
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 10 March 2020
Sec. Epilepsy
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.00144
This article is part of the Research Topic Cognitive and Psychiatric Comorbidities in Epilepsy: Insights from Neuroimaging Research View all 12 articles
 Corey Ratcliffe1,2
Corey Ratcliffe1,2 Britta Wandschneider1,2
Britta Wandschneider1,2 Sallie Baxendale1,2
Sallie Baxendale1,2 Pamela Thompson1,2Matthias J. Koepp1,2
Pamela Thompson1,2Matthias J. Koepp1,2 Lorenzo Caciagli1,2,3*
Lorenzo Caciagli1,2,3*Genetic generalized epilepsies (GGE), previously called idiopathic generalized epilepsies, constitute about 20% of all epilepsies, and include childhood absence epilepsy, juvenile absence epilepsy, juvenile myoclonic epilepsy, and epilepsy with generalized tonic-clonic seizures alone (CAE, JAE, JME, and GGE-GTCS, respectively). GGE are characterized by high heritability, likely underlain by polygenetic mechanisms, which may relate to atypical neurodevelopmental trajectories. Age of onset ranges from pre-school years, for CAE, to early adulthood for GGE-GTCS. Traditionally, GGE have been considered benign, a belief contrary to evidence from neuropsychology studies conducted over the last two decades. In JME, deficits in executive and social functioning are common findings and relate to impaired frontal lobe function. Studies using neuropsychological measures and cognitive imaging paradigms provide evidence for hyperconnectivity between prefrontal and motor cortices, aberrant fronto-thalamo-cortical connectivity, and reduced fronto-cortical and subcortical gray matter volumes, which are associated with altered cognitive performance. Recent research has also identified associations between abnormal hippocampal morphometry and fronto-temporal activation during episodic memory. Longitudinal studies on individuals with newly diagnosed JME have observed cortical dysmaturation, which is paralleled by delayed cognitive development compared to the patients' peers. Comorbidities and cognitive deficits observed in other GGE subtypes, such as visuo-spatial and language deficits in both CAE and JAE, have also been correlated with atypical neurodevelopment. Although it remains unclear whether cognitive impairment profiles differ amongst GGE subtypes, effects may become more pronounced with disease duration, particularly in absence epilepsies. Finally, there is substantial evidence that patients with JME and their unaffected siblings share patterns of cognitive deficits, which is indicative of an underlying genetic etiology (endophenotype), independent of seizures and anti-epileptic medication.
Genetic generalized epilepsies (GGE) are a group of generalized epilepsy syndromes underpinned by high heritability and complex polygenetic inheritance (1, 2). Though GGE have traditionally been regarded as benign, recent research indicates specific profiles of cognitive impairment (3–5), particularly encompassing functions reliant on frontal lobe processing. Potential underlying mechanisms of cognitive dysfunction have been elucidated via advanced neuroimaging techniques, which allow quantifying morphological and functional brain changes as well as their relation to neuropsychological test scores.
The etiology of cognitive impairment in GGE is often regarded as neurodevelopmental (6, 7). Recent research has focused on profiling first-order relatives alongside index patients, in an effort to characterize the cognitive phenotypes of GGE subgroups while identifying familial traits with likely genetic underpinnings. General linear models, on the other hand, have been used to assess the relationship between cognitive impairment and disease-associated variables, including age at onset, duration of epilepsy, or the influence of specific anti-epileptic medication.
Relatively recent reviews have detailed the cognitive profiles of mixed GGE samples (4) or individual GGE syndromes, particularly JME (3), providing evidence of frontal lobe dysfunction. However, there is a scarcity of work focusing on potential syndrome-specific patterns of impairment, attempting to characterize the neural correlates of dyscognitive traits, or identifying potential determinants of such abnormalities. An updated view on these topics is therefore timely and compelling. Improved knowledge may aid clinical practice, by highlighting the extent of interventional needs, informing patient counseling, and identifying targets for cognitive rehabilitation and novel therapeutic approaches.
In this review, we will first summarize evidence on the overarching cognitive profile of GGE. We will then detail subsyndrome-specific investigations, which suggest slightly distinct patterns of dysfunction in juvenile myoclonic epilepsy and absence epilepsies. We will also elucidate recent structural and functional imaging research, which shed light on the putative abnormalities underlying cognitive dysfunction. Finally, we will discuss investigations assessing patients and their first-order relatives, which indicate genetic underpinnings as relevant determinants of cognitive profiles in GGE.
For this review, we conducted a literature search on PubMed ranging from January 1, 1985 to June 30, 2019, querying the following terms and related synonyms: “genetic generalized epilepsy,” “idiopathic generalized epilepsy,” “childhood absence epilepsy,” “juvenile absence epilepsy,” “absence epilepsy,” “juvenile myoclonic epilepsy”, in combination with the following individual key terms: “neuropsychology,” “neuropsychological,” “cognition,” “cognitive test,” “MRI,” “functional MRI/fMRI,” “family study,” “relatives,” “siblings,” “intermediate phenotype,” “endophenotype”. Searches were also repeated using common abbreviations of disease names (i.e., “IGE,” “GGE,” “CAE,” “JAE,” “JME”). We restricted our initial search to articles published in English. In addition, we carried out manual searches on reference lists of the identified articles and selected review papers published in the last 5 years, and complemented the former with extraction of relevant manuscripts from our records. Final inclusion was based on originality and direct relevance to the topics discussed in this Review.
The investigations reviewed in this manuscript implemented a variety of neuropsychological tests addressing different cognitive functions. Here, we briefly detail the most commonly assessed cognitive abilities and associated neuropsychological tests, to aid the interpretation of findings across studies. A more in-depth description of frequently used tests, parsed by cognitive domain, is provided in Table 1.
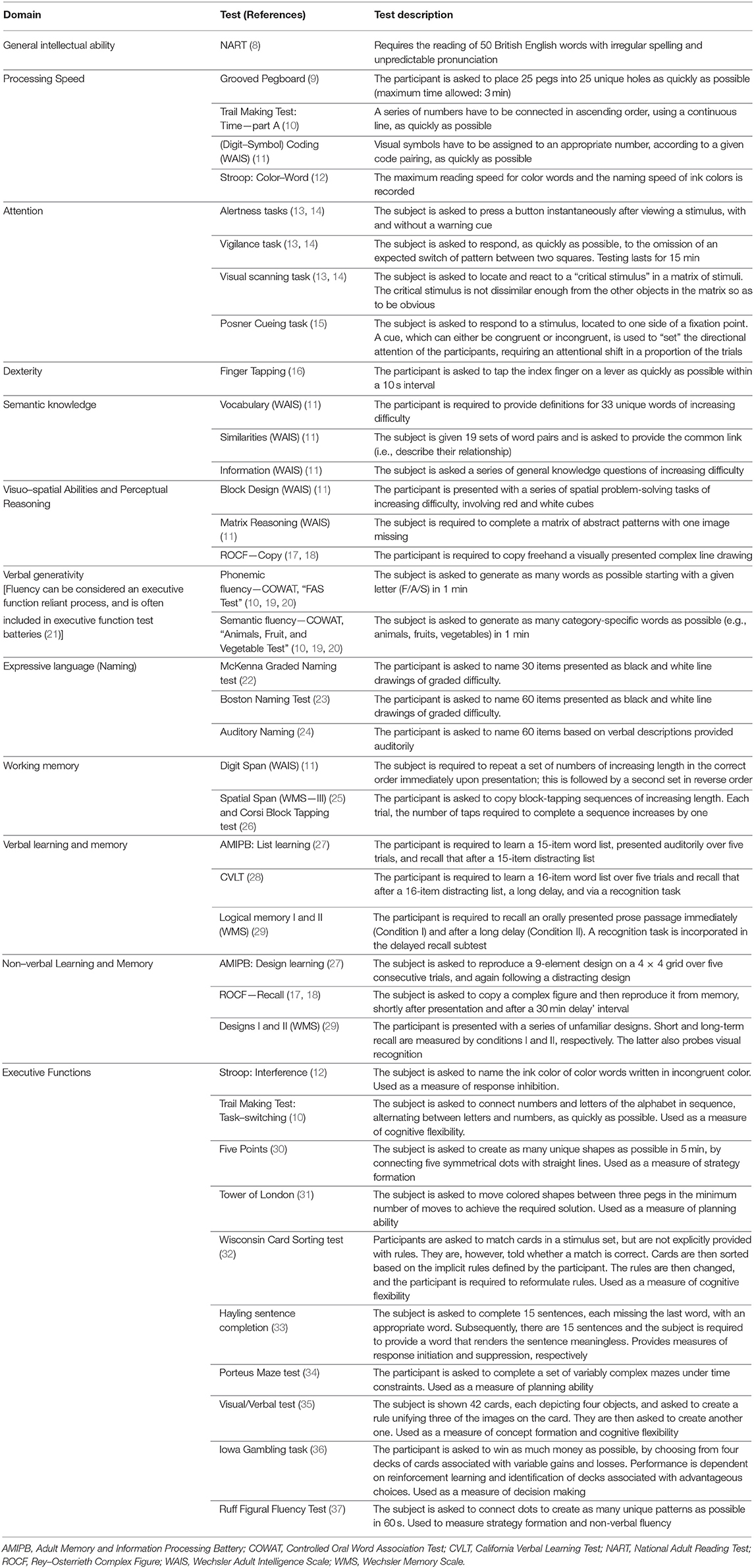
Table 1. Cognitive tests employed in GGE studies.
General cognitive ability, often denoted by g or intelligence quotient (IQ), broadly refers to the ability of an individual to solve problems across multiple domains, independent of educational level (38). Full-scale IQ scores are formally derived after completion of a set of tests included in the Wechsler Intelligence Scale, currently in its fourth edition [WAIS-IV; (11)]. Abbreviated assessments, such as the National Adult Reading Test for British English speakers (8), are also available. The latter tests provide IQ estimates based on an individual's ability of reading words with irregular spelling, thus probing vocabulary, and produce scores that are highly correlated with IQ measures obtained via the Wechsler Scale.
Processing speed, defined as the maximum speed at which elementary cognitive operations can be executed (39, 40), involves efficient allocation of processing resources and tracking of ongoing tasks, and relies on intact attention and visuo-spatial skills. Frequently employed processing speed tasks include the Trail Making Test-A (10), requiring an individual to connect numbers in ascending order with a continuous line, or the Grooved Pegboard test (9), assessing an individual's ability to match pegs to unique holes. Attention, defined as the cognitive process enabling selective focus on specific stimuli while ignoring other perceivable information, is assessed via standardized test batteries (13, 14) quantifying levels of alertness, vigilance, visual scanning, cueing and ability to simultaneously concentrate on different tasks. While also relying on visuo-spatial abilities, intact attention represents a prerequisite for optimal executive control (41).
Other frequently administered tests, such as the Rey-Osterrieth Complex Figure test [ROCF; (17, 18)], include an initial “Copy” condition that entails an accurate reproduction of a visually presented complex line drawing, and thus assesses visuo-spatial constructional abilities. More generally, visuo-spatial processing is common to a multiplicity of cognitive domains, including perceptual reasoning, probed via WAIS subtests involving recognition of spatial relationships among items with increasing complexity (Block Design, Matrix Reasoning), and motor dexterity, which refers to fine motor skills and coordination. Tests addressing the latter rely on the correct execution of controlled sequential motor responses, such as those assessed via the Finger Tapping test (16).
With regards to language abilities, manipulation of acquired verbal information is often subsumed under the term of semantic knowledge, and is assessed via WAIS subtests including “Vocabulary,” “Similarities” and “Information,” which collectively probe general verbal knowledge attained through education and environmental exposure. Tests assessing auditory and visual confrontation naming, on the other hand, require naming items from their auditory description or from related black and white line drawings, respectively (22–24, 42). Verbal fluency, often categorized into phonemic and semantic fluency, refers to verbal generativity, and is probed via tests such as the Controlled Oral Word Association or “FAS” test, for the phonemic component, and animal naming for the semantic one (19, 20). These tasks require an individual to generate the largest possible number of words starting with a given letter, or to name as many items as possible belonging to a given category (i.e., animals, in most cases) in a specified time frame.
Working memory refers to the cognitive system responsible for the short-term storage of recently acquired information for manipulation and immediate use (43, 44), and is generally parsed into a verbal and a visuo-spatial component. Common working memory tests are represented by the Digit Span and Arithmetic tasks for verbal cues, included in the WAIS, and the Corsi Block-Tapping test (26), addressing visuo-spatial abilities. Tests such as the California Verbal Learning Test [CLVT; (28)], and the List Learning subtests of the Adult Memory and Information Processing Battery [AMIPB; (27)], assess the ability to encode and retain verbal cues, referred to as verbal learning and memory. Similar batteries are available for testing visuo-spatial learning and memory, such as the Design Learning subtest of the AMIPB or the recall phases of the ROCF, which require an individual to reproduce complex line drawings from memory. Similarly, measures of immediate and delayed verbal and visual learning and memory are also provided by the Wechsler Memory Scale [WMS; (29)].
A cognitive domain frequently included in the assessments of GGE, and closely related to information manipulation (45), is represented by executive functions, which encompass the high-order, top-down mental processes required to pay attention, concentrate, evaluate the efficacy of automatic responses and suppress “default,” stereotyped output when appropriate (41, 46). Response inhibition, concept formation, cognitive flexibility, goal selection, strategy usage, planning and monitoring are all examples of executive functions, and overall enable purposeful, self-serving and adaptive behavior. While language-based, verbal fluency tasks also require executive control, and are frequently included in test batteries addressing executive function (21). Traditionally, successful executive cognition relies on the integrity of the frontal lobes, particularly the prefrontal cortex, whose dorsolateral, ventrolateral and rostral subdivisions may exhibit some degree of functional specialization (47–50). There is a large variety of cognitive tests assessing dysexecutive traits, and the neuropsychological test batteries implemented by Wandschneider et al. (51), Moschetta and Valente (52), Jackson et al. (53), or Wandschneider et al. (54) may provide helpful examples.
GGE constitute about 20% of all epilepsies and are composed of four main subsyndromes: childhood absence epilepsy, juvenile absence epilepsy, juvenile myoclonic epilepsy, and epilepsy with generalized tonic-clonic seizures alone (CAE, JAE, JME, and GGE-GTCS respectively). Whilst varying with regard to age of onset, combination of different seizure types, EEG traits and disease courses, all GGE share a genetically determined multi-factorial etiology.
CAE, which presents with frequent typical absence seizures, has an age of onset which peaks at 6 to 8 years, an incidence of 0.7/100,000/year, and is twice as common in females as in males (55, 56). Age of onset for JAE peaks between 9 and 13. The syndrome is characterized by typical, though less frequent, absence seizures, often accompanied by generalized tonic clonic seizures (GTCS), and a similar distribution between males and females (57). Whilst CAE and JAE are two independent clinical entities, it is commonly surmised that these two disorders have highly overlapping etiology and pathological mechanisms. Consequently, the majority of investigations into their cognitive profiles have collapsed both diseases into the unitary category of absence epilepsy (AE). The hallmark of the most common GGE subsyndrome, JME, is represented by myoclonic jerks occurring in the morning. Most patients also suffer from GTCS and, more rarely, absence seizures. Disease onset peaks during adolescence and early adulthood, between 12 and 18 years of age (range: 5–25). JME likely represents 15–20% of all GGE cases, and is slightly more common in females (ratio of 3:2) (56, 58). Finally, GGE-GTCS has the most variable age of onset, generally ranging from the second to the fourth decade of life, and is believed to account for up to 15% of GGE, though prevalence estimates are often inconsistent (59).
Although GGE have traditionally been regarded as benign, studies have consistently shown that executive functioning in GGE may be impaired. This has been complemented by research documenting a higher prevalence of impulsive personality traits (60, 61), cluster B personality disorders (62, 63), impaired emotion recognition and social cognition (64–66), suboptimal academic performance (53), and poor long-term social outcome (67, 68), particularly in JME. Moreover, meta-analytical syntheses of neuropsychological investigations conducted over the last three decades suggest that profiles of cognitive impairment may exhibit some degree of syndrome specificity (4). Here, we will discuss investigations of cognitive function in mixed groups of GGE patients, followed by studies detailing cognitive profiles in the most common GGE subsyndromes, juvenile myoclonic epilepsy and absence epilepsy.
In mixed GGE samples, general cognitive ability is often reported as affected, with meta-analyses (4, 69) documenting IQ scores ranging from 0.5 to 1 standard deviation lower than controls, indicative of moderate to large effect sizes. However, whilst most investigations described lower general intelligence in GGE compared to controls, the IQ measures reported for GGE groups generally fall within the normal range, clustering around average values at the population level, i.e., between 90 and 110 (53, 70–73). Hence, it remains unclear whether general intellectual abilities in GGE may be lower than normative values, or whether differences between patient and control samples may arise, for instance, from the recruitment of high-performing, non-representative control cohorts across investigations.
Patients with GGE also exhibit reduced ability to manipulate acquired information, i.e., semantic knowledge. The recent meta-analysis by Loughman et al. (4) points to significantly lower scores in GGE compared to controls on tests such as the Vocabulary and Information items of the WAIS. In parallel, the latter meta-analytical synthesis also indicated impaired problem solving and reasoning abilities, elsewhere referred to as fluid intelligence. Two reports also documented poorer performance on standardized arithmetic tests, assessing both knowledge of mathematical operations and problem-solving skills, with scores of GGE patients up to one standard deviation lower than control subjects (53). Rathouz et al. (72) found that scores of arithmetic subtests were lower in GGE than in patients with focal epilepsy, and that both groups performed worse than healthy controls.
Across studies, there is homogenous reporting of worse dexterity, attention and processing speed in GGE, with all studies documenting moderate to substantial impairment in patients (53, 73–77). While evidence for disrupted motor and cognitive processing speed is consistent, and may point to altered visuo-motor integration, more research is required to address its potential determinants, particularly in regard to the detrimental influence of anti-epileptic medication. As several of these have been associated with cognitive slowing (78–80), the extent to which abnormal processing speed may thus represent an intrinsic feature of GGE, rather than a medication-associated effect, remains unestablished.
A smaller number of investigations indicate that phonological processing may also be impaired in GGE, with scores for letter and category fluency falling about one standard deviation below population-level normative ranges (60, 71, 74, 77). Jackson et al. (53) found that reading and measures of vocabulary did not differ between controls and patients with GGE, but reported a selective phonemic fluency deficit in the latter. More abundant evidence of abnormal verbal generativity, however, has been conveyed by investigations separately assessing individual GGE syndromes.
Evidence for working memory impairment is conflicting. Whilst some studies found significant deficits in mixed GGE groups compared to controls (60, 71, 74), other studies did not (53, 73, 81, 82). One investigation (74) detected differences between patients and controls for non-verbal attention performance, but no specific working memory dysfunction. Deficits in working memory are reported more often for the verbal (74) than for the non-verbal domain, suggesting greater compromise of the phonological loop than the visuo-spatial sketchpad, which refers to the subsidiary working memory construct accounting for visuo-spatial processing (44). Similarly, there is less concordant evidence for learning and memory impairment in GGE. While some authors suggest moderate to large effect sizes (74, 76, 82, 83), particularly for long-term memory in pediatric cohorts, other studies did not detect significant differences (81, 84), and confidence intervals of effect estimates appear fairly wide across all investigations (4). While these findings may point to syndromic heterogeneity, and warrant further consideration in the context of individual GGE syndromes, it overall appears that memory deficits may not be a specific GGE trait.
Finally, widely-documented impairment of both verbal and non-verbal fluency, strategy formation (73, 77), attention (53, 71), response inhibition (72), concept formation and mental flexibility (4) indicates moderate to pronounced executive dysfunction in GGE, pointing to abnormal frontal lobe function.
In summary, the available evidence in GGE conveys a cognitive profile characterized by average general intelligence along with consistent impairment of processing speed, dexterity, verbal generativity, and executive function. Literature supporting weak semantic knowledge, problem-solving and visuo-spatial reasoning is also available, though less abundant, whilst findings pertaining to working memory, learning and long-term memory performance are conflicting.
An overview of the studies assessing the cognitive profile of JME is provided in Table 2. General intellectual abilities are consistently found to be within the average range, though slightly lower than in controls (53, 73, 88–90, 94, 99). As discussed in section Cognition in Mixed GGE Samples, it is possible that differences in general intelligence between JME and controls may be partially ascribed to the investigation of high-performing control cohorts.
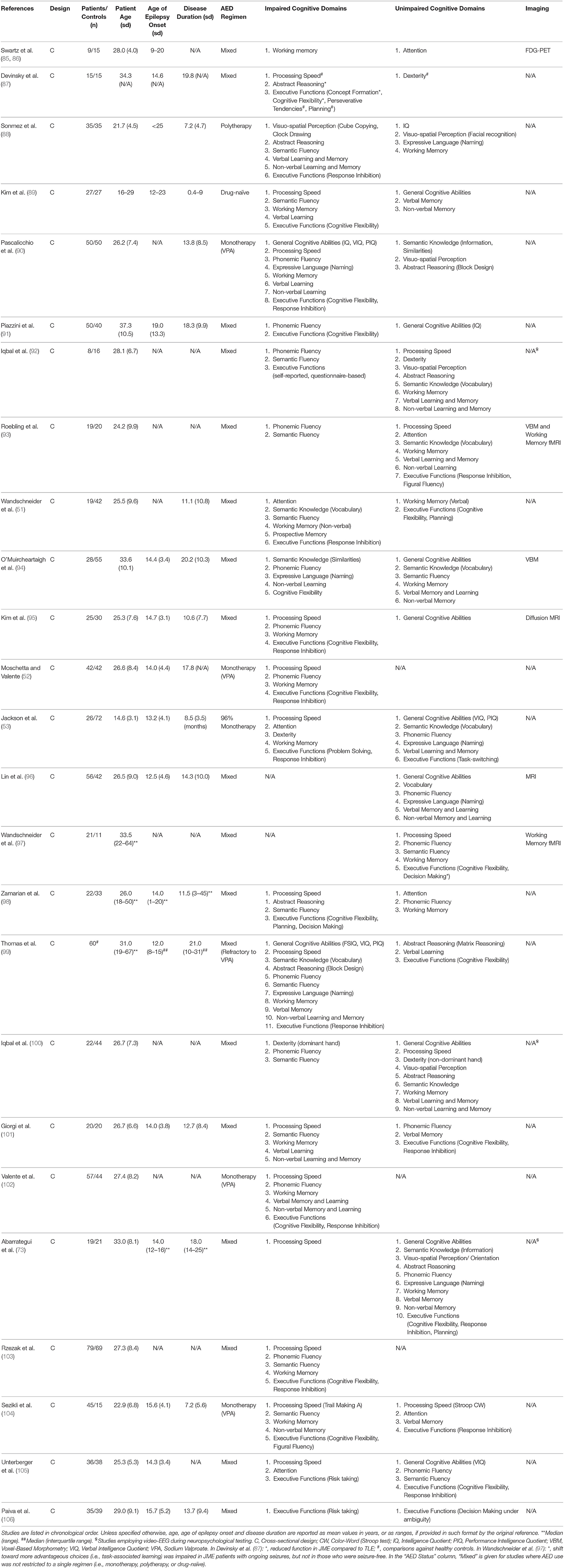
Table 2. Studies investigating cognitive function in JME.
Across studies summarized in the meta-analysis by Loughman et al. (4), there is evidence for consistent impairment of semantic knowledge and problem-solving skills, which recapitulates findings in mixed GGE samples. With regards to visuo-spatial abilities, visual attention has also been reported as impaired in JME (89, 90, 100, 104). While a meta-analytical synthesis (4) and more recent evidence (73, 104) suggested, on the other hand, that visuo-spatial thinking may be relatively intact, other findings (88) implicated minor visuo-spatial dysfunction, as assessed via clock drawing and cube copying tests. In line with evidence in mixed GGE samples, a number of studies documented impaired dexterity and processing speed (53, 73, 87, 90, 99, 100, 104, 105), with patients often performing more than one standard deviation below controls.
In relation to phonological processing, impairment of phonemic and semantic fluency was detailed in early investigations (88, 90) and confirmed by a large number of subsequent studies. Performance levels ranging between 0.5 and 1 standard deviation lower than controls have been reported by most investigations, indicative of moderate to consistent dysfunction (51, 91–95, 99, 100, 104). Medication-related effects might be involved, but have not yet been specifically addressed. Moschetta and Valente (52), for instance, highlighted an association between sodium valproate usage and worse performance on several cognitive tasks, including those assessing verbal fluency. As patients taking higher doses of valproate had a higher seizure frequency, however, it remains unclear whether worse executive performance may relate to epilepsy severity, anti-epileptic medication, or both the former. Information regarding treatment with topiramate, a drug commonly associated with adverse cognitive effects (107), was also lacking in several of the above investigations.
Most studies into working memory in JME reported some degree of impairment (90, 95, 99, 101). Other groups have examined dimension-specific performance, with some finding evidence for visuospatial impairment (51, 85, 86, 94, 101), and others documenting deficits in verbal working memory (52, 89, 101). While only few reports documented normal functioning (93, 100), whether working memory weaknesses may be more prominent in the verbal than non-verbal domain remains unclear.
Dysexecutive traits are very commonly described for JME, and may represent its hallmark. The typical profile encompasses impairment of response inhibition (51, 53, 90, 95, 99, 102), attention, goal maintenance, concept building, problem solving, task-switching, and cognitive flexibility (52, 53, 87, 89, 91, 94, 104). Two studies attempted within-groups stratification of effects, documenting moderate to severe deficits in executive functions in 83% and 68% of the respective samples (52, 99). Of note, however, Thomas et al. (99) explicitly focused on difficult-to-treat patients with JME, who had not experienced seizure freedom with sodium valproate. It is also reported that JME patients may experience more “everyday life problems” as a result of dysexecutive traits (92, 100). Decision-making, another high-level executive function, also appears affected. Patients with JME may exhibit difficulties in making advantageous decisions under ambiguity (98), and commit to more risky choices than controls (105, 106). Interestingly, Wandschneider et al. (97) suggested that risky decision making may be particularly relevant in the patient subgroup with poorly controlled seizures, pointing toward an interplay between epilepsy severity and cognitive outcome.
Prospective memory, a system of creating, retaining, and implementing prior intentions and plans, is heavily reliant on executive functions, and has been evaluated via a complex multi-step task (51). At the intention formation stage, patients with JME developed more rudimentary plans than controls, suggesting impaired planning and cognitive flexibility. Furthermore, patients also completed significantly fewer tasks, suggestive of deficits in the executive component underlying prospective memory.
The involvement of cognitive functions reliant on temporal and hippocampal processes in the JME profile is uncertain. Several studies reported normal levels of functioning on tests of learning and memory (51, 53, 73, 93, 96, 100, 108), whereas others detailed deficits in short and long-term recall when compared to controls (4, 90, 99, 101). Impaired memory has been considered a consequence of impoverished visual and verbal learning (88, 89, 104). Conflicting evidence may be partially due to syndromic heterogeneity.
Some reports have suggested that heterogeneity of cognitive performance in JME may relate to compensatory strategies, dependent on general intelligence level (103). While it can be argued that higher IQ in a proportion of JME cases may relate to more effective strategy formation, enabling successful compensation and thus normative executive performance, the hypothesis of IQ as a protective factor for cognitive dysfunction in JME lacks strong empirical support. Moschetta et al. (52) previously reported that cognitive performance in most domains was lower in JME than controls even after co-varying for IQ, thus suggesting independence of effects.
On balance, studies investigating cognition in JME documented average general intelligence, which is however paralleled by impairment of verbal generativity, working memory and a wide range of executive functions, with moderate to large effect sizes. Semantic knowledge, reasoning, processing speed and dexterity also appear affected, while evidence regarding learning and memory deficits is conflicting. Finally, the literature is overall not supportive of impairment of visuo-spatial abilities.
Table 3 summarizes findings of the investigations assessing cognitive function in CAE and JAE, often subsumed under the unitary category of AE, as specified earlier. Seminal research from Pavone et al. (109) found that AE may present with a subtle lowering of IQ compared to controls, which is corroborated by a recent review and several investigations (5, 73, 113, 114). As for mixed GGE samples and JME, however, IQ values are generally reported as within average ranges for the majority of AE patients. It is suggested that general cognitive ability may negatively correlate with disease duration (110, 111).
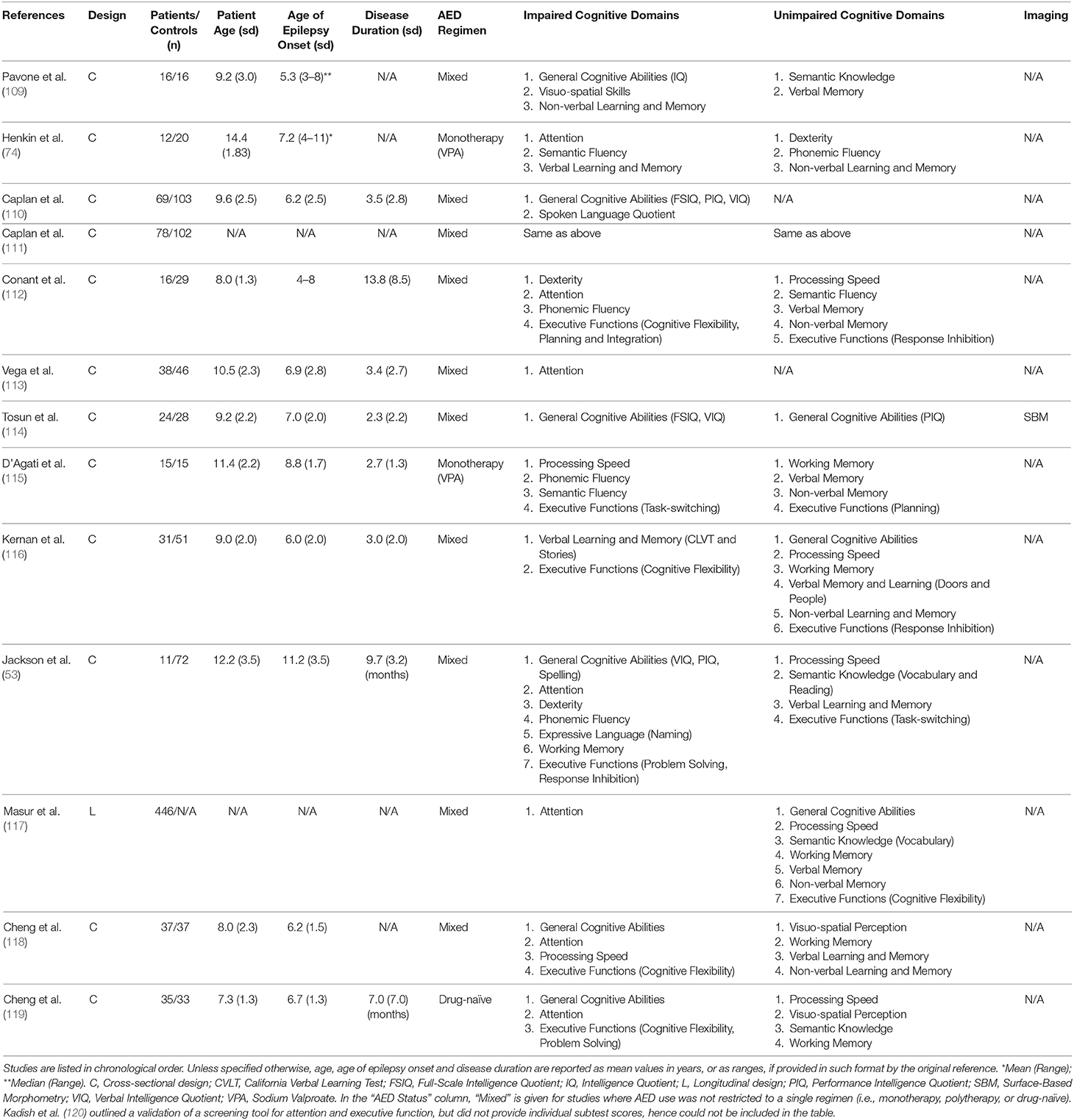
Table 3. Studies investigating cognitive function in AE.
Phonological processing represents one of the most frequently described domains of cognitive impairment in AE (5), and relates to reduced linguistic abilities, semantic knowledge, verbal intelligence quotient [VIQ; (53)] and spoken language quotient [SLQ; (110)]. Decline in several aspects of linguistic functioning may be associated with disease duration (111). Alongside expressive naming (53, 74, 116), both semantic and phonemic fluency have been found as weak in AE, with performances falling one standard deviation below those of normative controls (112, 115).
Early reports also documented impoverished performance on tests of visuo-spatial skills in AE, as measured by the Performance IQ (PIQ) component of the WISC-R (53, 109). This was associated with relatively poor scores on tests of dexterity (53, 74, 112) and processing speed (112, 115). Abstract visuo-spatial reasoning and line orientation may also be poorer in AE patients than controls (73). Most research has not found evidence for working memory deficits in AE, though a recent study suggest impairment of its visuo-spatial component (73). It is possible that this finding may be a consequence of more general disruptions in visuo-spatial processing.
As a distinguishing feature of AE, several studies reported impairment of attentional control, affecting both verbal and non-verbal modalities (73, 74, 112, 115–118, 120). In the largest investigation to date, involving over 400 individuals with newly diagnosed, drug-naïve CAE, attentional deficits were reported in more than a third of probands despite average intelligence, and persisted 16–20 weeks after treatment initiation, even when successful seizure control was attained (117). Moreover, causal modeling indicated downstream sequential effects of attentional deficits on memory, executive function and academic achievement (117), corroborating early reports that proposed impaired attention as the underlying mechanism for poor memory performance (109). Reduced attentional skills were elsewhere found associated with higher levels of distractibility and forgetfulness (113) and lower arithmetic proficiency (119).
Though impaired attention is the predominant finding in AE, dysexecutive traits are also reported in AE samples, in accord with typical findings in GGE, and include reduced scores for measures of problem-solving, response inhibition, processing speed, planning and mental flexibility (53, 112, 115, 118). Jackson et al. (53) indicated that impairment of attention and executive skills is clinically relevant, with performance of more than one standard deviation below normative levels in patients. We did not identify any investigation exploring decision-making or prospective memory in AE patients.
As in JME, evidence for impaired functions relying on mesiotemporal involvement in AE is controversial (5). Pavone et al. (109) reported abnormal non-verbal learning and memory, along with impaired delayed recall. Impoverished performance on standardized spelling tests has also been suggested as a potential indicator of altered long-term memory (53, 74, 116). Other studies, however, have found comparable performance on tests of learning and memory in patients and controls (73, 112, 115, 121). It is possible that learning and memory deficits may not be specific, and arise as a consequence of impaired phonological processing.
Lower IQ and impaired phonological ability in AE may be associated with anti-epileptic medication usage and disease duration. In the largest randomized controlled trial to date, sodium valproate appeared associated with significantly more frequent attentional deficits than ethosuximide and lamotrigine, independent of treatment response (117). Reduced FSIQ and PIQ appeared more prominent at a younger age and/or earlier age at disease onset than linguistic deficits, indicating a possible neurodevelopmental mechanism and differential modulatory effects of disease-related-variables (111). In a study considering cognitive dysfunction independently across GGE subsyndromes, Abarrategui et al. (73) posited that AE may present with the most severe cognitive impairment of all GGE, based on the assessment of a medicated cohort with a long disease duration (mean = 24.5 years). Other studies, however, report smaller effect sizes. On balance, it is maintained that inadequate seizure management relates to poor cognitive prognosis (68).
On balance, neuropsychological investigations in absence epilepsies also indicate average general intelligence, but principally substantiate impairment in two domains: phonological processing, which relates to most stages of language production and semantic knowledge, and attention, which represents the most commonly affected skill, and may in turn detrimentally affect executive function. Contrary to evidence in JME, however, there is a relative paucity of reports addressing high-level dysexecutive traits, and no evidence of altered decision making or risk-taking behavior. It remains to be established whether the latter traits may be specific to JME. Finally, while evidence for impaired verbal generativity is also widely documented for JME, its presence is mostly emphasized within the broader context of dysexecutive traits, rather than globally dysfunctional linguistic abilities. Future analyses directly comparing JME and AE across a test battery addressing language performance may shed further light on potential syndrome-specific cognitive features.
By ILAE definition, patients with GGE present with normal clinical MRI. Advanced post-processing methods such as voxel-based morphometry (122), surface-based MRI analysis (123), diffusion tensor imaging [DTI; (124)], and functional MRI have identified widespread structural and functional abnormalities in GGE, mostly implicating fronto-cortico-thalamic regions and their connections (125–133).
During the generalized spike-wave paroxysms typical of GGE, combined EEG-fMRI studies have documented the involvement of the thalamus and fronto-parietal cortices, mostly overlapping with default-mode network (DMN) areas (134–137). Overall, these findings have led to the conceptualization of GGE as disorders of thalamo-cortical connectivity. The diffuse abnormalities of cortical and subcortical structure, function, and connectivity in GGE may also relate to altered cognitive functioning, and most studies have investigated the neural correlates of cognitive function in separate GGE subsyndromes. Findings are summarized in Table 4.
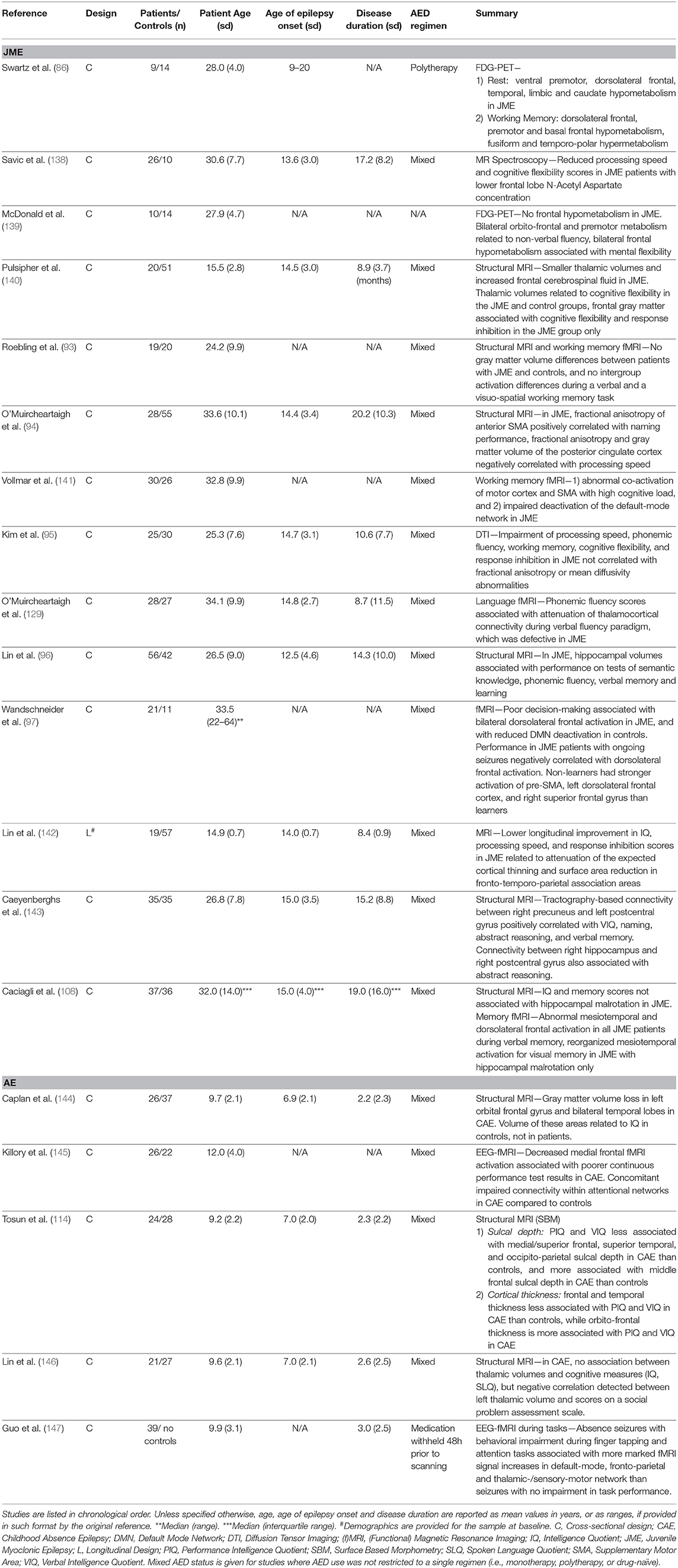
Table 4. Studies investigating imaging correlates of cognitive function in JME and AE.
In JME, early functional imaging studies aimed to identify the neural correlates of working memory and executive dysfunction. The first positron emission tomography (PET) investigation documented an association between impaired working memory performance in JME and reduced 18-fluorodeoxyglucose uptake within premotor, anterior frontal cortices and caudate nucleus (86). Subsequently, McDonald and collaborators detected an association between frontal PET hypometabolism and lower mental flexibility scores (139). In an MR-spectroscopy study, Savic and colleagues reported reduced frontal lobe N-Acetyl Aspartate (NAA) concentrations, a marker of neuronal damage or dysfunction, in JME patients (148). Low frontal NAA was more prominent in those with poorer performance on an abbreviated cognitive assessment addressing frontal lobe function (138). Collectively, these early investigations provided complementary evidence linking dysexecutive traits to markers of impaired frontal lobe function across imaging modalities.
Subsequent investigations assessed the neural underpinnings of cognitive function in JME using task-based fMRI. Initial reports did not detect activation differences between JME patients and controls during a working memory fMRI task, which included verbal and visuo-spatial modified versions of the Sternberg Item Recognition Test (93). More recently, however, Vollmar and collaborators identified abnormal motor co-activation and increased functional connectivity between motor system and prefrontal cognitive networks during a visuo-spatial working memory task, which entailed joystick usage (141). While not substantiating the pattern of “hypofrontality” suggested by early imaging work, these findings point instead to an altered interplay between functionally segregated brain networks, modulated by task complexity, and implicate a potential disruption of whole-brain functional network hierarchy. In keeping with evidence of enhanced structural connectivity between the cognitive pre-SMA and motor cortex (149), these results may also provide a mechanistic explanation of cognition-triggered myoclonus in JME, i.e., praxis induction (141, 150). During the same working memory fMRI task, increased activation of the left dorso-lateral frontal cortex, on the other hand, was detected in JME patients with poorer decision-making performance (97). The latter may be interpreted as a compensatory mechanism to adequately engage working memory networks, required to carry out a complex decision-making task, and is reminiscent of findings in other neuropsychiatric disorders, such as schizophrenia (151, 152).
Other investigations in JME attempted to link the putative substrates of ictogenesis, likely represented by fronto-thalamo-cortical circuitry (150), with the associated cognitive comorbidities. O'Muircheartaigh and collaborators (129) demonstrated aberrant fronto-cortico-thalamic connectivity in JME during a verbal fluency fMRI task, which was associated with impoverished fluency performance. Complementary evidence was provided by a structural imaging analysis in recent-onset JME, which detected an association between performance on executive function tests and both thalamic and frontal volumes (140). On balance, this work suggests that the same circuitry accounting for seizure generation in JME may also mediate impairment of executive skills.
Other analyses sought to identify the neural correlates of cognitive traits in JME via structural imaging methods. Altered microstructural integrity of the supplementary motor area was associated with reduced performance on an expressive language task, while both gray matter volume and microstructural integrity of the posterior cingulate cortex related to mental flexibility (94). In a diffusion MRI tractography analysis, connectivity between post-central gyrus and precuneus was positively associated with verbal IQ, expressive language as well as verbal memory scores (143). Other studies, however, reported no correlations between white matter markers and a wide range of neuropsychological test scores, most of which relating to frontal lobe functions (95). While implicating midline frontal, primary sensory and parietal regions, structural imaging findings provide a less cohesive picture, as opposed to the more concordant evidence garnered via functional imaging studies.
Longitudinal investigations in new-onset JME may offer a window into the developmental trajectories of cognitive comorbidities. Lin et al. (142) documented lower response inhibition and psychomotor speed in patients with JME compared to controls at baseline, accompanied by persistence of intergroup differences after a 2 year follow-up, and more limited increase of general intelligence scores in the JME group. The latter cognitive traits were paralleled by structural abnormalities of high-order fronto-temporo-parietal association cortices, as demonstrated by an attenuation of the expected cortical thinning and contraction of surface areas. These findings overall implicate disrupted cortical maturation, and point to a post-migrational neurodevelopmental mechanism (142). Interestingly, further support to the neurodevelopmental hypothesis comes from recent analyses, indicating increased cortical folding complexity and inefficient cortico-cortical connectivity of orbitofrontal, ventrolateral frontal, premotor and temporo-polar areas. The latter regions also displayed abnormal cognitive network embedding, with fronto-parietal, dorsal attention and limbic cognitive systems being most affected (132).
Finally, a recent multi-modal imaging investigation in JME focused on the mesiotemporal lobe. Structural morphometric analyses indicated anomalies of hippocampal shape and positioning, pointing to altered mesiotemporal neurodevelopment during the prenatal stages, which related to reduced memory-related activation of both hippocampus and dorsolateral frontal areas (108). This work thus substantiates morphometric and functional abnormalities in JME extending beyond the classically involved fronto-cortico-thalamic or fronto-parietal systems, and supports functional relevance of mesiotemporal structural alterations, which reverberate on a fronto-temporal network subserving episodic memory.
As opposed to evidence in JME, direct assessments of the imaging correlates of cognitive function in AE are less numerous. Orbito-frontal and temporal lobe gray matter volumes were described as diminished in CAE (144), though formal correlations between the latter imaging measures and IQ scores were statistically significant in controls only. An investigation relating cortical thickness and sulcal depth to verbal and performance IQ found differential patterns of association between cognitive and structural measures in CAE compared to controls. Effects were particularly prominent for thickness and sulcal depth of medial/superior frontal and superior temporal areas, and implicated a negative relation between the latter and verbal IQ, which was instead positive in typically developing controls (114). In CAE, however, the authors identified positive associations between intelligence measures and thickness of the orbitofrontal cortex as well as sulcal depth of the middle frontal gyrus. Overall, these findings indicate distinct patterns of morphological signatures associated with general cognitive abilities, which may result from disease-related plasticity and reorganization.
Subsequent investigations assessed subcortical structures, in light of increasing evidence suggesting thalamic involvement in the generation of seizures and interictal discharges (137, 153, 154). While one study identified smaller thalamic volumes in CAE compared to controls, it did not detect a significant association between the latter and IQ measures (146). In JAE, reductions of gray matter volume and surface area were detected in the frontal, cingulate, and mesiotemporal locations, but formal correlations with cognitive measures were not available (155).
Functional imaging investigations in AE principally addressed the neural correlates of attention. During a sustained attention paradigm, an association was detected between lower activation of the medial frontal cortex and impaired task performance in CAE, which co-existed with reduced resting-state connectivity within an attentional network encompassing anterior insula and medial frontal cortex (145). More recently, combined behavioral and EEG-fMRI investigations detailed an association between (a) entity of functional activity changes within default-mode, fronto-parietal task-positive and sensorimotor-thalamic networks, and (b) intensity of absence seizures and related behavioral impairment. These findings thus provide direct evidence of a relationship between seizure-related cognitive compromise and levels of activity within large-scale brain networks (147).
GGE are characterized by multi-factorial etiology and likely polygenetic underpinnings (156–158). A commonly held view regards GGE as heritable disorders of abnormal neurodevelopment, which may provide a unifying framework to understand vulnerability to seizure activity, distributed anomalies of functional and structural connectivity, as well as the associated cognitive and psychopathological comorbidities. Factors exerting additional modulation of the cognitive phenotype in GGE include disease-related variables, such as the combination of seizure types, seizure frequency and their responsiveness to treatment, disease duration, frequency of interictal epileptiform discharges, and specific effects of anti-epileptic medication (68, 107, 110).
Here, we will predominantly summarize research addressing genetic factors as determinants of cognitive impairment in GGE via family studies. Investigating neurobehavioral traits in first-order relatives of index cases provides the opportunity to account for potential effects of medication and seizures, whilst investigating individuals with comparable upbringing and socio-economic determinants. Common findings in patients and their relatives can be interpreted as intermediate phenotypes, or endophenotypes (159, 160) i.e., heritable traits co-segregating in affected families, underlying predisposition to disease and shedding light on its pathological mechanisms. Thus far, a few investigations have tested whether patterns of cognitive impairment in GGE may be heritable, and the majority of endophenotype research has focused on JME probands. While Levav et al. (121) detailed familial impairment in both JME and CAE samples, we are not aware of further subsyndrome-specific research in absence epilepsies or GGE-GTCS.
Levav et al. (121) demonstrated comparable deficits in attentional functioning for patients with GGE and their siblings relative to controls. More recently, Chowdhury et al. (71) showed that patients with GGE and first-degree relatives exhibited similar levels of impairment on tests of working memory, non-verbal reasoning, verbal fluency, and attention. In first-degree relatives, performances in the aforementioned domains mostly fell between patients and controls, suggesting a heritable component for cognitive impairment in GGE whilst implicating additional detrimental effects in patients, which may relate to a combination of seizures, anti-epileptic medication and/or greater genetic burden. In JME, two investigations described concomitant impairment of motor dexterity and phonemic fluency in probands and their siblings (92, 100). Semantic fluency and psychomotor speed also followed a similar trend, with relatives underperforming compared to controls. Interestingly, the familial similarities in cognitive performance were observed independent of abnormal interictal EEG in both studies. Furthermore, evidence suggests that JME probands and siblings both performed worse than controls during the memory formation and intention execution stages of a prospective memory task (51), which indicates heritability in relation to a complex cognitive skill, with tangible “everyday life” implications. Collectively, these investigations highlighted common neurobehavioural traits in patients and their unaffected siblings, mostly affecting executive function. Dyscognitive traits are thus implicated as a feature underpinned by genetic contribution, likely part of an extended disease-related phenotype, rather than mere consequence of seizure activity or anti-epileptic drug effects.
In parallel, recent imaging research complemented evidence on cognitive intermediate phenotypes. In patients with JME and their siblings, Wandschneider et al. (54) detected concomitant motor co-activation and abnormal connectivity between motor and prefrontal cognitive systems during a working-memory task, suggesting that altered interplay between functionally distinct macroscale networks may also be genetically driven. The previously detailed surface-based morphometry study, which investigated cortical folding complexity and cortico-cortical connectivity via a geodesic distance metric, identified concomitant abnormalities within high-order fronto-temporal cortices both in patients with JME and siblings. Similarly, abnormal embedding of the latter areas within large-scale cognitive networks, mostly affecting fronto-parietal, dorsal attention and limbic systems, was detected in both groups (132). Finally, recent work demonstrated co-segregation of abnormalities of hippocampal volume, shape and positioning both in patients with JME and their siblings, and showed their association with reorganization of both hippocampal and lateral frontal recruitment during a memory encoding functional MRI paradigm (108).
Collectively, these findings strongly indicate concomitant cognitive network abnormalities in patients with JME and their relatives, suggest involvement of cognitive domains beyond executive functions, and implicate high heritability.
There is substantial evidence that GGE present with widespread cognitive impairment, predominantly involving executive functions. Cognitive profiles may slightly diverge across GGE subsyndromes, with absence epilepsies mostly affected in regard to phonological processing and attention, while high-level dysexecutive and risk-taking traits may be more prominent in JME. Studies assessing the neural correlates of cognitive dysfunction are more abundant in JME, and have frequently implicated thalamo-fronto-cortical and motor to prefrontal connections. In AE, on the other hand, there is evidence for a relationship between abnormal fronto-cortical morphometry and IQ, and impaired attention is paralleled by altered activation and connectivity within fronto-insular attentional networks. Whilst the etiology of cognitive impairment in GGE is likely multi-factorial, assessments of first-degree relatives, mostly of JME index patients, support heritability of cognitive profiles and the associated neural underpinnings, which qualify as suitable intermediate phenotypes (endophenotypes). Further research is awaited to (1) characterize profiles of cognitive impairment in homogeneous JAE samples, instead of assessing those along with CAE cases, irrespective of syndromic distinction; (2) elucidate patterns of dysfunction in GGE-GTCS; and (3) advance our insights into the pathological mechanisms of cognitive abnormalities, which may entail longitudinal investigation of cognitive trajectories in patients and their relatives, and, ultimately, require analyses of multi-source datasets encompassing neuropsychology, neuroimaging, genetics and neurophysiology.
CR, BW, MK, and LC planned the manuscript. CR and LC wrote the manuscript and carried out the subsequent revisions. CR and LC prepared the supporting material. PT and SB assisted in the interpretation of cognitive test results. All the co-authors provided substantial contributions to the first manuscript draft and subsequent revised versions.
BW, MK, and LC acknowledged project support from the Wellcome Trust (Project Grant 079474) and a medical research grant from the Henry Smith Charity (ref 20133416). BW acknowledged previous support by a fellowship of the German Research Foundation (Deutsche Forschungs-gemeinschaft; WA 3135/1–1). LC was funded by a Berkeley Fellowship awarded by University College London and Gonville and Caius College, Cambridge, and acknowledged previous support from Brain Research UK. The funders had no role in study design, decision to publish, or preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Fisher RS, Cross JH, French JA, Higurashi N, Hirsch E, Jansen FE, et al. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. (2017) 58:522–30. doi: 10.1111/epi.13670
2. Scheffer IE, Berkovic S, Capovilla G, Connolly MB, French J, Guilhoto L, et al. ILAE classification of the epilepsies: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. (2017) 58:512–21. doi: 10.1111/epi.13709
3. Wandschneider B, Thompson PJ, Vollmar C, Koepp MJ. Frontal lobe function and structure in juvenile myoclonic epilepsy: a comprehensive review of neuropsychological and imaging data: cognition in Juvenile Myoclonic Epilepsy. Epilepsia. (2012) 53:2091–8. doi: 10.1111/epi.12003
4. Loughman A, Bowden SC, D'Souza W. Cognitive functioning in idiopathic generalised epilepsies: a systematic review and meta-analysis. Neurosci Biobehav Rev. (2014) 43:20–34. doi: 10.1016/j.neubiorev.2014.02.012
5. Verrotti A, Matricardi S, Rinaldi VE, Prezioso G, Coppola G. Neuropsychological impairment in childhood absence epilepsy: review of the literature. J Neurol Sci. (2015) 359:59–66. doi: 10.1016/j.jns.2015.10.035
6. Johnson MR, Shorvon SD. Heredity in epilepsy: neurodevelopment, comorbidity, and the neurological trait. Epilepsy Behav. (2011) 22:421–7. doi: 10.1016/j.yebeh.2011.07.031
7. Pulsipher DT, Dabbs K, Tuchsherer V, Sheth RD, Koehn MA, Hermann BP, et al. Thalamofrontal neurodevelopment in new-onset pediatric idiopathic generalized epilepsy. Neurology. (2011) 76:28–33. doi: 10.1212/WNL.0b013e318203e8f3
9. Roy EA, Square PA. Neuropsychology of movement sequencing disorders and apraxia. In: Zaidel D, editor. Neuropsychology. Amsterdam: Elsevier. (1994). p. 183–218. doi: 10.1016/B978-0-08-092668-1.50015-6
10. Tombaugh TN, Kozak J, Rees L. Normative data stratified by age and education for two measures of verbal fluency: FAS and animal naming. Arch Clin Neuropsychol. (1999) 14:167–77. doi: 10.1016/S0887-6177(97)00095-4
11. Wechsler D. Wechsler Adult Intelligence Scale, 4th ed (WAIS-IV). San Antonio, TX: Pearson (2008).
12. Homack S, Riccio C. A meta-analysis of the sensitivity and specificity of the Stroop Color and Word Test with children. Arch Clin Neuropsychol. (2004) 19:725–43. doi: 10.1016/j.acn.2003.09.003
13. Posner M, Rafal R. Cognitive theories of attention and the rehabilitation of attentional deficits. In: R. Meier, A. Benton, L. Diller, editors. Neuropsychological Rehabilitation (Edinburgh: Churchill Livingstone) (1987).
14. Zimmermann P, Fimm B. A test battery for attentional performance. In: Leclercq M, Zimmermann P, editors. Applied Neuropsychology of Attention: Theory, Diagnosis and Rehabilitation. New York, NY: Psychology Press (2002). p. 110–151.
15. Posner M, Inhoff A, Friedrich F, Cohen A. Isolating attentional systems: a cognitive-anatomical analysis. Psychobiology. (1987) 15:107–21.
16. Reitan RM, Wolfson D. The Halstead-Reitan Neuropsychological Test Battery: Theory and Clinical Interpretation, 2nd ed. Tucson, AZ: Neuropsychology Press (1993).
17. Osterrieth PA. Le test de copie d'une figure complex: contribution á l'étude de la perception et de la memoire. Arch Psychol. (1944) 30:286–350.
18. Shin M-S, Park S-Y, Park S-R, Seol S-H, Kwon JS. Clinical and empirical applications of the Rey–Osterrieth Complex Figure Test. Nat Protoc. (2006) 1:892–9. doi: 10.1038/nprot.2006.115
19. Benton AL, Hamsher KD, Sivan AB. Multilingual Aphasia Examination, 2nd ed. Iowa City, IA: AJA Associates (1989).
20. Bird CM, Papadopoulou K, Ricciardelli P, Rossor MN, Cipolotti L. Monitoring cognitive changes: psychometric properties of six cognitive tests. Br J Clin Psychol. (2004) 43:197–210. doi: 10.1348/014466504323088051
21. Shao Z, Janse E, Visser K, Meyer AS. What do verbal fluency tasks measure? Predictors of verbal fluency performance in older adults. Front Psychol. (2014) 5:772. doi: 10.3389/fpsyg.2014.00772
24. Hamberger MJ, Seidel WT. Auditory and visual naming tests: normative and patient data for accuracy, response time, and tip-of-the-tongue. J Int Neuropsychol Soc. (2003) 9:479–89. doi: 10.1017/S135561770393013X
25. Tulsky DS, Chiaravalloti ND, Palmer BW, Chelune GJ. The wechsler memory scale, 3rd ed. In: Ledbetter M, editor. Clinical Interpretation of the WAIS-III and WMS-III. Amsterdam: Elsevier. (2003). p. 93–139. doi: 10.1016/B978-012703570-3/50007-9
26. Corsi P. Memory and the medial temporal region of the brain. In Dissertation Abstracts International. Montreal: McGill. (1972). 34(2-B):891.
27. Coughlan AK, Hollows SE. The Adult Memory and Information Processing Battery (AMIPB): Test Manual. Leeds: A.K. Coughlin, Psychology Department, St James' Hospital (1985).
28. Delis DC, Kramer JH, Kaplan E, Ober BA. The California Verbal Learning Test: Research Edition, Adult Version. San Antonio, TX: The Psychological Corporation (1987).
30. Regard M, Strauss E, Knapp P. Children's production on verbal and non-verbal fluency tasks. Percept Mot Skills. (1982) 55:839–44. doi: 10.2466/pms.1982.55.3.839
31. Shallice T. Specific impairments of planning. Philos Trans R Soc Lond B Biol Sci. (1982) 298:199–209. doi: 10.1098/rstb.1982.0082
32. Grant DA, Berg E. A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigl-type card-sorting problem. J Exp Psychol. (1948) 38:404–11. doi: 10.1037/h0059831
33. Burgess P, Shallice T. The Hayling and Brixton Tests. Test Manual. Bury St Edmunds: Thames Valley Test Company (1997).
34. Cronbach LJ. The Porteus Maze test and intelligence. J Educ Psychol. (1950) 41:502–3. doi: 10.1037/h0050445
35. Feldman MJ, Drasgow J. A visual-verbal test for schizophrenia. Psychiatr Q Suppl. (1951) 25:55–64.
36. Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. (1994) 50:7–15. doi: 10.1016/0010-0277(94)90018-3
37. Ruff RM, Allen CC, Farrow CE, Niemann H, Wylie T. Figural fluency: differential impairment in patients with left versus right frontal lobe lesions. Arch Clin Neuropsychol. (1994) 9:41–55. doi: 10.1093/arclin/9.1.41
38. Devlin B, Daniels M, Roeder K. The heritability of IQ. Nature. (1997) 388:468–71. doi: 10.1038/41319
39. Kail R, Salthouse TA. Processing speed as a mental capacity. Acta Psychol. (1994) 86:199–225. doi: 10.1016/0001-6918(94)90003-5
40. Turken U, Whitfield-Gabrieli S, Bammer R, Baldo JV, Dronkers NF, Gabrieli JDE. Cognitive processing speed and the structure of white matter pathways: convergent evidence from normal variation and lesion studies. Neuroimage. (2008) 42:1032–44. doi: 10.1016/j.neuroimage.2008.03.057
41. Diamond A. Executive Functions. Annu Rev Psychol. (2013) 64:135–68. doi: 10.1146/annurev-psych-113011-143750
42. Trimmel K, van Graan AL, Caciagli L, Haag A, Koepp MJ, Thompson PJ, et al. Left temporal lobe language network connectivity in temporal lobe epilepsy. Brain. (2018) 141:2406–18. doi: 10.1093/brain/awy164
43. Baddeley A, Logie R. Working memory: the multiple-component model. In: Miyake A, Shah P, editors. Models of Working Memory: Mechanisms of Active Maintenance and Executive Control. Cambridge: Cambridge University Press. (1999). p. 28–61. doi: 10.1017/CBO9781139174909.005
45. Kane MJ, Engle RW. The role of prefrontal cortex in working-memory capacity, executive attention, and general fluid intelligence: an individual-differences perspective. Psychon Bull Rev. (2002) 9:637–71. doi: 10.3758/BF03196323
46. Gilbert SJ, Burgess PW. Executive function. Curr Biol. (2008) 18:R110–14. doi: 10.1016/j.cub.2007.12.014
47. Corbetta M, Shulman GL. Control of goal-directed and stimulus-driven attention in the brain. Nat Rev Neurosci. (2002) 3:201–15. doi: 10.1038/nrn755
48. Gilbert SJ, Spengler S, Simons JS, Steele JD, Lawrie SM, Frith CD, et al. Functional specialization within rostral prefrontal cortex (Area 10): a meta-analysis. J Cogn Neurosci. (2006) 18:932–48. doi: 10.1162/jocn.2006.18.6.932
49. Dosenbach NUF, Fair DA, Miezin FM, Cohen AL, Wenger KK, Dosenbach RAT, et al. Distinct brain networks for adaptive and stable task control in humans. Proc Natl Acad Sci USA. (2007) 104:11073–8. doi: 10.1073/pnas.0704320104
50. Szczepanski SM, Knight RT. Insights into human behavior from lesions to the prefrontal cortex. Neuron. (2014) 83:1002–18. doi: 10.1016/j.neuron.2014.08.011
51. Wandschneider B, Kopp UA, Kliegel M, Stephani U, Kurlemann G, Janz D, et al. Prospective memory in patients with juvenile myoclonic epilepsy and their healthy siblings. Neurology. (2010) 75:2161–7. doi: 10.1212/WNL.0b013e318202010a
52. Moschetta SP, Valente KD. Juvenile myoclonic epilepsy: the impact of clinical variables and psychiatric disorders on executive profile assessed with a comprehensive neuropsychological battery. Epilepsy Behav. (2012) 25:682–6. doi: 10.1016/j.yebeh.2012.10.002
53. Jackson DC, Dabbs K, Walker NM, Jones JE, Hsu DA, Stafstrom CE, et al. The neuropsychological and academic substrate of new/recent-onset epilepsies. J Pediatr. (2013) 162:1047–53.e1. doi: 10.1016/j.jpeds.2012.10.046
54. Wandschneider B, Centeno M, Vollmar C, Symms M, Thompson PJ, Duncan JS, et al. Motor co-activation in siblings of patients with juvenile myoclonic epilepsy: an imaging endophenotype? Brain. (2014) 137:2469–79. doi: 10.1093/brain/awu175
55. Berg AT, Shinnar S, Levy SR, Testa FM. Newly diagnosed epilepsy in children: presentation at diagnosis. Epilepsia. (1999) 40:445–52. doi: 10.1111/j.1528-1157.1999.tb00739.x
56. Jallon P, Latour P. Epidemiology of idiopathic generalized epilepsies. Epilepsia. (2005) 46:10–4. doi: 10.1111/j.1528-1167.2005.00309.x
57. Loiseau P, Duche B, Pedespan J-M. Absence epilepsies. Epilepsia. (1995) 36:1182–6. doi: 10.1111/j.1528-1157.1995.tb01060.x
58. Camfield CS, Striano P, Camfield PR. Epidemiology of juvenile myoclonic epilepsy. Epilepsy Behav. (2013) 28:S15–17. doi: 10.1016/j.yebeh.2012.06.024
59. Camfield P, Camfield C. Idiopathic generalized epilepsy with generalized tonic-clonic seizures (IGE-GTC): a population-based cohort with >20 year follow up for medical and social outcome. Epilepsy Behav. (2010) 18:61–3. doi: 10.1016/j.yebeh.2010.02.014
60. Shehata GA, Bateh AEM. Cognitive function, mood, behavioral aspects, and personality traits of adult males with idiopathic epilepsy. Epilepsy Behav. (2009) 14:121–4. doi: 10.1016/j.yebeh.2008.08.014
61. Moschetta S, Fiore LA, Fuentes D, Gois J, Valente KD. Personality traits in patients with juvenile myoclonic epilepsy. Epilepsy Behav. (2011) 21:473–7. doi: 10.1016/j.yebeh.2011.03.036
62. Gélisse P, Genton P, Samuelian JC, Thomas P, Bureau M. [Psychiatric disorders in juvenile myoclonic epilepsy]. Rev Neurol. (2001) 157:297–302.
63. de Araújo Filho GM, Pascalicchio TF, da Silva Sousa P, Lin K, Ferreira Guilhoto LMF, Yacubian EMT. Psychiatric disorders in juvenile myoclonic epilepsy: a controlled study of 100 patients. Epilepsy Behav. (2007) 10:437–41. doi: 10.1016/j.yebeh.2007.01.016
64. Jiang Y, Hu Y, Wang Y, Zhou N, Zhu L, Wang K. Empathy and emotion recognition in patients with idiopathic generalized epilepsy. Epilepsy Behav. (2014) 37:139–44. doi: 10.1016/j.yebeh.2014.06.005
65. Stewart E, Catroppa C, Gill D, Webster R, Lawson J, Mandalis A, et al. Theory of Mind and social competence in children and adolescents with genetic generalised epilepsy (GGE): relationships to epilepsy severity and anti-epileptic drugs. Seizure. (2018) 60:96–104. doi: 10.1016/j.seizure.2018.06.015
66. Guida M, Caciagli L, Cosottini M, Bonuccelli U, Fornai F, Giorgi FS. Social cognition in idiopathic generalized epilepsies and potential neuroanatomical correlates. Epilepsy Behav. 100(Pt B):106118. doi: 10.1016/j.yebeh.2019.01.003
67. Camfield CS, Camfield PR. Juvenile myoclonic epilepsy 25 years after seizure onset: a population-based study. Neurology. (2009) 73:1041–5. doi: 10.1212/WNL.0b013e3181b9c86f
68. Nickels KC, Zaccariello MJ, Hamiwka LD, Wirrell EC. Cognitive and neurodevelopmental comorbidities in paediatric epilepsy. Nat Rev Neurol. (2016) 12:465–76. doi: 10.1038/nrneurol.2016.98
69. Hommet C, Sauerwein HC, De Toffol B, Lassonde M. Idiopathic epileptic syndromes and cognition. Neurosci Biobehav Rev. (2006) 30:85–96. doi: 10.1016/j.neubiorev.2005.06.004
70. Cutting S, Lauchheimer A, Barr W, Devinsky O. Adult-Onset Idiopathic Generalized epilepsy: clinical and behavioral features. Epilepsia. (2002) 42:1395–8. doi: 10.1046/j.1528-1157.2001.14901.x
71. Chowdhury FA, Elwes RDC, Koutroumanidis M, Morris RG, Nashef L, Richardson MP. Impaired cognitive function in idiopathic generalized epilepsy and unaffected family members: an epilepsy endophenotype. Epilepsia. (2014) 55:835–40. doi: 10.1111/epi.12604
72. Rathouz PJ, Zhao Q, Jones JE, Jackson DC, Hsu DA, Stafstrom CE, et al. Cognitive development in children with new onset epilepsy. Dev Med Child Neurol. (2014) 56:635–41. doi: 10.1111/dmcn.12432
73. Abarrategui B, Parejo-Carbonell B, García García ME, Di Capua D, García-Morales I. The cognitive phenotype of idiopathic generalized epilepsy. Epilepsy Behav. (2018) 89:99–104. doi: 10.1016/j.yebeh.2018.10.007
74. Henkin Y, Sadeh M, Kivity S, Shabtai E, Kishon-Rabin L, Gadoth N. Cognitive function in idiopathic generalized epilepsy of childhood. Dev Med Child Neurol. (2005) 47:126–32. doi: 10.1017/S0012162205000228
75. Maganti R, Sheth RD, Hermann BP, Weber S, Gidal BE, Fine J. Sleep architecture in children with idiopathic generalized epilepsy. Epilepsia. (2005) 46:104–9. doi: 10.1111/j.0013-9580.2005.06804.x
76. Dickson JM. Idiopathic generalised epilepsy: a pilot study of memory and neuronal dysfunction in the temporal lobes, assessed by magnetic resonance spectroscopy. J Neurol Neurosurg Psychiatry. (2006) 77:834–40. doi: 10.1136/jnnp.2005.086918
77. Gelžiniene G, Jurkevičiene G, Marmiene V, Adomaitiene V, Endziniene M. Executive functions in adolescents with idiopathic generalized epilepsy. Medicina. (2011) 47:44. doi: 10.3390/medicina47060044
78. Meador KJ, Gilliam FG, Kanner AM, Pellock JM. Cognitive and behavioral effects of antiepileptic drugs. Epilepsy Behav. (2001) 2:SS1–17. doi: 10.1006/ebeh.2001.0235
79. Witt J-A, Elger CE, Helmstaedter C. Adverse cognitive effects of antiepileptic pharmacotherapy: each additional drug matters. Eur Neuropsychopharmacol. (2015) 25:1954–9. doi: 10.1016/j.euroneuro.2015.07.027
80. Caciagli L, Xiao F, Wandschneider B, Koepp MJ. Imaging biomarkers of anti-epileptic drug action: insights from magnetic resonance imaging. CPD. (2017) 23:5727–39. doi: 10.2174/1381612823666170809113636
81. Muhlert N, Grünewald RA, Hunkin NM, Reuber M, Howell S, Reynders H, et al. Accelerated long-term forgetting in temporal lobe but not idiopathic generalised epilepsy. Neuropsychologia. (2011) 49:2417–26. doi: 10.1016/j.neuropsychologia.2011.04.018
82. Gascoigne MB, Barton B, Webster R, Gill D, Antony J, Lah SS. Accelerated long-term forgetting in children with idiopathic generalized epilepsy: accelerated Long-Term Forgetting in Children. Epilepsia. (2012) 53:2135–40. doi: 10.1111/j.1528-1167.2012.03719.x
83. Grayson-Collins J, Gascoigne MB, Barton B, Webster R, Gill D, Lah S. Longitudinal study of accelerated long-term forgetting in children with genetic generalized epilepsy: evidence of ongoing deficits. Cortex. (2019) 110:5–15. doi: 10.1016/j.cortex.2017.08.028
84. Davidson M, Dorris L, O'Regan M, Zuberi SM. Memory consolidation and accelerated forgetting in children with idiopathic generalized epilepsy. Epilepsy Behav. (2007) 11:394–400. doi: 10.1016/j.yebeh.2007.05.004
85. Swartz BE, Halgren E, Simpkins F, Syndulko K. Primary memory in patients with frontal and primary generalized epilepsy. J Epilepsy. (1994) 7:232–41. doi: 10.1016/0896-6974(94)90034-5
86. Swartz BE, Simpkins F, Halgren E, Mandelkern M, Brown C, Krisdakumtorn T, et al. Visual working memory in primary generalized epilepsy: an 18 FDG-PET study. Neurology. (1996) 47:1203–12. doi: 10.1212/WNL.47.5.1203
87. Devinsky O, Gershengorn J, Brown E, Perrine K, Vazquez B, Luciano D. Frontal functions in juvenile myoclonic epilepsy. Neuropsychiatry Neuropsychol Behav Neurol. (1997) 10:243–6.
88. Sonmez F, Atakli D, Sari H, Atay T, Arpaci B. Cognitive function in juvenile myoclonic epilepsy. Epilepsy Behav. (2004) 5:329–36. doi: 10.1016/j.yebeh.2004.01.007
89. Kim S-Y, Hwang Y-H, Lee H-W, Suh C-K, Kwon S-H, Park S-P. Cognitive impairment in juvenile myoclonic epilepsy. J Clin Neurol. (2007) 3:86. doi: 10.3988/jcn.2007.3.2.86
90. Pascalicchio TF, de Araujo Filho GM, da Silva Noffs MH, Lin K, Caboclo LOSF, Vidal-Dourado M, et al. Neuropsychological profile of patients with juvenile myoclonic epilepsy: a controlled study of 50 patients. Epilepsy Behav. (2007) 10:263–7. doi: 10.1016/j.yebeh.2006.11.012
91. Piazzini A, Turner K, Vignoli A, Canger R, Canevini MP. Frontal cognitive dysfunction in juvenile myoclonic epilepsy. Epilepsia. (2008) 49:657–62. doi: 10.1111/j.1528-1167.2007.01482.x
92. Iqbal N, Caswell HL, Hare DJ, Pilkington O, Mercer S, Duncan S. Neuropsychological profiles of patients with juvenile myoclonic epilepsy and their siblings: a preliminary controlled experimental video-EEG case series. Epilepsy Behav. (2009) 14:516–21. doi: 10.1016/j.yebeh.2008.12.025
93. Roebling R, Scheerer N, Uttner I, Gruber O, Kraft E, Lerche H. Evaluation of cognition, structural, and functional MRI in juvenile myoclonic epilepsy. Epilepsia. (2009) 50:2456–65. doi: 10.1111/j.1528-1167.2009.02127.x
94. O'Muircheartaigh J, Vollmar C, Barker GJ, Kumari V, Symms MR, Thompson P, et al. Focal structural changes and cognitive dysfunction in juvenile myoclonic epilepsy. Neurology. (2011) 76:34–40. doi: 10.1212/WNL.0b013e318203e93d
95. Kim JH, Suh S, Park S-Y, Seo W-K, Koh I, Koh S-B, et al. Microstructural white matter abnormality and frontal cognitive dysfunctions in juvenile myoclonic epilepsy: white matter abnormality in JME. Epilepsia. (2012) 53:1371–8. doi: 10.1111/j.1528-1167.2012.03544.x
96. Lin K, de Araujo Filho GM, Pascalicchio TF, Silva I, Tudesco ISS, Guaranha MSB, et al. Hippocampal atrophy and memory dysfunction in patients with juvenile myoclonic epilepsy. Epilepsy Behav. (2013) 29:247–51. doi: 10.1016/j.yebeh.2013.06.034
97. Wandschneider B, Centeno M, Vollmar C, Stretton J, O'Muircheartaigh J, Thompson PJ, et al. Risk-taking behavior in juvenile myoclonic epilepsy. Epilepsia. (2013) 54:2158–65. doi: 10.1111/epi.12413
98. Zamarian L, Höfler J, Kuchukhidze G, Delazer M, Bonatti E, Kemmler G, et al. Decision making in juvenile myoclonic epilepsy. J Neurol. (2013) 260:839–46. doi: 10.1007/s00415-012-6715-z
99. Thomas RH, Walsh J, Church C, Sills GJ, Marson AG, Baker GA, et al. A comprehensive neuropsychological description of cognition in drug-refractory juvenile myoclonic epilepsy. Epilepsy Behav. (2014) 36:124–9. doi: 10.1016/j.yebeh.2014.04.027
100. Iqbal N, Caswell H, Muir R, Cadden A, Ferguson S, Mackenzie H, et al. Neuropsychological profiles of patients with juvenile myoclonic epilepsy and their siblings: an extended study. Epilepsia. (2015) 56:1301–8. doi: 10.1111/epi.13061
101. Giorgi FS, Guida M, Caciagli L, Pagni C, Pizzanelli C, Bonanni E, et al. Social cognition in Juvenile Myoclonic Epilepsy. Epilepsy Res. (2016) 128:61–7. doi: 10.1016/j.eplepsyres.2016.10.017
102. Valente KD, Rzezak P, Moschetta SP, de Vincentiis S, Coan AC, Guerreiro CAM. Delineating behavioral and cognitive phenotypes in juvenile myoclonic epilepsy: are we missing the forest for the trees? Epilepsy Behav. (2016) 54:95–9. doi: 10.1016/j.yebeh.2015.10.022
103. Rzezak P, Moschetta SP, Mendonça M, Paiva MLMN, Coan AC, Guerreiro C, et al. Higher IQ in juvenile myoclonic epilepsy: Dodging cognitive obstacles and “masking” impairments. Epilepsy Behav. (2018) 86:124–30. doi: 10.1016/j.yebeh.2018.05.029
104. Sezikli S, Pulat TA, Tekin B, Ak PD, Keskinkiliç C, Atakli D. Frontal lobe cognitive functions and electroencephalographic features in juvenile myoclonic epilepsy. Epilepsy Behav. (2018) 86:102–7. doi: 10.1016/j.yebeh.2018.06.009
105. Unterberger I, Zamarian L, Prieschl M, Bergmann M, Walser G, Luef G, et al. Risky decision making in juvenile myoclonic epilepsy. Front Neurol. (2018) 9:195. doi: 10.3389/fneur.2018.00195
106. Paiva ML, Rzezak P, Santos B, Lima EM, Moschetta SP, Vincentiis S, et al. Dissociation between decision making under ambiguity and risk in patients with juvenile myoclonic epilepsy. Epilepsy Behav. (2019) 101:106548. doi: 10.1016/j.yebeh.2019.106548
107. Wandschneider B, Burdett J, Townsend L, Hill A, Thompson PJ, Duncan JS, et al. Effect of topiramate and zonisamide on fMRI cognitive networks. Neurology. (2017) 88:1165–71. doi: 10.1212/WNL.0000000000003736
108. Caciagli L, Wandschneider B, Xiao F, Vollmar C, Centeno M, Vos SB, et al. Abnormal hippocampal structure and function in juvenile myoclonic epilepsy and unaffected siblings. Brain. (2019) 142:2670–87. doi: 10.1093/brain/awz215
109. Pavone P, Bianchini R, Trifiletti RR, Incorpora G, Pavone A, Parano E. Neuropsychological assessment in children with absence epilepsy. Neurology. (2001) 6. doi: 10.1212/WNL.56.8.1047
110. Caplan R, Siddarth P, Stahl L, Lanphier E, Vona P, Gurbani S, et al. Childhood absence epilepsy: behavioral, cognitive, and linguistic comorbidities. Epilepsia. (2008) 49:1838–46. doi: 10.1111/j.1528-1167.2008.01680.x
111. Caplan R, Siddarth P, Vona P, Stahl L, Bailey C, Gurbani S, et al. Language in pediatric epilepsy. Epilepsia. (2009) 50:2397–407. doi: 10.1111/j.1528-1167.2009.02199.x
112. Conant LL, Wilfong A, Inglese C, Schwarte A. Dysfunction of executive and related processes in childhood absence epilepsy. Epilepsy Behav. (2010) 18:414–23. doi: 10.1016/j.yebeh.2010.05.010
113. Vega C, Vestal M, DeSalvo M, Berman R, Chung M, Blumenfeld H, et al. Differentiation of attention-related problems in childhood absence epilepsy. Epilepsy Behav. (2010) 19:82–5. doi: 10.1016/j.yebeh.2010.06.010
114. Tosun D, Siddarth P, Toga AW, Hermann B, Caplan R. Effects of childhood absence epilepsy on associations between regional cortical morphometry and aging and cognitive abilities. Hum Brain Mapp. (2011) 32:580–91. doi: 10.1002/hbm.21045
115. D'Agati E, Cerminara C, Casarelli L, Pitzianti M, Curatolo P. Attention and executive functions profile in childhood absence epilepsy. Brain Dev. (2012) 34:812–7. doi: 10.1016/j.braindev.2012.03.001
116. Kernan CL, Asarnow R, Siddarth P, Gurbani S, Lanphier EK, Sankar R, et al. Neurocognitive profiles in children with epilepsy. Epilepsia. (2012) 53:2156–63. doi: 10.1111/j.1528-1167.2012.03706.x
117. Masur D, Shinnar S, Cnaan A, Shinnar RC, Clark P, Wang J, et al. Pretreatment cognitive deficits and treatment effects on attention in childhood absence epilepsy. Neurology. (2013) 81:1572–80. doi: 10.1212/WNL.0b013e3182a9f3ca
118. Cheng D, Yan X, Gao Z, Xu K, Zhou X, Chen Q. Neurocognitive profiles in childhood absence epilepsy: a focus on cognitive dysfunction associated with the frontal lobe. J Child Neurol. (2017) 32:46–52. doi: 10.1177/0883073816668465
119. Cheng D, Yan X, Gao Z, Xu K, Chen Q. Attention contributes to arithmetic deficits in new-onset childhood absence epilepsy. Front Psychiatry. (2017) 8:166. doi: 10.3389/fpsyt.2017.00166
120. Kadish NE, Baumann M, Pietz J, Schubert-Bast S, Reuner G. Validation of a screening tool for attention and executive functions (EpiTrack Junior®) in children and adolescents with absence epilepsy. Epilepsy Behav. (2013) 29:96–102. doi: 10.1016/j.yebeh.2013.06.004
121. Levav M, Mirsky AF, Herault J, Xiong L, Amir N, Andermann E. Familial association of neuropsychological traits in patients with generalized and partial seizure disorders. J Clin Exp Neuropsychol. (2002) 24:311–26. doi: 10.1076/jcen.24.3.311.985
122. Ashburner J, Friston KJ. Voxel-based morphometry—the methods. Neuroimage. (2000) 11:805–21. doi: 10.1006/nimg.2000.0582
124. Rugg-Gunn FJ, Eriksson SH, Symms MR, Barker GJ, Thom M, Harkness W, et al. Diffusion tensor imaging in refractory epilepsy. Lancet. (2002) 359:1748–51. doi: 10.1016/S0140-6736(02)08615-4
125. Woermann F. Quantitative MRI in patients with idiopathic generalized epilepsy. Evidence of widespread cerebral structural changes. Brain. (1998) 121:1661–7. doi: 10.1093/brain/121.9.1661
126. Seeck M, Dreifuss S, Lantz G, Jallon P, Foletti G, Despland P-A, et al. Subcortical nuclei volumetry in idiopathic generalized epilepsy. Epilepsia. (2005) 46:1642–5. doi: 10.1111/j.1528-1167.2005.00259.x
127. Betting LE, Mory SB, Li LM, Lopes-Cendes I, Guerreiro MM, Guerreiro CAM, et al. Voxel-based morphometry in patients with idiopathic generalized epilepsies. Neuroimage. (2006) 32:498–502. doi: 10.1016/j.neuroimage.2006.04.174
128. Liu M, Concha L, Beaulieu C, Gross DW. Distinct white matter abnormalities in different idiopathic generalized epilepsy syndromes: diffusion abnormalities in IGE syndromes. Epilepsia. (2011) 52:2267–75. doi: 10.1111/j.1528-1167.2011.03313.x
129. O'Muircheartaigh J, Vollmar C, Barker GJ, Kumari V, Symms MR, Thompson P, et al. Abnormal thalamocortical structural and functional connectivity in juvenile myoclonic epilepsy. Brain. (2012) 135:3635–44. doi: 10.1093/brain/aws296
130. Nuyts S, D'Souza W, Bowden SC, Vogrin SJ. Structural brain abnormalities in genetic generalized epilepsies: a systematic review and meta-analysis. Epilepsia. (2017) 58:2025–37. doi: 10.1111/epi.13928
131. Whelan CD, Altmann A, Botía JA, Jahanshad N, Hibar DP, Absil J, et al. Structural brain abnormalities in the common epilepsies assessed in a worldwide ENIGMA study. Brain. (2018) 141:391–408. doi: 10.1093/brain/awx341
132. Wandschneider B, Hong S-J, Bernhardt BC, Fadaie F, Vollmar C, Koepp MJ, et al. Developmental MRI markers cosegregate juvenile patients with myoclonic epilepsy and their healthy siblings. Neurology. (2019) 93:e1–e9. doi: 10.1212/WNL.0000000000008173
133. Wang Z, Larivière S, Xu Q, Vos de Wael R, Hong SJ, Wang Z, et al. Community-informed connectomics of the thalamocortical system in generalized epilepsy. Neurology. (2019) 93:e1112–22. doi: 10.1212/WNL.0000000000008096
134. Gotman J, Grova C, Bagshaw A, Kobayashi E, Aghakhani Y, Dubeau F. Generalized epileptic discharges show thalamocortical activation and suspension of the default state of the brain. Proc Natl Acad Sci USA. (2005) 102:15236–40. doi: 10.1073/pnas.0504935102
135. Hamandi K, Salek-Haddadi A, Laufs H, Liston A, Friston K, Fish DR, et al. EEG–fMRI of idiopathic and secondarily generalized epilepsies. Neuroimage. (2006) 31:1700–10. doi: 10.1016/j.neuroimage.2006.02.016
136. Xiao F, Caciagli L, Wandschneider B, Koepp M. Imaging cortical and subcortical circuitry in generalized epilepsies. In: Bernasconi A, Bernasconi N, Koepp M, editors. Imaging Biomarkers in Epilepsy. Cambridge: Cambridge University Press (2019). p. 124–34.
137. Caciagli L, Bernhardt BC, Bernasconi A, Bernasconi N. Network modeling of epilepsy using structural and functional MRI. In: Bernasconi A, Bernasconi N, Koepp M, editors. Imaging Biomarkers in Epilepsy. Cambridge: Cambridge University Press. (2019). p. 77–94.
138. Savic I, Österman Y, Helms G. MRS shows syndrome differentiated metabolite changes in human-generalized epilepsies. Neuroimage. (2004) 21:163–72. doi: 10.1016/j.neuroimage.2003.08.034
139. McDonald CR, Swartz BE, Halgren E, Patell A, Daimes R, Mandelkern M. The relationship of regional frontal hypometabolism to executive function: a resting fluorodeoxyglucose PET study of patients with epilepsy and healthy controls. Epilepsy Behav. (2006) 9:58–67. doi: 10.1016/j.yebeh.2006.04.007
140. Pulsipher DT, Seidenberg M, Guidotti L, Tuchscherer VN, Morton J, Sheth RD, et al. Thalamofrontal circuitry and executive dysfunction in recent-onset juvenile myoclonic epilepsy. Epilepsia. (2009) 50:1210–9. doi: 10.1111/j.1528-1167.2008.01952.x
141. Vollmar C, O'Muircheartaigh J, Barker GJ, Symms MR, Thompson P, Kumari V, et al. Motor system hyperconnectivity in juvenile myoclonic epilepsy: a cognitive functional magnetic resonance imaging study. Brain. (2011) 134:1710–9. doi: 10.1093/brain/awr098
142. Lin JJ, Dabbs K, Riley JD, Jones JE, Jackson DC, Hsu DA, et al. Neurodevelopment in new-onset juvenile myoclonic epilepsy over the first 2 years: JME neurodevelopment. Ann Neurol. (2014) 76:660–8. doi: 10.1002/ana.24240
143. Caeyenberghs K, Powell HWR, Thomas RH, Brindley L, Church C, Evans J, et al. Hyperconnectivity in juvenile myoclonic epilepsy: a network analysis. Neuroimage Clin. (2015) 7:98–104. doi: 10.1016/j.nicl.2014.11.018
144. Caplan R, Levitt J, Siddarth P, Wu KN, Gurbani S, Sankar R, et al. Frontal and temporal volumes in childhood absence epilepsy. Epilepsia. (2009) 50:2466–72. doi: 10.1111/j.1528-1167.2009.02198.x
145. Killory BD, Bai X, Negishi M, Vega C, Spann MN, Vestal M, et al. Impaired attention and network connectivity in childhood absence epilepsy. Neuroimage. (2011) 56:2209–17. doi: 10.1016/j.neuroimage.2011.03.036
146. Lin JJ, Siddarth P, Riley JD, Gurbani SG, Ly R, Yee VW, et al. Neurobehavioral comorbidities of pediatric epilepsies are linked to thalamic structural abnormalities. Epilepsia. (2013) 54:2116–24. doi: 10.1111/epi.12428
147. Guo JN, Kim R, Chen Y, Negishi M, Jhun S, Weiss S, et al. Impaired consciousness in patients with absence seizures investigated by functional MRI, EEG, and behavioural measures: a cross-sectional study. Lancet Neurol. (2016) 15:1336–45. doi: 10.1016/S1474-4422(16)30295-2
148. Savic I, Lekvall A, Greitz D, Helms G. mr spectroscopy shows reduced frontal lobe concentrations of N-acetyl aspartate in patients with juvenile myoclonic epilepsy. Epilepsia. (2000) 41:290–6. doi: 10.1111/j.1528-1157.2000.tb00158.x
149. Vollmar C, O'Muircheartaigh J, Symms MR, Barker GJ, Thompson P, Kumari V, et al. Altered microstructural connectivity in juvenile myoclonic epilepsy: the missing link. Neurology. (2012) 78:1555–9. doi: 10.1212/WNL.0b013e3182563b44
150. Wolf P, Yacubian EMT, Avanzini G, Sander T, Schmitz B, Wandschneider B, et al. Juvenile myoclonic epilepsy: a system disorder of the brain. Epilepsy Res. (2015) 114:2–12. doi: 10.1016/j.eplepsyres.2015.04.008
151. Tan H-Y, Callicott JH, Weinberger DR. Dysfunctional and Compensatory Prefrontal cortical systems, genes and the pathogenesis of Schizophrenia. Cereb Cortex. (2007) 17:i171–81. doi: 10.1093/cercor/bhm069
152. Potkin SG, Turner JA, Brown GG, McCarthy G, Greve DN, Glover GH, et al. Working memory and DLPFC inefficiency in schizophrenia: the FBIRN study. Schizophr Bull. (2009) 35:19–31. doi: 10.1093/schbul/sbn162
153. Moeller F, Siebner HR, Wolff S, Muhle H, Granert O, Jansen O, et al. Simultaneous EEG-fMRI in drug-naive children with newly diagnosed absence epilepsy. Epilepsia. (2008) 49:1510–9. doi: 10.1111/j.1528-1167.2008.01626.x
154. Bai X, Vestal M, Berman R, Negishi M, Spann M, Vega C, et al. Dynamic time course of typical childhood absence seizures: EEG, behavior, and functional magnetic resonance imaging. J Neurosci. (2010) 30:5884–93. doi: 10.1523/JNEUROSCI.5101-09.2010
155. Tondelli M, Vaudano AE, Ruggieri A, Meletti S. Cortical and subcortical brain alterations in Juvenile absence epilepsy. Neuroimage Clin. (2016) 12:306–11. doi: 10.1016/j.nicl.2016.07.007
156. Marini C, Scheffer IE, Crossland KM, Grinton BE, Phillips FL, McMahon JM, et al. Genetic architecture of idiopathic generalized epilepsy: clinical genetic analysis of 55 multiplex families. Epilepsia. (2004) 45:467–78. doi: 10.1111/j.0013-9580.2004.46803.x
157. Delgado-Escueta AV, Koeleman BPC, Bailey JN, Medina MT, Durón RM. The quest for Juvenile myoclonic epilepsy genes. Epilepsy Behav. (2013) 28:S52–7. doi: 10.1016/j.yebeh.2012.06.033
158. Helbig I. Genetic causes of generalized epilepsies. Semin Neurol. (2015) 35:288–92. doi: 10.1055/s-0035-1552922
159. Gottesman II, Gould TD. The endophenotype concept in psychiatry: etymology and strategic intentions. AJP. (2003) 160:636–45. doi: 10.1176/appi.ajp.160.4.636
Keywords: genetic generalized epilepsies, cognition, neuropsychology, neuroimaging, endophenotype
Citation: Ratcliffe C, Wandschneider B, Baxendale S, Thompson P, Koepp MJ and Caciagli L (2020) Cognitive Function in Genetic Generalized Epilepsies: Insights From Neuropsychology and Neuroimaging. Front. Neurol. 11:144. doi: 10.3389/fneur.2020.00144
Received: 03 October 2019; Accepted: 10 February 2020;
Published: 10 March 2020.
Edited by:
Udaya Seneviratne, Monash Medical Centre, AustraliaCopyright © 2020 Ratcliffe, Wandschneider, Baxendale, Thompson, Koepp and Caciagli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lorenzo Caciagli, bG9yZW56by5jYWNpYWdsaS4xMUB1Y2wuYWMudWs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.