 Maíra Glória de Freitas Cardoso1
Maíra Glória de Freitas Cardoso1 Rodrigo Moreira Faleiro2
Rodrigo Moreira Faleiro2 Jonas Jardim de Paula3
Jonas Jardim de Paula3 Arthur Kummer4
Arthur Kummer4 Paulo Caramelli5
Paulo Caramelli5 Antônio Lúcio Teixeira6
Antônio Lúcio Teixeira6 Leonardo Cruz de Souza7†
Leonardo Cruz de Souza7† Aline Silva Miranda8,9*† for the Minas Gerais' Traumatic Brain Injury Study Group
Aline Silva Miranda8,9*† for the Minas Gerais' Traumatic Brain Injury Study Group- 1Neuroscience Program, Laboratório Interdisciplinar em Investigação Médica, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 2Faculdade de Ciências Médicas de Minas Gerais, Fundação Hospitalar do Estado de Minas Gerais, Belo Horizonte, Brazil
- 3Faculdade de Ciências Médicas de Minas Gerais, Belo Horizonte, Brazil
- 4Laboratório Interdisciplinar em Investigação Médica, Eli Lilly and Company do Brasil, São Paulo, Brazil
- 5Departamento de Clínica Médica, Faculdade de Medicina da Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 6Santa Casa BH Ensino e Pesquisa, Neuropsychiatry Program, Department of Psychiatry and Behavioral Sciences, McGovern Medical School, University of Texas Health Science Center at Houston, Houston, TX, United States
- 7Laboratório Interdisciplinar em Investigação Médica, Departamento de Clínica Médica, Faculdade de Medicina da Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 8Laboratório Interdisciplinar em Investigação Médica, Faculdade de Medicina da Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 9Laboratório de Neurobiologia, Departamento de Morfologia, Instituto de Ciências Biológicas da Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
Patients with mild traumatic brain injury (mTBI) may present cognitive deficits within the first 24 h after trauma, herein called “acute phase,” which in turn may lead to long-term functional impairment and decrease in quality of life. Few studies investigated cognition in mTBI patients during the acute phase. The objectives of this study were to investigate the cognitive profile of patients with mTBI during the acute phase, compared to controls and normative data, and whether loss of consciousness (LOC), previous TBI and level of education influence cognition at this stage. Fifty-three patients with mTBI (aged 19–64 years) and 28 healthy controls participated in the study. All patients were evaluated at bedside within 24 h post-injury. Demographic and clinical data were registered. Cognitive function was assessed with the Mini-mental state examination (MMSE), the Frontal Assessment Battery (FAB), Digit Span (working memory), and the Visual Memory Test/Brief Cognitive Battery (for episodic memory). The clinical sample was composed mainly by men (58.5%). The mean age was 39 years-old and 64.3% of the patients had more than 8 years of education. The most common causes of mTBI were fall from own height (28.3%), aggression (24.5%), and fall from variable heights (24.5%). Compared to controls, mTBI patients exhibited significantly worse performance on MMSE, FAB, naming, incidental memory, immediate memory, learning, and delayed recall. Compared to normative data, 26.4% of patients had reduced global cognition as measured by the MMSE. Episodic memory impairment (13.2%) was more frequent than executive dysfunction (9.4%). No significant differences were found in cognitive performance when comparing patients with or without LOC or those with or without history of previous TBI. Patients with lower educational level had higher rates of cognitive impairment (VMT naming−28.6 vs. 4.2%; VMT immediate memory−32 vs. 4.2%; VMT learning−39.3 vs. 4.2%, all p < 0.05). In sum, we found significant cognitive impairment in the acute phase of mTBI, which was not associated with LOC or history of TBI, but appeared more frequently in patients with lower educational level.
Introduction
Traumatic brain injury (TBI) is a highly prevalent condition, affecting men and women of all ages and socioeconomic status worldwide (1, 2). The annual incidence of TBI is estimated in 295 for 100,000 people. Most TBIs occur in males and are mild (1). According to the World Health Organization, mild traumatic brain injury (mTBI) is defined as an acute brain injury resulting from external forces to the head that causes one or more of the following: confusion or disorientation; loss of consciousness (LOC) ≤30 min or other transient neurologic abnormalities; post-traumatic amnesia for <24 h; Glasgow Coma score ranging from 13 to 15 (3).
Patients with mTBI may experience cognitive deficits in the first hours following the trauma (4–7). It has been reported that at 3–5 days after injury, patients with mTBI performed significantly worse compared to orthopedically injured patients and healthy controls in different cognitive tasks, such as immediate recall, short-delayed recall, long-delayed recall, attention, working memory, processing speed and other executive functions (8–10). Importantly, some deficits may be detected even 1 year after the trauma (11).
Features such as loss of consciousness (LOC) or having a previous history of TBI seem to influence cognitive performance in patients with mTBI (12–15). A history of repetitive mTBI was associated with deficits in delayed memory and executive function in a meta-analysis that investigated neuropsychological impact of multiple concussions (15). Previous TBI and LOC were also prognostic markers of persistent post-concussive symptoms after mTBI in deployed-veterans (16).
Although high-quality epidemiological data are scarce in Brazil (17), it has been estimated that there are around 125,000 hospital admissions due to TBI per year, with an incidence of 65.7 admissions per 100,000 inhabitants and a hospital mortality of 5.1/100,000/year (18). Beyond direct costs with hospital expenses, the reliable quantification of the burden caused by TBI is difficult to establish owing to inadequate standardization and incomplete data collection on the incidence and outcome of brain injury.
Only few studies investigated the cognitive status of mTBI patients during the first 24 h post-injury, herein called “acute phase,” and the factors possibly associated with cognitive performance in this early stage (4–7), such as LOC and previous TBI.
In the current study, we aimed to investigate the cognitive performance of patients with acute mTBI, compared to healthy controls and normative data, as well as to address whether LOC or history of TBI influence cognition and whether years of education might present a potential protective role in mTBI-associated cognitive impairment.
Methods
Study Design and Participants
The present study was conducted at João XXIII Hospital/Fundação Hospitalar do Estado de Minas Gerais (FHEMIG), a trauma reference center situated in Belo Horizonte, Minas Gerais, Brazil (Southeast), which has more than 500 trauma dedicated beds. In 2015, 1,862 TBI patients were admitted to this Trauma center, with a mortality rate of 34% in cases of severe TBI.
During a period of 30 days, two times a day (at 12 p.m. and 6 p.m.), all patients admitted to the hospital were registered. We included patients with mTBI (scores between 13 and 15 at the Glasgow Coma Scale—GCS (19)—at first evaluation at the emergency department), with < 24 h post-TBI, aged between 18 and 65 years-old, who agreed to participate by providing written informed consent. Patients with epilepsy, history of neurosurgery, dementia, skull fracture, penetrating injury, or any acute intracranial findings on brain scan were excluded. Demographic, clinical and neuropsychological data were obtained.
During the study period from November 10th to December 10th, 2016, 268 patients with TBI were admitted to the emergency department. One-hundred and 99 patients did not meet the inclusion criteria. From the 69 patients included, 15 were excluded for having skull fracture, suspected dementia, history of neurosurgery or findings in the brain scan. One patient was excluded because he could not complete the cognitive tasks. The final sample was composed by 53 patients (Figure 1). All patients were assessed at the bedside.
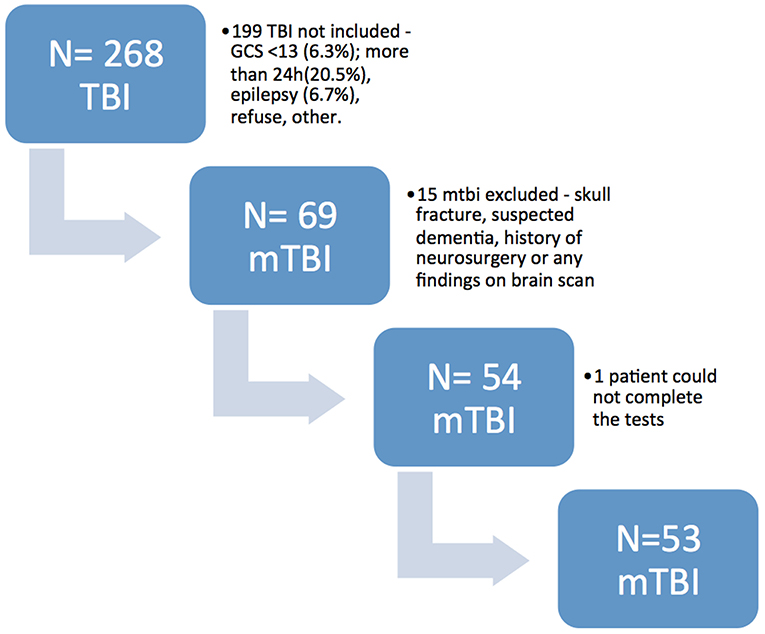
Figure 1. Flow diagram of patient's recruitment. TBI, traumatic brain injury; mTBI, mild traumatic brain injury.
This study was approved by the local ethics committees (protocol number CAAE: 49623015.0.0000.5149) and all patients provided written informed consent prior to study participation.
The control group was composed by 28 healthy participants recruited from the local community, aged between 18 and 65 years-old, who agreed to participate by providing written informed consent. Participants were included if they have no past history of TBI. Exclusion criteria were previous neurosurgery, neurodegenerative diseases, stroke, and epilepsy, other neurological disorders and/or cognitive decline (i.e., delirium or dementia) and significant sensory impairment.
Clinical Evaluation
All participants answered a sociodemographic and medical questionnaire. Cognitive performance was assessed with the following tests:
Mini Mental-State Examination—MMSE (20, 21)
This test evaluates global cognitive status. It includes tasks that evaluate temporal and spatial orientation, memory, attention, naming, following verbal and written commands, writing and copy.
Frontal Assessment Battery—FAB (22, 23)
This battery was designed to assess frontal lobe functions which mediate executive functioning. It contains six tasks that assess conceptualization and abstract reasoning, mental flexibility, motor programming, sensitivity to interference, inhibitory control and environmental autonomy.
Digit Span Subtest From the Wechsler WAIS-III (24)
This subtest is a number repetition task and is constituted by two tasks—digit span forward and digit span backward—which evaluate attention and working memory.
Episodic memory was assessed with the Visual Memory Test from the Brief Cognitive Battery—VMT (25, 26). This latter test consists of ten simple line drawings. Patients are asked to name the drawings and then an incidental recall is required. Drawings are shown again and patients are explicitly informed that they should memorize them. Patients undergo a new recall (immediate recall) and then the procedure is repeated (learning recall). Patients undergo an interference task and a delayed recall (5 min after) is required. The last procedure is a recognition task of the 10 original drawing among 10 distractors.
Statistical Analysis
Data analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 17 (SPSS Inc., Chicago, IL, USA). Descriptive data were analyzed in frequencies, mean, standard deviation, median and 25 and 75 percentiles. All variables were tested for normal distribution by employing the Shapiro-Wilk test.
Differences of sex distribution and educational level among groups were tested using Pearson Chi-square test for categorical data. Differences of age and neuropsychological performance between groups were tested using Mann-Whitney test. Pearson Chi-square test was used to compare frequencies between groups. Spearman's test was used to explore correlations among sociodemographic, clinical, and neuropsychological data. Cohen's d effect sizes were calculated for comparisons between clinical groups.
Deficit was defined as 2 standard deviations below test's normative data. The normative data provided different means and standard deviations according to the individual's educational level.
All statistical tests were two tailed and a significance level was set at 0.05.
Results
The final clinical sample was composed of 53 patients with mTBI (Figure 1). Sociodemographic and clinical features are shown in Table 1. The mTBI sample was composed mainly by men (58.5%) with a mean age of 39.1 years, ranging from 19 to 64 years. Most patients (92.5%) had a score of 15 at GCS and 64.3% had 8 or more years of education. The most frequent causes of TBI were fall from own height, accounting for 28.3% of cases, aggression (24.5%) and fall from variable heights (24.5%). Only 7.5% of mTBIs were caused by traffic accidents. Eleven patients (20%) reported alcohol consumption in the previous 12 h.
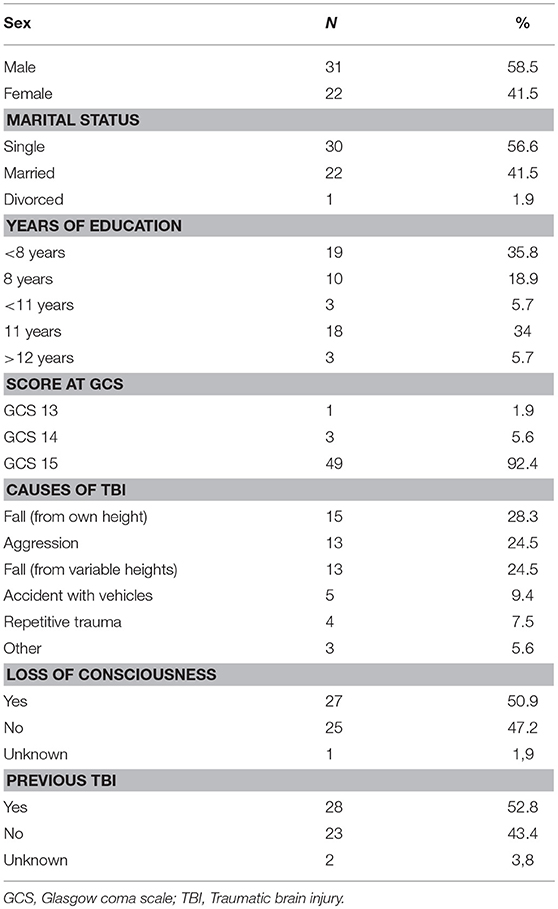
Table 1. Sociodemographic and clinical features of patients with acute mild traumatic brain injury.
Regarding cognitive performance, mTBI patients presented the following means and standard deviations: MMSE (mean = 23.8, SD = 4.1, n = 52), FAB (mean = 12.2, SD = 2.8, n = 53), Visual Memory Test naming (mean = 9.8, SD = 0.4, n = 53), VMT incidental memory (mean = 5.7, SD = 1.3, n = 52), VMT immediate recall (mean = 7.7, SD = 1.5, n = 52), VMT learning (mean = 8.2, SD = 1.5, n = 52), VMT delayed recall (mean = 7.5, SD = 1.7, n = 52), VMT recognition (mean = 9.9; SD = 0.3, n = 52), Digit Span Forward (mean = 4.7, SD = 1.0, n = 53) and Digit Span Backward (mean = 3.3, SD = 1.2, n = 53).
The healthy control group was composed by 28 participants aged between 18 and 63 years-old (mean = 39.4, SD = 12.8), 50% (N = 14) of the sample was composed by men, and 71% had 8 or more years of education. Controls showed the following means and standard deviations on cognitive tests: MMSE (mean = 27.2, SD = 2.1), FAB (mean = 13.6, SD = 3), Visual Memory Test naming (mean = 10), VMT incidental memory (mean = 7.1, SD = 1.5), VMT immediate recall (mean = 8.7, SD = 0.9), VMT learning (mean = 9.4, SD = 0.9), VMT delayed recall (mean = 9, SD = 1.1), VMT recognition (mean = 10), Digit Span Forward (mean = 5.2, SD = 1.3), and Digit Span Backward (mean = 3.5, SD = 0.7).
Controls had no significant differences from mTBI patients on age (p = 0.94), sex (p = 0.47), and years of education (p = 0.15). Comparison between groups' cognitive performance is shown on Table 2. Patients significantly differed from controls on MMSE (p < 0.001), VMT naming (p = 0.02), VMT incidental memory (p = 0.001), VMT immediate recall (p = 0.003), VMT learning (p < 0.001), VMT delayed recall (p < 0.001), and FAB (p = 0.047) scores. There were no significant differences between groups on VMT recognition, Digit Span forward and Digit Span backward scores.
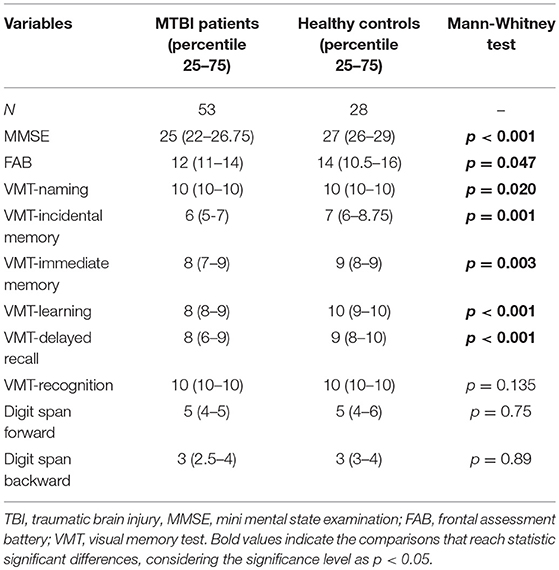
Table 2. Cognitive performance comparison between mTBI patients and healthy controls.
When compared to normative published data, 26.4% of patients showed deficit at MMSE and 9.4% at the FAB. In the Visual Memory Test, 17% exhibited deficits on naming, 3.8% (n = 2) on VMT incidental memory, 18.9% (n = 10) on VMT immediate recall, 22.6% (n = 12) on VMT learning, 13.2% (n = 7) on VMT delayed recall, and 7.5% (n = 4) at VMT recognition. There were no patients with deficits at the Digit Span test.
History of Previous TBI
In order to investigate whether a history of previous TBI influenced cognitive performance, patients with previous TBI (TBI+) was compared to those without a previous history of TBI (TBI-). The comparison is shown in Table 3. These data were available for 51 out 53 participants. Twenty and eight patients (54.9%) composed the TBI+ group and 23 (45%) the TBI- group. The groups were similar regarding sex (p = 0.76), age (p = 0.23), and years of education (p = 0.78). No significant differences were found between groups regarding cognitive performance (Table 3).
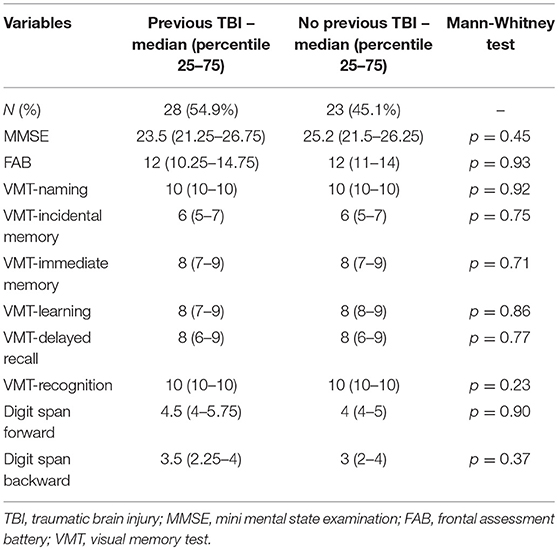
Table 3. Cognitive performance comparison between patients with and without previous TBI history.
Loss of Consciousness
In order to investigate whether loss of consciousness (LOC) influenced cognitive performance, patients who had LOC (LOC+) were compared to those without LOC (LOC–). The comparison is shown in Table 4. This information was available for 52 out 53 participants. Twenty and seven patients (51.9%) composed the LOC+ group and 25 (48%) the LOC– group. No significant differences regarding sex (p = 0.15) and years of education (p = 0.86) were found. There was a significant difference of age (p = 0.04; d = 0.588), with the LOC+ group (Mean = 43.2; SD = 13.6) being older than the LOC– group (Mean = 35.4; SD = 12.7). No significant difference was found between groups regarding cognitive performance (Table 4).
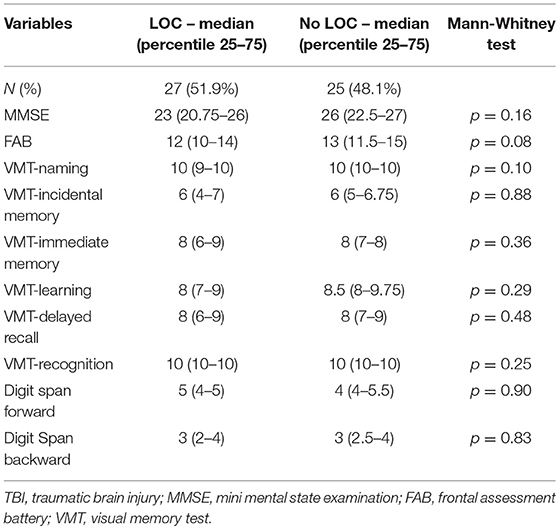
Table 4. Cognitive performance comparison between patients with and without loss of consciousness.
Years of Education
To investigate a potential protective role of years of education in mTBI-associated cognitive deficits, patients were divided into two groups and their scores compared. Twenty-nine patients (54.7%) had accomplished basic education or less (until 8 years of formal education) and 24 patients (45.3%) had accomplished more than 8 years of education. No significant differences regarding sex (p = 0.56) and age (p = 0.23) were observed. Significant differences were found in MMSE (≤8 years – median = 22; >8 years – median = 26; p < 0.01; d = 1.115), FAB (≤8 years – median = 12; >8 years – median = 14; p < 0.01; d = 1.094), Digit Span forward (≤8 years – median = 4; >8 years – median = 5; p < 0.01; d = 0.732) and Digit Span backward (≤8 years – median = 3; >8 years – median = 4; p < 0.02; d = 0.669). Differences were also significant in VMT naming (≤8 years – median = 10; >8 years – median = 10; p < 0.02; d = 0.672), VMT immediate memory (≤8 years – median = 7; >8 years – median = 8; p < 0.03; d = 0.638) and VMT learning (≤8 years – median = 8; >8 years – median = 8.5; p < 0.049; d = 0.567). No differences were found in VMT incidental memory (p < 0.26), VMT recall (p < 0.12), and VMT recognition (p < 0.38).
The frequency of impairment (i.e., more than 2 standard deviations below mean) between these two groups were also compared (Table 5). Significant differences were found between groups in VMT naming (p < 0.02; d = 0.679), VMT immediate memory (p < 0.01; d = 0.756) and VMT learning (p < 0.01; d = 0.913), with increased frequency of impairment in the group with ≤ 8 years of education.
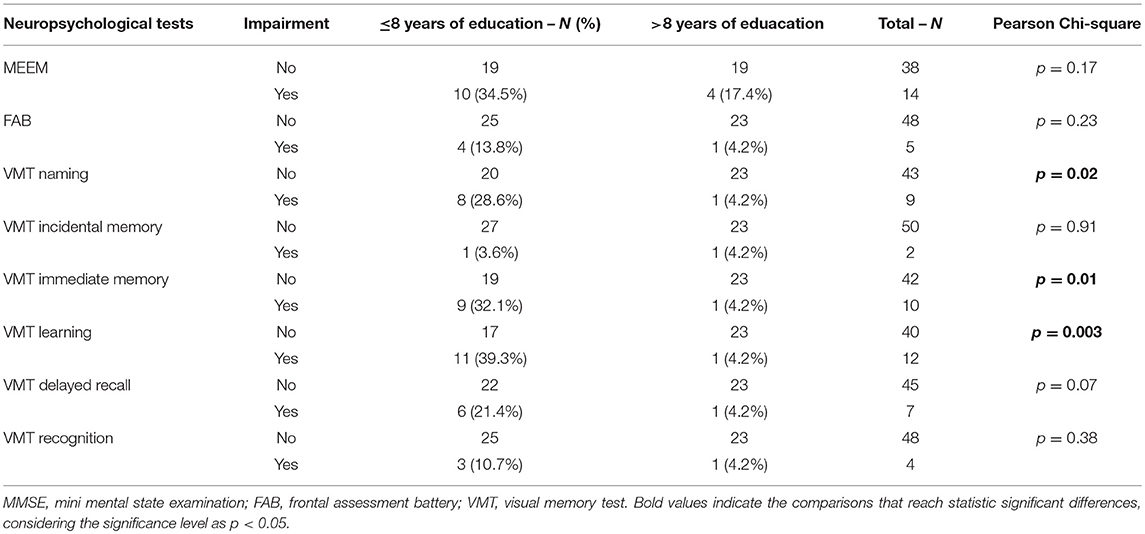
Table 5. Frequencies of cognitive deficits among mTBI patients according to education.
Correlations
We explored correlations between clinical variables (age, GCS, alcohol, and drugs) and neuropsychological tests among patients. Significant negative correlation was observed between age and VMT naming (r = −0.308; p < 0.02). GCS was positively correlated with FAB (r = 0.354; p < 0.009) and negatively with alcohol use (r = −0.372; p < 0.006).
As there was a difference of age between patients who had LOC and those who had not was found, we investigated whether age and LOC were correlated. Age significantly correlated with LOC (r = 0.285; p = 0.04). Moreover, when control group was included in the analysis of age and naming, the correlation remained significant (r = −237, p = 0.03).
Discussion
To the best of our knowledge, this is the first study to investigate the incidence of cognitive impairment following acute mTBI in a Brazilian population and to identify factors that may play a protective role at the acute phase. Previous Brazilian studies evaluated TBI-related cognitive deficits only in its chronic phase and with different severity (27–29).
We found cognitive dysfunction in a significant percentage of people with mTBI, especially in general cognitive ability (26.4%), learning memory (22.6%), and immediate memory (18.9%). Also, compared to a healthy control group, mTBI patients showed significantly worse cognitive performance on general cognitive ability, naming, incidental memory, immediate memory, learning memory, delayed recall, and executive functioning. Our findings are in agreement with previous studies that reported significant cognitive deficits in the acute phase of post-TBI, mainly associated with episodic memory (4–9). A meta-analysis also reported significant impairment in verbal and visual memories immediately after mTBI (30), thus supporting our data. Moreover, compared with healthy controls, patients with mTBI performed significantly worse in attention, memory, language and executive functions at acute phase of TBI and at 6 month follow-up (4). Neuropsychological measures at the acute phase were also significantly associated with changes in white matter integrity in brain regions such as the splenium of corpus callosum and cingulum (4). A more recent study showed impairment in selective attention/inhibitory control, divided attention, and working memory in acute mTBI (<7 days) (31). These deficits were associated with gray matter morphological changes (31). Taken together, these studies reinforce our findings by providing evidence of impairment in several cognitive domains in the acute phase of mTBI.
It has been reported that LOC might be associated with increased cognitive deficits following mTBI. For instance, military service members with blast-related mTBI with LOC presented severe memory impairment, sleep disorders, post-traumatic symptoms, and slow simple reaction times at 72 h post-brain injury (13). LOC was also associated with avoidance symptoms, worse quality of life and post-concussion symptoms in veterans with mTBI and comorbid PTSD (32). LOC might also influence cognitive outcome since uncomplicated mTBI patients without LOC presented early recovery compared with those who had LOC at 45 days following the TBI event (12). Patients who presented mTBI with LOC were more likely to present deficits in executive functions and associated disruption in white matter integrity in ventral prefrontal areas (14). We did not find significant differences in cognitive performance between mTBI patients with and without LOC at 24 h post-brain injury. Methodological differences, including an early time point evaluation (24 h post-mTBI) and the cognitive tests applied, might explain, at least in part, these results. In our study, we used mainly screening tests, while the above-mentioned studies used computerized tests or a more comprehensive neuropsychological assessment, which are more sensitive.
Similarly to LOC, we did not find any difference in the cognitive performance between patients with and without history of previous TBI. Our findings are in agreement with Comerford et al. (6) who reported that mTBI patients with history of previous TBI did not show lower cognitive performance than those without history. On the other hand, repetitive mTBIs have been associated with a worse outcome than a single, uncomplicated mTBI, often leading to long-term cognitive impairment and persistent post-concussive syndrome, which also includes somatic and emotional symptoms (15, 30, 33–36). It has been postulated that a single mTBI, without findings on brain scan, has a complete resolution after 3 months (15, 30, 35). However, this does not seem to be true for all mTBI cases since cognitive and behavioral changes have been reported longer than 3 months after a single traumatic event (10, 37). Similarly to the LOC results, these controversial findings might also be at least in part explained by different methodological approaches.
Years of education seem to influence cognitive performance following acute mTBI since patients with 8 years or less of education showed a higher frequency of deficits in the cognitive tests compared with those with higher educational levels. These findings support a protective role of education in cognitive decline associated with mTBI. Similar to our findings, Sumowski et al. (38) found that higher educational level attenuated the deleterious effects of TBI. Individuals with moderate to severe TBI and higher educational attainment performed better in cognitive tests than TBI patients with low educational attainment. As observed by Leary et al. (39), years of education were associated with measures of memory, learning, working memory and processing speed in patients with TBI. Education is one of the factors that constitute the so-called “cognitive reserve,” a protective factor associated with better TBI outcome. Indeed, a meta-analysis showed that higher education and higher pre-morbid IQ were found to be associated with better outcomes following TBI (40). Conversely, lower levels of cognitive reserve, as measured by educational attainment, premorbid IQ and occupational skill level, were associated with worse recovery, higher risk for post-concussive symptoms in mTBI patients 3 months after injury (41). Together, these findings support that education is a protective factor against TBI, and our findings indicate that education may be a protective factor at early stages of mTBI, as in the first 24 h.
It is worth mentioning that other characteristics such as baseline GCS may also influence TBI-associated cognitive impairment. Dikmen et al. (36) found that patients with GCS of 15 and abnormal findings on CT presented significant impairment in episodic memory and functional outcome. Cognitive performance was even more impaired in patients with GCS 13-14 and abnormal CT findings, with significant deficits in episodic memory, attention, inhibitory control, cognitive flexibility, processing speed, motor performance, verbal intelligence, and functional outcome (36). In the current study, the GCS was 15 for the majority of the patients (92.4%) and those with abnormal findings on CT were excluded, suggesting that other features like years of education might be taken into account in order to better characterize cognitive functions in acute mTBI population.
In the current study, a positive correlation between GCS and FAB score was found along with a positive association between GCS and alcohol use report. In accordance with our findings, Yue et al. (42) showed an association between higher blood alcohol levels and lower score in the GCS at the acute stage in patients with uncomplicated mTBI. Blood alcohol levels were also associated with prolonged LOC. Excessive alcohol consumption was associated with decreased non-verbal processing speed and worse recovery at 6 months after injury. Contrary to our findings, Rojas et al. (43) found no correlation between GCS and FAB score when assessing patients with TBI at the acute stage. However, they found that the combined GCS and FAB scores can be used as predictors of TBI outcome at the acute stage. This difference may be accounted by differences in sample, since this latter study evaluated mild and moderate TBI and observed no difference of performance at FAB between those groups.
In our sample, mTBI patients performed significantly worse than healthy controls on naming, and naming correlated negatively with age. In agreement to our findings, Gauthier et al. (44) observed that patients with mTBI performed significantly worse than controls on naming when evaluated within 2 weeks post-TBI. Also, they found that age predicted performance on naming, with older age being associated with worse naming scores. It is well known that aging is associated with name retrieval difficulties, that may not be apparent in the speech, in which the subject can use similar words to replace the forgotten one, but do appear in naming tasks, where the answer is more restricted (45). Naming may be affected not only by age, but by low education, that can interfere in naming tasks (46).
Interestingly, a significant difference in age between patients with and without LOC was found. Moreover, age and LOC also correlated positively. Accordingly, LOC has been pointed out as a potential predictor of intracranial lesion in older patients with mTBI (47), supporting the hypothesis that older age might be associated with poorer outcomes. Brain imaging and gene expression studies also revealed that aging is associated with worse neural recovery in response to an acute mTBI (48).
Our study has limitations that must be considered. Other factors not evaluated in our study may have influenced cognitive performance, such as psychological stress, premorbid psychiatric status and previous cognitive decline (49, 50). Future studies must control these factors.
In sum, we found that patients with mTBI present cognitive deficits at acute stage (<24 h), mainly in episodic memory and executive function. Factors such as LOC and previous TBI seem to have minor influence during this period. On the other hand, factors such age and years of education may influence cognition, with younger ages and higher education level playing protective roles.
Minas Gerais' Traumatic Brain Injury Study Group
Ananda Peixoto Silva; Antônio Bernardes Bacilar Campos, Camila Carvalhais Costa, Christian Pereira Antônio, Daniela Lanna e Melo Loures, Eduarda Félix Ponte, Felipe Vieira Guarçoni, Guilherme Ribeiro Mansur Barbosa, Ilanna Naoli Santos Miranda, Jordana Campos Queiroz, Leonardo Gomes Salomão, Letícia Monteiro de Souza Oliveira, Maria Cecília Landim Nassif, Mariana Braga Valadão, Millena Vieira Brandão Moura, Otávio Fonseca Rodrigues, Pedro Henrique Lodde Leal, Tatiana Costa Diamantino, Letícia Siqueira Araújo, Thiago de Oliveira Furlan, Ewelin Wasner Machado da Silva, Isadora Gonçalves Roque, Alessandra Noronha da Silva.
Author Contributions
MGFC in the experimental design, carried out neuropsychological assays, data analysis, and drafted the manuscript. RMF participated in the study design and coordination and revised and edited the manuscript. JJP participated in the study design and neuropsychological data analysis and revised the manuscript. AK participated in the study design, data analysis and edited the manuscript. PC was responsible for analysis and interpretation of data and revised and edited the manuscript. ALT participated in the design and coordination of the study, revised, and edited the manuscript. LCS and ASM designed and coordinated the study, were responsible for data interpretation, revised, and edited the manuscript. All authors have read and approved the final version of the manuscript.
Funding
This work was supported by the 2016 NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation (grant number 25414), and FAPEMIG to ASM. LCS is supported by CNPq and MGFC is supported by CAPES.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Nguyen R, Fiest KM, McChesney J, Kwon CS, Jette N, Frolkis AD, et al. The international incidence of traumatic brain injury: a systematic review and meta-analysis. Can J Neurol Sci. (2016) 43:774–85. doi: 10.1017/cjn.2016.290
2. Gardner AJ, Zafonte R. Neuroepidemiology of traumatic brain injury. In: Rosano C, Ikram MA, Ganguli M, editors. Handbook of Clinical Neurology. Amsterdam: Elsevier (2016) p. 207–23.
3. Kristman VL, Borg J, Godbolt AK, Salmi LR, Cancelliere C, Carroll LJ, et al. Methodological issues and research recommendations for prognosis after mild traumatic brain injury: results of the international collaboration on mild traumatic brain injury prognosis. Arch Phys Med Rehabil. (2014) 95:S265–77. doi: 10.1016/j.apmr.2013.04.026
4. Veeramuthu V, Narayanan V, Kuo TL, Delano-Wood L, Chinna K, Bondi MW, et al. Diffusion tensor imaging parameters in mild traumatic brain injury and its correlation with early neuropsychological impairment: a longitudinal study. J Neurotrauma. (2015) 32:1497–509. doi: 10.1089/neu.2014.3750
5. Kou Z, Gattu R, Kobeissy F, Welch RD, O'Neil BJ, Woodard JL, et al. Combining biochemical and imaging markers to improve diagnosis and characterization of mild traumatic brain injury in the acute setting: results from a pilot study. PLoS ONE. (2013) 8:e80296. doi: 10.1371/journal.pone.0080296
6. Comerford VE, Geffen GM, May C, Medland SE, Geffen LB. A rapid screen of the severity of mild traumatic brain injury. J Clin Exp Neuropsychol. (2002) 24:409–19. doi: 10.1076/jcen.24.4.409.1044
7. Blodstein PA, Jones SJ, Buechler CM, Vandongen S. Cognitive screening in mild traumatic brain injuries: analysis of the neurobehavioral cognitive status examination when utilized during initial trauma hospitalization. J Neurotrauma. (1997) 14:171–7. doi: 10.1089/neu.1997.14.171
8. McCauley RL, Wilde EA, Barnes A, Hanten G, Hunter JV, Levin HS, et al. Patterns of early emotional and neuropsychological sequelae after mild traumatic brain injury. J Neurotrauma. (2014) 31:914–25. doi: 10.1089/neu.2012.2826
9. Sivák Š, Bittšanský M, Grossmann J, Nosál' V, Kantorová E, Siváková J, et al. Clinical correlations of proton magnetic resonance spectroscopy findings in acute phase after mild traumatic brain injury. Brain Inj. (2014) 28:341–6. doi: 10.3109/02699052.2013.865270
10. Barker-Collo S, Jones K, Theadom A, Starkey N, Dowell A, McPherson K, et al. Neuropsychological outcome and its correlates in the first year after adult mild traumatic brain injury: a population-based New Zealand study. Brain Inj. (2015) 29:1604–16. doi: 10.3109/02699052.2015.1075143
11. Theadom A, Parag V, Dowell T, McPherson K, Starkey N, Barker-Collo S, et al. Persistent problems 1 year after mild traumatic brain injury: a longitudinal population study in New Zealand. Br J Gen Pract. (2016) 66:e16–23. doi: 10.3399/bjgp16X683161
12. Nelson LD, Furger RE, Ranson J, Tarima S, Hammeke TA, Randolph C, et al. Acute clinical predictors of symptom recovery in emergency department patients with uncomplicated mild Traumatic BrainInjury (mTBI) or non-TBI injuries. J Neurotrauma. (2018) 35:249–59. doi: 10.1089/neu.2017.4988
13. Norris JN, Sams R, Lundblad P, Frantz E, Harris E. Blast-related mild traumatic brain injury in the acute phase: acute stress reactions partially mediate the relationship between loss of consciousness and symptoms. Brain Inj. (2014) 28:1052–62. doi: 10.3109/02699052.2014.891761
14. Sorg SF, Delano-Wood L, Luc N, Schiehser DM, Hanson KL, Nation DA, et al. White matter integrity in veterans with mild traumatic brain injury: associations with executive function and loss of consciousness. J Head Trauma Rehabil. (2014) 29:21–32. doi: 10.1097/HTR.0b013e31828a1aa4
15. Belanger HG, Spiegel E, Vanderploeg RD. Neuropsychological performance following a history of multiple self-reported concussions: a meta-analysis. J Int Neuropsychol Soc. (2010) 16:262–7. doi: 10.1017/S1355617709991287
16. Stein MB, Ursano RJ, Campbell-Sills L, Colpe LJ, Fullerton CS, Heeringa SG, et al. Prognostic indicators of persistent post-concussive symptoms after deployment-related mild traumatic brain injury: a prospective longitudinal study in U.S. Army Soldiers. J Neurotrauma. (2016) 33:2125–32. doi: 10.1089/neu.2015.4320
17. Magalhães ALG, de Souza LC, Faleiro RM, Teixeira AL, Miranda AS. Epidemiologia no traumatismo cranioencefálico no Brasil. Rev Brasil Neurol. (2017) 53:15–22.
18. De Almeida CER, de Sousa Filho JL, Dourado JC, Gontijo PA, Dellaretti MA, Costa BS, et al. Traumatic brain injury epidemiology in Brazil. World Neurosur. (2016) 87:540–7. doi: 10.1016/j.wneu.2015.10.020
19. Teasdale G, Jennet B. Assessment of coma and impaired consciousness: a practical scale. Lancet. (1974) 304:81–4. doi: 10.1016/S0140-6736(74)91639-0
20. Folstein MF, Folstein SE, McHugh PR. Mini-mental state - A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
21. Brucki S, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arquiv Neuropsiquiat. (2003) 61:777–81. doi: 10.1590/S0004-282X2003000500014
22. Dubois B, Slachevsky A, Litvan I, Pillon B. The FAB: a frontal assessment battery at bedside. Neurology. (2000) 55:1621–6. doi: 10.1212/WNL.55.11.1621
23. Beato R, Nitrini R, Formigoni AP, Caramelli P. Brazilian version of the Frontal Assessment Battery (FAB): preliminary data on administration to healthy elderly. Dement Neuropsychol. (2007) 1:59–65. doi: 10.1590/S1980-57642008DN10100010
24. Figueiredo VLM, Nascimento E. Desempenhos nas duas tarefas do subteste dígitos do WISC-III e do WAIS-III. Psicologia. (2007) 23:313–8. doi: 10.1590/S0102-37722007000300010
25. Nitrini R, Lefèvre BH, Mathias SC, Caramelli P, Carrilho PEM, Sauaia N, et al. Testes neuropsicológicos de aplicação simples para o diagnóstico de demência. Arquiv Neuropsiquiat. (1994) 52:457–65. doi: 10.1590/S0004-282X1994000400001
26. Castro S, Damin AE, Porto CS, Caramelli P, Nitrini R. The abbreviated form of the Brief Cognitive Battery in the diagnosis of dementia in Alzheimer's disease. Dement Neuropsychol. (2009) 3:327–31. doi: 10.1590/S1980-57642009DN30400011
27. Miotto EC, Cinalli FZ, Serrao VT, Benute GG, Lucia MCS, Scaff M. Cognitive deficits in patients with mild to moderate traumatic brain injury. Arquiv Neuropsiq. (2010) 68:862–8. doi: 10.1590/S0004-282X2010000600006
28. Fonseca RP, Zimmermann N, Cotrena C, Cardoso C, Kristensen CH, Grassi-Oliveira R. Neuropsychological assessment of executive functions in traumatic brain injury: hot and cold components. Psychol Neurosci. (2012) 5:183–90. doi: 10.3922/j.psns.2012.2.08
29. Pereira N, Holz M, Hermes Pereira A, Bresolin AP, Zimmermann N, Paz Fonseca R. Frequência de déficits neuropsicológicos após traumatismo cranioencefálico. Acta Colomb Psicol. (2016) 19:105–15. doi: 10.14718/.acP.2016.19.2.6
30. Rohling ML, Binder LM, Demakis GJ, Larrabee GJ, Ploetz DM, Langhinrichsen-Rohling J. A meta-analysis of neuropsychological outcome after mild traumatic brain injury: re-analyses and reconsiderations of Binder et al. (), Frencham et al. (), and Pertab et al. (). Clin Neuropsychol. (2011) 25: 608–23. doi: 10.1080/13854046.2011.565076
31. DallAcqua P, Johannes S, Mica L, Simmen HP, Glaab R, Fandino J, et al. Prefrontal cortical thickening after mild traumatic brain injury: a 1year MRI study. J Neurotrauma. (2017) 34:3270–9. doi: 10.1089/neu.2017.5124
32. Sofko CA, Currier JM, Hill BD, Drescher KD. History of loss of consciousness with mild traumatic brain injury affects PTSD symptom presentation in treatment-seeking Iraq/Afghanistan veterans. Brain Inj. (2016) 30:1561–9. doi: 10.1080/02699052.2016.1199897
33. Bigler ED. Neuropsychology and clinical neuroscience of persistent post-concussive syndrome. J Int Neuropsychol Soc. (2008) 14:1–22. doi: 10.1017/S135561770808017X
34. Larabee GJ, Rohling ML. Neuropsychological differential diagnosis of mild traumatic brain injury. Behav Sci Law. (2013) 31:686–701. doi: 10.1002/bsl.2087
35. Karr JE, Areshenkoff CN, Garcia-Barrera MA. The neuropsychological outcomes of concussion: a systematic review of meta-analyses on the cognitive sequelae of mild traumatic brain injury. Neuropsychology. (2014) 28:321–36. doi: 10.1037/neu0000037
36. Dikmen S, Machamer J, Temkin N. Mild traumatic brain injury: longitudinal study of cognition, functional status, and post-traumatic symptoms. J Neurotrauma. (2016) 34:1524–30. doi: 10.1089/neu.2016.4618
37. Bigler ED, Farrer TJ, Pertab JL, James K, Petrie JA, Hedges DW. Reaffirmed limitations of meta-analytic methods in the study of mild traumatic brain injury: a response to Rohling et al. Clin Neuropsychol. (2013) 27:176–214. doi: 10.1080/13854046.2012.693950
38. Sumowski JF, Chiaravalloti N, Krch D, Paxton J, Deluca J. Education attenuates the negative impact of traumatic brain injury on cognitive status. Arch Phys Med Rehabil. (2013) 94:2562–4. doi: 10.1016/j.apmr.2013.07.023
39. Leary JB, Kim GY, Bradley CL, Hussain UZ, Sacco M, Bernad M, et al. The association of cognitive reserve in chronic-phase functional and neuropsychological outcomes following traumatic brain injury. J Head Trauma Rehabil. (2018) 33:E28–35.
40. Mathias LJ, Wheaton P. Contribution of brain or biological reserve and cognitive or neural reserve to outcome after TBI: a meta-analysis (prior to 2015). Neurosci Biobehav Rev. (2015) 55:573–93. doi: 10.1016/j.neubiorev.2015.06.001
41. Oldenburg C, Lundin A, Edman G, Nygren-de Boussard C, Bartfai A. Cognitive reserve and persistent post-concussion symptoms—A prospective mild traumatic brain injury (mTBI) cohort study. Brain Inj. (2016) 30:146–55. doi: 10.3109/02699052.2015.1089598
42. Yue JK, Ngwenya LB, Upadhyayula PS, Deng H, Winkler EA, Burke JF, et al. Emergency department blood alcohol level associates with injury factors and six-month outcome after uncomplicated mild traumatic brain injury. J Clin Neurosci. (2017) 45:293–8. doi: 10.1016/j.jocn.2017.07.022
43. Rojas N, Laguë-Beauvais M, Belisle A, Lamoureux J, AlSideiri G, Marcoux J, Maleki M, et al. Frontal assessment battery (FAB) performance following traumatic brain injury hospitalized in an acute care setting. Appl Neuropsychol Adult. (2018) 19:1–12. doi: 10.1080/23279095.2017.1422506
44. Gauthier S, LeBlanc J, Seresova A, Laberge-Poirier A, Correa J, Abdulrahman A, et al. Acute prediction of outcome and cognitive-communication impairments following traumatic brain injury: the influence of age, education and site of lesion. J Commun Disord. (2018) 77:77–90. doi: 10.1016/j.jcomdis.2018.04.003
45. Mortensen L, Meyer A, Humphreys GW. Age-related effects on speech production: a review. Lang Cogn Proc. (2006) 21:238–90. doi: 10.1080/01690960444000278
46. Paolieri D, Marful A, Morales L, Bajo MT. The modulating effect of education on semantic interference during healthy aging. PLoS ONE. (2018) 13:e0191656. doi: 10.1371/journal.pone.0191656
47. Ibañez Pérez De La Blanca MA, Fernández Mondéjar E, Gómez Jimènez FJ, Alonso Morales JM, Lombardo MDQ, Viso Rodriguez JL. Risk factors for intracranial lesions and mortality in older patients with mild traumatic brain injuries. Brain Inj. (2018) 32:99–104. doi: 10.1080/02699052.2017.1382716
48. Cho Y, Latour LL, Kim H, Turtzo LC, Olivera A, Livingston WS, et al. Older age results in differential gene expression after mild traumatic brain injury and is linked to imaging differences at acute follow-up. Front Aging Neurosci. (2016) 8:168. doi: 10.3389/fnagi.2016.00168
49. Massey JS, Meares S, Batchelor J, Bryant RA. An exploratory study of the association of acute posttraumatic stress, depression, and pain to cognitive functioning in mild traumatic brain injury. Neuropsychology. (2015) 29:530–42. doi: 10.1037/neu0000192
Keywords: traumatic brain injury, cognitive impairment, loss of consciousness, Brazilian patients, episodic memory
Citation: Cardoso MGF, Faleiro RM, de Paula JJ, Kummer A, Caramelli P, Teixeira AL, de Souza LC and Miranda AS (2019) Cognitive Impairment Following Acute Mild Traumatic Brain Injury. Front. Neurol. 10:198. doi: 10.3389/fneur.2019.00198
Received: 28 October 2018; Accepted: 15 February 2019;
Published: 08 March 2019.
Edited by:
Denes V. Agoston, Karolinska Institute (KI), SwedenReviewed by:
Sergio Bagnato, Institute Foundation G.Giglio, ItalyFrancisco Capani, University of Buenos Aires, Argentina
Copyright © 2019 Cardoso, Faleiro, de Paula, Kummer, Caramelli, Teixeira, de Souza and Miranda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aline Silva Miranda, bWlyYW5kYXMuYWxpbmVAZ21haWwuY29t
†These authors have contributed equally to this work