
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Neurol., 30 January 2019
Sec. Stroke
Volume 10 - 2019 | https://doi.org/10.3389/fneur.2019.00044
 Jong-Won Chung1
Jong-Won Chung1 Suk Jae Kim1
Suk Jae Kim1 Jaechun Hwang2
Jaechun Hwang2 Mi Ji Lee1
Mi Ji Lee1 Jun Lee3Kyung-Yul Lee4Man-Seok Park5Sang Min Sung6Keon Ha Kim7Pyoung Jeon7Oh Young Bang1*
Jun Lee3Kyung-Yul Lee4Man-Seok Park5Sang Min Sung6Keon Ha Kim7Pyoung Jeon7Oh Young Bang1*Background and Purpose: Patients undergoing carotid artery stenting (CAS) who show low responsiveness to clopidogrel may have a higher risk of peri-procedural embolic events. This study aimed to compare the effectiveness and safety of clopidogrel and ticlopidine plus Ginkgo biloba in clopidogrel-resistant patients undergoing CAS.
Methods: In this multi-center, randomized, controlled trial, we used platelet reactivity test to select patients undergoing CAS who showed clopidogrel resistance, and compared treatments using clopidogrel and ticlopidine plus ginkgo. The primary outcome was the incidence of new ischemic lesion in the ipsilateral hemisphere of CAS. Detection of microembolic signal on transcranial Doppler was the secondary outcome. The clinical outcomes were also monitored.
Results: This trial was discontinued after 42 patients were randomized after preplanned interim sample size re-estimation indicated an impractical sample size. The primary endpoint occurred in 12/22 patients (54.5%) in the clopidogrel group and 13/20 patients (65.0%) in the ticlopidine–ginkgo group (P = 0.610). No significant differences in the presence of microembolic signal (15.0 vs. 11.8%, P = 0.580), clinical outcomes (ischemic stroke or transient ischemic attack, 0.0 vs. 5.5%; acute myocardial infarction 0.0 vs. 0.0%; all-cause death, 4.5 vs. 0.0%), or incidence of adverse events were found in the two groups. In terms of resistance to clopidogrel, treatment with ticlopidine–ginkgo significantly increased the P2Y12 Reaction Units (difference, 0.0 [−0.3–3.0] vs. 21.0 [6.0–35.0], P < 0.001).
Conclusions: In patients who showed clopidogrel resistance, ticlopidine–ginkgo treatment was safe and increased P2Y12 Reaction Units; however, compared to clopidogrel, it failed to improve surrogate and clinical endpoints in patients undergoing CAS. This multimodal biomarker-based clinical trial is feasible in neurointerventional research.
Clinical Trial Registration: http://www.clinicaltrials.gov. Unique identifier: NCT02133989.
Antiplatelet agents are used to prevent stent thrombosis and peri-procedural complications. The extent of inhibition of platelet function by aspirin and clopidogrel differs among individuals, and is related to recurrent cerebrovascular or cardiovascular events during the use of antiplatelet agents. While the Clopidogrel in High-risk patients with Acute Non-disabling Cerebrovascular Events (CHANCE) trial showed that in comparison with aspirin alone, combined treatment with clopidogrel and aspirin decreases the 90-day risk of stroke without increasing hemorrhage (1), it also showed that this effect was not observed in CYP2C19 loss-of-function alleles (2).
Several studies have dealt with the association between genetic (e.g., CYP2C19 loss-of-function alleles) and laboratory (e.g., point-of-care tests for platelet aggregation) features of clopidogrel resistance with cardiovascular events and stroke in subjects receiving clopidogrel (3–8). However, few clinical trials have been conducted to test antiplatelet strategies to overcome clopidogrel resistance in patients with stroke or in those who undergo carotid intervention. The use of P2Y12 receptor inhibitors other than clopidogrel, such as ticlopidine or novel thienopyridines, could be a possible strategy against clopidogrel resistance. The use of thienopyridine prodrugs with more rapid and consistent actions (ticlopidine and prasugrel have more pathways resulting in active metabolites and are not deactivated by de-esterification) or direct-acting P2Y12 inhibitors (cangrelor and ticagrelor) could be alternatives to the standard clopidogrel therapy (9). Although a recent clinical trial tested the role of ticagrelor over aspirin in patients with ischemic stroke/transient ischemic attack (TIA), further studies are required to determine the optimal candidate for this novel thienopyridine (10–12). Current guidelines do not recommend the use of novel thienopyridines in patients with stroke.
Biomarker-based diagnostic tests are increasingly being used as surrogate markers in clinical trials in cancer (13), cardiovascular disease (14), renal disease (15, 16), and neurological disorder (17, 18), and they might add important information from the neurointerventional point of view. In these clinical trials, instead of clinical events, laboratory outcomes were measured. In the present study, we selected three laboratory outcomes (Figure 1). First, ischemic brain lesions on diffusion-weighted images (DWIs), a marker of an increased risk of cerebrovascular events in the International Carotid Stenting Study (the recipient site) (19). Second, microembolic signals (MES) on transcranial duplex (TCD) ultrasound monitoring, which were related to clinical events and were used as markers for antiplatelet effects in patients with carotid and intracranial stenosis (migrating emboli) (20, 21). Third, the occurrence of restenosis on follow-up carotid duplex (the donor site). As an exploratory research, we tested the feasibility and usefulness of this multidisciplinary and comprehensive laboratory approach in a drug trial in the setting of a small number of patients with few clinical events.
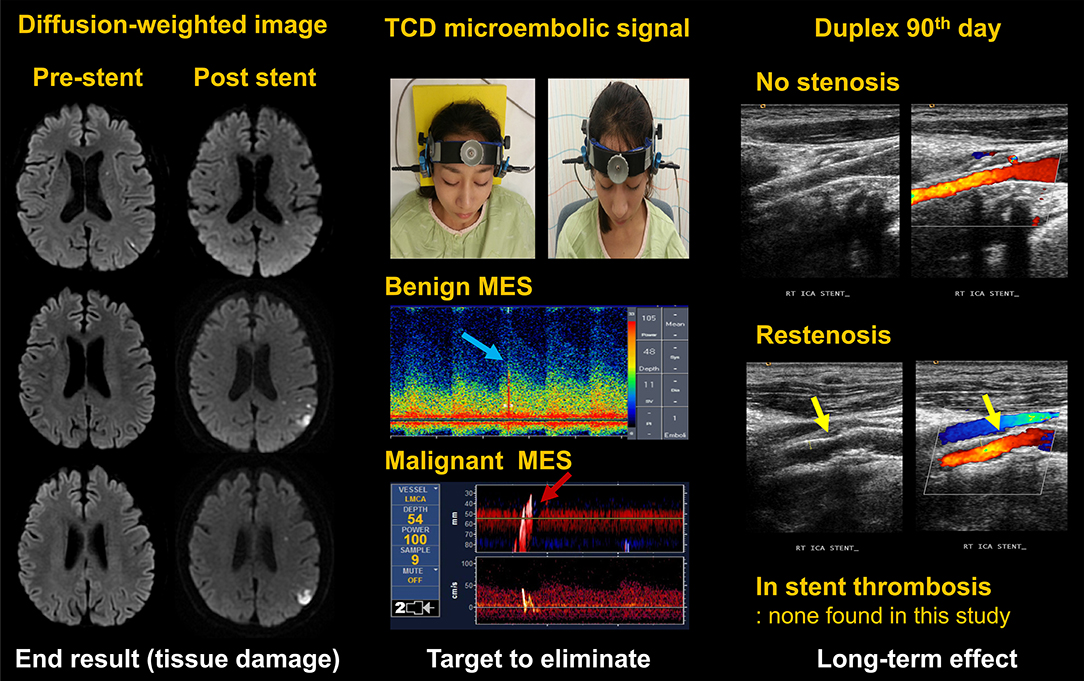
Figure 1. Measurement of laboratory outcomes. TCD, transcranial doppler; MES, microembolic signal. Written informed consent was obtained from the individual appearing in this figure (top, middle).
The usefulness of ticlopidine in patients with loss-of-function CYP2C19 polymorphism carriers have been reported (22). In addition, an experiment demonstrated augmented antithrombotic and antiplatelet effects with ticlopidine and Ginkgo biloba (23, 24). This trial aimed to evaluate the efficacy and safety of ticlopidine plus Ginkgo biloba compared to clopidogrel using surrogate biomarkers in patients showing clopidogrel resistance who undergo carotid artery stent (CAS) placement.
The Clopidogrel Resistance and Embolism in Carotid Artery Stenting (CRECAS) trial is a multicenter prospective, randomized, open-label, blinded-endpoint trial. This study is registered with ClinicalTrials.gov (identifier, NCT02133989). Patients were enrolled from January 2014 through August 2017 at six sites in South Korea. The trial was approved by the appropriate national regulatory authorities and relevant ethnics committees at each participating site. All participants provided written informed consents.
The executive committee was responsible for the overall design, interpretation, and supervision of the trial, including the development of the protocol and any amendments. The executive committee was also responsible for ensuring the integrity of the data, analysis, and presentation of results. An independent data and safety monitoring committee reported to the executive committee, and regularly assessed the safety outcomes, overall study integrity, and study conduct. The sponsor had no influence or involvement in the design, conduct, analysis, and decision to terminate this trial. The sponsor was not part of the executive committee.
CRECAS-randomized patients had provided informed consent, were scheduled for stent implantation owing to carotid stenosis of 70% or more, and showed resistance to clopidogrel, defined by platelet inhibition rate < 20% measured by the VerifyNow system (Accumetrics, San Diego, CA, USA) in patients taking a clopidogrel dose of 75 mg/d for ≥7 days or 24 h after a loading dose of 300 mg for clopidogrel-naïve patients. Premedication with clopidogrel 75 mg for ≥7 days or 300 mg for ≥24 h showed similar platelet inhibition (25). All patients underwent brain MRI including DWI within 1 months prior to carotid stenting.
Patients were not eligible for participation in the trial if they were scheduled for other specific antiplatelet therapy or anticoagulation therapy or for carotid, cerebrovascular, or coronary revascularization that would require discontinuation of the study treatment within 60 days after randomization. Similarly, patients unable to undergo MR imaging; those with hematologic abnormalities including neutrophil count <1,500/μL, platelet count <100,000/μL, or AST/ALT >120 U/L; and those who failed to understand or comply with the study procedures or follow-up were excluded from the study.
Eligible patients were randomly assigned in a 1:1 ratio to one of two treatment groups, using random permuted blocks. Patients were 1:1 randomized to clopidogrel 75 mg daily or ticlopidine 250 mg/Ginkgo biloba 80 mg twice daily, together with a daily dose of aspirin 100 mg for a 60-day treatment period. At the end of 24 weeks of study treatment, patients were treated at the discretion of investigators and followed up.
Carotid stenting was performed according to the standardized method by skilled and experienced operators. CAS was performed as soon as possible in the clopidogrel group, and after 96 h of study medication in the ticlopidine–ginkgo group. All patients received high-intensity statins according to the current international guidelines before carotid stenting.
The primary endpoint for the trial was the presence of new ischemic lesions in the ipsilateral hemisphere on DWI performed within 24 h after carotid stenting. The predefined secondary endpoints were the number and volume of new ischemic lesions on DWI performed within 24 h after carotid stenting, and total and malignant MES on TCD monitoring performed within 24 h after carotid stenting. TCD (Pioneer TC 8080; Nicolet Vascular, Madison, WI, USA) was used to monitor both middle cerebral arteries (MCAs) with insonation depths of 40–60 mm for microemboli using two 2-MHz probes fixed with a head frame (Marc 500; Spencer Technologies, Northborough, MA, USA). All MES' were automatically saved to the computer hard disk for review, and all analyses were performed blinded to individual patient details. Bilateral recordings were performed for 30 min, with the patients in a supine position. Patients who had ≥1 MES during the 30 min of TCD recording were classified as MES positive. In the present study, we also measured malignant MES, a larger-sized embolus requiring more clinical attention (26, 27). MES' with a relative energy index >1.0 were considered malignant.
Other exploratory endpoints included ischemic stroke/TIA, myocardial infarction, or death within 24 weeks after carotid stenting. The safety endpoints included puncture-site hematoma, hematological abnormalities, namely neutrophil count <1,500/μL, platelet count <100,000/μL, or AST/ALT level >120 U/L. We also measured the changes of clopidogrel resistance, by using the VerifyNow system. Clinical and laboratory follow-up was conducted on Day 1, Day 7, Week 4, and Week 24 after carotid stenting.
A total of 82 patients were required to detect a hazard ratio of 0.55, with a final two-sided significance level of 5 and 80% power, as observed in a previous observational study (28). To apply the 5% dropout rate, 86 patients were scheduled to be enrolled. A single pre-specified interim analysis for efficacy and futility was performed when half of the patients were enrolled for sample size recalculation or early discontinuation of the trial.
Statistical analyses were performed using PASW Statistics 18 (IBM, Chicago, IL, USA). Continuous variables are presented as means with standard deviations, and categorical variables are presented as frequencies and percentages. Variables were compared by independent t-test, chi-square test, Mann–Whitney U-test, and Fisher's exact test. A two-tailed value of p < 0.05 was considered statistically significant.
This trial was discontinued after prespecified interim analysis for futility and power re-estimation after enrolment of 42 participants. The primary endpoint, new ischemic lesions in the ipsilateral hemisphere of carotid stenting, was detected in 54.5% (12 of 22) of patients in the clopidogrel group and 55.0% (11 of 20) of patients in the ticlopidine–ginkgo group. Based on this result, the sample size was recalculated, and the estimated number of patients required to show significant difference in the two groups was 155,000 (Z-test with pooled variance statistics; power, 0.80; two-sided significance level, 0.05, with two independent proportions power analyses). PASS 12 (NCSS, Kaysville, Utah, USA) software was used to perform the sample size estimates. In addition, owing to the recently decreasing role of carotid intervention in patients with asymptomatic carotid stenosis, slow patient recruitment for the study was expected. The executive committee concluded that it was impractical to continue the study and decided to terminate it prematurely.
From June 2014 through October 2017, we recruited 42 patients, 22 of whom were assigned to the clopidogrel group and 20, to the ticlopidine–ginkgo group (Supplementary Table 1). The baseline characteristics of the IIT-analysis population are described in Table 1. Baseline characteristics were well-balanced between the groups, except that compared to the clopidogrel group (63.3%), more symptomatic (acute stroke or transient ischemic attack) patients were enrolled in the ticlopidine–ginkgo group (80.0%) (P = 0.037).
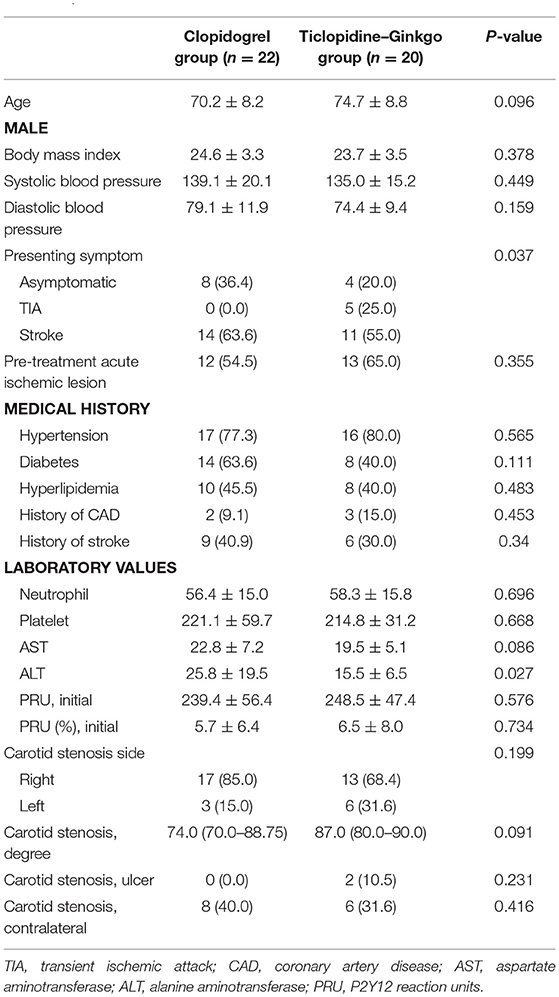
Table 1. Baseline characteristics.
Before carotid stenting, acute ischemic lesions were found in 12 (54.5%) patients in the clopidogrel group and 13 (65.0%) patients in the ticlopidine–ginkgo group. The primary endpoint of new ischemic lesion(s) in ipsilateral carotid stenting occurred in 12 patients (54.5%) in the clopidogrel group and 11 patients (55.0%) in the ticlopidine–ginkgo group (P = 0.610). There were no significant differences between the groups with regard to microembolic signal and carotid duplex imaging. However, compared to persistent clopidogrel treatment, treatment with ticlopidine–ginkgo for a median duration of 7 days significantly improved P2Y12 Reaction Units (Figure 2). The details of laboratory outcomes are demonstrated in Table 2. During a median follow-up period of 178 days after carotid stenting, one patient in the ticlopidine–ginkgo group experienced stroke recurrence and one patient in the clopidogrel group died owing to lung cancer. None of the patients enrolled in the study experienced any hematologic or procedure-related adverse event. The clinical and adverse events are summarized in Table 3.
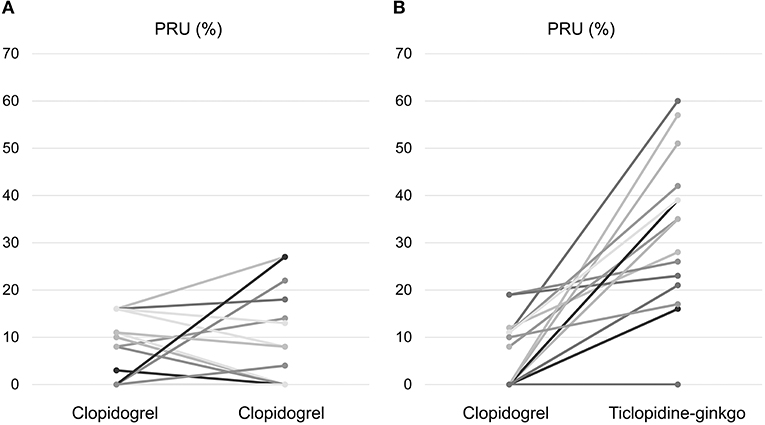
Figure 2. Changes in P2Y12 Reaction Units. Change in P2Y12 Reaction Units in the (A) clopidogrel and (B) ticlopidine–ginkgo group.
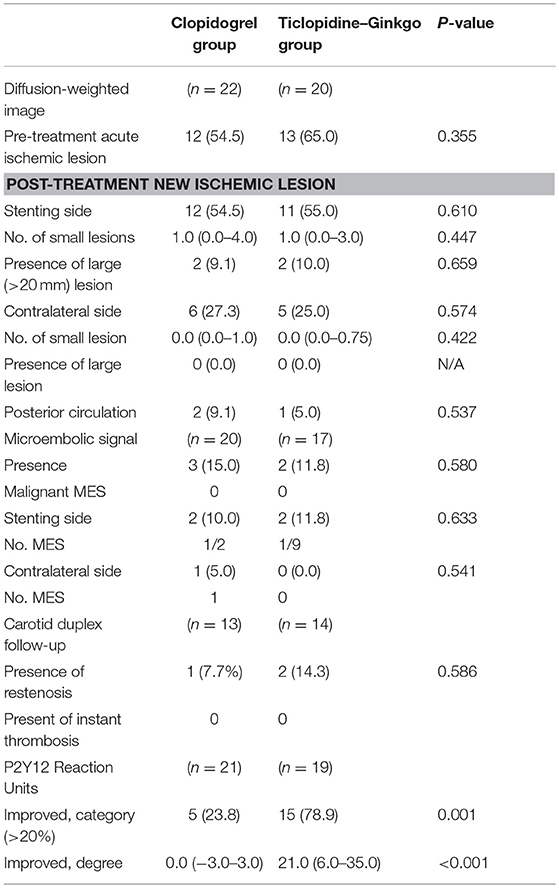
Table 2. Laboratory outcomes.
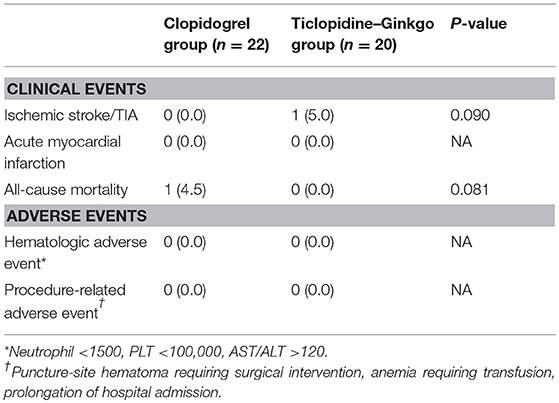
Table 3. Clinical and adverse events.
The main findings of this trial are as follows: (1) clinical events including ischemic stroke, acute myocardial infarction, and all-cause death related to carotid stenting were rare, while surrogate biomarker outcome events, detected by DWI and TCD, were highly frequent; (2) the primary outcome, new ischemic lesion on follow-up DWI, did not show significant difference between the two study groups; (3) ticlopidine–ginkgo treatment significantly improved drug resistance (P2Y12 Reaction Units). There were no safety concerns identified within this small group of patients.
During the study screening period, 45.9% (106/231) of patients treated with CAS showed clopidogrel resistance, which may be related to both genetic and non-genetic factors (e.g., concomitant use of statins, proton pump inhibitors, and presence of diabetes) (29–33). The reported prevalence of clopidogrel resistance in cerebrovascular intervention ranges from 28.8 to 65.8% (28, 34–36), and it is more prevalent in Asian individuals (37).
The failure of this study could be attributed to the following reasons. First, our study population showed a low rate of vascular events (one stroke and one death) during the follow-up period. With the advances in neurointerventional technique and the use of high-intensity statins prior to CAS, the incidence of periprocedural stroke/TIA has substantially decreased (38). Another explanation is the short duration of follow-up in this study. Most clinical trials testing the role of antiplatelet agents in patients with high on-treatment residual platelet reactivity had a long follow-up period (3, 5, 39, 40), while only peri-procedural laboratory events were measured in the present trial. The third reason is the differences in the baseline characteristics (more asymptomatic patients in the clopidogrel group) and treatment protocol (stenting with a delay of at least 4 days of randomization in the ticlopidine–ginkgo group) between the groups.
Although this trial failed to show the superiority of ticlopidine–ginkgo over standard clopidogrel therapy in patients with high on-treatment platelet reactivity undergoing CAS placement, it has some clinical implications. Our results suggest the possibility of clinical trials that use comprehensive surrogate markers of three different sites (donor, migrating, and recipient). Relatively small number of patients and a short follow-up period may be required to evaluate the efficacy of drug therapy. For example, the efficacy of antiplatelet agents has been successfully tested using MES as a surrogate marker in clinical trials with a small cohort (n = ~100 patients) (20, 21). In addition, a recent meta-analysis showed that 1 out of 10 patients with silent DWI lesions during invasive vascular or cardiac procedures experienced stroke or TIA (41). In the present study, several patients showed embolism on DWI or TCD measures, while only two patient showed a clinical event. In this context, surrogate biomarker outcome-based clinical studies may be helpful before starting a large clinical trial. Further clinical trials using this approach and testing other thienopyridines in various neurointerventional settings (e.g., endovascular aneurysmal repair) are warranted. Lastly, the results of this trial showed considerable improvement in P2Y12 Reaction Units without hematologic or adverse effects by using ticlopidine–ginkgo. Further studies with a larger cohort and long-term follow-up are warranted.
This study has several limitations. First, the primary outcome was the surrogate endpoint; further studies are required to evaluate the long-term clinical efficacy of ticlopidine–ginkgo. However, based on our results, it is unlikely that long-term clinical efficacy events would differ between the groups. Second, only Korean patients were included in the study; this may limit the generalizability of our results, since a high prevalence of clopidogrel resistance has been reported in the Asian population (42). Third, more symptomatic patients with carotid stenosis were enrolled in the ticlopidine–ginkgo group. Symptomatic carotid stenosis is associated with a higher risk for recurrent thromboembolism, and the imbalance in the baseline in this trial may have affected the study endpoints. Finally, 96 h waiting periods for the ticlopidine–ginkgo group could have affected the study results.
Our findings indicate that a multimodal biomarker-based clinical trial is feasible in research related to clinical stroke, with more frequent endpoint events observed than those observed from clinical outcomes. Compared to continued treatment with clopidogrel, treatment with ticlopidine–ginkgo significantly improved drug resistance. No adverse effects were observed within this small group of patients. However, no difference was observed in early surrogate biomarkers between the treatment groups.
OB was the principal investigator, participated in the study design, obtained funding, and wrote the report. J-WC contributed to the data collection, data analysis, and wrote the report. SK, JH, ML, JL, K-YL, M-SP, SS, KK, and PJ contributed to data collection and interpretation and design of the study, reviewed the report, and gave scientific advice.
This study was supported by grants from YuYu Pharma, Inc. Seoul, South Korea, which collaborated in the execution of the trial and collected the data. All authors had full access to the data and data analysis. The sponsor of the study had no role in the study design, data analysis, data interpretation, writing of the report, or decision to publish the results. The corresponding author assumed the final responsibility for the decision to submit this manuscript for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2019.00044/full#supplementary-material
1. Wang Y, Wang Y, Zhao X, Liu L, Wang D, Wang C, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med. (2013) 369:11–9. doi: 10.1056/NEJMoa1215340
2. Wang Y, Zhao X, Lin J, Li H, Johnston SC, Lin Y, et al. Association between CYP2C19 loss-of-function allele status and efficacy of clopidogrel for risk reduction among patients with minor stroke or transient ischemic attack. JAMA (2016) 316:70–8. doi: 10.1001/jama.2016.8662
3. Mega JL, Close SL, Wiviott SD, Shen L, Hockett RD, Brandt JT, et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N Engl J Med. (2009) 360:354–62. doi: 10.1056/NEJMoa0809171
4. Pan Y, Chen W, Xu Y, Yi X, Han Y, Yang Q, et al. Genetic polymorphisms and clopidogrel efficacy for acute ischemic stroke or transient ischemic attack: a systematic review and meta-analysis. Circulation (2017) 135:21–33. doi: 10.1161/CIRCULATIONAHA.116.024913
5. Campo G, Fileti L, de Cesare N, Meliga E, Furgieri A, Russo F, et al. Long-term clinical outcome based on aspirin and clopidogrel responsiveness status after elective percutaneous coronary intervention: a 3T/2R (tailoring treatment with tirofiban in patients showing resistance to aspirin and/or resistance to clopidogrel) trial substudy. J Am Coll Cardiol. (2010) 56:1447–55. doi: 10.1016/j.jacc.2010.03.103
6. Sun X, Tong X, Lo WT, Mo D, Gao F, Ma N, et al. Risk factors of subacute thrombosis after intracranial stenting for symptomatic intracranial arterial stenosis. Stroke (2017) 48:784–6. doi: 10.1161/STROKEAHA.116.015538
7. Hwang G, Huh W, Lee JS, Villavicencio JB, Villamor RB Jr, Ahn SY, et al. Standard vs. modified antiplatelet preparation for preventing thromboembolic events in patients with high on-treatment platelet reactivity undergoing coil embolization for an unruptured intracranial aneurysm: a randomized clinical trial. JAMA Neurol. (2015) 72:764–72. doi: 10.1001/jamaneurol.2015.0654
8. Delgado Almandoz JE, Crandall BM, Scholz JM, Fease JL, Anderson RE, Kadkhodayan Y, et al. Pre-procedure P2Y12 reaction units value predicts perioperative thromboembolic and hemorrhagic complications in patients with cerebral aneurysms treated with the pipeline embolization device. J Neurointerv Surg. (2013) 5(Suppl. 3):iii3–10. doi: 10.1136/neurintsurg-2012-010582
9. Wallentin L. P2Y(12) inhibitors: differences in properties and mechanisms of action and potential consequences for clinical use. Eur Heart J. (2009) 30:1964–77. doi: 10.1093/eurheartj/ehp296
10. Johnston SC, Amarenco P, Albers GW, Denison H, Easton JD, Evans SR, et al. Ticagrelor versus aspirin in acute stroke or transient ischemic attack. N Engl J Med. (2016) 375:35–43. doi: 10.1056/NEJMoa1603060
11. Amarenco P, Albers GW, Denison H, Easton JD, Evans SR, Held P, et al. Efficacy and safety of ticagrelor versus aspirin in acute stroke or transient ischaemic attack of atherosclerotic origin: a subgroup analysis of SOCRATES, a randomised, double-blind, controlled trial. Lancet Neurol. (2017) 16:301–10. doi: 10.1016/S1474-4422(17)30038-8
12. Wang Y, Lin Y, Meng X, Chen W, Chen G, Wang Z, et al. Effect of ticagrelor with clopidogrel on high on-treatment platelet reactivity in acute stroke or transient ischemic attack (PRINCE) trial: rationale and design. Int J Stroke (2017) 12:321–5. doi: 10.1177/1747493017694390
13. Mandrekar SJ, Sargent DJ. Clinical trial designs for predictive biomarker validation: theoretical considerations and practical challenges. J Clin Oncol. (2009) 27:4027–34. doi: 10.1200/JCO.2009.22.3701
14. Bikdeli B, Punnanithinont N, Akram Y, Lee I, Desai NR, Ross JS, et al. Two decades of cardiovascular trials with primary surrogate endpoints: 1990–2011. J Am Heart Assoc. (2017) 6:e005285. doi: 10.1161/JAHA.116.005285
15. Hartung EA. Biomarkers and surrogate endpoints in kidney disease. Pediatr Nephrol. (2016) 31:381–91. doi: 10.1007/s00467-015-3104-8
16. Besarab A, Bolton WK, Browne JK, Egrie JC, Nissenson AR, Okamoto DM, et al. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med. (1998) 339:584–90. doi: 10.1056/NEJM199808273390903
17. Staner L. Surrogate outcomes in neurology, psychiatry, and psychopharmacology. Dialogues Clin Neurosci. (2006) 8:345–52.
18. Caroli A, Prestia A, Wade S, Chen K, Ayutyanont N, Landau SM, et al. Alzheimer disease biomarkers as outcome measures for clinical trials in MCI. Alzheimer Dis Assoc Disord. (2015) 29:101–9. doi: 10.1097/WAD.0000000000000071
19. Gensicke H, van der Worp HB, Nederkoorn PJ, Macdonald S, Gaines PA, van der Lugt A, et al. Ischemic brain lesions after carotid artery stenting increase future cerebrovascular risk. J Am Coll Cardiol. (2015) 65:521–9. doi: 10.1016/j.jacc.2014.11.038
20. Markus HS, Droste DW, Kaps M, Larrue V, Lees KR, Siebler M, et al. Dual antiplatelet therapy with clopidogrel and aspirin in symptomatic carotid stenosis evaluated using doppler embolic signal detection: the clopidogrel and aspirin for reduction of emboli in symptomatic carotid stenosis (CARESS) trial. Circulation (2005) 111:2233–40. doi: 10.1161/01.CIR.0000163561.90680.1C
21. Wong KS, Chen C, Fu J, Chang HM, Suwanwela NC, Huang YN, et al. Clopidogrel plus aspirin versus aspirin alone for reducing embolisation in patients with acute symptomatic cerebral or carotid artery stenosis (CLAIR study): a randomised, open-label, blinded-endpoint trial. Lancet Neurol. (2010) 9:489–97. doi: 10.1016/S1474-4422(10)70060-0
22. Maeda A, Ando H, Asai T, Ishiguro H, Umemoto N, Ohta M, et al. Differential impacts of CYP2C19 gene polymorphisms on the antiplatelet effects of clopidogrel and ticlopidine. Clin Pharmacol Ther. (2011) 89:229–33. doi: 10.1038/clpt.2010.268
23. Kim YS, Pyo MK, Park KM, Park PH, Hahn BS, Wu SJ, et al. Antiplatelet and antithrombotic effects of a combination of ticlopidine and ginkgo biloba ext (EGb 761). Thromb Res. (1998) 91:33–8.
24. Hong JM, Shin DH, Lim YA, Lee JS, Joo IS. Ticlopidine with ginkgo biloba extract: a feasible combination for patients with acute cerebral ischemia. Thromb Res. (2013) 131:e147–53. doi: 10.1016/j.thromres.2013.01.026
25. Pandya DJ, Fitzsimmons BF, Wolfe TJ, Hussain SI, Lynch JR, Ortega-Gutierrez S, et al. Measurement of antiplatelet inhibition during neurointerventional procedures: the effect of antithrombotic duration and loading dose. J Neuroimaging (2010) 20:64–9. doi: 10.1111/j.1552-6569.2008.00322.x
26. Choi Y, Saqqur M, Stewart E, Stephenson C, Roy J, Boulanger JM, et al. Relative energy index of microembolic signal can predict malignant microemboli. Stroke (2010) 41:700–6. doi: 10.1161/STROKEAHA.109.573733
27. Almekhlafi MA, Demchuk AM, Mishra S, Bal S, Menon BK, Wiebe S, et al. Malignant emboli on transcranial Doppler during carotid stenting predict postprocedure diffusion-weighted imaging lesions. Stroke (2013) 44:1317–22. doi: 10.1161/STROKEAHA.111.000659
28. Song TJ, Suh SH, Min PK, Kim DJ, Kim BM, Heo JH, et al. The influence of anti-platelet resistance on the development of cerebral ischemic lesion after carotid artery stenting. Yonsei Med J. (2013) 54:288–94. doi: 10.3349/ymj.2013.54.2.288
29. Simon T, Verstuyft C, Mary-Krause M, Quteineh L, Drouet E, Meneveau N, et al. Genetic determinants of response to clopidogrel and cardiovascular events. N Engl J Med. (2009) 360:363–75. doi: 10.1056/NEJMoa0808227
31. Ho PM, Maddox TM, Wang L, Fihn SD, Jesse RL, Peterson ED, et al. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome. JAMA (2009) 301:937–44. doi: 10.1001/jama.2009.261
32. Lin Y, Wang A, Li J, Lin J, Wang D, Meng X, et al. Impact of glycemic control on efficacy of clopidogrel in transient ischemic attack or minor stroke patients with CYP2C19 genetic variants. Stroke (2017) 48:998–1004. doi: 10.1161/STROKEAHA.116.016463
33. Hu L, Chang L, Zhang Y, Zhai L, Zhang S, Qi Z, et al. Platelets express activated P2Y12 receptor in patients with diabetes mellitus. Circulation (2017) 136:817–33. doi: 10.1161/CIRCULATIONAHA.116.026995
34. Prabhakaran S, Wells KR, Lee VH, Flaherty CA, Lopes DK. Prevalence and risk factors for aspirin and clopidogrel resistance in cerebrovascular stenting. AJNR Am J Neuroradiol. (2008) 29:281–5. doi: 10.3174/ajnr.A0818
35. Reavey-Cantwell JF, Fox WC, Reichwage BD, Fautheree GL, Velat GJ, Whiting JH, et al. Factors associated with aspirin resistance in patients premedicated with aspirin and clopidogrel for endovascular neurosurgery. Neurosurgery (2009) 64:890–5; discussion 5–6. doi: 10.1227/01.NEU.0000341904.39691.2F
36. Adeeb N, Griessenauer CJ, Foreman PM, Moore JM, Shallwani H, Motiei-Langroudi R, et al. Use of platelet function testing before pipeline embolization device placement: a multicenter cohort study. Stroke (2017) 48:1322–30. doi: 10.1161/STROKEAHA.116.015308
37. Shahin MH, Johnson JA. Clopidogrel and warfarin pharmacogenetic tests: what is the evidence for use in clinical practice? Curr Opin Cardiol. (2013) 28:305–14. doi: 10.1097/HCO.0b013e32835f0bbc
38. Hong JH, Sohn SI, Kwak J, Yoo J, Chang HW, Kwon OK, et al. Dose-dependent effect of statin pretreatment on preventing the periprocedural complications of carotid artery stenting. Stroke (2017) 48:1890–4. doi: 10.1161/STROKEAHA.117.016680
39. Brar SS, Ten Berg J, Marcucci R, Price MJ, Valgimigli M, Kim HS, et al. Impact of platelet reactivity on clinical outcomes after percutaneous coronary intervention. A collaborative meta-analysis of individual participant data. J Am Coll Cardiol. (2011) 58:1945–54. doi: 10.1016/j.jacc.2011.06.059
40. Stone GW, Witzenbichler B, Weisz G, Rinaldi MJ, Neumann FJ, Metzger DC, et al. Platelet reactivity and clinical outcomes after coronary artery implantation of drug-eluting stents (ADAPT–DES): a prospective multicentre registry study. Lancet (2013) 382:614–23. doi: 10.1016/S0140-6736(13)61170-8
41. Cho SM, Deshpande A, Pasupuleti V, Hernandez AV, Uchino K. Radiographic and clinical brain infarcts in cardiac and diagnostic procedures: a systematic review and meta-analysis. Stroke (2017) 48:2753–9. doi: 10.1161/STROKEAHA.117.017541
Keywords: clopidogrel resistance, carotid stenosis, stroke, ischemia, ticlopidine, surrogate endpoint
Citation: Chung J-W, Kim SJ, Hwang J, Lee MJ, Lee J, Lee K-Y, Park M-S, Sung SM, Kim KH, Jeon P and Bang OY (2019) Comparison of Clopidogrel and Ticlopidine/Ginkgo Biloba in Patients With Clopidogrel Resistance and Carotid Stenting. Front. Neurol. 10:44. doi: 10.3389/fneur.2019.00044
Received: 31 July 2018; Accepted: 14 January 2019;
Published: 30 January 2019.
Edited by:
Bruce Campbell, The University of Melbourne, AustraliaReviewed by:
Claus Ziegler Simonsen, Aarhus University Hospital, DenmarkCopyright © 2019 Chung, Kim, Hwang, Lee, Lee, Lee, Park, Sung, Kim, Jeon and Bang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oh Young Bang, b2h5b3VuZy5iYW5nQHNhbXN1bmcuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.