
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 10 April 2019
Sec. Multiple Sclerosis and Neuroimmunology
Volume 10 - 2019 | https://doi.org/10.3389/fneur.2019.00337
 Emanuele D'Amico1*†
Emanuele D'Amico1*† Clara G. Chisari1†
Clara G. Chisari1† Sebastiano Arena1Aurora Zanghì1Simona Toscano1Salvatore Lo Fermo1Davide Maimone2Marine Castaing3Salvatore Sciacca3Mario Zappia1Francesco Patti1*
Sebastiano Arena1Aurora Zanghì1Simona Toscano1Salvatore Lo Fermo1Davide Maimone2Marine Castaing3Salvatore Sciacca3Mario Zappia1Francesco Patti1*Introduction: The complexity of understanding cancer risk in MS is increased by inconsistencies in study design, and the lack of age-, sex-, and ethnicity-specific risk estimates. Aims of our study were to estimate the incidence of cancers in the MS population of Catania (Italy) and to evaluate the impact of disease-modifying treatments (DMTs) in cancer risk.
Materials and Methods: We screened 2,730 PwMS according to the MS criteria of Mc Donald 2010 referring to MS center of Catania in the period between 2003 and 2013. We matched database of MS patients with the Integrated Cancer of Catania-Messina-Siracusae-Enna. We calculated age and sex specific standardized incidence ratios (SIR) and the relative risk (RR) of developing cancer in MS patients treated with at least two different DMTs compared to who received one or no treatment.
Results: Out of 2,730, 1,180 MS patients (67.1% females; mean age 41.2 ± 12.9) were enrolled. We found 36 cancers. Global SIR was 1.18 (CI95% 0.78–1.58), with a significantly higher risk in men with a range age of 20 to 50 years [2.84; (CI95% 1.59–4.09)] and in women over 50 years [1.82 (CI95% 1.08–2.55)]. RR of developing cancer was 1.99 (CI95% 1.14–3.45) in MS patients switching one DMT and 3.38 (CI95% 1.83–6.22) in who switched at least twice.
Discussion: Our results demonstrated that cancer risk was not increased in our MS population; but age and sex different distribution may partly drive cancer risk. Higher cancer risk in MS patients switching more than two DMTs should take into account in treatment decision making.
Multiple Sclerosis (MS) is a severe acquired autoimmune neurodegenerative disease of the central nervous system (CNS) with extremely variable disease course, that usually affects persons in their third/four decades of life, even if late onset is described (1). Women had a prevalence/incidence rate approximately double than men (2, 3). In Italy, the MS prevalence ranged from 122 to 232 cases/100,000 in the mainland and Sicily, with an average of more than 109,000 MS patients in Italy (4) and an incidence of 7.0 cases /100,000 in Catania in Sicily (5).
It was suggested that MS and cancer may share some aberrant functions of immune system (6).
Indeed, in MS there is an alteration of the function of regulatory T cells (Tregs), or suppressor T cells, modulating the immunoreaction by suppressing the activation of the immune system (7). Regarding tumorigenesis, Tregs may either promote tumor growth by impeding immune surveillance, or may inhibit the growth of certain malignancies with inflammatory features (8, 9). As it is well-known that the immune system plays an important role in cancer, it is also plausible that cancer risk is modified by auto-immune diseases such as MS. It was also hypothesized that some immunological characteristics of MS disease activity could improve antitumor surveillance (10). Indeed, autoimmunity is a form of hypervigilance against self-antigens and is one of the mechanisms leading to the development of MS [11]. Following this theory, antitumor immunosurveillance should provide a physiological explanation for a reduced cancer risk in MS patients (11–14), but conflicting data exist (15, 16).
In the last 10 years, we have witnessed to great changes in the therapeutic scenario of the MS (17). Currently, available disease modifying treatments (DMTs) are able to ameliorate the course of the disease, by reducing the inflammatory activity (new clinical relapse and new radiological inflammatory lesions at brain and spine) of the immune system (18). However, the impressive results in term of controlling the disease activity by the new DMTs were accompanied by more severe safety concerns and, among them, the raised cancer incidence during the use of such drugs (teriflunomide, dimethyl fumarate, fingolimod, alemtuzumab, cladribine, and ocrelizumab) (19). In particular, cancer risk related to immunosuppressive (IS) treatments used for MS has been widely explored showing an increase cancer incidence in these patients (19, 20), but the relationship between the disease and cancer, as well as the safety profile of MS immune treatments (19, 21–24) have been not fully understood (10, 25, 26). For all these reasons, a reappraisal of cancer risk in real word MS studies (outside of the reality of clinical trials) is timely.
We aimed to compare cancer incidence among persons affected by MS to that in the general population settled in the geographic area of Catania (Italy). Moreover, we evaluated any correlation among DMTs use and cancer development.
An observational retrospective analysis of prospectively collected data of patients with MS was performed at our tertiary MS center of Catania, Italy. Catania, Italy, is the second populated (1,112.328 inhabitants) and largest province of Sicily, Italy (182.90 km2) (www.interno.gov.it)1.
Patients were prospectively included using a computerized database, iMed software (iMed, Merck Serono SA; Geneva). We screened all patients who received their diagnosis between January 1st, 2003 and June 31th, 2013. Once entered the clinics, patients were followed up prospectively with at least one scheduled visit per year.
Inclusion criteria were: (a) age ≥18 years; (b) lived in the city of Catania; (c) diagnosis of MS according to the Mc Donald criteria (27); (d) at least one follow-up visit performed in the Multiple Sclerosis Center of the “Policlinico Vittorio Emanuele” of Catania in the index window.
About the DMTs use, we stratified our MS cohort according to the number of switch MS treatment (the change of treatment during to MS course due to inefficacy or safety alert):
A) “no DMTs” group including patients not treated with any DMT in their MS history;
B) “no switch” group including patients treated with only one DMT in their MS history;
C) “1 switch” group including patients who experienced one therapeutic switch;
D) “≥2 switches” group including patients who experienced at least two switches.
The study protocol was approved by the local ethics committee (Comitato Etico Catania 1) (19/2017/PO on 6th July 2017). All patients provided written informed consent. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and with the appropriate national regulations.
At the time of first visit in our center, in our clinical practice for each patient, we collected the following clinical data: data of disease onset, MS clinical course, type and duration of DMTs, different switch strategy, total number of relapses, disability level assessed by Expanded Disability Status Scale (EDSS).
Oncological data regarding cancers occurred after diagnosis. We included in our analysis oncological diagnosis occurred at least 2 years after the MS diagnosis. Main groups of cancers were considered: brain and nervous system, breast, bones and joints, digestive system, endocrine system, eye and orbit, female genital system, male genital system, oral cavity and larynx, respiratory system, skin, urinary system and lymphoma-myeloma-hematopoietic or lymphatic cancer of MS were collected. We matched such data with the data of Integrated Cancer Registry of Catania-Messina-Siracusae-Enna, considering all during the observation period. We calculated age and sex specific standardized incidence ratios (SIR), as measure of the relative cancer risk.
We aimed to investigate the cancer incidence among persons affected by MS to that in the general population settled in the geographic area of Catania and the relative risk (RR) of developing cancer in MS patients treated with at least two different DMTs compared to who received one or no treatment (for this analysis we included all cancer cases occurring after at least 2 years from the DMT initiation).
We also examined whether the cancer risk was different in patients with different treatment strategy: induction strategy where immunosuppressive (IS) is followed by immunomodulatory (IM) treatment, and escalation strategy where IM drugs where followed by IS treatment. Those who used interferon beta and glatiramer acetate were classified into the IM group, and those who used methotrexate, mitoxantrone, fingolimod, and azathioprine were classified into IS group. Natalizumab were included in the IS group even if its mechanism of action is not typically immunosuppressive, but because it is considered as second-line therapy.
Skewness and kurtosis tests were applied to the continuous variables to confirm a normal distribution and results were expressed as means and standard deviations (SD). The Mann-Whitney test was used to compare continuous and categorical variables, and Pearson's chi-square test or Fisher's exact test was used to evaluate the categorical variables.
Overall, sex-specific and age-specific estimates were reported expressed in rates per 100.000 residents associated to their relative confidence intervals, or all cancers and for main groups of cancers. These estimates were compared to those present in the Integrated Cancer Registry, available for the same period through the calculation of the rate ratios.
SIR was calculated by dividing the number of observed cases of cancer by the numbers of expected cancer cases, represented a measure of the relative risk of cancer. Wald's test assuming a Poisson distribution of the observed cases was used for determining 95% confidence interval (CI) for SIR. All statistical analysis was performed by SPSS software (Version 22; SPSS Inc., Chicago, IL, USA). Unconditional logistic regression analysis were performed using binomial “cancer yes/no” as outcome; we considered age, sex, disease duration, MS type, baseline EDSS, DMT duration (in months) and number of switches as independent factors. In order to investigate the independent effect of a risk or protective factor after adjustment for one or several other factors or to adjust for confounding variables, we carried out a multivariate model. Multivariate analysis was performed with conditional logistic regression, adjusting in the model for clinical and genetic covariables that will be significantly different to univariate analysis between cases and controls (p-value < 0.10). The selection of the multiple regression model will be done with the “all possible models” approach, then a regression analysis will be performed for all possible combinations. The Likelihood ratio test will be used to compare the log-likelihood of the regression model in which the aforementioned variable has been excluded. In the same way, the possible interaction (Joint effect) between two variables (“test of the violation of the proportional odds”) will be evaluated. The “test for linear trend” and the “test for departure from linear trend” will be used for quantitative variables in order to evaluate a possible dose dependent effect (“linear or trend effect”).
Out of 2,730 patients screened 1,180 MS (67.1% females; mean age 41.2 ± 12.9) satisfied the inclusion criteria and were enrolled for the study (Table 1, Figure 1). The mean age at MS diagnosis was 32.8 ± 17.5 years with a median observation period of 9.1 years and 8,338 person-years (2,702.2 in males and 5,636.0 in females). Demographic characteristics and clinical features of studied patients were summarized in Tables 1, 2.
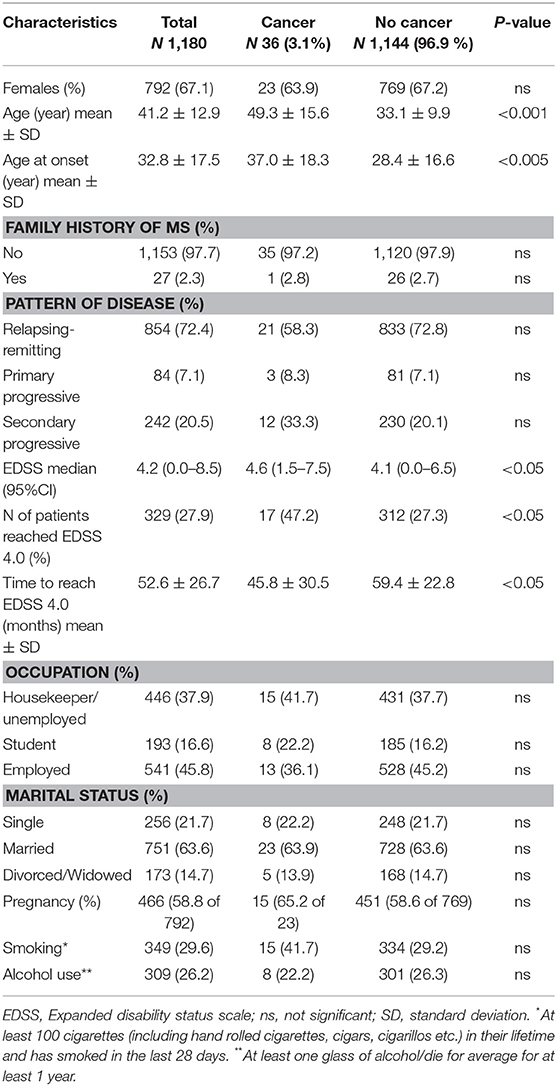
Table 1. Clinical and demographical characteristics of the study cohort.
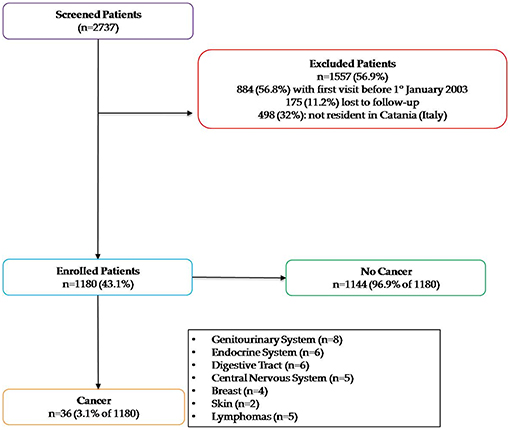
Figure 1. Study enrollment flowchart.
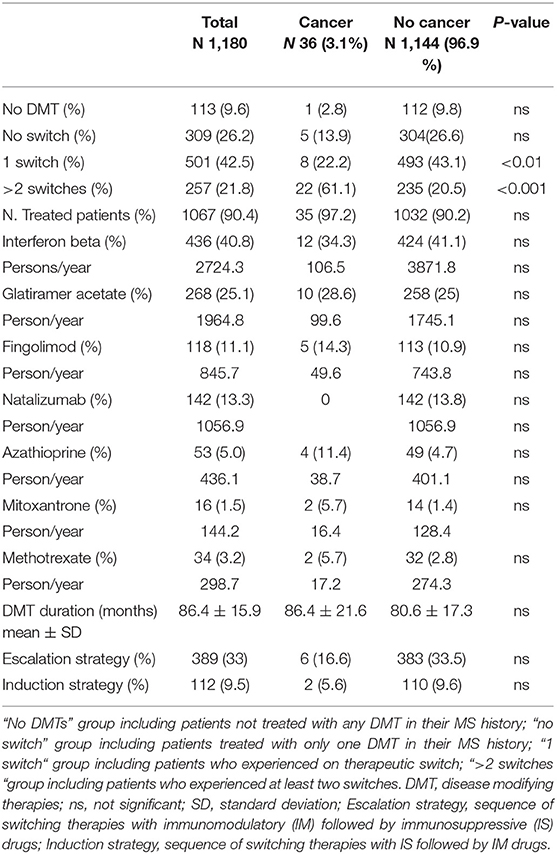
Table 2. Therapeutic characteristics of the cohort.
We found 36 cancers in 36 patients (3.1% of enrolled population). Global SIR of 1.18 (CI 95% 0.78–1.58) was obtained. Stratifying for age and sex, we found a significantly higher risk in men with the range age 20–50 years (2.84; CI 95% 1.59–4.09) and in women over 50 years (1.82; CI 95% 1.08–2.55) (Table 3).
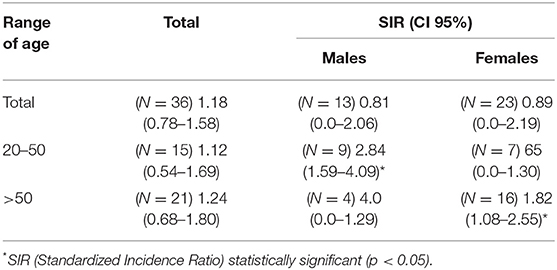
Table 3. Standardized incidence ratios.
About the 36 cancers, 8 (22.2%) were primary located in the genitourinary system (all bladder cancers), 6 (16.7%) thyroid cancers, 6 (16.7%) were colon cancers, 5 (13.9%) were of the CNS, 5 (13.9%) were lymphomas, 4 (11.1%) were breast cancers and 2 (5.6%) were melanomas. Further analyses with respect to the cancer sites in MS patients resulted in an increased risk of genitourinary cancer [SIR = 1.65 (95% CI, 1.34–2.35)], and for thyroid cancer [SIR = 1.32 (95% CI, 1.03–2.49)], but not for breast cancers [SIR = 1.17 (95% CI, 0.98–2.42)] and cancers which are located in nervous system [SIR = 1.03 (95% CI, 1.01–5.05)].
Patients with cancer were older than others (49.3 ± 15.6 vs. 33.1. ± 9.9, p < 0.001), with higher age at MS onset (37.0 ± 18.3 vs. 28.4 ± 16.6, p < 0.005). Moreover, MS patients with cancer had longer MS disease duration, worse disability (higher mean EDSS), that is an increased percentage of patients who got EDSS 4.0 (47.2 vs. 27.3%, p < 0.05) which means a limitation in ambulation (Tables 1, 2).
About DMTs use, the RR of developing cancer in “no DMTs” group was 1.03 CI 95% (0.56–1.41), in “no switch” group was 1.17 CI 95% (1.02–2.34), 1.99 (CI 95% 1.14–3.45) in MS patients who switched one DMT and 3.38 (CI 95% 1.83–6.22) in MS patients who switched at least twice.
The multivariate analysis showed that age, age at onset, disease duration, and more that 2 switches were associated with a higher risk of developing cancer (Table 4).
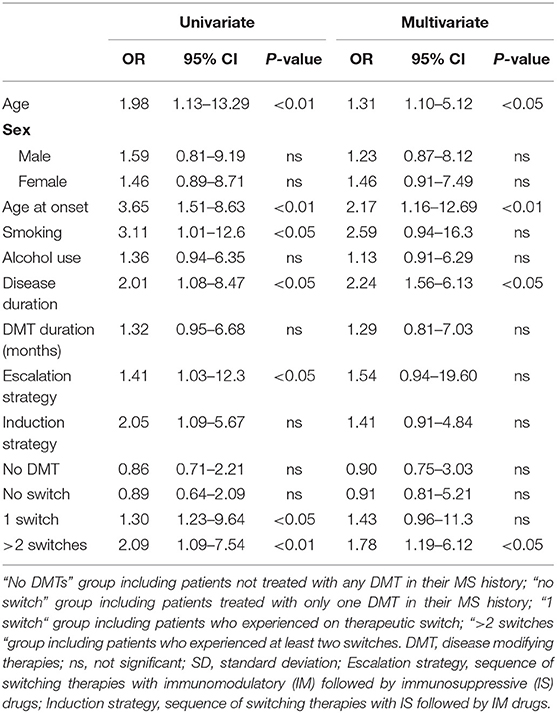
Table 4. Multivariate analysis.
Our results showed that incidence of cancer in our MS cohort was not higher than general population. However, we found a significantly higher incidence of cancer in men in the range age 20–50 years and in women over 50 years. Our MS patients who experienced at least two therapeutic switches DMTs had a higher risk for the development of cancers. Moreover, in our multivariate analysis, age, disease duration and more than 2 switches were associated with a higher cancer risk. As described above, data about MS and cancer risk are conflicting with a majority of these evidences suggesting that patients with MS are at reduced or at least not overall increased risk for the development of cancer (10, 16, 26, 28).
Our finding of a higher risk in younger men and older women in our MS population deserves attention. For most MS cohorts reported in the literature, there is no relevant difference in cancer risk between men and women (10, 24, 29, 30). It has been widely demonstrated that aging is able to drive degenerative diseases and hyperplastic pathology; indeed, it has been demonstrated that senescent cells are able to promote the development of a tissue microenvironment that is permissive for the cancer initiation and progression (31). Thus, we could speculate that any increase in cancer prevalence in such cohorts (men 20–50 and women over 50) could be influenced by several factors, such as hormonal change, that may drive cancer risk in these subpopulations (32). The gender difference in cancer sensibility is a consistent finding in cancer epidemiology studies. The expression of X-linked genes and sex steroid hormones interacting with specific receptors, may influence the immunological response to several stimuli, possibly resulting in the different male/female cancer risk incidence ratio (33). Indeed, the higher incidence of cancers in women over 50 years, may support these data, as the estrogens levels are typically reduced in this age range.
About cancer site, our data are in agree with the current literature, showing that, although the overall risk for malignancies in the MS patients does not seem to be increased, a possible raising of certain cancers such as breast cancer (11, 15) cancers of the CNS (15, 34), the urinary tract system and nasopharynx (15) was described. To better study such phenomenon, we should understand the pharmacokinetic of the administered drugs. In fact, the majority of molecules used for MS treatment have the ability to be retained (in the form of various metabolites) for extremely variable time in certain tissues (35). Indeed, about the genitourinary tract, some Authors found not significantly increase in bladder cancer risk (25). However, stratifying for sex and age, females patients with MS at the ages of 30 to 39 years and female patients with MS for more than 10 years exhibited an increased risk of bladder cancer, whereas in men the risk of bladder cancer was increased 1 to 9 years after MS diagnosis (25, 26).
An interesting data is the higher incidence of thyroid cancer in our cohort, not confirmed by other reports (36, 37). It has been well-described that thyroid cancer incidence is increased in volcanic area such as Catania (38, 39). However, this data could be explained by the immune-mediated inflammation of this organ that is a common comorbidity with MS (40).
A small but significantly increased risk of breast cancer in patients with MS was reported in a few studies; in detail a 1.6-fold (RR = 1.56) increased risk of breast cancer was found among a cohort of 11,817 MS patients (25, 41). The higher report of CNS tumors in the literature could be due to a misclassification of benign MS lesions, as explained in other studies (10, 42). Moreover, some Authors suggested that a potential surveillance bias could lead to more cases of meningioma in MS patients compared to the controls (43).
In our cohort, we demonstrated that the risk of cancer in patients who had received only one DMT was not increased, in line with other studies (22, 42, 44). A recent Italian study demonstrated that cancer risk was higher in MS patients with previous IS exposure compared with patients not exposed to IS, matched for age. In this study the risk of cancer in MS patients exposed to IS was related to the duration of exposure and the cumulative dose, but not to a specific IS (24). Conversely, we did not reply this result, but we found a higher cancer risk in MS patients switching more than two DMTs. This latter is in line with another study showing that RR of cancer in patients treated with only one immunomodulating drug was not increased, but it raised in patients treated with more than three immunomodulating drugs and/or IS (44). Thus, we may hypothesize that MS patients experiencing therapeutic failure with different immunomodulating and/or IS could have an enhanced risk of cancer because to being exposed to different molecules with different mechanisms of action may negatively influence the innate and adaptive immune systems and make these patients more sensitive of carcinogenesis (19, 26, 45).
Finally, we observed that MS patients with cancer diagnosis had a worse EDSS and got EDSS 4.0 faster compared to other MS patients. Indeed, it has been well-demonstrated that MS course depend not only on disease characteristics but also on several factors including comorbidities, as cancer (20, 46, 47). It has been demonstrated that mortality is increased in MS with psychiatric, cerebrovascular, cardiovascular, lung, diabetes, cancer, or Parkinson disease comorbidities (48). However, the impact of cancer diagnosis on the course of MS, as well as on life expectancy and of quality of life of MS patients, are not fully understood (46).
Our multivariate analysis showed that age, age at onset, disease duration and >2 switches, are associated with a higher cancer risk (Table 4). As for aging, it is also known that higher age at onset may expose patients to more frequent comorbidities (49) and, thus, to higher cancer risk as well. More interestingly, the higher risk in those patients switching twice may suggest that the mechanisms by which DMTs influence the immune system of MS patients are not fully understood and this may significantly impact the MS management leading to a more careful evaluation of the reasons to switching therapy.
Our study had several limitations. Firstly, the restricted area in which it was conducted may lead to a number of cancer cases that is too small to obtain conclusions for each cancer subtype. Moreover, we cannot exclude also the underestimation of the number of cancers due to the possible absence of follow-up or non-registered cancers. Secondly, we did not take into account data about the duration of DMTs exposure, as the cancer risk could be time-dependent. In addition, the intensity and duration of exposure of other factor as alcohol consumption, tobacco use, sun exposure, hormone therapy etc., need to be evaluated in the next studies, as the impact of dose is well-known for carcinogenesis. Moreover, we carried out our study in the period between 2003–2013, when dimethyl fumarate, teriflunomide, cladribine, alemtuzumab, and ocrelizumab were not available yet; hence, this could prevent us to understand the possible impact of these new drugs on carcinogenesis. A recent review showed that for dimethyl fumarate and teriflunomide an increased cancer risk was not demonstrated, whilst the use of alemtuzumab and cladribine require caution because of their potential risk of developing malignancies (19). However, real experience studies are needed in order to assess the cancer risk in patients treated with these molecules. Finally, other risk factors should be also explored in future studies (estrogen use, UV exposure, nutritional habits, body mass index, viral infections, etc).
In conclusion, our results suggest that some MS subpopulations may be more susceptible to the risk of develop cancer. The relationship between MS and risk of cancer is complex- Although the immune-mediated pathogenesis of MS enhancing the immune surveillance due to activation of inflammatory cells (23), may “protect” from carcinogenesis, on the other hand, current studies indicate that MS is largely a heterogeneous disease process, which involves a dysregulation of both innate and adaptive immune-mediated inflammatory mechanisms that ultimately contribute to demyelination and neurodegeneration (50). Thus, we could speculate that the dysregulation of the immune system typically responsible for the pathogenesis of MS disease, and the immunological consequences of using drugs with different mechanisms of action may enhance cancer risk.
Furthermore, the finding of higher cancers risk in patients who switched at least twice may have significant implications on MS management, influencing treatment decision making process. Indeed, our results raised the question of long-term toxicity of MS drugs, highlighting the importance of taking into account the consequences of a succession exposure to many different molecules, in particular with the development of new MS therapies more and more powerful.
More prospective researches are needed via epidemiology and experimental study designs to confirm these data.
This study was carried out in accordance with the recommendations of the Ethics Committee of Catania (Catania 1) with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Ethics Committee of Catania (Catania 1) (No. 19/2017/PO).
The results described in this paper were partially presented as poster presentation at ECTRIMS meeting, 25th−28th October 2017 Paris, France.
ED and CC contributed to data curation, and drafting, reviewing and editing the manuscript. SA contributed to data curation and investigation. AZ, ST, SLF, and DM contributed to data curation. MC contributed to data curation, methodology and formal analysis. SS contributed to data curation and formal analysis. MZ performed conceptualization, supervision and validation. FP contributed to the methodology, supervision, and reviewing, editing and validation of the manuscript.
ED received personal fees by Biogen and Sanofi Genzyme. He also received travel funding from Bayer, Biogen, TEVA, Sanofi Genzyme and Merck. CC received personal fees by Sanofi Genzyme. She also received travel funding from Bayer, TEVA, Sanofi Genzyme, Almirall, Novartis, Roche, Biogen, and Merck. AZ received travel funding from Bayer and Sanofi Genzyme. ST received travel funding from Biogen. SL received travel funding from from Bayer, TEVA, Sanofi Genzyme, Novartis, Biogen, and Merck. DM served on the advisory board for Bayer, Biogen, Merck, Novartis, Roche, Sanofi, TEVA, and also received personal fees for speaking activities at congresses or sponsored symposia. MZ has received honoraria for speaking activities by Bayer Schering, Biogen, Merck, Novartis, TEVA and Sanofi Aventis; he also served as advisory board member the following companies: Bayer Schering, Biogen, Merck, Novartis; he received grant for congress participation from Bayer Schering, Biogen Idec, Merck, Novartis, Sanofi Aventis and TEVA. FP has received honoraria for speaking activities by Bayer Schering, Biogen, Merck, Novartis, Roche, TEVA and Sanofi Aventis; he also served as advisory board member the following companies: Bayer Schering, Roche, Biogen, Merck, Novartis; he was also funded by Pfeizer and FISM for epidemiological studies; finally he received grant for congress participation from Bayer Schering, Roche, Biogen, Merck, Novartis, Sanofi Aventis, and TEVA.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. ^Censis Report. 42° Rapporto Censis sulla Società Italiana. (2008). Available online at: www.interno.gov.it (accessed April 27, 2017).
1. D'Amico E, Patti F, Zanghi A, Chisari CG, Lo Fermo S, Zappia M. Late-onset and young-onset relapsing-remitting multiple sclerosis: evidence from a retrospective long-term follow-up study. Eur J Neurol. (2018) 25:1425–31. doi: 10.1111/ene.13745
2. Compston A, Coles A. Multiple sclerosis. Lancet. (2008) 372:1502–17. doi: 10.1016/S0140-6736(08)61620-7
3. Confavreux C, Vukusic S. The clinical course of multiple sclerosis. Handb Clin Neurol. (2014) 122:343–69. doi: 10.1016/B978-0-444-52001-2.00014-5
4. Battaglia MA, Bezzini D. Estimated prevalence of multiple sclerosis in Italy in 2015. Neurol Sci. (2017) 38:473–9. doi: 10.1007/s10072-016-2801-9
5. Nicoletti A, Patti F, Lo Fermo S, Messina S, Bruno E, Quattrocchi G, et al. Increasing frequency of multiple sclerosis in Catania, Sicily: a 30-year survey. Mult Scler. (2011) 17:273–80. doi: 10.1177/1352458510386995
6. Cools N, Ponsaerts P, Van Tendeloo VF, Berneman ZN. Regulatory T cells and human disease. Clin Dev Immunol. (2007) 2007:89195. doi: 10.1155/2007/89195
7. Shevach EM. Regulatory T cells in autoimmmunity. Annu Rev Immunol. (2000) 18:423–49. doi: 10.1146/annurev.immunol.18.1.423
8. Dranoff G. The therapeutic implications of intratumoral regulatory T cells. Clin Cancer Res. (2005) 11:8226–9. doi: 10.1158/1078-0432.CCR-05-2035
9. Oleinika K, Nibbs RJ, Graham GJ, Fraser AR. Suppression, subversion and escape: the role of regulatory T cells in cancer progression. Clin Exp Immunol. (2013) 171:36–45. doi: 10.1111/j.1365-2249.2012.04657.x
10. Hofer S, Linnebank M, Weller M, Bahmanyar S, Montgomery SM, Hillert J, et al. Cancer risk among patients with multiple sclerosis and their parents. Neurology. (2010) 74:614–5; author reply 615. doi: 10.1212/WNL.0b013e3181c777b7
11. Midgard R, Glattre E, Gronning M, Riise T, Edland A, Nyland H. Multiple sclerosis and cancer in Norway. A retrospective cohort study Acta Neurol Scand. (1996) 93:411–5.
12. Swann JB, Smyth MJ. Immune surveillance of tumors. J Clin Invest. (2007) 117:1137–46. doi: 10.1172/JCI31405
13. Vesely MD, Kershaw MH, Schreiber RD, Smyth MJ. Natural innate and adaptive immunity to cancer. Annu Rev Immunol. (2011) 29:235–71. doi: 10.1146/annurev-immunol-031210-101324
14. Etemadifar M, Jahanbani-Ardakani H, Ghaffari S, Fereidan-Esfahani M, Changaei H, Aghadoost N, et al. Cancer risk among patients with multiple sclerosis: a cohort study in Isfahan, Iran. Caspian J Intern Med. (2017) 8:172–7. doi: 10.22088/cjim.8.3.172
15. Moller H, Kneller RW, Boice JD Jr. Olsen JH Cancer incidence following hospitalization for multiple sclerosis in Denmark. Acta Neurol Scand. (1991) 84:214–20.
16. Kyritsis AP, Boussios S, Pavlidis N. Cancer specific risk in multiple sclerosis patients. Crit Rev Oncol Hematol. (2016) 98:29–34. doi: 10.1016/j.critrevonc.2015.10.002
17. Vidal-Jordana A. New advances in disease-modifying therapies for relapsing and progressive forms of multiple sclerosis. Neurol Clin. (2018) 36:173–83. doi: 10.1016/j.ncl.2017.08.011
18. English C, Aloi JJ. New FDA-approved disease-modifying therapies for multiple sclerosis. Clin Ther. (2015) 37:691–715. doi: 10.1016/j.clinthera.2015.03.001
19. Lebrun C, Rocher F. Cancer risk in patients with multiple sclerosis: potential impact of disease-modifying drugs. CNS Drugs. (2018) 32:939–49. doi: 10.1007/s40263-018-0564-y
20. Marrie RA, Reider N, Cohen J, Stuve O, Trojano M, Sorensen PS, et al. A systematic review of the incidence and prevalence of cancer in multiple sclerosis. Mult Scler. (2015) 21:294–304. doi: 10.1177/1352458514564489
21. Lebrun C, Debouverie M, Vermersch P, Clavelou P, Rumbach L, de Seze J, et al. [CARIMS (Cancer Risk In Multiple Sclerosis) project: impact of long-term treatment]. Rev Neurol. (2007) 163:38–46.
22. Kingwell E, Evans C, Zhu F, Oger J, Hashimoto S, Tremlett H. Assessment of cancer risk with beta-interferon treatment for multiple sclerosis. J Neurol Neurosurg Psychiatry. (2014) 85:1096–102. doi: 10.1136/jnnp-2013-307238
23. Gaindh D, Kavak KS, Teter B, Vaughn CB, Cookfair D, Hahn T, et al. Decreased risk of cancer in multiple sclerosis patients and analysis of the effect of disease modifying therapies on cancer risk. J Neurol Sci. (2016) 370:13–7. doi: 10.1016/j.jns.2016.09.005
24. Ragonese P, Aridon P, Vazzoler G, Mazzola MA, Lo Re V, Lo Re M, et al. Association between multiple sclerosis, cancer risk, and immunosuppressant treatment: a cohort study. BMC Neurol. (2017) 17:155. doi: 10.1186/s12883-017-0932-0
25. Nielsen NM, Rostgaard K, Rasmussen S, Koch-Henriksen N, Storm HH, Melbye M, et al. Cancer risk among patients with multiple sclerosis: a population-based register study. Int J Cancer. (2006) 118:979–84. doi: 10.1002/ijc.21437
26. Kingwell E, Bajdik C, Phillips N, Zhu F, Oger J, Hashimoto S, et al. Cancer risk in multiple sclerosis: findings from British Columbia, Canada. Brain. (2012) 135 (Pt 10):2973–9. doi: 10.1093/brain/aws148
27. Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. (2011) 69:292–302. doi: 10.1002/ana.22366
28. Moisset X, Perie M, Pereira B, Dumont E, Lebrun-Frenay C, Lesage FX, et al. Decreased prevalence of cancer in patients with multiple sclerosis: a case-control study. PLoS ONE. (2017) 12:e0188120. doi: 10.1371/journal.pone.0188120
29. Fois AF, Wotton CJ, Yeates D, Turner MR, Goldacre MJ. Cancer in patients with motor neuron disease, multiple sclerosis and Parkinson's disease: record linkage studies. J Neurol Neurosurg Psychiatry. (2010) 81:215–21. doi: 10.1136/jnnp.2009.175463
30. Norgaard M, Veres K, Didden EM, Wormser D, Magyari M. Multiple sclerosis and cancer incidence: a Danish nationwide cohort study. Mult Scler Relat Disord. (2018) 28:81–5. doi: 10.1016/j.msard.2018.12.014
31. Campisi J. Aging, cellular senescence, and cancer. Annu Rev Physiol. (2013) 75:685–705. doi: 10.1146/annurev-physiol-030212-183653
32. Key TJ, Appleby PN, Reeves GK, Roddam A, Dorgan JF, Longcope C, et al. Body mass index, serum sex hormones, and breast cancer risk in postmenopausal women. J Natl Cancer Inst. (2003) 95:1218–26. doi: 10.1093/jnci/djg022
33. Dorak MT, Karpuzoglu E. Gender differences in cancer susceptibility: an inadequately addressed issue. Front Genet. (2012) 3:268. doi: 10.3389/fgene.2012.00268
34. Catala-Lopez F, Suarez-Pinilla M, Suarez-Pinilla P, Valderas JM, Gomez-Beneyto M, Martinez S, et al. Inverse and direct cancer comorbidity in people with central nervous system disorders: a meta-analysis of cancer incidence in 577,013 participants of 50 observational studies. Psychother Psychosom. (2014) 83:89–105. doi: 10.1159/000356498
35. Auricchio F, Scavone C, Cimmaruta D, Di Mauro G, Capuano A, Sportiello L, et al. Drugs approved for the treatment of multiple sclerosis: review of their safety profile. Expert Opin Drug Saf. (2017) 16:1359–71. doi: 10.1080/14740338.2017.1388371
36. Nuyen J, Schellevis FG, Satariano WA, Spreeuwenberg PM, Birkner MD, van den Bos GA, et al. Comorbidity was associated with neurologic and psychiatric diseases: a general practice-based controlled study. J Clin Epidemiol. (2006) 59:1274–84. doi: 10.1016/j.jclinepi.2006.01.005
37. Sun LM, Lin CL, Chung CJ, Liang JA, Sung FC, Kao CH. Increased breast cancer risk for patients with multiple sclerosis: a nationwide population-based cohort study. Eur J Neurol. (2014) 21:238–44. doi: 10.1111/ene.12267
38. Pellegriti G, De Vathaire F, Scollo C, Attard M, Giordano C, Arena S, et al. Papillary thyroid cancer incidence in the volcanic area of Sicily. J Natl Cancer Inst. (2009) 101:1575–83. doi: 10.1093/jnci/djp354
39. Malandrino P, Russo M, Ronchi A, Minoia C, Cataldo D, Regalbuto C, et al. Increased thyroid cancer incidence in a basaltic volcanic area is associated with non-anthropogenic pollution and biocontamination. Endocrine. (2016) 53:471–9. doi: 10.1007/s12020-015-0761-0
40. Niederwieser G, Buchinger W, Bonelli RM, Berghold A, Reisecker F, Koltringer P, et al. Prevalence of autoimmune thyroiditis and non-immune thyroid disease in multiple sclerosis. J Neurol. (2003) 250:672–5. doi: 10.1007/s00415-003-1053-9
41. Coldman A, Phillips N. Incidence of breast cancer and estimates of overdiagnosis after the initiation of a population-based mammography screening program. CMAJ. (2013) 185:E492–498. doi: 10.1503/cmaj.121791
42. Lebrun C, Debouverie M, Vermersch P, Clavelou P, Rumbach L, de Seze J, et al. Cancer risk and impact of disease-modifying treatments in patients with multiple sclerosis. Mult Scler. (2008) 14:399–405. doi: 10.1177/1352458507083625
43. Di Patre PL, Castillo V, Delavelle J, Vuillemoz S, Picard F, Landis T. “Tumor-mimicking” multiple sclerosis. Clin Neuropathol. (2003) 22:235–9.
44. Lebrun C, Vermersch P, Brassat D, Defer G, Rumbach L, Clavelou P, et al. Cancer and multiple sclerosis in the era of disease-modifying treatments. J Neurol. (2011) 258:1304–11. doi: 10.1007/s00415-011-5929-9
45. Handel AE, Ramagopalan SV. Multiple sclerosis and risk of cancer: a meta-analysis. J Neurol Neurosurg Psychiatry. (2010) 81:1413–4. doi: 10.1136/jnnp.2009.195776
46. Haussleiter IS, Brune M, Juckel G. Psychopathology in multiple sclerosis: diagnosis, prevalence and treatment. Ther Adv Neurol Disord. (2009) 2:13–29. doi: 10.1177/1756285608100325
47. Bsteh G, Ehling R, Lutterotti A, Hegen H, Di Pauli F, Auer M, et al. Long term clinical prognostic factors in relapsing-remitting multiple sclerosis: insights from a 10-year observational study. PLoS ONE. (2016) 11:e0158978. doi: 10.1371/journal.pone.0158978
48. Thormann A, Sorensen PS, Koch-Henriksen N, Laursen B, Magyari M. Comorbidity in multiple sclerosis is associated with diagnostic delays and increased mortality. Neurology. (2017) 89:1668–75. doi: 10.1212/WNL.0000000000004508
49. Awad A, Stuve O. Multiple sclerosis in the elderly patient. Drugs Aging. (2010) 27:283–94. doi: 10.2165/11532120-000000000-00000
Keywords: multiple sclerosis, cancer risk, disease modifying therapies, immunosuppressive drugs, switching therapies
Citation: D'Amico E, Chisari CG, Arena S, Zanghì A, Toscano S, Lo Fermo S, Maimone D, Castaing M, Sciacca S, Zappia M and Patti F (2019) Cancer Risk and Multiple Sclerosis: Evidence From a Large Italian Cohort. Front. Neurol. 10:337. doi: 10.3389/fneur.2019.00337
Received: 04 January 2019; Accepted: 19 March 2019;
Published: 10 April 2019.
Edited by:
Jorge Matias-Guiu, Complutense University of Madrid, SpainReviewed by:
Xavier Moisset, INSERM U1107 Douleur et Biophysique Neurosensorielle (Neuro-Dol), FranceCopyright © 2019 D'Amico, Chisari, Arena, Zanghì, Toscano, Lo Fermo, Maimone, Castaing, Sciacca, Zappia and Patti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emanuele D'Amico, ZW1hbnVlbGUuZGFtaWNvQHVuaWN0Lml0
Francesco Patti, cGF0dGlAdW5pY3QuaXQ=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.