 Bérenger Largeau1*†
Bérenger Largeau1*† David Boels2†
David Boels2† Caroline Victorri-Vigneau3†
Caroline Victorri-Vigneau3† Clara Cohen4†
Clara Cohen4† Charlotte Salmon Gandonnière5†
Charlotte Salmon Gandonnière5† Stephan Ehrmann6†
Stephan Ehrmann6†- 1CHU de Nantes, Service de Pharmacologie Clinique—Centre Régional de Pharmacovigilance, Nantes, France
- 2CHU de Nantes, Service de Pharmacologie Clinique—Unité de Toxicologie Clinique et Toxicosurveillance Médicamenteuse, Nantes, France
- 3Université de Nantes, Université de Tours, INSERM, Methods in Patients-Centered Outcomes and Health Research (SPHERE)—UMR 1246, CHU de Nantes, Service de Pharmacologie Clinique—Centre d'Évaluation et d'Information sur la Pharmacodépendance et d'Addictovigilance, Nantes, France
- 4Université de Tours, CHRU de Tours, Service de Neuroradiologie Diagnostique et Interventionnelle, Tours, France
- 5CHRU de Tours, Service de Médecine Intensive Réanimation, CIC 1415, réseau CRICS-TRIGGERSEP, Tours, France
- 6Université de Tours, INSERM, Centre d'Étude des Pathologies Respiratoires (CEPR)—UMR 1100, CHRU de Tours, Service de Médecine Intensive Réanimation, CIC 1415, Réseau CRICS-TRIGGERSEP, Tours, France
Background: Posterior reversible encephalopathy syndrome (PRES) is a rare clinical and radiological entity characterized by a typical brain edema. Although several case reports have described PRES in a context of poisoning, to our knowledge, a comprehensive assessment has not been performed. The aim of this systematic review was to raise awareness on poisoning-specific PRES features and to encourage consistent and detailed reporting of substance abuse–and drug overdose–associated PRES.
Methods: Medline/PubMed, Web of Science, and PsycINFO were screened through May 31, 2019, to systematically identify case reports and case series describing PRES associated with poisoning (i.e., alcohol, drugs, illicit drugs, natural toxins, chemical substances) in accidental context, intentional overdose, and substance abuse. The methodological quality of eligible case reports/series was assessed. Patients and exposure characteristics were recorded; relevant toxicological, radiological, and clinical data were extracted.
Results: Forty-one case reports and one case series reporting 42 unique cases were included. The median time to PRES onset from the start of exposure was 3 days (IQR 2–10). Acute high blood pressure, visual disturbance, and seizure were reported in 70, 55, and 50% of patients, respectively. The initial clinical presentation was alertness disorders in 64% of patients. Nine patients (21%) required mechanical ventilation. One-third of patients had at least one risk factor for PRES such as chronic hypertension (17%) or acute/chronic kidney failure (24%). The main imaging pattern (67%) was the combination of classical parieto-occipital edema with another anatomical region (e.g., frontal, basal ganglia, posterior fossa involvement). Vasogenic edema was found in 86% of patients. Intracranial hemorrhage occurred in 14% of patients. Both brain infarction and reversible cerebral vasoconstriction syndrome were diagnosed in 5% of patients. Three patients (12%, 3/25) had non-reversible lesions on follow-up magnetic resonance imaging. The median time required to hospital discharge was 14 days (IQR 7–18). Mortality and neurological recurrence rate were null.
Conclusions: Comorbidities such as chronic hypertension and kidney failure were less frequent than in patients with other PRES etiologies. Imaging analysis did not highlight a specific pattern for poisoning-induced PRES. Although less described, PRES in the context of poisoning, which shares most of the clinical and radiological characteristics of other etiologies, is not to be ignored.
Introduction
Posterior reversible encephalopathy syndrome (PRES) is a rare radiological and clinical entity characterized by a typical brain edema and various symptoms such as high blood pressure (75–80%), encephalopathy (50–80%), headache (50%), visual disturbances (33%), focal neurological deficits (10–15%), seizures (60–75%), and status epilepticus (5–15%) (1). Kidney injury is highly prevalent during PRES (up to 55%), and more than half of patients have chronic hypertension (1). PRES can occur in a number of complex clinical conditions, classically dichotomized into iatrogenic (e.g., antineoplastic therapy, calcineurin inhibitors) and PRES-associated medical conditions (e.g., eclampsia, sepsis, autoimmune disorders), requiring mechanical ventilation for 3–7 days in 35–40% of patients (2). Although there is currently no unified diagnostic algorithm, neuroimaging usually yields bilateral cortical–subcortical vasogenic edema according to three anatomic patterns: dominant parieto-occipital involvement, variant atypical PRES, and combination of different patterns. Variant atypical PRES gathers superior frontal sulcus, holohemispheric watershed, cerebellum, basal ganglia, brainstem, and spinal cord involvements (3, 4). The atypical or combined patterns are more common than the typical PRES with isolated parieto-occipital involvement.
The pathophysiology of PRES is still debated through hypoperfusion and hyperperfusion theories. Impaired cerebral autoregulation responsible for disruption of the blood–brain barrier (BBB) is one of the two main hypotheses, the other one being endothelial dysfunction (5). A recent review suggests that arginine vasopressin (AVP) axis stimulation could precipitate PRES development through an increase in AVP secretion or AVP receptor density. Activation of vasopressin V1a receptors leads to cerebral vasoconstriction, endothelial dysfunction, and subsequent brain edema (5).
Thus, PRES is a syndrome whose circumstances of occurrence and radiological features are associated with significant clinical and radiological polymorphism, making it difficult to characterize. Drug toxicity is one of the potential etiologies. Data are available in the literature regarding PRES occurring at therapeutic drug doses, but to the best of our knowledge, no review focused specifically on cases of accidental or intentional poisoning-associated PRES.
In order to investigate the occurrence of PRES in poisoned patients, the authors systematically reviewed the scientific literature of case reports and case series concerning PRES associated with poisoning (i.e., alcohol, drugs, illicit drugs, natural toxins, chemical substances) in accidental context, intentional overdose, and substance abuse. The authors did not include cases of calcineurin inhibitor overexposure, which has already been covered (6). The purpose of this study is to raise awareness of the features of PRES in poisoned patients and encourage consistent and detailed reporting of PRES in a context of overdose and substance abuse.
Methods
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (7).
Eligibility Criteria
All language case reports and cases series were eligible if they concerned human subjects and included full-text. Records were screened if they were explicitly labeled as PRES based on head MRI (magnetic resonance imaging) or CT (computed tomography) scans. Case reports were included if PRES occurred in temporal connection with poisoning (i.e., alcohol, drugs, illicit drugs, chemical substances, natural toxins) in accidental context, intentional overdose, or substance abuse and/or a causal relationship was assumed by the authors of the report.
Data Sources, Search Strategy, and Data Extraction
A search using Medline/PubMed, Web of Science and PsycINFO was performed without any limits through May 31, 2019. The search terms in Medline were a combination of medical subject heading (MeSH) terms and keywords. The search strategy consisted of using the health multi-terminology portal HeTOP (8) for each term (i.e., text words OR MeSH OR title/abstract) with the following search algorithm: ([posterior leukoencephalopathy syndrome] AND ([poisoning] OR [overdose] OR [intoxication] OR [substance abuse] OR [solvents] OR [organophosphates] OR [licorice] OR [venoms] OR [scorpion] OR [mushroom] OR [lysergic acid] OR [cathinone] OR [cocaine] OR [amphetamine] OR [heroin] OR [cannabis] OR [alcohol])). A manual search and screening of the bibliographies of selected articles was performed, in addition to the computerized search. The search strategy is summarized in Supplementary Figure 1.
Extracted data included the following clinical and toxicological considerations: age, gender, risk factors of PRES occurrence, and exposure characteristics to the causative agent. Clinical and radiological data on PRES, its time course, and outcomes were also extracted. Unreported data were considered absent. Neuroimaging results were classified according to three different patterns. Briefly, the classical PRES pattern, involving only parieto-occipital lobes; the variant, including isolated various anatomical regions (e.g., frontal, cerebellum, brainstem, basal ganglia); and finally, the combined pattern, which includes combination of various regions.
Methodological Quality Assessment
The methodological quality of case reports and cases series was assessed using the tool proposed by Murad et al. (9) modified to adapt it to the analysis of toxicological exposures associated with PRES. The selected items were based on scores used for causality assessment in drug overdose (10, 11). This new tool converges into 10 items that can be categorized into six domains: selection, ascertainment, diagnosis, causality, follow-up, and reporting (Supplementary Table 1). Briefly, items included time to onset of PRES, exposure characteristics (e.g., dose, drug detection, identification of species), radiological features, clinical data (e.g., symptoms, risk factors), dechallenge phenomenon, differential diagnosis, pharmacological properties of the causative agent, and clinical/radiological follow-up. The results of this modified tool have been summarized by summing the scores of the 10 binary responses into an aggregate score (Supplementary Tables 1, 2).
Results
Case Selection
The literature search revealed a total of 149 non-duplicate records of which 95 were excluded because they did not report poisoning-associated PRES or were not case reports or case series. Out of 54 full-texts assessed for eligibility, 13 were excluded because they did not report poisoning-associated PRES or outcomes of interest (i.e., symptoms, brain edema features, follow-up). Finally, 40 case reports and 1 case series reporting a total of 42 unique cases were included (Supplementary Figure 1).
Synthesized Findings
Demographic Characteristics and Clinico-Biological Findings
Demographic data, substances involved, and clinico-radiological characteristics are summarized in Supplementary Table 3. Out of 42 patients included, 22 were female (52%); median age was 41 years (IQR 27–55, range 3–73). Four children were included (12–15). The median time to PRES onset from the start of exposure or intoxication diagnosis was 3 days (IQR 2–10) and ranged from 2 h (13) to 4 months (16, 17). The initial clinical presentation was alertness disorders in 64% of patients (13–15, 18–40). Visual disturbances were reported in 55% of patients (23/42) (12, 13, 15, 16, 19–21, 23, 25–27, 29, 34, 35, 37, 39, 41–47) including photophobia (19, 20, 35), visual hallucination (21, 23, 26, 27), and cortical blindness (15, 16, 24, 29, 34, 37). Four patients had concurrent acute kidney failure with PRES (13, 19, 44, 48). When performed (33, 39, 43), hypomagnesemia was found in one patient (39). Cerebral spinal fluid (CSF) analysis (20, 21, 23, 24, 34, 36, 37, 45, 47, 49) showed elevated CSF protein in one patient (34). Nine patients (21%) required mechanical ventilation (14, 21, 28, 33, 38, 46–48). The median time required to hospital discharge was 14 days (IQR 7–18). Mortality and neurological recurrence rate were null.
Radiological Features
Radiological diagnosis was based on brain MRI and CT scans in 91% (38/42) and 9% (4/42) (35, 38, 40, 43), respectively. The neuroimaging findings, including anatomical pattern, diffusion-weighted imaging (DWI), apparent diffusion coefficient (ADC), edema type, symmetry, and arterial characteristics, are summarized in Supplementary Table 3. Five patients (19, 24, 26, 34, 44) had normal initial brain CT (5/9, 56%) (19, 20, 24, 26, 34, 42, 44, 48, 50). All patients exhibited cortical and/or subcortical edema, characterized by hyperintensities in T2-weighted and/or T2 fluid-attenuated inversion recovery (FLAIR) imaging, which was consistent with PRES diagnosis in MRI. Symmetrical lesions were reported in 76% of patients (25/33) (12–15, 19, 22–25, 27, 29, 32–34, 36, 37, 39, 40, 43, 44, 46, 47, 49, 50). The combined pattern, which includes combination of various regions, was the most frequent with 67% of patients (13, 14, 17–22, 24–26, 28, 30–35, 38, 39, 41, 44, 46–49, 51). The classical PRES pattern, involving only parieto-occipital lobes, was found in 19% (8/42) of patients (12, 16, 23, 27, 37, 40, 42, 45). The variant pattern of PRES (6/42, 14%), including isolated anatomical region such as occipital (29, 36, 43, 50) and cerebellum (15, 52), occurred in 9 and 5%, respectively. In five reports, angiography (by contrast-enhanced arteriography in CT, or MRI sequences including non-contrast time-of-flight and angio-MRI or digital subtraction angiography) showed narrowing of the cerebral arteries (16, 28, 36, 37, 49). Reversible cerebral vasoconstriction syndrome (16, 49) was diagnosed in 5% of patients (2/42).
DWI was positive in 60% of patients (12/20), totally or partially in correspondence with T2/FLAIR hyperintensities, with focal or larger extent (20, 25, 26, 29, 30, 36, 37, 39, 47–49). When data related to ADC were provided, positive DWI due to vasogenic edema (i.e., no restricted ADC) (16, 17, 19, 21, 23, 25, 26, 28–31, 33, 34, 36, 45, 47–49) and cytotoxic edema (i.e., restricted ADC) (20, 24, 39, 49) were found in 86 and 19% of cases, respectively. T2* (gradient echo) or susceptibility weighted imaging revealed intracranial hemorrhage in 14% of patients (16, 20, 30, 31, 36, 43). The median time of follow-up imaging was 21 days (IQR 11–60). Out of 25 patients with follow-up imaging, 22 (88%) showed complete resolution of brain edema (12–14, 16, 21, 22, 24, 26, 29–31, 33, 38, 43–47, 50, 51).
Characteristics According to the Causative Agent
Exposure characteristics, clinico-radiological features, and follow-up data of the included cases are shown in Table 1.
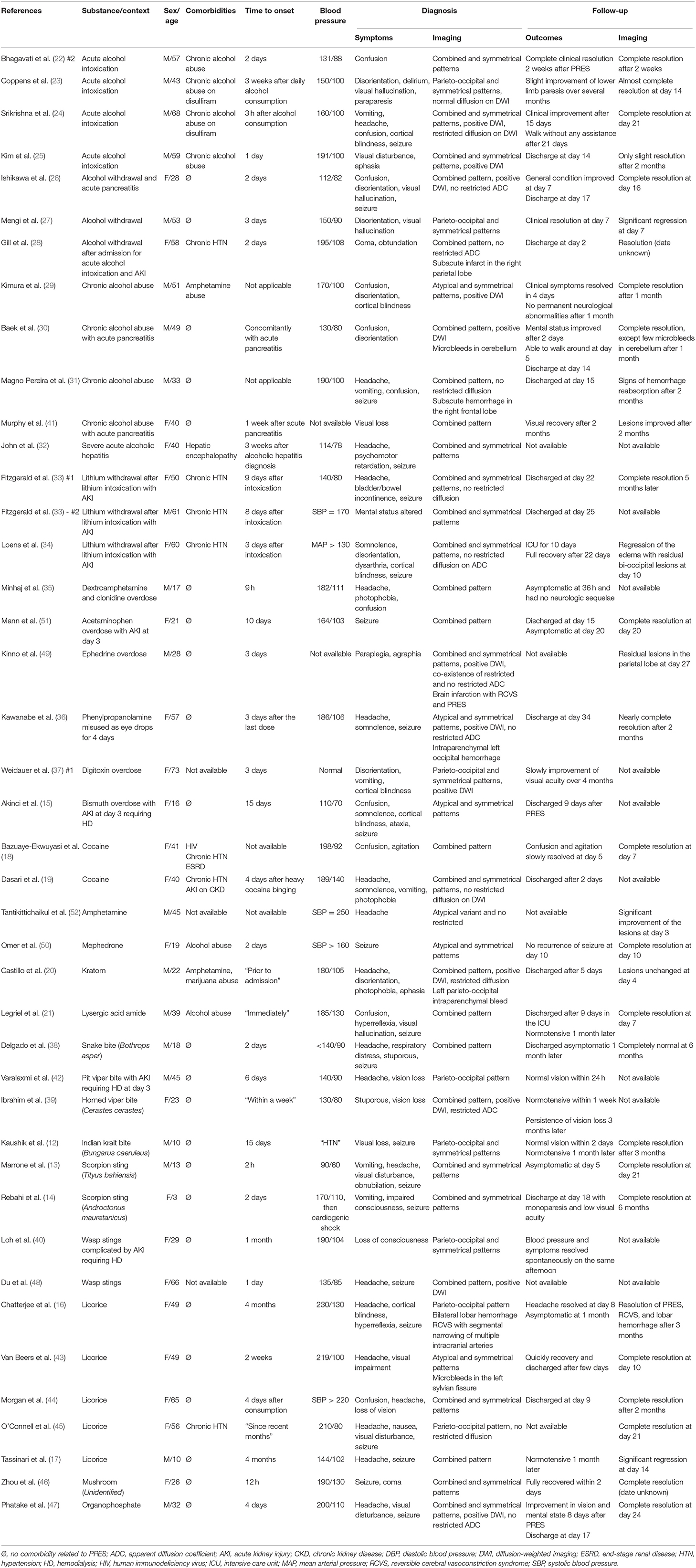
Table 1. Characteristics of the 42 included cases.
Alcohol
In alcohol-induced PRES, three different situations have been described: chronic alcohol intoxication (29–32, 41), acute alcohol intoxication (22–25), and alcohol withdrawal (26–28). PRES in chronic alcohol abusers occurred in conjunction with other complications of alcoholism such as acute pancreatitis (26, 30, 41) and hepatic encephalopathy due to severe acute alcoholic hepatitis (32). PRES onset occurred at the same time as acute pancreatitis (26, 30) or 1 week later (41), whereas it occurred 3 weeks after acute alcoholic hepatitis onset (32). All but four patients were hypertensive. Patients were normotensive in acute alcoholic pancreatitis (26, 30) and acute alcoholic hepatitis (32). Headache was reported in only 17% of patients (2/12) (24, 32). In three patients, PRES was complicated by intracranial hemorrhage (30, 31) or brain infarction (28).
Drug Overdose
Nine patients experienced PRES in a context of drug overdose, involving lithium (33, 34), dextroamphetamine (35), acetaminophen (51), ephedrine (49), phenylpropanolamine (36), digitoxin (37), and bismuth (15). The median time to PRES onset from the intoxication was 3 days, and two distinct situations were identified. PRES occurred during the acute phase of poisoning (35–37, 49) or at distance from intoxication (i.e., after stopping the causative drug) (15, 33, 34, 51). Three case reports indicated an association between lithium and PRES (33, 34). All these cases occurred after lithium discontinuation in patients with hypothyroidism, with chronic hypertension, and for whom intoxication was complicated by acute kidney injury (33, 34). Acute kidney injury occurred before the onset of neurological disturbances in five patients (56%) (15, 33, 34, 51). Angiography showed narrowing of the cerebral arteries in three cases (36, 37, 49). Infarction (49) and intraparenchymal hemorrhage (36) were also reported.
Illicit Drug
We collected six reports of illicit drug–induced PRES, involving cocaine (18, 19), amphetamine (52), mephedrone (50), kratom (20), and lysergic acid amide (21). Acute high blood pressure was reported in all patients (18–21, 50, 52). Patients had several risk factors for PRES such as chronic hypertension (18, 19), chronic kidney disease (18, 19), alcohol abuse (21, 50), and HIV infection (18).
Natural Toxin
In venom-induced PRES, snake bites [Cerastes cerastes (39), Bothrops asper (38), pit viper (42), Bungarus caeruleus (12)] were involved in four patients, scorpion stings in two cases [Tityus bahiensis (13), Androctonus mauretanicus (14)], and multiple wasp stings in two patients (40, 48). PRES was associated with mushroom (46) and licorice (16, 17, 43–45) in one and five patients, respectively. In 36% (5/14) of patients (12, 16, 17, 40, 43), the time from exposure start to PRES onset was more than 1 week. Patients required mechanical ventilation in 29% (4/14) of cases (14, 38, 46, 48); the duration of mechanical ventilation ranged from 2 (46) to 14 days (38). Acute kidney failure occurred in 36% (5/14) of patients (13, 40, 42, 44, 48), requiring hemodialysis in two cases (40, 42). Among the five patients with licorice-associated PRES, brain hemorrhage occurred in two patients (16, 43), one of which was associated with reversible cerebral vasoconstriction syndrome (16).
Chemical Substance
Phatake et al. (47) reported a patient complaining of headache and blurred vision 4 days after coma induced by consumption of organophosphorus compounds with suicidal intention. Brain MRI showed multifocal hyperintensities mainly in subcortical areas of parietal and occipital areas with increase ADC, suggesting PRES.
Discussion
Are Toxic PRES Different From Other Etiologies?
As in other etiologies, poisoning-associated PRES are very polymorphic in terms of both exposure characteristics and patient comorbidities. Regardless of the substances involved, the median of 3 days for time to onset of PRES can dichotomize the presentation of this syndrome into two distinct situations. Indeed, PRES occurring after 3 days seems to be more related to a rebound effect of intoxication or to complications related to the management of the poisoning, whereas a shorter period would support a direct link between the causative agent and PRES.
Clinical and Biological Findings
Clinically, the prevalence of symptoms usually reported in PRES patients was consistent with the published literature (1). Indeed, acute high blood pressure, visual disturbance, and seizure were reported in 70, 55, and 50% of patients, respectively. Seizure is the most common symptom found in children (53), and all children had seizures (12–15). However, comorbidities such as chronic hypertension (17%, 7/42) and acute or chronic kidney failure (24%, 10/42) were less frequently reported than in patients with other PRES etiologies, where their estimated prevalence is about 50% (1). In the literature, the frequency of isolated CSF protein elevation without pleocytosis, as a biomarker of permeability disruption of the BBB, varies from 60% (54) to 75% (55). In this review, although few cases reported CSF analysis, only one case (1/10, 10%) (34) described elevated CSF protein.
Radiological Features
All reviewed patients presented cortical and/or subcortical T2/FLAIR hyperintensities or hypodensities on CT when MRI was not performed, which was consistent with the main findings of PRES (3, 4). These hyperintensities correspond to the brain edema caused by vascular dysregulation, leading to acute vasodilatation and classically vasogenic edema, with proven pathological/imaging correlation (56). While parieto-occipital involvement (12–14, 16–18, 20–34, 36–51) was predominant (39/42, 93%), as described in the literature (57), the isolated parieto-occipital was not the main pattern in this review, supplanted by the pattern combining various anatomical regions involved. Frontal (13, 17, 18, 20, 22, 24–26, 28, 31, 33, 38, 44, 46, 48, 49, 51), temporal lobe (18, 25, 26, 30, 32, 33, 47), and cerebellum (14, 15, 18–21, 30, 35, 41, 52) involvement occurred in 41% (17/42), 17% (7/42), and 24% of patients (10/42), respectively. In this review, the prevalence of frontal and temporal involvement is lower than previously described, where it can be seen in up to 75% of cases (3). Indeed, temporal involvement was rarely reported, even though MRI images seemed to show involvement in this region. This may partially explain the difference in prevalence, especially since the whole brain MRI was not available for neuroradiological analysis.
The atypical distribution involving the thalamus (18, 19, 21, 34), basal ganglia (18, 19, 46), midbrain (18, 19), and corpus callosum (39) was less commonly reported, as described in the literature. As with other PRES etiologies, atypical imaging appearances including hemorrhage, contrast enhancement, and restricted diffusion on MRI were reported in similar proportions (58). Intracranial hemorrhage occurred in 14% of cases included (6/42) (16, 20, 30, 31, 36, 43). Among these cases, minimal occipital intraparenchymal (20, 36), microbleeds in the cerebellum (30) and sylvian fissure (43), and subarachnoid hemorrhage (31) were reported. Regarding contrast enhancement (19, 20, 22, 23, 30, 31, 38, 52), only one case described gyriform enhancement (20). In this case of PRES induced by kratom, brain MRI showed multifocal areas of abnormal T2 FLAIR; restricted diffusion in the superior parietal lobes, both occipital lobes, and both cerebellar hemispheres; and minimal hemorrhage in the left superior parietal lobe consistent with atypical PRES (20). DWI positivity (20, 25, 26, 29, 30, 36, 37, 39, 47–49) due to advanced edema was higher (12/20, 60%) than previously described in other PRES etiologies. The occurrence of cytotoxic edema (19%, 4/21) was consistent with the literature (15–30%) (3). Areas of restricted diffusion can be reversible or, conversely, progress to frank infarction (58). For instance, Kinno et al. (49) reported a case of PRES with reversible cerebral vasoconstriction syndrome due to ephedrine overdose. Initial brain MRI showed vasogenic edema in the left occipital and both parietal lobes with some hyperintense lesions on DWI with restricted diffusion on ADC maps, indicating the co-existence of cytotoxic edema. Follow-up MRI 1 month later showed residual partial hypertense areas in the superior parietal gyri bilaterally (49). Persistence of brain lesions on follow-up imaging (25, 49, 51) found in 12% of patients (3/25) is a proportion classically reported in various series of PRES.
Imaging analysis did not highlight a specific pattern for poisoning-associated PRES but reinforces the fact that PRES is neither only posterior nor always reversible.
Are Toxic PRES Different According to the Causative Agents?
Similarities
Neurological complications such as hemorrhage (16, 20, 30, 31, 36, 43), reversible cerebral vasoconstriction syndrome (16, 49), and infarction (28, 49) occurred independently of toxic etiology, i.e., kratom (20), alcohol (28, 30, 31), drug overdose (36, 49), and licorice (16, 43).
Vasoconstriction and endothelial dysfunction
Most of the pharmacological and toxicological agents involved in this review are known to induce either or both vasoconstriction and endothelial dysfunction. High alcohol concentrations have been associated with dose-related vasoconstriction and impaired dilatation of cerebral vessels (22). In addition, chronic alcoholism and long-term lithium exposure increase reactive oxygen species and nitric oxide in brain endothelial cells. This oxidative stress can induce endothelial dysregulation, leading to the BBB breakdown (27, 34). Cocaine, amphetamines, lysergic acid amide, mephedrone, kratom, and phenylpropanolamine have sympathetic and/or serotoninergic effects that cause vasoconstriction or vasculitis, leading to severe hypertension (36, 59).
In alcohol withdrawal, the hypothalamic–pituitary–adrenal system is stimulated, leading to increased levels of catecholamine and AVP, which can induce acute hypertension (27, 28). Similarly, the biologically active component of licorice, glycyrrhizic acid, inhibits 11 β-hydroxysteroid dehydrogenase, leading to hypervolemic hypertension (16). After snakebite envenomation and organophosphate severe poisoning, neurotoxins (14) and nicotinic stimulation (60), respectively, lead to autonomic dysregulation with massive release of catecholamines and angiotensin II. These effects, in combination with the presence of sympathetic denervated vasculature in the brain posterior area, may induce failure of the cerebral autoregulatory system (14). The increase in proinflammatory mediators, either exogenous, originating from the substance (e.g., venom itself), or endogenous (e.g., in acute alcoholic pancreatitis, induced by venom), can damage the BBB and is likely to cause the leakage of blood contents into the surrounding brain tissue (14, 30).
Cerebral hypoperfusion
In several reports, angiography showed multiple areas of narrowing of the intracranial arteries (16, 28, 36, 37, 49), especially in drug overdose (36, 37, 49) with sympathomimetic agents such as ephedrine (49) and phenylpropanolamine (36). Interestingly, in ephedrine overdose–induced PRES (49), although MRI revealed bilateral superior parietal lesions, single-photon emission computed tomography showed selective hypoperfusion in the left superior parietal region.
AVP axis hyperstimulation
A recent review highlighted that AVP overstimulation seems to be involved in PRES development and subsequent symptoms, in particular because of both its pathophysiological mechanism in brain edema formation and its involvement in most PRES etiologies (5). AVP hypersecretion could be the trigger of PRES through a dysregulation of ionic/water transglial flux via astrocytic ion channel dysfunction and subsequent brain edema. In the periphery, AVP receptor stimulation could be responsible for symptoms usually reported in PRES such as hyponatremia, acute hypertension, and impaired renal function (5, 61). The use of cocaine, amphetamine (62), and lysergic acid diethylamide (63) and co-administration of alcohol with disulfiram (5) are known situations to stimulate AVP neurons. Thus, these agents could be directly responsible for the pharmacological cascade described above. In several cases, patients received multiple psychotropic drugs such as quetiapine (20, 33, 34), duloxetine (33), sertraline (33), amitriptyline (33), escitalopram (51), and valproate (51); it could be argued that these drugs, known to induce AVP release (64) and cerebrovascular effects, may serve as a contributing factor in the genesis of PRES.
In hepatic encephalopathy, in addition to dysregulation of cerebral blood flow and consequent cerebral vasodilation induced by hyperammonemia (32), ammonia reaching the astrocytes is detoxified in glutamine, and its overproduction promotes, through AVP stimulation, astrocytic swelling, resulting in brain edema (65). In contrast, acute alcohol intoxication (62) and licorice (66) inhibit AVP release, and lithium inhibits renal effects of AVP (5). In PRES associated with alcohol withdrawal (26–28), licorice (44), and lithium intoxication (33, 34), the onset of neurological symptoms ranged from 2 to 9 days after intoxication; this chronology of events may suggest a rebound phenomenon on the AVP axis (5).
Specific Characteristics
Visual hallucinations have only been reported in concomitant administration of disulfiram with alcohol (22) and in alcohol withdrawal (26, 27). Visual hallucinations may be a symptom of delirium tremens but also occur in patients with PRES (2). In natural toxin–and chemical substance–associated PRES, seizure was the most frequent symptom, accounting for 67% (10/15) of cases (12–14, 16, 17, 38, 45–48). Similarly, alertness disorders were at the forefront (92%, 11/12) in alcohol-associated PRES (22–32).
Multiple risk factors in substance abuse patients
In substance abuse–related PRES, patients had several risk factors for PRES such as chronic hypertension (18, 19), chronic kidney disease (18, 19), and HIV infection (18). In these cases, the different risk factors should act synergistically on the different pathophysiological pathways leading to PRES. For instance, cocaine has the ability to synergistically increase the pathologic processes induced by HIV infection (18) including endothelial dysfunction and disruption of the BBB integrity. Interestingly, single nucleotide polymorphisms in AVP gene and AVP V1a receptor have been associated with drug abuse disorders (67), suggesting a different probability of PRES occurrence in patients with substance abuse.
In patients with multiple risk factors of PRES or in the context of multiple drug intake (20), causality assessment is difficult. In addition, combined drug intoxication also exposes to a risk of drug cocktail effect. As with drug–drug interactions, illicit drug–drug interactions can occur both at the pharmacodynamic (i.e., interactions in which drugs influence each other's effects directly) and pharmacokinetic level (i.e., modification of drug absorption, distribution, metabolism, or excretion). In pharmacodynamic illicit drug–drug interactions, the neurotoxicity and/or endothelial toxicity of both the drug and illicit drug act synergistically, which can promote the occurrence of PRES. Legriel et al. (21) reported a case of lysergic acid amide–induced PRES in a depressed patient treated with clomipramine. The analysis of urinary catecholamines and serotonin metabolites showed a massive sympathetic storm with high urinary serotonin levels, supporting the pharmacodynamic convergence of these two adrenergic and serotoninergic agents. Castillo et al. (20) reported a case of kratom-induced PRES in a patient on fluoxetine for depression with dextroamphetamine misuse. Kratom exerts α2-adrenoreceptor agonistic effects and is known to induce high blood pressure, particularly when combined with other drugs (68). Mitragynine, the major indole-based alkaloid of kratom, is extensively metabolized by hepatic cytochrome P450 (CYP) isoform 3A4 and 2D6 (69). Amphetamine metabolism primarily involves CYP2D6 (70). Fluoxetine and its main metabolite, norfluoxetine, are well-known inhibitors of CYP2D6 and CYP3A4, respectively (71). Taken together, a probable pharmacokinetic illicit drug–drug interaction occurred between mitragynine/dextroamphetamine and fluoxetine, causing overexposure in mitragynine and dextroamphetamine. This case of kratom/amphetamine interaction shares the pharmacological characteristics of PRES induced by clonidine, another α2-adrenoreceptor agonist, and dextroamphetamine overdose described by Minhaj et al. (35).
Coagulopathy
Characteristics of PRES associated with snake bite included normal blood pressure (38, 39, 42), coagulopathy (12, 38, 39), and respiratory failure (12, 38). The mechanism of PRES associated with snake venom does not appear to be related to direct toxic effects of the venom within the central nervous system, because venom proteins do not cross the BBB. Instead, neurological manifestations are most often related to blockage of the neuromuscular transmission, causing paralysis, and abnormalities in the coagulation cascade, producing cerebrovascular events (38).
A Lack of Standardization in Reported Data on Poisoning-Induced PRES
The assessment of the methodological quality of the cases showed that the data reported are very heterogeneous, with a median overall score of 5/10 (IQR 3–6). In addition, none of the case reports met the domain selection criteria (Supplementary Table 1). An unclear selection approach leaves the reader with uncertainty as to whether this is the whole experience of the researchers or only the most serious case, and suggests possible selection bias. As the scientific literature on PRES is almost exclusively represented by case series and case reports, we propose a checklist with various items that should at least be reported in case reports of substance-induced PRES (Supplementary Table 4). Indeed, it seems essential to standardize the reporting of outcome so that studies collecting a large amount of data can be conducted.
Conclusions
PRES in a context of poisoning does not exhibit a specific imaging pattern. The predominance of various anatomical implications outside the parieto-occipital lobes in PRES, including toxic etiologies, is a key message for clinicians and radiologists. The prevalence of the neurological symptoms was also consistent with the published literature on other etiologies of PRES. In addition to toxic exposure, one-third of patients had at least one other risk factor of PRES. Chronic hypertension (17%) was less frequent than reported in other causes of PRES.
As in iatrogenic PRES, toxicology cases do not always have a temporally close relationship. PRES occurring after 3 days seems to be more related to a rebound effect of poisoning, to secondary brain damage, or to complications related to the management of the poisoning, whereas a shorter period would support a direct link between the causative agent and PRES. Poisoned patients may have a lower threshold for developing PRES. It may also be caused by the convergence of various pathophysiological processes (e.g., high blood pressure, endothelial dysfunction, AVP axis overstimulation) induced directly by the poison and/or indirectly by acting in concert with other factors such as drug–drug interaction or hypomagnesemia that ultimately causes the cerebrovascular cascade leading to PRES.
Although less described, PRES in a context of poisoning, which shares most of the clinical and radiological characteristics of other etiologies, is not to be ignored. The characterization of the pathophysiological mechanisms is essential to individualize management according to the presence of risk factors and/or specific features of PRES. Standardization of data reported in future case series of substance-induced PRES is required in order to better characterize and thus manage this syndrome.
Data Availability Statement
Publicly available datasets were analyzed.
Author Contributions
BL, CS, and SE conceived the idea. BL wrote the manuscript and performed the selection and summary of published literature on PRES in clinical toxicology. DB, CV-V, CS, and SE helped to design, write, and revise the paper. CC contributed in improving the article, notably enriching the analysis of neuroimaging data.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2019.01420/full#supplementary-material
References
1. Toledano M, Fugate JE. Chapter 26 - Posterior reversible encephalopathy in the intensive care unit. In: Wijdicks EFM, Kramer AH, editors. Handbook of Clinical Neurology Critical Care Neurology Part II. Elsevier. (2017). p. 467–483. doi: 10.1016/B978-0-444-63599-0.00026-0
2. Legriel S, Pico F, Azoulay E. Understanding posterior reversible encephalopathy syndrome. In: Vincent, J-L, editor. Annual Update in Intensive Care and Emergency Medicine 2011, vol. 1. Berlin, Heidelberg: Springer Berlin Heidelberg. (2011). p. 631–53. doi: 10.1007/978-3-642-18081-1_56
3. Fugate JE, Rabinstein AA. Posterior reversible encephalopathy syndrome: clinical and radiological manifestations, pathophysiology, and outstanding questions. Lancet Neurol. (2015) 14:914–25. doi: 10.1016/S1474-4422(15)00111-8
4. Tetsuka S, Ogawa T. Posterior reversible encephalopathy syndrome: a review with emphasis on neuroimaging characteristics. J Neurol Sci. (2019) 404:72–9. doi: 10.1016/j.jns.2019.07.018
5. Largeau B, Le Tilly O, Sautenet B, Salmon Gandonnière C, Barin-Le Guellec C, Ehrmann S. Arginine vasopressin and posterior reversible encephalopathy syndrome pathophysiology: the missing link? Mol Neurobiol. (2019) 56:6792–806. doi: 10.1007/s12035-019-1553-y
6. Song T, Rao Z, Tan Q, Qiu Y, Liu J, Huang Z, et al. Calcineurin inhibitors associated posterior reversible encephalopathy syndrome in solid organ transplantation: report of 2 cases and literature review. Medicine. (2016) 95:e3173. doi: 10.1097/MD.0000000000003173
7. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) 62:e1–34. doi: 10.1016/j.jclinepi.2009.06.006
8. Grosjean J, Merabti T, Dahamna B, Kergourlay I, Thirion B, Soualmia LF, et al. Health multi-terminology portal: a semantic added-value for patient safety. Stud Health Technol Inform. (2011) 166:129–38. doi: 10.3233/978-1-60750-740-6-129
9. Murad MH, Sultan S, Haffar S, Bazerbachi F. Methodological quality and synthesis of case series and case reports. BMJ Evid Based Med. (2018) 23:60–3. doi: 10.1136/bmjebm-2017-110853
10. Seger D, Barker K, McNaughton C. Misuse of the naranjo adverse drug reaction probability scale in toxicology. Clin Toxicol. (2013) 51:461–6. doi: 10.3109/15563650.2013.811588
11. Mascolo A, Scavone C, Sessa M, di Mauro G, Cimmaruta D, Orlando V, et al. Can causality assessment fulfill the new European definition of adverse drug reaction? A review of methods used in spontaneous reporting. Pharmacol Res. (2017) 123:122–9. doi: 10.1016/j.phrs.2017.07.005
12. Kaushik JS, Chakrabarty B, Gulati S, Patel H, Lodha R, Pai G, et al. Unusual late neurological complication in a child after an Indian krait bite. Pediatr Neurol. (2014) 51:130–2. doi: 10.1016/j.pediatrneurol.2014.02.014
13. Marrone LCP, Marrone BF, Neto FK, Costa FC, Thomé GG, Aramburu MB, et al. Posterior reversible encephalopathy syndrome following a scorpion sting. J Neuroimaging. (2013) 23:535–6. doi: 10.1111/jon.12017
14. Rebahi H, Mouaffak Y, Dilai M-O, Haimeur N, Eladib A-G, Younous S. Posterior reversible encephalopathy syndrome in a child stung by Androctonus mauretanicus scorpion. J Stroke Cerebrovasc Dis. (2015) 24:e129–32. doi: 10.1016/j.jstrokecerebrovasdis.2014.12.007
15. Akinci E, Köylü R, Yortanli M, Gümüş H, Köylü Ö, Altintepe L, et al. Acute bismuth intoxication: acute renal failure, tonsillar ulceration and posterior reversible encephalopathy syndrome. Hong Kong J Emerg Med. (2015) 22:121–5. doi: 10.1177/102490791502200208
16. Chatterjee N, Domoto-Reilly K, Fecci PE, Schwamm LH, Singhal AB. Licorice-associated reversible cerebral vasoconstriction with PRES. Neurology. (2010) 75:1939–41. doi: 10.1212/WNL.0b013e3181feb299
17. Tassinari D, Bergamaschi R, Corsini I, Landini S, Romanin B, Ballarini E, et al. Posterior reversible encephalopathy syndrome associated with licorice consumption: a case report in a 10-year-old boy. Pediatr Neurol. (2015) 52:457–9. doi: 10.1016/j.pediatrneurol.2014.12.001
18. Bazuaye-Ekwuyasi E, Chow RD, Schmalzle S. An atypical subacute presentation of posterior reversible encephalopathy syndrome. J Community Hosp Intern Med Perspect. (2017) 7:269–74. doi: 10.1080/20009666.2017.1369381
19. Dasari V, Donohoe CD. Cocaine-induced posterior reversible encephalopathy syndrome (PRES): a case report and review of the literature. J Neuroimaging Psychiatry Neurol. (2018). doi: 10.17756/jnpn.2018-025
20. Castillo A, Payne JD, Nugent K. Posterior reversible leukoencephalopathy syndrome after kratom ingestion. Proc (Bayl Univ Med Cent). (2017) 30:355–7. doi: 10.1080/08998280.2017.11929647
21. Legriel S, Bruneel F, Spreux-Varoquaux O, Birenbaum A, Chadenat ML, Mignon F, et al. Lysergic acid amide-induced posterior reversible encephalopathy syndrome with status epilepticus. Neurocrit Care. (2008) 9:247–52. doi: 10.1007/s12028-008-9096-5
22. Bhagavati S, Choi J. Atypical cases of posterior reversible encephalopathy syndrome. Clinical and MRI features. Cerebrovasc Dis. (2008) 26:564–6. doi: 10.1159/000164556
23. Coppens S, Naeije G, Mavroudakis N. Posterior reversible encephalopathy syndrome following disulfiram intoxication. J Neurol. (2011) 258:1548–50. doi: 10.1007/s00415-011-5945-9
24. Srikrishna Nukala SN. Posterior reversible encephalopathy syndrome (PRES) following alcohol induced disulfuram toxicity. IOSR J Dental Med Sci. (2013) 7:16–8. doi: 10.9790/0853-0731618
25. Kim HS, Choi JY, Seo MR. Posterior reversible encephalopathy syndrome (PRES) in a chronic alcoholic patient after having steam bath: a case report. Brain Neurorehabil. (2014) 7:66. doi: 10.12786/bn.2014.7.1.66
26. Ishikawa H, Natsume N, Matsui K, Tsuda H. Acute alcohol withdrawal accompanied by posterior reversible encephalopathy syndrome. Psychiatry Clin Neurosci. (2013) 67:189–9. doi: 10.1111/pcn.12033
27. Mengi T, Seçil Y, Çoban A, Beckmann Y. [Posterior reversible encephalopathy syndrome triggerred by alcohol withdrawal]. Turk Psikiyatri Derg. (2017) 28:217–20. doi: 10.5080/u18397
28. Gill D, Zayac A, Goyes Ruiz V, Sheikh N, Bhardwaj A. Alcohol withdrawal induced posterior reversible encephalopathy syndrome. Hypertens Curr Concepts Ther. (2017) 1. doi: 10.15761/HCCT.1000105
29. Kimura R, Yanagida M, Kugo A, Taguchi S, Matsunaga H. Posterior reversible encephalopathy syndrome in chronic alcoholism with acute psychiatric symptoms. Gen Hosp Psychiatry. (2010) 32:447.e3–5. doi: 10.1016/j.genhosppsych.2009.11.006
30. Baek HS, Lee S-J. A case of posterior reversible encephalopathy syndrome associated with acute pancreatitis and chronic alcoholism. Gen Hosp Psychiatry. (2015) 37:192.e3–5. doi: 10.1016/j.genhosppsych.2014.12.004
31. Magno Pereira V, Marote Correia L, Rodrigues T, Serrão Faria G. Acute pancreatitis and posterior reversible encephalopathy syndrome: a case report. Acta Med Port. (2016) 29:567–71. doi: 10.20344/amp.7368
32. John ES, Sedhom R, Dalal I, Sharma R. Posterior reversible encephalopathy syndrome in alcoholic hepatitis: hepatic encephalopathy a common theme. World J Gastroenterol. (2017) 23:373–6. doi: 10.3748/wjg.v23.i2.373
33. Fitzgerald RT, Fitzgerald CT, Samant RS, Kumar M, Ramakrishniah R, Van Hemert R, et al. Lithium toxicity and PRES: a novel association. J Neuroimaging. (2015) 25:147–9. doi: 10.1111/jon.12094
34. Loens S, Conzen J, Welte GS, Scharn N, Schrader C, Weissenborn K. Reversible posterior leukoencephalopathy syndrome after withdrawal of antipsychotic medication in the context of lithium intoxication. Gen Hosp Psychiatry. (2015) 37:274.e3–5. doi: 10.1016/j.genhosppsych.2015.02.011
35. Minhaj FS, Schult RF, Dvorak P, Nacca N. Amphetamine and clonidine toxicity resulting in posterior reversible encephalopathy syndrome. Pediatr Emerg Care. (2019) doi: 10.1097/PEC.0000000000001819. [Epub ahead of print].
36. Kawanabe T, Tanaka R, Sakaguchi Y, Akiyama O, Shimura H, Yasumoto Y, et al. Posterior reversible encephalopathy syndrome complicating intracranial hemorrhage after phenylpropanolamine exposure. Neurol Med Chir. (2011) 51:582–5. doi: 10.2176/nmc.51.582
37. Weidauer S, Gaa J, Sitzer M, Hefner R, Lanfermann H, Zanella FE. Posterior encephalopathy with vasospasm: MRI and angiography. Neuroradiology. (2003) 45:869–76. doi: 10.1007/s00234-003-1059-0
38. Delgado ME, Del Brutto OH. Reversible posterior leukoencephalopathy in a venomous snake (Bothrops asper) bite victim. Am J Trop Med Hyg. (2012) 86:496–8. doi: 10.4269/ajtmh.2012.11-0610
39. Ibrahim AM, ElSefi TT, Ghanem M, Fayed AM, Shaban NA. A horned viper bite victim with PRES. Case Rep Neurol Med. (2017) 2017:1835796. doi: 10.1155/2017/1835796
40. Loh HH, Tan CHH. Acute renal failure and posterior reversible encephalopathy syndrome following multiple wasp stings: a case report. Med J Malaysia. (2012) 67:133–5.
41. Murphy T, Al-Sharief K, Sethi V, Ranger GS. Posterior reversible encephalopathy syndrome (PRES) after acute pancreatitis. West J Emerg Med. (2015) 16:1173–4. doi: 10.5811/westjem.2015.8.28347
42. Varalaxmi B, Ram R, Sandeep P, Siva Kumar V. Posterior reversible encephalopathy syndrome in a patient of snake bite. J Postgrad Med. (2014) 60:89–90. doi: 10.4103/0022-3859.128830
43. van Beers EJ, Stam J, van den Bergh WM. Licorice consumption as a cause of posterior reversible encephalopathy syndrome: a case report. Crit Care. (2011) 15:R64. doi: 10.1186/cc10040
44. Morgan RD, Chou SH, Stelfox HT. Posterior reversible encephalopathy syndrome in a patient following binge liquorice ingestion. J Neurol. (2011) 258:1720–2. doi: 10.1007/s00415-011-5995-z
45. O'Connell K, Kinsella J, McMahon C, Holian J, O'Riordan S. Posterior reversible encephalopathy syndrome (PRES) associated with liquorice consumption. Ir J Med Sci. (2016) 185:945–7. doi: 10.1007/s11845-014-1214-0
46. Zhou T, Huang F, Jiang H, Yao X. Posterior reversible encephalopathy syndrome with bad imaging of cerebral venous sinus: a case report. Commun Disord Deaf Stud Hearing Aids. (2016) 4:4. doi: 10.4172/2375-4427.1000165
47. Phatake R, Desai S, Lodaya M, Deshpande S, Tankasali N. Posterior reversible encephalopathy syndrome in a patient of organophosphate poisoning. Indian J Crit Care Med. (2014) 18:250–2. doi: 10.4103/0972-5229.130580
48. Du G, Yang X, Du X. Posterior reversible encephalopathy syndrome following multiple wasp stings: a case report. Int J Clin Exp Med. (2017) 10:1446–8. Available online at: http://www.ijcem.com/files/ijcem0038214.pdf
49. Kinno R, Ohashi H, Mori Y, Shiromaru A, Ono K. Agraphia of the left hand with dysfunction of the left superior parietal region without callosal lesions. eNeurologicalSci. (2018) 10:16–8. doi: 10.1016/j.ensci.2018.01.005
50. Omer TA, Doherty C. Posterior reversible encephalopathy syndrome (PRES) complicating the “legal high” mephedrone. BMJ Case Rep. (2011) 2011. doi: 10.1136/bcr.02.2011.3904
51. Mann G, Gunja N. Paracetamol overdose complicated by posterior reversible encephalopathy syndrome (PRES). Clin Toxicol. (2019) 58:68–70. doi: 10.1080/15563650.2019.1609023
52. Tantikittichaikul S, Ruthirago D, Ali S, Claudio A, Jongyeol K. Posterior reversible encephalopathy syndrome with multiple cerebellar mass-like lesions secondary to amphetamine. Neurology. (2016) 86(Suppl. 16). Available online at: https://n.neurology.org/content/86/16_Supplement/P4.403
53. Chen T-H, Lin W-C, Tseng Y-H, Tseng C-M, Chang T-T, Lin T-J. Posterior reversible encephalopathy syndrome in children: case series and systematic review. J Child Neurol. (2013) 28:1378–86. doi: 10.1177/0883073813500714
54. Ellis CA, McClelland AC, Mohan S, Kuo E, Kasner SE, et al. Cerebrospinal fluid in posterior reversible encephalopathy syndrome: implications of elevated protein and pleocytosis. Neurohospitalist. (2019) 9:58–64. doi: 10.1177/1941874418802061
55. Datar S, Singh TD, Fugate JE, Mandrekar J, Rabinstein AA, et al. Albuminocytologic dissociation in posterior reversible encephalopathy syndrome. Mayo Clin Proc. (2015) 90:1366–71. doi: 10.1016/j.mayocp.2015.07.018
56. Sarbu N, Shih RY, Jones RV, Horkayne-Szakaly I, Oleaga L, et al. White matter diseases with radiologic-pathologic correlation. Radiographics. (2016) 36:1426–47. doi: 10.1148/rg.2016160031
57. Gao B, Lyu C, Lerner A, McKinney AM. Controversy of posterior reversible encephalopathy syndrome: what have we learnt in the last 20 years? J Neurol Neurosurg Psychiatry. (2018) 89:14–20. doi: 10.1136/jnnp-2017-316225
58. Saad AF, Chaudhari R, Wintermark M. Imaging of atypical and complicated posterior reversible encephalopathy syndrome. Front Neurol. (2019) 10:964. doi: 10.3389/fneur.2019.00964
59. King A, Dimovska M, Bisoski L. Sympathomimetic toxidromes and other pharmacological causes of acute hypertension. Curr Hypertens Rep. (2018) 20:8. doi: 10.1007/s11906-018-0807-9
60. Vale A, Lotti M. Organophosphorus and carbamate insecticide poisoning. Handb Clin Neurol. (2015) 131:149–68. doi: 10.1016/B978-0-444-62627-1.00010-X
61. Wong So J, Largeau B, Beau-Salinas F, Ehrmann S, Magni C, Meunier J. Pazopanib-induced posterior reversible encephalopathy syndrome with possible syndrome of inappropriate secretion of antidiuretic hormone: an incidental or pathophysiological association? Neural Regen Res. (2020) 15:1166–8. doi: 10.4103/1673-5374.270420
62. Godino A, Renard GM. Effects of alcohol and psychostimulants on the vasopressin system: behavioural implications. J Neuroendocrinol. (2018) 30:e12611. doi: 10.1111/jne.12611
63. Kies MW, Horst D, Evarts EV, Goldstein NP. Antidiuretic effect of lysergic acid diethylamide in humans. AMA Arch Neurol Psychiatry. (1957) 77:267–9. doi: 10.1001/archneurpsyc.1957.02330330053006
64. Shepshelovich D, Schechter A, Calvarysky B, Diker-Cohen T, Rozen-Zvi B, Gafter-Gvili A. Medication-induced SIADH: distribution and characterization according to medication class. Br J Clin Pharmacol. (2017) 83:1801–7. doi: 10.1111/bcp.13256
65. Park J, Masaki T, Mezaki Y, Yokoyama H, Nakamura M, Maehashi H, et al. Alpha-1 antichymotrypsin is involved in astrocyte injury in concert with arginine-vasopressin during the development of acute hepatic encephalopathy. PLoS ONE. (2017) 12:e0189346. doi: 10.1371/journal.pone.0189346
66. Schambelan M. Licorice ingestion and blood pressure regulating hormones. Steroids. (1994) 59:127–30. doi: 10.1016/0039-128X(94)90089-2
67. Randesi M, Levran O, Correa da Rosa J, Hankins J, Rule J, Kreek MJ, et al. Association of variants of arginine vasopressin and arginine vasopressin receptor 1A with severe acetaminophen liver injury. Cell Mol Gastroenterol Hepatol. (2017) 3:500–5. doi: 10.1016/j.jcmgh.2017.01.008
68. Michael White C. Pharmacologic and clinical assessment of kratom. Am J Health Syst Pharm. (2018) 75:261–7. doi: 10.2146/ajhp161035
69. Kamble SH, Sharma A, King TI, León F, McCurdy CR, Avery BA. Metabolite profiling and identification of enzymes responsible for the metabolism of mitragynine, the major alkaloid of Mitragyna speciosa (kratom). Xenobiotica. (2018) 49:1279–88. doi: 10.1080/00498254.2018.1552819
70. Krishnan S, Moncrief S. An evaluation of the cytochrome p450 inhibition potential of lisdexamfetamine in human liver microsomes. Drug Metab Dispos. (2007) 35:180–4. doi: 10.1124/dmd.106.011973
Keywords: leukoencephalopathy syndrome, hypertensive encephalopathy, blood–brain barrier, substance abuse, alcohol, poisoning
Citation: Largeau B, Boels D, Victorri-Vigneau C, Cohen C, Salmon Gandonnière C and Ehrmann S (2020) Posterior Reversible Encephalopathy Syndrome in Clinical Toxicology: A Systematic Review of Published Case Reports. Front. Neurol. 10:1420. doi: 10.3389/fneur.2019.01420
Received: 06 July 2019; Accepted: 30 December 2019;
Published: 12 February 2020.
Edited by:
Bo Gao, Affiliated Hospital of Guizhou Medical University, ChinaReviewed by:
Andrea Bink, University Hospital Zürich, SwitzerlandMehmet Akif Topçuoglu, Hacettepe University, Turkey
Copyright © 2020 Largeau, Boels, Victorri-Vigneau, Cohen, Salmon Gandonnière and Ehrmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bérenger Largeau, YmVyZW5nZXIubGFyZ2VhdUBldHUudW5pdi10b3Vycy5mcg==
†ORCID: Bérenger Largeau orcid.org/0000-0002-6824-7283
David Boels orcid.org/0000-0001-5599-9593
Caroline Victorri-Vigneau orcid.org/0000-0002-3745-2532
Clara Cohen orcid.org/0000-0002-8200-2784
Charlotte Salmon Gandonnière orcid.org/0000-0001-7675-9564
Stephan Ehrmann orcid.org/0000-0001-6221-4467