 Oleg A. Levada
Oleg A. Levada Alexandra S. Troyan
Alexandra S. Troyan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 16 July 2018
Sec. Stroke
Volume 9 - 2018 | https://doi.org/10.3389/fneur.2018.00577
Poststroke depression (PSD) is the most prevalent psychiatric disorder after stroke, which is independently correlated with negative clinical outcome. The identification of specific biomarkers could help to increase the sensitivity of PSD diagnosis and elucidate its pathophysiological mechanisms. The aim of current study was to review and summarize literature exploring potential biomarkers for PSD diagnosis. The PubMed database was searched for papers published in English from October 1977 to December 2017, 90 of which met inclusion criteria for clinical studies related to PSD biomarkers. PSD biomarkers were subdivided into neuroimaging, molecular, and neurophysiological. Some of them could be recommended to support PSD diagnosing. According to the data, lesions affecting the frontal-subcortical circles of mood regulation (prefrontal cortex, basal nuclei, and thalamus) predominantly in the left hemisphere can be considered as neuroimaging markers and predictors for PSD for at least 1 year after stroke. Additional pontine and lobar cerebral microbleeds in acute stroke patients, as well as severe microvascular lesions of the brain, increase the likelihood of PSD. The following molecular candidates can help to differentiate PSD patients from non-depressed stroke subjects: decreased serum BDNF concentrations; increased early markers of inflammation (high-sensitivity C-reactive protein, ferritin, neopterin, and glutamate), serum pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-18, IFN-γ), as well as pro-inflammatory/anti-inflammatory ratios (TNF-α/IL-10, IL-1β/IL-10, IL-6/IL-10, IL-18/IL-10, IFN-γ/IL-10); lowered complement expression; decreased serum vitamin D levels; hypercortisolemia and blunted cortisol awakening response; S/S 5-HTTLPR, STin2 9/12, and 12/12 genotypes of the serotonin transporter gene SLC6A4, 5-HTR2a 1438 A/A, and BDNF met/met genotypes; higher SLC6A4 promoter and BDNF promoter methylation status. Neurophysiological markers of PSD, that reflect a violation of perception and cognitive processing, are the elongation of the latency of N200, P300, and N400, as well as the decrease in the P300 and N400 amplitude of the event-related potentials. The selected panel of biomarkers may be useful for paraclinical underpinning of PSD diagnosis, clarifying various aspects of its multifactorial pathogenesis, optimizing therapeutic interventions, and assessing treatment effectiveness.
Poststroke depression (PSD) is the most prevalent psychiatric disorder after stroke, which affects nearly one-third of the survivors during first 5 years after disease onset (1–3). The diagnosis of PSD includes the following characteristics: (1) presence of major/minor depressive episode according to DSM-III-IV-5 or other valid approaches; (2) evidence of stroke from history, physical examination, and/or neuroimaging data; and (3) onset of PSD is temporally related to the stroke (3). Several epidemiological findings have demonstrated that PSD is independently linked to negative clinical outcomes, such as significantly longer hospitalization; more severe functional disability (3–6); profound diminutions in physical, psycho-social, cognitive, and eco-social domains of quality of life (3, 7); unsatisfactory results of poststroke rehabilitation (8); elevated rates of mortality (3, 9–11); higher risks of recurrent stroke at 1 year (12); as well as considerable strain for caregivers (13). Data mentioned above highlight the importance of identifying PSD among stroke survivors.
The detection of depressive symptoms at early stroke stages and recognition subjects at risk for PSD diagnosis remains challenging. Clinical measures currently used to assess PSD, especially in the acute poststroke patients, may lack the specificity necessary to detect symptoms (14, 15). From this point of view, the identification of specific biomarkers might help to increase the sensitivity of PSD diagnosis. Moreover, it could be helpful for elucidating the pathophysiological mechanisms of PSD and ultimately lead to choosing specific targeted treatment (16).
Thus, we aimed to review and summarize the literature exploring potential biomarkers for PSD diagnosis.
We searched PubMed database for studies published in English using keywords: “poststroke depression” and “depression after stroke.” The search covered a period from October 1977 to December 2017. We also reviewed the reference lists of obtained articles for additional information. Further, human clinical articles related to biomarkers of PSD were subjected to a comprehensive analysis. The inclusion criteria were: (1) peer-reviewed original studies with case-control design and all types of reviews, where the relationship between PSD and possible biomarkers was studied; (2) age of participants ≥ 18 years; (3) patients had ischemic or hemorrhage stroke at the time of entry; (4) valid instruments for PSD assessment; (5) standardized measurements for biomarkers. We excluded duplicate articles with the same data set and studies without sufficient data. All articles were reviewed and analyzed by the first author (O.L.). Received results were checked for accuracy by the second investigator (A.T.). Discrepancies if occurred were resolved by discussion and consensus.
At the first stage, 764 clinical and experimental articles were identified, 90 of which met inclusion criteria and underwent a detailed analysis at the second stage (Figure 1). The results of included studies were subdivided according to the type of investigated biomarkers into neuroimaging, molecular, and neurophysiological. In turn, molecular PSD biomarkers were categorized into monoamines, growth factors, markers of neuroinflammation, markers of the hypothalamic-pituitary-adrenal axis, markers of oxidative damage, other metabolites, and genetic markers for convenient structural representation of the data obtained.
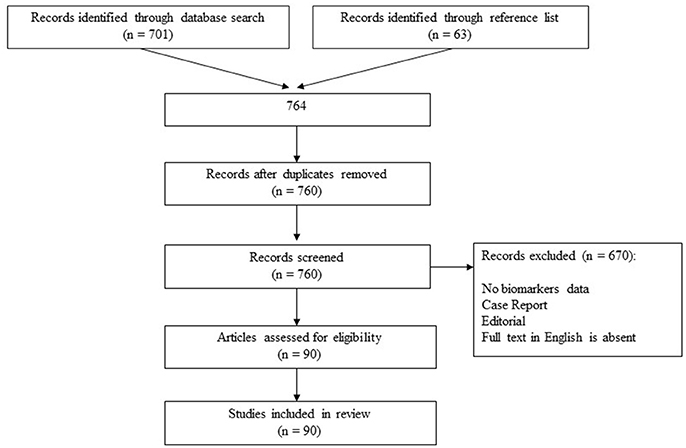
Figure 1. Study selection process.
In spite of being one of the straight roots of depression, a question if a stroke-determined neuroanatomical substrate is actually contributing to the development of PSD remains a matter of debate (17, 18). The results of neuroimaging research in PSD patients are presented in Table 1. Methodological peculiarities of the main studies allow having an idea of the importance of clinical-anatomical relationships in this cohort of patients.
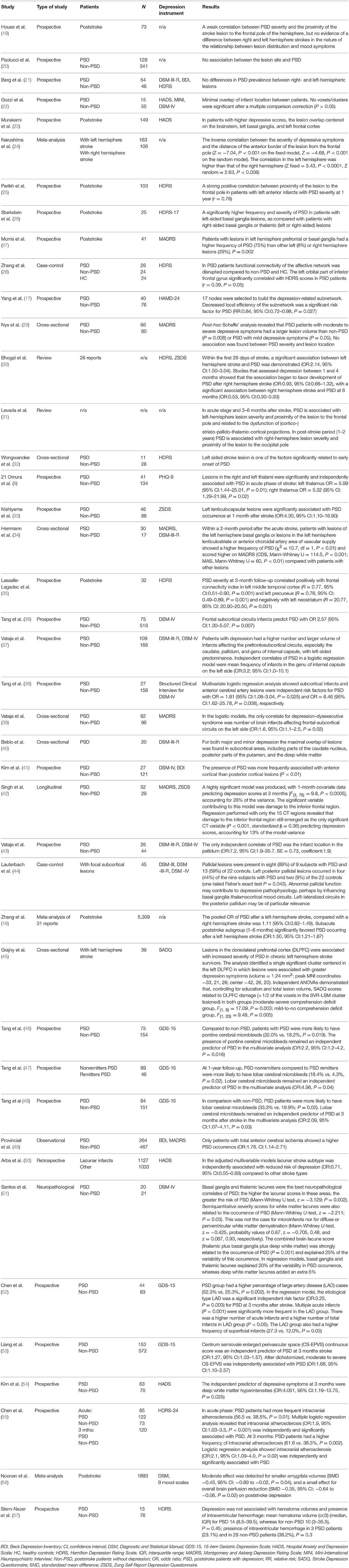
Table 1. Summary of neuroimaging biomarkers of PSD.
The results of some well-organized studies using different MRI/CT techniques do not yield evidence that lesions in a distinct neuroanatomical region induce PSD (19–22). In contrast, a large number of clinical-neuroimaging investigations found significant associations between stroke location and PSD. Murakami et al. revealed that PSD was associated with infarcts located in the left frontal cortical region, left basal ganglia, and brainstem (23). These data are partially in line with the earlier results, which pointed to the importance of closeness of the damage focus to the left frontal pole (24), involving prefrontal or basal ganglia structures (25–27), for the PSD appearance.
A resting-state functional MRI study (28) identified changes in the affective network in PSD subjects and revealed that the stroke of the left orbital part of the inferior frontal gyrus was tightly associated with PSD severity. Yang et al. studied the neuroanatomical basis of PSD in relation to white matter connectivity (17). The researchers separated 17 nodes to construct a PSD-related subnetwork. They demonstrated that local efficiency of the subnetwork was significantly declined and this functional decrease was a predictor of PSD (RR:0.84, 95% CI:0.72–0.98). Damages in the left putamen, right insular cortex, and right superior longitudinal fasciculus were found to be correlated with PSD. According to Nys et al., PSD was connected to lesion size but not to lesion location (29).
The discrepancies among studies could be explained by the fact that the relationship between the stroke focus and the likelihood of developing depression may depend on the time since the onset of an acute cerebrovascular accident (30, 31). A large amount of data confirming this point of view has been accumulated. Left-sided stroke lesion was a factor contributing to early onset of PSD (in 2 weeks) (32). Thalamic lesions were significantly associated with PSD in the acute stage of stroke (8). Left lenticulocapsular infarcts were an independent predictor of depressive symptoms at 1 month after stroke onset (33). These data are in agreement with one of the earliest CT-investigations, which revealed the importance of the left hemisphere and basal ganglia lesions for PSD existence at 2 months of the disease (34).
The results of Lassalle-Lagadec et al. study demonstrated that a deterioration of default mode network, which play a key role in mood control, was correlated with PSD severity (35). The investigators revealed that the PSD score at 3-month follow-up was associated with changes in functional connectivity of the left middle temporal cortex and precuneus at 10 days after a first stroke. Ischemic lesions in the frontal-subcortical paths were significantly correlated with depression in contrast to non-depressed subjects at 3 months after stroke onset (36). Moreover, in further logistic regression analysis after adjusting for relevant confounders the relationship (OR:2.6, 95% CI:1.3–5.1) was still significant. Similar data about the crucial role of frontal-subcortical lesions with left-sided predominance (37–39) or without it (40–42) for PSD were also received earlier. Furthermore, Vataja et al. and Lauterbach et al. pointed to the special role of the left pallidum lesions for the onset of PSD (43, 44).
According to a meta-analysis of 31 reports involving 5,309 subjects (18), patients with left hemisphere infarcts might be more vulnerable to PSD during first 6 months after disease onset (OR:1.5, 95% CI:1.2–1.9). Lesions in the left dorsolateral prefrontal cortex are linked to more severe PSD in chronic poststroke patients (45).
It was demonstrated that additional pontine microbleeds in acute ischemic stroke patients significantly increased the possibility of PSD (46), whereas lobar microbleeds decreased the remission rate of PSD (47). Tang et al. also received results, which suggested that lobar microbleeds might be crucial for the PSD onset in subjects with lacunar infarcts (48).
The results of some studies revealed that the type of ischemic stroke might be a risk factor for PSD. Subjects with total anterior cerebral infarcts had a greater prevalence of depression (OR:1.76, 95% CI:1.1–2.7) (49). At the same time, Arba et al., exploring the association between different subcortical ischemic stroke lesions and occurrence of PSD at 1 year after disease onset, established that the lacunar subtype was least associated with PSD (OR:0.71, 95% CI:0.55–0.93) compared to other stroke variants (50). Nevertheless, accumulation of subcortical lacunar lesions in the deep white matter, basal ganglia, and thalamus might be a more significant predictor of PSD than solitary lacunas (51, 52).
In some studies, the influence of different types of cerebral vasculopathy for PSD in ischemic stroke patients was assessed. Enlarged perivascular spaces (markers of cerebral small vessel disease) in the centrum semiovale on axial T2 weighted MRI independently predicted PSD occurrence at a 3-month period after stroke, according to the Liang et al. data (53). Severe white matter hyperintensities, another cerebral sign that reflects cerebral microvasculopathy, were identified as an independent factor of PSD at 3 months after stroke onset (54). Moreover, intracranial atherosclerosis on MRI scans might be essential for prediction of PSD in ischemic stroke subjects (55). In general, mentioned data are in accordance with the meta-analytical evidence that the reduction of overall brain perfusion has an impact on PSD (56).
Few studies have examined clinical and neuroimaging correlations of PSD after hemorrhagic stroke. Stern-Nezer et al. after investigating 89 patients with spontaneous intracerebral hemorrhage concluded that PSD was not associated with hematoma volumes and presence of intraventricular hemorrhage (57).
Summarizing obtained neuroimaging data in PSD patients, the conclusion can be made that clinical-anatomical correlations were found only for ischemic stroke lesions. Localization of the focus, the volume of ischemia, and additional burdening anatomical factors were contributing to PSD occurrence. For 1 year after the stroke onset, lesions affecting the frontal-subcortical affective network (prefrontal cortex, basal nuclei, and thalamus) predominantly in the left hemisphere can be considered as neuroimaging markers for PSD and as predictors of PSD development. Total anterior cerebral infarcts lead to a higher PSD occurrence, whereas lacunar lesions less often cause depression symptoms. Supplementary pontine and lobar cerebral microbleeds in acute stroke patients, as well as severe brain microvasculopathy, increase the likelihood of PSD.
Molecular markers of PSD are presented in Table 2. It was revealed that PSD patients had significantly lower liquor concentrations of 5-hydroxyindoleacetic acid (a 5-HT metabolite) compared to non-depressed subjects with acute stroke lesions and non-depressed patients without stroke lesions (92). The results demonstrate that serotonergic mechanisms are implicated in PSD pathogenesis. Nevertheless, these data need to be further confirmed.
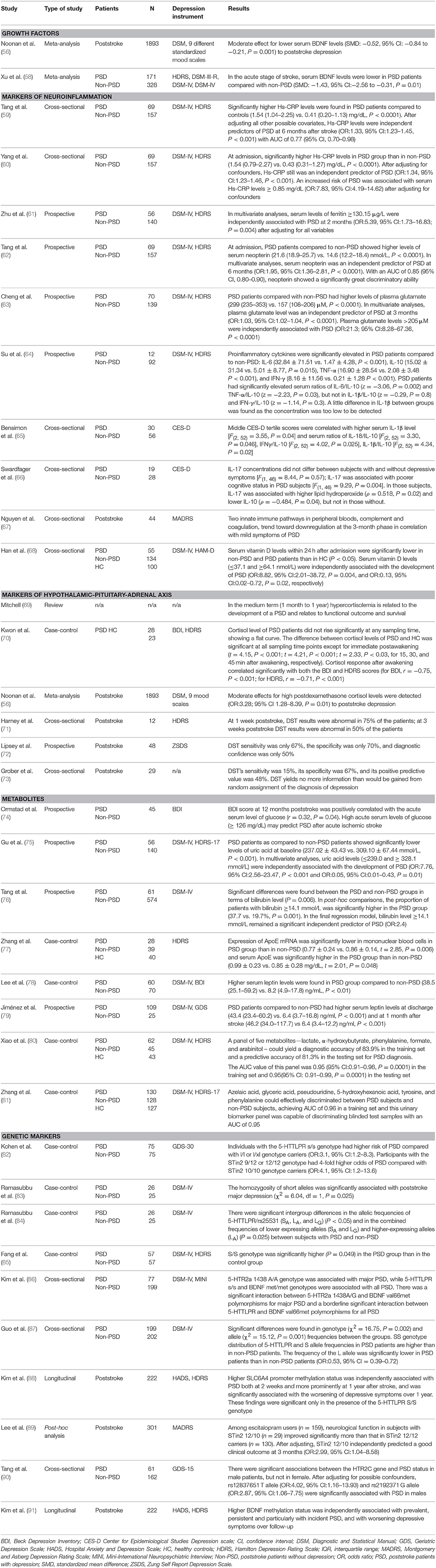
Table 2. Summary of molecular biomarkers of PSD.
Accumulating evidence shows that expression of brain-derived neurotrophic factor (BDNF) is involved in the pathophysiological mechanisms of depression (93) and PSD (94). A meta-analysis of four studies including 499 stroke patients (58) revealed that significant decrease in serum BDNF concentrations in the early period after stroke predisposed to the development of depression. The data correspond to the results of an earlier meta-analysis Noonan et al. (56).
A growing amount of evidence indicates the pathogenic influence of insulin-like growth factor 1 (IGF-1) on a major depressive disorder (MDD) (95). Most of the studies showed that increased peripheral IGF-1 levels might predict the occurrence of MDD, whereas decreased IGF-1 levels might reflect the treatment effectiveness (96). Nevertheless, Yue et al. found no differences in serum IGF-1 concentrations in PSD patients as opposed to non-depressed poststroke patients and persons with MDD (97). On the other hand, the authors revealed significantly greater serum IGF-1 mRNA concentrations in PSD group compared to depressed subjects without stroke (97).
Therefore, the decrease of serum BDNF concentrations after stroke can be used as a PSD predictor.
Despite serious methodological issues, current research found that immune dysfunction is crucial for the pathophysiology of PSD (98). Immunological mechanisms can initiate the inflammation-bound cell death in mood-related cerebral areas (99). Therefore, markers of neuroinflammation could be helpful for PSD diagnosing.
It was shown that increased early markers of inflammation predicted further PSD development. Tang et al. found that elevated serum concentrations of high-sensitivity C-reactive protein (Hs-CRP) in the acute stroke phase independently predisposed to PSD occurrence at 6 months after its onset (OR:1.3, 95% CI:1.2–1.5, and AUC value of 0.765, 95% CI:0.701–0.983) (59). Similar results were published by Yang et al. (60). The authors also established that higher risk of PSD is related to serum Hs-CRP concentrations ≥ 0.85 mg/dL (OR:7.8, 95% CI:4.2–14.6) (60).
Serum level of ferritin (an inflammatory acute phase protein) ≥ 130.15 μg/L was independently related to depression after a 2-month period of stroke onset (OR:5.4, 95% CI:1.7–16.8) in accordance with Zhu et al. (61). Patients with PSD showed higher levels of serum neopterin (a marker of cellular immune system activation) at admission compared with non-depressive poststroke subjects (21.6 vs. 14.6 nmol/L) (62). Furthermore, serum neopterin independently predicted PSD occurrence after 6 months of stroke onset (OR:1.95, 95% CI:1.36–2.81) and demonstrated a prominently higher discriminatory ability when compared to Hs-CRP.
Increased plasma glutamate concentrations (>205 μM) at early stage predicted PSD development at 3 months after stroke (OR:21.3, 95% CI:8.3–67.4) (63). It was suggested that glutamate has an inflammatory potential due to its ability to initiate immunological processes in the nervous system (100).
Particular attention has been paid to cytokine-related markers of PSD. Su et al. found significant increases of several serum cytokines [tumor necrosis factor α (TNF-α), interleukin-6 (IL-6), interferon-γ (IFNγ)], as well as in the pro-inflammatory/anti-inflammatory ratios of TNF-α/IL-10 and IL-6/IL-10 in PSD subjects after 1, 3, 6, 9, and 12 months of stroke (64). Interleukin-1β was too low to show any difference (64). Moreover, Bensimon et al. showed that serum concentrations of pro-inflammatory cytokine IL-1β and serum pro-inflammatory/anti-inflammatory ratios of IL-18/IL-10, IFNγ/IL-10, and IL-1β/IL-10 were increased in patients with moderate severity of PSD (65). At the same time, peripheral kynurenine/tryptophan ratios, which had been earlier suggested to connect neuroinflammatory, neurotoxical, and neurotransmitter processes, were not associated with PSD (65).
Interestingly, IL-17 serum levels did not distinguish poststroke patients with and without PSD in Swardfager et al. study (66). Nevertheless, IL-17 was correlated with lower cognitive functioning in PSD patients. In those depressive individuals, IL-17 was related to increased lipid hydroperoxide, a measure of oxidative stress (ρ = 0.52), and decreased IL-10 (ρ = −0.48), in contrast to subjects without PSD (66). Authors concluded that cognitive PSD symptoms might be linked to IL-17 related signaling, including pro-inflammatory and anti-inflammatory imbalance and hyperoxidation.
Cytokines can realize their pathogenic impact by driving intrinsic apoptotic pathways, involving intracellular calcium, glutamate excitotoxicity, and reactive oxygen species, which significantly elevates the risk of depression (99). It was also hypothesized that the increased production of pro-inflammatory cytokines due to stroke may amplify the pro-inflammatory processes, predominantly in limbic regions, extensively activate indoleamine 2, 3-dioxygenase, and, consequently, reduce serotonin production in paralimbic areas, including ventral lateral frontal and polar temporal cortex, as well as basal ganglia. The sequential physiological dysregulation might result in PSD (101).
The complement system is usually considered to be an essential part of the innate immunity and a linkage to the acquired immunity throughout pro-inflammatory cytokine transmission. Nguyen et al. revealed that lowered complement expression in serum was associated with PSD symptoms at 3 months after stroke (67).
Some studies revealed that decreased concentrations of vitamin D, which is essential for immunoregulation, were associated with depression in poststroke patients (68, 102). PSD subjects had significantly decreased serum concentrations of vitamin D within 24 h after admission compared to non-depressed individuals. Serum vitamin D lower than 37.1 nmol/L were independently related to the onset of PSD (OR:8.8, 95% CI:2.0–38.7) (68).
Thus, increased early markers of inflammation (Hs-CRP, ferritin, neopterin, and glutamate), in addition to elevated serum pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-18, IFN-γ) and pro-inflammatory/anti-inflammatory ratios (TNF-α/IL-10, IL-1β/IL-10, IL-6/IL-10, IL-18/IL-10, IFN-γ/IL-10) might be used for underpin of PSD diagnosis. PSD is also characterized by lowered complement expression and decreased serum vitamin D levels. The relationship between IL-17 levels and cognitive functioning in PSD patients need to be replicated in further investigations.
According to review (69), persistent HPA dysregulation occurs in up to 40% of stroke patients. The level of hypercortisolemia is moderately determined by the volume and location of the infarct. In 1-month to 1-year term after stroke onset hypercortisolemia is correlated with PSD (69). Kwon et al. compared the cortisol awakening response (measuring saliva cortisol directly, 15, 30, and 45 min after wakening) in PSD patients (2 months after a stroke or longer) with age-matched controls (70). In PSD group, salivary cortisol concentrations did not increase considerably at any measured time, demonstrating the blunted cortisol awakening response. Furthermore, a prominent adverse association between the cortisol awakening response and the severity of depression in PSD group was shown (70).
It was detected in the meta-analysis Noonan et al. that dexamethasone moderately suppressed elevated cortisol concentrations (OR:3.3, 95% CI:1.3–8.4) in PSD patients (56). Abnormal dexamethasone suppression test (DST) results at 3 weeks after stroke might be a potential PSD predictor (71). Nevertheless, some investigators declared low utility of the test. Thus, Lipsey et al. found that DST sensitivity and specificity was only 67 and 70%, respectively (72). Grober et al. indicated that the DST sensitivity and specificity was only 15 and 67%, respectively, whereas, the positive predictive value was 48% (73). Therefore, it was concluded that the DST provides no more information for PSD diagnosis (73).
Thereafter, it can be suggested that among HPA axis dysfunction markers, hypercortisolemia and the blunted cortisol awakening response are the most prominent in PSD patients.
A great amount of evidence suggests that stroke is accompanied by oxidative stress. Some studies investigated the links between oxidative stress and PSD. Cichon et al. evaluated a possible relationship between plasma protein oxidative damage and the likelihood of PSD (103). The research showed that oxidative proteins damage was associated with the severity of PSD. Liu et al. found a positive correlation between serum malondialdehyde (oxidative stress biomarker) levels and PSD severity (r = 0.54) during 1 month follow up after stroke onset (104). According to the ROC-analysis, the optimal cutoff value of serum malondialdehyde concentrations as an indicator to support a PSD diagnosis was 2.898 nmol/mL, which yielded a sensitivity and a specificity of 77.9 and 81.1%, respectively, with AUC of 0.883 (95% CI:0.836–0.929). Elevated malondialdehyde higher than 2.898 nmol/mL was an independent predictive marker of PSD (OR:24.3, 95% CI:9.5–62.4).
Nevertheless, specificity of mentioned oxidative markers for delineating PSD and non-PSD poststroke patients should be supported in larger sample studies. Therefore, they couldn't be recommended for routine clinical practice.
Evidence suggests that elevated acute serum glucose concentrations might be a predictor of PSD after ischemic stroke. The PSD score (according to Beck Depression Inventory) at 12 months after a stroke had a positive association with the serum glucose concentration at admission (r = 0.32) (74). The authors established that the acute glucose concentrations higher than 126 mg/dL could be a predictor of PSD occurrence.
Gu et al. examined a possible association between serum uric acid levels within 24 h after stroke onset and the development of PSD at a 3-month poststroke period (75). They demonstrated that uric acid concentrations lower than 239.0 and higher than 328.1 μmol/L were independently related to the onset of PSD (OR:7.76, 95% CI:2.56–23.47, and OR:0.05, 95% CI:0.01–0.43, respectively). Summarizing previously obtained data, authors concluded that possible antidepressant effects of uric acid could be explained by its multiple antioxidant (scavenging of free radicals and reactive oxygen species, chelation of transition metals, prevention of lipid peroxidation) and anti-inflammatory roles, decreasing blood-brain barrier permeability, and, consequently, diminishing central nervous tissue damage and neuronal death (75).
Substantial differences were established between the PSD and non-PSD patients with acute stroke regarding bilirubin concentrations (76). In post-hoc comparisons, the percentage of subjects with bilirubin ≥ 14.1 μmol/L was significantly greater among PSD patients (37.7 vs. 19.7%). After the final regression analysis, bilirubin concentration ≥ 14.1 μmol/L still independently predicted PSD. According to the authors‘ view, high bilirubin concentrations in PSD patients may reflect the intensity of initial oxidative stress, as well as indicate a higher level of perceived psychological stress (76).
ApoE plays a key role in lipid metabolism regulation. It was indicated that PSD individuals are more likely to demonstrate dyslipidemia and abnormal serum ApoE levels (105). Zhang et al. established that compared to non-depressed poststroke patients, PSD subjects had decreased peripheral ApoE microRNA expression and increased serum ApoE (77). Higher serum leptin (a hormone predominantly made by adipose cells) concentrations were found in PSD group in comparison with non-PSD poststroke individuals (38.5 vs. 8.2 ng/mL) (78). Increased serum levels of leptin at 7th and 30th day of poststroke also showed a correlation with later onset of PSD (79).
Xiao et al. used nuclear magnetic resonance spectroscopy-based metabonomic analysis to determine urine metabolites that are significantly altered in PSD patients (80). This approach could differentiate PSD patients from healthy control and non-depressed poststroke patients with high accuracy. Authors identified the panel of urinary metabolites, which included arabinitol, formate, lactate, phenylalanine, and α-hydroxybutyrate. They found that PSD patients had higher urine concentrations of lactate and α-hydroxybutyrate and lower urine concentrations of phenylalanine, formate, and arabinitol compared to healthy controls. The satisfactory predictability of the panel (AUC of 0.946) demonstrated that it could be a “good” classifier for PSD diagnosing (80).
Zhang and Zhang (81) proposed a combined panel of six urinary biomarkers (azelaic acid, glyceric acid, phenylalanine, pseudouridine, tyrosine, and 5-hydroxyhexanoic acid) that might separate PSD patients from non-depressed poststroke individuals with AUC of 0.961 in a training set and 0.954 in discriminating blinded test samples.
Overall, considerable amount of limitations including restricted ethnical groups, a single metabolomics platform, inability to differentiate PSD from stroke patients with other neuropsychiatric disorders, and the necessity to collect cerebrospinal fluid from PSD patients to ensure that mentioned above serum/plasma/urinary markers are relevant to the focus of disease pathogenesis require future multinational investigations with appropriate methodology.
A number of studies consider that PSD might be caused by genetic susceptibility. Much attention has been paid to the serotonin transporter gene SLC6A4 polymorphisms, especially 5-HTTLPR, STin2 VNTR, and rs25531. Summarizing data about them were presented in Kohen et al. review (82). The SERT gene is found on chromosome 17q11.1-17q12 and includes 14 exons. SERT most often studied variant 5-HTTLPR, which is found in the promoter region, is divided into a long (L) and short (S) allele, based on the absence or presence of a 43 bp deletion/insertion polymorphism. rs25531 is a single nucleotide polymorphism (SNP), existing in a common (A) or rare (G) variant, which location is immediately upstream of 5-HTTLPR in the SERT gene. A STin2 VNTR SERT polymorphism is situated in intron 2 and comprises a variable number of nearly equal 17 bp segments (usually 9, 10, or 12).
Several studies were devoted to the serotonin transporter gene-linked polymorphic region (5-HTTLPR) genotype in PSD subjects. Most studies showed that S/S (short allele) 5-HTTLPR genotype was significantly more frequent in PSD patients compared to non-depressed poststroke subjects (82–87). In contrast, LL (long allele) genotype was more prevalent in non-depressed poststroke subjects compared to PSD patients (87). This regularity can be explained by the fact that the transcription capacity of the S allele is lower to that of the L allele, leading to poor serotonin expression in the areas of action (106).
In addition to the 5-HTTLPR polymorphism, expression of SLC6A4 is influenced by DNA methylation status. Kim et al. found that hypermethylation of SLC6A4 promoter was independently related to PSD at 2 weeks and 1 year after ischemic brain incident. Moreover, it was significantly linked to the increase of depression severity during a 1-year poststroke period (88).
Stroke patients with the STin2 9/12 or 12/12 genotype showed a 4-fold elevated risk of PSD occurrence than individuals with STin2 10/10 genotype (OR:4.1, 95% CI:1.2–13.6) (82). It was also shown that serotonin transporter intron 2 (STin2) 12/10 variable number tandem repeat genotype might be associated with a good clinical outcome in PSD patients after 3 months of selective serotonin reuptake inhibitors (escitalopram) therapy (89). An association of rs25531 with PSD was not established (82).
Few studies assessed the association between some serotonin receptors (5-HTR) and growth factors genotypes and PSD. 5-HTR2a (serotonin 2a receptor) 1438 A/A genotype was linked to major PSD, whereas BDNF met/met genotype was linked to major as well as minor PSD (86). The authors found a substantial association between 5-HTR2a 1438A/G and BDNF val66met polymorphisms for major PSD and a marginally significant association between BDNF val66met polymorphisms for both (major and minor) PSD (86). Furthermore, Tang et al. established considerable interactions between the HTR2c gene and PSD presence in the male Chinese poststroke individuals (90). They showed that rs12837651 T allele and rs2192371 G allele significantly correlated to PSD status with OR of 4.02, 95% CI:1.16–13.93, and 2.87, 95% CI:1.06–7.75, respectively (90).
Along with genetic profiles, BDNF secretion is influenced by epigenetic factors. In this regard, Kim et al. (91) demonstrated that BDNF promoter hypermethylation independently correlated with the prevalence, persistence, and incidence of PSD, as well as with aggravating of depression severity over a 1-year period after stroke (91).
A potential role of microRNAs in PSD pathogenesis was observed in the review of experimental studies by Yan et al. (107). Implementation of those results into clinical practice may be helpful for the diagnosis and prognosis of PSD.
On the whole, genetic markers, namely S/S 5-HTTLPR, STin2 9/12, and 12/12 genotypes of the serotonin transporter gene SLC6A4, 5-HTR2a 1438 A/A, and BDNF met/met genotypes, can reflect the hereditary predisposition of PSD. To epigenetic factors of PSD, higher SLC6A4 promoter and BDNF promoter methylation status can be referred.
To assess abnormalities in EEG complexity in PSD subjects Zhang et al. used Lempel-Ziv Complexity (108). It was shown that PSD individuals had lower neural complexity in whole cerebral areas compared with poststroke non-depressed persons and healthy controls. As screening indicators for PSD, Lempel-Ziv Complexity parameters demonstrated more than 85% in specificity, sensitivity, and accuracy (Table 3). The lack of severe PSD patients in this study and absence of correlations between a stroke location and neurophysiological data do not allow expanding obtained data on the entire PSD population currently.
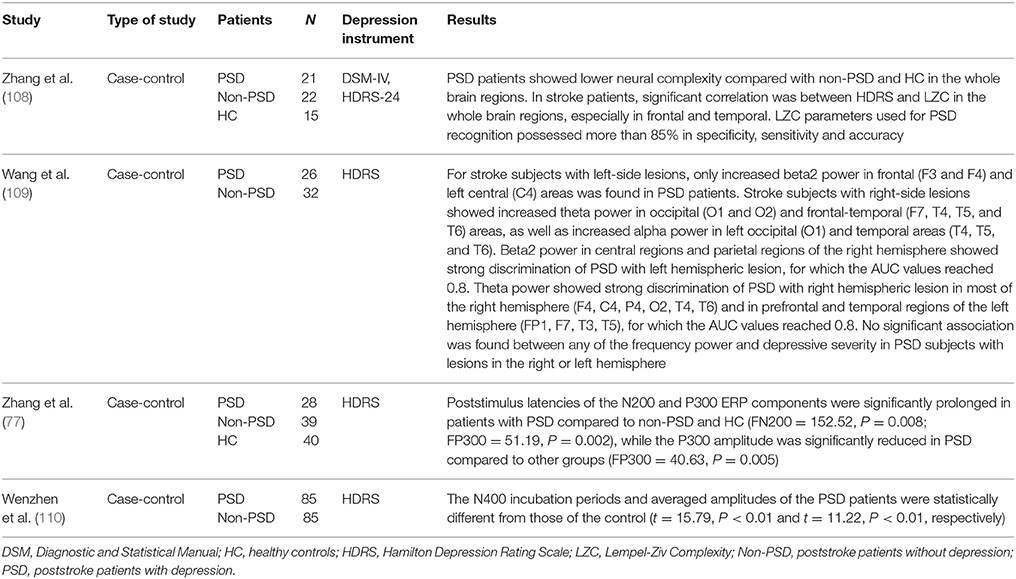
Table 3. Summary of neurophysiological markers of PSD.
Wang et al. examined quantitative EEG changes in PSD subjects with basal ganglia infarcts (109). Left-hemisphere PSD patients showed increased beta2 power in frontal and central areas, whereas right-hemisphere PSD ones showed increased theta and alpha power mainly in occipital and temporal regions. Additionally, for left-hemisphere lesions, beta2 power in central and right parietal regions provided high discrimination between PSD and poststroke non-depressed subjects, and for right-hemisphere lesions, theta power was similarly discriminative in most regions, especially in temporal regions. No relationship was found between the symptoms of depression and the power of abnormal bands. Small sample size of patients including basal ganglia lesions selectively do not provide an opportunity to recommend the methodology without replication in further studies.
Zhang et al. assessed event-related potentials (ERPs) in PSD patients (77). The average incubation period of N200 and P300 ERPs waves was prolonged, and the P300 amplitude was decreased in PSD subjects in comparison with non-PSD stroke patients and healthy individuals (P < 0.01). Wenzhen et al. also revealed that the incubation period of N400 was significantly prolonged and the average amplitude of the ERPs component was reduced in PSD group in comparison with those in the non-PSD group (110). These findings demonstrate that PSD subjects are prominently worse at recognizing target stimuli, indicating lower perceptual abilities and/or cognitive processing (77, 110). Therefore, neurophysiological markers of PSD, reflecting a violation of perception and cognitive processing, are the elongation of the latency of N200, P300, and N400, as well as a decrease in the P300 and N400 amplitude of the ERPs, could be used in the diagnosis process.
Summarizing obtained data, we can highlight that revealed biomarkers reflect complicated neurobiological mechanisms of PSD (111). They are caused by neuroanatomical substrates and involve different molecular signal pathways including serotonergic dysfunction, growth factors failure, neuroinflammation, HPA dysregulation, oxidative stress, and metabolic abnormalities. These acquired pathogenic mechanisms proceed against the background of a hereditary vulnerability, which links mainly to the serotonergic system of the brain and the mechanisms of neurotrophic support. Together, they lead to violations of emotional and cognitive processing. Some of them could be recommended to support the PSD diagnosis, while others need to be clarified before routine clinical use.
Concerning neuroimaging data, we can conclude that ischemic stroke lesion localization, its size, and additional burdening anatomical factors are pathogenically related to PSD. Lesions affecting the frontal-subcortical circles of mood regulation (prefrontal cortex, basal nuclei, and thalamus) predominantly in the left hemisphere can be considered as imaging markers for PSD and also as predictors of PSD development for at least 1 year after the stroke onset. Total anterior cerebral ischemia leads to a higher PSD occurrence; lacunar infarcts less often cause depression symptoms. Additional pontine and lobar cerebral microbleeds in acute stroke patients, as well as severe microvascular lesions of the brain, increase the likelihood of PSD occurrence. Considering that the maximal recovery after stroke is reached within the first year from its onset, it may be recommended to take into account the indicated localizations of stroke lesions in an acute period for preventive and therapeutic strategies of depression.
Resuming the studies on molecular markers, we can distinguish the following candidates, with the help of which PSD patients can be differentiated from non-depressed stroke patients. A significant decrease in serum BDNF concentrations at the early stage of stroke predisposes to the development of PSD. Increased early markers of inflammation (Hs-CRP, ferritin, neopterin, and glutamate), as well as serum pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-18, IFN-γ) and pro-inflammatory/anti-inflammatory ratios (TNF-α/IL-10, IL-1β/IL-10, IL-6/IL-10, IL-18/IL-10, IFN-γ/IL-10) are associated with PSD development. PSD is also characterized by lowered complement expression and decreased serum vitamin D levels. Hypercortisolemia and the blunted cortisol awakening response are the most prominent features of HPA axis dysfunction in PSD. In our view, studies of treatment effects directed on the above mentioned immunological and neuroendocrine mechanisms can validate these markers to be incorporated in routine clinical practice.
Genetic markers, namely S/S 5-HTTLPR, STin2 9/12 and 12/12 genotypes of the serotonin transporter gene SLC6A4, 5-HTR2a 1438 A/A and BDNF met/met genotypes, can reflect the genetic basis for the hereditary predisposition of PSD. To epigenetic markers of PSD, higher SLC6A4 promoter and BDNF promoter methylation status can be assigned.
Neurophysiological markers of PSD, reflecting a violation of perception and cognitive processing, are the elongation of the latency of N200, P300, and N400, as well as a decrease in the P300 and N400 amplitude of the ERPs. The validity of this biological marker should be additionally checked after antidepressant treatment.
In our opinion, taking into account previous remarks, the selected panel of biological markers may be useful for paraclinical underpinning of PSD diagnosis, clarifying various aspects of its multifactorial pathogenesis, optimizing therapeutic interventions, and assessing treatment effectiveness.
The validity of mentioned bellow markers for clinical practice has to be confirmed in further research. Among them are lower 5-hydroxyindoleacetic acid levels in cerebrospinal fluid, increased IL-17 serum levels, elevated serum concentrations of malondialdehyde and oxidative damage of proteins, high serum levels of glucose, uric acid, bilirubin, ApoE, and leptin together with changes in urine concentrations of arabinitol, azelaic acid, formate, glyceric acid, lactate, phenylalanine, pseudouridine, tyrosine, α-hydroxybutyrate, and 5-hydroxyhexanoic acid.
OL formulated the main concept, searched the literature, and wrote the manuscript. AT provided critical review and revision of the article. Both authors prepared the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Ayerbe L, Ayis S, Crichton S, Wolfe CD, Rudd AG. The natural history of depression up to 15 years after stroke: the South London Stroke Register. Stroke (2013) 44:1105–10. doi: 10.1161/STROKEAHA.111.679340
2. Babkair LA. Risk factors for poststroke depression: an integrative review. J Neurosci Nurs. (2017) 49:73–84. doi: 10.1097/JNN.0000000000000271
3. Towfighi A, Ovbiagele B, El Husseini N, Hackett ML, Jorge RE, Kissela BM, et al. Poststroke depression: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke (2017) 48:e30–43. doi: 10.1161/STR.0000000000000113
4. Sugawara N, Metoki N, Hagii J, Saito S, Shiroto H, Tomita T, et al. Effect of depressive symptoms on the length of hospital stay among patients hospitalized for acute stroke in Japan. Neuropsychiatr Dis Treat. (2015) 11:2551–6. doi: 10.2147/NDT.S91303
5. Ullberg T, Zia E, Petersson J, Norrving B. Perceived unmet rehabilitation needs 1 year after stroke: an observational study from the Swedish stroke register. Stroke (2016) 47:539–41. doi: 10.1161/STROKEAHA.115.011670
6. Karaahmet OZ, Gurcay E, Avluk OC, Umay EK, Gundogdu I, Ecerkale O, et al. Poststroke depression: risk factors and potential effects on functional recovery. Int J Rehabil Res. (2017) 40:71–5. doi: 10.1097/MRR.0000000000000210
7. Sarfo FS, Jenkins C, Singh A, Owolabi M, Ojagbemi A, Adusei N, et al. Post-stroke depression in Ghana: characteristics and correlates. J Neurol Sci. (2017) 379:261–5. doi: 10.1016/j.jns.2017.06.032
8. Omura T, Kimura M, Kim K, Mishina M, Mizunari T, Kobayashi S, et al. Acute poststroke depression is associated with thalamic lesions and clinical outcomes: a case-control study. J Stroke Cerebrovasc Dis. (2017) 27:499–505. doi: 10.1016/j.jstrokecerebrovasdis.2017.09.028
9. de Mello RF, Santos Ide S, Alencar AP, Benseñor IM, Lotufo PA, Goulart AC. Major depression as a predictor of poor long-term survival in a Brazilian stroke cohort (Study of Stroke Mortality and Morbidity in Adults) EMMA study. J Stroke Cerebrovasc Dis. (2016) 25:618–25. doi: 10.1016/j.jstrokecerebrovasdis.2015.11.021
10. Razmara A, Valle N, Markovic D, Sanossian N, Ovbiagele B, Dutta T, et al. Depression is associated with a higher risk of death among stroke survivors. J Stroke Cerebrovasc Dis. (2017) 26:2870–9. doi: 10.1016/j.jstrokecerebrovasdis.2017.07.006
11. Robinson RG, Jorge RE, Long J. Prevention of poststroke mortality using problem-solving therapy or escitalopram. Am J Geriatr Psychiatry (2017) 25:512–9. doi: 10.1016/j.jagp.2016.10.001
12. Yuan HW, Wang CX, Zhang N, Bai Y, Shi YZ, Zhou Y, et al. Poststroke depression and risk of recurrent stroke at 1 year in a Chinese cohort study. PLoS ONE (2012) 7:e46906. doi: 10.1371/journal.pone.0046906
13. Hung JW, Huang YC, Chen JH, Liao LN, Lin CJ, Chuo CY, et al. Factors associated with strain in informal caregivers of stroke patients. Chang Gung Med J. (2012) 35:392–401.
14. Li J, Oakley LD, Li Y, Luo Y. Development and initial validation of a clinical measure to assess early symptoms of post-stroke depression in the acute stroke patient. J Clin Nurs. (2017) 27:784–94. doi: 10.1111/jocn.14099
15. Ojagbemi A, Owolabi M, Akinyemi J, Ovbiagele B. Proposing a new stroke-specific screening tool for depression: examination of construct validity and reliability. eNeurol Sci. (2017) 9:14–8. doi: 10.1016/j.ensci.2017.10.002
16. Robinson RG, Jorge RE. Post-stroke depression: a review. Am J Psychiatry (2016) 173:221–31. doi: 10.1176/appi.ajp.2015.15030363
17. Yang S, Hua P, Shang X, Cui Z, Zhong S, Gong G, et al. A significant risk factor for poststroke depression: the depression-related subnetwork. J Psychiatry Neurosci. (2015)40:259–68. doi: 10.1503/jpn.140086
18. Zhang Y, Zhao H, Fang Y, Wang S, Zhou H. The association between lesion location, sex and poststroke depression: meta-analysis. Brain Behav. (2017) 7:e00788. doi: 10.1002/brb3.788
19. House A, Dennis M, Warlow C, Hawton K, Molyneux A. Mood disorders after stroke and their relation to lesion location. A CT scan study. Brain (1990) 113 (Pt 4):1113–29.
20. Paolucci S, Antonucci G, Pratesi L, Traballesi M, Grasso MG, Lubich S. Poststroke depression and its role in rehabilitation of inpatients. Arch Phys Med Rehabil. (1999) 80:985–90. doi: 10.1016/S0003-9993(99)90048-5
21. Berg A, Palomäki H, Lehtihalmes M, Lönnqvist J, Kaste M. Poststroke depression: an 18-month follow-up. Stroke (2003) 34:138–43. doi: 10.1161/01.STR.0000048149.84268.07
22. Gozzi SA, Wood AG, Chen J, Vaddadi K, Phan TG. Imaging predictors of poststroke depression: methodological factors in voxel-based analysis. BMJ Open (2014) 4:e004948. doi: 10.1136/bmjopen-2014-004948
23. Murakami T, Hama S, Yamashita H, Onoda K, Kobayashi M, Kanazawa J, et al. Neuroanatomic pathways associated with poststroke affective and apathetic depression. Am J Geriatr Psychiatry (2013) 21:840–7. doi: 10.1016/j.jagp.2013.01.057
24. Narushima K, Kosier JT, Robinson RG. A reappraisal of poststroke depression, intra- and inter-hemispheric lesion location using meta-analysis. J Neuropsychiatry Clin Neurosci. (2003) 15:422–30. doi: 10.1176/jnp.15.4.422
25. Parikh RM, Lipsey JR, Robinson RG, Price TR. A two year longitudinal study of poststroke mood disorders: prognostic factors related to one and two year outcome. Int J Psychiatry Med. (1988) 18:45–56. doi: 10.2190/LW46-3E9F-KYJM-WXGQ
26. Starkstein SE, Robinson RG, Berthier ML, Parikh RM, Price TR. Differential mood changes following basal ganglia vs thalamic lesions. Arch Neurol. (1988) 45:725–30. doi: 10.1001/archneur.1988.00520310031013
27. Morris PL, Robinson RG, Raphael B, Hopwood MJ. Lesion location and poststroke depression. J Neuropsychiatry Clin Neurosci. (1996) 8:399–403. doi: 10.1176/jnp.8.4.399
28. Zhang P, Xu Q, Dai J, Wang J, Zhang N, Luo Y. Dysfunction of affective network in post ischemic stroke depression: a resting-state functional magnetic resonance imaging study. Biomed Res Int. (2014) 2014:846830. doi: 10.1155/2014/846830
29. Nys GM, van Zandvoort MJ, van der Worp HB, de Haan EH, de Kort PL, Kappelle LJ. Early depressive symptoms after stroke: neuropsychological correlates and lesion characteristics. J Neurol Sci. (2005) 228:27–33. doi: 10.1016/j.jns.2004.09.031
30. Bhogal SK, Teasell R, Foley N, Speechley M. Lesion location and poststroke depression: systematic review of the methodological limitations in the literature. Stroke (2004) 35:794–802. doi: 10.1161/01.STR.0000117237.98749.26
31. Levada OA, Slivko EI. Post-stroke depression. Zh Nevrol Psikhiatr Im S S Korsakova (2006) 16:73–9.
32. Wongwandee M, Tangwongchai S, Phanthumchinda K. Relationship between poststroke depression and ischemic lesion location. J Med Assoc Thai. (2012) 95:330–6.
33. Nishiyama Y, Komaba Y, Ueda M, Nagayama H, Amemiya S, Katayama Y. Early depressive symptoms after ischemic stroke are associated with a left lenticulocapsular area lesion. J Stroke Cerebrovasc Dis. (2010) 19:184–9. doi: 10.1016/j.jstrokecerebrovasdis.2009.04.002
34. Herrmann M, Bartels C, Schumacher M, Wallesch CW. Poststroke depression. Is there a pathoanatomic correlate for depression in the postacute stage of stroke? Stroke (1995) 26:850–6. doi: 10.1161/01.STR.26.5.850
35. Lassalle-Lagadec S, Sibon I, Dilharreguy B, Renou P, Fleury O, Allard M. Subacute default mode network dysfunction in the prediction of post-stroke depression severity. Radiology (2012) 264:218–24. doi: 10.1148/radiol.12111718
36. Tang WK, Lu JY, Chen YK, Chu WC, Mok V, Ungvari GS, et al. Association of frontal subcortical circuits infarcts in poststroke depression: a magnetic resonance imaging study of 591 Chinese patients with ischemic stroke. J Geriatr Psychiatry Neurol. (2011) 24:44–9. doi: 10.1177/0891988710392375
37. Vataja R, Pohjasvaara T, Leppävuori A, Mäntylä R, Aronen HJ, Salonen O, et al. Magnetic resonance imaging correlates of depression after ischemic stroke. Arch Gen Psychiatry (2001) 58:925–31. doi: 10.1001/archpsyc.58.10.925
38. Tang WK, Chan SS, Chiu HF, Ungvari GS, Wong KS, Kwok TC, et al. Poststroke depression in Chinese patients: frequency, psychosocial, clinical, and radiological determinants. J Geriatr Psychiatry Neurol. (2005) 18:45–51. doi: 10.1177/0891988704271764
39. Vataja R, Pohjasvaara T, Mäntylä R, Ylikoski R, Leskelä M, Kalska H, et al. Depression-executive dysfunction syndrome in stroke patients. Am J Geriatr Psychiatry (2005) 13:99–107. doi: 10.1176/appi.ajgp.13.2.99
40. Beblo T, Wallesch CW, Herrmann M. The crucial role of frontostriatal circuits for depressive disorders in the postacute stage after stroke. Neuropsychiatry Neuropsychol Behav Neurol. (1999) 12:236–46.
41. Kim JS, Choi-Kwon S. Poststroke depression and emotional incontinence: correlation with lesion location. Neurology (2000) 54:1805–10.
42. Singh A, Black SE, Herrmann N, Leibovitch FS, Ebert PL, Lawrence J, et al. Functional and neuroanatomic correlations in poststroke depression: the Sunnybrook Stroke Study. Stroke (2000) 31:637–44. doi: 10.1161/01.STR.31.3.637
43. Vataja R, Leppävuori A, Pohjasvaara T, Mäntylä R, Aronen HJ, Salonen O, et al. Poststroke depression and lesion location revisited. J Neuropsychiatry Clin Neurosci. (2004) 16:156–62. doi: 10.1176/jnp.16.2.156
44. Lauterbach EC, Jackson JG, Wilson AN, Dever GE, Kirsh AD. Major depression after left posterior globus pallidus lesions. Neuropsychiatry Neuropsychol Behav Neurol. (1997) 10:9–16.
45. Grajny K, Pyata H, Spiegel K, Lacey EH, Xing S, Brophy C, et al. Depression symptoms in chronic left hemisphere stroke are related to dorsolateral prefrontal cortex damage. J Neuropsychiatry Clin Neurosci. (2016) 28:292–8. doi: 10.1176/appi.neuropsych.16010004
46. Tang WK, Liu XX, Chen YK, Abrigo J, Chu WC, Mok VC, et al. Pontine microbleeds and depression in stroke. J Geriatr Psychiatry Neurol. (2014) 27:159–64. doi: 10.1177/0891988714522699
47. Tang WK, Chen Y, Liang H, Chu WC, Mok VC, Ungvari GS, et al. Cerebral microbleeds as a predictor of 1-year outcome of poststroke depression. Stroke (2014) 45:77–81. doi: 10.1161/STROKEAHA.113.002686
48. Tang WK, Chen YK, Lu JY, Chu WC, Mok VC, Ungvari GS, et al. Cerebral microbleeds and depression in lacunar stroke. Stroke (2011) 42:2443–6. doi: 10.1161/STROKEAHA.111.614586
49. Provinciali L, Paolucci S, Torta R, Toso V, Gobbi B, Gandolfo C. Depression after first-ever ischemic stroke: the prognostic role of neuroanatomic subtypes in clinical practice. Cerebrovasc Dis. (2008) 26:592–9. doi: 10.1159/000165112
50. Arba F, Ali M, Quinn TJ, Hankey GJ, Lees KR, Inzitari D; VISTA Collaboration Lacunar infarcts, depression, and anxiety symptoms one year after stroke. J Stroke Cerebrovasc Dis. (2016) 25:831–4. doi: 10.1016/j.jstrokecerebrovasdis.2015.12.018
51. Santos M, Gold G, Kövari E, Herrmann FR, Bozikas VP, Bouras C, et al. Differential impact of lacunes and microvascular lesions on poststroke depression. Stroke (2009) 40:3557–62. doi: 10.1161/STROKEAHA.109.548545
52. Chen Y, Chen X, Mok VC, Lam WW, Wong KS, Tang WK. Poststroke depression in patients with small subcortical infarcts. Clin Neurol Neurosurg. (2009) 111:256–60. doi: 10.1016/j.clineuro.2008.10.008
53. Liang Y, Chan YL, Deng M, Chen YK, Mok V, Wang F, et al. Enlarged perivascular spaces in the centrum semiovale are associated with poststroke depression: a 3-month prospective study. J Affect Disord. (2017) 228:166–72. doi: 10.1016/j.jad.2017.11.080
54. Kim JT, Park MS, Yoon GJ, Jung HJ, Choi KH, Nam TS, et al. White matter hyperintensity as a factor associated with delayed mood disorders in patients with acute ischemic stroke. Eur Neurol. (2011) 66:343–9. doi: 10.1159/000332585
55. Chen YK, Qu JF, Xiao WM, Li WY, Li W, Fang XW, et al. Intracranial atherosclerosis and poststroke depression in Chinese patients with ischemic stroke. J Stroke Cerebrovasc Dis. (2016) 25:998–1004. doi: 10.1016/j.jstrokecerebrovasdis.2015.12.038
56. Noonan K, Carey LM, Crewther SG. Meta-analyses indicate associations between neuroendocrine activation, deactivation in neurotrophic and neuroimaging markers in depression after stroke. J Stroke Cerebrovasc Dis. (2013) 22:e124–35. doi: 10.1016/j.jstrokecerebrovasdis.2012.09.008
57. Stern-Nezer S, Eyngorn I, Mlynash M, Snider RW, Venkatsubramanian C, Wijman CAC, et al. Depression one year after hemorrhagic stroke is associated with late worsening of outcomes. NeuroRehabilitation (2017) 41:179–87. doi: 10.3233/NRE-171470
58. Xu HB, Xu YH, He Y, Xue F, Wei J, Zhang H, et al. Decreased serum brain-derived neurotrophic factor may indicate the development of poststroke depression in patients with acute ischemic stroke: a meta-analysis. J Stroke Cerebrovasc Dis. (2017) 27:709–15. doi: 10.1016/j.jstrokecerebrovasdis.2017.10.003
59. Tang CZ, Zhang YL, Wang WS, Li WG, Shi JP. Serum levels of high-sensitivity C-Reactive Protein at Admission Are More Strongly Associated with Poststroke depression in acute ischemic stroke than homocysteine levels. Mol Neurobiol. (2016) 53:2152–60. doi: 10.1007/s12035-015-9186-2
60. Yang RR, Lu BC, Li T, Du YF, Wang X, Jia YX. The relationship between high-sensitivity C-reactive protein at admission and post stroke depression: a 6-month follow-up study. Int J Geriatr Psychiatry (2016) 31:231–9. doi: 10.1002/gps.4315
61. Zhu L, Han B, Wang L, Chang Y, Ren W, Gu Y, et al. The association between serum ferritin levels and post-stroke depression. J Affect Disord. (2016) 190:98–102. doi: 10.1016/j.jad.2015.09.074
62. Tang CZ, Zhang YL, Wang WS, Li WG, Shi JP. Elevated serum levels of neopterin at admission predicts depression after acute ischemic stroke: a 6-month follow-up study. Mol Neurobiol. (2016) 53:3194–204. doi: 10.1007/s12035-015-9220-4
63. Cheng SY, Zhao YD, Li J, Chen XY, Wang RD, Zeng JW. Plasma levels of glutamate during stroke is associated with development of post-stroke depression. Psychoneuroendocrinology (2014) 47:126–35. doi: 10.1016/j.psyneuen.2014.05.006
64. Su JA, Chou SY, Tsai CS, Hung TH. Cytokine changes in the pathophysiology of poststroke depression. Gen Hosp Psychiatry (2012) 34:35–9. doi: 10.1016/j.genhosppsych.2011.09.020
65. Bensimon K, Herrmann N, Swardfager W, Yi H, Black SE, Gao FQ, et al. Kynurenine and depressive symptoms in a poststroke population. Neuropsychiatr Dis Treat. (2014) 10:1827–35. doi: 10.2147/NDT.S65740
66. Swardfager W, Herrmann N, Andreazza AC, Swartz RH, Khan MM, Black SE, et al. Poststroke neuropsychiatric symptoms: relationships with IL-17 and oxidative stress. Biomed Res Int. (2014) 2014:245210. doi: 10.1155/2014/245210
67. Nguyen VA, Carey LM, Giummarra L, Faou P, Cooke I, Howells DW, et al. A pathway proteomic profile of ischemic stroke survivors reveals innate immune dysfunction in association with mild symptoms of depression - a pilot study. Front Neurol (2016) 7:85. doi: 10.3389/fneur.2016.00085
68. Han B, Lyu Y, Sun H, Wei Y, He J. Low serum levels of vitamin D are associated with post-stroke depression. Eur J Neurol. (2015) 22:1269–74. doi: 10.1111/ene.12607
69. Mitchell AJ. Clinical implications of poststroke hypothalamo-pituitary adrenal axis dysfunction: a critical literature review. J Stroke Cerebrovasc Dis. (1997) 6:377–88. doi: 10.1016/S1052-3057(97)80038-9
70. Kwon OJ, Kim M, Lee HS, Sung KK, Lee S. The cortisol awakening response in patients with poststroke depression is blunted and negatively correlated with depressive mood. Biomed Res Int. (2015) 2015:709230. doi: 10.1155/2015/709230
71. Harney JH, Fulton C, Ross ED, Rush AJ. Dexamethasone suppression test and onset of poststroke depression in patients with ischemic infarction. J Clin Psychiatry (1993) 54:343–8.
72. Lipsey JR, Robinson RG, Pearlson GD, Rao K, Price TR. The dexamethasone suppression test and mood following stroke. Am J Psychiatry (1985) 142:318–23. doi: 10.1176/ajp.142.3.318
73. Grober SE, Gordon WA, Sliwinski MJ, Hibbard MR, Aletta EG, Paddison PL. Utility of the dexamethasone suppression test in the diagnosis of poststroke depression. Arch Phys Med Rehabil. (1991) 72:1076–9.
74. Ormstad H, Aass HC, Amthor KF, Lund-Sørensen N, Sandvik L. Serum levels of cytokines, glucose, and hemoglobin as possible predictors of poststroke depression, and association with poststroke fatigue. Int J Neurosci. (2012) 122:682–90. doi: 10.3109/00207454.2012.709892
75. Gu Y, Han B, Wang L, Chang Y, Zhu L, Ren W, et al. Low serum levels of uric acid are associated with development of poststroke depression. Medicine (2015) 94:e1897. doi: 10.1097/MD.0000000000001897
76. Tang WK, Liang H, Chu WC, Mok V, Ungvari GS, Wong KS. Association between high serum total bilirubin and post-stroke depression. Psychiatry Clin Neurosci. (2013) 67:259–64. doi: 10.1111/pcn.12051
77. Zhang Z, Mu J, Li J, Li W, Song J. Aberrant apolipoprotein E expression and cognitive dysfunction in patients with poststroke depression. Genet Test Mol Biomarkers (2013) 17:47–51. doi: 10.1089/gtmb.2012.0253
78. Lee JY, Lim OK, Lee JK, Park Y, Kim C, Yoon JW, et al. The association between serum leptin levels and post-stroke depression: a retrospective clinical study. Ann Rehabil Med. (2015) 39:786–92. doi: 10.5535/arm.2015.39.5.786
79. Jiménez I, Sobrino T, Rodríguez-Yáñez M, Pouso M, Cristobo I, Sabucedo M, et al. High serum levels of leptin are associated with post-stroke depression. Psychol Med. (2009) 39:1201–9. doi: 10.1017/S0033291709005637
80. Xiao J, Zhang J, Sun D, Wang L, Yu L, Wu H, et al. Discriminating poststroke depression from stroke by nuclear magnetic resonance spectroscopy-based metabonomic analysis. Neuropsychiatr Dis Treat. (2016)12:1919–25. doi: 10.2147/NDT.S110613
81. Zhang W, Zhang XA. A novel urinary metabolite signature for non-invasive post-stroke depression diagnosis. Cell Biochem Biophys. (2015) 72:661–7. doi: 10.1007/s12013-014-0472-9
82. Kohen R, Cain KC, Mitchell PH, Becker K, Buzaitis A, Millard SP, et al. Association of serotonin transporter gene polymorphisms with poststroke depression. Arch Gen Psychiatry (2008) 65:1296–302. doi: 10.1001/archpsyc.65.11.1296
83. Ramasubbu R, Tobias R, Buchan AM, Bech-Hansen NT. Serotonin transporter gene promoter region polymorphism associated with poststroke major depression. J Neuropsychiatry Clin Neurosci. (2006) 18:96–9. doi: 10.1176/jnp.18.1.96
84. Ramasubbu R, Tobias R, Bech-Hansen NT. Extended evaluation of serotonin transporter gene functional polymorphisms in subjects with post-stroke depression. Can J Psychiatry (2008) 53:197–201. doi: 10.1177/070674370805300310
85. Fang J, Yan W, Jiang GX, Li W, Cheng Q. Serotonin transporter gene polymorphism in Chinese patients with poststroke depression: a case-control study. Stroke (2011) 42:1461–3. doi: 10.1161/STROKEAHA.110.598672
86. Kim JM, Stewart R, Bae KY, Kim SW, Kang HJ, Shin IS. Serotonergic and BDNF genes and risk of depression after stroke. J Affect Disord. (2012) 136:833–40. doi: 10.1016/j.jad.2011.09.029
87. Guo WY, Zhang ZH, Mu JL, Liu D, Zhao L, Yao ZY, et al. Relationship between 5-HTTLPR polymorphism and post-stroke depression. Genet Mol Res. (2016) 15:gmr7460. doi: 10.4238/gmr.15017460
88. Kim JM, Stewart R, Kang HJ, Kim SW, Shin IS, Kim HR, et al. A longitudinal study of SLC6A4 DNA promoter methylation and poststroke depression. J Psychiatr Res. (2013) 47:1222–7. doi: 10.1016/j.jpsychires.2013.04.010
89. Lee EJ, Oh MS, Kim JS, Chang DI, Park JH, Cha JK, et al. Serotonin transporter gene polymorphisms may be associated with poststroke neurological recovery after escitalopram use. J Neurol Neurosurg Psychiatry (2017) 89:271–76. doi: 10.1136/jnnp-2017-316882
90. Tang WK, Tang N, Liao CD, Liang HJ, Mok VC, Ungvari GS, et al. Serotonin receptor 2C gene polymorphism associated with post-stroke depression in Chinese patients. Genet Mol Res. (2013) 12:1546–53. doi: 10.4238/2013.May.13.8
91. Kim JM, Stewart R, Kang HJ, Kim SY, Kim SW, Shin IS, et al. A longitudinal study of BDNF promoter methylation and genotype with poststroke depression. J Affect Disord. (2013) 149:93–9. doi: 10.1016/j.jad.2013.01.008
92. Bryer JB, Starkstein SE, Votypka V, Parikh RM, Price TR, Robinson RG. Reduction of CSF monoamine metabolites in poststroke depression: a preliminary report. J Neuropsychiatry Clin Neurosci. (1992) 4:440–2. doi: 10.1176/jnp.4.4.440
93. Levada OA, Cherednichenko NV. Brain-derived Neurotrophic Factor (BDNF): neurobiology and marker value in neuropsychiatry. Lik Sprava (2015) 15–25.
94. Li Y, Peng C, Guo X, You JJ, Yadav HP. Expression of brain-derived neurotrophic factor and tyrosine kinase B in cerebellum of poststroke depression rat model. Chin Med J. (2015) 128:2926–31. doi: 10.4103/0366-6999.168058
95. Szczesny E, Slusarczyk J, Głombik K, Budziszewska B, Kubera M, Lason W, et al. Possible contribution of IGF-1 to depressive disorder. Pharmacol Rep. (2013) 65:1622–31. doi: 10.1016/S1734-1140(13)71523-8
96. Levada OA, Troyan AS. Insulin-like growth factor-1: a possible marker for emotional and cognitive disturbances, and treatment effectiveness in major depressive disorder. Ann Gen Psychiatry (2017) 16:38. doi: 10.1186/s12991-017-0161-3
97. Yue Y, Jiang H, Liu R, Yin Y, Zhang Y, Liang J, et al. Towards a multi protein and mRNA expression of biological predictive and distinguish model for post stroke depression. Oncotarget (2016) 7:54329–38. doi: 10.18632/oncotarget.11105
98. Becker KJ. Inflammation and the Silent Sequelae of Stroke. Neurotherapeutics (2016) 13:801–10. doi: 10.1007/s13311-016-0451-5
99. Pascoe MC, Crewther SG, Carey LM, Crewther DP. Inflammation and depression: why poststroke depression may be the norm and not the exception. Int J Stroke (2011) 6:128–35. doi: 10.1111/j.1747-4949.2010.00565.x
100. Miller AH. Conceptual confluence: the kynurenine pathway as a common target for ketamine and the convergence of the inflammation and glutamate hypotheses of depression. Neuropsychopharmacology (2013) 38:1607–8. doi: 10.1038/npp.2013.140
101. Spalletta G, Bossù P, Ciaramella A, Bria P, Caltagirone C, Robinson RG. The etiology of poststroke depression: a review of the literature and a new hypothesis involving inflammatory cytokines. Mol Psychiatry (2006) 11:984–91. doi: 10.1038/sj.mp.4001879
102. Kaloglu A, Canbaz B, Kara O, Arik G, Sengul Aycicek G, Sumer F, et al. Low serum levels of vitamin D are associated with post-stroke depression. Eur J Neurol. (2016) 23:e27. doi: 10.1111/ene.12938
103. Cichon N, Bijak M, Miller E, Niwald M, Saluk J. Poststroke depression as a factor adversely affecting the level of oxidative damage to plasma proteins during a brain stroke. Oxid Med Cell Longev (2015) 2015:408745. doi: 10.1155/2015/408745
104. Liu Z, Zhu Z, Zhao J, Ren W, Cai Y, Wang Q, et al. Malondialdehyde: a novel predictive biomarker for post-stroke depression. J Affect Disord. (2017) 220:95–101. doi: 10.1016/j.jad.2017.05.023
105. Petkeviciene J, Smalinskiene A, Luksiene DI, Jureniene K, Ramazauskiene V, Klumbiene J, et al. Associations between apolipoprotein E genotype, diet, body mass index, and serum lipids in Lithuanian adult population. PLoS ONE (2012) 7:e41525. doi: 10.1371/journal.pone.0041525
106. Gonda X, Fountoulakis KN, Rihmer Z, Lazary J, Laszik A, Akiskal KK, et al. Towards a genetically validated new affective temperament scale: a delineation of the temperament phenotype of 5-HTTLPR using the TEMPS-A. J Affect Disord. (2009) 112:19–29. doi: 10.1016/j.jad.2008.03.012
107. Yan H, Fang M, Liu XY. Role of microRNAs in stroke and poststroke depression. Sci World J. (2013) 2013:459692. doi: 10.1155/2013/459692
108. Zhang Y, Wang C, Sun C, Zhang X, Wang Y, Qi H, et al. Neural complexity in patients with poststroke depression: a resting EEG study. J Affect Disord. (2015)188:310–8. doi: 10.1016/j.jad.2015.09.017
109. Wang C, Chen Y, Zhang Y, Chen J, Ding X, Ming D. Quantitative EEG abnormalities in major depressive disorder with basal ganglia stroke with lesions in different hemispheres. J Affect Disord. (2017) 215:172–178. doi: 10.1016/j.jad.2017.02.030
110. Wenzhen H, Cai D, Lin L, Fang Y, Zheng X. Clinical studies on event-related potentials (ERPs) N400 and the related factors in patients with poststroke depression (PSD). Int J Psychiatry Med. (2010) 40:349–59. doi: 10.2190/PM.40.3.i
Keywords: poststroke depression, neuroimaging biomarkers, molecular biomarkers, neurophysiological biomarkers, diagnosis
Citation: Levada OA and Troyan AS (2018) Poststroke Depression Biomarkers: A Narrative Review. Front. Neurol. 9:577. doi: 10.3389/fneur.2018.00577
Received: 08 February 2018; Accepted: 26 June 2018;
Published: 16 July 2018.
Edited by:
Rick Dijkhuizen, University Medical Center Utrecht, NetherlandsReviewed by:
Alejandro Bustamante, Hospital Universitari Vall d'Hebron, SpainCopyright © 2018 Levada and Troyan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oleg A. Levada, b2xldmFkYUB6bWFwby5lZHUudWE=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.