots were used to reveal linear correlations between the degree of MCA-M1 stenosis, SIR, and the ipsilateral ARWMC scale, all as continuous variables.
In addition to the degree of MCA-M1 stenosis and its hemodynamic significance by SIR, the differences in the following factors among patients with different supratentorial ARWMC scales by quartiles were also assessed in univariate analyses, including patient demographics, characteristics of the index stroke or TIA, and vascular risk factors, using chi-square tests for categorical variables and ANOVA for continuous variables. Factors with two-sided p < 0.1 in univariate analyses were further analyzed in a multivariate, ordinal logistic regression model, to identify factors independently associated with the ARWMC scale in quartiles. Two-sided p < 0.05 were considered statistically significant. All statistical analyses were performed using SAS software version 9.1 (SAS Institute Inc, Cary, NC).
Of the 1,335 patients with ICAS recruited to the CICAS study (13), 415 had 50–99% stenosis [WASID criteria (15)] of unilateral or bilateral MCA-M1(s) in time-of-flight MRA. After excluding 18 patients with insufficient image quality, 179 patients with stenosis located adjacent to an arterial bifurcation or trifurcation, or a perforator, and 38 patients without axial T2-FLAIR images, 180 patients were analyzed in the current study (flow chart shown in Figure 1).
Among the 180 patients, 116 were men and 64 were women, with a mean age of 63.7 ± 11.6 years. Premorbid modified Rankin scale was 0–2 in all patients. The median interval between symptom onset and admission was 2 days [interquartile range (IQR), 1–4]. The median National Institutes of Health Stroke Scale (NIHSS) upon admission was 4 (IQR 2–7). Among the patients, 126 (71.2%) had a history of hypertension, 34 (23.1%) had dyslipidemia, and 55 (31.1%) had diabetes mellitus (Table 1). No patient had a history of intracranial hemorrhage or atrial fibrillation.
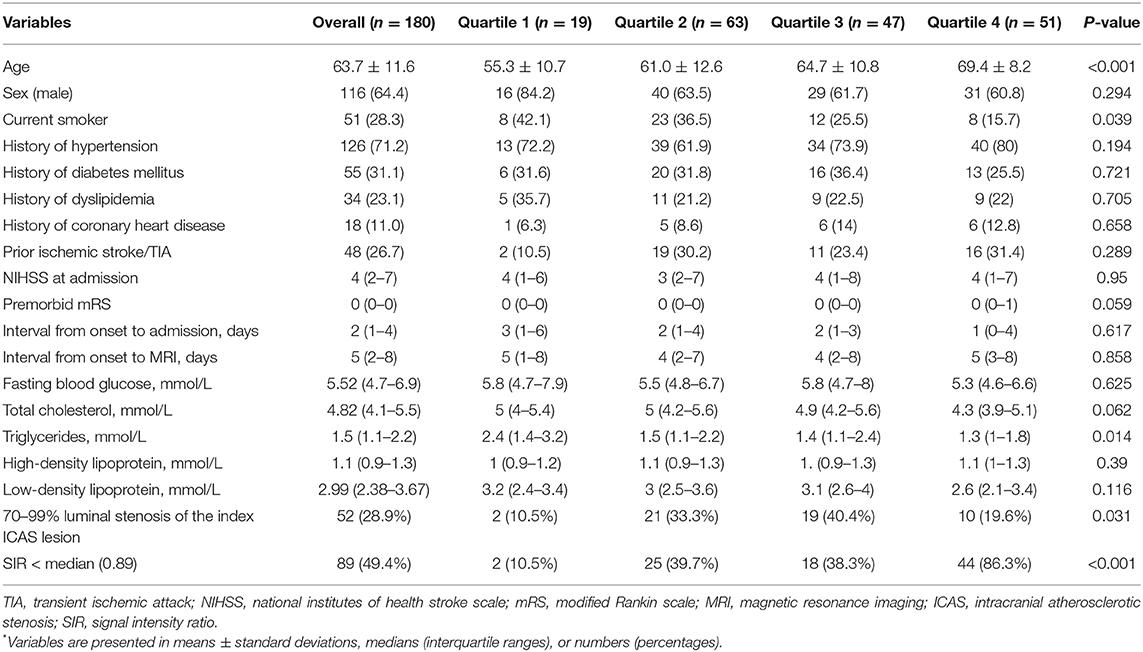
Table 1. Univariate comparisons of clinical and imaging characteristics* in patients grouped by ARWMC scales in quartiles.
The median interval between symptom onset and MRI examination was 2 days (IQR 1–4). Sixty-seven (37.2%) patients underwent 1.5-T MR exams and 113 (62.8%) underwent 3.0-T MR exams. Fifty-two (28.9%) and 128 (71.1%) patients had severe (70–99%) and moderate (50–69%) MCA-M1 stenosis, respectively. The mean SIR of all index MCA-M1 lesions was 0.86 ± 0.21, and the median SIR was 0.89 (IQR 0.73–0.97). The median ipsilesional, supratentorial ARWMC scale was 2 (IQR 1–2).
As shown in Table 1, the proportions of cases with severe (70–99%) MCA-M1 stenosis (p = 0.031) and a SIR < median (p < 0.001) were significantly higher in those with higher ARWMC scale in univariate analyses. However, the severity of MCA luminal stenosis was not significantly, linearly related to ipsilesional ARWMC scale (Spearman correlation coefficient, 0.007; p = 0.93; Figure 2).
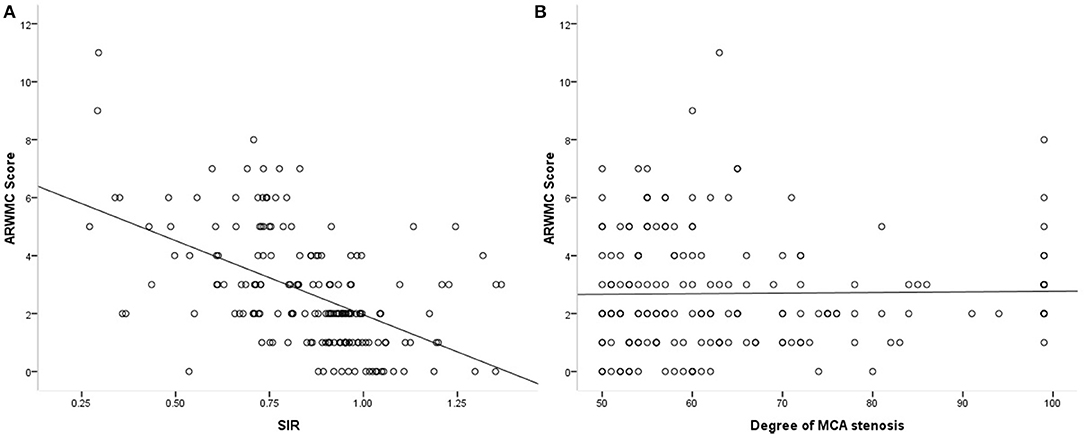
Figure 2. Scatterplots showing the correlations of SIR and degree of MCA stenosis (in percentage) with ipsilateral ARWMC scale.
The proportions of patients with SIR < median were significantly higher in those with a higher ARWMC scale (p < 0.001), which was 86.3% in those with an ARWMC in the highest quartile (Table 1). SIR and the ipsilateral ARWMC scale were significantly, linearly, and negatively correlated (Spearman correlation coefficient, −0.543; p < 0.001; Figure 2), which means that lower SIR (more hemodynamically significant) of MCA-M1 stenosis was associated with more severe ipsilesional WMC. Figure 3 shows the MRA and FLAIR images of two cases, one with a high SIR and a low ARWMC scale, and the other with a low SIR and a high ARWMC scale.
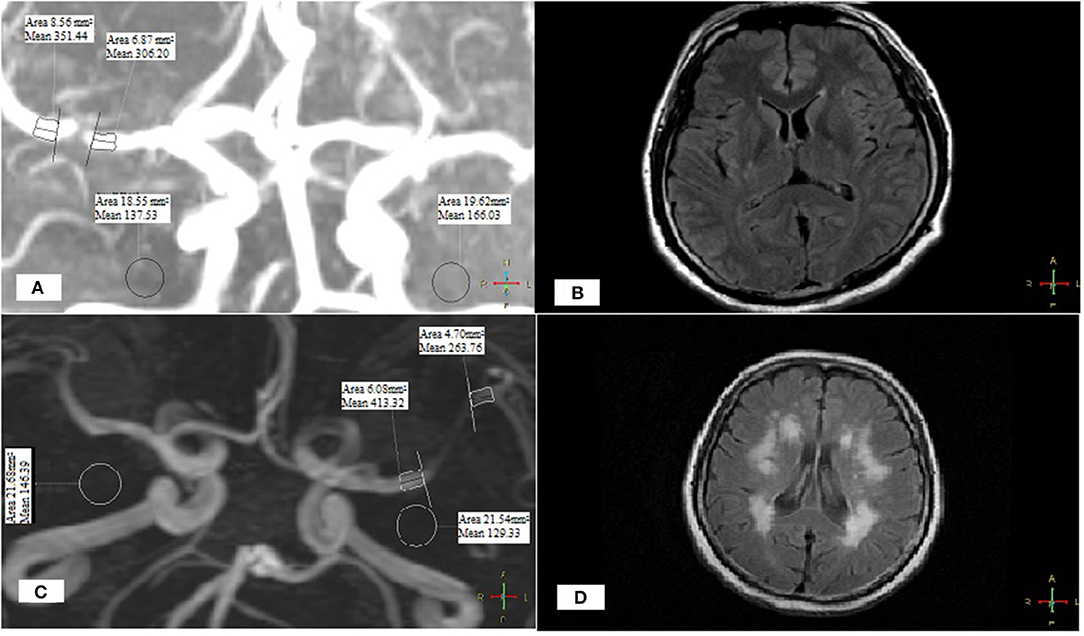
Figure 3. Two cases with different SIR and ARWMC scales.
In addition to the severity of MCA-M1 stenosis and the SIR, other factors differed (p < 0.1) between patients with different ARWMC scales by quartiles in univariate analyses, including age (p < 0.001), current smoker (p = 0.039), premorbid modified Rankin Scale (p = 0.059), and total cholesterol (p = 0.062) and triglycerides (p = 0.014) levels (Table 1). These factors were included in multivariate, ordinal logistic regression analysis, which revealed that older age (OR = 1.037, 95% CI 1.008–1.066; p = 0.011) and lower SIR (OR = 0.010, 95% CI 0.002–0.058; < 0.001), but not the degree of MCA stenosis (OR = 0.725, 95% CI 0.374–1.403; p = 0.340), were significantly, independently associated with a higher ipsilateral ARWMC scale (Table 2).
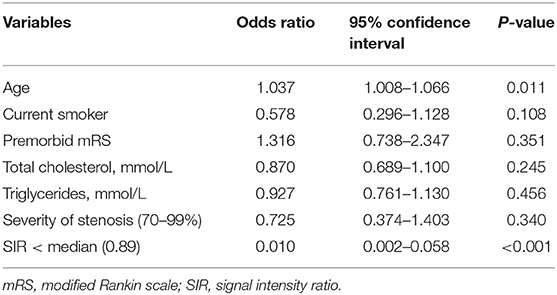
Table 2. Multivariate ordinal logistic regression analysis for independent predictors of the ipsilateral ARWMC scale in quartiles.
In the present study, we investigated whether the severity of luminal stenosis and the hemodynamic significance of MCA stenosis (as quantified by SIR in time-of-flight MRA) were associated with the severity of ipsilateral WMC (as assessed by the ARWMC scale in MRI). The results showed that SIR was significantly, linearly, and negatively correlated with ipsilateral, supratentorial ARWMC scale, and multivariate analyses further corroborated the association of lower SIR with higher ARWMC scale, independent of other confounding factors. The findings indicated that patients with hemodynamically more severe MCA stenosis were more likely to have more severe WMC in the ipsilateral hemisphere. However, the degree of luminal narrowing in MCA stenosis was not significant associated with the severity of ipsilateral WMC in this study. Of note, older age, as an established risk factor of WMC, was also found as an independent predictor of higher ARWMC scale in the current study.
For patients with ICAS, SIR could be easily obtained with the wide application of time-of-flight MRA in clinical practice. Based on the contrast mechanism (flow-related enhancement) of time-of-flight MRA, a lower SIR of an ICAS lesion could, to some extent, reflect downstream hemodynamic impairment caused by the stenotic lesion, which has been correlated with prolonged cerebral perfusion (12), larger acute infarct volume (10), and higher risk of recurrent stroke (11), in patients with a recent ischemic stroke or TIA in previous studies. With previously demonstrated intra- and inter-rater reproducibilities (16), the index SIR could be considered as a simple and effective marker to gauge the hemodynamic significance of ICAS, to be used in relevant research areas. On the other hand, for inter-rater reproducibility of ARWMC assessment in the current study, the kappa test result was 0.79 for frontal lobe, 0.957 for parietal–occipital lobe, 0.773 for temporal lobe, and 1 for basal ganglia, indicating substantial agreement between two observers, which had been demonstrated in previous studies (18). Therefore, this ARWMC assessment scale is operational in clinical practice for assessment of severity of WMC (18).
The roles of extracranial and intracranial large artery atherosclerosis in the development and progression of WMC are uncertain. As mentioned earlier, previous studies showed conflicting results concerning the correlations of presence/extent of WMC with different stages of carotid atherosclerosis (increased intima-media thickness, non-stenotic and stenotic carotid plaques) and intracranial atherosclerosis (mostly intracranial stenosis) (5–8). Some of the studies reported significant correlations while others not. The current study indicated that it might be the hemodynamic impact of ICAS lesions and the possibly subsequent hypoperfusion, but not the degree of luminal stenosis, that governs the severity of ipsilateral WMC. Such inferences are supported by significant correlations between larger white matter lesion volumes and reduced total cerebral blood flow in previous large cohort studies (19–21). Compared with the cortex, the white matter might be more vulnerable to hemodynamic insufficiency, which is supplied by single source subependymal arteries with scarce anastomoses (22–24). This may partly explain the conflicting results in previous studies: the diverse hemodynamic severities of extra- and intra-cranial atherosclerotic lesions in those studies might have interfered with the analyses of their correlations with WMC.
The current findings in the important role of hemodynamic impact of ICAS in determining the severity of WMC may have clinical implications in the management of ICAS patients. As mentioned above, WMC have been related to increased risks of cognitive impairment, dementia, and stroke (1–4). Thus, in this regard, patients with ICAS may benefit from hemodynamic restoring treatment methods, such as angioplasty/stenting, and other treatment methods such as external counter pulsation that can enhance cerebral perfusion (25, 26). However, these inferences need further investigations in future prospective studies.
This study had several limitations. First, patients who underwent 1.5- and 3.0-T MR exams were both included in the present study. The relatively inferior quality of 1.5-T MR images might, to some extent, interfere with the evaluation of SIR and ARWMC, and the severity of MCA luminal stenosis may be overestimated with time-of-flight MRA (27). Second, the influence of isolated or concurrent extracranial stenosis was not considered in the present study, which may be a potential confounder in the correlations between ICAS and WMC. Third, treatment strategies such as medications of the patients receiving may interfere with the associations between SIR and ARWMC, which were not adjusted in the multivariate ordinal logistic regression analyses. Last but not least, the flow-dependent artery visualization mechanism of time-of-flight MRA prohibits accurate calculation of SIR when an ICAS lesion is located adjacent to arterial bifurcations, trifurcations, or perforators, in which case the SIs may alter with or without the presence of ICAS. A considerable number of patients were excluded from the current study due to this reason, which may arouse selection bias.
In conclusion, older age and lower SIR, but not the percentage of luminal stenosis, were independent predictors of higher ipsilateral ARWMC in stroke or TIA patients with MCA-M1 stenosis. In other words, in patients with atherosclerotic MCA stenosis, the hemodynamic impact of the stenotic lesion, rather than the severity of luminal narrowing, may partly determine the severity of ipsilateral WMC. However, it is unclear how the hemodynamic significance of ICAS affects the development and progression of white matter changes based on this cross-sectional study. Further longitudinal studies with sequential imaging exams are warranted.
All datasets generated for this study are included in the article/supplementary material.
The studies involving human participants were reviewed and approved by Ethics Committee of the Tiantan Hospital. The patients/participants provided their written informed consent to participate in this study.
All authors participated in the interpretation of study results and in the drafting, critical revision, and approval of the final version of the article. HF and XL was responsible for study design, data analyses, and drafting and revising the article. HF was responsible for acquisition of data, data analyses, and drafting the article. YPu, XZo, BS, YS, TL, CW, XZh, YiW, and YoW were involved in revising the article for important intellectual content. YPa conducted the statistical analysis. LL and YX was responsible for study concept or design, technical, material support, administrative, and supervision.
This study was supported by the Project of Beijing Institute for Brain Disorders (Reference No. 1152130306) and Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (Reference No. ZYLX201502), Beijing, China; the National Natural Science Foundation of China (Reference No. 81501004); the Education Department of Henan Province (172102310086), China; the Young Elite Scientist Sponsorship Program 2017–2019 (Reference No. 2017QNRC001); and the China Association for Science and Technology.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. (2010) 341:c3666. doi: 10.1136/bmj.c3666
2. de Groot JC, de Leeuw FE, Oudkerk M, van Gijn J, Hofman A, Jolles J, et al. Cerebral white matter lesions and cognitive function: the rotterdam scan study. Ann Neurol. (2000) 47:145–51. doi: 10.1002/1531-8249(200002)47:2<145::aid-ana3>3.3.co;2-p
3. Thomas AJ, Kalaria RN, O'Brien JT. Depression and vascular disease: what is the relationship? J Affect Disord. (2004) 79:81–95. doi: 10.1016/S0165-0327(02)00349-X
4. Kuller LH, Longstreth WT Jr, Arnold AM, Bernick C, Bryan RN, Beauchamp NJ Jr, et al. White matter hyperintensity on cranial magnetic resonance imaging: a predictor of stroke. Stroke J Cereb Circul. (2004) 35:1821–5. doi: 10.1161/01.STR.0000132193.35955.69
5. Bots ML, van Swieten JC, Breteler MM, de Jong PT, van Gijn J, Hofman A, et al. Cerebral white matter lesions and atherosclerosis in the rotterdam study. Lancet. (1993) 341:1232–7.
6. Pico F, Dufouil C, Levy C, Besancon V, de Kersaint-Gilly A, Bonithon-Kopp C, et al. Longitudinal study of carotid atherosclerosis and white matter hyperintensities: the EVA-MRI cohort. Cerebrovasc Dis. (2002) 14:109–15. doi: 10.1159/000064741
7. Chutinet A, Biffi A, Kanakis A, Fitzpatrick KM, Furie KL, Rost NS. Severity of leukoaraiosis in large vessel atherosclerotic disease. AJNR Am J Neuroradiol. (2012) 33:1591–5. doi: 10.3174/ajnr.A3015
8. Park JH, Kwon HM, Lee J, Kim DS, Ovbiagele B. Association of intracranial atherosclerotic stenosis with severity of white matter hyperintensities. Eur J Neurol. (2015) 22:44–52.e2-3. doi: 10.1111/ene.12431
9. Leng X, Wong LKS, Soo Y, Leung T, Zou X, Wang Y, et al. Signal intensity ratio as a novel measure of hemodynamic significance for intracranial atherosclerosis. Int J Stroke. (2013) 8:E46. doi: 10.1111/ijs.12080
10. Leng X, Wong KS, Soo Y, Leung T, Zou X, Wang Y, et al. Magnetic resonance angiography signal intensity as a marker of hemodynamic impairment in intracranial arterial stenosis. PLoS ONE. (2013) 8:e80124. doi: 10.1371/journal.pone.0080124
11. Liebeskind DS, Kosinski AS, Lynn MJ, Scalzo F, Fong AK, Fariborz P, et al. Noninvasive fractional flow on mra predicts stroke risk of intracranial stenosis. J Neuroimaging. (2015) 25:87–91. doi: 10.1111/jon.12101
12. Lan L, Leng X, Abrigo J, Fang H, Ip VH, Soo YO, et al. Diminished signal intensities distal to intracranial arterial stenosis on time-of-flight MR angiography might indicate delayed cerebral perfusion. Cerebrovasc Dis. (2016) 42:232–9. doi: 10.1159/000445842
13. Wang Y, Zhao X, Liu L, Soo YO, Pu Y, Pan Y, et al. Prevalence and outcomes of symptomatic intracranial large artery stenoses and occlusions in China: the Chinese intracranial atherosclerosis (CICAS) study. Stroke J Cereb Circul. (2014) 45:663–9. doi: 10.1161/strokeaha.113.003508
14. Pu Y, Liu L, Wang Y, Zou X, Pan Y, Soo Y, et al. Geographic and sex difference in the distribution of intracranial atherosclerosis in China. Stroke. (2013) 44:2109–14. doi: 10.1161/strokeaha.113.001522
15. Samuels OB, Joseph GJ, Lynn MJ, Smith HA, Chimowitz MZ. A standardized method for measuring intracranial1 arterial stenosis. Am J Neuroradiol. (2000) 21:643–6.
16. Leng X, Ip H, Soo Y, Leung T, Liu L, Feldmann E. Interobserver reproducibility of signal intensity ratio on magnetic resonance angiography for hemodynamic impact of intracranial atherosclerosis. J Stroke Cerebrovasc Dis. (2013) 22:e615–e9. doi: 10.1016/j.jstrokecerebrovasdis.2013.07.036
17. Wahlund LO, Barkhof F, Fazekas F, Bronge L, Augustin M, Sjogren M, et al. A new rating scale for age-related white matter changes applicable to MRI and CT. Stroke. (2001) 32:1318–22. doi: 10.1161/01.str.32.6.1318
18. Xiong Y, Yang J, Wong A, Wong CH, Chan SS, Li HH, et al. Operational definitions improve reliability of the age-related white matter changes scale. Eur J Neurol. (2011) 18:744–9. doi: 10.1111/j.1468-1331.2010.03272.x
19. Appelman AP, van der Graaf Y, Vincken KL, Tiehuis AM, Witkamp TD, Mali WP, et al. Total cerebral blood flow, white matter lesions and brain atrophy: the SMART-MR study. J Cereb Blood Flow Metab. (2008) 28:633–9. doi: 10.1038/sj.jcbfm.9600563
20. Vernooij MW, van der Lugt A, Ikram MA, Wielopolski PA, Vrooman HA, Hofman A, et al. Total cerebral blood flow and total brain perfusion in the general population: the rotterdam scan study. J Cereb Blood Flow Metab. (2008) 28:412–9. doi: 10.1038/sj.jcbfm.9600526
21. Appelman AP, Exalto LG, van der Graaf Y, Biessels GJ, Mali WP, Geerlings MI. White matter lesions and brain atrophy: more than shared risk factors? A systematic review. Cerebrovasc Dis. (2009) 28:227–42. doi: 10.1159/000226774
22. Moody DM, Bell MA, Challa VR. Features of the cerebral vascular pattern that predict vulnerability to perfusion or oxygenation deficiency: an anatomic study. AJNR Am J Neuroradiol. (1990) 11:431–9.
23. Mayer PL, Kier EL. The controversy of the periventricular white matter circulation: a review of the anatomic literature. AJNR Am J Neuroradiol. (1991) 12:223–8.
24. Pantoni L. Pathophysiology of age-related cerebral white matter changes. Cerebrovasc Dis. (2002) 13:7–10. doi: 10.1159/000049143
25. Lin W, Xiong L, Han J, Leung TW, Soo YO, Chen X, et al. External counterpulsation augments blood pressure and cerebral flow velocities in ischemic stroke patients with cerebral intracranial large artery occlusive disease. Stroke. (2012) 43:3007–11. doi: 10.1161/STROKEAHA.112.659144
26. Xiong L, Lin W, Han J, Chen X, Leung T, Soo Y, et al. Enhancing cerebral perfusion with external counterpulsation after ischaemic stroke: how long does it last? J Neurol Neurosurg Psychiatry. (2016) 87:531–6. doi: 10.1136/jnnp-2014-309842
Keywords: ischemic stroke, intracranial atherosclerosis, magnetic resonance angiography, imaging, white matter changes
Citation: Fang H, Leng X, Pu Y, Zou X, Pan Y, Song B, Soo YOY, Leung TWH, Wang C, Zhao X, Wang Y, Wang Y, Wong KS, Liu L and Xu Y (2020) Hemodynamic Significance of Middle Cerebral Artery Stenosis Associated With the Severity of Ipsilateral White Matter Changes. Front. Neurol. 11:214. doi: 10.3389/fneur.2020.00214
Received: 11 December 2019; Accepted: 09 March 2020;
Published: 15 April 2020.
Edited by:
Daniel Behme, University Medical Center Göttingen, GermanyReviewed by:
Maurice Giroud, Centre Hospitalier Regional Universitaire De Dijon, FranceCopyright © 2020 Fang, Leng, Pu, Zou, Pan, Song, Soo, Leung, Wang, Zhao, Wang, Wang,Wong, Liu and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liping Liu, bGlwaW5nc2lzdGVyQGdtYWlsLmNvbQ==; Yuming Xu, eHV5dW1pbmdAenp1LmVkdS5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.